Paeds · respiratory-sleep-and-airway
Obstructive sleep apnoea in children
Also known as Paediatric OSA · Childhood obstructive sleep apnoea syndrome · OSAS in children · Sleep-disordered breathing in children · Obstructive sleep apnea (paediatric)
Fellowship guide to obstructive sleep apnoea in children: the spectrum of sleep-disordered breathing and the paediatric severity thresholds, why adenotonsillar hypertrophy and obesity narrow the airway, the pathophysiology that links intermittent hypoxaemia and sleep fragmentation to cardiovascular, neurobehavioural and growth morbidity, the bedside assessment and the role of polysomnography and oximetry, adenotonsillectomy as first-line therapy with continuous positive airway pressure and medical adjuncts, and the high-risk populations that change the plan.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Obstructive sleep apnoea in children is a disorder of breathing during sleep in which the upper airway repeatedly narrows or collapses despite continued respiratory effort, disrupting normal ventilation and sleep. The American Academy of Pediatrics frames it as recurrent partial or complete upper-airway obstruction during sleep, associated with disturbed gas exchange and sleep architecture, and it sits at the severe end of a wider spectrum of sleep-disordered breathing that begins with simple snoring. [1] [2]
The clinical importance of the condition is that it is common, it is treatable, and it is easy to dismiss. A child who snores loudly every night is not simply a noisy sleeper; habitual snoring is the entry symptom of a spectrum that can end in cardiovascular strain, growth failure, and measurable harm to daytime behaviour and learning. The examiner's expectation is that a candidate separates benign primary snoring from true obstructive sleep apnoea and knows that the distinction changes the child's trajectory. [4] [9]
Classification
The useful way to hold the disease in mind is as a graded spectrum rather than a single diagnosis, because where a child sits on the spectrum decides how hard you pursue treatment. Primary snoring is snoring without gas-exchange abnormality or arousal; upper-airway resistance and obstructive hypoventilation are intermediate states with increased work of breathing; and obstructive sleep apnoea proper adds true apnoeas and hypopnoeas with hypoxaemia and arousal. Naming the position on this spectrum is the first step an examiner wants. [1] [4]
Severity in children is graded on the obstructive apnoea–hypopnoea index — the number of obstructive events per hour of sleep — and the paediatric thresholds are deliberately lower than the adult ones, because children are harmed at event rates an adult sleep physician would consider trivial. An index of one to five per hour is mild, five to ten is moderate, and more than ten is severe. Reproducing these paediatric-specific cut-offs, and noting that they differ from adult criteria, is a high-yield discriminator. [1] [4]
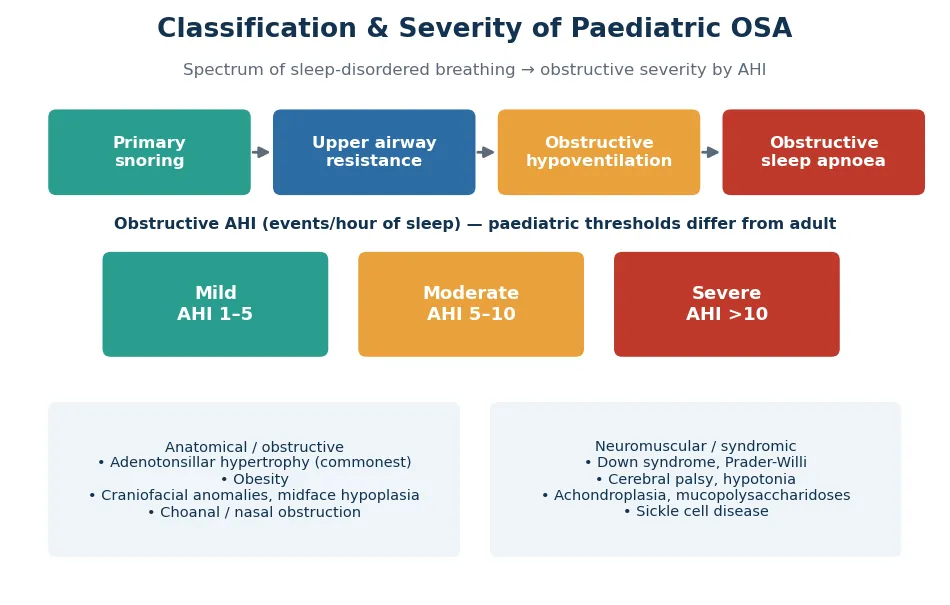
It also helps to classify by mechanism, because the cause steers the treatment. The anatomical or obstructive group is dominated by adenotonsillar hypertrophy and, increasingly, by obesity, with craniofacial and nasal anomalies adding fixed narrowing. The neuromuscular and syndromic group — Down syndrome, cerebral palsy, the mucopolysaccharidoses, achondroplasia and Prader-Willi syndrome — combines anatomical crowding with reduced airway tone, and these children behave differently and are harder to cure with surgery alone. [4] [5]
Epidemiology & Risk Factors
Habitual snoring is very common in childhood, reported in up to a tenth of children, whereas true obstructive sleep apnoea affects a smaller group — most estimates place the prevalence at roughly one to five percent. The peak incidence is between two and eight years of age, coinciding with the period when the adenoids and tonsils are largest relative to the airway. These figures anchor the epidemiology answer and explain why the disease clusters in the preschool and early school years. [1] [2]
