Paeds · respiratory-sleep-and-airway
Foreign-body aspiration
Also known as Foreign-body aspiration · Inhaled foreign body · Airway foreign body · Aspirated foreign body · Tracheobronchial foreign body · Choking in children
Fellowship guide to foreign-body aspiration in children: the choking toddler and the three clinical phases, why the small paediatric airway and organic objects make aspiration dangerous, the anatomy that sends objects into the right bronchus, the valve mechanisms that produce air trapping or collapse, the crucial teaching that a normal chest radiograph does not exclude aspiration, the choking basic-life-support algorithm, and rigid bronchoscopy as the definitive diagnostic and therapeutic step.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A well toddler is eating peanuts on the sofa when he suddenly coughs, splutters and goes briefly blue, then settles and looks completely normal within a minute. That single sequence is the whole of foreign-body aspiration in miniature: a dramatic choking event, a deceptively quiet interval, and a child who is now carrying an inhaled object in the airway. Foreign-body aspiration is the inhalation of any solid or semi-solid object below the vocal cords into the trachea or bronchi, and it is one of the commonest preventable causes of death and serious airway morbidity in early childhood. [1]
The reason it earns a whole topic is that the diagnosis is made by suspicion, not by any single test. The choking history is the most powerful clue there is, yet the event is often unwitnessed, the child looks well by the time they arrive, and the chest radiograph is frequently normal. A clinician who waits for confidence before acting is the clinician who misses the object, and a missed foreign body smoulders on into recurrent pneumonia and bronchiectasis. The skill is to keep the diagnosis alive on a suggestive story and to move to the airway team early. [1] [3]
Classification
The most clinically useful way to sort an inhaled foreign body is by where it sits, because the location dictates how dangerous it is and how fast you must act. A laryngeal or supraglottic object is the rarest but the deadliest, because it can cause complete obstruction and asphyxia at the doorway of the airway. A tracheal object is also immediately life-threatening and may be mobile, producing an audible slap and a to-and-fro wheeze. A bronchial object is by far the commonest and the one behind the classic missed-diagnosis story, and it settles more often on the right. [2] [4]
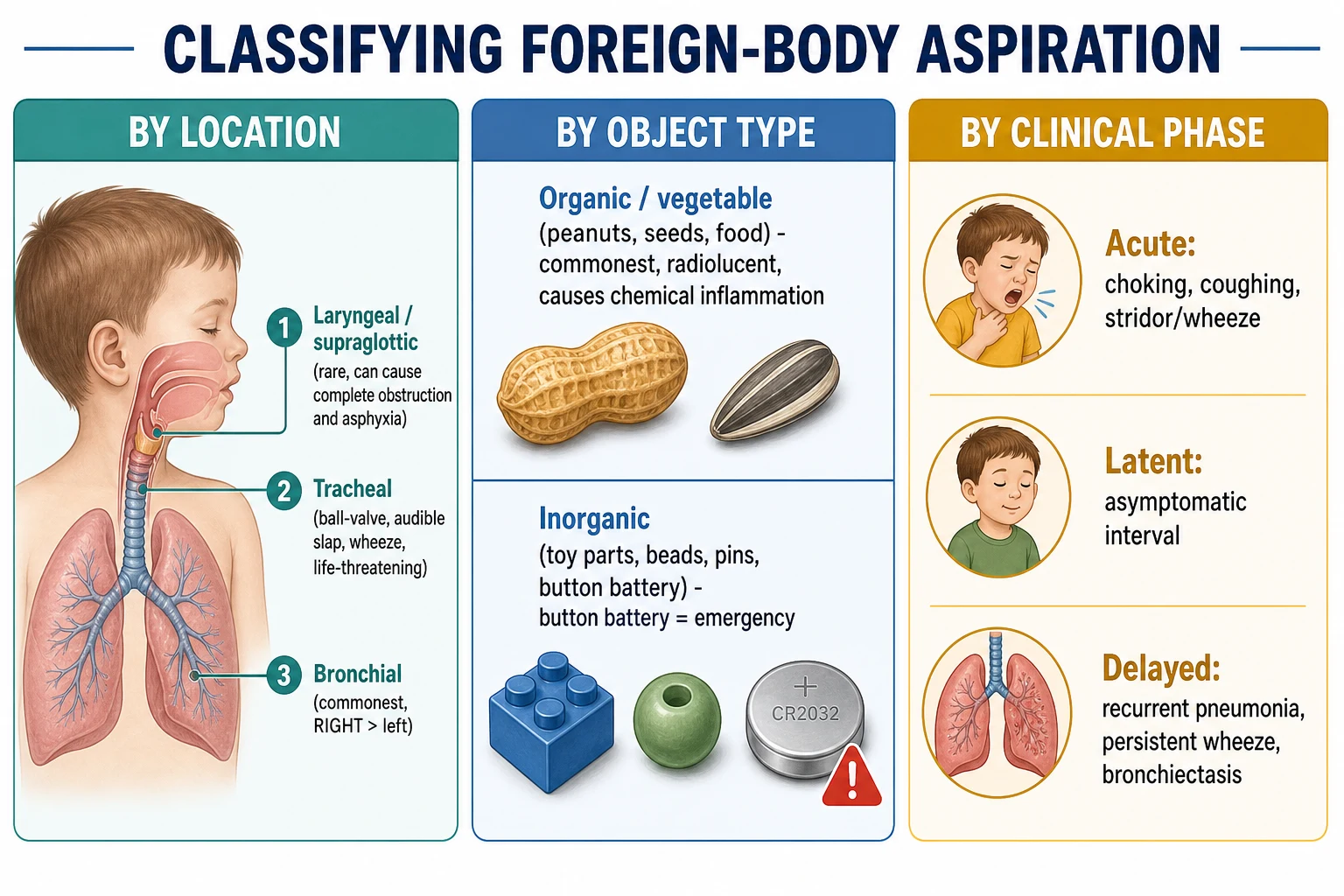
