Paeds · respiratory-sleep-and-airway
Oxygen therapy and home oxygen in children
Also known as Oxygen therapy in children · Supplemental oxygen · Home oxygen · Long-term oxygen therapy · LTOT · Domiciliary oxygen · Oxygen delivery devices · Nasal cannula · High-flow nasal cannula · Oxygen saturation targets
Fellowship guide to oxygen therapy and home oxygen in children: how to treat hypoxaemia safely without tipping a child into hyperoxia. The page covers the oxygen delivery devices from low-flow nasal cannula through high-flow nasal cannula, Venturi and non-rebreather masks to head boxes, the saturation targets that differ between the acutely unwell child, the extremely preterm neonate and the child with cyanotic heart disease, the physiology of the oxyhaemoglobin dissociation curve that makes those targets matter, the criteria and equipment for discharging a child on home oxygen, and the structured weaning that gets a child off oxygen safely.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child with pneumonia sits quietly in a parent's lap, pink lips, not obviously struggling, and yet the pulse oximeter reads eighty-eight per cent. Oxygen therapy is the treatment for that gap between how a child looks and how well their blood is actually carrying oxygen: it is the delivery of a gas at a higher concentration than room air to correct hypoxaemia, and its whole purpose is to keep tissue oxygen delivery adequate while the underlying illness is treated. [3] [10]
Oxygen is a drug, and like any drug it has a target, a dose and a toxicity. The target is a saturation band, not the highest number obtainable; the dose is the flow and concentration needed to reach that band; and the toxicity is the harm of hyperoxia, which matters most in the newborn. This framing separates the two commonest errors in paediatric practice, which are leaving a hypoxaemic child untreated because they do not look distressed, and drowning a child in oxygen far above the target because more seems safer. [3] [7]
Home oxygen is the same drug carried into the community for the child whose lungs or circulation cannot yet maintain safe saturations on room air, most often after extreme prematurity. It converts a hospital dependence into a life at home, but it demands stability, the right equipment, trained carers and a plan to wean, so that the child is neither discharged unsafely nor kept on oxygen a day longer than needed. [1] [2]
Classification
Oxygen delivery is best understood by asking one question first: does the device deliver a concentration that varies with how the child breathes, or a fixed concentration that does not. Low-flow systems such as the nasal cannula, simple face mask and non-rebreather mask blend with the child's own inspired air, so the actual concentration delivered rises and falls with the child's breathing pattern and minute ventilation. Fixed-performance systems such as the Venturi mask and high-flow nasal cannula deliver a set concentration regardless of how the child breathes. [3] [6]
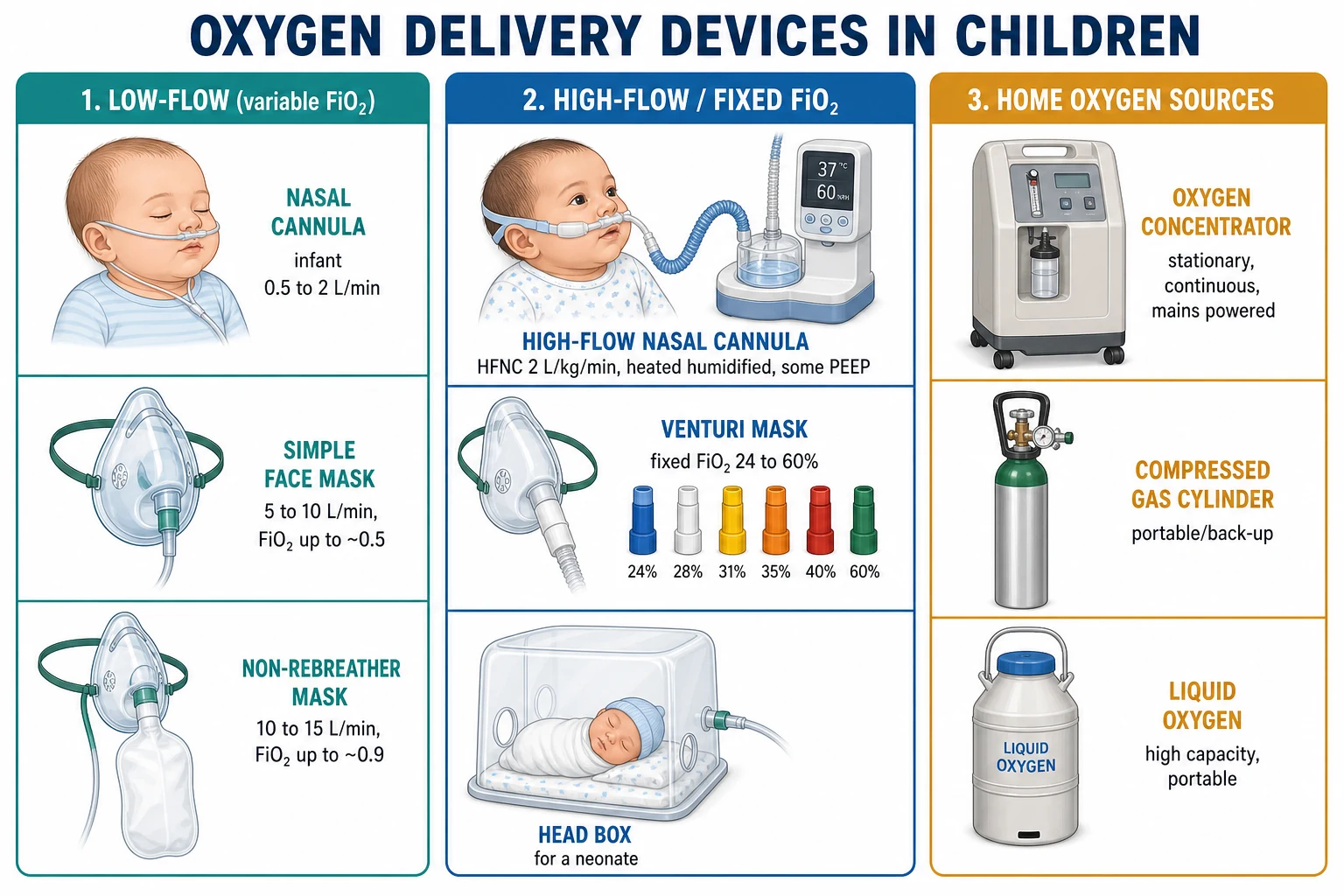
The nasal cannula is the workhorse for children because it is comfortable, allows feeding and speech, and suits the low flows most children need. It delivers a variable concentration that depends on flow and on the child's breathing, and at the higher flows a heated humidified circuit becomes a high-flow nasal cannula that provides a more reliable concentration and a small amount of positive airway pressure. The non-rebreather mask with its reservoir bag is reserved for the acutely unwell child who needs a high concentration quickly. [5] [6]
Low-flow (variable concentration)
- Nasal cannula, simple face mask, non-rebreather mask