The classic community study of risk factors is Redline and colleagues' work, which quantified the associations that still frame the topic: obesity, a history of respiratory problems such as wheeze, and ethnicity all independently increased the risk of sleep-disordered breathing. Their central message is that OSA in children is not a single-cause disease but the product of several converging risks, and that obesity in particular has grown into a major driver as childhood obesity rates have risen. [5]
Beyond adenotonsillar size and obesity, the risk factors an examiner expects are the syndromic and structural ones. Down syndrome combines midface hypoplasia, macroglossia, hypotonia and a small airway, giving very high rates of OSA; craniofacial conditions such as Pierre Robin sequence, achondroplasia and the mucopolysaccharidoses narrow the airway; and neuromuscular disease reduces the tone that keeps it open. Prematurity, a family history of OSA, and allergic rhinitis add further weight, and in the Australian and New Zealand context Aboriginal and Torres Strait Islander and Māori and Pacific children carry a higher burden linked to recurrent respiratory infection and access barriers. [4] [5]
Pathophysiology
The mechanical core of the disease is a mismatch between the size of the airway and the forces that keep it open. During sleep, pharyngeal muscle tone falls, and in a child whose airway is already crowded by large tonsils and adenoids, obesity, or craniofacial narrowing, the negative inspiratory pressure collapses the soft-walled pharynx. The result is a cycle of obstruction, falling oxygen and rising carbon dioxide, an arousal that restores tone and airway patency, and then a return to sleep and the next obstruction. [1] [2]
Two downstream pathways carry the harm, and both should be named. The first is intermittent hypoxaemia and hypercapnia, which drives oxidative stress, systemic and vascular inflammation, and — when chronic and severe — pulmonary vasoconstriction that can progress to pulmonary hypertension and cor pulmonale. The second is repeated arousal and sleep fragmentation, which produces non-restorative sleep and the daytime neurobehavioural consequences that dominate the child's presentation. [2] [9]
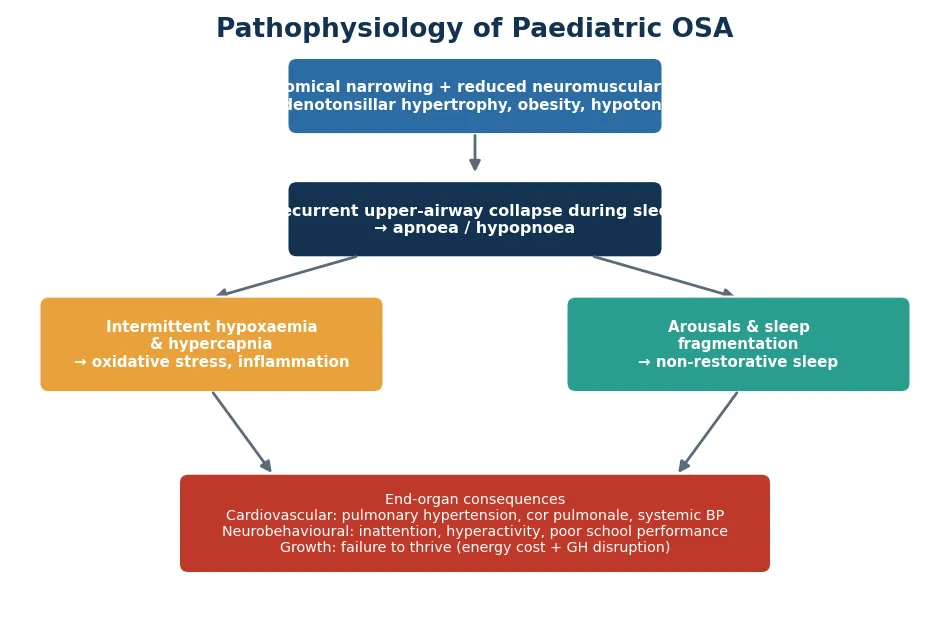
The growth consequence deserves its own mechanism because it surprises candidates. Children with significant OSA can fail to thrive through the increased work of breathing during sleep, which raises energy expenditure, and through disruption of the nocturnal growth-hormone surge that normally occurs in deep sleep. The clinically important corollary is that this growth failure is reversible: catch-up growth after effective treatment is one of the most striking demonstrations that the airway, not the diet, was the problem. [1] [3]
Clinical Presentation
The nocturnal history is where the diagnosis lives, and it must be taken deliberately. Loud snoring on most nights is the entry symptom, and the discriminating features are witnessed pauses in breathing, gasping or snorting arousals, restless sleep with unusual positions such as neck hyperextension, sweating, and paradoxical chest and abdominal movement. Secondary nocturnal enuresis in a previously dry child and mouth breathing round out the picture that separates obstructive disease from benign snoring. [1] [4]
The daytime story in children is characteristically behavioural rather than sleepy. Rather than nodding off, children with OSA are more likely to be irritable, hyperactive, inattentive and to struggle at school, and the overlap with attention-deficit hyperactivity disorder is real enough that a snoring child labelled with ADHD deserves a sleep history. Gozal's classic study showed that first-grade children with sleep-disordered breathing had significantly poorer school performance, and that treatment improved it, which is the evidence an examiner expects on this point. [9]
