Paeds · respiratory-sleep-and-airway
Neuromuscular respiratory failure and airway clearance
Also known as Neuromuscular respiratory failure · Respiratory failure in neuromuscular disease · Airway clearance in neuromuscular weakness · Assisted cough · Cough assist · Mechanical insufflation-exsufflation · Breath stacking · Lung volume recruitment · DMD respiratory care · SMA respiratory care · Secretion management
Fellowship guide to neuromuscular respiratory failure and airway clearance in children: the two-part respiratory pump-and-cough failure that follows weakness of the diaphragm, expiratory and bulbar muscles in Duchenne muscular dystrophy, spinal muscular atrophy and related disorders. The page covers how inspiratory weakness produces nocturnal then daytime hypoventilation while expiratory and bulbar weakness produce an ineffective cough with secretion retention, how to monitor with vital capacity, peak cough flow and overnight carbon dioxide, and the ladder of airway clearance from manual assisted cough through breath stacking and lung volume recruitment to mechanical insufflation-exsufflation, alongside non-invasive ventilation, the chest-infection rule to clear secretions and ventilate rather than merely oxygenate, and the surveillance that has transformed survival.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a boy with Duchenne muscular dystrophy who is well by day but wakes with a headache, dozes at school and has had three chest infections this winter. His lungs are structurally normal, yet the muscles that drive breathing and cough are too weak to do their work. This is neuromuscular respiratory failure: the respiratory pump and the cough fail because the diaphragm, the expiratory muscles and the bulbar muscles are weak, not because the lung itself is diseased. [1] [3]
The single most useful idea is that neuromuscular weakness attacks breathing in two separate ways. Weak inspiratory muscles, chiefly the diaphragm, cause hypoventilation that appears first in sleep and later by day, so carbon dioxide rises. Weak expiratory and bulbar muscles cause an ineffective cough, so secretions are retained and chest infections become frequent and dangerous. A child can have one problem, the other, or both, and each needs its own treatment. [1] [6]
The reason the topic matters so much is that proactive respiratory care changes the outcome. Anticipating hypoventilation and starting non-invasive ventilation, putting airway clearance in place before the cough fails, and following a clear plan during chest infections have all lengthened and improved life in Duchenne muscular dystrophy and spinal muscular atrophy. The clinician's task is to monitor the pump and the cough over time, and to act before a predictable crisis rather than after it. [2] [4]
Classification
Sort these children first by where the weakness sits in the motor unit, because that names the disease and its trajectory, and then by which of the three respiratory problems dominates, because that decides the treatment. The figure below maps the motor-unit levels onto their diseases and lays the three respiratory problems and the markers of severity alongside them. [1] [6]

Group the diseases by the level of the motor unit that is affected. Anterior horn cell disease is led by spinal muscular atrophy; peripheral nerve disease includes Guillain-Barre syndrome and the hereditary neuropathies; neuromuscular junction disease includes myasthenia and congenital myasthenic syndromes and infant botulism; and muscle disease includes Duchenne muscular dystrophy, the congenital myopathies and myotonic dystrophy. The level predicts the tempo, whether the weakness is fixed, progressive or fluctuating, and the pattern of respiratory involvement. [1] [5]