The nature of the object is the second axis, and it changes both the tissue reaction and what you see on imaging. Organic material — nuts, seeds and other food — is the commonest culprit, is almost always radiolucent, and provokes a brisk chemical inflammation as it releases oils into the mucosa. Inorganic objects such as toy parts, beads and pins behave more inertly, and some are radio-opaque and visible on plain films. A button battery is a category of its own: an aspirated or ingested battery is an emergency because it burns tissue rapidly through a caustic and electrical injury. [1] [11]
[2] [4]Epidemiology & Risk Factors
Foreign-body aspiration is overwhelmingly a disease of the toddler, clustering in the one-to-three-year age group, and boys are affected more often than girls. Children of this age explore the world with their mouths, have immature dentition that cannot grind hard food, and lack the coordinated airway protection of older children, so a peanut or a seed slips past the larynx with ease. Nuts, seeds and other food items are the commonest objects worldwide, with small toy parts and household items making up much of the rest. [2] [1]
The epidemiology of the objects themselves is remarkably consistent across large series. A meta-analysis of published series confirmed the toddler peak, the male predominance and the food predominance, and the anatomical series show that bronchial lodgement is far commoner than laryngotracheal lodgement, with a right-sided predominance. Nonfatal choking on food is common enough to be tracked as a public-health problem, and hard, round and compressible foods — nuts, hard sweets, grapes and hot dog pieces — are repeatedly identified as the highest-risk items. [2] [5]
The preventable nature of the problem drives its public-health approach. High-risk foods are discouraged for young children, small toy parts are regulated and age-labelled, and supervision during eating is emphasised, all of which the paediatric prevention literature underpins. Risk is higher where these safeguards are weaker, so socioeconomic disadvantage and settings with less food and toy regulation carry a greater burden. Button-battery injuries are rising despite safety efforts, which keeps the aspirated or ingested battery firmly on the agenda. [6] [11]
Pathophysiology
The paediatric airway is small, and small airways obstruct catastrophically, because resistance to flow rises steeply as the lumen narrows. When an object lodges in a bronchus it rarely blocks it cleanly; instead it behaves like a valve, and the type of valve determines what happens to the lung beyond it. Understanding these valve mechanisms explains the whole spectrum of clinical signs and radiographic findings, from a normal film to dramatic hyperinflation to a collapsed lobe. [1] [4]
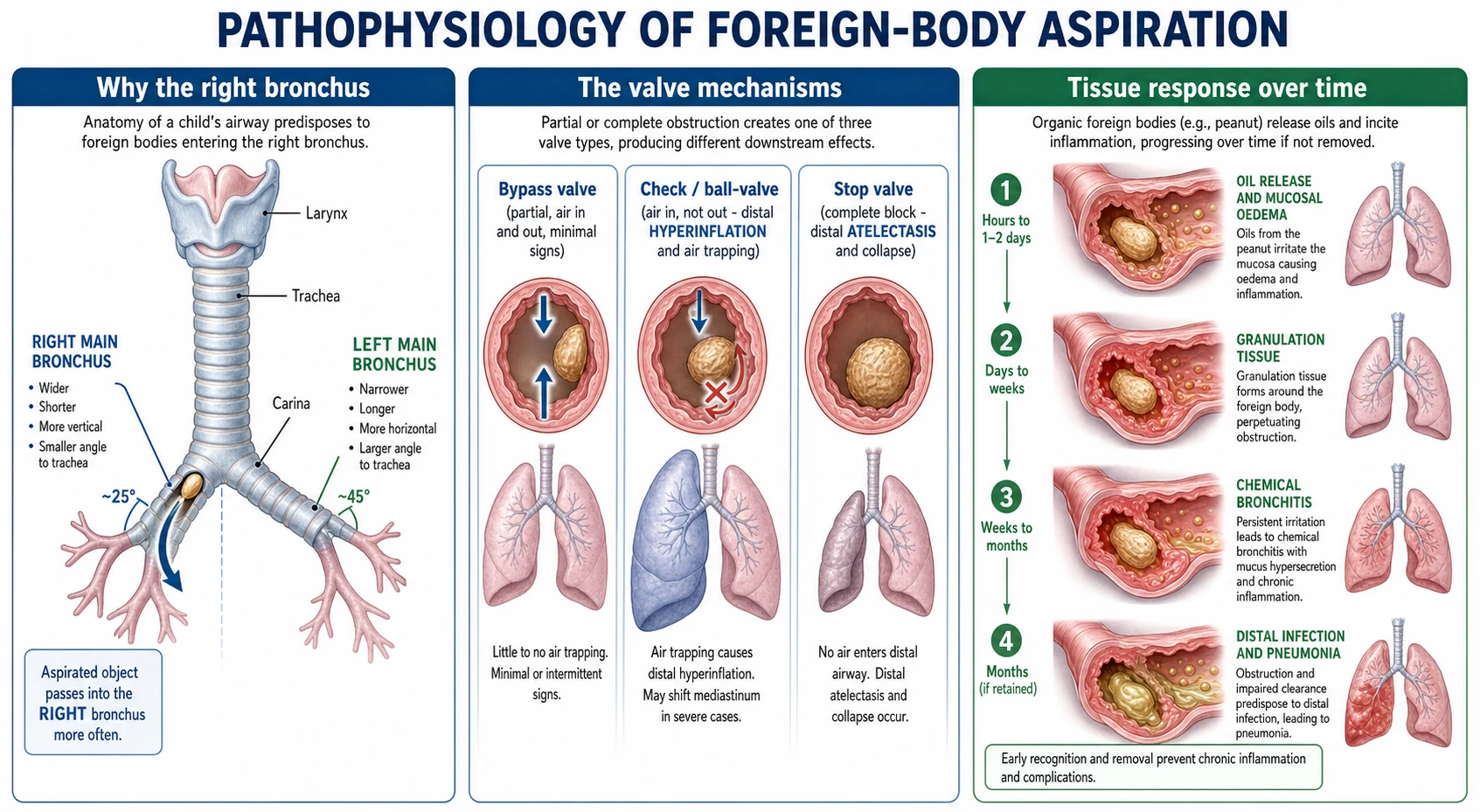