On examination the aim is to find the anatomical cause and the consequences. The airway examination looks for enlarged tonsils, adenoidal facies with mouth breathing and a hyponasal voice, midface hypoplasia, micrognathia or retrognathia, a high-arched palate and macroglossia, while the general examination plots growth (both failure to thrive and obesity), checks blood pressure, and looks for the signs of pulmonary hypertension and right heart strain. A normal examination in the daytime never excludes OSA, because the obstruction is a sleep phenomenon. [1] [4]
Differential Diagnosis
The first fork is to separate true obstructive sleep apnoea from primary snoring, because the two look identical to a parent but diverge completely in consequence and management. Primary snoring is snoring without apnoeas, hypoxaemia, hypercapnia or arousals, and it does not carry the cardiovascular and growth risk of OSA — although emerging evidence that even primary snoring may affect behaviour keeps the threshold for investigation low. A sleep study is what settles the question when symptoms or morbidity are present. [1] [4]
The daytime presentation opens a second differential. Because childhood OSA presents with inattention and hyperactivity, it must be distinguished from — and can coexist with — attention-deficit hyperactivity disorder, and a sleep history is part of the workup of any child being assessed for ADHD. Other causes of disturbed sleep, such as parasomnias, restless legs and periodic limb movements, insufficient sleep from poor sleep hygiene, and central sleep apnoea in the child with a brainstem or neuromuscular disorder, complete the differential. [1] [9]
Clinical & Bedside Assessment
Bedside assessment is built on a structured sleep history, because that is where the sensitivity lies. The history quantifies the snoring (how many nights, how loud), asks specifically about witnessed apnoeas, gasping, restlessness, sweating, sleeping position and secondary enuresis, and then maps the daytime consequences of behaviour, attention, school performance and growth. A validated tool such as the Pediatric Sleep Questionnaire helps standardise this and improves the reliability of the clinical assessment. [1] [8]
The value and the limit of questionnaires must both be stated. Chervin and colleagues validated the Pediatric Sleep Questionnaire as a reliable measure of sleep-disordered breathing, snoring, sleepiness and behavioural problems, and it is genuinely useful for identifying children who need investigation. Its limitation is that clinical history and questionnaires cannot reliably distinguish primary snoring from OSA or grade severity — they raise suspicion but do not replace an objective study. [8] [2]
The examination pulls the threads together: the airway findings that identify the surgical target, the growth centiles that reveal failure to thrive or obesity, the blood pressure, and the cardiac and hepatic signs that betray pulmonary hypertension. In the child with a syndrome or neuromuscular disorder the bedside assessment is broadened to the whole airway and the underlying condition, because these children are both more likely to have OSA and less likely to be cured by tonsil surgery alone. [1] [4]
Investigations
Overnight, attended, laboratory polysomnography is the reference standard, and stating so plainly is expected. It records airflow, respiratory effort, oxygen saturation, carbon dioxide, electroencephalography and other channels to measure the obstructive apnoea–hypopnoea index, the degree of hypoxaemia and hypercapnia, and the disruption of sleep architecture, and it is the only test that reliably distinguishes primary snoring from OSA and grades severity. Both the American Academy of Pediatrics and the European Respiratory Society position polysomnography as the diagnostic gold standard. [1] [4]
