Paeds · respiratory-sleep-and-airway
Exercise-induced bronchoconstriction
Also known as Exercise-induced bronchoconstriction · Exercise-induced asthma · Exercise-induced bronchospasm · EIB in children · Sport-related wheeze
Fellowship guide to exercise-induced bronchoconstriction in children: the transient airway narrowing that follows a burst of exercise, why it usually signals inadequate asthma control, how it is confirmed objectively with an exercise or eucapnic voluntary hyperpnoea challenge and a ten-percent fall in FEV1, the osmotic and thermal mechanisms that drive it, the mimics that catch the unwary — above all inducible laryngeal obstruction — and the management that keeps a child fully in sport, built on controlling the underlying asthma, a warm-up, and a pre-exercise reliever.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child sprints across the playground, and a few minutes later — often just as they stop — the cough starts, the chest tightens, and a wheeze appears that eases again with rest. That sequence is exercise-induced bronchoconstriction: a transient narrowing of the lower airways provoked by a burst of vigorous exercise, coming on during or shortly after the effort, peaking five to fifteen minutes after it ends, and resolving spontaneously within thirty to sixty minutes. It is the airway, not the heart or the legs, that limits the child, and the whole clinical task is to prove that, treat the airway, and get the child back to full sport. [3] [5]
The term names a physiological event, not a disease of its own. Most children who bronchoconstrict with exercise have asthma, and their exercise symptoms are simply the most exertion-sensitive expression of the same twitchy, inflamed airway; in a smaller group — some athletes and otherwise well children — the narrowing occurs without any other features of asthma, and is called isolated exercise-induced bronchoconstriction. Holding this distinction in mind matters, because in the child with asthma the exercise symptoms are usually a marker that the underlying disease is under-treated. [3] [4]
Classification
The most useful first question at the bedside is whether the child who wheezes with sport also has asthma the rest of the time. When exercise symptoms sit alongside interval symptoms, nocturnal cough, atopy and a history of wheeze, this is exercise-induced bronchoconstriction occurring within asthma, and the exercise component is a barometer of overall control. When a careful history and testing find no other feature of asthma — as in some competitive athletes and otherwise healthy children — the label is isolated exercise-induced bronchoconstriction, which is managed for the exercise trigger alone. [3] [4]
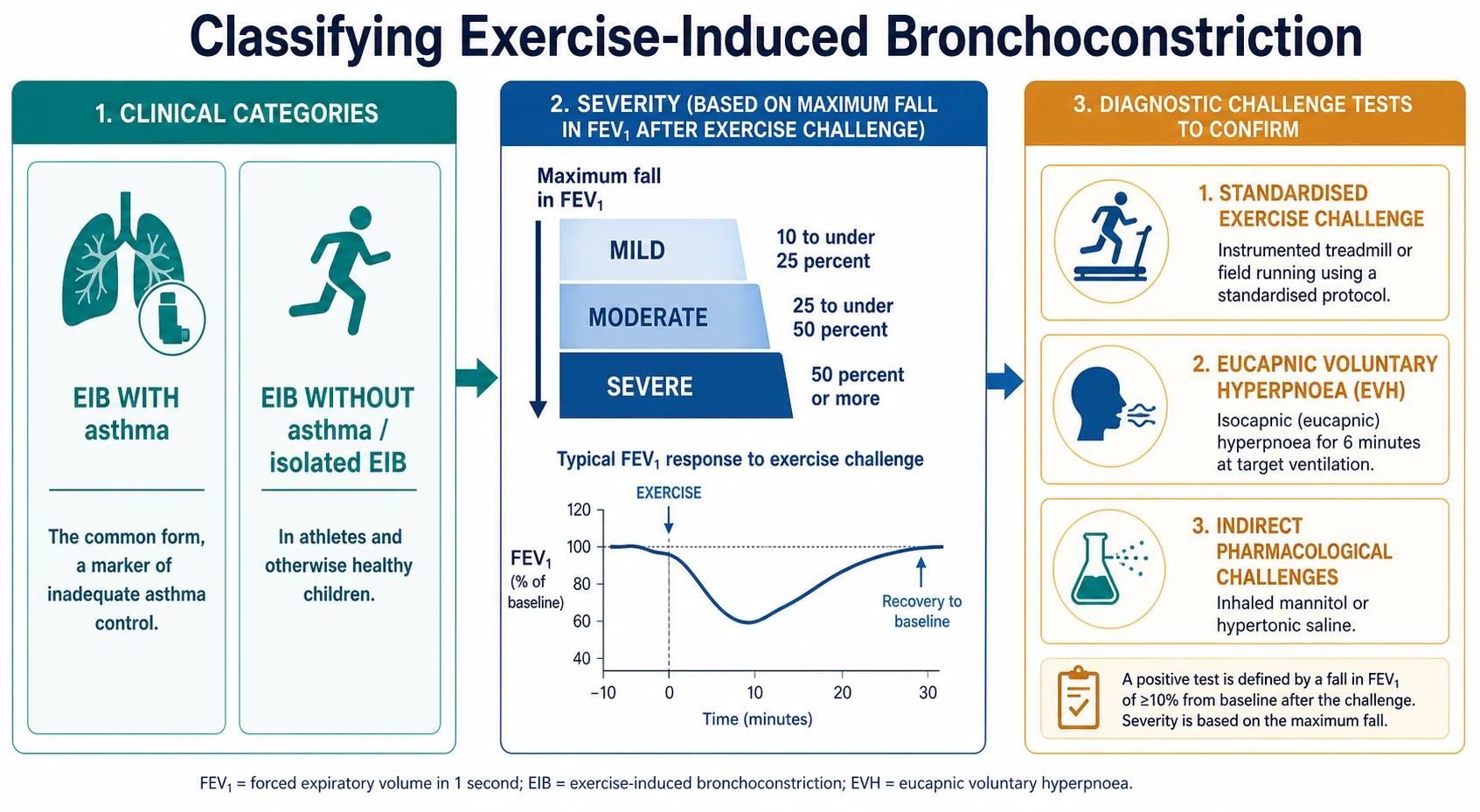
The second axis is severity, and it is defined objectively by how far the FEV1 falls at its worst after a standardised exercise challenge. A fall of ten percent or more confirms the diagnosis; a maximum fall of ten to just under twenty-five percent is mild, twenty-five to just under fifty percent is moderate, and fifty percent or more is severe. Grading matters because it guides how aggressively to treat and how carefully to supervise return to sport, and because a large fall in a child who feels only mildly limited flags an airway that is more reactive than the history suggests. [3] [5]
Epidemiology & Risk Factors