Airway geometry is the first piece. In older children and adults the right main bronchus is wider, shorter and more vertical than the left, so an aspirated object tends to follow the more direct path to the right, and the right-sided predominance is reflected in the large surgical series. The valve mechanism is the second piece. A partial bypass obstruction lets air move in and out with few signs; a check or ball-valve lets air in but not out and over-inflates the lung beyond it; and a complete stop-valve blocks all flow, so the trapped gas resorbs and the lung collapses into atelectasis. [4] [1]
The nature of the object then decides the tissue reaction over time. An inert inorganic object may sit quietly, but organic material — the peanut being the archetype — releases oils that irritate the mucosa and set off a chemical bronchitis. Mucosal oedema and granulation tissue form around the object, worsening the obstruction and making later removal harder and bloodier. Impaired clearance behind the obstruction then invites bacterial infection, so a retained organic foreign body marches from chemical inflammation to recurrent pneumonia and, if left, to permanent bronchiectasis. [1] [12]
Clinical Presentation
The textbook presentation is the acute choking crisis: a previously well toddler who suddenly coughs, gags, splutters, and may develop stridor, wheeze or transient cyanosis while eating or playing with a small object. Many present in exactly this way and the story is unmistakable. But the aspiration event is frequently unwitnessed, and by the time the child reaches medical attention the acute phase has passed, so the clinician meets a well-looking child with a normal or near-normal examination and must reconstruct the event from the parents. [1] [3]
The classic bronchial triad of cough, unilateral wheeze and decreased breath sounds on the affected side is highly suggestive but is present in only a minority of children, so its absence never excludes aspiration. Far commoner is a single persistent sign: an unexplained new cough, a focal monophonic wheeze that does not shift, or reduced air entry over one lung field. Tracheal and laryngeal objects are more dramatic, with stridor, a hoarse or absent voice, and, at worst, complete obstruction and asphyxia. [1] [7]
[1] [7]The delayed presentation is the one that trips clinicians. A child with a retained bronchial object may present weeks later with recurrent pneumonia that always affects the same lobe, a wheeze that does not respond to bronchodilators, a chronic cough, or a lobar collapse found on a film taken for another reason. Any of these focal, fixed and recurrent respiratory patterns should prompt a careful search for a choking history and a low threshold for bronchoscopy. [1] [12]
Differential Diagnosis
