Paeds · respiratory-sleep-and-airway
Pneumothorax and air-leak syndromes
Also known as Paediatric pneumothorax · Tension pneumothorax in children · Air-leak syndrome · Pneumomediastinum · Pulmonary interstitial emphysema · Pneumopericardium · Primary spontaneous pneumothorax
A fellowship approach to pneumothorax and the wider family of air-leak syndromes in children: recognise tension physiology and decompress before imaging, understand the Macklin route by which alveolar air tracks to the pleura, mediastinum, interstitium and pericardium, separate primary spontaneous from secondary, traumatic and neonatal disease, size the leak, and match management from observation and oxygen through needle decompression, aspiration and chest drainage to surgery for persistent or recurrent leaks.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A previously well 16-year-old, tall and slim, drops to the floor at school with sudden left-sided chest pain and breathlessness; his left chest is quiet and hyper-resonant. Two cots away in the neonatal unit, a ventilated 27-weeker suddenly desaturates and his blood pressure falls, the left chest transilluminating like a lantern. Both children have air in the wrong place, but the physiology, the risk, and the drain you reach for differ — and reading those differences is what this page teaches. [5] [7]
This hub owns the air-leak logic: how air escapes, where it goes, when it is under tension, and how to size and drain it. Disease-specific pages carry the underlying conditions — acute severe asthma, bronchiolitis, and the broader respiratory distress and failure framework into which the collapsing child fits. [2] [8]
A.I.R. L.E.A.K.
Overview & Definition
Watch normal breathing and the two pleural layers glide against each other on a thin film of fluid, held together by a slightly negative pressure that keeps the lung expanded. A pneumothorax breaks that seal: air enters the pleural space, the negative pressure is lost, and the elastic lung recoils inward and collapses away from the chest wall. The child feels it as sudden pleuritic pain and breathlessness. [3] [11]
Pneumothorax is the best-known member of a wider family of air-leak syndromes, all of which begin with air escaping the alveolus or airway into a space it should never reach. That air can settle in the pleura, dissect into the mediastinum as pneumomediastinum, remain trapped within the lung tissue as pulmonary interstitial emphysema, ring the heart as pneumopericardium, or push out into the neck and chest wall as surgical emphysema. The compartment it reaches determines the picture and the danger. [7] [12]
The single most important distinction is not where the air is but whether it is under tension. A simple pneumothorax is a stable collection that the child tolerates; a tension pneumothorax is a progressively enlarging collection that shifts the mediastinum, obstructs venous return, and kills if not decompressed. Tension is recognised at the bedside and treated immediately, and this urgency frames everything else on the page. [2] [7]
Classification
Rather than memorise a list, sort every child with air leak along the questions a clinician actually asks. [5] [11]
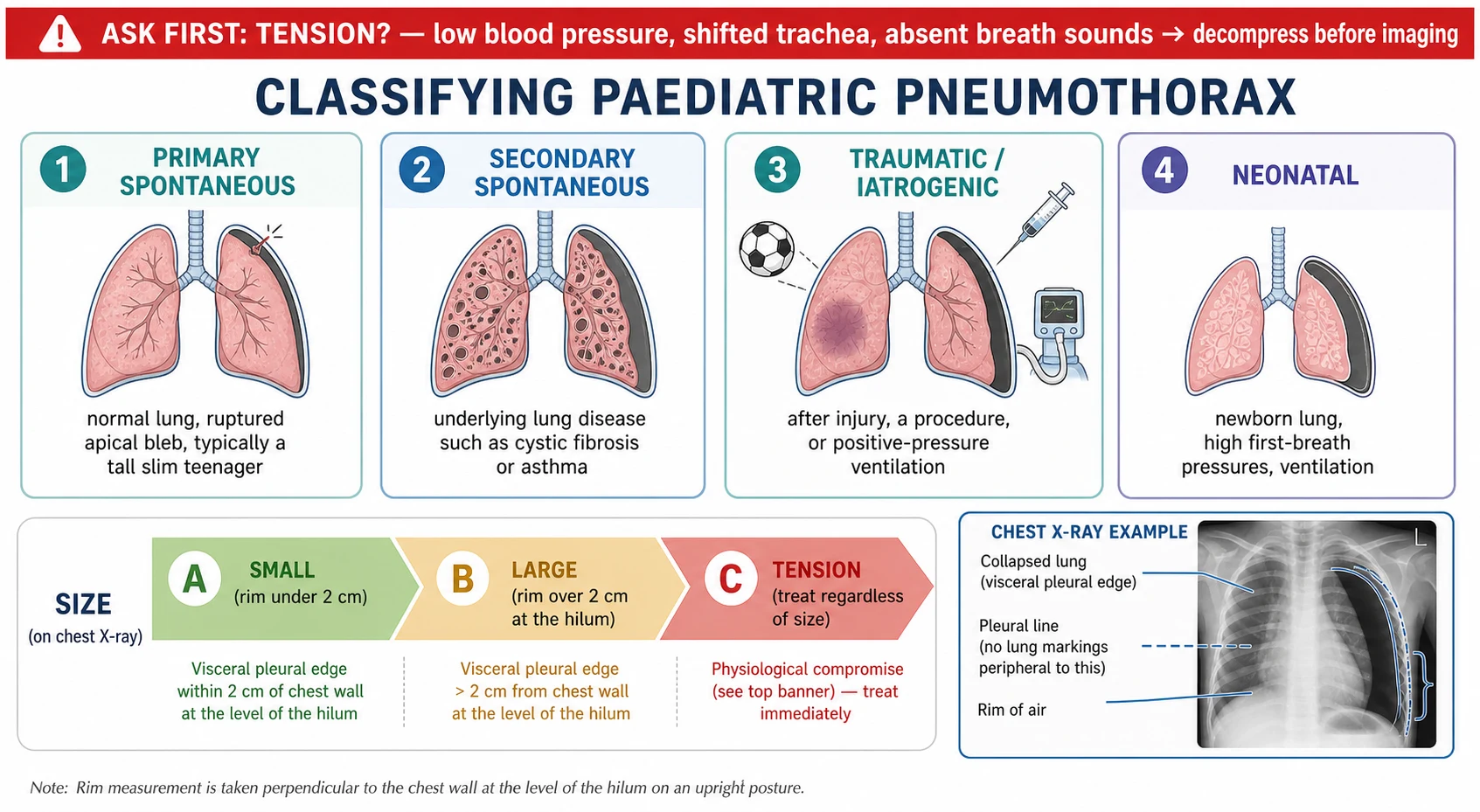
The first cut is tension versus no tension, because it changes the next sixty seconds. A tension pneumothorax with cardiovascular compromise is decompressed on clinical grounds; everything else can be imaged and sized first. This axis drives urgency, not diagnosis. [2] [7]