Then classify by the respiratory problem, because a child may need ventilation, airway clearance, or both. Nocturnal hypoventilation is the failure of the inspiratory pump and appears first in rapid eye movement sleep. Ineffective cough with secretion retention is the failure of the expiratory and bulbar muscles, measured by a falling peak cough flow. Aspiration is the failure of the bulbar muscles to protect the airway during swallowing. Severity is graded by the vital capacity, the peak cough flow, the carbon dioxide in sleep and then by day, and finally by ventilator dependence. [1] [6]
Pump failure (inspiratory)
- Weak diaphragm and inspiratory muscles
- Low vital capacity; supine drop with diaphragm weakness
- Nocturnal hypoventilation first, then daytime hypercapnia
- Treated by non-invasive ventilation
Cough failure (expiratory and bulbar)
- Weak expiratory and bulbar muscles
- Low peak cough flow; cannot clear secretions
- Mucus plugging, atelectasis, recurrent pneumonia
- Treated by assisted cough and mechanical insufflation-exsufflation
Bulbar failure (swallow)
- Unsafe swallow with weak or wet voice
- Drooling, choking on feeds, silent aspiration
- Can limit a face-mask cough assist
- Treated by feeding support and secretion control
Epidemiology & Risk Factors
Respiratory failure is the leading cause of death across the paediatric neuromuscular disorders, so its epidemiology is really the epidemiology of the diseases that cause it. Duchenne muscular dystrophy affects roughly one in five thousand boys and follows a predictable course, with respiratory decline beginning after ambulation is lost and vital capacity falling through the second decade. Spinal muscular atrophy affects about one in ten thousand births and, in its severe infantile form, threatens the breathing from the first months of life. [2] [5]
The risk of respiratory failure within any of these diseases is driven by the severity and the tempo of the weakness and by a few powerful modifiers. Progressive scoliosis and a stiff chest wall worsen the restrictive defect; recurrent aspiration from bulbar weakness accelerates lung injury; and each chest infection can cause a step down from which the child does not fully recover. Obesity, poor nutrition and missed immunisations add avoidable risk on top of the disease itself. [1] [3]
The other neuromuscular disorders each carry a characteristic respiratory risk. Guillain-Barre syndrome can cause rapidly progressive weakness that reaches the diaphragm and demands intensive-care monitoring and sometimes ventilation. Congenital myopathies and myotonic dystrophy can cause respiratory failure disproportionate to the limb weakness, and myotonic dystrophy adds central and bulbar contributions. Recognising which disease carries which respiratory risk lets the team monitor the right thing at the right time. [1] [4]
Pathophysiology
To understand why breathing fails, follow the two jobs of the respiratory muscles. The inspiratory muscles, above all the diaphragm, generate the tidal breath and keep the lungs expanded. When they are weak, the vital capacity falls, small areas of lung collapse, and the child breathes rapidly and shallowly. Because muscle tone and accessory-muscle help are lost in sleep, and especially in rapid eye movement sleep, hypoventilation appears there first, so carbon dioxide climbs at night long before it rises by day. [1] [7]
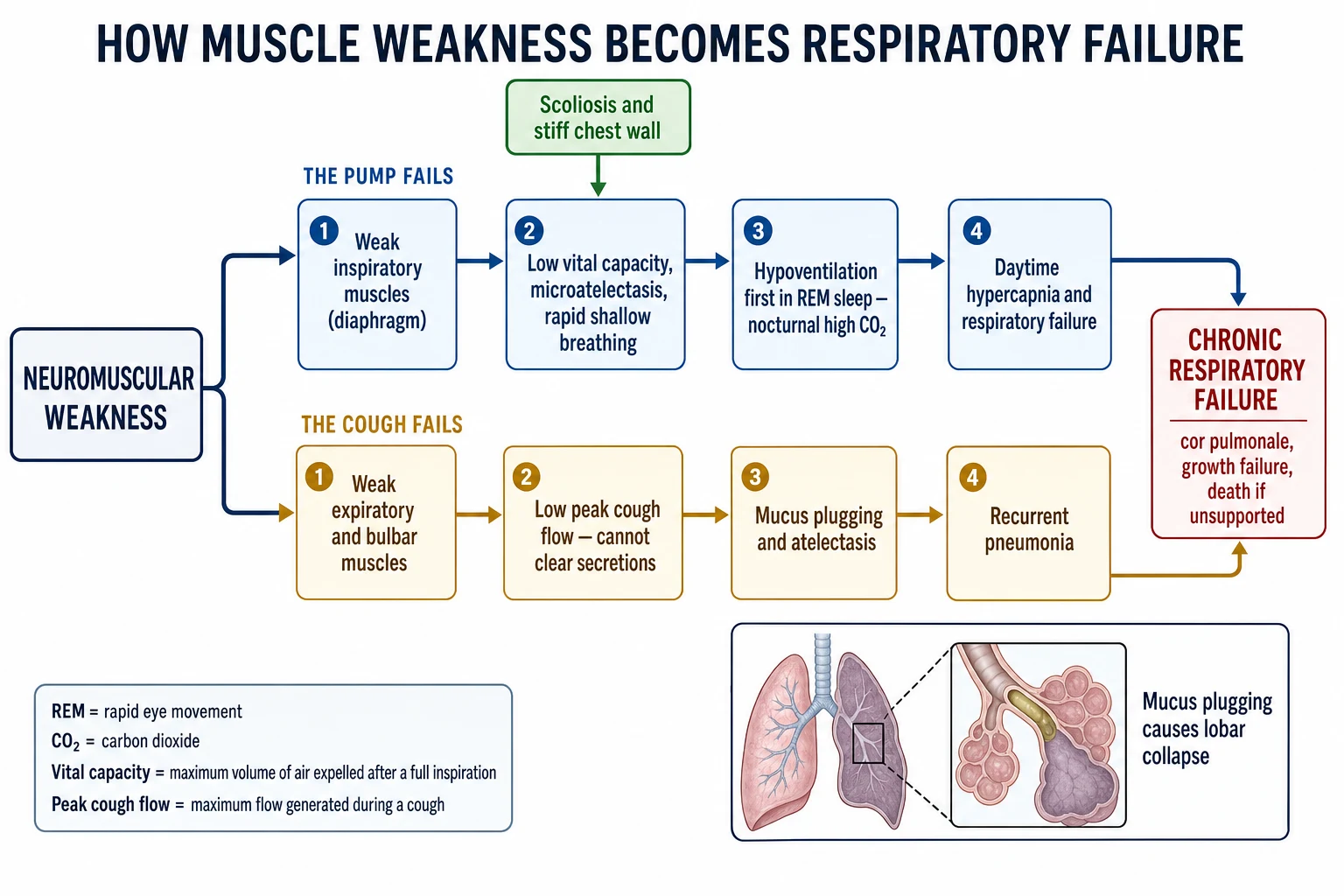
The cough is a second, separate mechanism, and it fails by its own route. An effective cough needs a deep breath in, a tight glottic closure, and a forceful expiratory blast. Weak inspiratory muscles reduce the breath in, bulbar weakness weakens the glottic seal, and weak abdominal and expiratory muscles reduce the blast, so the peak cough flow falls. Below a threshold the cough can no longer shift secretions, they pool in the airways, and mucus plugging causes atelectasis and pneumonia. This is why a child can ventilate adequately yet still drown in their own secretions during a cold. [6] [1]