Exercise-induced bronchoconstriction is common, and its frequency tracks the population being studied. It can be demonstrated in the great majority of children with asthma when they are challenged carefully, and it is found in a substantial minority of elite athletes and in a smaller proportion of the general childhood population who have no diagnosed asthma at all. Because it is so tightly linked to asthma, its burden falls hardest on the same disadvantaged and Indigenous children who carry the greatest asthma burden in Australia and New Zealand. [4] [6]
The strongest risk factor is underlying asthma, particularly when it is poorly controlled, and the atopic background that drives asthma — eczema, allergic rhinitis, allergic sensitisation — carries across to the exercise trigger. On top of that disease predisposition sit the environmental amplifiers that determine how much dry, cold or irritant air reaches the lower airway during a given effort: exercise in cold dry air, high ventilation endurance sports, and exposure to chlorine by-products in swimming pools or to airborne pollutants and pollens all raise the risk and the severity. [6] [7]
The type of sport shapes the risk in a way examiners like to draw out. Endurance disciplines that demand sustained high minute ventilation — distance running, cycling, cross-country skiing — and sports played in cold dry air or over chlorinated pools expose the lower airway to the largest volumes of poorly conditioned air, and they carry the highest rates. Sports with brief bursts and long rests, and those played in warm humid air such as swimming in a warm indoor pool, provoke far less. This explains why a child can be limited by one sport and untroubled by another. [6] [7]
Pathophysiology
The engine of exercise-induced bronchoconstriction is the huge increase in breathing that vigorous exercise demands. To move that much air, the child breathes through the mouth and bypasses the nose, so the lower airways receive large volumes of air that is cooler and drier than they are used to conditioning. The airway lining has to warm and humidify this air, and in doing so it loses water from the thin film of airway surface liquid that coats it. That water loss is the trigger from which everything else follows. [2] [11]
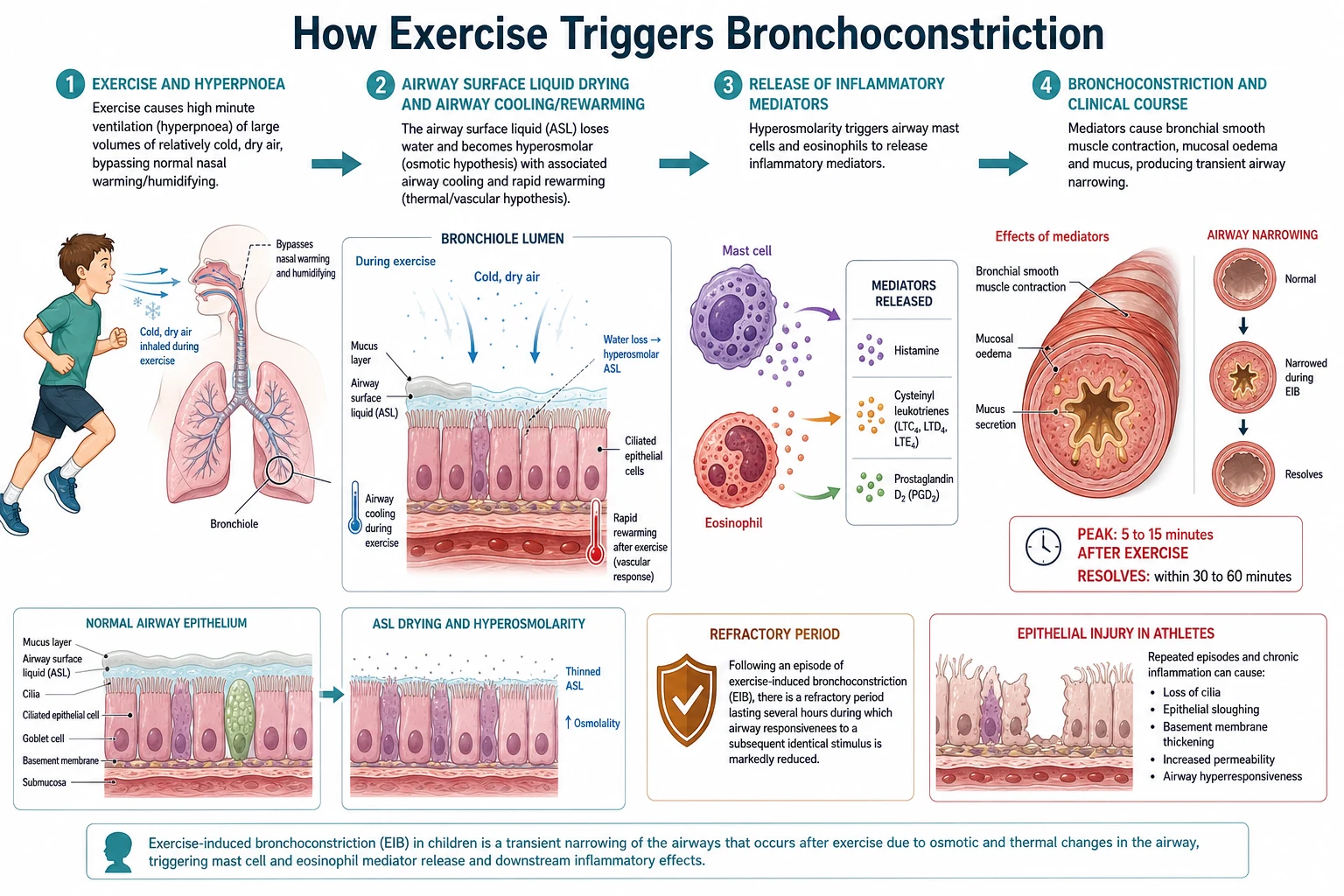
Two connected mechanisms explain how water loss narrows the airway. In the osmotic hypothesis, the loss of water concentrates the airway surface liquid and makes it hyperosmolar; this osmotic stress activates airway mast cells to release bronchoconstrictor mediators — histamine, the cysteinyl leukotrienes and prostaglandin D2 — which contract airway smooth muscle and produce mucosal swelling and mucus. In the thermal or vascular hypothesis, the airway cools during exercise and then rapidly rewarms afterwards, and the reactive engorgement of the bronchial vasculature adds to the narrowing. The osmotic mechanism is considered the dominant one, with the thermal changes contributing, especially in cold dry conditions. [2] [11]
A distinctive and clinically useful feature follows from this mediator biology: after an episode there is a refractory period, lasting up to a few hours, during which an identical bout of exercise provokes much less narrowing because the mast cell mediators have been partly depleted and not yet replenished. This is the physiological basis of the pre-exercise warm-up, which deliberately induces a small, tolerable episode so that the main effort falls within the refractory window. In children with asthma, chronic airway inflammation lowers the threshold for all of this, which is why controlling the inflammation reduces the exercise response. [2] [5]
