Paeds · respiratory-sleep-and-airway
Asthma diagnosis and long-term control
Also known as Asthma diagnosis and long-term control · Childhood asthma · Paediatric asthma management · Preschool wheeze and asthma · Reactive airways disease in children
Fellowship guide to the diagnosis and long-term control of asthma in children: recognising the variable, reversible airflow obstruction that defines the disease, confirming it with spirometry, bronchodilator reversibility and exhaled nitric oxide, distinguishing the preschool wheeze phenotypes and using the Asthma Predictive Index, separating current control from future risk, and delivering the stepwise controller ladder built on the inhaled corticosteroid — including the shift to anti-inflammatory reliever therapy from the SYGMA trials, the ICS-and-growth evidence from CAMP, and the written action plan.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Asthma is the commonest chronic disease of childhood, and yet it has no single confirmatory test — it is a clinical diagnosis built from a characteristic pattern of symptoms and the demonstration that airflow obstruction is both variable and reversible. The child has recurrent episodes of wheeze, cough, breathlessness and chest tightness that come and go, are worse at night and with triggers, and improve with a bronchodilator. The whole skill of paediatric asthma lies in confirming that pattern, excluding the mimics, and then keeping the airway quiet with the smallest effective treatment. [5] [10]
The reason the disease behaves this way is that the underlying lesion is chronic airway inflammation. Inflammation makes the airways twitchy, so they narrow excessively in response to triggers that a normal airway would ignore; the narrowing is intermittent, which is why symptoms are variable, and it is caused by smooth-muscle spasm and mucosal swelling that a bronchodilator and an inhaled corticosteroid can reverse, which is why the obstruction is reversible. Holding these two ideas — variable and reversible — in mind is what separates asthma from the fixed obstruction of a structural airway problem. [5]
Classification
Childhood asthma is classified along two independent axes that answer two different questions: what kind of asthma is this (the phenotype), and how well is it controlled right now (the level of control). Both matter, because the phenotype shapes the long-term prognosis and the choice of controller, while the level of control drives the day-to-day adjustment of therapy. [5] [10]
The phenotype axis is most useful in the preschool years, where wheeze is common but only a minority of wheezy toddlers become asthmatic school-age children. The Tucson cohort separated transient early wheezers, who wheeze with viral infections in the first three years and then grow out of it, from persistent wheezers, whose wheeze continues and who carry the allergic, atopic asthma phenotype. In practical terms preschool wheeze is grouped into episodic (viral) wheeze — discrete viral-triggered episodes with wellness in between — and multiple-trigger wheeze, where symptoms also occur between infections and the risk of true asthma is higher. [1] [5]
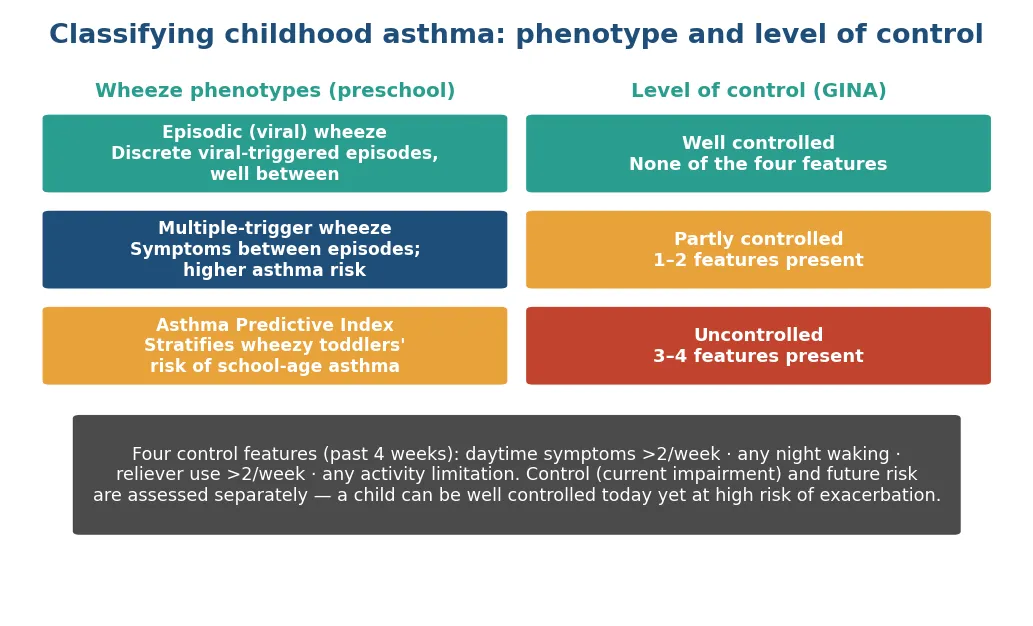
The control axis is the workhorse of every review. The Global Initiative for Asthma grades control over the preceding four weeks on four features: daytime symptoms more than twice a week, any night waking due to asthma, reliever needed more than twice a week, and any activity limitation. None of the four means well controlled; one or two means partly controlled; three or four means uncontrolled. Crucially, control (current impairment) is assessed separately from future risk — a child can be symptom-free today yet still carry a high risk of a severe exacerbation because of poor lung function, high reliever use or a recent flare. [10]
Epidemiology & Risk Factors