Two further factors amplify both failures. A progressive scoliosis and a stiff, poorly grown chest wall add a restrictive load that the weak muscles cannot overcome, reducing lung volumes further. Bulbar weakness allows saliva and feeds to be aspirated, seeding infection and inflammation directly into the lungs. The end result of untreated pump failure and cough failure is the same: chronic hypoxaemia and hypercapnia, pulmonary hypertension and cor pulmonale, and death from respiratory failure if the child is not supported. [2] [3]
Clinical Presentation
The presentation is often quiet and easily missed, because the earliest failure is nocturnal. Ask specifically for the symptoms of sleep hypoventilation: morning headache that eases through the day, unrefreshing sleep and daytime sleepiness, poor concentration and falling school performance, and poor appetite or weight gain. Frequent night waking, restless sleep and, in younger children, faltering growth are common. These symptoms in a child with known muscle weakness point to nocturnal hypoventilation until a sleep study says otherwise. [1] [7]
The cough failure declares itself through the chest. A child with a weak cough has recurrent and prolonged chest infections, takes far longer to clear a simple cold, and develops lobar or segmental collapse on the chest radiograph. Parents describe a cough that sounds weak and ineffective and an inability to bring up secretions, and the child may need repeated courses of antibiotics or admissions each winter. Each infection can leave the child a step worse than before. [6] [1]
Bulbar involvement adds its own signs. Listen for a weak, wet or nasal voice, watch for drooling and pooling of secretions, and ask about coughing or choking on feeds and prolonged mealtimes. A child with an unsafe swallow aspirates saliva and food, which both causes lung injury and can make a face-mask cough assist harder to deliver because the upper airway collapses. Recognising bulbar weakness reshapes both the feeding plan and the airway-clearance plan. [4] [6]
Differential Diagnosis
When a child with muscle weakness presents with respiratory symptoms, the first task is to decide which of the three failures is driving the picture, because each is managed differently. Nocturnal hypoventilation is suggested by morning headache and daytime sleepiness and confirmed by a raised carbon dioxide in sleep; cough failure is suggested by recurrent chest infections and collapse and confirmed by a low peak cough flow; and aspiration is suggested by choking on feeds and confirmed by a swallow assessment. Often more than one is present at once. [1] [6]
Nocturnal hypoventilation
- Morning headache, daytime sleepiness, poor growth
- Carbon dioxide rises in sleep, worst in REM
- Confirmed on overnight oximetry and capnography
- Answer is non-invasive ventilation
Cough failure
- Recurrent, prolonged chest infections and collapse
- Weak, ineffective cough; secretions not cleared
- Confirmed by a low peak cough flow
- Answer is assisted cough and cough assist
Other explanations
- Asthma or intercurrent viral wheeze
- Cardiomyopathy in Duchenne muscular dystrophy
- Aspiration lung disease from an unsafe swallow
- Obstructive sleep apnoea coexisting with weakness
It is also important to exclude explanations that are not simply the neuromuscular disease. A child with Duchenne muscular dystrophy can develop a cardiomyopathy that causes breathlessness and fatigue and needs its own treatment, so cardiac and respiratory causes must be separated. Coexisting asthma, obstructive sleep apnoea from a large tongue or tonsils, and intercurrent viral illness can all add to the picture. The discipline is to attribute symptoms to a mechanism, confirmed by measurement, rather than to the diagnosis in general. [2] [1]
Clinical & Bedside Assessment