Clinical Presentation
The history is the heart of the diagnosis, and its shape is characteristic. The child develops cough, wheeze, chest tightness or breathlessness a few minutes into sustained exercise or, classically, just after stopping; the symptoms build over the next several minutes, then ease on their own with rest over half an hour or so. Parents and coaches describe a child who starts well but fades, who coughs at the end of a run, or who avoids the sports the other children enjoy. Younger children may simply cough, complain their chest hurts, or opt out of activity rather than report a wheeze. [1] [3]
The clues that make the pattern airway-related, rather than a normal limit of fitness, are the timing and the response. Symptoms that appear after a few minutes of effort and peak after it ends, that are worse in cold dry air and in high-ventilation sports, and that improve with a bronchodilator, all point to the airway. In a child with asthma the exercise limitation sits alongside the other features — nocturnal cough, atopy, interval wheeze — and its severity rises and falls with overall control. In the isolated form there are no such interval features, and exercise is the only provoker. [3] [5]
Age changes the presentation and the report. The preschooler with recurrent viral wheeze may show exercise-triggered cough during play, but is too young for objective confirmation and is managed within the wheeze pathway. The school-age child gives the clearest classic pattern and can perform the tests. The adolescent — particularly the competitive athlete — may under-report symptoms for fear of losing a place in the team, or may over-attribute ordinary breathlessness to asthma, so both under- and over-diagnosis are common and objective testing becomes essential. [5] [8]
Differential Diagnosis
The single most important alternative is inducible laryngeal obstruction, also called vocal cord dysfunction, in which paradoxical adduction of the vocal cords narrows the airway at the larynx. It is distinguished by its pattern: the breathlessness comes on at the peak of exertion rather than after it, the noise is inspiratory stridor rather than an expiratory wheeze, the child feels the tightness in the throat, and the symptoms clear within a minute or two of stopping without a bronchodilator. Mistaking it for exercise-induced bronchoconstriction leads to futile escalation of asthma treatment. [3] [5]
Beyond the larynx, several other conditions masquerade as exercise-limited airways. Simple physical deconditioning produces exertional breathlessness with a normal challenge test and is common in the overweight child. Dysfunctional breathing and hyperventilation cause breathlessness, dizziness and tingling with normal spirometry. Cardiac disease — an arrhythmia, an outflow obstruction, or a channelopathy — is rare but must be considered when there is exertional chest pain, palpitations or syncope, because these are the features that never belong to the airway. [3] [5]
Clinical & Bedside Assessment
