Paeds · respiratory-sleep-and-airway
Non-invasive ventilation and home respiratory support
Also known as Home ventilation in children · Long-term ventilation (LTV) · Paediatric CPAP and BiPAP · Domiciliary non-invasive ventilation · High-flow nasal cannula therapy
Fellowship guide to non-invasive ventilation and home respiratory support in children: what CPAP, bilevel non-invasive ventilation and high-flow nasal cannula actually do, how to tell an obstructive problem that needs CPAP from a hypoventilation problem that needs bilevel and a central problem that needs ventilation with a back-up rate, the interfaces and their complications, the assessment and sleep-study titration that guide therapy, the acute use of high-flow and CPAP in respiratory failure, the stepwise set-up of long-term home ventilation with secretion clearance and caregiver training, and the neuromuscular, central and technology-dependent populations that define the field.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Non-invasive ventilation is respiratory support delivered through a mask or nasal interface, using positive pressure or heated high flow, without an invasive artificial airway such as an endotracheal tube or tracheostomy. The umbrella of home respiratory support then covers everything a child may go home on: supplemental oxygen, continuous positive airway pressure, bilevel non-invasive ventilation, and — for the most dependent children — invasive ventilation through a tracheostomy. The organising idea for an exam is that the interface and the machine are chosen to fix a specific respiratory problem, and naming that problem first is what separates a competent answer from a list of gadgets. [2] [1]
The topic matters because the number of children living at home on ventilatory support has grown steadily, driven by better survival in neuromuscular disease, prematurity and complex conditions, and by the recognition that untreated nocturnal hypoventilation is harmful and treatable. Two distinctions carry most of the marks. The first is between continuous positive airway pressure, which applies one steady pressure to splint the airway open and recruit the lung, and bilevel ventilation, which adds a higher inspiratory pressure to actually augment each breath. The second is between an acute, in-hospital course of support and a long-term home programme with all its training and safety planning. [2] [3]
Classification
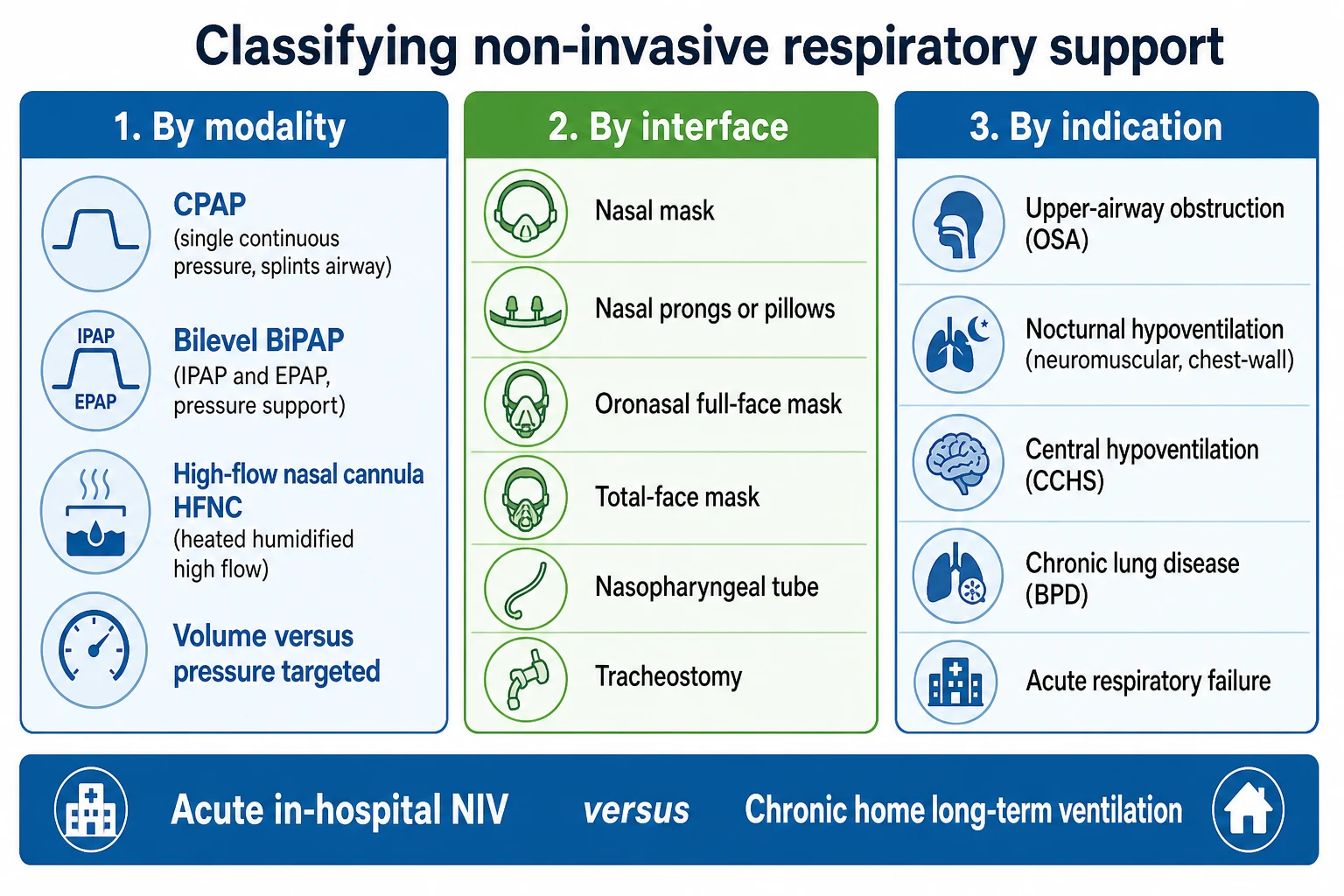
The most useful way to hold this field together is to answer three questions at the bedside: what is the machine doing, how is it connected to the child, and what problem is it treating. By modality, continuous positive airway pressure delivers one constant distending pressure; bilevel ventilation adds inspiratory pressure support with or without a set back-up rate; and high-flow nasal cannula delivers heated, humidified gas at flows above the child's inspiratory demand, giving washout of dead space and a little distending pressure. Devices are further described as pressure-targeted or volume-targeted, and modern hybrid modes aim at an average tidal volume while varying pressure. [2] [3]