The bedside assessment starts with watching the child breathe and cough, awake and, if possible, asleep. Count the respiratory rate, look for shallow breathing, paradoxical abdominal movement and accessory-muscle use, and ask the child to take a deep breath and cough so you can judge the strength of the cough directly. Observe a period of sleep or a nap where you can, watching for shallow breathing and desaturation and noting that the child may look comfortable even as ventilation fails. [1] [7]
Examine for the consequences and the amplifiers. Look for the signs of cor pulmonale such as a loud pulmonary second sound and hepatomegaly, assess the spine for scoliosis and the chest for deformity and reduced expansion, and listen for the crackles and reduced air entry of retained secretions or collapse. Assess bulbar function through the voice, the handling of saliva and a feeding observation, because an unsafe swallow changes the plan. Chart the weight and growth, which fall when hypoventilation and effort of breathing go untreated. [2] [6]
The bedside numbers to gather are simple and repeatable. A hand-held spirometer gives the vital capacity sitting and lying, where a large fall on lying flat points to diaphragm weakness; a peak flow meter gives the peak cough flow; and overnight oximetry with carbon dioxide, arranged from clinic, extends the bedside into sleep. Tracking these over time turns a single snapshot into the trajectory that drives decisions about when to start ventilation and airway clearance. [1] [12]
Investigations
The investigations answer two questions in turn: is the pump failing, and is the cough failing. For the pump, lung function with the forced vital capacity, measured sitting and supine, is the anchor, because a low or falling vital capacity and a large supine drop mark inspiratory and diaphragm weakness. Respiratory muscle strength can be quantified with maximal inspiratory and expiratory pressures or a sniff nasal pressure, and these decline before symptoms appear. Sleep is then studied to catch hypoventilation early. [1] [7]
Sleep study is the investigation that reveals hypoventilation, because oxygen desaturation is a late sign and the earlier change is a rising carbon dioxide. Overnight oximetry combined with transcutaneous or end-tidal carbon dioxide, and where available full polysomnography, characterises the nocturnal breathing and can be performed at home with transcutaneous carbon dioxide monitoring in children with neuromuscular disorders. Carbon dioxide monitoring is equally central to running long-term non-invasive ventilation well, guiding the settings so that ventilation, not merely oxygenation, is corrected. [12] [10]
What to monitor in neuromuscular breathing — the mnemonic PUMP
The rest of the work-up looks for consequences and amplifiers. An echocardiogram and electrocardiogram screen for cor pulmonale and, in Duchenne muscular dystrophy, for the cardiomyopathy that runs alongside the respiratory disease. A chest radiograph shows collapse and consolidation during infections and the spinal curve; a spinal assessment quantifies scoliosis; and a swallow assessment, clinical or with videofluoroscopy, defines aspiration risk. Together these define the whole respiratory burden rather than a single number. [2] [4]
Management — Resuscitation
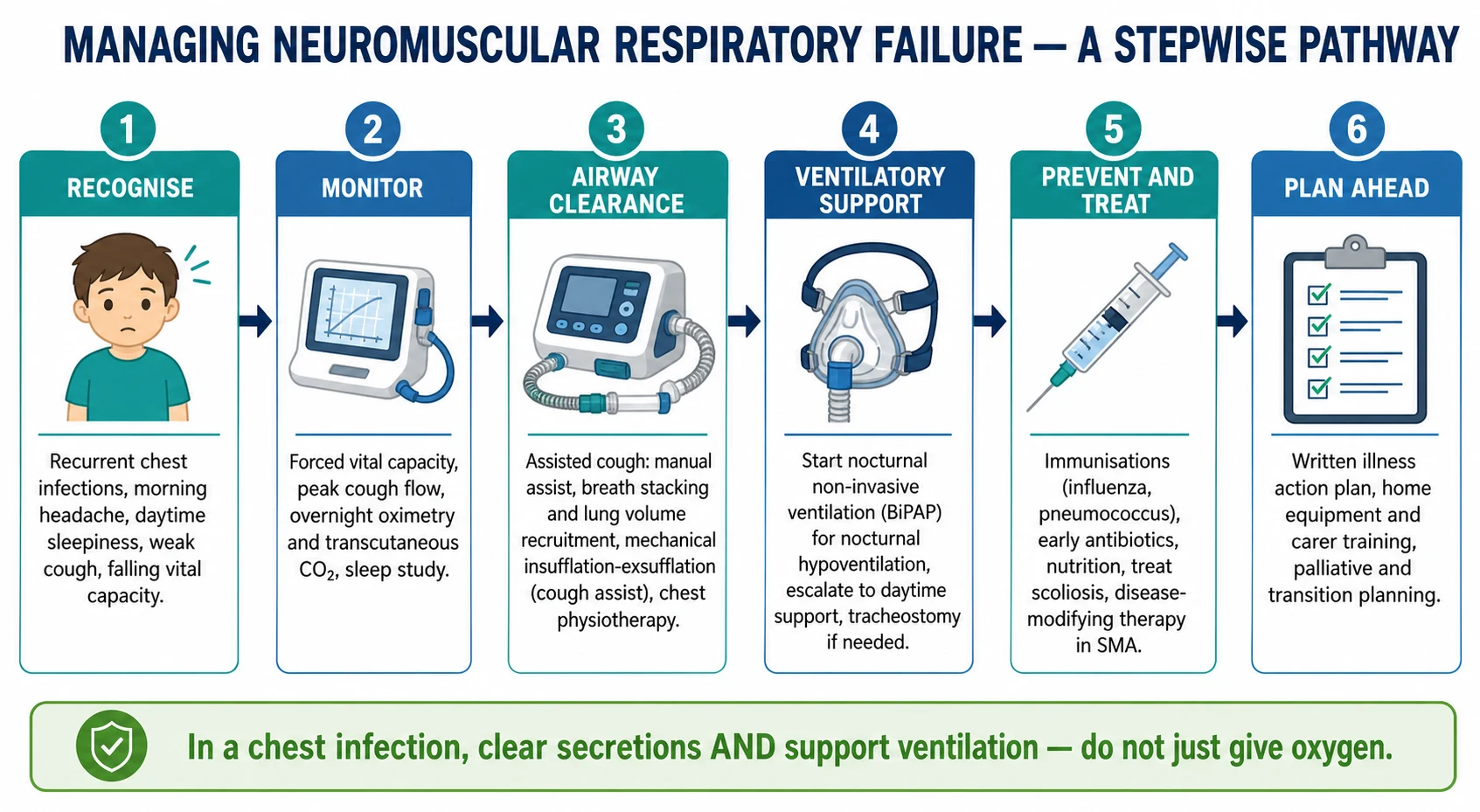
The acute crisis in a neuromuscular child is usually a chest infection, and its management follows one governing rule: clear the secretions and support ventilation, do not merely give oxygen. Retained secretions and worsening hypoventilation are the twin problems, so intensify airway clearance with assisted cough and mechanical insufflation-exsufflation, support breathing with non-invasive ventilation, and treat the infection with prompt antibiotics. Oxygen is added only on top of adequate ventilation and clearance, never as a substitute. [1] [3]