Assessment begins with a history that pins down the timing, the triggering sports and conditions, and the response to any reliever already tried, and that then widens to ask about interval asthma symptoms, atopy, family history and — in the adolescent athlete — the pressures that shape reporting. Quantifying how often the child needs a reliever to get through sport, and whether they are using it daily, matters as much as the exercise story itself, because heavy reliever use is both a marker of poor control and a cause of tolerance. [4] [5]
Between episodes the physical examination is usually normal, which is entirely consistent with the diagnosis and must not be taken as reassurance that the airway is fine. When the child is examined during or soon after a provoking effort, an expiratory polyphonic wheeze and a prolonged expiratory phase may be heard. The examination also looks actively for the atopic stigmata that support underlying asthma and for the features that would redirect the diagnosis — a cardiac murmur, signs of deconditioning, or the inspiratory noise of a laryngeal cause. [3] [5]
Investigations
Because symptoms are unreliable and both over- and under-diagnosis are common, the diagnosis should be confirmed objectively wherever the child is old enough to perform the tests, usually from about six years. The reference approach is to measure the fall in FEV1 after a standardised provocation: baseline spirometry is followed by a challenge, and serial FEV1 measurements over the next twenty to thirty minutes capture the maximum fall. A fall of ten percent or more from baseline confirms exercise-induced bronchoconstriction, and the size of the fall grades its severity. [3] [10]
The provocation itself can be a direct exercise challenge or a surrogate that reproduces the same airway drying. A standardised exercise challenge on a treadmill or cycle ergometer, ideally breathing dry air at a high enough intensity, is the most physiological. Eucapnic voluntary hyperpnoea, in which the child voluntarily overbreathes dry air for six minutes, is a sensitive surrogate widely used to certify athletes. Indirect pharmacological challenges with inhaled mannitol or hypertonic saline dehydrate the airway osmotically and provoke the same mediator-driven response, and they are practical office tests. [6] [10]
Two points about interpretation are examined often. First, a normal resting spirometry does not exclude the diagnosis, because between episodes the airway is open; the value of spirometry lies in the challenge, not the baseline. Second, a direct methacholine challenge tests airway hyperresponsiveness in general and can be negative in isolated exercise-induced bronchoconstriction, so an indirect challenge that mimics the exercise stimulus — exercise, eucapnic voluntary hyperpnoea or mannitol — is preferred when the exercise trigger is the specific question. [10] [7]
Management — Resuscitation
Exercise-induced bronchoconstriction is rarely an emergency, because it is transient and self-limiting, but a child can have a genuine acute exacerbation triggered by exercise, and that is managed exactly as any acute asthma attack. The child who does not settle promptly with rest and their reliever, who remains breathless and wheezy, or who shows increasing work of breathing, should be treated as having an acute exacerbation rather than a simple exercise event, and should not be sent back to play. [3] [12]
Salbutamol (acute exercise-triggered bronchospasm, MDI plus spacer)
Loading dose