By connection, the interface runs from nasal masks and nasal prongs or pillows through oronasal (full-face) and total-face masks to nasopharyngeal tubes, with tracheostomy reserved for invasive support. Interface choice is not a detail: leak, comfort, skin tolerance and the risk of long-term facial growth effects all follow from it. By problem, the indications sort into upper-airway obstruction that needs splinting, nocturnal or chronic hypoventilation that needs the breath augmented, central hypoventilation that needs a machine to remember to breathe, and parenchymal or chronic lung disease that needs recruitment and oxygen. [2] [4]
Epidemiology & Risk Factors
Home ventilation was once rare and is now an established part of paediatric practice, with prevalence rising across high-income health systems as survival improves and as chronic hypoventilation is recognised earlier. Most children on long-term non-invasive support use it overnight for sleep-related hypoventilation or obstruction, while a smaller, more dependent group needs invasive ventilation through a tracheostomy. The shift toward non-invasive support reflects both better interfaces and a preference for the least invasive option that controls the child's gas exchange. [2] [1]
The children who need this support cluster into recognisable groups. Neuromuscular disease — spinal muscular atrophy, Duchenne muscular dystrophy and congenital myopathies — is the largest, because progressive weakness first causes nocturnal hypoventilation and later daytime respiratory failure. Chest-wall and skeletal disorders such as severe scoliosis, central hypoventilation syndromes such as congenital central hypoventilation syndrome, craniofacial anomalies with severe upper-airway obstruction, and chronic lung disease of prematurity make up much of the rest. [2] [4]
Pathophysiology
Respiratory support is chosen against the type of failure it must correct. Type 1 (hypoxaemic) failure is a problem of oxygenation from collapsed or diseased lung, and it responds to recruitment and oxygen; type 2 (hypercapnic) failure is a problem of ventilation, where the child cannot move enough air to clear carbon dioxide, and it needs the breath augmented. Many children combine both, and the examiner wants a candidate who reaches for CPAP or high flow when the issue is oxygenation and recruitment but for bilevel when the issue is a rising carbon dioxide. [2]
Continuous positive airway pressure works by raising the pressure inside the airway throughout the respiratory cycle. That constant distending pressure holds open a pharynx that would otherwise collapse — the mechanism that treats obstruction — and it splints open small airways and alveoli, raising functional residual capacity and improving oxygenation in atelectatic or chronically diseased lung. In adherent children it reliably abolishes obstructive events, which is why it is the mainstay for obstructive sleep apnoea that surgery has not fixed. [2] [9]
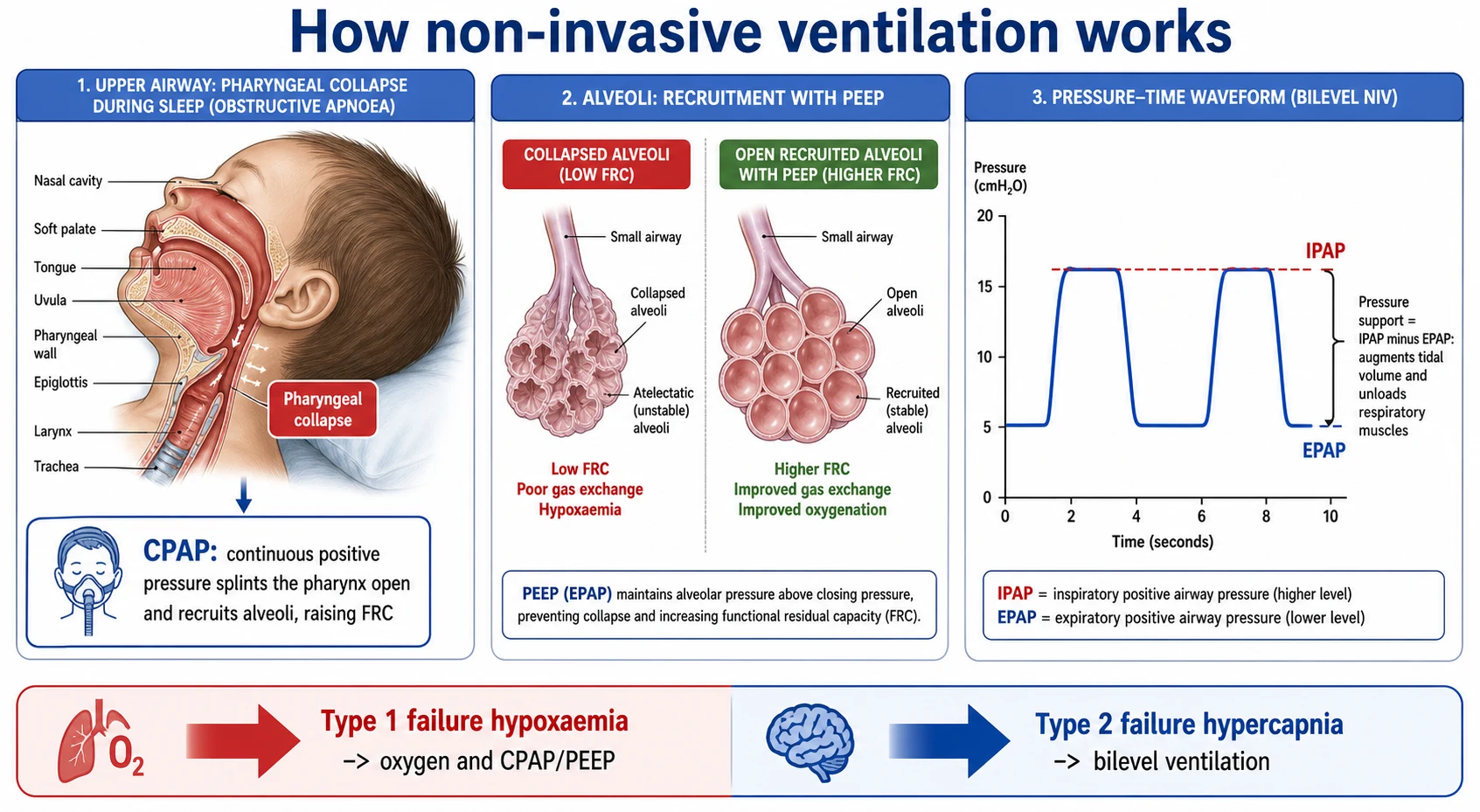
Bilevel ventilation adds a higher inspiratory pressure to the expiratory baseline, and the gap between the two is the pressure support that drives each breath in, increasing tidal volume and unloading fatiguing respiratory muscles. A set back-up rate makes the machine deliver breaths when the child's own drive is weak or absent, which is essential in central hypoventilation. The reason support is so often overnight is that ventilation is most vulnerable in sleep: muscle tone and drive fall, and in rapid-eye-movement sleep the accessory muscles switch off, so hypoventilation appears first in sleep and only later spills into the day. [6] [5]