The second cut is why the lung leaked. A primary spontaneous pneumothorax happens in a structurally normal lung, classically from a ruptured apical bleb in a tall, thin, often smoking adolescent boy. A secondary spontaneous pneumothorax happens on abnormal lung — cystic fibrosis, asthma, connective-tissue disease, or necrotising infection — and behaves worse because reserve is already spent. A traumatic or iatrogenic pneumothorax follows a penetrating or blunt injury, a central line, or positive-pressure ventilation. A neonatal air leak arises around birth from the high transpulmonary pressures of the first breaths, respiratory distress syndrome, meconium aspiration, or ventilation. [5] [8]
The third cut names which compartment holds the air, because pneumomediastinum, interstitial emphysema and pneumopericardium each read differently on examination and imaging and carry their own risks. Sizing then completes the description: a small leak sits close to the lung edge, a large one shows a visible rim of more than two centimetres at the hilum on an erect film, and any leak with tension physiology is treated as an emergency regardless of measured size. [3] [12]
Epidemiology & Risk Factors
Primary spontaneous pneumothorax is predominantly a disease of the tall, thin, adolescent and young-adult male, with a striking body-habitus association and a strong link to smoking that matters greatly for counselling a teenager. It is uncommon before puberty and then rises through the teenage years, which is why it earns a place in paediatric practice despite being rare in young children. [11] [5]
The systematic review literature places primary spontaneous pneumothorax firmly in this demographic and documents its high tendency to recur, particularly on the same side, which shapes the conversation about definitive surgery after a first or second event. Recurrence risk is the single most important epidemiological fact for planning follow-up. [11] [6]
Secondary pneumothorax tracks its underlying disease. Children with cystic fibrosis carry a meaningful lifetime risk and a worse prognosis when it occurs, and pneumothorax in that group signals advanced lung disease. Severe asthma, necrotising pneumonia, connective-tissue disorders such as Marfan syndrome, and catamenial disease in adolescent girls each add their own risk. [8] [2]
At the other end of childhood, symptomatic pneumothorax is most common in the neonatal period of any age group, driven by the high pressures of the first breaths, respiratory distress syndrome, meconium aspiration, and mechanical ventilation. Preterm infants on positive-pressure support are especially prone to pulmonary interstitial emphysema and its progression to overt air leak. [7] [12]
Pathophysiology
Air leak begins when the pressure inside an airspace exceeds what its wall can hold. An overdistended alveolus — from high ventilator pressures, a Valsalva against a closed glottis, gas trapping in asthma, or the huge negative swings of a first neonatal breath — ruptures at its base, where it is least supported. The escaping air then follows the path of least resistance. [12] [7]
The classic route is the Macklin effect: air from the ruptured alveolus dissects along the perivascular and peribronchial sheaths toward the hilum and mediastinum, producing pneumomediastinum, and from there it can decompress into the neck as surgical emphysema or rupture into the pleura as a pneumothorax. When air stays trapped within the interstitial tissue planes of the lung instead of escaping, it forms pulmonary interstitial emphysema, which is both a marker of barotrauma and a precursor to larger leaks. [12] [7]
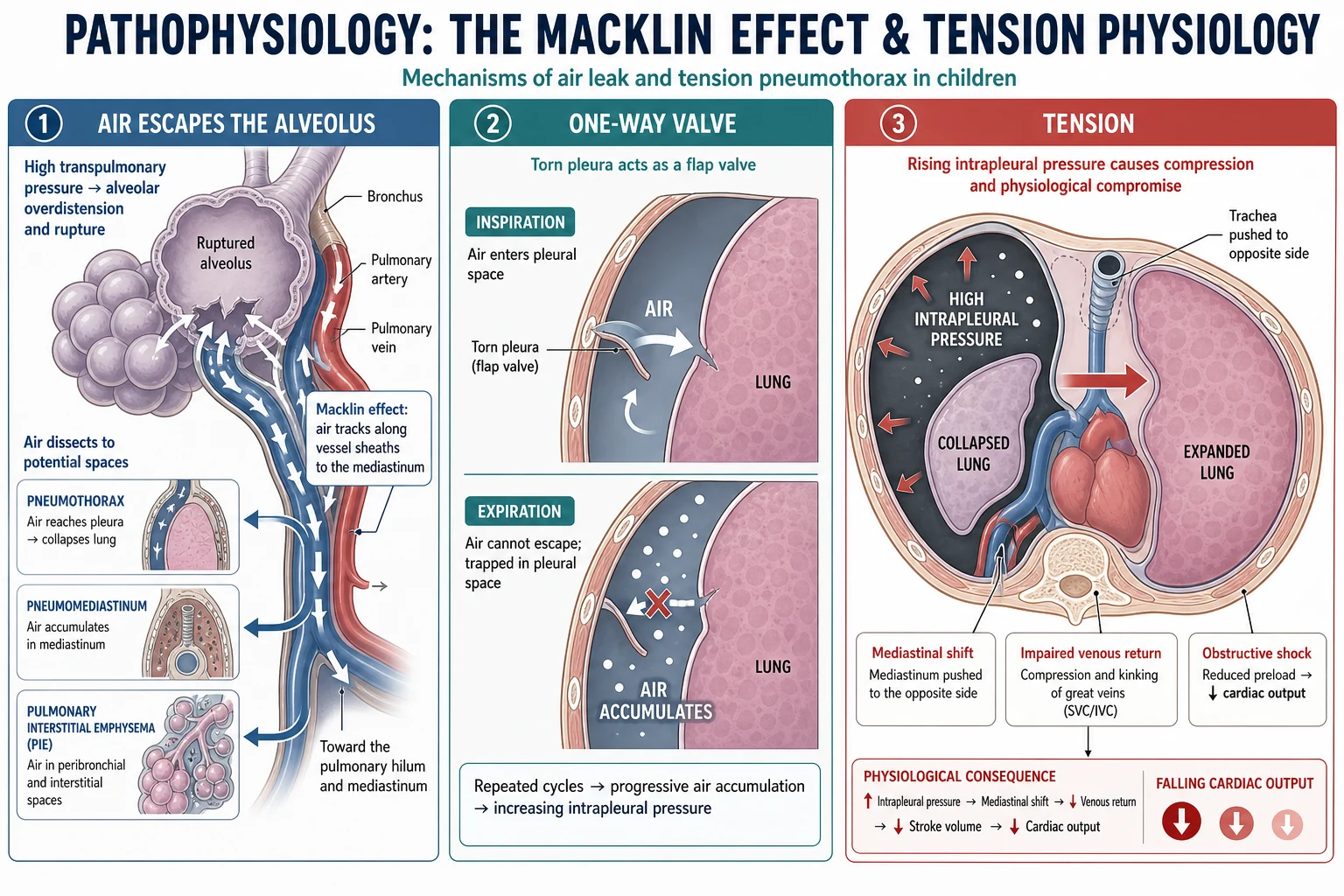
Tension develops when the leak behaves like a one-way valve. Torn pleura or lung admits air into the pleural space on inspiration but seals on expiration, so each breath adds trapped air that cannot escape. Positive-pressure ventilation feeds the valve relentlessly, which is why ventilated children and neonates tension so fast. [2] [7]
