Paeds · respiratory-sleep-and-airway
Recurrent wheeze in preschool children
Also known as Preschool wheeze · Episodic viral wheeze · Multiple-trigger wheeze · Viral-induced wheeze · Wheezy toddler
Fellowship guide to recurrent wheeze in preschool children: the phenotype framework (episodic viral versus multiple-trigger wheeze), the Asthma Predictive Index and atopy as the risk stratifier, the small-airway and inflammatory pathophysiology, the bedside assessment that separates wheeze from mimics, the acute and preventive management with the pivotal randomised trials (PEAK, MIST, Ducharme, Bacharier, Panickar), and the natural history that lets most children outgrow it.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Watch a two-year-old with a cold and you will often hear it: a high-pitched, musical, expiratory whistle that comes and goes with each viral illness, then vanishes when the child is well. Wheeze is that continuous musical sound generated by turbulent airflow through narrowed intrathoracic airways, and in the preschool years it is one of the commonest reasons a family brings a child to a doctor. The task the clinician faces is not to hear the wheeze — parents already report it — but to decide what it means and what, if anything, to do about it. [2]
Recurrent wheeze in preschool children is a descriptive label, not a diagnosis. It covers the child under six years with repeated episodes of wheeze, and it deliberately avoids the word "asthma" because most of these children will never have persistent asthma. The landmark Tucson cohort of Martinez and colleagues reframed the whole field by showing that early wheeze is a mix of quite different trajectories, most of which remit, and only a minority of which represent early atopic asthma. Getting the frame right — phenotype and trajectory, not a single disease — is the whole point of the topic. [1] [2]
Classification
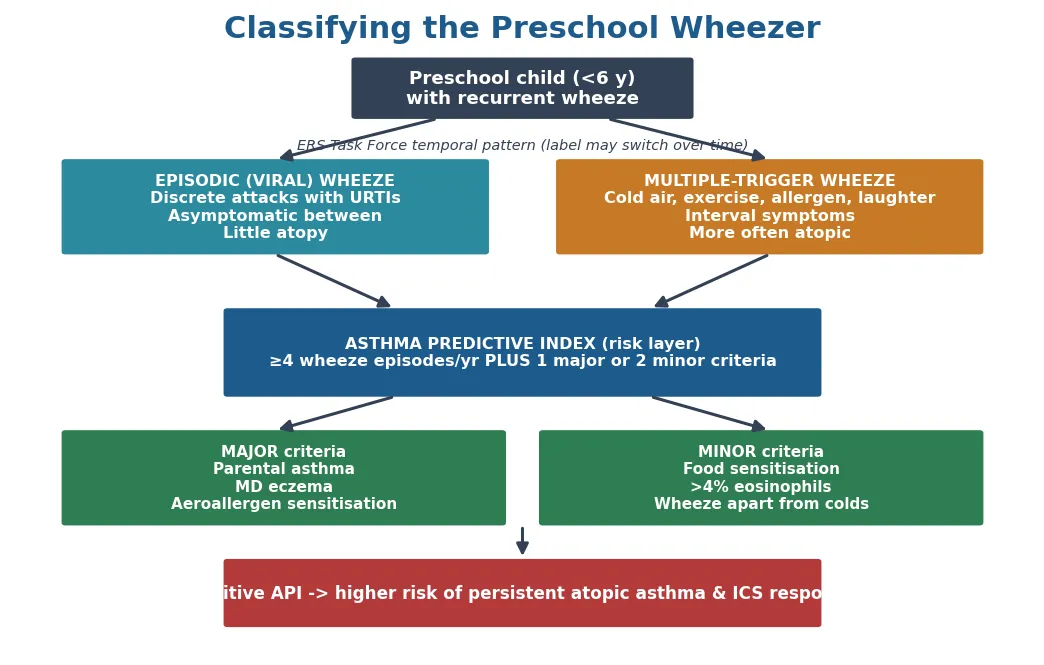
The most useful classification at the bedside is by trigger pattern, because it is what parents can describe and it guides the first treatment decision. The European Respiratory Society Task Force of Brand and colleagues split preschool wheeze into two temporal phenotypes. Episodic (viral) wheeze is wheeze during discrete respiratory illnesses — usually colds — with the child completely well between episodes. Multiple-trigger wheeze is wheeze that also occurs between viral illnesses, provoked by exercise, laughter, crying, cold air, or allergen, implying interval symptoms and a more asthma-like picture. [2]
These phenotypes are practical but unstable, and the candidate must say so. The 2014 update from Brand and colleagues stressed that a child's phenotype can switch between episodic and multiple-trigger over months, that the labels overlap, and that they should guide rather than dictate treatment. The temporal phenotype is therefore a starting point for the conversation about therapy, reviewed at every visit, not a permanent stamp on the child's record. [9]
The second frame is the epidemiological trajectory from the Tucson study, which classifies children retrospectively by when their wheeze starts and stops. Transient early wheezers wheeze in the first three years and then stop; late-onset wheezers begin after three; and persistent wheezers wheeze from infancy onward and are the group enriched for atopy and true asthma. This framework cannot be applied prospectively to the child in front of you, but it explains why most preschool wheeze remits and why atopy marks the group that persists. [1]
Epidemiology & Risk Factors