Clinical Presentation
Chronic nocturnal hypoventilation announces itself quietly, and the history has to go looking for it. The classic clues are morning headaches from overnight carbon dioxide retention, unrefreshing sleep with frequent waking, daytime sleepiness or fatigue, poor concentration and declining school performance, orthopnoea in the child with a weak diaphragm, faltering growth, and recurrent or slow-to-clear chest infections. In neuromuscular disease a falling exercise tolerance and a weakening cough often precede any change in the daytime blood gas. [6] [3]
The acute presentation is different and usually louder. An infant with bronchiolitis or a child with an asthma exacerbation or pneumonia arrives with visible respiratory distress, hypoxaemia and rising work of breathing, and it is here that high-flow nasal cannula and CPAP are used to support the child and try to avoid intubation. The examiner expects a candidate to recognise both faces of the topic: the slow, easily-missed drift into chronic hypoventilation, and the acute failure where non-invasive support is a time-critical intervention. [10] [11]
Differential Diagnosis
The first and most important fork is deciding which of three mechanisms is driving the failure, because it selects the machine. Upper-airway obstruction, where effort continues against a closed airway, is treated by splinting with CPAP; hypoventilation from weak or restricted breathing, where the child cannot move enough air, needs the breath augmented with bilevel; and central hypoventilation, where drive itself fails, needs bilevel with a reliable back-up rate. Getting this wrong — reaching for CPAP in a hypoventilating child — leaves the carbon dioxide uncontrolled. [2] [4]
The symptom set of chronic hypoventilation overlaps with other conditions, and these must be separated. Daytime sleepiness and poor school performance can be primary sleep deprivation, depression, obstructive sleep apnoea or the effect of medications; recurrent chest infections can be aspiration, bronchiectasis, immunodeficiency or cystic fibrosis; and faltering growth has a broad differential of its own. The discriminator is to look specifically for the physiology — nocturnal carbon dioxide retention and a weak cough — rather than treating the symptoms in isolation. [3]
Clinical & Bedside Assessment
Bedside assessment has two jobs: judge how well the child is breathing and judge how well the interface and support are working. The respiratory examination looks for signs of increased work and fatigue, chest-wall shape and scoliosis, diaphragm strength (orthopnoea and paradoxical abdominal movement lying flat), and the child's conscious state and ability to protect the airway. In the child already on support, the interface is inspected for fit and leak, the skin over the nasal bridge and cheeks for pressure injury, and the midface for the flattening that long-term mask use can cause. [2] [3]
Cough strength is a specific and high-yield bedside judgement in neuromuscular disease, because a child who cannot clear secretions will fail during a chest infection. Cough is assessed clinically and, in older children, by cough peak flow, with the British Thoracic Society thresholds widely quoted: a stable value below about 270 litres per minute warns that cough will become ineffective when the child is unwell, and a value below about 160 litres per minute means cough is inadequate to clear secretions. These numbers tell you when to introduce airway-clearance techniques and a cough-assist device. [3] [7]