In the acute setting the differential for a sudden choking, coughing or wheezing episode in a toddler includes croup, an acute viral wheeze or asthma attack, anaphylaxis with laryngeal oedema, and epiglottitis. What sets aspiration apart is the abruptness in a previously well, afebrile child, the frequent link to eating or to a small object, and the focal rather than diffuse chest signs. A history of a discrete choking event, even a brief one, shifts the balance decisively toward a foreign body and away from the infective and diffuse causes. [1] [3]
In the child who presents later, the differential becomes the causes of a persistent focal or recurrent chest problem: recurrent or non-resolving pneumonia, poorly controlled or atypical asthma, a congenital lung malformation, an endobronchial mass, and tuberculosis in the right setting. The discriminators for a retained foreign body are the fixed, one-sided and recurring nature of the findings — the pneumonia that keeps returning to the same lobe, the monophonic wheeze that never moves, the collapse that will not re-expand — against a background that may include a forgotten choking episode. [1] [12]
Clinical & Bedside Assessment
Assessment begins with stability, exactly as for any airway problem. In the acutely choking child the first judgement is whether the cough is effective: a child who is coughing forcefully, crying or speaking is moving air and should be encouraged to cough, whereas a child with a silent or feeble cough, a silent chest, cyanosis or falling consciousness has a critical obstruction and needs immediate intervention. This effective-versus-ineffective cough decision drives the whole choking algorithm and must be made in seconds. [6] [1]
In the stable child the history is the assessment, and it is worth more than any examination finding. Ask specifically about a choking, coughing or gagging episode, what the child was eating or playing with, and whether symptoms began abruptly, because a positive choking history is the strongest single predictor of aspiration. The examination looks for asymmetry: a focal monophonic wheeze, reduced air entry or dullness over one lung field, and any stridor or voice change that would suggest a laryngotracheal object. [3] [7]
The key clinical point, borne out by the meta-analyses of preoperative findings, is that the history, the examination and the chest radiograph each have imperfect sensitivity, so no single one can exclude aspiration. A positive choking history, abnormal auscultation and abnormal imaging each raise the probability, but a normal result on any of them does not lower it enough to abandon the diagnosis. When the story is convincing, the assessment concludes at the same place regardless of the examination: refer for bronchoscopy. [7] [3]
Investigations