Asthma affects a large minority of children in high-income countries — of the order of one in ten — and both its prevalence and its severity are unequally distributed, falling hardest on socioeconomically disadvantaged and, in Australia and New Zealand, on Indigenous children. Recurrent wheeze in the preschool years is even commoner than asthma itself, which is why the central epidemiological task is not counting wheeze but predicting which wheezy toddlers will go on to have persistent disease. [1] [2]
The Tucson Children's Respiratory Study defined this natural history: most wheeze in the first three years is transient and viral, associated with smaller airways rather than atopy, and resolves; a smaller group has persistent atopic wheeze that becomes school-age asthma. The Asthma Predictive Index built on this by combining recurrent wheeze with major criteria (parental asthma, physician-diagnosed eczema) and minor criteria (allergic rhinitis, wheeze apart from colds, blood eosinophilia) to stratify a wheezy toddler's risk of later asthma. [1] [2]
The risk factors divide into the genetic and the environmental. Asthma is strongly heritable and polygenic — the GABRIEL genome-wide association study identified multiple susceptibility loci, including the 17q21 (ORMDL3) region for childhood-onset disease — and it clusters with the other atopic diseases (eczema, allergic rhinitis, food allergy) in the individual and the family. The environmental contributors are allergen sensitisation, viral respiratory infections in early life (rhinovirus and respiratory syncytial virus), tobacco smoke exposure including in utero, air pollution and obesity. The practical message is that atopy and a family history are the strongest predictors, and that modifiable exposures — above all tobacco smoke — are worth addressing at every visit. [6] [2]
Pathophysiology
Asthma is, at its root, a disease of chronic airway inflammation, and every feature of the disease flows from that single fact. In the sensitised, atopic child, a T-helper-2 (Th2) immune response drives eosinophilic inflammation of the airway wall: mast cells, eosinophils and their cytokines produce mucosal oedema, mucus hypersecretion and, over time, structural change. This inflamed airway is hyperresponsive — it narrows excessively in response to triggers, a property called bronchial hyperresponsiveness, so that an allergen, a virus, exercise or cold air that a normal airway tolerates provokes obstruction. [5]
When the airway narrows in asthma, three things are happening at once, and a bronchodilator and an anti-inflammatory treat them to different degrees. Bronchoconstriction — the acute spasm of airway smooth muscle — is the fastest and most reversible, and it is what a beta-agonist relieves within minutes. Airway wall oedema and mucus plugging are slower to develop and slower to resolve, and they respond to corticosteroid rather than bronchodilator. This is why the reliever eases the immediate wheeze but does nothing for the underlying disease, and why the controller is the treatment that matters. [5] [10]
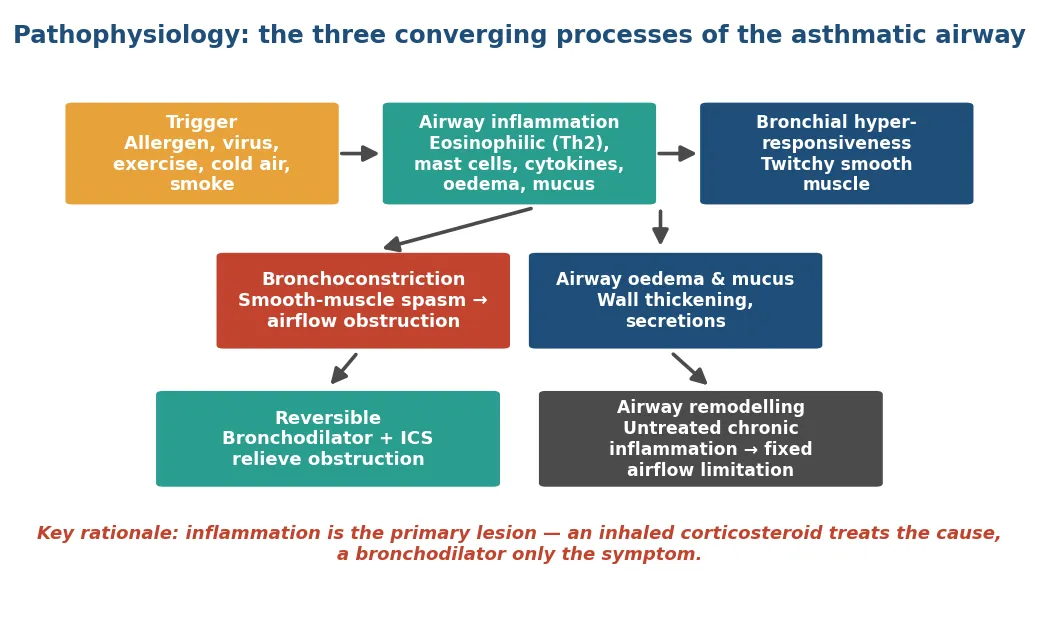
The final concept is airway remodelling. When the inflammation runs unchecked for years, the airway wall undergoes structural change — subepithelial fibrosis, smooth-muscle hypertrophy, angiogenesis and mucous-gland hyperplasia — that is only partly reversible and produces a component of fixed, no-longer-variable airflow limitation. Remodelling is the biological argument for treating the inflammation early and continuously rather than chasing symptoms with a reliever: an inhaled corticosteroid treats the primary lesion, whereas a bronchodilator only masks it, and it is the inflammation, left untreated, that permanently narrows the airway. [5] [3]
Clinical Presentation
The presentation of asthma is a pattern rather than a single symptom, and eliciting that pattern is the diagnosis. The core symptoms are recurrent wheeze (an expiratory, musical, polyphonic sound), cough (often dry and nocturnal), breathlessness and chest tightness. What makes them asthmatic is their behaviour: they are episodic and variable, worse at night and in the early morning, provoked by recognisable triggers, and relieved by a bronchodilator. A history that lacks this variability should prompt doubt about the diagnosis. [5] [10]