Investigations
The reference investigation is attended polysomnography with carbon dioxide monitoring, ideally used to titrate the settings while the child sleeps, because it shows both obstruction and hypoventilation and lets the team set the right pressures and back-up rate. Where full polysomnography is scarce, overnight oximetry combined with transcutaneous or end-tidal carbon dioxide is the pragmatic core, and the crucial teaching point is that oximetry alone can miss hypoventilation — the saturation may hold while carbon dioxide rises, so carbon dioxide must be measured directly. [2] [6]
Around the sleep study sit the tests that stage the underlying disease and time intervention. A blood gas (capillary or arterial) documents daytime carbon dioxide; spirometry tracks a falling forced vital capacity, with a persistent fall a recognised trigger to assess for nocturnal support; and measures of respiratory muscle strength and cough — sniff nasal inspiratory pressure and cough peak flow — identify the child heading toward failure. These are trended over time rather than read once, so that support is started before a crisis. [3] [6]
Management — Resuscitation
In the acutely deteriorating child, non-invasive support is used to correct hypoxaemia, reduce the work of breathing, and buy time. In bronchiolitis, high-flow nasal cannula has the strongest paediatric evidence: the large PARIS trial showed that early high-flow oxygen reduced escalation of care compared with standard oxygen in infants, and the HFWHO trial similarly found fewer treatment failures with high flow in moderate disease, though neither shortened the illness. CPAP is the next step for the infant who continues to obstruct or tire, and persisting failure despite non-invasive support is the signal to intubate rather than to persevere. [10] [11]
The acute-on-chronic scenario in a neuromuscular child is managed differently, because the enemy is often secretions rather than the primary infection. Bilevel ventilation supports the tiring child, but it must be paired with aggressive airway clearance, including mechanical insufflation-exsufflation, to move the secretions a weak cough cannot. Non-invasive ventilation is unsafe, and intubation is the correct choice, when the child cannot protect the airway, has a depressed conscious state, copious uncleared secretions, facial trauma or is vomiting. Recognising these contraindications is as important as knowing when to start a mask. [3] [7]
Escalation in acute respiratory failure
Optimise position, secretions and oxygen; measure carbon dioxide if hypoventilation is possible
High-flow nasal cannula for hypoxaemic distress, especially in bronchiolitis
CPAP for continuing obstruction or atelectasis; bilevel if carbon dioxide is rising
In neuromuscular children pair support with airway clearance and cough assist
Reassess frequently; failure to improve is a signal to intubate, not to wait
Intubate now if the child cannot protect the airway, is obtunded, or has copious secretions or vomiting
Management — Definitive & Stepwise
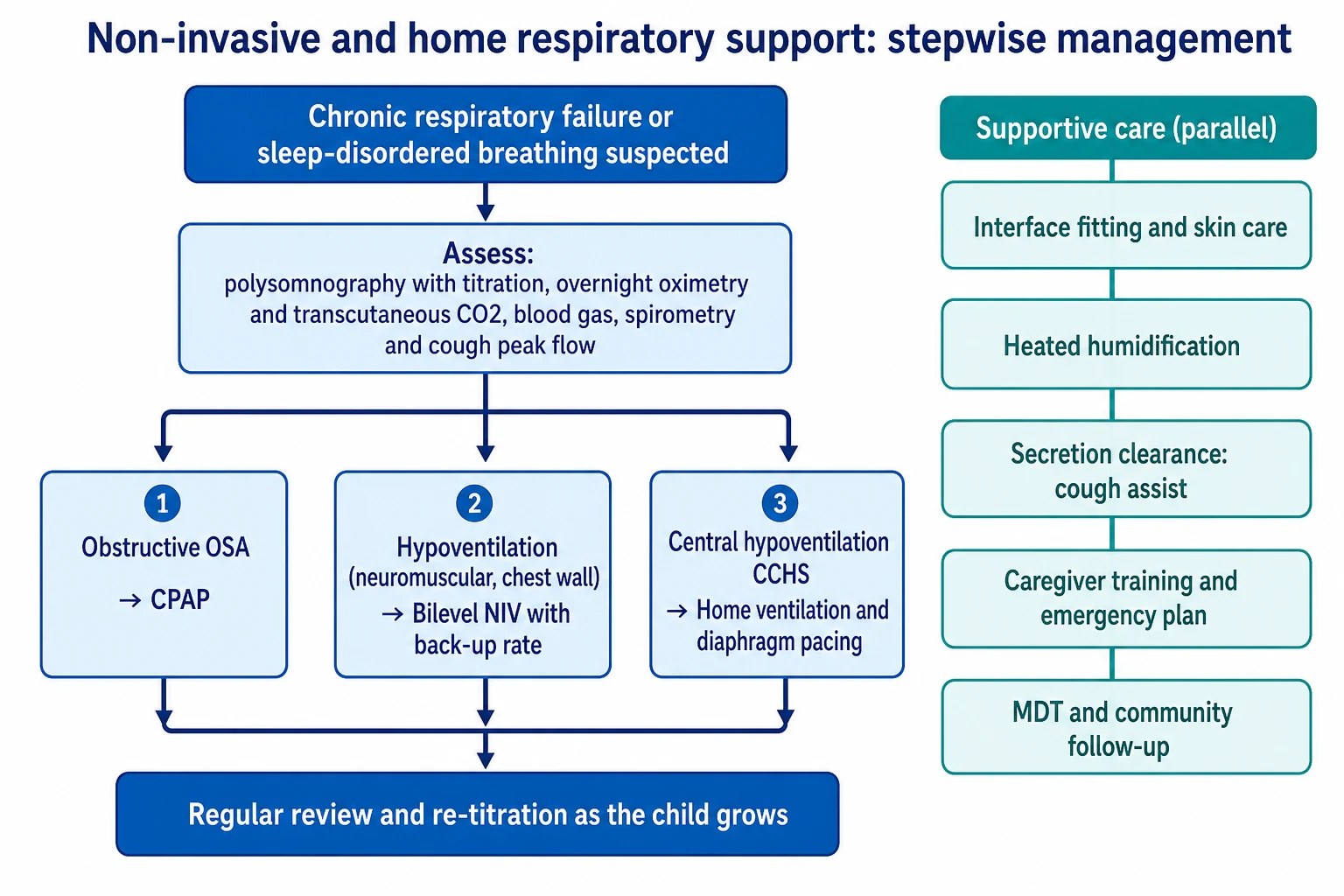