Preschool wheeze is one of the most common conditions in all of paediatrics. Community cohorts show that roughly one in three children has at least one episode of wheeze by their third birthday and up to half by age six, which is why every general paediatrician and general practitioner meets it constantly. The great majority of these children do not have and will not develop asthma, and the Tucson study established that most early wheeze is transient and resolves as the airways grow. [1]
The risk factors divide neatly into those for wheezing at all and those for wheeze that persists into asthma. Transient early wheeze is driven by anything that reduces airway calibre in infancy: prematurity, small airways, maternal smoking in pregnancy, and viral lower respiratory infection, especially respiratory syncytial virus and rhinovirus bronchiolitis. Persistent, asthma-type wheeze is driven instead by the atopic constitution — parental asthma, the child's own eczema, and early allergic sensitisation — which is the biology the Asthma Predictive Index was built to capture. [1] [3]
Environmental tobacco smoke deserves separate emphasis because it is the single most important modifiable risk factor, increasing both the frequency and severity of wheeze; smoking cessation advice to the whole household is a core part of every consultation. Socioeconomic disadvantage, indoor allergen and mould exposure, and — in the ANZ context — the higher burden of respiratory disease and bronchiectasis among Aboriginal and Torres Strait Islander and Māori and Pacific children shape both risk and the threshold for investigating a wheeze that does not behave typically. [2] [9]
Pathophysiology
Wheeze is a mechanical event: it is the sound of air forced at speed through an airway whose lumen has been narrowed. In the preschool child three processes narrow that lumen — mucosal oedema and mucus from viral inflammation, bronchial smooth-muscle constriction, and, in the atopic child, allergic airway inflammation — and the small starting calibre of the young airway amplifies all of them. Because airway resistance rises with the fourth power of the fall in radius, a small absolute reduction in a small airway produces a large rise in resistance and audible wheeze. [2]
The crucial pathophysiological insight is that the balance of these mechanisms differs between the phenotypes, and that difference explains why the drugs behave so unpredictably. In episodic viral wheeze the dominant process is virus-driven airway narrowing in a largely non-atopic, structurally small airway, and eosinophilic, steroid-responsive inflammation is often absent — which is precisely why inhaled and oral corticosteroids so often disappoint in this group. In multiple-trigger and atopic wheeze, Th2-driven eosinophilic inflammation is present, and this is the biology that responds to inhaled corticosteroid. [4] [8]
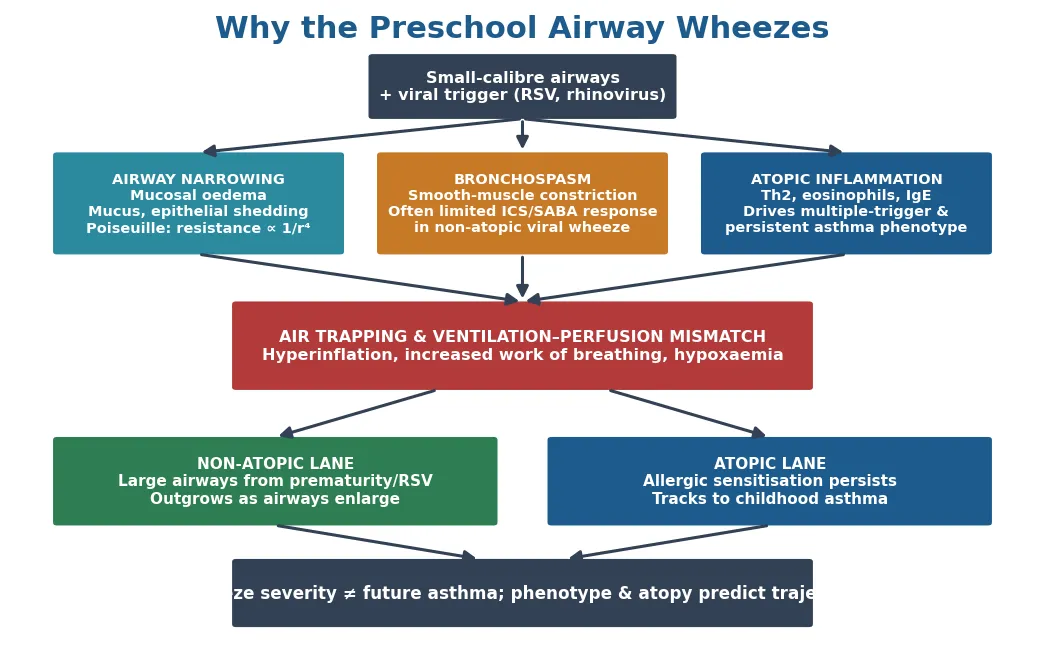
The convergent endpoint of all three mechanisms is the same acute physiology: narrowed airways cause air trapping and hyperinflation, increase the work of breathing, and produce ventilation-perfusion mismatch and hypoxaemia in the severe attack. Understanding this shared endpoint explains the acute treatment — bronchodilation to reduce constriction, oxygen for the mismatch, and steroid where eosinophilic inflammation is contributing. [2] [8]
The natural-history divergence is equally mechanistic. In the non-atopic child the airways enlarge with growth, resistance falls, and the wheeze is outgrown; in the atopic child, allergic inflammation persists and remodels the airway, and the wheeze tracks into school-age asthma. This is why atopy, not the severity of any single attack, is the best predictor of who will still be wheezing at school age. [1] [3]
