Paeds · respiratory-sleep-and-airway
Central sleep apnoea and hypoventilation syndromes
Also known as Central sleep apnoea · Central sleep apnea · Congenital central hypoventilation syndrome · CCHS · Ondine's curse · ROHHAD · ROHHAD-NET · Central alveolar hypoventilation · Sleep-related hypoventilation · Disorders of control of breathing
Fellowship guide to central sleep apnoea and hypoventilation syndromes in children: the disorders in which the brain fails to generate an adequate breathing signal, so airflow and effort fall together (central apnoea) or tidal volume is chronically inadequate (hypoventilation), worst during sleep. The page covers congenital central hypoventilation syndrome and its PHOX2B genetic basis, ROHHAD and ROHHAD-NET, the acquired central apnoeas of Chiari malformation, brainstem lesions and prematurity, the polysomnography and capnography that define the pattern, and the lifelong ventilatory support from mask non-invasive ventilation through tracheostomy to diaphragm pacing that keeps these children alive.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a child who breathes normally while awake, chatting and playing, then falls asleep and simply stops making the effort to breathe. This is the paradox at the heart of central sleep apnoea and hypoventilation: the lungs and airway are competent, but the brainstem fails to send an adequate signal to breathe, and the failure is unmasked by sleep when behavioural and wakefulness drive are withdrawn. Central sleep apnoea is a pause in which airflow and respiratory effort stop together, with no paradoxical chest and abdominal movement, because there is no drive to breathe rather than an obstruction to overcome. [3] [1]
Central hypoventilation is the chronic cousin of central apnoea: rather than discrete pauses, the child breathes continuously but with inadequate tidal volume, so carbon dioxide climbs and oxygen falls, most severely during sleep. The defining laboratory finding is a raised carbon dioxide during sleep, which is why capnography or transcutaneous carbon dioxide monitoring, not oxygen saturation alone, is the measurement that makes the diagnosis. Because these children lack the chemoreceptor drive that would make a healthy person gasp, they often do not look distressed even as their gases become dangerous. [1] [3]
What makes these conditions dangerous is precisely the absence of the warning that protects the rest of us. The healthy response to a rising carbon dioxide is air hunger and increased ventilation; in central hypoventilation that reflex is blunted or absent, so the child sleeps peacefully into hypercapnia and hypoxaemia. The discipline that saves these children is to measure carbon dioxide in sleep in any child with unexplained cyanosis, cor pulmonale, polycythaemia, failure to wean from ventilation, or apnoea that is worse in quiet sleep, and never to be reassured by a child who is not visibly struggling. [1] [4]
Classification
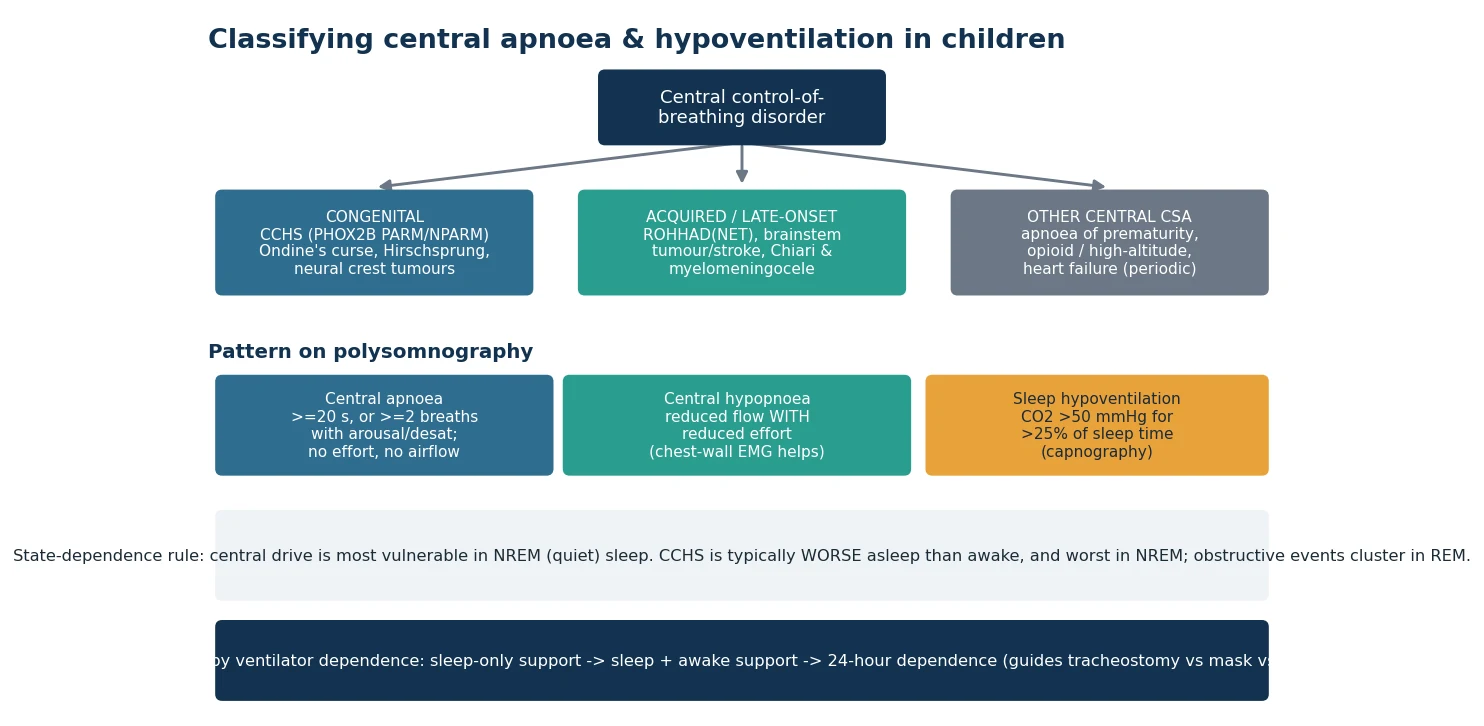
Sort these disorders first by whether the failure of breathing control is congenital or acquired, then by the pattern seen on the sleep study, because those two axes decide the genetic work-up, the search for a treatable lesion, and the type of ventilatory support. The figure below lays out the congenital causes led by congenital central hypoventilation syndrome, the acquired and late-onset causes led by ROHHAD and brainstem disease, and the other central apnoeas of prematurity, opioids and heart failure, alongside the polysomnographic patterns of central apnoea, central hypopnoea and sleep hypoventilation. [1] [3]
Congenital central hypoventilation syndrome deserves the first slot because it is the prototype and the most heavily examined. It is caused in almost all cases by a mutation in the PHOX2B gene, most commonly an expansion of a polyalanine repeat, with rarer non-polyalanine-repeat mutations carrying a more severe phenotype that includes Hirschsprung disease and neural crest tumours. The classic description of breathing that is adequate awake but fails asleep gave the historical name Ondine's curse, and the severity ranges from sleep-only hypoventilation to continuous ventilator dependence awake and asleep. [1] [15]