Setting up long-term support is a planned, staged process rather than a single prescription. The team selects the modality from the physiology (CPAP for obstruction, bilevel for hypoventilation, bilevel with a back-up rate for central drive failure), fits an interface that seals with minimal leak and protects the skin and growing face, adds heated humidification for comfort and secretion handling, and titrates the pressures and rate against a sleep study with carbon dioxide monitoring. Interfaces are rotated and re-fitted as the child grows, and settings are reviewed regularly because a child who has outgrown the prescription is effectively undertreated. [2]
Airway clearance is built in from the start for children with a weak cough. Mechanical insufflation-exsufflation (a cough-assist device) delivers a positive then negative pressure swing that mimics a cough, and Chatwin and colleagues showed that it produces a higher cough peak flow than unassisted or other techniques in neuromuscular weakness, which is why it is central to keeping these children out of intensive care. Around this sit assisted-coughing techniques, physiotherapy and a clear sick-day plan for when infections strike. [7] [3]
Success at home depends as much on people and adherence as on pressures. Marcus and colleagues showed that positive airway pressure works in children when it is worn but that real-world adherence falls well short of the prescription, so structured desensitisation, mask choice, and behavioural support are part of the treatment rather than optional extras. A safe discharge requires trained caregivers, back-up equipment and power planning, a written emergency plan, and a multidisciplinary community team, which is the framework the American Thoracic Society guideline sets out for the ventilator-dependent child. [8] [1]
Stepwise set-up of long-term support
Define the physiology: obstruction, hypoventilation or central drive failure
Choose the modality: CPAP, bilevel, or bilevel with a back-up rate
Fit and rotate an interface that seals, protects skin and spares the growing face
Add heated humidification and titrate settings against a sleep study with carbon dioxide
Build in airway clearance and cough assist for the weak-cough child
Support adherence with desensitisation, mask choice and behavioural strategies
Train caregivers, plan back-up power and equipment, and write an emergency plan
Review regularly and re-titrate as the child grows and the disease evolves
Specific Subtypes & Scenarios
Obstructive sleep apnoea that adenotonsillectomy has not cured, or that has no surgical target, is the commonest reason a child is put on CPAP. The American Academy of Pediatrics positions CPAP as the main option when surgery is unsuitable or leaves residual disease, and it is highly effective at abolishing obstruction when it is actually worn, which returns the discussion to the adherence problem that dominates paediatric positive airway pressure. This is the scenario where CPAP, not bilevel, is correct, because the problem is obstruction rather than a failure to ventilate. [9] [8]