The triggers themselves are diagnostic clues and management targets. Viral upper respiratory infections are the commonest trigger of exacerbations in children; exercise-induced symptoms are characteristic, and cough or wheeze that appears a few minutes into running and settles with rest is a strong pointer; allergens (house dust mite, pet dander, pollens, moulds), cold air, cigarette smoke, and emotional upset or laughter all feature. A careful trigger history both supports the diagnosis and identifies the exposures — above all tobacco smoke and allergens — that can be reduced. [5]
Age changes the presentation. In the preschool child, wheeze is dominant and is usually viral-triggered, and the challenge is to decide whether it is transient viral wheeze or early asthma. In the school-age child and adolescent, the full pattern emerges with exercise limitation, nocturnal cough and clear trigger responses, and the new challenge is adherence and inhaler technique. In every age group the two symptoms that families most under-report — and that examiners most want you to ask about — are night waking and the exercise the child can no longer keep up with. [1] [10]
Differential Diagnosis
The differential of recurrent wheeze and cough in a child is wide, and the discipline is to keep the mimics in mind precisely because asthma is so common that it is over-diagnosed. The great imitators fall into groups: the structural airway lesions (an inhaled foreign body causing sudden monophonic wheeze, tracheomalacia or bronchomalacia, a vascular ring compressing the airway), the suppurative lung diseases (cystic fibrosis, primary ciliary dyskinesia and protracted bacterial bronchitis, all producing a chronic wet cough), and the systemic (immunodeficiency, gastro-oesophageal reflux, and cardiac failure with pulmonary congestion). [5]
Certain features should redirect the diagnosis away from asthma altogether. A chronic productive (wet) cough rather than a dry one, symptoms present from the neonatal period, failure to thrive, digital clubbing, focal or fixed chest signs, a monophonic rather than polyphonic wheeze, and — decisively — a failure to respond to an adequate trial of inhaled corticosteroid all argue against simple asthma and for one of the mimics. The single most useful discriminator is the therapeutic trial: asthma responds to inhaled corticosteroid, and the mimics do not. [5] [10]
In the adolescent, two functional mimics are worth naming because they are commonly missed. Inducible laryngeal obstruction (vocal cord dysfunction) produces inspiratory stridor and throat tightness that mimic an exacerbation but do not respond to bronchodilator and show a truncated inspiratory flow-volume loop. Dysfunctional breathing and hyperventilation produce breathlessness with normal spirometry. Recognising these avoids escalating asthma therapy in a child whose airways are not the problem. [5]
Clinical & Bedside Assessment
Bedside assessment in asthma is directed at three questions: is the diagnosis right, how well is the child controlled, and what is their future risk. The history does most of the work: characterise the pattern and its variability, list the triggers, quantify the symptoms over the last four weeks (daytime symptoms, night waking, reliever use, activity limitation), count reliever canisters used over the year, ask about exacerbations and admissions, and probe adherence and inhaler technique directly and non-judgementally. A child who says they "hardly ever" use the reliever but collects a canister a month is telling you two different things, and the pharmacy record settles it. [10]