The practical problem is access, because paediatric polysomnography is scarce, and the examiner will want to know what you do when it is unavailable. Nocturnal pulse oximetry is the best-studied abbreviated alternative: Brouillette and colleagues showed that a clearly positive oximetry trace, with clusters of desaturation, has a high positive predictive value for OSA and can be used to expedite treatment. Its weakness is that a normal or non-diagnostic oximetry does not exclude OSA, so a negative result still needs full polysomnography if suspicion remains. [7] [2]
Targeted additional tests follow the clinical picture rather than being routine. A child with severe or long-standing disease, or clinical signs of right heart strain, needs an ECG and echocardiogram to assess for pulmonary hypertension; the obese adolescent may warrant metabolic screening; and the child with a syndrome or complex airway may need nasendoscopy, imaging and multidisciplinary airway assessment before surgery. The examiner rewards a candidate who tailors investigation to risk rather than ordering everything. [1] [4]
Management — Resuscitation

Acute, life-threatening decompensation from OSA itself is uncommon, but two scenarios demand immediate management and should be recognised. The first is the child in respiratory failure with cor pulmonale from severe untreated disease, who needs oxygen, non-invasive ventilatory support and urgent stabilisation before definitive airway surgery, managed in a setting able to escalate. The second is the peri-operative airway, which is where children with OSA most often become acutely unwell. [1] [4]
The peri-operative risk is a heavily examined point. Children with severe OSA, those under about three years of age, and those with obesity, Down syndrome, craniofacial or neuromuscular disorders, or established pulmonary hypertension are at high risk of post-adenotonsillectomy respiratory compromise, including obstruction from oedema and opioid sensitivity. These high-risk children should have their surgery and overnight monitored recovery in a centre able to manage a paediatric airway, and opioids must be used cautiously because the OSA airway is unusually sensitive to respiratory depressants. [1] [4]
Supplemental oxygen deserves a specific caution that examiners like to probe. Giving oxygen to a child with severe OSA can relieve hypoxaemia but risks worsening hypercapnia in the child who is retaining carbon dioxide, so it is used with monitoring of carbon dioxide and as a bridge, not a treatment, while definitive management is arranged. The principle is that resuscitation buys time to fix the airway, and the fix is surgical or ventilatory, not oxygen alone. [1] [2]
Management — Definitive & Stepwise
Adenotonsillectomy is the first-line definitive treatment for the child with OSA and adenotonsillar hypertrophy, and the Childhood Adenotonsillectomy Trial provides the pivotal evidence. Marcus and colleagues randomised children with OSA to early adenotonsillectomy or watchful waiting and found that surgery produced significantly greater improvement in behaviour, quality of life and polysomnographic measures, though not in the primary neurocognitive attention score — a nuance worth quoting. Roughly half of the watchful-waiting group resolved without surgery, which supports a period of observation in milder disease. [3]
The limits of surgery must be stated alongside its success, because they drive the stepwise plan. Bhattacharjee and colleagues' large multicentre study showed that adenotonsillectomy normalises the sleep study in the majority of otherwise healthy children but that residual OSA is common in the obese child and in those with severe baseline disease, asthma or older age. The practical consequence is that these higher-risk children need post-operative reassessment with a repeat sleep study rather than an assumption of cure. [6]