- Delivered concentration rises and falls with the child's breathing
- Comfortable, cheap, suits most children needing modest oxygen
- Nasal cannula allows feeding and speech; non-rebreather for emergencies
High-flow / fixed concentration
- High-flow nasal cannula, Venturi mask, head box
- Delivers a set concentration independent of breathing pattern
- Heated humidified high-flow adds some positive airway pressure
- Used when a reliable concentration or flow support is needed
Home oxygen sources
- Concentrator: stationary, continuous, mains powered
- Cylinder: portable and for back-up or outings
- Liquid oxygen: high capacity and portable
- Chosen for the flow the child needs and the family's life
Epidemiology & Risk Factors
Hypoxaemia is one of the most common and most dangerous findings in acutely unwell children worldwide, and it is a strong independent predictor of death in children with pneumonia and other lower respiratory infections. The children who need acute oxygen are therefore drawn from the huge pool of bronchiolitis, pneumonia, asthma and croup that fills paediatric wards, which is why competence with oxygen is a core rather than a specialist skill. [10] [6]
The children who need home oxygen are a much smaller and more selected group. The largest single indication is chronic lung disease of prematurity, the bronchopulmonary dysplasia of the ex-preterm infant whose lungs cannot yet hold safe saturations in air, and the remainder come from pulmonary hypertension, interstitial and other chronic lung diseases, and children needing oxygen for comfort in palliative care. Prematurity is thus the dominant risk factor that leads a child towards a home oxygen programme. [1] [2]
Access shapes who receives oxygen safely. In well-resourced systems the challenge is avoiding overuse and hyperoxia, while in low-resource settings and in remote communities the challenge is the reverse, ensuring that a hypoxaemic child is even detected with a pulse oximeter and reaches a reliable oxygen source. In Australia and New Zealand this equity gap is felt most by rural, remote and Indigenous families, for whom both acute oxygen and a home oxygen programme can be harder to deliver. [10] [1]
Pathophysiology
Oxygen moves from the air to the mitochondria down a series of falling partial pressures known as the oxygen cascade, starting at about one hundred and fifty millimetres of mercury in humidified inspired air and ending at the very low tension the mitochondria work at. Supplemental oxygen raises the pressure at the top of that cascade, lifting the alveolar and then the arterial oxygen tension, which is how it corrects hypoxaemia caused by low inspired oxygen, hypoventilation or ventilation-perfusion mismatch. It cannot help where the problem is a true shunt or a failure of oxygen carriage or delivery. [3] [10]
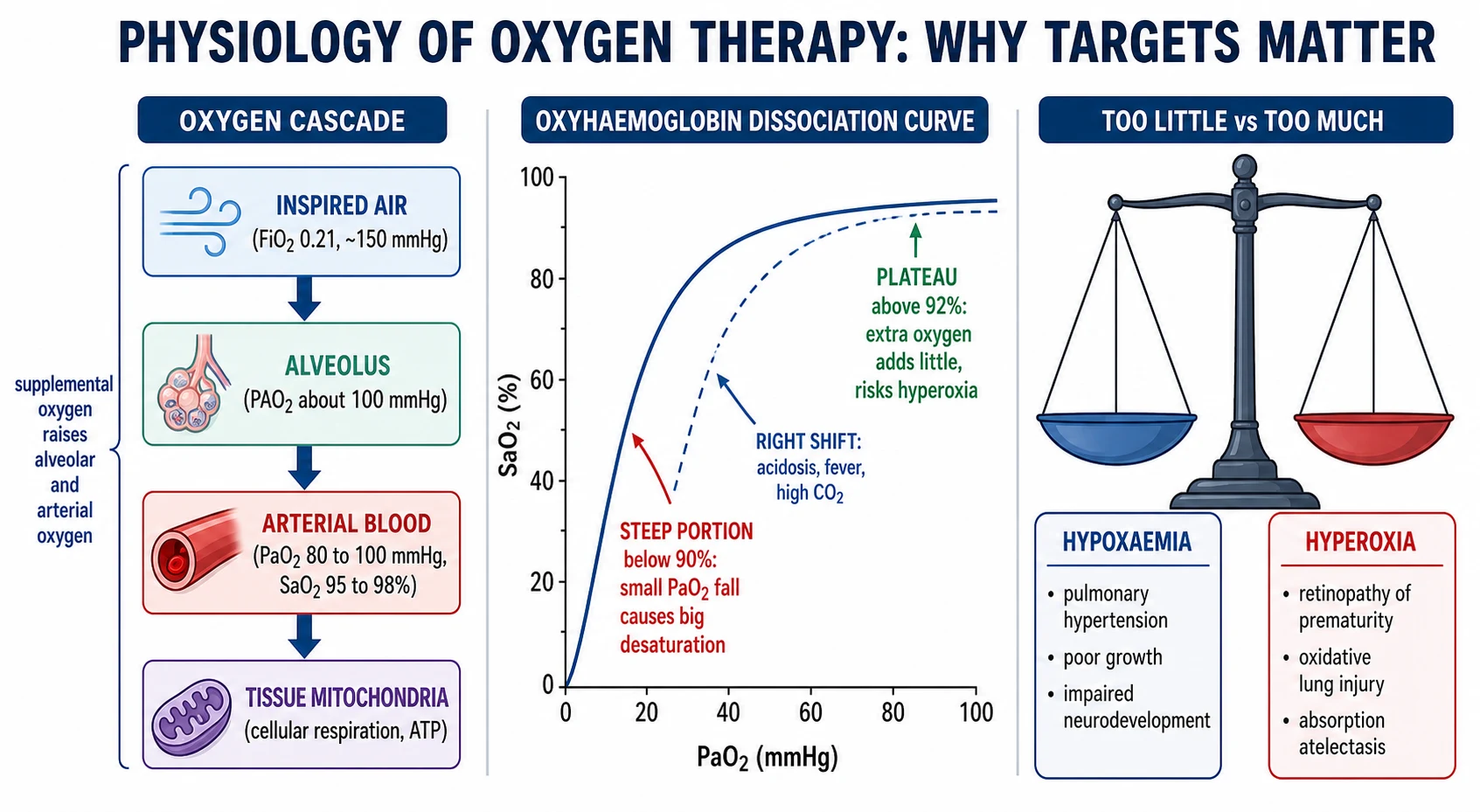
The oxyhaemoglobin dissociation curve explains why the saturation target sits where it does. The curve is sigmoid, so on its steep lower limb, below a saturation of about ninety per cent, a small fall in arterial oxygen tension produces a large fall in saturation, which is why a hypoxaemic child can decompensate quickly. On its flat upper plateau, above a saturation of about ninety-two per cent, pushing more oxygen in barely raises the saturation while it does raise the risk of hyperoxia, which is why chasing one hundred per cent is pointless and potentially harmful. [3] [7]
The harm of too much oxygen is not theoretical, and it is greatest in the extremely preterm neonate. Uncontrolled high oxygen generates reactive oxygen species that injure the immature retina, driving retinopathy of prematurity, and injure the developing lung, and it can cause absorption atelectasis when it washes out the nitrogen that splints alveoli open. This is why neonatal oxygen is blended with air to a set concentration and titrated to a defined saturation band rather than given freely. [7] [9]