Imaging supports the diagnosis but never rules it out, and the first-line test is a chest radiograph. Because most objects are radiolucent, the film is read for the indirect signs of the valve mechanism: unilateral air trapping with hyperinflation and mediastinal shift away from the affected side, or lobar or segmental collapse. Inspiratory and expiratory films, or lateral decubitus views in an uncooperative toddler, can unmask air trapping that a single inspiratory film misses. A radio-opaque object is directly visible, but this is the minority. [10] [7]
The crucial teaching point is that a completely normal chest radiograph is common in confirmed aspiration and does not exclude it. The meta-analytic yield of preoperative findings shows that imaging, like history and examination, is only moderately sensitive, so a normal film in a child with a convincing choking history must not lead to discharge. Computed tomography can characterise an object and the airway in selected, stable and diagnostically uncertain cases, but it is not required before bronchoscopy when the history is convincing and adds radiation and delay. [7] [10]
[7] [8]Bronchoscopy is both the final investigation and the treatment, and it is the only test that definitively confirms or excludes an airway foreign body. A convincing choking history is itself an indication for bronchoscopy, which is undertaken to inspect the airway directly and to remove any object found. When history, examination and imaging are all equivocal, the balance is between a negative bronchoscopy in a small number of children and a missed foreign body in the rest, and a low threshold is the safer error. [8] [12]
Management — Resuscitation
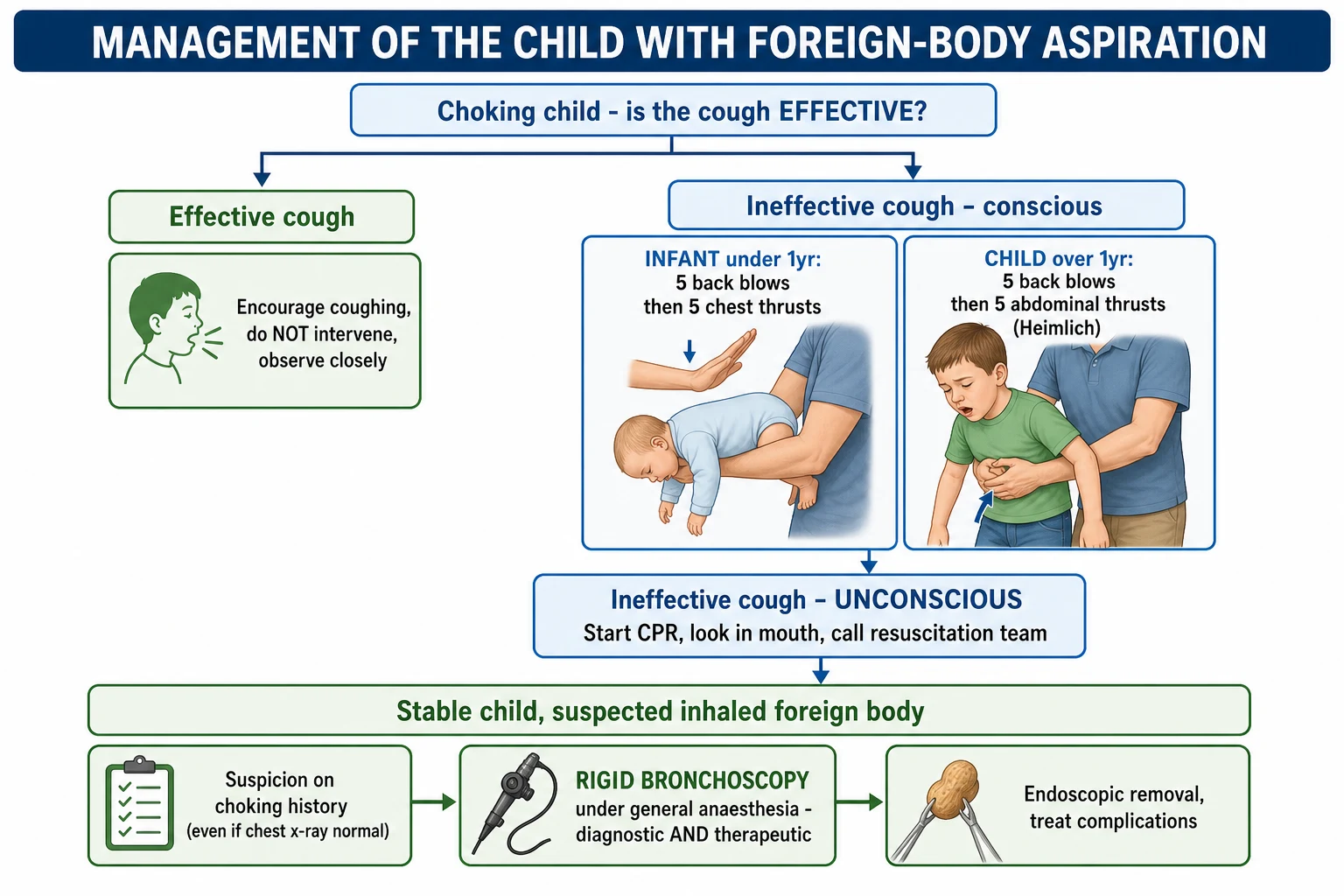
The acutely choking child is managed by the choking basic-life-support algorithm, and its first branch is the effective-versus-ineffective cough. If the cough is effective, do not intervene beyond encouraging the child to keep coughing and watching closely, because forced manoeuvres can convert a partial obstruction into a complete one. If the cough is ineffective but the child is still conscious, deliver airway clearance manoeuvres appropriate to the age, alternating and reassessing after each cycle. [6] [1]
The manoeuvres differ by age, and getting this right is a common exam and clinical point. An infant under one year is given five back blows followed by five chest thrusts, held head-down along the rescuer's forearm, and abdominal thrusts are avoided because of the risk of visceral injury. A child over one year is given five back blows followed by five abdominal thrusts (the Heimlich manoeuvre), and the cycles are repeated. Blind finger sweeps are not performed, because they can push the object further down. [6] [1]
The choking child algorithm
Assess the cough: is it effective or ineffective?