Continuous positive airway pressure is the second-line and the mainstay when surgery is not appropriate or does not cure — the child with residual disease, no surgical target, obesity or a complex airway. It is highly effective when worn, but Marcus and colleagues showed that adherence is the central problem in children, with actual use well below prescribed hours, so success depends on structured support, mask fitting and behavioural strategies as much as on the prescription itself. Medical adjuncts — intranasal corticosteroids and the leukotriene antagonist montelukast — have a role in mild disease and in residual symptoms, and treating nasal allergy, managing weight and optimising sleep position support the overall plan. [10] [1]
Stepwise management of the child with OSA
Confirm and grade with polysomnography (or nocturnal oximetry if PSG is unavailable)
Identify the surgical target: assess adenotonsillar size and the airway
Adenotonsillectomy first-line for the child with adenotonsillar hypertrophy
Risk-stratify for surgery: monitored operation and overnight stay for high-risk children
Reassess high-risk or severe cases with a post-operative sleep study
CPAP for residual disease, no surgical target, obesity or complex airway, with adherence support
Add adjuncts: intranasal corticosteroid or montelukast for mild or residual disease
Manage the drivers: weight, nasal allergy, and sleep position
Intranasal corticosteroid / montelukast (mild or residual OSA adjunct)
Loading dose
Montelukast: 4 mg once daily (2–5 yr), 5 mg once daily (6–14 yr)
Maintenance dose
Intranasal corticosteroid: standard age-appropriate once-daily nasal spray for 6–12 weeks
Specific Subtypes & Scenarios
The obese child with OSA is the scenario that has grown most in importance and behaves least like the classic case. Obesity narrows the airway with soft-tissue deposition, adds a restrictive load, and — critically — predicts residual OSA after adenotonsillectomy, so these children need weight management alongside surgery and a low threshold for a post-operative sleep study and CPAP. The examiner expects recognition that obesity shifts the disease toward the adult phenotype and lowers the cure rate of surgery. [5] [6]
The child with Down syndrome is the archetypal syndromic scenario and a favourite of examiners. The combination of midface hypoplasia, macroglossia, hypotonia, a small airway and a high prevalence of OSA means that many children with Down syndrome have significant disease even without dramatic symptoms, which is why guidelines recommend proactive sleep assessment. Adenotonsillectomy helps but often leaves residual disease, so ongoing surveillance, CPAP and multidisciplinary airway management are frequently needed. [1] [4]
Across Australia, New Zealand, the United Kingdom and comparable systems, adenotonsillectomy for OSA is a very common paediatric operation and the shared model is the same: confirm and grade sleep-disordered breathing (with polysomnography where available and oximetry as a pragmatic alternative given limited sleep-laboratory capacity), operate on the child with adenotonsillar hypertrophy, and reserve monitored surgery and CPAP for high-risk children. In the ANZ setting, Aboriginal and Torres Strait Islander and Māori and Pacific children carry a higher burden of otitis media, recurrent respiratory infection and sleep-disordered breathing, and rural and remote families face real access barriers to sleep studies and specialist surgery, so oximetry-guided pathways and telehealth are important to equitable care. [4] [7]
The child with a craniofacial or neuromuscular disorder — Pierre Robin sequence, achondroplasia, the mucopolysaccharidoses, cerebral palsy — represents the complex-airway scenario in which no single operation cures the disease. These children need multidisciplinary assessment, may require a range of interventions from adenotonsillectomy through CPAP to more complex airway surgery or, rarely, tracheostomy, and they illustrate the principle that treatment is matched to the mechanism of obstruction rather than applied by reflex. [1] [4]
Complications & Pitfalls