The harm of too little oxygen sits on the other pan of the scale. Sustained hypoxaemia drives pulmonary vasoconstriction and, over time, pulmonary hypertension and cor pulmonale, it impairs growth by diverting energy from thriving to breathing, and in the developing brain it contributes to impaired neurodevelopment. Home oxygen for the ex-preterm infant is prescribed precisely to prevent this chronic hypoxic damage during the months the lungs need to mature. [2] [1]
Clinical Presentation
Hypoxaemia often announces itself softly. Some children show the expected signs of tachypnoea, nasal flaring, recession, grunting and, late, cyanosis, but many are dangerously hypoxaemic while looking deceptively settled, feeding poorly, mildly irritable or simply quiet. This silent hypoxaemia is why saturation is measured routinely in any acutely unwell child rather than estimated from appearance, because the eye is an unreliable oximeter and cyanosis is a very late sign. [10] [6]
The child who needs escalating oxygen presents differently and more ominously. A steadily rising oxygen requirement, a child who needed a whiff of oxygen yesterday and a high flow today, signals a worsening disease and impending respiratory failure, and it is the trend rather than any single reading that should trigger reassessment. Signs of exhaustion, a falling respiratory rate in a tiring child, altered conscious state or apnoeas mark the transition from a child who needs oxygen to a child who needs ventilatory support. [11] [5]
The child on home oxygen presents in clinic as a story of stability and growth rather than acute distress. The questions are whether the child is thriving, how much oxygen is needed and when, whether saturations sit in the target band during feeding, activity and especially sleep, and whether the family is coping with the equipment. A child who is growing well and holding saturations on a low flow is on the path to weaning, while one who is not thriving or needs more oxygen needs the underlying disease reviewed. [1] [2]
Differential Diagnosis
A low saturation reading is a symptom, not a diagnosis, and the first task is to separate true hypoxaemia from a false one. A poor pulse oximeter trace from cold peripheries, movement, poor perfusion, nail polish or a malpositioned probe can read low without the child being hypoxaemic, so the reading is confirmed with a good waveform and correlated with the child before oxygen is escalated. Once true, the hypoxaemia points to a cause that oxygen supports but does not cure. [3] [10]
Responds well to oxygen
- Low inspired oxygen: altitude, transport at height
- Hypoventilation: correct the drive or ventilate as well
- Ventilation-perfusion mismatch: pneumonia, bronchiolitis, asthma
- Diffusion problems: interstitial and chronic lung disease
Responds poorly to oxygen
- Right-to-left shunt: cyanotic congenital heart disease
- Fixed intrapulmonary shunt: dense consolidation, collapse
- Do not chase a normal saturation that oxygen cannot reach
- A hyperoxia test helps separate cardiac from lung causes
Not truly hypoxaemic
- Artefact: poor trace, movement, cold, poor perfusion
- Methaemoglobinaemia: saturation reads around eighty-five regardless
- Carbon monoxide: oximeter overreads a poisoned child
- Confirm with the waveform and the clinical picture