Give repeated inhaled salbutamol by metered-dose inhaler and spacer for an attack that does not settle with rest; escalate to standard acute-asthma dosing (for example 4 to 12 puffs of 100 microgram per actuation, repeated as needed) if the child deteriorates
Maintenance dose
Reassess after each treatment; a child needing repeated or continuous bronchodilator has an acute exacerbation and needs urgent asthma management, not return to sport
The safe rule for sport is that a child who has had exercise symptoms should stop, rest, and use their reliever, and should return to play only once they are symptom-free. Any child who fails to recover quickly, or who has recurrent severe episodes, needs review of the diagnosis and of asthma control rather than reassurance. Recognising when a self-limiting exercise event has become an acute exacerbation is the resuscitation skill that matters here. [3] [12]
Management — Definitive & Stepwise
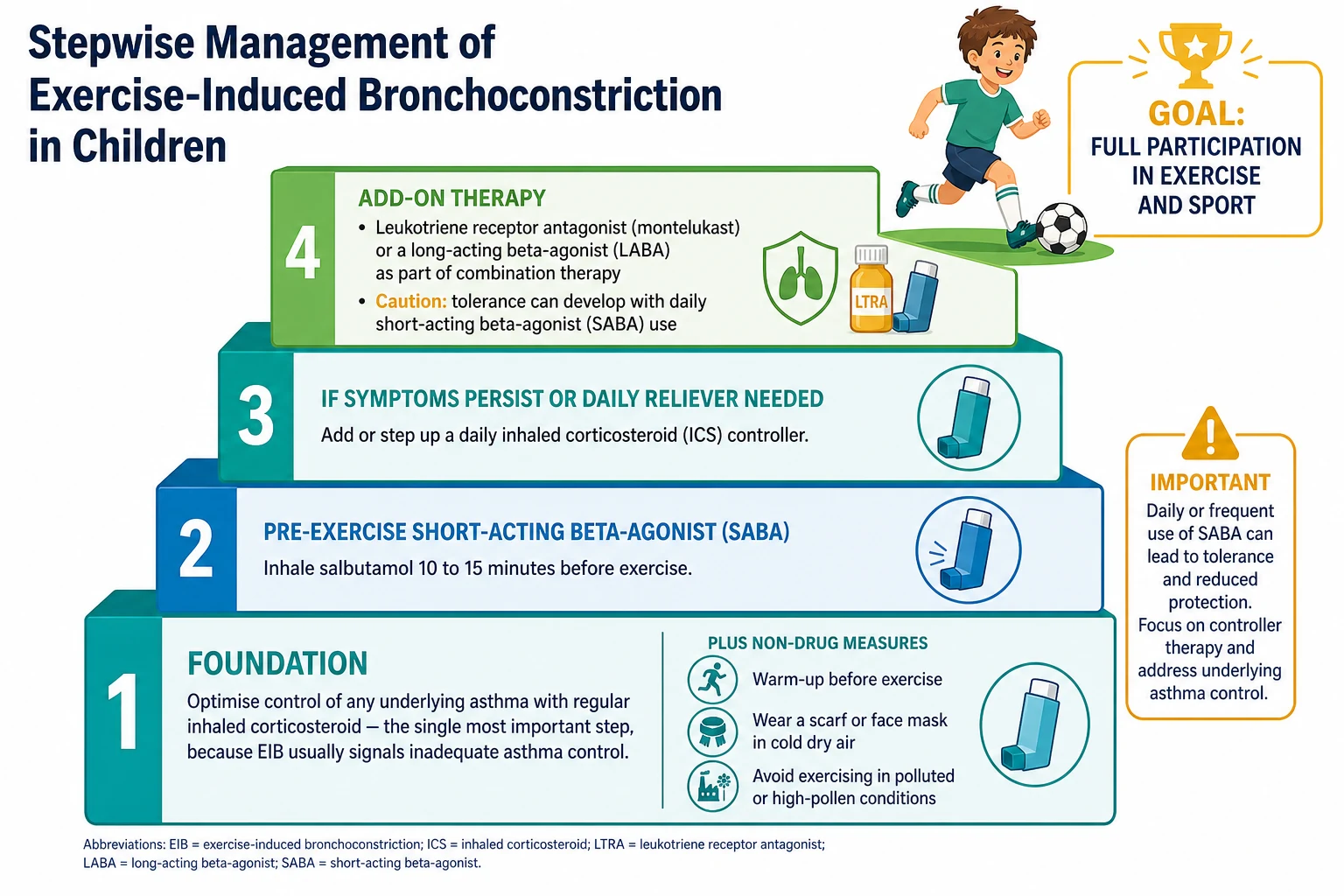
The overriding principle is stated in one sentence: control the underlying asthma first, because in most children exercise symptoms are a manifestation of inadequate control and improve dramatically once the daily inhaled corticosteroid is optimised. Before adding anything exercise-specific, confirm the diagnosis, check adherence and inhaler technique, address triggers, and step up the controller if interval symptoms or a poor challenge result show the airway is under-treated. Treating the disease is what returns most children to unrestricted sport. [4] [12]
Alongside the controller sit the non-drug measures, which are genuinely effective and cost nothing. A ten-to-fifteen-minute warm-up before the main effort induces the refractory period and blunts the subsequent response; breathing through a scarf or a heat-and-moisture-exchange mask warms and humidifies inspired air in the cold; and avoiding exercise in very cold, dry, polluted or high-pollen conditions where possible reduces the provocation. Improving general fitness and, in the overweight child, weight all help. These measures are advised for every child and are the mainstay for the isolated form. [3] [5]
For breakthrough exercise symptoms, an inhaled short-acting beta-agonist taken ten to fifteen minutes before exercise is the standard pre-exercise reliever and protects most children for two to three hours. The crucial caveat is that daily use of a short-acting beta-agonist induces tolerance and reduces this bronchoprotection, so a child needing it every day should have their controller stepped up rather than relying on the reliever. Where symptoms persist despite an optimised inhaled corticosteroid and a pre-exercise reliever, add-on options include a leukotriene receptor antagonist, which specifically blunts the leukotriene-driven exercise response, or an inhaled corticosteroid combined with a long-acting beta-agonist — never a long-acting beta-agonist on its own. [3] [5]
Stepwise approach to the child with exercise-induced bronchoconstriction
Confirm the diagnosis objectively with an exercise or eucapnic voluntary hyperpnoea challenge and exclude the mimics, above all inducible laryngeal obstruction
Optimise control of any underlying asthma with a regular inhaled corticosteroid, and check adherence and inhaler technique
Add non-drug measures: a warm-up before exercise, a scarf or mask in cold dry air, and avoidance of high-pollen and polluted conditions