ROHHAD sits in the acquired and late-onset group and is the great mimic. The acronym captures its sequence: rapid-onset obesity, hypothalamic dysfunction, hypoventilation and autonomic dysregulation, with the suffix NET added when a neural crest tumour is present. Unlike congenital central hypoventilation syndrome it presents after a period of normal development, usually between ages two and seven, with dramatic weight gain preceding the breathing failure, and it has no single diagnostic gene, so it is a clinical diagnosis that demands a hunt for an occult tumour. [2] [6]
Central apnoea / hypoventilation
- No drive to breathe: airflow AND effort fall together
- No paradoxical chest-abdomen movement during the event
- Carbon dioxide rises; child often not distressed
- Worst in NREM (quiet) sleep when wakefulness drive is gone
Obstructive apnoea (contrast)
- Drive present: effort continues against a blocked airway
- Paradoxical chest-abdomen movement and snoring
- Child works hard, sweats, has arousals
- Clusters in REM sleep and with adenotonsillar hypertrophy
Congenital vs acquired central
- Congenital central hypoventilation syndrome: PHOX2B, lifelong
- ROHHAD: rapid obesity then hypoventilation, hunt for tumour
- Chiari and brainstem lesions: may be neurosurgically reversible
- Prematurity: immature drive, resolves with maturation
Epidemiology & Risk Factors
Congenital central hypoventilation syndrome is rare, with an estimated incidence in the order of one per two hundred thousand live births, but its true weight in paediatrics comes from its lifelong technology dependence and its multisystem surveillance burden rather than its numbers. It presents most often in the newborn period with cyanosis, apnoea or a failure to establish spontaneous breathing, and a smaller group with milder PHOX2B genotypes present later in infancy or childhood with hypoventilation unmasked by a respiratory infection or an anaesthetic. Boys and girls are affected equally. [1] [4]
ROHHAD is rarer still and clusters in the preschool and early school years, with the cardinal risk marker being the tempo of the weight gain: a previously normally grown child who gains weight explosively over months, then develops hypothalamic and breathing problems. Roughly forty per cent of ROHHAD cases harbour a neural crest tumour, so the epidemiological association that matters at the bedside is the link to ganglioneuroma, ganglioneuroblastoma and neuroblastoma that must be actively excluded. [6] [7]
The other central apnoeas carry their own risk profiles. Apnoea of prematurity is almost universal below twenty-eight weeks of gestation and reflects an immature brainstem respiratory network rather than a fixed lesion, resolving as the infant matures. Acquired central apnoea complicates Chiari malformations and myelomeningocele through brainstem compression, opioid exposure through direct suppression of the respiratory centre, and heart failure through the unstable feedback loop that produces periodic breathing. Recognising the context steers the work-up to the treatable cause. [11] [12]
Pathophysiology
To understand why the drive fails, follow the breathing signal from its origin. Ventilation is generated by a respiratory rhythm network in the brainstem and modulated by chemoreceptors that sense carbon dioxide and oxygen, and by wakefulness drive when the child is awake. In congenital central hypoventilation syndrome the PHOX2B mutation disrupts the development of the autonomic nervous system, including the chemoreceptor pathways, so the brainstem does not mount a ventilatory response to a rising carbon dioxide or a falling oxygen. When sleep removes the wakefulness drive, the deficient chemoreceptor drive is exposed and ventilation collapses. [1] [3]
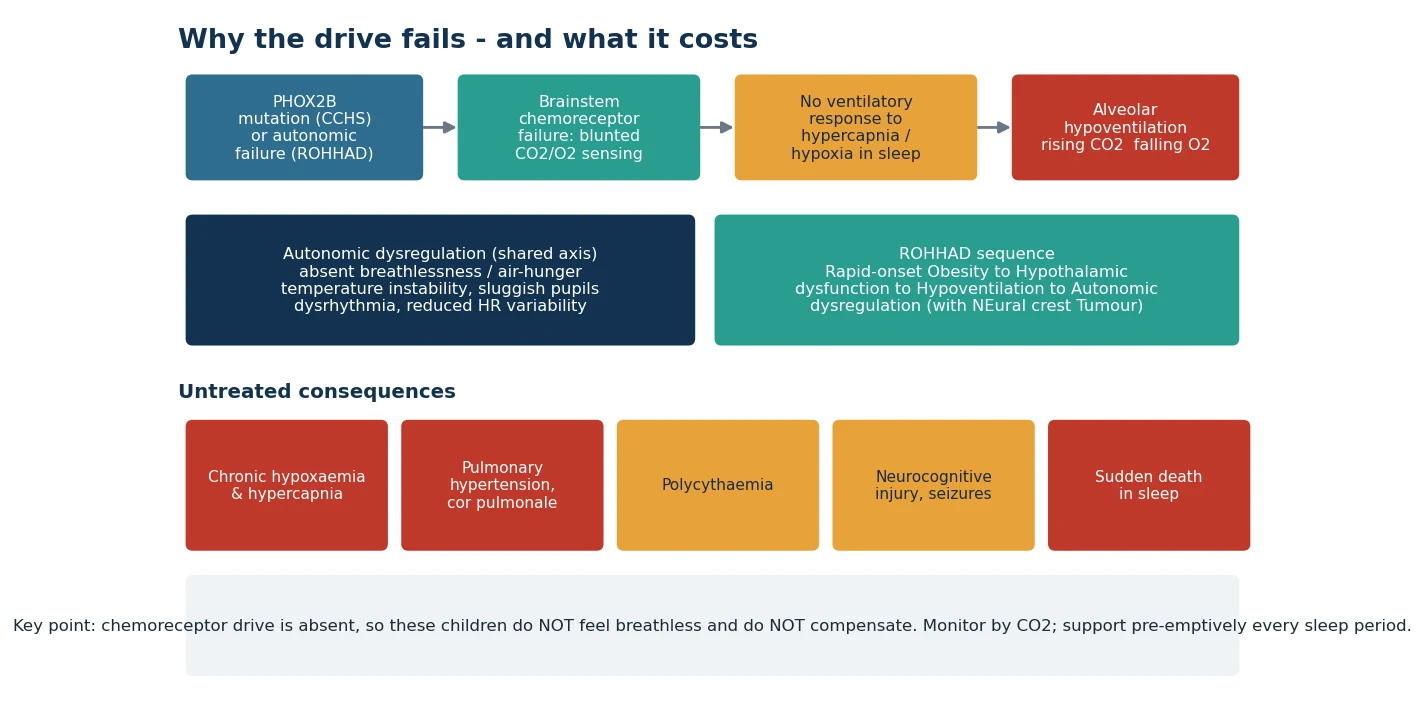
The autonomic dimension is what turns a breathing disorder into a multisystem disease. Because PHOX2B is a master regulator of autonomic neuron development, congenital central hypoventilation syndrome carries a package of autonomic features: reduced heart rate variability and dangerous sinus pauses, temperature instability, abnormal pupillary responses, altered gut motility with Hirschsprung disease, and a striking absence of the perception of breathlessness. That missing air hunger is the single most dangerous feature, because it removes the symptom that would otherwise prompt the child or family to act. [1] [2]