Two poisonings deserve special mention because they fool the pulse oximeter. In carbon monoxide poisoning the oximeter cannot distinguish carboxyhaemoglobin from oxyhaemoglobin and reads falsely high, so a normal saturation is meaningless and co-oximetry on a blood gas is needed. In methaemoglobinaemia the saturation tends to sit around eighty-five per cent regardless of the true oxygen content. Recognising that the number can lie is part of interpreting oxygen therapy safely. [3] [10]
The child who does not correct with oxygen raises the possibility of a right-to-left shunt, most importantly cyanotic congenital heart disease in the neonate. A hyperoxia test, observing how much the oxygen tension rises after a period in high inspired oxygen, helps separate a cardiac shunt that barely responds from a lung disease that responds well, and it prevents the trap of pouring oxygen into a duct-dependent circulation that needs prostaglandin rather than oxygen. [3] [1]
Clinical & Bedside Assessment
The bedside assessment of the hypoxaemic child begins with a reliable saturation, which means a good waveform, an appropriately sized probe and a moment to let a settled trace appear before believing a low reading. The saturation is then read together with the work of breathing, the perfusion and the conscious state, because a child with a borderline saturation but severe recession and exhaustion is in more danger than the number alone suggests. Assessing the child, not just the monitor, is the governing principle. [10] [3]
The child being considered for home oxygen needs a different, longer assessment centred on stability over time rather than a single moment. This means recorded oximetry across the day and, crucially, during sleep and feeding when saturations dip lowest, evidence of steady weight gain and feeding, and a clear picture of how much oxygen is needed and when. A single clinic saturation is not enough to prescribe or to stop home oxygen, because the vulnerable periods are the ones not seen in clinic. [1] [2]
Assessment also extends to the home and the family. Before discharge on oxygen the team assesses whether carers understand and can manage the equipment, whether the home has reliable power and is safe, whether there is a smoke-free environment given the fire risk, and whether the family has an emergency plan and support. The bedside skill here is as much social and educational as physiological, because unsafe home oxygen is worse than a longer admission. [2] [1]
Investigations
Pulse oximetry is the central investigation of oxygen therapy, cheap, non-invasive and continuous, and it is the tool that both detects hypoxaemia and guides titration to the target band. Its limitations must be held in mind: it measures saturation not ventilation, it can be fooled by poor perfusion and by carbon monoxide and methaemoglobin, and on the flat upper plateau of the dissociation curve it cannot detect dangerous hyperoxia because the saturation reads high across a wide range of oxygen tensions. [10] [3]
A blood gas is the investigation that answers the questions oximetry cannot. It measures the oxygen tension, and more importantly the carbon dioxide and pH, so it reveals the hypercapnia and respiratory acidosis of a tiring or centrally hypoventilating child in whom oxygen alone would be dangerous. It also allows co-oximetry to detect carboxyhaemoglobin and methaemoglobin, unmasking the poisonings that fool the pulse oximeter. [3] [10]
Investigations beyond the gas are directed at the cause and the consequences. A chest radiograph identifies the pneumonia, effusion, pneumothorax or chronic lung changes behind the oxygen need, and in a child on or heading towards home oxygen an echocardiogram screens for the pulmonary hypertension that chronic hypoxaemia causes. Recorded overnight and feeding oximetry is the specific investigation that decides both the prescription and the eventual weaning of home oxygen. [1] [2]