Escalation is planned, not improvised, and is guided by the child's own respiratory plan wherever one exists. A child who cannot maintain ventilation despite non-invasive support and aggressive clearance may need intubation and mechanical ventilation, but the goal from the outset is to extubate back onto non-invasive ventilation and cough assist rather than to a bare face mask, because the underlying weakness has not changed. Avoid sedatives and unnecessary respiratory depressants, involve intensive care early, and make resuscitation decisions in the light of any agreed advance care plan. [4] [2]
Guillain-Barre syndrome is the neuromuscular emergency that most often presents to general paediatrics without a prior diagnosis, and it needs a different vigilance. Because the weakness can ascend rapidly to involve the diaphragm, monitor the vital capacity serially, watch for a weakening cough and bulbar signs, and move the child to a monitored or intensive-care setting before respiratory failure arrives rather than after. Anticipating the fall is the whole of good care here. [1] [7]
Management — Definitive & Stepwise
Definitive management runs on two tracks in parallel, ventilation for the pump and airway clearance for the cough, each escalated as the disease progresses. The figure sets out the whole pathway from recognition and monitoring, through airway clearance and ventilatory support, to prevention and forward planning. The art is to start each intervention proactively, guided by the monitoring numbers, so that support is already in place when a crisis comes. [1] [6]
Airway clearance is laddered to the severity of the cough failure. Manual assisted cough, where a carer times an abdominal thrust to the child's cough, and breath stacking or lung volume recruitment, using a bag or a mouthpiece to stack breaths into a bigger inspiration, augment a moderately weak cough. When these are insufficient, mechanical insufflation-exsufflation, the cough assist device, delivers a positive pressure to inflate the lungs then a rapid negative pressure to simulate the expiratory blast, and it is the mainstay for a severely weak cough. Long-term mechanical assisted cough is valued by families and reduces the burden of secretion-related illness. [6] [8]
Ventilatory support is laddered to the severity of the pump failure. Nocturnal non-invasive ventilation through a mask is started for nocturnal hypoventilation and is the treatment that reverses the morning headaches and daytime sleepiness and rests the respiratory muscles. As the disease progresses, support is extended into the day, and only a minority go on to need a tracheostomy and continuous ventilation. Settings are guided by carbon dioxide, and the aim throughout is adequate ventilation across every sleep period, with the interface and mode chosen to fit the child. [7] [10]
Around the two ladders sits prevention and organised care. Keep immunisations current, treat chest infections early and vigorously, support nutrition and growth, and manage scoliosis, which itself worsens the restrictive defect. In spinal muscular atrophy, disease-modifying therapy has changed the trajectory, and the respiratory management of children treated with nusinersen and related agents remains a core part of care rather than being replaced by it. A written home programme with trained carers, reliable equipment and an emergency plan holds the whole plan together. [5] [9]
Specific Subtypes & Scenarios
Duchenne muscular dystrophy is the archetype of predictable, progressive respiratory decline. While the boy is walking the lungs are usually well; after ambulation is lost the forced vital capacity falls, nocturnal hypoventilation appears and the cough weakens, so anticipatory monitoring, timely non-invasive ventilation and cough assist, and attention to the accompanying cardiomyopathy are the pillars of care. Proactive respiratory management, set out in the ATS statement and the care considerations, has substantially lengthened survival. [3] [2]