ROHHAD reaches the same endpoint of hypoventilation by a different route. Its leading hypothesis is an autoimmune or paraneoplastic hypothalamic and brainstem dysfunction, which is why it is associated with neural crest tumours and why immunomodulation is explored in refractory cases. The hypothalamic injury explains the obesity, the temperature and water balance disturbances and the endocrine failures, while the brainstem involvement explains the hypoventilation and autonomic instability. The sequence of the acronym mirrors the usual clinical timeline. [2] [6]
Whatever the route to hypoventilation, the downstream physiology converges. Chronic nocturnal hypoxaemia drives pulmonary vasoconstriction and, over time, pulmonary hypertension and cor pulmonale, while the low oxygen stimulates erythropoiesis and polycythaemia. Repeated or sustained hypoxaemia injures the developing brain, contributing to neurocognitive impairment and seizures, and an unsupported apnoeic or hypoventilating episode in sleep can be fatal. This is the mechanistic case for pre-emptive assisted ventilation during every sleep period rather than reactive treatment of desaturation. [3] [1]
Clinical Presentation
The presentation depends on the age and the cause, but a few pictures recur. The neonate with congenital central hypoventilation syndrome is often a term baby who is unexpectedly cyanosed or apnoeic, breathes shallowly or not at all when asleep yet pinks up and breathes when stimulated or awake, and cannot be weaned from respiratory support despite normal lungs and heart on investigation. The mismatch between a well-looking awake baby and a baby who hypoventilates the moment sleep arrives is the classic clue. [1] [4]
The child with milder or later-onset congenital disease may reach infancy or early childhood before diagnosis, presenting with a hypoventilation crisis during a chest infection or after an anaesthetic, with cyanotic spells, seizures from hypoxaemia, or the incidental discovery of cor pulmonale, right heart strain or polycythaemia. Some are picked up only after a sibling is diagnosed or after PHOX2B testing is prompted by autonomic features such as constipation, sweating abnormalities or a documented sinus pause. [4] [15]
ROHHAD announces itself with the weight before the breathing. A previously well child, usually between two and seven years, gains weight rapidly over a few months, then over the following months to years develops hypothalamic features such as disordered thirst and sodium balance, precocious or delayed puberty, growth hormone deficiency and temperature dysregulation, followed by the hypoventilation that brings them to respiratory attention. Autonomic features such as pupillary abnormalities, altered sweating, gut dysmotility and bradycardia accompany the picture, and some children present acutely with a cardiorespiratory arrest during sleep. [6] [2]
The acquired central apnoeas present in their clinical context. An infant with a Chiari malformation or repaired myelomeningocele may have central apnoeas, stridor, swallowing difficulty and apnoeic episodes from brainstem compression; a premature infant has recurrent apnoea, bradycardia and desaturation on the neonatal unit; and a child on opioids or with heart failure shows central pauses or a waxing and waning periodic breathing pattern. In each, the breathing abnormality is a signpost to the underlying disorder. [11] [12]
Differential Diagnosis
The first fork is central versus obstructive sleep-disordered breathing, because the two are managed in opposite ways. Obstructive apnoea shows continued or exaggerated respiratory effort against a blocked airway, with paradoxical chest and abdominal movement, snoring and arousals, and is usually treated by relieving the obstruction; central apnoea shows effort and airflow ceasing together with no paradox, and is treated by supporting or driving ventilation. Mixed events combine both. The polysomnogram, ideally with measures of effort and carbon dioxide, settles the question. [10] [3]
Central hypoventilation
- Effort and airflow fall together; no paradox
- Carbon dioxide high; oxygen low; little distress
- Worse in NREM sleep; may be normal awake
- Think PHOX2B, ROHHAD, brainstem lesion
Obstructive apnoea
- Effort continues against a closed airway
- Snoring, paradoxical movement, arousals
- Worse in REM; adenotonsillar hypertrophy
- Think tonsils, obesity, craniofacial anomaly
Mimics to exclude
- Seizures and breath-holding spells
- Neuromuscular weakness causing hypoventilation