The complications of untreated OSA are the reason the diagnosis matters, and they should be recited by system. Cardiovascular harm runs from systemic hypertension to pulmonary hypertension and, at the extreme, cor pulmonale and right heart failure; neurobehavioural harm includes inattention, hyperactivity, impaired executive function and poor school performance; and growth is impaired to the point of failure to thrive. Metabolic consequences and reduced quality of life complete the picture, and the encouraging counterpoint is that many of these harms improve or reverse with effective treatment. [2] [9]
The pitfalls cluster around under-diagnosis and over-confidence. The commonest error is dismissing habitual snoring with obstructive symptoms as benign; the next is assuming that adenotonsillectomy has cured every child, when the obese, severe or syndromic child frequently has residual disease; and a third is failing to anticipate the high-risk peri-operative airway. A quieter pitfall is treating the behavioural presentation as ADHD alone without ever asking about sleep. [1] [6]
Prognosis & Disposition
The prognosis in the otherwise healthy child with adenotonsillar hypertrophy is excellent, and this optimism should be conveyed. Adenotonsillectomy resolves OSA in the majority, with measurable gains in behaviour, quality of life, blood pressure and growth, and the Childhood Adenotonsillectomy Trial also showed that a substantial proportion of children with milder disease improve without surgery, which supports watchful waiting in selected cases. Catch-up growth after treatment is a particularly satisfying and examinable outcome. [3] [6]
The prognosis is more guarded, and the disposition more prolonged, in the obese, severe or syndromic child. Bhattacharjee and colleagues' data make clear that these children often have residual disease after surgery, so their disposition is not discharge after the operation but structured follow-up, a post-operative sleep study, and frequently CPAP with adherence support. The child with Down syndrome, a complex airway or a neuromuscular disorder needs lifelong airway surveillance rather than a single intervention. [6] [1]
Disposition is therefore matched to risk. The uncomplicated child is treated, seen once to confirm resolution of symptoms, and discharged; the high-risk child is treated in a monitored setting, re-studied, and enrolled in ongoing sleep and airway follow-up; and every child benefits from attention to the modifiable drivers of weight, nasal allergy and general health. Equitable access to sleep testing and surgery, especially for rural, remote and Indigenous families, is part of good disposition planning in the ANZ context. [4] [7]
Special Populations
Children with Down syndrome are the special population most examined, and they warrant proactive rather than reactive assessment. Because OSA is so prevalent and often clinically silent in this group, guidelines recommend a sleep assessment in early childhood regardless of reported symptoms, and management commonly extends beyond adenotonsillectomy to CPAP and specialist airway care because residual disease is frequent. This is the clearest example of screening a whole population for OSA rather than waiting for the classic history. [1] [4]
The obese adolescent is the second special population and increasingly the face of the modern disease. Their OSA blends the childhood and adult phenotypes, is less likely to be cured by surgery, and demands genuine weight management alongside CPAP and adjuncts, with attention to the metabolic comorbidity that accompanies it. Framing obesity as both a cause and a barrier to cure is the sophisticated answer here. [5] [6]
Children with neuromuscular disease, complex craniofacial anomalies, and those in rural, remote and Indigenous communities each need a tailored approach. The neuromuscular and craniofacial child needs multidisciplinary airway assessment and often long-term ventilatory support; the rural, remote and Indigenous child faces access barriers to sleep studies and surgery that oximetry-guided pathways and telehealth help to bridge, in a group already carrying a higher burden of respiratory disease. Matching the intensity of assessment and follow-up to the risk of the population is the unifying principle. [4] [7]