Between exacerbations the physical examination is often entirely normal, which is itself consistent with asthma and must not be taken as reassurance that the disease is controlled. When signs are present they include an expiratory polyphonic wheeze, a prolonged expiratory phase, hyperinflation and, in poorly controlled chronic disease, a Harrison's sulcus. The examination also actively looks for the features that argue against asthma — clubbing, a wet cough, focal signs, failure to thrive — and for the associated atopic conditions (eczema, allergic rhinitis) that support it. [5]
The most instructive part of the assessment is watching the child use their inhaler. Poor inhaler technique and non-adherence are the two commonest reasons that asthma appears uncontrolled, and both are invisible unless specifically checked. Ask the child to demonstrate their device with the spacer they actually use, correct the technique, and confirm that a spacer is used with every metered-dose inhaler. Checking adherence, technique and trigger control is the mandatory first step before any escalation of therapy. [10] [12]
Investigations
Asthma has no single confirmatory test, so investigations aim to demonstrate variable airflow limitation objectively and to exclude the mimics. In a child old enough to perform it reliably — usually from about six years — spirometry is the key test. It shows an obstructive pattern (a reduced FEV1/FVC ratio) and, most importantly, reversibility: an improvement in FEV1 of 12 percent or more after a bronchodilator confirms the reversible obstruction that defines asthma. A normal spirogram between episodes does not exclude asthma, because the obstruction is by nature variable. [10] [5]
When resting spirometry is normal but the history is suggestive, variability can be sought in other ways: peak expiratory flow monitored over two weeks showing diurnal variability, an exercise or bronchial challenge test provoking a fall in FEV1, or a documented response to a trial of controller therapy. The fractional exhaled nitric oxide (FeNO) test measures eosinophilic airway inflammation and supports the diagnosis of the atopic, corticosteroid-responsive phenotype; the ATS guideline positions an elevated FeNO as evidence of eosinophilic inflammation and a likely steroid response, though it is an adjunct and not a stand-alone diagnostic test. [7] [10]
The remaining investigations are aimed at the differential rather than at confirming asthma. A chest radiograph is not routine but is obtained when the presentation is atypical — focal signs, a wet cough, suspected foreign body or failure to respond — and is typically normal in asthma. Allergy testing (skin prick or specific IgE) identifies sensitisations that guide trigger avoidance and phenotype. A sweat test, immunological workup or flexible bronchoscopy are reserved for the child whose features point to cystic fibrosis, immunodeficiency or a structural lesion. The guiding principle is to test to confirm variability and to exclude the mimics, not to test reflexively. [5] [10]
Management — Resuscitation
Although this topic is about long-term control, every child with asthma will at some point present with an acute exacerbation, and the fundamentals of that emergency belong here. The severity of an acute attack is graded at the bedside on the ability to speak, the respiratory and heart rate, the work of breathing, oxygen saturation and mental state; a silent chest, exhaustion, cyanosis, saturations below 92 percent and altered consciousness mark a life-threatening attack. The immediate treatment is oxygen to keep saturations at or above 94 percent, repeated inhaled short-acting beta-agonist (salbutamol, best delivered by metered-dose inhaler and spacer in mild-to-moderate attacks and by nebuliser in severe ones), and early systemic corticosteroid. [10] [12]
Salbutamol (acute paediatric asthma, MDI + spacer)
Loading dose
Age <6 years: 2–6 puffs (100 microgram/puff); age ≥6 years: 4–12 puffs, repeated every 20 minutes for the first hour as needed
Maintenance dose
Titrate frequency down to response; escalate to continuous nebulised salbutamol in severe or life-threatening attacks