Clinical Presentation
The typical child is a toddler or preschooler brought in during or after a cold with noisy breathing that the parents call wheeze. The pattern that defines episodic viral wheeze is a discrete attack — cough, audible wheeze, and increased work of breathing over a day or two with a viral illness — that settles completely, leaving the child entirely well between colds, feeding normally, thriving, and running about without symptoms. The number of colds a preschooler catches means such attacks can recur many times a year and still represent this benign phenotype. [2]
The multiple-trigger presentation is different and more asthma-like. Here the parents describe wheeze or cough not only with colds but also with exertion, laughter, crying, cold air, or exposure to a pet or pollen, and often a background of interval cough, nocturnal symptoms, and a personal or family history of atopy. This is the child in whom a positive Asthma Predictive Index and a trial of preventive therapy become relevant. [2] [3]
The history must actively hunt for the features that reclassify the child as something other than preschool wheeze. Onset from birth, a monophonic or fixed noise, symptoms with feeding, a choking episode, chronic wet or productive cough, poor growth, or recurrent pneumonia all shift the differential toward structural, aspiration, or suppurative disease. A careful description of exactly what the parent means by "wheeze" is essential, because upper-airway noise, stertor, and stridor are frequently mislabelled as wheeze. [2]
Differential Diagnosis
The first differential is not between phenotypes but between wheeze and its mimics, because a parental report of "wheeze" is unreliable. Upper-airway rattly noises (transmitted secretions), inspiratory stridor from laryngeal or tracheal narrowing, and stertor from the nasopharynx are all misheard as wheeze, and distinguishing them redirects the whole workup. Where possible, auscultatory confirmation of a genuine expiratory polyphonic wheeze is worth more than the label the family brings. [2]
Once a true lower-airway wheeze is established, the serious structural and suppurative mimics must be excluded before the wheeze is dismissed as benign. An inhaled foreign body causes sudden monophonic wheeze, classically after a choking episode and often with a normal chest radiograph, and demands bronchoscopy. Cystic fibrosis, primary ciliary dyskinesia, bronchiectasis, and immunodeficiency present with a chronic wet cough, failure to thrive, and recurrent infection. Tracheobronchomalacia and vascular rings cause a fixed or positional wheeze from early life. Recurrent aspiration and gastro-oesophageal reflux, and cardiac failure from a large left-to-right shunt, complete the list. [2] [9]
Only after the mimics are considered does the differential become the one the topic is really about: which wheeze phenotype is this, and what is the child's future asthma risk? That question is answered by the trigger pattern, the atopic history, and the Asthma Predictive Index rather than by any single test. [3]
Clinical & Bedside Assessment