Prescribe a pre-exercise short-acting beta-agonist 10 to 15 minutes before exercise for breakthrough symptoms
Avoid daily short-acting beta-agonist use, which causes tolerance; step up the controller instead if the reliever is needed most days
Add a leukotriene receptor antagonist or an ICS with a long-acting beta-agonist if symptoms persist despite the above
Aim for full, unrestricted participation in sport as the measure of success
Specific Subtypes & Scenarios
The competitive adolescent athlete is the scenario that most tests judgement. Objective certification with a standardised exercise challenge or eucapnic voluntary hyperpnoea is essential here, both because symptoms are unreliable and because anti-doping rules require documented diagnosis before some inhaled therapies are permitted. Environmental control matters more in these high-ventilation athletes, and the management balances effective bronchoprotection against the tolerance that comes from the daily reliever use a heavy training schedule can encourage. [6] [8]
Isolated exercise-induced bronchoconstriction, without other asthma features, is managed for the trigger rather than for a chronic disease. The emphasis falls on the non-drug measures — warm-up, air conditioning of inspired air, avoidance of the worst conditions — and on a pre-exercise reliever, with a trial of a leukotriene antagonist or a low-dose inhaled corticosteroid if these are insufficient. It is still worth periodic review, because some children with apparently isolated disease declare interval asthma over time. [3] [4]
The winter and pool athlete deserves specific mention, because the environment is doing much of the work. Cross-country skiers, ice-hockey players and swimmers exposed to cold dry air or chlorine by-products have high rates of airway hyperresponsiveness and, over years of heavy training, can develop airway epithelial injury. For them, environmental modification — warming inspired air, improving pool ventilation and water treatment — is as important as any inhaler, and the airway changes may persist after the sport is given up. [6] [7]
Complications & Pitfalls
The complications of exercise-induced bronchoconstriction are mostly those of missed or mismanaged disease. A child whose exercise symptoms go unrecognised or untreated withdraws from sport and physical activity, with lasting costs to fitness, weight, bone health, social participation and self-esteem, and a documented reduction in athletic performance where sport matters to the child. In the child with asthma, persistent exercise symptoms signal ongoing uncontrolled inflammation, with its own risk of exacerbations. [9] [12]
The pitfalls are what examiners probe, and the first is over-diagnosis: labelling every breathless child as asthmatic without an objective test, and thereby treating deconditioning, dysfunctional breathing or, most dangerously, inducible laryngeal obstruction as asthma. The second is under-treatment of the underlying asthma, reaching for a pre-exercise reliever while leaving the daily controller inadequate. The third is the tolerance produced by daily short-acting beta-agonist use, which erodes the very bronchoprotection the child depends on. [3] [5]
Prognosis & Disposition