Evidence, Guidelines & Regional Differences
The guideline backbone of this topic is the American Academy of Pediatrics clinical practice guideline and its technical report, which together define childhood OSA, set out the diagnostic role of polysomnography, and position adenotonsillectomy as first-line treatment for the child with adenotonsillar hypertrophy. The European Respiratory Society statement complements them with a detailed, stepwise framework for the two- to eighteen-year-old child, and the two bodies agree on the essentials while the ERS document is more granular about the spectrum and the stepwise plan. [1] [2] [4]
The pivotal trial evidence is the Childhood Adenotonsillectomy Trial, which established the benefits of early surgery on behaviour, quality of life and polysomnography and, equally importantly, the reasonableness of watchful waiting in milder disease. The outcome literature is anchored by Bhattacharjee on residual OSA after surgery, by Marcus on the effectiveness and adherence problem of CPAP, by Brouillette on the pragmatic use of oximetry, and by Gozal on the link between sleep-disordered breathing and school performance — the studies that together define modern practice. [3] [6] [7] [9] [10]
The regional differences are pragmatic rather than conceptual. High-resource systems agree on the principles, but access to attended paediatric polysomnography varies widely, and in Australia, New Zealand and much of the United Kingdom limited sleep-laboratory capacity means oximetry-guided and symptom-based pathways are used to prioritise surgery, with post-operative re-study reserved for high-risk children. The ANZ context adds the equity dimension of higher disease burden and access barriers among Indigenous and rural populations, which shapes how services are delivered rather than what the target of treatment is. [4] [7]
Exam Pearls
Screen for OSA — 'SNORE-BAG'
References
- [1]Marcus CL; Brooks LJ; Draper KA; Gozal D; Halbower AC; Jones J; et al Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics, 2012.PMID 22926173
- [2]Marcus CL; Brooks LJ; Draper KA; Gozal D; Halbower AC; Jones J; et al Diagnosis and management of childhood obstructive sleep apnea syndrome (technical report). Pediatrics, 2012.PMID 22926176
- [3]Marcus CL; Moore RH; Rosen CL; Giordani B; Garetz SL; Taylor HG; et al A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med, 2013.PMID 23692173
- [4]Kaditis AG; Alonso Alvarez ML; Boudewyns A; Alexopoulos EI; Ersu R; Joosten K; et al Obstructive sleep disordered breathing in 2- to 18-year-old children: diagnosis and management. Eur Respir J, 2016.PMID 26541535
- [5]Redline S; Tishler PV; Schluchter M; Aylor J; Clark K; Graham G Risk factors for sleep-disordered breathing in children. Associations with obesity, race, and respiratory problems. Am J Respir Crit Care Med, 1999.PMID 10228121
- [6]Bhattacharjee R; Kheirandish-Gozal L; Spruyt K; Mitchell RB; Promchiarak J; Simakajornboon N; et al Adenotonsillectomy outcomes in treatment of obstructive sleep apnea in children: a multicenter retrospective study. Am J Respir Crit Care Med, 2010.PMID 20448096
- [7]Brouillette RT; Morielli A; Leimanis A; Waters KA; Luciano R; Ducharme FM Nocturnal pulse oximetry as an abbreviated testing modality for pediatric obstructive sleep apnea. Pediatrics, 2000.PMID 10654964
- [8]Chervin RD; Hedger K; Dillon JE; Pituch KJ Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med, 2000.PMID 10733617
- [9]Gozal D Sleep-disordered breathing and school performance in children. Pediatrics, 1998.PMID 9738185
- [10]Marcus CL; Rosen G; Ward SL; Halbower AC; Sterni L; Lutz J; et al Adherence to and effectiveness of positive airway pressure therapy in children with obstructive sleep apnea. Pediatrics, 2006.PMID 16510622