- Metabolic and cardiac causes of collapse
- Gastro-oesophageal reflux with apnoea in infants
Within central disease, the task is to separate the congenital from the acquired and to find the treatable cause. Congenital central hypoventilation syndrome is confirmed by PHOX2B testing and typically presents from birth; ROHHAD is a later clinical diagnosis defined by the obesity-first timeline and demands tumour imaging; brainstem causes such as Chiari malformation, tumour, stroke and previous posterior fossa surgery are found on magnetic resonance imaging; and neuromuscular disorders cause hypoventilation through weak respiratory muscles rather than absent drive, distinguished by the examination, the creatine kinase and the neurophysiology. [1] [11]
Do not forget the reversible and the benign. Apnoea of prematurity is a maturational phenomenon that resolves and responds to caffeine, opioid-induced central apnoea reverses when the drug is stopped or reversed, and the periodic breathing of a young infant is a normal variant when brief and not associated with significant desaturation. Distinguishing these from a fixed central disorder prevents both under-treatment of dangerous disease and over-medicalisation of a normal infant. [12] [10]
Clinical & Bedside Assessment
The bedside assessment begins with observing the child breathing across the wake-sleep transition, because the disorder is often invisible when the child is awake and alert. Watch for the tell-tale drop in tidal volume, the shallow or paused breathing and the desaturation that appear as the child falls asleep, and note the absence of the compensatory air hunger, gasping or arousal that a healthy child would show. In central apnoea there is no paradoxical see-saw movement of the chest and abdomen, unlike the effortful obstructed breath. [3] [10]
Examine for the consequences and the associations. Look for the signs of pulmonary hypertension and right heart strain such as a loud pulmonary second sound, a right ventricular heave and hepatomegaly, for the plethora of polycythaemia, and for growth failure or, in ROHHAD, rapid excessive weight gain. Search for autonomic clues: abnormal pupils, cool mottled peripheries, sweating abnormalities, constipation suggesting Hirschsprung disease, and a low resting heart rate or documented pauses. In the child with a Chiari malformation, assess for lower cranial nerve signs, stridor and swallowing difficulty. [1] [2]
The overnight or nap observation is itself a bedside test. Documenting the breathing pattern, effort, saturation and carbon dioxide during natural sleep, and how they respond to arousal, distinguishes the child who hypoventilates only in sleep from the child who fails awake as well, which in turn defines the intensity of support the child needs. This graded assessment, from wake to sleep and from quiet to active sleep, is the clinical bridge to the formal sleep study. [3] [4]
Investigations
The definitive investigation is attended polysomnography with carbon dioxide monitoring, which characterises the events as central, obstructive or mixed, quantifies the central apnoea and hypopnoea burden, and, crucially, measures sleep hypoventilation as a carbon dioxide that stays above fifty millimetres of mercury for more than a quarter of the sleep period. Because oxygen desaturation is a late and unreliable marker, the carbon dioxide channel is the one that reveals hypoventilation, and chest-wall effort recording helps classify hypopnoeas as central or obstructive. [10] [3]
A blood gas anchors the acute assessment: a raised carbon dioxide with a compensatory bicarbonate rise signals chronic hypoventilation rather than an acute event. Where the picture fits congenital central hypoventilation syndrome, targeted PHOX2B genetic testing is the confirmatory test and also predicts severity, since the polyalanine repeat length and the non-polyalanine-repeat mutations correlate with the phenotype, the risk of Hirschsprung disease and the tumour risk. A computer-aided facial phenotype screen has been described as an adjunct that flags children who should be tested. [1] [15]