Assessment rests on the history, because there is no confirmatory test for preschool wheeze and lung-function testing is generally impossible before school age. The history establishes the trigger pattern (colds only versus multiple triggers), the interval symptoms, the response to any previous treatment, the atopic background (the child's eczema and food allergy, and parental asthma), the environmental exposures (above all tobacco smoke), and the red-flag features that would reclassify the child. A three-generation atopic family history and an environmental smoking history are not optional extras but core data. [2] [3]
Examination has two jobs: to assess severity in the acute setting and to look for the clues to a mimic in the well child. In the acute attack the severity is judged clinically — respiratory rate, recession and accessory muscle use, the ability to feed and talk, oxygen saturation, and, at the dangerous end, a silent chest, exhaustion, cyanosis, and altered consciousness. In the well child the examination should confirm normal growth, look for eczema, and specifically seek clubbing, chest-wall deformity, a fixed added sound, or signs of a chronic suppurative process that would take the diagnosis elsewhere. [2]
Acute preschool wheeze — clinical severity
Severe
SpO2 <92%, marked recession, too breathless to feed or talk, agitation
Objective testing has a limited role. Formal spirometry is unreliable under about six years; a chest radiograph is not routine and is reserved for atypical presentations, focal signs, or suspected foreign body or structural disease; and a trial of treatment with a clear plan to review the response is often the most informative "investigation" of all. Where atopy is in question, allergen sensitisation can be assessed by skin-prick testing or specific IgE to inform the Asthma Predictive Index. [3] [9]
Investigations
There is no single investigation that diagnoses preschool wheeze; the diagnosis is clinical, and investigation is directed at excluding mimics and at stratifying atopic risk rather than at confirming the label. In the child whose story and examination are entirely typical of episodic viral wheeze, no investigation is required at all beyond a good history and a smoking and environmental assessment. [2]
Investigation is triggered by atypia. A chest radiograph is indicated for focal or persistent signs, suspected foreign body, or a suppurative picture, though its yield is low in typical wheeze. A sweat test and cystic fibrosis genetics are mandatory when growth is poor or the cough is chronically wet. Tests for primary ciliary dyskinesia, an immune workup, a video fluoroscopic swallow for aspiration, and bronchoscopy for a suspected foreign body or structural lesion are each driven by specific red flags. [2] [9]
A directed approach to investigating recurrent preschool wheeze
Confirm the noise really is expiratory wheeze, not stridor, stertor, or transmitted upper-airway rattles
If the story is typical episodic viral wheeze and the child thrives, investigate no further
Assess atopy (eczema, food allergy, family asthma; skin-prick or specific IgE) to inform the Asthma Predictive Index
Reserve the chest radiograph for focal signs, atypical course, or suspected foreign body or structural disease
Order a sweat test and CF genetics for failure to thrive or chronic wet cough
Escalate to bronchoscopy, PCD testing, immune workup, or swallow study when the corresponding red flag is present