The prognosis for a correctly diagnosed and treated child is excellent, and the explicit goal is full, unrestricted participation in sport. Once the underlying asthma is controlled and the non-drug measures and a pre-exercise reliever are in place, the overwhelming majority of children exercise normally and compete without limitation. Exercise-induced bronchoconstriction should never be a reason to advise a child to avoid physical activity; regular exercise is beneficial and, with treatment, entirely achievable. [5] [12]
Most children are managed in the community, and disposition is defined by whether the diagnosis is secure and the asthma controlled. A child with a clear history and a good response to controller optimisation and a pre-exercise reliever needs only primary-care follow-up and a plan for sport. Referral for objective challenge testing and specialist review is warranted when the diagnosis is uncertain, when a mimic such as inducible laryngeal obstruction is suspected, when a competitive athlete needs certification, or when symptoms persist despite good asthma control and correct inhaler use. [3] [8]
Special Populations
Socioeconomically disadvantaged and Indigenous children in Australia and New Zealand carry the heaviest asthma burden, and with it the greatest burden of exercise limitation, compounded by less access to objective testing, to affordable controller medication and spacers, and to safe places to exercise. Culturally safe care, reliable access to preventer therapy, and support to keep these children in sport matter more to their outcome than any refinement of the drug ladder, and exercise should be actively encouraged rather than restricted. [4] [12]
The competitive adolescent athlete is a special population in their own right, because reporting is distorted by the desire to keep playing, because anti-doping regulation requires documented diagnosis for some inhaled medicines, and because the transition to self-management and to adult services must be planned. The consultation should engage the young person directly, confirm the diagnosis objectively, and choose a regimen that fits a demanding training schedule while avoiding the daily-reliever tolerance trap. [8] [5]
Younger children and those with neurodisability who cannot perform or coordinate the tests and inhalers need adapted care. In the preschooler, exercise-triggered symptoms are managed within the recurrent-wheeze pathway rather than by formal challenge testing, and delivery uses a spacer with a mask. In the child with disability, the priority is a device and a plan the child and carers can actually use, and the same principle applies — enable participation in activity rather than restrict it. [4] [5]
Evidence, Guidelines & Regional Differences
The governing statements come from respiratory and allergy societies. The American Thoracic Society clinical practice guideline (Parsons 2013) defines the diagnosis by a fall in FEV1 of at least ten percent on challenge, grades severity, and sets out the treatment hierarchy of controlling asthma, a pre-exercise reliever, and add-on therapy; the joint allergy practice parameter (Weiler 2010) and its 2016 update (Weiler 2016) give the pathogenesis, prevalence and management in detail. The European Respiratory Society technical standard (Hallstrand 2018) codifies the indirect challenge methodology, and the Global Initiative for Asthma strategy (Levy 2023) frames exercise symptoms as a marker of asthma control. [3] [10] [12]