Systemic corticosteroid is given early in any moderate or severe exacerbation because it treats the inflammatory basis of the attack and shortens its course; oral prednisolone (1 to 2 mg/kg, maximum 40 to 50 mg, for three to five days) is the usual choice, with intravenous steroid reserved for the child who cannot take oral medication. Severe and life-threatening attacks that do not respond to inhaled bronchodilator and steroid are escalated to inhaled ipratropium, intravenous magnesium sulfate, and intravenous bronchodilators (salbutamol or aminophylline) in a high-dependency or intensive-care setting. The child who deteriorates despite maximal therapy needs senior and intensive-care involvement early. [10] [12]
Immediate management of an acute paediatric asthma exacerbation
Assess severity: speech, respiratory and heart rate, work of breathing, saturations, mental state — recognise the silent chest and exhaustion of a life-threatening attack
Give oxygen to keep saturations at or above 94 percent
Give repeated inhaled salbutamol — MDI + spacer for mild-to-moderate, oxygen-driven nebuliser for severe attacks
Give early systemic corticosteroid (oral prednisolone 1–2 mg/kg)
Add ipratropium bromide for severe or poorly responding attacks
Escalate severe/life-threatening cases to IV magnesium sulfate and IV bronchodilators in HDU/ICU with senior support
Reassess frequently; arrange admission or safe discharge with a written action plan and a controller review
Management — Definitive & Stepwise
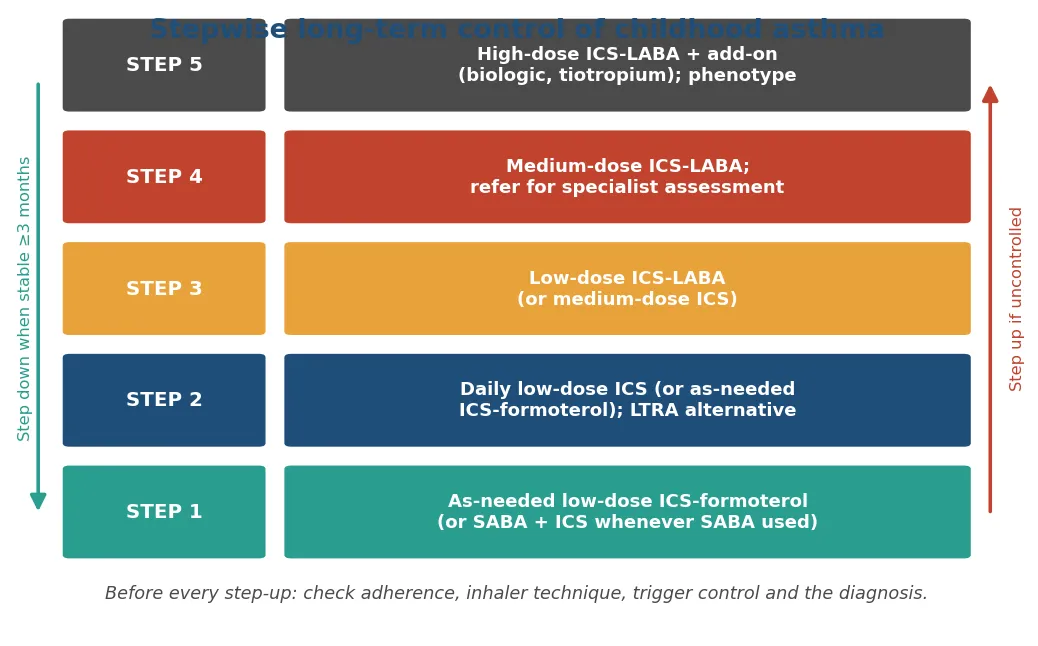
Definitive management of asthma is long-term control, and its aim is stated in one sentence: to achieve good symptom control and to minimise future risk — of exacerbations, of fixed airflow limitation and of treatment side-effects — at the lowest effective dose. This is delivered through a stepwise ladder in which treatment is stepped up when control is inadequate and stepped down when control has been maintained, typically for three months, always after checking that inadequate control is not simply due to poor adherence, poor inhaler technique, an unaddressed trigger or a wrong diagnosis. [10] [12]
The foundation of the ladder is the inhaled corticosteroid, which is the controller for all but the mildest disease. A major recent change, driven by the SYGMA trials, is the shift away from a short-acting beta-agonist as the sole reliever toward an anti-inflammatory reliever — an as-needed combination of low-dose inhaled corticosteroid with the fast-acting long-acting beta-agonist formoterol — so that every reliever actuation also delivers anti-inflammatory treatment. From there the ladder climbs through daily low-dose inhaled corticosteroid, the addition of a long-acting beta-agonist (as combined ICS-LABA), medium and then high doses, and finally specialist add-on therapy including biologics for severe eosinophilic disease. [8] [9] [10]
The evidence base has three points examiners return to. First, the SYGMA 1 and SYGMA 2 trials established that as-needed budesonide-formoterol controls mild asthma and reduces severe exacerbations compared with as-needed short-acting beta-agonist, underpinning the anti-inflammatory reliever strategy. Second, the CAMP trial showed that long-term inhaled budesonide improves control and reduces exacerbations but is associated with a small, largely one-off reduction in attained height — a real but modest effect that is outweighed by the benefit and reassures families that inhaled steroids at controller doses are safe. Third, the Cochrane comparison of leukotriene-receptor antagonists with inhaled corticosteroids found inhaled corticosteroids superior, confirming the ICS as first-line controller and the LTRA as an alternative or add-on rather than a substitute. [8] [9] [3] [11]
The SYGMA and CAMP evidence — the trials examiners expect you to cite