Neuromuscular disease is the archetypal hypoventilation scenario and the reason bilevel exists. Mellies and colleagues showed that nocturnal non-invasive ventilation corrects the sleep hypoventilation and gas exchange and improves symptoms in children and adolescents with neuromuscular disorders, and that sleep-disordered breathing predictably precedes daytime failure. Ward and colleagues added an important boundary: their randomised trial found that starting nocturnal ventilation once nocturnal hypoventilation is present prevents progression, whereas there is no benefit to starting it prophylactically before hypoventilation has appeared. Timing, guided by the sleep study, is therefore the key. [6] [5]
Across Australia, New Zealand and the United Kingdom the model is a coordinated long-term ventilation service: tertiary respiratory and sleep teams initiate and titrate support, and shared care with local services and families supports the child at home. Guideline frameworks — the European Respiratory Society statement on paediatric long-term non-invasive support, the British Thoracic Society neuromuscular guideline and the American Thoracic Society home invasive ventilation guideline — are broadly aligned, and differences are pragmatic, turning on access to sleep studies and equipment funding. In the ANZ context, delivering safe home ventilation to rural, remote and Indigenous families raises real equity and logistical challenges, and telehealth and outreach are used to bridge distance for titration and follow-up. [2] [1]
Congenital central hypoventilation syndrome is the scenario that shows why a back-up rate matters. These children, with PHOX2B mutations, hypoventilate most severely in sleep and some around the clock, and because the failure is one of automatic drive rather than muscle or airway, they need reliable machine-triggered breaths — bilevel with a back-up rate, mask or tracheostomy ventilation, and in selected children diaphragm pacing — for life, as set out in the American Thoracic Society statement. Getting the mechanism right (drive failure, not obstruction) is the whole point. [4]
Complications & Pitfalls
The complications of non-invasive support are mostly those of the interface and the pressure. Masks cause skin pressure injury over the nasal bridge, and long-term use in a growing child can flatten the midface, which is why interfaces are rotated and reviewed; leak causes eye irritation and ineffective ventilation; and positive pressure can distend the stomach, raising aspiration risk, and rarely contributes to air leak. In the tracheostomy-ventilated child the feared events are tube blockage or displacement and circuit disconnection, all of which can be rapidly fatal. [2]
The pitfalls are errors of reasoning as much as of technique. The recurring mistakes are treating a hypoventilating child with CPAP or oxygen when the breath needs augmenting, letting oxygen mask a rising carbon dioxide, ignoring a weakening cough until a chest infection turns into intensive care, and failing to re-titrate a child who has outgrown the settings. A quieter pitfall is under-supporting the family, so that a technically correct prescription fails at home for want of training, equipment or adherence support. [3] [1]
Prognosis & Disposition
Prognosis is dominated by the underlying condition rather than by the ventilation itself, but appropriate support changes the trajectory. In progressive neuromuscular disease, nocturnal non-invasive ventilation relieves symptoms, corrects nocturnal gas exchange and is associated with improved survival and quality of life, and it can defer or avoid tracheostomy in many children. For central hypoventilation and the most dependent children, support is lifelong, and the goal shifts to a safe, sustainable life at home with the fewest hospital admissions. [6] [1]