The mechanistic evidence is worth citing precisely. Anderson and Daviskas (2000) articulated the osmotic hypothesis that airway water loss and hyperosmolarity drive mast cell mediator release, and Kippelen and colleagues (2018) summarised the mediators and biomarkers involved. The diagnostic and athlete literature — Rundell and Slee (2008) on indirect challenges, Rundell and colleagues (2004) comparing field exercise with eucapnic voluntary hyperpnoea, and Boulet and O'Byrne (2015) on athletes — established that symptoms alone are unreliable and objective testing is required, while Price and colleagues (2014) documented the measurable effect of untreated disease on athletic performance. [2] [7] [9]
The regional differences are of emphasis and access rather than principle. All the major frameworks agree on objective confirmation, on controlling the underlying asthma first, and on the warm-up and pre-exercise reliever, and they differ mainly in preferred challenge methods, licensed ages and devices, anti-doping rules for athletes, and the local arrangements for affordable preventer and spacer access. The live controversies are how best to confirm the diagnosis in ordinary practice where formal challenge testing is scarce, and how to recognise and manage the frequently co-existing inducible laryngeal obstruction. [3] [5]
Exam Pearls
The exercise-induced bronchoconstriction essentials — 'RUN-SPORT'
References
- [1]McFadden ER Jr; Gilbert IA Exercise-induced asthma. N Engl J Med, 1994.PMID 8152449
- [2]Anderson SD; Daviskas E The mechanism of exercise-induced asthma is ... J Allergy Clin Immunol, 2000.PMID 10984363
- [3]Parsons JP; Hallstrand TS; Mastronarde JG; Kaminsky DA; Rundell KW; Hull JH; et al An official American Thoracic Society clinical practice guideline: exercise-induced bronchoconstriction. Am J Respir Crit Care Med, 2013.PMID 23634861
- [4]Weiler JM; Anderson SD; Randolph C; Bonini S; Craig TJ; Pearlman DS; et al Pathogenesis, prevalence, diagnosis, and management of exercise-induced bronchoconstriction: a practice parameter. Ann Allergy Asthma Immunol, 2010.PMID 21167465
- [5]Weiler JM; Brannan JD; Randolph CC; Hallstrand TS; Parsons J; Silvers W; et al Exercise-induced bronchoconstriction update-2016. J Allergy Clin Immunol, 2016.PMID 27665489
- [6]Rundell KW; Slee JB Exercise and other indirect challenges to demonstrate asthma or exercise-induced bronchoconstriction in athletes. J Allergy Clin Immunol, 2008.PMID 18678339
- [7]Rundell KW; Anderson SD; Spiering BA; Judelson DA Field exercise vs laboratory eucapnic voluntary hyperventilation to identify airway hyperresponsiveness in elite cold weather athletes. Chest, 2004.PMID 15006949
- [8]Boulet LP; O'Byrne PM Asthma and exercise-induced bronchoconstriction in athletes. N Engl J Med, 2015.PMID 25671256
- [9]Price OJ; Hull JH; Backer V; Hostrup M; Ansley L The impact of exercise-induced bronchoconstriction on athletic performance: a systematic review. Sports Med, 2014.PMID 25129699
- [10]Hallstrand TS; Leuppi JD; Joos G; Hall GL; Carlsen KH; Kaminsky DA; et al ERS technical standard on bronchial challenge testing: pathophysiology and methodology of indirect airway challenge testing. Eur Respir J, 2018.PMID 30361249
- [11]Kippelen P; Anderson SD; Hallstrand TS Mechanisms and Biomarkers of Exercise-Induced Bronchoconstriction. Immunol Allergy Clin North Am, 2018.PMID 29631728
- [12]Levy ML; Bacharier LB; Bateman E; Boulet LP; Brightling C; Buhl R; et al Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Prim Care Respir Med, 2023.PMID 36754956