The Asthma Predictive Index is the nearest thing to a risk investigation. Castro-Rodríguez and colleagues derived it from the Tucson cohort: a child with frequent wheeze (four or more episodes in the past year, in the stringent version) plus either one major criterion (a parent with asthma, doctor-diagnosed eczema, or aeroallergen sensitisation) or two of three minor criteria (food sensitisation, blood eosinophilia of four percent or more, or wheeze apart from colds) has a substantially higher risk of persistent asthma at school age. Its strength is a high specificity — a positive stringent index meaningfully raises the probability of later asthma — while its sensitivity is only moderate, so a negative index does not guarantee the child will not develop asthma. [3]
Management — Resuscitation
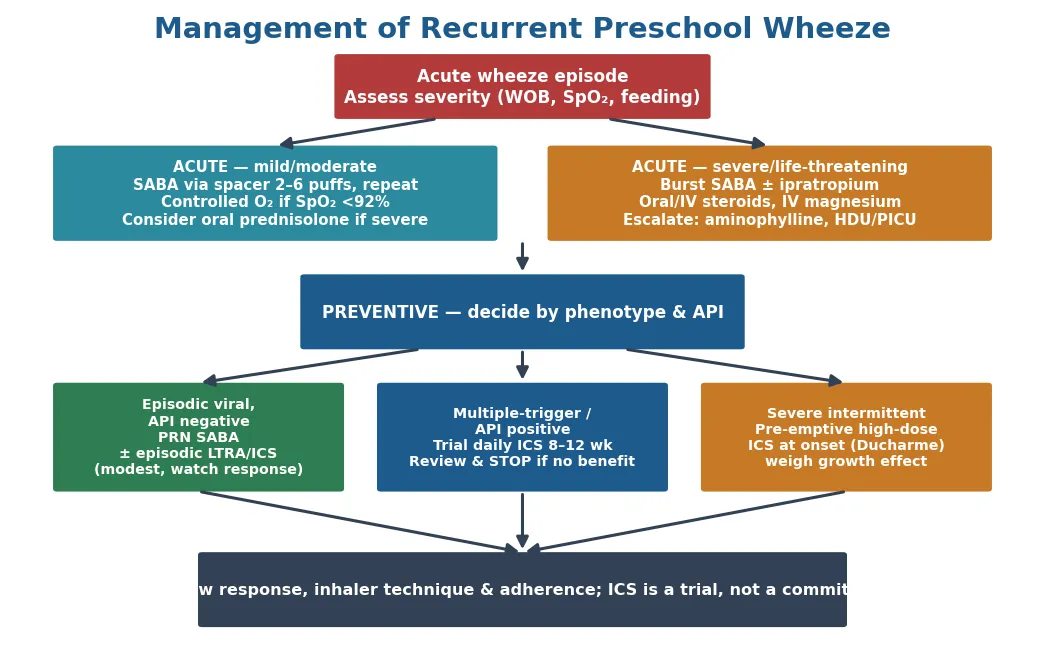
The resuscitation scenario is the preschooler in an acute severe or life-threatening attack, and the priorities are the same as for acute childhood asthma. Assess the airway, breathing, and circulation; give controlled oxygen to keep saturations at or above 92 percent; and deliver a bronchodilator immediately. For a child who is not in extremis, salbutamol by metered-dose inhaler and spacer is as effective as a nebuliser and is preferred; for the severe or life-threatening attack, nebulised salbutamol driven by oxygen, with nebulised ipratropium added, is used and repeated. [2] [8]
Systemic corticosteroid is given in the severe attack and to the child who requires admission, while recognising the limits of the evidence in this age group. Panickar and colleagues' randomised trial showed that oral prednisolone did not shorten hospital stay in preschool children admitted with mild-to-moderate virus-induced wheeze, which has led many services to reserve systemic steroid for severe attacks, for children with a strong atopic or asthma phenotype, and for those needing intensive care rather than giving it reflexively to every wheezy admission. The severity of the attack, not the wheeze label alone, drives the decision. [8]
Salbutamol (acute preschool wheeze)
Loading dose
MDI + spacer: 2–6 puffs (100 mcg/puff), repeat every 20 min as needed; nebulised 2.5 mg if severe
Maintenance dose
Space out as the child improves; step down to as-needed
Immediate management of the acute severe wheeze attack
Assess ABC and clinical severity; give controlled oxygen to keep SpO2 ≥92%
Salbutamol MDI + spacer for moderate; nebulised salbutamol with ipratropium for severe, repeated
Give a systemic corticosteroid (oral prednisolone, or IV if not tolerating oral) for the severe attack or admission
Reassess response continuously; escalate the bronchodilator frequency for non-response
For life-threatening features add IV magnesium sulphate and consider IV salbutamol or aminophylline
Involve senior and PICU/retrieval teams early for the exhausted, silent-chest, or deteriorating child
The disposition after stabilisation depends on the response: the child who improves promptly and maintains saturations on stretching bronchodilators can go home with a clear action plan and follow-up, while the child who needs frequent bronchodilators, oxygen, or is exhausted is admitted, and the deteriorating or life-threatening child is escalated to high-dependency or intensive care. [2]
Management — Definitive & Stepwise
Preventive management is where preschool wheeze diverges most sharply from school-age asthma, and the guiding principle is that pharmacotherapy is matched to the phenotype and offered as a monitored trial. For the child with genuine episodic viral wheeze and a negative Asthma Predictive Index, the default is a reliever (salbutamol via spacer) for attacks and no maintenance treatment, because the evidence for daily controllers in this group is weak and the phenotype usually remits. Intermittent strategies — an episodic leukotriene receptor antagonist or episodic inhaled corticosteroid at the onset of a cold — have been studied and offer at best modest benefit. [2] [6] [9]