The complications and associations drive a parallel work-up. An echocardiogram screens for pulmonary hypertension and cor pulmonale, an electrocardiogram and Holter monitor detect the sinus pauses and reduced heart rate variability of autonomic dysfunction, and a full blood count reveals polycythaemia. In ROHHAD, the hypothalamic and endocrine axis is assessed with sodium and water balance, pituitary hormones and metabolic studies, and dedicated imaging with metaiodobenzylguanidine or cross-sectional scanning searches for the neural crest tumour. In suspected brainstem disease, magnetic resonance imaging of the posterior fossa and craniocervical junction is essential. [6] [11]
Management — Resuscitation
The acute management of a child who presents with a central apnoeic or hypoventilation crisis follows airway, breathing and circulation, with one overriding principle: ventilate, do not merely oxygenate. Support the breathing with bag-mask ventilation or non-invasive positive pressure, and escalate to intubation and mechanical ventilation if the child cannot maintain adequate ventilation, because the problem is inadequate minute ventilation and carbon dioxide clearance, not primarily oxygen transfer. Continuous carbon dioxide monitoring guides the adequacy of the support. [3] [1]
Stabilise the whole child while supporting ventilation. Attach cardiorespiratory monitoring to detect the sinus pauses and bradyarrhythmias of autonomic dysfunction, obtain a blood gas to quantify the carbon dioxide and its chronicity, and correct hypoxaemia, acidosis and any precipitating illness such as a chest infection. Avoid sedatives, opioids and other respiratory depressants that further blunt an already deficient drive, and if such agents are unavoidable, do so only with the airway secured and ventilation controlled. Early involvement of paediatric intensive care and a respiratory or sleep service is essential. [13] [3]
Where the crisis is driven by a treatable structural cause, resuscitation runs in parallel with definitive treatment. A child whose central apnoea stems from a Chiari malformation with brainstem compression may need urgent neurosurgical assessment for posterior fossa decompression, and a child with a hypoventilation crisis unmasked by an occult tumour needs that tumour identified. Stabilising ventilation buys the time to find and treat the cause. [11] [6]
Management — Definitive & Stepwise
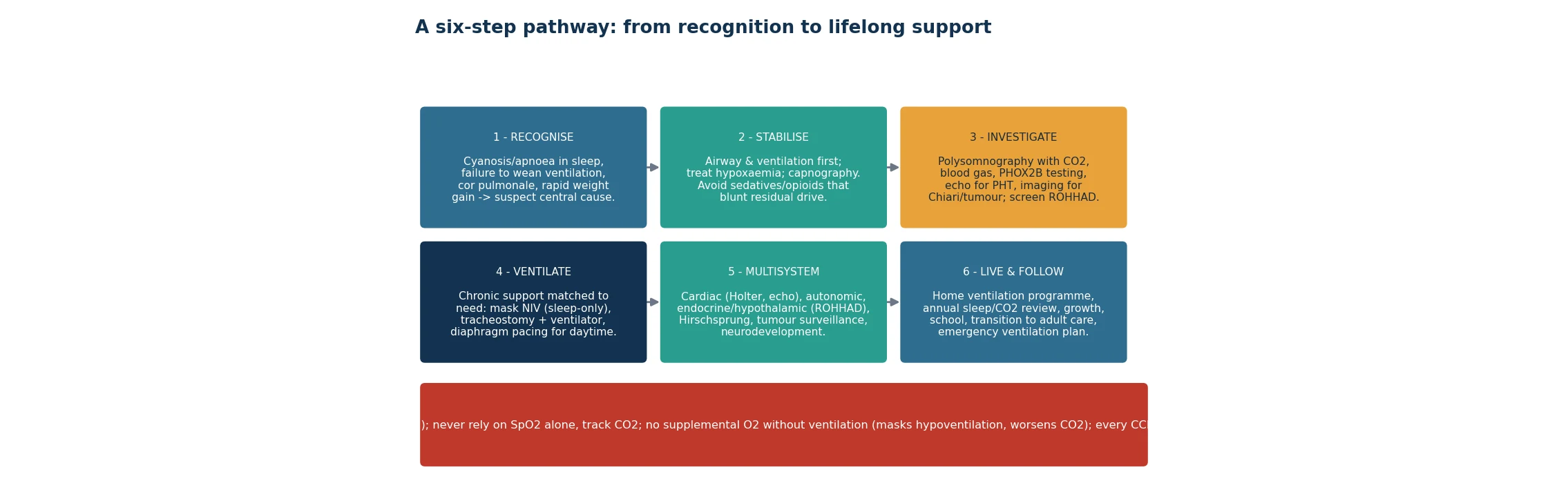
Definitive management is lifelong assisted ventilation matched to the child's degree of dependence, delivered so that it supports every sleep period and, where needed, waking hours too. The stepwise ladder runs from mask non-invasive ventilation for children who hypoventilate only in sleep, through tracheostomy with positive-pressure ventilation for those needing more support or who are too young for reliable mask ventilation, to diaphragm pacing for selected children needing daytime support who wish to be free of a ventilator circuit. The figure sets out the whole pathway from recognition to lifelong follow-up. [1] [4]
The choice of interface and device is a shared, staged decision. A tracheostomy and home ventilator give the most secure and adjustable support and are often the safest choice in infancy, while mask non-invasive ventilation suits older, milder or partially dependent children and avoids a tracheostomy. Diaphragm (phrenic nerve) pacing offers portable daytime support and can allow a previously tracheostomised child to be decannulated in selected cases, though it requires functioning phrenic nerves and diaphragms and careful patient selection. Whichever route is chosen, the aim is normocapnia and normoxaemia throughout sleep. [8] [9]
Treat the cause where the cause is treatable. Posterior fossa decompression can improve or resolve the central apnoea of a Chiari malformation, the neural crest tumour of ROHHAD-NET is resected and its histology guides oncological treatment, and immunomodulation is explored for the presumed autoimmune component of refractory ROHHAD. Apnoea of prematurity is managed with caffeine citrate, typically a loading dose of about 20 mg/kg followed by a daily maintenance dose of 5 to 10 mg/kg, alongside general neonatal support until the drive matures. [11] [12]
Around all of this sits a home ventilation programme. Families are trained in the equipment, suctioning and tracheostomy or mask care, resuscitation and an emergency plan; the child has reliable power, back-up equipment and community nursing support; and regular review adjusts the settings to growth. Anaesthesia and sedation are planned carefully, since these children are exquisitely sensitive to respiratory depressants and need controlled ventilation and extended monitoring around any procedure. [13] [5]