SYGMA 1 (O'Byrne 2018) and SYGMA 2 (Bateman 2018) tested as-needed budesonide-formoterol in mild asthma: it was superior to as-needed short-acting beta-agonist for exacerbation prevention and non-inferior to maintenance budesonide for severe exacerbations, at a much lower steroid dose — the trials that ended the SABA-only reliever era. CAMP (Szefler 2000, the Childhood Asthma Management Program) randomised children to inhaled budesonide, nedocromil or placebo: budesonide improved airway responsiveness and reduced exacerbations, and the much-discussed finding was a small reduction (about 1 cm) in attained height that did not progress — the evidence that lets you counsel families honestly that the growth effect of controller-dose inhaled steroid is small and the benefit large. [8] [9] [3]
Beyond the pharmacological ladder, definitive management is a package. Every child needs a written asthma action plan that tells the family what to do as symptoms change and when to seek help; a scheduled review to reassess control, technique and adherence and to step down when possible; attention to comorbidities (allergic rhinitis, obesity, reflux); trigger reduction with tobacco-smoke elimination as the priority; and immunisation including influenza. This structured, plan-based, regularly reviewed care is what converts a correct prescription into controlled asthma. [10] [12]
Specific Subtypes & Scenarios
Preschool wheeze is the first and commonest scenario. Most is transient viral wheeze that will resolve, so the task is to stratify risk with the Asthma Predictive Index and to avoid both under- and over-treatment: episodic viral wheeze is often managed with as-needed bronchodilator, while a child with multiple-trigger wheeze and a positive predictive index may benefit from a trial of daily inhaled corticosteroid. The PEAC/PEAK-era evidence (Guilbert 2006) showed that continuous inhaled corticosteroid in high-risk preschoolers controls symptoms while treatment continues but does not alter the natural history once it is stopped, so it is a control measure, not a cure. [1] [2] [4]
Exercise-induced bronchoconstriction is a scenario in its own right. Symptoms that appear a few minutes into exercise and settle with rest are the hallmark, and their presence usually signals inadequate overall control rather than a separate disease — the correct response is to optimise the daily controller. Where symptoms persist despite good control, a pre-exercise reliever (short-acting beta-agonist, or the ICS-formoterol reliever) and an adequate warm-up help. Exercise-induced symptoms should never be used as a reason to restrict activity; the goal is a child who can play sport freely. [5] [10]
The adolescent with poor control is the scenario that most tests clinical judgement, because the commonest cause is not severe disease but poor adherence and inhaler technique, compounded by the reluctance of teenagers to be seen using an inhaler. The approach is to build rapport, check the pharmacy record honestly, observe technique, negotiate a simple regimen (a single combination inhaler used as maintenance-and-reliever therapy improves adherence), and address smoking and vaping. Genuinely severe, treatment-resistant asthma is diagnosed only after adherence and technique have been confirmed and the child referred for specialist assessment and possible biologic therapy. [10] [12]
Complications & Pitfalls
The complications of asthma follow from uncontrolled inflammation. Acutely, the child is at risk of severe and life-threatening exacerbations, and asthma deaths — though rare — are concentrated among children with poor control, high reliever use, previous near-fatal attacks and poor engagement with care. Chronically, persistent uncontrolled inflammation drives airway remodelling and a component of fixed airflow limitation, and poorly controlled disease impairs school attendance, sleep, exercise and quality of life. The complications of the disease and the complications of its treatment (oral thrush and dysphonia from inhaled steroid without a spacer, and the small growth effect of controller-dose steroid) are both minimised by good technique and the lowest effective dose. [10] [3]