Effective cough: encourage coughing, do not intervene, observe closely
Ineffective cough, conscious infant under 1 year: five back blows then five chest thrusts, repeat and reassess
Ineffective cough, conscious child over 1 year: five back blows then five abdominal thrusts, repeat and reassess
Do not perform blind finger sweeps
If the child becomes unconscious: start CPR, look for and remove a visible object only, call the resuscitation or emergency team
After relief or removal, assess for aspiration and airway injury
If the child becomes unconscious, the priority shifts to cardiopulmonary resuscitation: begin chest compressions and ventilations, look inside the mouth and remove an object only if it is clearly visible, and summon the resuscitation or emergency team. In hospital, direct laryngoscopy allows a visualised object at the glottis to be removed with Magill forceps by an experienced operator. A critical laryngeal or tracheal obstruction that cannot be relieved needs immediate advanced airway rescue by the anaesthetic and ENT team. [1] [4]
Management — Definitive & Stepwise
For the stable child with a suspected inhaled foreign body, the definitive management is rigid bronchoscopy under general anaesthesia, which is simultaneously the diagnostic and the therapeutic procedure. It is undertaken semi-urgently once the diagnosis is suspected on history, because an object left in place drives ongoing inflammation and infection and becomes harder to remove as granulation tissue forms around it. The airway is inspected, the object is grasped and extracted, and the airway is re-inspected for a second fragment or object. [12] [8]
[8] [9]Rigid bronchoscopy remains the standard for removal because it secures and ventilates the airway through the scope while the object is manipulated, which is why it is the workhorse in the large paediatric series. Flexible bronchoscopy is increasingly used for diagnosis and for selected retrievals, and comparative reviews show it can be effective in appropriate cases, but rigid bronchoscopy is preferred for large, impacted or awkwardly shaped objects and for the child in whom airway control is paramount. The choice is made by the airway team according to the object and the child. [8] [9]
The procedure is a coordinated anaesthetic and surgical undertaking, and the shared airway is its central challenge. The anaesthetic literature on thousands of cases sets out the balance between spontaneous and controlled ventilation, the risk of dislodging the object during instrumentation, and the management of hypoxia, laryngospasm and bronchospasm around extraction. After removal, the child is observed for airway oedema and post-obstructive complications, and any residual pneumonia or collapse is treated. Complications are more likely with delayed presentation, retained granulation tissue and organic objects. [4] [9]
Specific Subtypes & Scenarios
The organic bronchial object, the peanut, is the archetype and the one an examiner expects in full. It lodges in a bronchus, more often the right, sets off a chemical bronchitis as it releases oils, and, if unrecognised, produces the delayed picture of recurrent focal pneumonia and eventual bronchiectasis. It is usually radiolucent, so the diagnosis rests on the choking history and the indirect radiographic signs, and it is removed by rigid bronchoscopy. The organic object is both the commonest and the most inflammatory scenario. [1] [12]
The laryngotracheal object is the airway emergency. An object at the larynx can cause complete obstruction and asphyxia within minutes, and a mobile tracheal object can produce a to-and-fro audible slap while threatening to impact at the glottis. These children present acutely and dramatically, and management follows the choking algorithm and, in hospital, urgent laryngoscopy and airway rescue rather than a semi-elective bronchoscopy pathway. Recognising the laryngotracheal object as immediately life-threatening is the key distinction from the bronchial object. [1] [4]
Across Australia, New Zealand, the United Kingdom and Europe the approach is uniform: the choking child is managed by the resuscitation-council basic-life-support algorithm, and the stable child with a suggestive choking history is referred for rigid bronchoscopy regardless of a normal chest radiograph. Prevention is coordinated through food and small-parts regulation and public education about high-risk foods and supervision. A child in a rural or remote setting with a suspected airway foreign body is stabilised and retrieved to a centre with paediatric airway and anaesthetic expertise, because bronchoscopy requires a skilled shared-airway team. [6] [9]