Specific Subtypes & Scenarios
Congenital central hypoventilation syndrome is the archetype: a PHOX2B-confirmed disorder presenting usually from birth, requiring lifelong assisted ventilation in sleep and sometimes awake, with the severity graded by the genotype. The polyalanine repeat mutations produce a graded severity by repeat length, while the non-polyalanine-repeat mutations cause the most severe disease with the highest risk of continuous ventilator dependence, Hirschsprung disease and neural crest tumours. Management is multidisciplinary and monitoring is lifelong. [1] [15]
ROHHAD and ROHHAD-NET form the second key scenario. The child presents after normal early development with rapid-onset obesity, then hypothalamic dysfunction, hypoventilation and autonomic dysregulation, and in a large minority a neural crest tumour. The pitfalls are attributing the obesity to simple over-eating and missing the tumour, and the priorities are to confirm the hypoventilation, hunt for and treat the tumour, manage the endocrine and autonomic complications, and consider immunomodulation in refractory disease. Its perioperative care demands meticulous ventilatory planning. [6] [7] [14]
The acquired central apnoeas make up the third group. A Chiari malformation or myelomeningocele can compress the brainstem and cause central apnoea that may improve with posterior fossa decompression; a brainstem tumour, stroke or the aftermath of posterior fossa surgery can injure the respiratory centres; and apnoea of prematurity reflects an immature but ultimately maturing drive that responds to caffeine. Recognising a reversible or self-limiting cause changes the trajectory entirely from that of a fixed congenital disorder. [11] [12]
Complications & Pitfalls
The complications of inadequately treated central hypoventilation follow directly from chronic hypoxaemia and hypercapnia: pulmonary hypertension and cor pulmonale, polycythaemia, neurocognitive impairment and seizures from hypoxic brain injury, and sudden death during an unsupported sleep period. In congenital central hypoventilation syndrome the autonomic package adds its own complications, including dangerous sinus pauses that may need a pacemaker, Hirschsprung-related bowel disease, and the neural crest tumours of the more severe genotypes. [1] [2]
The great pitfall, repeated across every scenario, is to be reassured by oxygen saturation and by a child who does not look distressed. A second pitfall is giving oxygen without ventilation, which corrects the number the team is watching while the carbon dioxide climbs to narcosis. A third is administering sedatives, opioids or anaesthesia without anticipating the exquisite sensitivity of these children to respiratory depression, precipitating a crisis. Each of these errors stems from forgetting that the defect is drive, not oxygen transfer. [13] [1]
Diagnostic pitfalls compound the treatment pitfalls. Central apnoea is mislabelled as obstructive and treated with adenotonsillectomy that cannot help; ROHHAD is dismissed as simple obesity and its tumour missed; a Chiari malformation causing reversible central apnoea is overlooked because imaging was not obtained; and apnoea of prematurity is over-treated as if it were a fixed disorder. The remedy is a structured approach that classifies the events, measures carbon dioxide, and actively seeks the treatable cause. [11] [6]
Prognosis & Disposition
The prognosis is defined by the cause and by the quality of the ventilatory support. Congenital central hypoventilation syndrome is a lifelong condition, but with well-organised home ventilation, careful surveillance for its cardiac, autonomic and tumour complications and attention to normocapnia in sleep, many children grow, attend school and reach adulthood, and long-term ventilatory outcomes have improved with modern multidisciplinary care. Neurocognitive outcome is best when hypoxaemia and hypercapnia are prevented rather than merely treated. [4] [5]
ROHHAD carries a more guarded prognosis, driven by the tumour where present, the hypothalamic and autonomic complications, and the risk of sudden cardiorespiratory death, so it demands intensive surveillance and prompt treatment of its components. The acquired central apnoeas often carry the best outlook when the cause is reversible: posterior fossa decompression can resolve Chiari-related central apnoea, and apnoea of prematurity resolves with maturation. In every case, the disposition is a structured home programme with clear escalation and emergency planning. [6] [11]