For the child with multiple-trigger wheeze or a positive Asthma Predictive Index — the atopic phenotype — a trial of daily inhaled corticosteroid for eight to twelve weeks is the key intervention, reviewed formally at the end of the trial and continued only if it clearly helps. The PEAK study of Guilbert and colleagues is the anchor evidence: two years of daily inhaled fluticasone in preschool children at high risk of asthma improved symptoms during treatment but conferred no lasting disease-modifying benefit once stopped and produced a small, transient reduction in growth. The message is that inhaled steroid controls symptoms in the responsive child but does not change the natural history, so it is used for control, reviewed, and stepped down. [4] [9]
Two randomised trials refine the intermittent option and are high-yield. Ducharme and colleagues showed that pre-emptive high-dose inhaled fluticasone started at the first sign of a cold reduced the use of rescue oral corticosteroids in preschool children with recurrent moderate-to-severe virus-induced wheeze, but at the cost of a small reduction in growth, so it is reserved for selected children with severe episodes. Bacharier and colleagues compared episodic inhaled corticosteroid with episodic montelukast against placebo in intermittent wheezing and found neither strategy dramatically superior, reinforcing that intermittent controllers give only modest benefit. Zeiger and colleagues' MIST study then showed that intermittent high-dose budesonide at the onset of illness was broadly comparable to daily low-dose budesonide for the frequency of severe exacerbations, with less total steroid exposure. [5] [6] [7]
[4] [5] [7]Non-pharmacological management underpins every plan: eliminating tobacco-smoke exposure, correcting inhaler and spacer technique (which is the commonest reason a "controller failure" is really a delivery failure), checking adherence, providing a written action plan, and arranging review. Any preventive drug that does not produce a clear, reviewed benefit is stopped rather than continued or escalated. [2] [9]
Specific Subtypes & Scenarios
The frequently-relapsing viral wheezer is the scenario that most tests judgement. This is the non-atopic child with repeated severe attacks needing acute care but who is well between them, and the temptation is to escalate to daily inhaled steroid as one would in asthma. The evidence — PEAK, Bacharier, and MIST — argues instead for a pre-emptive or intermittent strategy targeted at the episodes, with Ducharme's pre-emptive high-dose inhaled steroid reserved for the severe end, and with an honest acknowledgement to the family that the aim is to blunt the attacks, not to cure a disease the child may not have. [4] [5] [7]
The atopic multiple-trigger child heading toward asthma is the mirror scenario. Here the interval symptoms, the eczema and allergic sensitisation, and a positive Asthma Predictive Index all point to eosinophilic, steroid-responsive disease, and a daily inhaled-corticosteroid trial is both more justified and more likely to work. This child needs the atopic comorbidities addressed, the family educated about the likely persistence into school-age asthma, and structured follow-up. [3] [4]
PEAK (Guilbert 2006) — daily ICS in high-risk preschoolers
Practice change
Inhaled corticosteroid controls symptoms in the responsive high-risk child but does not modify the natural history of asthma — so it is a monitored controller, not a cure, and is reviewed and stepped down.