As the trapped air accumulates, intrapleural pressure climbs above atmospheric, collapses the ipsilateral lung completely, and pushes the mediastinum toward the opposite side. That shift kinks the great veins and reduces venous return to the heart, so cardiac output falls and the child develops obstructive shock — hypotension, tachycardia and distended neck veins — on top of the respiratory failure. This is the mechanism that makes tension lethal and the reason decompression is immediate. [2] [10]
Children are structurally primed for rapid decline. A small chest, a mobile mediastinum, high oxygen demand and little reserve mean a leak that an adult would tolerate can collapse an infant quickly, and a neonate's compliant mediastinum shifts with alarming ease. The younger the child, the shorter the runway. [10] [7]
Clinical Presentation
The typical spontaneous pneumothorax announces itself as sudden pleuritic chest pain and breathlessness, often at rest, in an adolescent who was previously well. Pain may be sharp and localised to the affected side, and dyspnoea ranges from mild to severe depending on the size of the leak and the reserve of the lung underneath it. [5] [11]
On examination the classic signs are reduced or absent breath sounds and a hyper-resonant percussion note on the affected side, often with reduced chest expansion. These signs are useful when present but can be subtle in a small leak, so their absence never excludes a pneumothorax in a child with a compatible story. [3] [9]
Tension changes the picture into a resuscitation emergency: worsening respiratory distress, hypoxia, tachycardia and hypotension, distended neck veins, and tracheal deviation away from the affected side. In a ventilated child or neonate the first clue is often a sudden rise in oxygen requirement, a fall in blood pressure, or a change in the ventilator trace rather than any physical sign. Trust the physiology. [7] [2]
The other compartments present in their own way. Pneumomediastinum gives central chest pain, a change in voice, and sometimes Hamman's crunch — a crackling sound synchronous with the heartbeat — plus surgical emphysema felt as crackling under the skin of the neck. Pneumopericardium in a neonate can present as sudden collapse with muffled heart sounds and a low-voltage or globular cardiac silhouette, and pulmonary interstitial emphysema shows as worsening gas exchange and a bubbly lucency on the film of a ventilated preterm infant. [12] [7]
Differential Diagnosis
Sudden pleuritic chest pain and breathlessness in an adolescent is not always a pneumothorax, and the differential is worth rehearsing. Musculoskeletal chest-wall pain, pleurisy from a viral or bacterial infection, pericarditis, pulmonary embolism, and anxiety with hyperventilation all mimic it, and only careful examination and a chest film reliably separate them. [11] [9]
When the child clearly has air-leak physiology, the task shifts to naming the compartment. A large pneumothorax, a pneumomediastinum, and surgical emphysema can coexist because they share the Macklin origin, and distinguishing them guides both imaging and drainage. A tension pneumothorax must be separated from other causes of obstructive shock such as cardiac tamponade and massive pulmonary embolism, which is why the combination of unilateral absent breath sounds with shock points so strongly to the chest. [2] [12]