The disposition plan is therefore as important as the diagnosis. These children need a defined home ventilation programme, reliable community and equipment support, regular sleep and cardiac review, endocrine and tumour surveillance where relevant, developmental follow-up, and a planned transition to adult respiratory and sleep services. A written emergency plan that tells any clinician to ventilate rather than merely oxygenate, and to avoid respiratory depressants, protects the child during intercurrent illness and unplanned presentations. [5] [4]
Special Populations
The neonate is the highest-stakes population, because congenital central hypoventilation syndrome most often declares itself in the newborn period and can be fatal if the hypoventilation in sleep is not recognised. A term baby who cannot wean from ventilation, or who is cyanosed and apnoeic in sleep with normal lungs and heart, warrants PHOX2B testing and a control-of-breathing assessment, and the family needs early, honest counselling about a lifelong technology-dependent course. Autonomic screening for Hirschsprung disease and sinus pauses is part of the neonatal work-up. [1] [4]
The premature infant is a distinct population in whom central apnoea is usually maturational apnoea of prematurity rather than a fixed disorder, managed with caffeine and resolving with time, but in whom a persistent or atypical pattern should still prompt consideration of a structural or genetic cause. Distinguishing the common maturational problem from the rare fixed disorder prevents both unnecessary alarm and dangerous complacency. [12] [10]
The technology-dependent child on home ventilation, whatever the underlying diagnosis, has particular needs: equipment reliability and back-up, trained carers, clear emergency plans, careful perioperative management given the sensitivity to respiratory depressants, and support for the family carrying a heavy caregiving load. In settings with limited resources and in geographically remote or Indigenous communities, equitable access to home ventilation, community nursing and specialist review is a real challenge that must be planned for explicitly rather than assumed. [13] [5]
Evidence, Guidelines & Regional Differences
The cornerstone guidance is the American Thoracic Society clinical policy statement on congenital central hypoventilation syndrome, which sets out the genetic basis, the diagnostic approach centred on PHOX2B testing, and the principles of ventilatory management and multisystem surveillance, and it remains the reference framework internationally. Subsequent reviews have consolidated the understanding of the disorders of control of ventilation and the long-term ventilatory outcomes achievable with modern care. [1] [3] [4]
The evidence for the acquired and specific scenarios is more varied in strength. Posterior fossa decompression for Chiari-related central apnoea is supported by observational outcome series, diaphragm pacing by case series and cohort experience in specialist centres, and caffeine for apnoea of prematurity by robust randomised and systematic-review evidence that also informs its long-term safety. ROHHAD guidance rests on systematic reviews of the clinical timeline and expert recommendations rather than trials, reflecting its rarity. [11] [8] [12] [6]
Regional differences are practical rather than definitional. The diagnostic thresholds and the PHOX2B basis of congenital central hypoventilation syndrome are consistent across jurisdictions, but access to attended paediatric polysomnography with carbon dioxide monitoring, to genetic testing, to home ventilation programmes and to diaphragm pacing varies widely between and within countries. In Australia and New Zealand, as elsewhere, care is concentrated in tertiary paediatric respiratory and sleep centres, and equitable access for rural, remote and Indigenous families is an explicit service priority. [5] [4]
Exam Pearls