The child from a household with tobacco smoke, and the child from a background with a high burden of chronic suppurative lung disease, form a third scenario cluster. In the smoking household the highest-value intervention is cessation support for the caregivers; in the Aboriginal, Torres Strait Islander, Māori, or Pacific child, or any child with a chronically wet cough, the threshold to investigate for bronchiectasis and protracted bacterial bronchitis is deliberately lower, because a "wheeze" that is really recurrent wet cough has a different and treatable cause. [2] [9]
Complications & Pitfalls
The complications of recurrent preschool wheeze are those of the acute attack, of the missed alternative diagnosis, and of the treatment itself. A severe attack can progress to respiratory failure needing intensive care, and — in the child whose wheeze is actually a foreign body, cystic fibrosis, or aspiration — the complication is the progressive lung damage and bronchiectasis that follows a diagnosis delayed by an "asthma" label. The treatment complications are the small, largely transient growth effect of inhaled corticosteroid seen in PEAK and Ducharme's trial, and the adverse effects of repeated courses of oral steroid given reflexively for viral wheeze that does not need them. [4] [5] [8]
The pitfalls are predictable and examinable. The first is diagnostic: labelling every wheezy preschooler "asthmatic" and thereby both over-treating the transient viral wheezer and missing the red-flag child. The second is therapeutic: continuing or escalating an inhaled or oral steroid that has never been shown to help this particular child, when the evidence says its benefit in non-atopic viral wheeze is modest at best. The third is technical: attributing a controller "failure" to inadequate drug when the real problem is poor spacer technique, poor adherence, or ongoing tobacco-smoke exposure. [4] [8] [9]
Prognosis & Disposition
The prognosis of recurrent preschool wheeze is, for most children, excellent, and this is the single most reassuring and most important message for families. The Tucson cohort showed that transient early wheeze — the largest group — resolves by school age as the airways grow, and that most preschool wheeze does not become asthma. The prognostic pivot is atopy: the child with a positive Asthma Predictive Index, eczema, allergic sensitisation, and interval symptoms is the one at real risk of persistent, school-age asthma, while the well-between-colds non-atopic child is highly likely to outgrow the problem. [1] [3]
Importantly, no treatment given in the preschool years has been shown to change this trajectory. The PEAK study established that even two years of daily inhaled corticosteroid in high-risk preschoolers did not alter the natural history once treatment stopped, which is why preventive therapy is framed to families as symptom control during a difficult phase rather than as a disease-modifying cure. This honesty prevents both false hope and unnecessary long-term treatment. [4] [7]
Disposition is mostly to primary and general paediatric care with structured review, a written action plan, and clear escalation advice. Referral to a paediatric respiratory service is reserved for diagnostic doubt, red-flag features, severe or frequent attacks, poor response to a properly delivered trial of treatment, or failure to thrive — the same triggers that prompt investigation for a mimic. The acutely severe child is disposed by response, from home with a plan to admission to intensive care. [2] [9]
Special Populations
The child exposed to household tobacco smoke is the first special population because the exposure is both common and modifiable, and it worsens every aspect of wheeze. The most effective single intervention for such a child is not a new inhaler but supported smoking cessation for the caregivers and a smoke-free home and car, and this advice belongs in every consultation. The evidence that environmental smoke drives wheeze frequency and severity makes this a core, not optional, part of management. [2] [9]
Aboriginal and Torres Strait Islander children in Australia, and Māori and Pacific children in New Zealand, carry a disproportionate burden of chronic respiratory disease, protracted bacterial bronchitis, and bronchiectasis, and this changes the assessment of a preschool "wheeze". In these children, and in any child from a background of socioeconomic disadvantage or crowded housing, a chronic wet cough must not be dismissed as wheeze, and the threshold for investigating for a suppurative process and for arranging respiratory follow-up is deliberately lower. [9]