Spinal muscular atrophy spans a wide severity range and shows the two failures early. In the severe infantile form the weak cough and hypoventilation threaten life in the first months, and the classic bell-shaped chest and paradoxical breathing reflect the intercostal-predominant weakness with a relatively spared diaphragm. Standard-of-care respiratory management centres on airway clearance and non-invasive ventilation, proactive planning for infections, and clear, values-based decisions about the intensity of support, now made in the changed context of disease-modifying therapy. [4] [9]
The other scenarios each have their own emphasis. Guillain-Barre syndrome demands serial vital-capacity monitoring for rapidly ascending weakness that may reach the diaphragm; congenital myopathies and myotonic dystrophy can cause respiratory failure out of proportion to limb weakness and need early respiratory surveillance; and myasthenic crises cause fluctuating, treatable weakness that can involve the respiratory and bulbar muscles. Recognising the disease-specific respiratory risk directs the monitoring and the timing of support. [1] [7]
Complications & Pitfalls
The complications of untreated neuromuscular respiratory failure follow directly from the two failures. Cough failure brings recurrent pneumonia, lobar collapse and progressive lung injury; pump failure brings chronic nocturnal then daytime hypercapnia, pulmonary hypertension and cor pulmonale, faltering growth and, ultimately, death from respiratory failure. Aspiration from bulbar weakness adds a further stream of lung injury and infection. Each severe chest infection can leave a lasting step down in function. [1] [2]
The great management pitfall is to treat the child as if the lungs were the problem. Giving oxygen without clearing secretions and supporting ventilation corrects the number on the monitor while the real problems worsen, and it is the classic error in the emergency department. A second pitfall is failing to measure the cough, so that a child with a dangerously low peak cough flow reaches the next infection without airway clearance in place. A third is missing nocturnal hypoventilation because the child looks well by day. [1] [6]
Peri-procedural care is a recurring trap. These children are sensitive to sedatives and anaesthetic agents, and elective surgery, including scoliosis correction, must be preceded by respiratory optimisation and planned recovery onto non-invasive ventilation and cough assist rather than extubation to a bare face mask. Under-recognising the cardiomyopathy in Duchenne muscular dystrophy, and attributing all breathlessness to the lungs, is another avoidable error. Anticipation and a written plan prevent most of these pitfalls. [2] [3]
Prognosis & Disposition
The prognosis has been transformed by proactive respiratory care. In Duchenne muscular dystrophy the systematic use of nocturnal then daytime non-invasive ventilation and of assisted cough has added years of life and shifted the cause and timing of death, so that boys now commonly reach adulthood. The trajectory is still one of progressive weakness, but its respiratory consequences are now largely manageable when monitoring is regular and support is timely. Cardiac disease increasingly shares the prognostic stage with respiratory disease. [2] [3]
In spinal muscular atrophy the outlook depends on the severity and, increasingly, on disease-modifying therapy, but respiratory care remains central whatever the treatment. Airway clearance and non-invasive ventilation, combined with clear and compassionate decisions about the intensity of support, define the day-to-day prognosis, and the respiratory phenotype of treated children continues to require active management. Across all the disorders, the quality of the home respiratory programme is a powerful determinant of both survival and quality of life. [4] [9]