Disposition is a discharge-planning exercise as much as a medical one. The child is only ready for home when caregivers are trained and competent, equipment and back-up power are in place, an emergency plan is written, and a community and tertiary team share the follow-up, with regular re-titration as the child grows. For some children with a progressive or life-limiting condition, advance care planning and integration with palliative care are part of good disposition, ensuring support matches the family's goals. [1] [2]
Special Populations
Children with neuromuscular disease are the defining special population, and their care is proactive and cough-focused. Guidelines recommend surveillance of respiratory muscle strength and sleep, early introduction of airway clearance and cough assist when cough weakens, and nocturnal bilevel ventilation timed to the appearance of hypoventilation rather than delayed until daytime failure. Around planned surgery and acute illness these children need explicit respiratory plans, because their reserve is low and secretions are the usual trigger for deterioration. [3] [5]
Children with central hypoventilation and the wider technology-dependent group need lifelong, highly coordinated care. Congenital central hypoventilation syndrome demands reliable machine-triggered ventilation and specialist oversight for its autonomic and neural-crest associations, while the child on invasive home ventilation needs a trained care team, respite support and a service built around family sustainability, as the American Thoracic Society guideline describes. The burden on families is substantial and is part of what the team manages. [4] [1]
Rural, remote and Indigenous families, and those facing socioeconomic disadvantage, meet real barriers to home ventilation — distance from titration and repair services, power and housing reliability, and the cost of consumables. Equitable delivery uses telehealth for follow-up, outreach for titration, and careful attention to the home environment, so that the standard of support does not fall away with distance from the tertiary centre. Matching the intensity of the service to the needs and circumstances of the family is the unifying principle across every special population. [2] [1]
Evidence, Guidelines & Regional Differences
The guideline backbone is four documents that a candidate should be able to name. The European Respiratory Society statement on paediatric long-term non-invasive respiratory support frames modern practice across modalities and interfaces; the British Thoracic Society guideline covers respiratory management of children with neuromuscular weakness, including cough thresholds and airway clearance; the American Thoracic Society clinical practice guideline addresses the child on chronic home invasive ventilation; and the American Thoracic Society statement on congenital central hypoventilation syndrome governs the central-drive child. Together they define who to support, when and how. [2] [1] [3] [4]