In the collapsing ventilated child the differential for sudden deterioration is captured by the DOPES discipline — displaced tube, obstructed tube, pneumothorax, equipment failure, and stacked breaths — and pneumothorax must be actively excluded rather than assumed away. In the neonate, a large thymus, congenital lobar emphysema, and a congenital pulmonary airway malformation can mimic or coexist with air leak on imaging. [7] [12]
Finally, do not forget that a pneumothorax may be the first presentation of underlying lung disease. A spontaneous pneumothorax in a child with cough, clubbing or failure to thrive should prompt thought about cystic fibrosis, and one in a tall child with a high-arched palate and long limbs about Marfan syndrome. [8] [5]
Clinical & Bedside Assessment
1. First impression and tension check. Before anything else, decide whether this is a tension pneumothorax: severe distress, hypoxia, hypotension, distended neck veins, tracheal deviation, and unilateral absent breath sounds. If those are present, treat now and image later. [2] [7]
2. Focused history. Ask about the onset of pain and breathlessness, previous episodes, smoking and vaping, known lung disease such as cystic fibrosis or asthma, connective-tissue features, trauma, recent procedures, and in a girl any relation to menses. The story often names the category before you touch the child. [5] [8]
3. Structured respiratory examination. Look for reduced expansion, feel for tracheal position and surgical emphysema, percuss for hyper-resonance, and listen for reduced or absent breath sounds on the affected side. Palpable crackling under the skin points to air tracking into the soft tissues. [3] [12]
4. Read the monitors. Continuous oximetry quantifies hypoxia, and in a ventilated child a rising oxygen requirement or a change in the pressure or flow trace can be the earliest sign of a developing leak. Numbers and traces detect what the stethoscope may miss. [7] [10]
5. Point-of-care ultrasound where skilled. In trained hands, absence of lung sliding and of the normal comet-tail artefacts, with a lung point, is sensitive for pneumothorax at the bedside and faster than radiography, as the lung-ultrasound literature established. Use it to confirm, not to delay treatment of tension. [9] [2]
6. Neonatal transillumination. In a small infant a bright cold-light source held to the chest wall lights up the affected hemithorax when a large pneumothorax is present, giving a rapid bedside clue while imaging is arranged. It supports, but does not replace, clinical judgement in the collapsing neonate. [7] [12]
Investigations
Imaging confirms and sizes the leak once the child is stable — it never precedes decompression of a tension pneumothorax. The erect chest radiograph remains the standard first test, showing the visceral pleural line with absent lung markings beyond it, and it lets you measure the rim of air used to grade size. In a supine infant, air collects anteriorly and gives subtler signs such as a deep sulcus and unusually sharp cardiac and diaphragmatic borders. [3] [2]
Point-of-care lung ultrasound has become a valuable adjunct, with loss of lung sliding and the presence of a lung point offering high accuracy at the bedside as described in the BLUE-protocol work. It is particularly useful in the emergency and critical-care setting where moving a sick child to radiology is undesirable. [9] [2]
Computed tomography is reserved for defined questions rather than routine use: characterising blebs and bullae before surgery, clarifying complex or loculated collections, and evaluating suspected underlying lung disease. It should not delay treatment and carries a radiation cost that matters in children. [2] [5]