Management — Resuscitation
In the acutely hypoxaemic or critically ill child, oxygen is given immediately and generously, because in an emergency the priority is to correct life-threatening hypoxaemia rather than to fine-tune a target. A high concentration is delivered through a non-rebreather mask with a reservoir bag, or by bag-mask if the child is not breathing adequately, while the airway is secured and the cause is addressed. Once the child is stabilised, the oxygen is titrated down to the target band rather than left at maximum. [3] [6]
Escalation of respiratory support is the next step when simple oxygen is failing. Heated humidified high-flow nasal cannula delivers a reliable high concentration with a small amount of positive pressure and is widely used in bronchiolitis and other acute illness, and the evidence shows it reduces the need to escalate to more intensive support even though it does not replace low-flow oxygen for milder disease. Continuous positive airway pressure and non-invasive or invasive ventilation follow when high-flow is not enough. [5] [11]
The neonatal resuscitation of the hypoxaemic newborn follows its own rule, that oxygen is titrated rather than given freely. Resuscitation begins with a carefully chosen inspired concentration guided by pre-ductal saturation targets that rise minute by minute after birth, using blended oxygen and air, precisely because a flood of oxygen into a preterm baby is itself harmful. This restraint in the delivery room is the first application of the principle that governs all neonatal oxygen use. [7] [9]
Management — Definitive & Stepwise
Definitive oxygen management is a simple, disciplined loop: set the target band, choose the least invasive device that achieves it, titrate to keep the child in the band, and reassess to escalate or wean. The target band is chosen for the child and the disease, the device starts low and steps up only as needed, and the flow is turned down as the child recovers so that oxygen is never continued beyond its purpose. The figure sets out this pathway from recognition through to home oxygen and weaning. [1] [3]
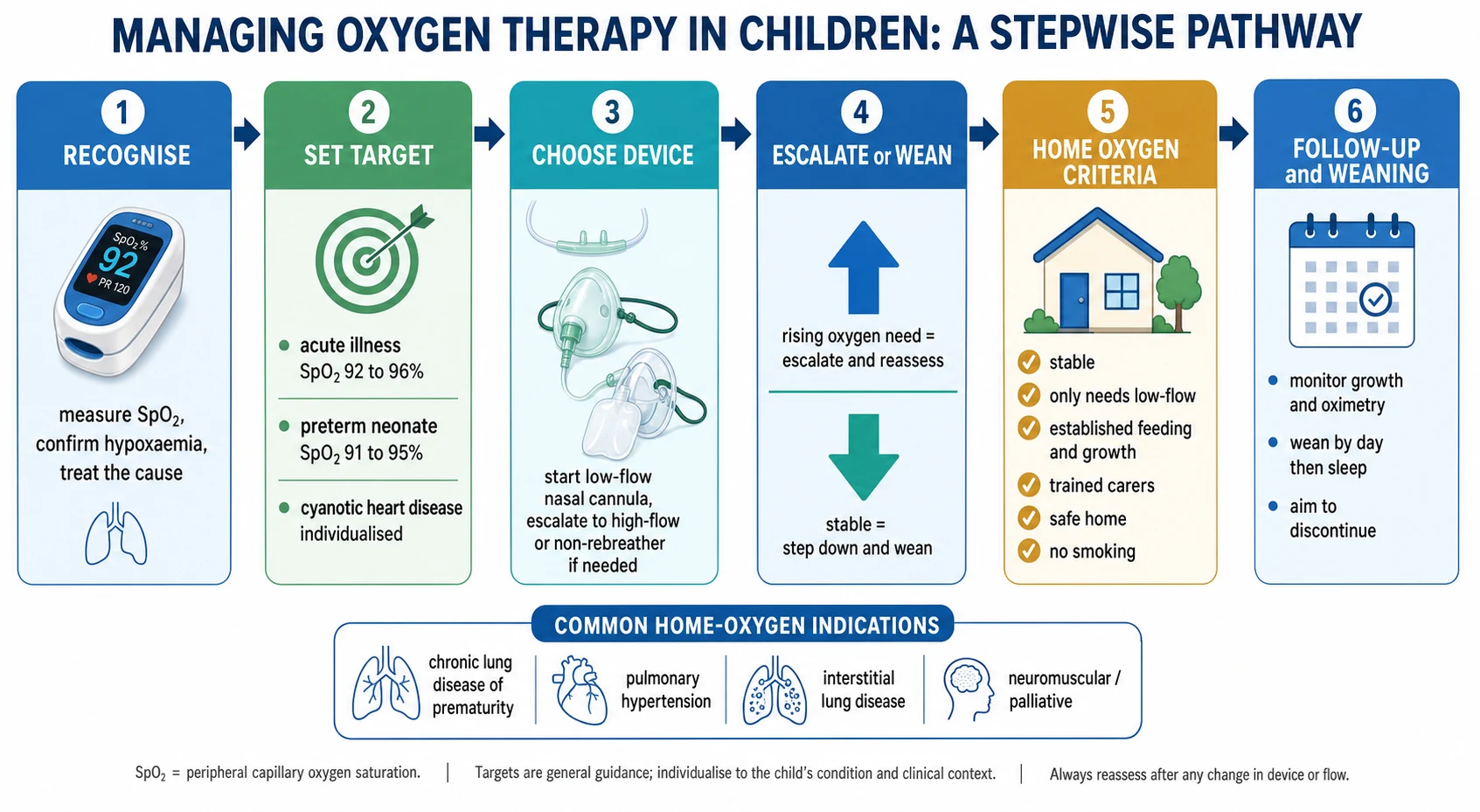
The saturation target is set to the child, and this is where examiners probe. For the acutely unwell child breathing air or oxygen, a band of around ninety-two to ninety-six per cent is widely used, and there is good trial evidence in bronchiolitis that a target of ninety per cent is as safe as ninety-four per cent and shortens oxygen use and admission, showing that higher is not automatically better. For the extremely preterm neonate the prescribed band is a defined range that balances death and disability against retinopathy, and for cyanotic heart disease the target is individualised and often well below the usual range. [4] [7]
The transition to home oxygen is a defined decision, not a drift. A child is considered for home oxygen when the acute illness has resolved and the only remaining problem is a low-flow oxygen requirement, when feeding and growth are established, when saturations sit in the target band on a stable low flow including during sleep, and when the home and carers are ready. Discharge then provides the equipment, the target, a clear flow prescription, carer training, an emergency plan and structured follow-up. [1] [2]
Specific Subtypes & Scenarios
Chronic lung disease of prematurity is the classic home oxygen scenario. The ex-preterm infant with bronchopulmonary dysplasia is discharged on low-flow nasal cannula oxygen to keep saturations in the target band through feeding and sleep, protecting growth and the pulmonary circulation while the lungs mature over the following months. These infants are then weaned gradually as they grow, and most come off oxygen within the first year or two of life. [1] [2]