The pitfalls are as important as the complications, and examiners probe them. The commonest is treating apparently uncontrolled asthma by stepping up the drugs without first checking adherence, inhaler technique, trigger exposure and the diagnosis itself — the four things that account for most "difficult" asthma. The second is over-reliance on the reliever with under-use of the controller, the pattern that precedes severe attacks. The third is the mislabel: continuing to treat a child as asthmatic despite a wet cough, failure to thrive or no response to steroid, and thereby missing cystic fibrosis, bronchiectasis or a foreign body. [5] [10]
Prognosis & Disposition
The prognosis of childhood asthma is, for most children, good, and it is shaped by phenotype. Transient early wheezers resolve and do well. Many children with mild-to-moderate atopic asthma improve markedly through adolescence, though a proportion continue to have symptoms into adult life, and the atopic, early-sensitised phenotype with reduced lung function carries the greatest likelihood of persistence. Importantly, no controller has been shown to change the natural history of the disease once stopped — inhaled corticosteroid controls the disease while it is taken but does not cure it — so the goal is durable control rather than modification of the underlying trajectory. [1] [4]
Disposition is defined by control, risk and the reliability of follow-up. A child with well-controlled asthma is managed in the community with a written action plan and scheduled reviews to step therapy up or down. A child with frequent exacerbations, high reliever use, low lung function or a near-fatal attack needs closer specialist follow-up. After an acute presentation, safe discharge requires that the child is stable on reduced reliever frequency, that inhaler technique has been checked, that a written action plan and a short course of oral steroid (if indicated) are provided, and that a controller review and follow-up are arranged — the discharge is where the next admission is prevented. [10] [12]
Special Populations
Socioeconomically disadvantaged and Indigenous children carry a disproportionate burden of asthma prevalence, severity and mortality, driven by higher tobacco-smoke and housing-related exposures, reduced access to preventive care and lower rates of controller use. Culturally safe care, attention to the social determinants, tobacco-smoke elimination, reliable access to affordable controller medication and spacers, and proactive follow-up are the interventions that narrow this gap, and they matter more to outcome in these children than any refinement of the drug ladder. [10] [12]
Adolescents are a special population because of the transition of care and the particular challenges of adherence, body image, smoking and vaping, and the move to self-management. The consultation should increasingly address the young person directly, negotiate a regimen that fits their life, use a single combination inhaler where possible to simplify the regimen, and plan a structured transition to adult services for those with persistent disease. [10]
Children with obesity, with significant allergic rhinitis (the united airway), or with neurodisability form further groups needing tailored care: obesity worsens control and complicates the diagnosis (breathlessness may be deconditioning rather than asthma), allergic rhinitis should be treated because controlling the upper airway improves the lower, and children who cannot coordinate a device need a spacer with a mask and carer-delivered therapy. In each case the principle is the same — confirm the diagnosis objectively where possible, and match the delivery device and the review structure to the child. [5] [10]
[10]Evidence, Guidelines & Regional Differences
The governing international framework is the Global Initiative for Asthma (GINA) strategy, updated annually, whose central recent shifts are the move away from short-acting beta-agonist as the sole reliever toward the anti-inflammatory (ICS-formoterol) reliever, and the explicit separation of current symptom control from future risk. The 2022 GINA update and its primary-care summary (Levy 2023) codify the controller ladder and the maintenance-and-reliever therapy approach used across ages. In the United States the NAEPP 2020 Focused Updates (Cloutier 2020) similarly endorse ICS-formoterol as maintenance-and-reliever therapy and clarify the roles of FeNO, LTRAs and add-on long-acting muscarinic antagonists. [10] [12]