Investigations of the underlying cause follow the clinical suspicion. A first spontaneous pneumothorax with any suggestive feature warrants thought about a sweat test or genetic testing for cystic fibrosis, echocardiography and connective-tissue assessment where Marfan syndrome is possible, and review of the ventilation strategy in a neonate or a child in intensive care. [8] [7]
Anchors for sizing and escalation
Management — Resuscitation
When tension is suspected in a compromised child, decompress immediately — do not wait for a film. Give high-concentration oxygen, and insert a cannula or perform a finger thoracostomy to release the trapped air, converting a tension pneumothorax to a simple open one, then place a chest drain definitively. The relief of a rush of air and improving observations confirms the diagnosis. [2] [7]
Choose the decompression site with the child's anatomy in mind. The traditional second intercostal space in the mid-clavicular line and the alternative fourth-or-fifth space in the anterior axillary line are both used, and paediatric chest-wall measurements show that cannula length and site must be matched to a child's thinner chest wall to reach the pleura without injuring deeper structures. In small children a fine cannula reaches the space that a standard adult needle might overshoot or fall short of. [10] [2]
In the collapsing neonate, a large tension pneumothorax is decompressed by needle aspiration and then an intercostal drain, and pneumopericardium causing tamponade needs pericardial aspiration. Run the wider resuscitation in parallel — airway, oxygen, and circulatory support — and remember that a sudden deterioration on a ventilator is air leak until proven otherwise. [7] [12]
Management — Definitive & Stepwise
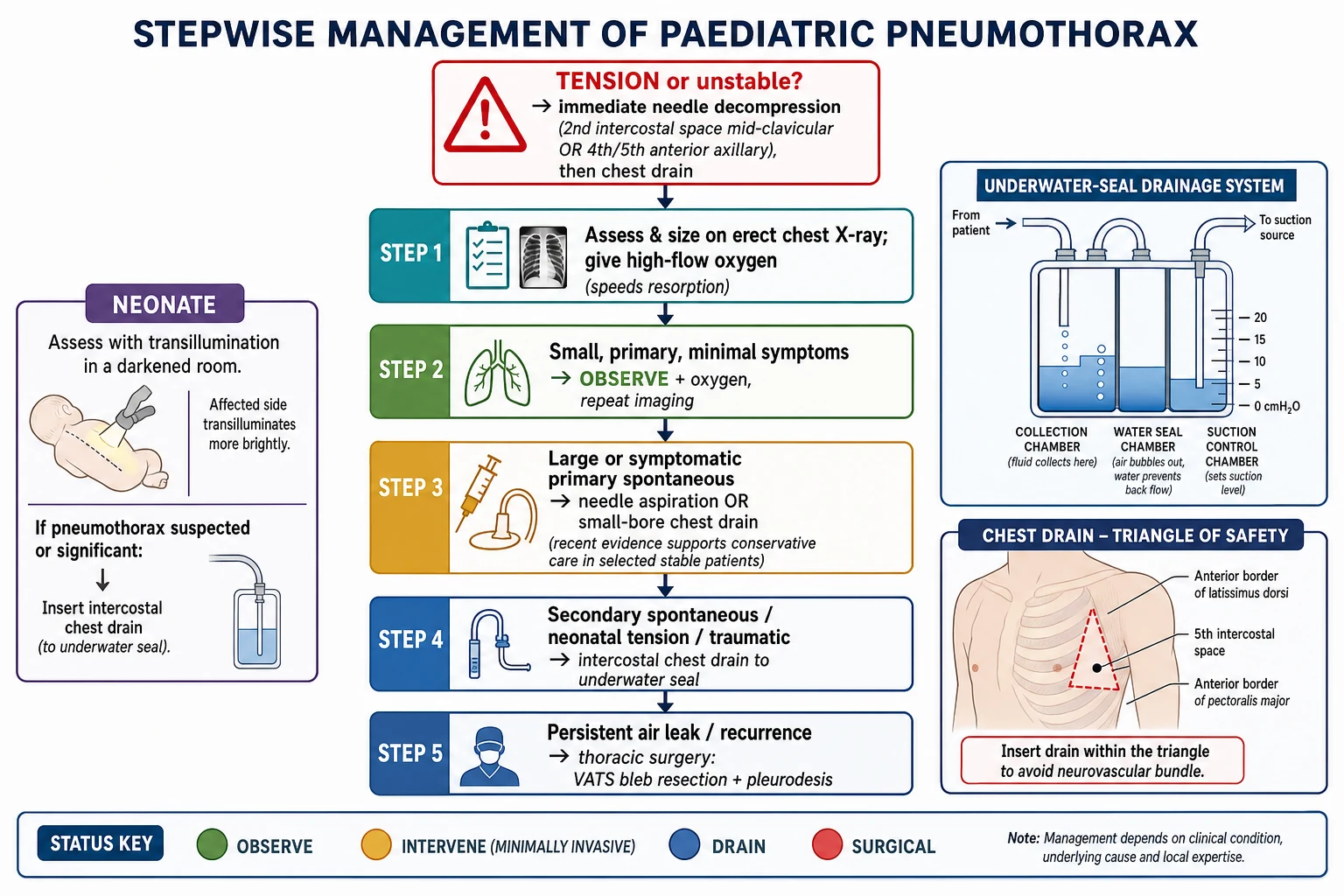
Step 1 — Exclude tension and give oxygen. Every pathway starts by ruling out tension and starting high-concentration oxygen, which relieves hypoxia and speeds resorption of pleural air by widening the nitrogen gradient. Oxygen is useful even when no drain is needed. [2] [3]
Step 2 — Small, primary, minimally symptomatic: observe. A small primary spontaneous pneumothorax in a stable adolescent can be observed with oxygen and repeat imaging rather than drained. The landmark trial of conservative versus interventional treatment showed non-inferior lung re-expansion with fewer adverse events from a watch-and-wait approach in selected patients, and paediatric practice is moving in the same direction. [1] [5]
Step 3 — Larger or symptomatic primary: aspirate or place a small-bore drain. For a larger or symptomatic primary pneumothorax, needle aspiration or a small-bore (Seldinger) chest drain is first-line, reserving larger tubes for cases that fail. Ambulatory devices allow selected stable patients to be managed with a small one-way valve and early discharge, as the ambulatory-management trial demonstrated. [4] [3]
Step 4 — Secondary, traumatic and neonatal leaks: intercostal drain. Secondary spontaneous pneumothorax on abnormal lung, a significant traumatic pneumothorax, and a neonatal tension leak generally need an intercostal chest drain to an underwater seal because reserve is low and the leak is more likely to persist. Admit these children and monitor the drain closely. [8] [7]
Step 5 — Persistent air leak or recurrence: surgery. A prolonged air leak, failure of the lung to re-expand, or a second ipsilateral pneumothorax is an indication for thoracic surgery — usually video-assisted thoracoscopic bleb resection with mechanical or chemical pleurodesis — which markedly reduces recurrence. Discuss surgery early after a first secondary or a recurrent primary event. [6] [11]