Bronchiolitis is the commonest acute scenario in which oxygen decisions are made, and it has reshaped practice. The evidence that a saturation target of ninety per cent is as safe as ninety-four per cent, and that oxygen requirement and work of breathing predict intensive care admission better than saturation alone, has pushed practice towards lower, more permissive targets and away from admitting a well-feeding infant for a slightly low number. High-flow nasal cannula is used when simple oxygen is failing rather than routinely. [4] [11]
HOME — deciding a child is ready for home oxygen
Pulmonary hypertension, interstitial and chronic lung diseases, and palliative care make up the other home oxygen scenarios. In pulmonary hypertension oxygen is used to blunt hypoxic pulmonary vasoconstriction, in interstitial lung disease to correct a diffusion defect, and in palliative care to relieve distress and support a child at home near the end of life. Each shares the same framework of a target, a device and a review, but the goals and the weaning differ with the underlying disease. [1] [2]
Complications & Pitfalls
The complications of oxygen therapy fall into those of too much and those of doing it carelessly. Hyperoxia in the preterm neonate drives retinopathy of prematurity and oxidative lung injury and is the reason neonatal oxygen is so tightly controlled, while in any child excessive oxygen can cause absorption atelectasis and, in the child who depends on hypoxic drive or retains carbon dioxide, worsening hypercapnia. Local complications include nasal trauma, drying and epistaxis from unhumidified high flows. [7] [9]
The great pitfall is treating the number instead of the child. Chasing a saturation of one hundred per cent achieves nothing on the plateau of the curve while exposing the child to hyperoxia, and leaving a recovering child on a high flow out of inertia prolongs admission and dependence. The opposite pitfall, being falsely reassured by a normal saturation, is just as dangerous when the child has carbon monoxide poisoning, is hypoventilating, or has a rising oxygen requirement that the single reassuring number conceals. [3] [10]
For home oxygen the pitfalls are practical and safety-critical. Oxygen supports combustion, so smoking or naked flames near the equipment risk fire and burns, cylinders must be secured and stored correctly, and a power failure must not leave a concentrator-dependent child without oxygen, which is why a cylinder back-up and an emergency plan are mandatory. Failing to arrange follow-up oximetry means a child may be kept on oxygen long after they no longer need it. [2] [1]
Prognosis & Disposition
For the acutely hypoxaemic child, the prognosis is that of the underlying disease, and oxygen is the support that buys time for that disease to be treated or to resolve. Most children with bronchiolitis, pneumonia and asthma need oxygen only transiently and recover fully, and the disposition is driven by the trajectory of the oxygen requirement and the work of breathing rather than by a single saturation, with a falling requirement pointing towards discharge and a rising one towards escalation. [11] [6]
For the child on home oxygen, the outlook is generally good and the destination is usually to come off oxygen. Most infants with chronic lung disease of prematurity are successfully weaned as their lungs grow, often within the first year or two, and the home oxygen programme is the bridge that lets that maturation happen safely at home rather than in hospital. The prognosis of the smaller group with pulmonary hypertension or progressive lung disease follows their specific condition. [1] [2]