The trial and cohort evidence fills in the specifics. Ward established that nocturnal ventilation should begin when nocturnal hypoventilation appears and not prophylactically before it; Mellies showed that long-term non-invasive ventilation corrects nocturnal gas exchange and symptoms in neuromuscular children; Chatwin quantified the benefit of mechanical insufflation-exsufflation on cough; and in acute care the PARIS and HFWHO trials defined the role of high-flow nasal cannula in bronchiolitis, while Marcus documented both the effectiveness and the adherence problem of positive airway pressure. [5] [6] [7] [10] [11] [8]
Regional differences are pragmatic rather than conceptual. High-income systems agree on the principles — match the machine to the mechanism, titrate against a sleep study, build in cough support, and wrap the child in a trained team — but they differ in access to attended polysomnography, in how equipment and consumables are funded, and in how far services reach into rural and remote areas. In Australia and New Zealand the equity dimension, especially for Indigenous and remote families, shapes how the service is delivered rather than what the therapeutic target is. [1] [2]
Exam Pearls
Set up home support — 'VENTILATE'
References
- [1]Sterni LM; Collaco JM; Baker CD; Carroll JL; Sharma GD; Brozek JL; et al An Official American Thoracic Society Clinical Practice Guideline: Pediatric Chronic Home Invasive Ventilation. Am J Respir Crit Care Med, 2016.PMID 27082538
- [2]Fauroux B; Abel F; Amaddeo A; Bignamini E; Chan E; Corel L; et al ERS statement on paediatric long-term noninvasive respiratory support. Eur Respir J, 2022.PMID 34916265
- [3]Hull J; Aniapravan R; Chan E; Chatwin M; Forton J; Gallagher J; et al British Thoracic Society guideline for respiratory management of children with neuromuscular weakness. Thorax, 2012.PMID 22730428
- [4]Weese-Mayer DE; Berry-Kravis EM; Ceccherini I; Keens TG; Loghmanee DA; Trang H An official ATS clinical policy statement: Congenital central hypoventilation syndrome: genetic basis, diagnosis, and management. Am J Respir Crit Care Med, 2010.PMID 20208042
- [5]Ward S; Chatwin M; Heather S; Simonds AK Randomised controlled trial of non-invasive ventilation (NIV) for nocturnal hypoventilation in neuromuscular and chest wall disease patients with daytime normocapnia. Thorax, 2005.PMID 16299118
- [6]Mellies U; Ragette R; Dohna Schwake C; Boehm H; Voit T; Teschler H Long-term noninvasive ventilation in children and adolescents with neuromuscular disorders. Eur Respir J, 2003.PMID 14582916
- [7]Chatwin M; Ross E; Hart N; Nickol AH; Polkey MI; Simonds AK Cough augmentation with mechanical insufflation/exsufflation in patients with neuromuscular weakness. Eur Respir J, 2003.PMID 12662009
- [8]Marcus CL; Rosen G; Ward SL; Halbower AC; Sterni L; Lutz J; et al Adherence to and effectiveness of positive airway pressure therapy in children with obstructive sleep apnea. Pediatrics, 2006.PMID 16510622
- [9]Marcus CL; Brooks LJ; Draper KA; Gozal D; Halbower AC; Jones J; et al Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics, 2012.PMID 22926173
- [10]Franklin D; Babl FE; Schlapbach LJ; Oakley E; Craig S; Neutze J; et al A Randomized Trial of High-Flow Oxygen Therapy in Infants with Bronchiolitis. N Engl J Med, 2018.PMID 29562151
- [11]Kepreotes E; Whitehead B; Attia J; Oldmeadow C; Collison A; Searles A; et al High-flow warm humidified oxygen versus standard low-flow nasal cannula oxygen for moderate bronchiolitis (HFWHO RCT): an open, phase 4, randomised controlled trial. Lancet, 2017.PMID 28161016