Hold one sentence for the viva: a child who breathes adequately awake but hypoventilates in sleep, who is not distressed despite a high carbon dioxide, has a central control-of-breathing disorder, and the rule that protects the child is to ventilate rather than merely oxygenate and to measure carbon dioxide rather than trust the saturation. Congenital central hypoventilation syndrome is confirmed by PHOX2B testing; ROHHAD is a later clinical diagnosis that demands a hunt for a neural crest tumour. [1] [3] [6]
State the frequently tested facts correctly. Central apnoea shows airflow and effort ceasing together with no paradoxical movement, unlike obstructive apnoea. Congenital central hypoventilation syndrome is caused by PHOX2B mutations, usually a polyalanine repeat expansion, with non-polyalanine-repeat mutations giving the most severe disease, Hirschsprung disease and tumours. Sleep hypoventilation is defined by a carbon dioxide above fifty millimetres of mercury for more than a quarter of sleep. ROHHAD stands for rapid-onset obesity, hypothalamic dysfunction, hypoventilation and autonomic dysregulation, with NET for the neural crest tumour. Caffeine treats apnoea of prematurity. [1] [10] [6] [12]
The high-yield pairings do most of the diagnostic work: a neonate who cannot wean from ventilation with normal lungs and heart suggests congenital central hypoventilation syndrome; rapid childhood weight gain then hypoventilation suggests ROHHAD; central apnoea with a Chiari malformation may be relieved by posterior fossa decompression; central apnoea in a preterm infant is usually apnoea of prematurity; and a comfortable child with a dangerously high carbon dioxide is the signature of absent chemoreceptor drive. Remember always to ventilate, not simply oxygenate. [11] [4] [2]
References
- [1]Weese-Mayer DE; Berry-Kravis EM; Ceccherini I; et al An official ATS clinical policy statement: Congenital central hypoventilation syndrome: genetic basis, diagnosis, and management. Am J Respir Crit Care Med, 2010.PMID 20208042
- [2]Ceccherini I; Kurek KC; Weese-Mayer DE Developmental disorders affecting the respiratory system: CCHS and ROHHAD. Handb Clin Neurol, 2022.PMID 36031316
- [3]Kasi AS; Perez IA Congenital Central Hypoventilation Syndrome and Disorders of Control of Ventilation. Clin Chest Med, 2024.PMID 39069329
- [4]Fain ME; Westbrook AL; Kasi AS Congenital Central Hypoventilation Syndrome: Diagnosis and Long-Term Ventilatory Outcomes. Clin Med Insights Pediatr, 2023.PMID 37256017
- [5]Kasi AS; Li H; Harford KL; et al Congenital Central Hypoventilation Syndrome: Optimizing Care with a Multidisciplinary Approach. J Multidiscip Healthc, 2022.PMID 35360554
- [6]Harvengt J; Gernay C; Mastouri M; et al ROHHAD(NET) Syndrome: Systematic Review of the Clinical Timeline and Recommendations for Diagnosis and Prognosis. J Clin Endocrinol Metab, 2020.PMID 32407531
- [7]Marpuri I; Ra E; Naguib MN; et al Weight management in youth with rapid-onset obesity with hypothalamic dysregulation, hypoventilation, autonomic dysregulation, and neural crest tumor (ROHHAD-NET): literature search and case report. J Pediatr Endocrinol Metab, 2022.PMID 34954931
- [8]Tsolakis N; Sindelar R; Markström A; et al Applying diaphragm pacing in previously tracheostomised children with congenital central hypoventilation syndrome is a safe tool. Acta Paediatr, 2022.PMID 35266201
- [9]Dozor AJ; Vincent R Assessment of Phrenic Nerve Pacers in a Patient With Congenital Central Hypoventilation Syndrome. Pediatr Pulmonol, 2025.PMID 39688338
- [10]Berry RB; Ryals S; Wagner MH Use of Chest Wall EMG to Classify Hypopneas as Obstructive or Central. J Clin Sleep Med, 2018.PMID 29734977
- [11]Okai BK; Jaikumar V; Francois HB; et al Posterior fossa decompression in patients with Chiari malformation type 1: effect on sleep apnea and follow-up outcomes. Childs Nerv Syst, 2024.PMID 39365303
- [12]Marques KA; Bruschettini M; Roehr CC; et al Methylxanthine for the prevention and treatment of apnea in preterm infants. Cochrane Database Syst Rev, 2023.PMID 37905735
- [13]Basu SM; Chung FF; AbdelHakim SF; et al Anesthetic Considerations for Patients With Congenital Central Hypoventilation Syndrome: A Systematic Review of the Literature. Anesth Analg, 2017.PMID 27918326
- [14]Puri S; Yaddanapudi S; Menon P Peri-operative management of a child with ROHHAD-NET syndrome undergoing neural crest tumour excision. Anaesth Rep, 2022.PMID 35756834
- [15]Slattery SM; Wilkinson J; Mittal A; et al Computer-aided diagnostic screen for Congenital Central Hypoventilation Syndrome with facial phenotype. Pediatr Res, 2024.PMID 38238566