The disposition of a child on home oxygen is a structured programme rather than a discharge. It includes the equipment and its back-up, a clear prescription of flow and target, carer training, an emergency plan for power or equipment failure, and scheduled review with recorded oximetry to guide weaning. Weaning is done gradually and in a defined order, reducing daytime oxygen first while monitoring saturations and growth, then the more vulnerable sleep-time oxygen, and finally discontinuing once the child holds the target in air. [2] [1]
Special Populations
The extremely preterm neonate is the population in whom oxygen is most dangerous and most tightly governed. Both too little and too much oxygen cause harm, and the large collaborative trials show that a lower saturation target reduces retinopathy but at the cost of more death and necrotising enterocolitis, so a defined prescribed band, delivered with blended oxygen and air and close monitoring, is used to walk this narrow line. This is the clearest example of oxygen as a drug with a true therapeutic window. [7] [8]
The child with cyanotic congenital heart disease is a population in whom the usual saturation target does not apply. Their baseline saturation is low by the nature of their circulation, oxygen barely shifts a fixed right-to-left shunt, and in the duct-dependent neonate high oxygen can be harmful by encouraging the duct to close, so the target is individualised and prostaglandin, not oxygen, may be the treatment. Recognising when a low saturation is expected and should not be chased is essential. [3] [1]
The technology-dependent child on home oxygen, and families in rural, remote and Indigenous communities, form the final special populations. The technology-dependent child needs reliable equipment, trained carers, an emergency plan and careful coordination, while remote and Indigenous families face real barriers to both acute oxygen and a home oxygen programme, from the distance to a pulse oximeter to the logistics of concentrators and cylinders. Equitable access must be planned for explicitly rather than assumed. [1] [10]
Evidence, Guidelines & Regional Differences
The framework for home oxygen in children rests on two guidelines, the American Thoracic Society clinical practice guideline on home oxygen therapy for children and the earlier British Thoracic Society guideline, which together set out the indications, the assessment centred on recorded oximetry, the equipment and the approach to weaning. For acute and emergency oxygen use, the British Thoracic Society guideline on oxygen use establishes the central principle of prescribing to a target saturation band rather than giving oxygen indiscriminately. [1] [2] [3]
The saturation targets for acute illness and for the neonate rest on strong trial evidence. The bronchiolitis trial showing that a target of ninety per cent is equivalent to ninety-four per cent, the collaborative neonatal meta-analyses of saturation targeting, and the systematic reviews of the neonatal target range are the studies that define where the bands sit and why they matter, and they underpin the modern move towards lower, evidence-based targets. The Cochrane review of oxygen for childhood respiratory infection frames the acute indication. [4] [7] [8] [6]
Regional differences are practical rather than definitional. The physiology and the targets are consistent internationally, but access to pulse oximetry, to reliable oxygen sources and to home oxygen programmes varies enormously, and the biggest global contribution of recent work is to reframe pulse oximetry and oxygen as tools whose absence in primary care costs children's lives. In Australia and New Zealand, as elsewhere, the equity focus is on reaching rural, remote and Indigenous children with both acute and home oxygen. [10] [1]