The disposition is a structured, anticipatory home programme. The child needs regular respiratory and sleep review, monitoring of vital capacity, peak cough flow and nocturnal carbon dioxide, reliable home equipment for ventilation and cough assist with trained carers, and a written illness action plan that tells any clinician to clear secretions and ventilate rather than simply oxygenate. Planned transition to adult respiratory services, and honest advance care planning where appropriate, complete the picture. [1] [8]
Special Populations
The infant with severe spinal muscular atrophy is the highest-stakes population, because the weak cough and hypoventilation threaten life from the first months and every decision is made against a backdrop of profound weakness and, now, disease-modifying therapy. Care combines meticulous airway clearance and non-invasive support with early, honest and values-based conversations with the family about the goals and intensity of respiratory treatment, ideally before a crisis forces the issue. [4] [9]
The child facing surgery, and the adolescent transitioning to adult care, each need particular attention. Perioperative care demands respiratory optimisation beforehand, careful use of sedatives and anaesthesia, and planned recovery onto non-invasive ventilation and cough assist, whether the operation is scoliosis correction or an unrelated procedure. The transition years, when a young person moves to adult services, are a vulnerable time when established respiratory routines and equipment must be handed over without interruption. [2] [1]
Equity of access shapes outcomes as much as biology. Home non-invasive ventilation, cough assist devices, sleep studies and specialist review are concentrated in tertiary centres, and children in rural, remote and Indigenous communities can face real barriers to the technology and follow-up that keep them well. Telehealth, outreach and deliberate service planning are needed to give these children the same anticipatory respiratory care that transforms the prognosis elsewhere. [1] [8]
Evidence, Guidelines & Regional Differences
The evidence base is anchored by disease-specific consensus guidelines. The American Thoracic Society statement on respiratory care in Duchenne muscular dystrophy and the Duchenne care considerations set out the anticipatory monitoring, the thresholds for non-invasive ventilation and the airway-clearance approach, while the spinal muscular atrophy standard-of-care statements do the same for that disease. The British Thoracic Society guideline provides the broad framework for respiratory management across children with neuromuscular weakness. [3] [2] [1]
The evidence for individual techniques is a mix of physiological study, cohort experience and expert consensus rather than large randomised trials, which is characteristic of a field of rare, heterogeneous diseases. State-of-the-art reviews synthesise the airway-clearance techniques and their indications, cohort and user-reported studies support long-term mechanical assisted cough, and carbon dioxide monitoring is established as central to both diagnosis and the running of non-invasive ventilation. Disease-modifying therapy has added a new and evolving dimension to the respiratory literature in spinal muscular atrophy. [6] [8] [9]
Regional differences are practical rather than definitional. The principles of monitoring the pump and the cough and of supporting both are consistent across jurisdictions, but access to home non-invasive ventilation, cough assist devices, paediatric sleep studies and disease-modifying therapy varies widely between and within countries. In Australia and New Zealand, care is concentrated in tertiary paediatric respiratory and neuromuscular services, and equitable access for rural, remote and Indigenous families is an explicit service priority. [1] [12]
Exam Pearls