The landmark trials that underpin the guidelines are worth citing precisely. The Tucson cohort (Martinez 1995) defined the wheeze phenotypes; the Asthma Predictive Index (Castro-Rodríguez 2000) operationalised risk stratification in preschoolers; CAMP (Szefler 2000) established the efficacy and the modest, non-progressive growth effect of inhaled budesonide; the PEAK study (Guilbert 2006) showed that inhaled corticosteroid controls but does not modify the disease in high-risk preschoolers; the Cochrane review (Chauhan 2012) placed the inhaled corticosteroid above the leukotriene antagonist as first-line controller; and the SYGMA trials (O'Byrne and Bateman 2018) established anti-inflammatory reliever therapy. The GABRIEL genome-wide association study (Moffatt 2010) mapped the genetic architecture. [1] [2] [3] [4] [11] [8] [9] [6]
The regional differences are of emphasis rather than principle. All the major frameworks agree on the inhaled corticosteroid as the controller foundation, on the stepwise up-and-down titration, on assessing control and risk separately, and on the shift to anti-inflammatory reliever therapy; they differ in the exact preferred regimens at each step, the licensed age thresholds for particular inhalers, and the local device and access arrangements. The controversies that remain live are the optimal management of preschool wheeze (who to treat and with what), the place of biologics and their cost-effectiveness in severe paediatric disease, and how best to close the equity gap in outcomes. [10] [12]
Exam Pearls
Asthma control and step-up — 'CONTROL-STEP'
References
- [1]Martinez FD; Wright AL; Taussig LM; Holberg CJ; Halonen M; Morgan WJ Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N Engl J Med, 1995.PMID 7800004
- [2]Castro-Rodríguez JA; Holberg CJ; Wright AL; Martinez FD A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med, 2000.PMID 11029352
- [3]Childhood Asthma Management Program Research Group; Szefler S; Weiss S; Tonascia J; Adkinson NF; Bender B; et al Long-term effects of budesonide or nedocromil in children with asthma. N Engl J Med, 2000.PMID 11027739
- [4]Guilbert TW; Morgan WJ; Zeiger RS; Mauger DT; Boehmer SJ; Szefler SJ; et al Long-term inhaled corticosteroids in preschool children at high risk for asthma. N Engl J Med, 2006.PMID 16687711
- [5]Bacharier LB; Boner A; Carlsen KH; Eigenmann PA; Frischer T; Götz M; et al Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy, 2008.PMID 18053013
- [6]Moffatt MF; Gut IG; Demenais F; Strachan DP; Bouzigon E; Heath S; et al A large-scale, consortium-based genomewide association study of asthma. N Engl J Med, 2010.PMID 20860503
- [7]Dweik RA; Boggs PB; Erzurum SC; Irvin CG; Leigh MW; Lundberg JO; et al An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med, 2011.PMID 21885636
- [8]O'Byrne PM; FitzGerald JM; Bateman ED; Barnes PJ; Zhong N; Keen C; et al Inhaled Combined Budesonide-Formoterol as Needed in Mild Asthma. N Engl J Med, 2018.PMID 29768149
- [9]Bateman ED; Reddel HK; O'Byrne PM; Barnes PJ; Zhong N; Keen C; et al As-Needed Budesonide-Formoterol versus Maintenance Budesonide in Mild Asthma. N Engl J Med, 2018.PMID 29768147
- [10]Levy ML; Bacharier LB; Bateman E; Boulet LP; Brightling C; Buhl R; et al Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Prim Care Respir Med, 2023.PMID 36754956
- [11]Chauhan BF; Ducharme FM Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/or chronic asthma in adults and children. Cochrane Database Syst Rev, 2012.PMID 22592685
- [12]Cloutier MM; Baptist AP; Blake KV; Brooks EG; Bryant-Stephens T; et al 2020 Focused Updates to the Asthma Management Guidelines: A Report from the National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group. J Allergy Clin Immunol, 2020.PMID 33280709