Exam Pearls
Hold one sentence for the viva: oxygen is a drug given to correct hypoxaemia, titrated to a prescribed saturation target band rather than to the highest number, because the oxyhaemoglobin dissociation curve makes extra oxygen useless on its plateau while both too little and too much oxygen cause real harm, most sharply in the preterm neonate. Treat the child and the trend, not the monitor alone. [3] [7]
State the frequently tested facts correctly. Low-flow devices such as the nasal cannula deliver a variable concentration that depends on the child's breathing, while Venturi masks and high-flow nasal cannula deliver a fixed concentration. A common acute target is ninety-two to ninety-six per cent, but the bronchiolitis trial showed ninety per cent is as safe as ninety-four per cent. The pulse oximeter reads falsely high in carbon monoxide poisoning and cannot detect hyperoxia on the plateau. Home oxygen is most often for chronic lung disease of prematurity. [4] [10] [1]
The high-yield pairings do the diagnostic and management work: a rising oxygen requirement means deterioration, not a dose tweak; a normal saturation on high oxygen with a rising carbon dioxide means ventilate rather than oxygenate; uncontrolled oxygen in the preterm neonate means retinopathy of prematurity; a child who does not correct with oxygen suggests a right-to-left shunt and cyanotic heart disease; and weaning home oxygen proceeds day first, then sleep, then off. Always target the band and read the child. [11] [7] [2]
References
- [1]Hayes D Jr; Wilson KC; Krivchenia K; et al Home Oxygen Therapy for Children. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med, 2019.PMID 30707039
- [2]Balfour-Lynn IM; Field DJ; Gringras P; et al BTS guidelines for home oxygen in children. Thorax, 2009.PMID 19586968
- [3]O'Driscoll BR; Howard LS; Earis J; et al BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax, 2017.PMID 28507176
- [4]Cunningham S; Rodriguez A; Adams T; et al Oxygen saturation targets in infants with bronchiolitis (BIDS): a double-blind, randomised, equivalence trial. Lancet, 2015.PMID 26382998
- [5]Franklin D; Babl FE; Schlapbach LJ; et al A Randomized Trial of High-Flow Oxygen Therapy in Infants with Bronchiolitis. N Engl J Med, 2018.PMID 29562151
- [6]Rojas-Reyes MX; Granados Rugeles C; Charry-Anzola LP Oxygen therapy for lower respiratory tract infections in children between 3 months and 15 years of age. Cochrane Database Syst Rev, 2014.PMID 25493690
- [7]Askie LM; Darlow BA; Finer N; et al Association Between Oxygen Saturation Targeting and Death or Disability in Extremely Preterm Infants in the Neonatal Oxygenation Prospective Meta-analysis Collaboration. JAMA, 2018.PMID 29872859
- [8]Manja V; Lakshminrusimha S; Cook DJ Oxygen saturation target range for extremely preterm infants: a systematic review and meta-analysis. JAMA Pediatr, 2015.PMID 25664703
- [9]Saugstad OD; Aune D Optimal oxygenation of extremely low birth weight infants: a meta-analysis and systematic review of the oxygen saturation target studies. Neonatology, 2014.PMID 24247112
- [10]Graham HR; King C; Duke T; et al Hypoxaemia and risk of death among children: rethinking oxygen saturation, risk-stratification, and the role of pulse oximetry in primary care. Lancet Glob Health, 2024.PMID 38914087
- [11]Franklin D; Babl FE; Neutze J; et al Predictors of Intensive Care Admission in Hypoxemic Bronchiolitis Infants, Secondary Analysis of a Randomized Trial. J Pediatr, 2023.PMID 36528052