The button battery deserves separate emphasis because it is rising and uniquely dangerous. An aspirated or ingested button battery causes rapid caustic and electrical injury to the tissue it contacts, so it is an emergency that mandates urgent localisation and removal rather than the watchful pathway used for an inert object. Injuries are increasing despite safety efforts, which keeps the battery a live problem in any child with an unexplained airway or oesophageal presentation and a possible access to small electronics. [11] [1]
Complications & Pitfalls
The complications of aspiration fall into the immediate and the delayed. The immediate danger is complete airway obstruction and asphyxia from a laryngeal or tracheal object, which can kill within minutes and is the reason the choking algorithm exists. The delayed complications follow a retained bronchial object: recurrent or persistent pneumonia in the same territory, lobar or segmental collapse, post-obstructive infection, and, if the object stays long enough, permanent bronchiectasis of the affected segment. Removal itself carries the risks of airway oedema, bleeding from granulation tissue, and fragmentation of the object. [1] [12]
The pitfalls are almost all failures of suspicion. The commonest is to be reassured by a well-looking child in the latent phase, or by a normal chest radiograph, and to discharge a child who has aspirated. The second is to misdiagnose a retained foreign body as asthma or recurrent infection and to treat the symptom for months while the object smoulders. The third is to distress or intervene inappropriately in a child with an effective cough, converting a partial obstruction into a complete one. The fourth is to underestimate the button battery. [1] [11]
Prognosis & Disposition
The prognosis of a promptly recognised and removed foreign body is excellent, and the great majority of children recover fully after uncomplicated rigid bronchoscopy. The large endoscopic series show high success rates for removal with low complication rates when the object is retrieved early and by an experienced team. The outlook worsens with delay: a long-retained organic object causes granulation, chronic infection and bronchiectasis, and can leave permanent localised lung damage even after removal. Timely diagnosis is therefore the main determinant of outcome. [12] [1]
Disposition follows the phase and the stability of the child. A child who is actively choking with a critical obstruction is a resuscitation emergency managed on the spot and then in a high-dependency or intensive-care setting. A stable child with a suspected foreign body is admitted and referred for bronchoscopy on a semi-urgent basis, kept fasted in anticipation of anaesthesia. After successful removal, a well child with no complications is observed and discharged, while a child with post-obstructive pneumonia or airway injury stays for treatment. [9] [12]
The rural and remote child needs a disposition plan of its own. Because bronchoscopy requires a skilled shared-airway team that a small hospital may not have, a child with a suspected airway foreign body is stabilised locally, kept calm and fasted, and retrieved to a paediatric centre, with the retrieval service and the receiving airway team involved early. The aim is to move the child to definitive care before the object causes further harm. [9] [1]
Special Populations
The child with a neurodisability or an unsafe swallow is at higher risk and presents atypically. Impaired airway protection, abnormal oral behaviour and difficulty giving a history mean aspiration may be unwitnessed and the presentation delayed, so a low threshold and a careful collateral history are essential. These children may also aspirate food and secretions chronically, and distinguishing a discrete inhaled object from ongoing aspiration requires attention to a focal, fixed respiratory change. [1] [3]
Socioeconomic disadvantage and settings with weaker food and toy regulation carry a greater burden, because the preventive safeguards that reduce exposure to high-risk foods and small parts are less effective there. The prevention literature emphasises regulation of small parts, labelling and public education, and the benefits of these measures are unevenly distributed. Equitable prevention therefore targets access to safe food guidance and product safety in the communities at greatest risk. [6] [5]
The rural and remote child, discussed under disposition, is a special population by geography. The absence of a local shared-airway team turns a straightforward removal into a retrieval problem, and the management pivots on early stabilisation, calm handling to avoid dislodging a mobile object, and prompt transfer. Indigenous and other under-served children are over-represented among those for whom distance and access shape the outcome, which makes early recognition and retrieval planning a matter of equity as well as clinical care. [9] [1]