Hold one framework for the viva: neuromuscular disease attacks breathing in two separate ways, and you treat them separately. Weak inspiratory muscles cause nocturnal then daytime hypoventilation, treated by non-invasive ventilation; weak expiratory and bulbar muscles cause an ineffective cough and secretion retention, treated by assisted cough and mechanical insufflation-exsufflation. In a chest infection the rule is to clear secretions and ventilate, not merely to oxygenate. [1] [6]
State the frequently tested numbers and facts correctly. Hypoventilation appears first in rapid eye movement sleep and is detected by measuring carbon dioxide, not oxygen. A peak cough flow falling towards 270 litres per minute is a warning and below 160 litres per minute is an ineffective cough in older children and adolescents. A large fall in vital capacity from sitting to supine indicates diaphragm weakness. Cough assist works by an insufflation then a rapid exsufflation to mimic a cough. [6] [1]
The high-yield pairings do the diagnostic work. A boy with Duchenne muscular dystrophy, morning headaches and daytime sleepiness has nocturnal hypoventilation needing non-invasive ventilation; the same boy with recurrent pneumonias and a weak cough needs cough assist; an infant with spinal muscular atrophy, a bell-shaped chest and paradoxical breathing has intercostal weakness with a spared diaphragm; and a child with ascending weakness and a falling vital capacity has Guillain-Barre syndrome approaching the diaphragm. Always clear secretions and ventilate before you reach for oxygen alone. [2] [4] [1]
References
- [1]Hull J; Aniapravan R; Chan E; et al British Thoracic Society guideline for respiratory management of children with neuromuscular weakness. Thorax, 2012.PMID 22730428
- [2]Birnkrant DJ; Bushby K; Bann CM; et al Diagnosis and management of Duchenne muscular dystrophy, part 2: respiratory, cardiac, bone health, and orthopaedic management. Lancet Neurol, 2018.PMID 29395990
- [3]Finder JD; Birnkrant D; Carl J; et al Respiratory care of the patient with Duchenne muscular dystrophy: ATS consensus statement. Am J Respir Crit Care Med, 2004.PMID 15302625
- [4]Finkel RS; Mercuri E; Meyer OH; et al Diagnosis and management of spinal muscular atrophy: Part 2: Pulmonary and acute care; medications, supplements and immunizations; other organ systems; and ethics. Neuromuscul Disord, 2018.PMID 29305137
- [5]Mercuri E; Finkel RS; Muntoni F; et al Diagnosis and management of spinal muscular atrophy: Part 1: Recommendations for diagnosis, rehabilitation, orthopedic and nutritional care. Neuromuscul Disord, 2018.PMID 29290580
- [6]Chatwin M; Toussaint M; Gonçalves MR; et al Airway clearance techniques in neuromuscular disorders: A state of the art review. Respir Med, 2018.PMID 29501255
- [7]Fauroux B; Khirani S; Griffon L; et al Non-invasive Ventilation in Children With Neuromuscular Disease. Front Pediatr, 2020.PMID 33330262
- [8]Hov B; Andersen T; Toussaint M; et al User-perceived impact of long-term mechanical assisted cough in paediatric neurodisability. Dev Med Child Neurol, 2023.PMID 36787316
- [9]Menard J; Seferian AM; Fleurence E; et al Respiratory management of spinal muscular atrophy type 1 patients treated with Nusinersen. Pediatr Pulmonol, 2022.PMID 35307979
- [10]Paiva R; Krivec U; Aubertin G; et al Carbon dioxide monitoring during long-term noninvasive respiratory support in children. Intensive Care Med, 2009.PMID 19172246
- [11]Caldarelli V; Borel JC; Khirani S; et al Polygraphic respiratory events during sleep with noninvasive ventilation in children: description, prevalence, and clinical consequences. Intensive Care Med, 2013.PMID 23344829
- [12]Withers A; Pettigrew G; Filmer K; et al Comparing home polysomnography with transcutaneous CO(2) monitoring to laboratory polysomnography in children with neuromuscular disorders. J Clin Sleep Med, 2025.PMID 39663926