Step 6 — Treat the cause and counsel. Optimise the underlying disease — airway clearance and antibiotics in cystic fibrosis, control in asthma, lung-protective ventilation in intensive care — and counsel every adolescent to stop smoking and vaping and to avoid diving and unpressurised flight until cleared. Cause-directed care prevents the next leak. [8] [2]
Specific Subtypes & Scenarios
Primary spontaneous pneumothorax in an adolescent. Confirm it is primary and stable, size it, and choose between observation and a small-bore drain; counsel firmly about smoking, vaping and recurrence, and involve surgery after a recurrence or persistent leak. [1] [5]
Secondary pneumothorax in cystic fibrosis. Treat as a marker of advanced disease with an intercostal drain, early specialist and surgical input, and careful attention to airway clearance; a pneumothorax here changes prognosis and transplant discussions. [8] [6]
Neonatal tension pneumothorax. Suspect it in any ventilated or distressed newborn who suddenly deteriorates, confirm rapidly with transillumination or a film if time allows, and decompress with needle aspiration then an intercostal drain while optimising ventilation. [7] [12]
Pulmonary interstitial emphysema in a preterm infant. Recognise the bubbly interstitial lucency as barotrauma, reduce ventilator pressures, consider gentle or high-frequency ventilation and lateral decubitus positioning of the affected side, and watch for progression to overt air leak. [12] [7]
Pneumomediastinum and surgical emphysema. Isolated pneumomediastinum, often after an asthma attack, forceful vomiting or a Valsalva, is usually benign and self-limiting with rest, oxygen and observation, but exclude an oesophageal or airway injury when the story fits. [12] [2]
Pneumopericardium in a neonate. Suspect it when a ventilated infant collapses with muffled heart sounds and a globular cardiac shadow; a tamponading collection needs urgent pericardial aspiration. [7] [12]
Tension in the ventilated child. Run the DOPES check for sudden deterioration, decompress a suspected tension leak immediately, and adjust ventilation to reduce ongoing barotrauma once the drain is in. [7] [10]
Complications & Pitfalls
- Waiting for a chest X-ray before decompressing an obvious tension pneumothorax. [2]
- Using an adult-length needle in a small child and either overshooting into deeper structures or failing to reach the thin chest wall's pleura. [10]
- Draining a small, stable, primary spontaneous pneumothorax that could safely have been observed. [1]
- Under-treating a secondary pneumothorax as if it were primary, when reserve is low and the leak is likely to persist. [8]
- Missing a developing air leak in a ventilated neonate because the stethoscope was trusted over the rising oxygen requirement and falling blood pressure. [7]
- Forgetting to look for underlying disease — cystic fibrosis or a connective-tissue disorder — after a first spontaneous pneumothorax. [5]
- Failing to counsel an adolescent about smoking, vaping, diving and flying, and so setting up an avoidable recurrence. [11]
Prognosis & Disposition
Most primary spontaneous pneumothoraces in adolescents resolve well, and the shift toward conservative management has reduced the harms of over-intervention without compromising re-expansion in selected stable patients. The dominant long-term issue is recurrence, which is common on the same side and drives the decision to offer definitive surgery after a repeat event. [1] [11]
Prognosis in secondary disease follows the underlying illness. A pneumothorax in cystic fibrosis marks advanced lung disease and a worse outlook, and recurrence and persistent air leak are both more likely, so these children need close specialist follow-up and earlier surgical discussion. [8] [6]