Evidence, Guidelines & Regional Differences
The evidence base rests on large series and meta-analyses rather than randomised trials, which fits a diagnosis made by suspicion and treated by a procedure. The meta-analysis of published airway-foreign-body series established the demographics — the toddler peak, the male and food predominance, and the bronchial and right-sided predominance — and the large anaesthetic review of nearly thirteen thousand cases mapped the location distribution and the anaesthetic challenges of the shared airway. Together they define who aspirates, what they aspirate and where it goes. [2] [4]
The diagnostic evidence is dominated by the meta-analyses of preoperative findings, which quantify the imperfect sensitivity of history, examination and imaging and underpin the central teaching that no single one excludes aspiration. The comparative reviews of rigid and flexible bronchoscopy define the modern removal debate, confirming rigid bronchoscopy as the standard while establishing a growing role for flexible bronchoscopy in diagnosis and selected retrieval. The button-battery injury data document a rising and preventable harm. [7] [8] [11]
[2] [8]Across ANZ, the United Kingdom, Europe and North America the core is uniform: the resuscitation-council choking algorithm for the acute obstruction, rigid bronchoscopy for the stable suspected foreign body regardless of a normal radiograph, and prevention through food and small-parts regulation and public education. What varies is the local availability of paediatric airway teams and the retrieval arrangements for rural and remote children, and the residual burden of preventable choking, which tracks food guidance, product regulation and socioeconomic factors. The unifying message is to suspect the diagnosis early and to refer for bronchoscopy. [6] [9]
Exam Pearls
Approach to the choking child — 'CHOKING'
References
- [1]Salih AM; Alfaki M; Alam-Elhuda DM Airway foreign bodies: A critical review for a common pediatric emergency. World J Emerg Med, 2016.PMID 27006731
- [2]Foltran F; Ballali S; Passali FM; Kern E; Morra B; Passali GC; Berchialla P; Lauriello M; Gregori D Foreign bodies in the airways: a meta-analysis of published papers. Int J Pediatr Otorhinolaryngol, 2012.PMID 22333317
- [3]Sink JR; Kitsko DJ; Georg MW; Winger DG; Simons JP Predictors of Foreign Body Aspiration in Children. Otolaryngol Head Neck Surg, 2016.PMID 27071446
- [4]Fidkowski CW; Zheng H; Firth PG The anesthetic considerations of tracheobronchial foreign bodies in children: a literature review of 12,979 cases. Anesth Analg, 2010.PMID 20802055
- [5]Chapin MM; Rochette LM; Annest JL; Haileyesus T; Conner KA; Smith GA Nonfatal choking on food among children 14 years or younger in the United States, 2001-2009. Pediatrics, 2013.PMID 23897916
- [6]Committee on Injury, Violence, and Poison Prevention Prevention of choking among children. Pediatrics, 2010.PMID 20176668
- [7]Zoizner-Agar G; Merchant S; Wang B; April MM Yield of preoperative findings in pediatric airway foreign bodies - A meta-analysis. Int J Pediatr Otorhinolaryngol, 2020.PMID 33068947
- [8]Safia A; Abd Elhadi U; Bader R; Khater A; Karam M; Bishara T; Massoud S; Merchavy S; Farhat R Flexible versus Rigid Bronchoscopy for Tracheobronchial Foreign Body Removal in Children: A Comparative Systematic Review and Meta-Analysis. J Clin Med, 2024.PMID 39337140
- [9]Keil O; Huzhva Y; Rigterink V; Dennhardt N; Boethig D; Nickel K; Carlens J; Dittrich AM; Grychtol R; Wetzke M; Hansen G; Schwerk N; Schütz K; Beck CE Rigid and Flexible Bronchoscopy for Foreign Body Removal in Children: Complications, Risk Factors and Anesthetic Management. Pediatr Pulmonol, 2025.PMID 40844046
- [10]Kvist O; Garcia JP Has the cat got your tongue, or is something obstructing your throat? A review of imaging of ingested and aspirated foreign bodies in the paediatric population. Pediatr Radiol, 2024.PMID 39419854
- [11]Diamond-Pott H; Shaari DS; Iraj L; O'Sullivan-Bakshi S; Londino A; Wong SJ; Laitman BM Rising Pediatric Button Battery Injuries Despite Safety Efforts: An Analysis of National Injury Data. Laryngoscope, 2026.PMID 42411449
- [12]De Palma A; Brascia D; Fiorella A; Quercia R; Garofalo G; Genualdo M; Pizzuto O; Costantino M; Simone V; De Iaco G; Nex G; Maiolino E; Schiavone M; Signore F; Panza T; Cardinale F Endoscopic removal of tracheobronchial foreign bodies: results on a series of 51 pediatric patients. Pediatr Surg Int, 2020.PMID 32468145