The former premature infant and the child with chronic neonatal lung disease are a third group. Their wheeze often reflects small, structurally altered airways rather than atopic asthma, tends to be episodic and viral, and usually improves with airway growth, so bronchodilators may help acute episodes but daily inhaled steroid is frequently unhelpful. Recognising the mechanism prevents both over-treatment and the mislabelling of a mechanical problem as asthma. [1] [2]
Evidence, Guidelines & Regional Differences
The evidence base is unusually well defined for a paediatric respiratory topic and is built from a small set of pivotal studies. The framing comes from the Tucson study of Martinez and colleagues, which established the wheeze phenotypes and their natural history, and from the European Respiratory Society Task Force of Brand and colleagues, updated in 2014, which gave the episodic-versus-multiple-trigger classification and its caveats. The risk-prediction tool is the Asthma Predictive Index of Castro-Rodríguez and colleagues. [1] [2] [3] [9]
The pharmacological evidence is a series of randomised trials that a candidate should be able to name and summarise. PEAK (Guilbert) showed daily inhaled corticosteroid controls but does not modify the disease; Ducharme showed pre-emptive high-dose inhaled steroid reduces rescue oral steroid at a small growth cost; Bacharier showed episodic inhaled steroid and montelukast give only modest benefit; MIST (Zeiger) showed intermittent and daily budesonide are broadly comparable for exacerbations; and Panickar showed oral prednisolone does not shorten admission for mild-to-moderate viral wheeze. Together they justify a phenotype-matched, trial-based, evidence-tempered approach rather than treating every preschool wheezer as an asthmatic. [4] [5] [6] [7] [8]
[1] [4] [8]Across Australia, New Zealand, the United Kingdom and Europe the consensus is the same in principle: classify the phenotype, avoid the premature 'asthma' label, treat acute attacks by severity, and offer preventive therapy only as a monitored trial matched to the atopic phenotype. Australian and New Zealand guidance and the British and ERS approaches all emphasise the weak evidence for daily controllers in non-atopic viral wheeze and the central place of tobacco-smoke elimination and inhaler technique. The regionally distinctive issue in ANZ is the higher burden of chronic wet cough and bronchiectasis in Aboriginal, Torres Strait Islander, Māori and Pacific children, which lowers the threshold to investigate a wheeze that does not behave like simple preschool wheeze. [2] [9]
Exam Pearls
Preschool wheeze — 'WHEEZY' checklist
References
- [1]Martinez FD; Wright AL; Taussig LM; Holberg CJ; Halonen M; Morgan WJ Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N Engl J Med, 1995.PMID 7800004
- [2]Brand PL; Baraldi E; Bisgaard H; Boner AL; Castro-Rodriguez JA; Custovic A; et al Definition, assessment and treatment of wheezing disorders in preschool children: an evidence-based approach. Eur Respir J, 2008.PMID 18827155
- [3]Castro-Rodríguez JA; Holberg CJ; Wright AL; Martinez FD A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med, 2000.PMID 11029352
- [4]Guilbert TW; Morgan WJ; Zeiger RS; Mauger DT; Boehmer SJ; Szefler SJ; et al Long-term inhaled corticosteroids in preschool children at high risk for asthma. N Engl J Med, 2006.PMID 16687711
- [5]Ducharme FM; Lemire C; Noya FJ; Davis GM; Alos N; Leblond H; et al Preemptive use of high-dose fluticasone for virus-induced wheezing in young children. N Engl J Med, 2009.PMID 19164187
- [6]Bacharier LB; Phillips BR; Zeiger RS; Szefler SJ; Martinez FD; Lemanske RF Jr; et al Episodic use of an inhaled corticosteroid or leukotriene receptor antagonist in preschool children with moderate-to-severe intermittent wheezing. J Allergy Clin Immunol, 2008.PMID 18973936
- [7]Zeiger RS; Mauger D; Bacharier LB; Guilbert TW; Martinez FD; Lemanske RF Jr; et al Daily or intermittent budesonide in preschool children with recurrent wheezing. N Engl J Med, 2011.PMID 22111718
- [8]Panickar J; Lakhanpaul M; Lambert PC; Kenia P; Stephenson T; Smyth A; et al Oral prednisolone for preschool children with acute virus-induced wheezing. N Engl J Med, 2009.PMID 19164186
- [9]Brand PL; Caudri D; Eber E; Gaillard EA; Garcia-Marcos L; Hedlin G; et al Classification and pharmacological treatment of preschool wheezing: changes since 2008. Eur Respir J, 2014.PMID 24525447