Disposition is matched to category and reserve. A small, observed primary pneumothorax may be managed with a short admission or, with ambulatory devices and clear safety-netting, even as an outpatient in the right setting, whereas secondary, traumatic, neonatal and tension leaks are admitted, and the sickest need intensive care and retrieval. Every discharge carries explicit advice on warning signs and on avoiding diving and unpressurised flight until reviewed. [4] [2]
Special Populations
Children with cystic fibrosis and chronic lung disease: a pneumothorax signals advanced disease, needs an intercostal drain and specialist input, and complicates future transplant candidacy; balance definitive pleurodesis against transplant considerations with the CF team. [8] [6]
Adolescents with connective-tissue disorders: Marfan and related syndromes predispose to spontaneous pneumothorax, so a tall child with a first leak deserves cardiac and connective-tissue assessment and genetic counselling. [5] [11]
Neonates and preterm infants: high first-breath pressures, respiratory distress syndrome, meconium aspiration and ventilation make air leak the commonest form of pneumothorax in childhood, and gentle lung-protective ventilation is the best prevention. [7] [12]
Technology-dependent and ventilated children: positive-pressure ventilation feeds any leak, so suspect tension early in sudden deterioration, run the DOPES check, and adjust ventilation once drained. [7] [10]
Indigenous, rural and remote families: longer transfer times and a higher burden of severe respiratory disease mean a lower threshold for decompression, early drain placement, and retrieval activation, delivered with culturally safe, family-centred care. [2] [8]
Evidence, Guidelines & Regional Differences
The strongest recent evidence is the trial of conservative versus interventional treatment for spontaneous pneumothorax, which showed that watchful waiting was non-inferior for re-expansion with fewer adverse events in selected stable patients and reshaped first-line thinking away from routine drainage. [1]
The ambulatory-management trial extended this by showing that selected patients can be managed with a small one-way valve device and early discharge rather than an inpatient drain, supporting a less invasive, more outpatient-oriented pathway where services allow. [4]
The British Thoracic Society pleural disease guidance provides the operational framework for sizing, aspiration versus drainage, and escalation, updated in 2023 from the earlier 2010 statement, and remains the reference standard that most ANZ and UK units adapt locally. Paediatric-specific reviews translate this adult-derived evidence for children, where the primary-spontaneous demographic and neonatal air leak both differ from adult practice. [2] [3] [5]
For special groups the evidence is disease-specific: the cystic fibrosis pulmonary guidelines set out the management and prognostic weight of pneumothorax in that population, single-institution paediatric protocol analyses inform when children go to surgery, and the classic descriptions of pulmonary interstitial emphysema still anchor neonatal air-leak recognition. [8] [6] [12]
Australian and New Zealand units follow ANZCOR paediatric life support for tension decompression and adapt British Thoracic Society pleural guidance for sizing and drainage, with local protocols such as those from the Royal Children's Hospital Melbourne. Strong retrieval systems shape time-to-drain for rural and remote children, and care for Aboriginal, Torres Strait Islander, Māori and Pasifika families must be culturally safe and family-centred. [2] [8]
UK practice is anchored directly in the British Thoracic Society pleural disease guideline, with growing use of conservative and ambulatory management for primary spontaneous pneumothorax and clear pathways for aspiration, small-bore drainage and surgical referral. [2] [4]
US emergency and critical-care practice follows ATS and CHEST-aligned pleural management with high uptake of point-of-care ultrasound for bedside diagnosis, and paediatric surgical societies guide the timing of video-assisted thoracoscopic surgery for recurrence. [9] [6]
Canadian paediatric practice aligns with the same conservative-versus-interventional evidence base and BTS-style pathways, with RCPSC EPAs anchoring recognition of the deteriorating child and family communication, and provincial retrieval systems supporting rural transfer. [1] [2]
Exam Pearls
- Air leak is defined by where the air goes and whether it is under tension; ask about tension before anything else. [2]
- Tension pneumothorax is a clinical diagnosis treated by immediate decompression, never a chest X-ray first. [7]
- The Macklin effect explains why pneumothorax, pneumomediastinum, interstitial emphysema and surgical emphysema share an origin and often coexist. [12]
- Separate primary spontaneous disease in a tall thin adolescent from secondary disease on abnormal lung — the second behaves worse. [5]
- Conservative observation is non-inferior for selected small, stable, primary spontaneous pneumothoraces. [1]
- A large leak shows a rim of more than two centimetres at the hilum on an erect film, but tension is treated on physiology regardless of size. [3]
- Match needle length and site to a child's thinner chest wall, and give oxygen throughout to speed resorption. [10]
One-line viva opener
"With air leak I first decide whether it is under tension — if the child is shocked with unilateral absent breath sounds I decompress before any film. Once stable, I ask why the lung leaked: primary spontaneous in a tall thin teenager, secondary on abnormal lung, traumatic, or neonatal, then I size it and escalate from oxygen and observation through aspiration and drainage to surgery for a persistent or recurrent leak, while treating the underlying cause." [1] [2] [5]
References
- [1]Brown SGA Conservative versus Interventional Treatment for Spontaneous Pneumothorax. N Engl J Med, 2020.PMID 31995686
- [2]Roberts ME British Thoracic Society Guideline for pleural disease. Thorax, 2023.PMID 37553157
- [3]MacDuff A Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax, 2010.PMID 20696690
- [4]Hallifax RJ Ambulatory management of primary spontaneous pneumothorax: an open-label, randomised controlled trial. Lancet, 2020.PMID 32622394
- [5]Lieu N Update in management of paediatric primary spontaneous pneumothorax. Paediatr Respir Rev, 2022.PMID 34511373
- [6]Stewart S Management of Primary Spontaneous Pneumothorax in Children: A Single Institution Protocol Analysis. J Pediatr Surg, 2023.PMID 36803908
- [7]Jhaveri V Pneumothorax in a term newborn. J Perinatol, 2024.PMID 38409329
- [8]Flume PA Cystic fibrosis pulmonary guidelines: pulmonary complications: hemoptysis and pneumothorax. Am J Respir Crit Care Med, 2010.PMID 20675678
- [9]Lichtenstein DA Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest, 2008.PMID 18403664
- [10]Terboven T Chest wall thickness and depth to vital structures in paediatric patients - implications for prehospital needle decompression of tension pneumothorax. Scand J Trauma Resusc Emerg Med, 2019.PMID 30992028
- [11]Mendogni P Epidemiology and management of primary spontaneous pneumothorax: a systematic review. Interact Cardiovasc Thorac Surg, 2020.PMID 31858124
- [12]Rose SJ Pulmonary interstitial emphysema. Arch Dis Child, 1985.PMID 3885872