Paeds · respiratory-sleep-and-airway
Respiratory distress and failure in children
Also known as Paediatric respiratory distress · Acute respiratory failure in children · Increased work of breathing · Impending respiratory arrest · Hypoxaemic and hypercapnic respiratory failure
A fellowship approach to the child in respiratory distress and failure: recognise the continuum from compensated increased work of breathing to exhaustion, clear the pre-arrest threat gate, localise the cause to airway, lung, pump or drive, distinguish type 1 from type 2 failure, and escalate oxygen and support from low-flow through high-flow nasal cannula, CPAP and mechanical ventilation while treating the cause.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A toddler arrives grunting, nostrils flaring, ribs sucking in with every breath, and oxygen saturations of 88 per cent. Beside the trolley, a mother says her older child "has gone quiet" after an hour of laboured breathing. Both children are in trouble, but the quiet one may be closer to arrest. Reading that difference — rising effort versus failing effort — is the core skill this page teaches. [1] [12]
This hub owns the presentation logic for the child who cannot breathe well enough. Sister pages carry the disease-specific algorithms: acute severe asthma, bronchiolitis, croup and upper-airway obstruction, community-acquired pneumonia, and paediatric acute respiratory distress syndrome. [2] [6]
W.O.R.K. D.O.W.N.
Overview & Definition
Watch a well child breathe and you see almost nothing: quiet, effortless, regular. Respiratory distress is the visible extra effort a child recruits when that quiet breathing is no longer enough — you can see it from the end of the bed as tachypnoea, chest recession, nasal flaring, head-bobbing, tracheal tug, and grunting. The child is telling you their gas exchange is under threat and they are paying for it in muscle work. [1]
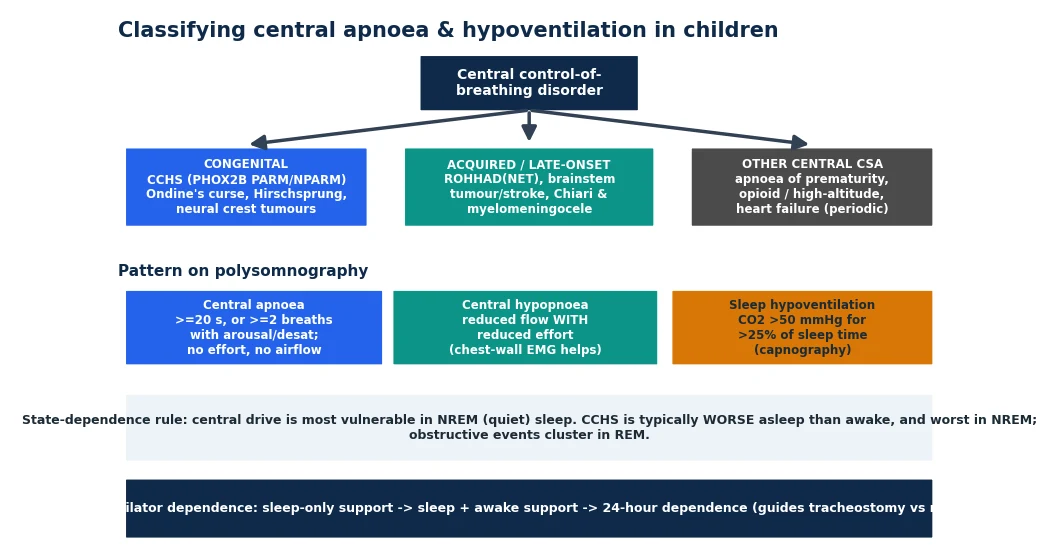
Respiratory failure is the point where the effort no longer succeeds. Defined physiologically, it is inadequate gas exchange: hypoxaemia despite supplemental oxygen (type 1) or carbon dioxide retention with respiratory acidosis (type 2), and often both as a child tires. The clinical face of failure is not a blood gas number but a child whose effort is falling, whose chest is going quiet, and whose conscious level is slipping. [6] [8]
The single most important teaching point is the direction of travel. A child ramps up effort to compensate, and while effort is high they are buying time. When a previously tachypnoeic, working child settles into a slower rate with less recession and no clinical improvement, that is exhaustion — the pre-arrest phase — not recovery. Mistaking fatigue for improvement is a classic and dangerous error. [1] [11]
Classification
Sort the breathless child along two axes rather than memorising a long list. [1] [6]
By severity — distress that is compensated versus failure that is not. Compensated distress shows high effort with maintained saturations and a normal conscious state. Decompensation brings hypoxaemia, hypercapnia, and a change in behaviour or alertness. Pre-arrest features are falling effort, a silent chest, bradycardia, and gasping. This severity axis drives urgency. [1] [8]
By anatomical origin — where the problem lives. Upper-airway problems give stridor and a hoarse or barking voice. Lower-airway problems give wheeze and prolonged expiration. Lung-tissue problems give crackles, focal signs, and hypoxaemia. Pump-and-drive problems — neuromuscular weakness, chest-wall disease, or depressed central drive — give shallow, poor, or irregular effort. This origin axis drives the specific treatment. [6] [7]
Physiologists add the blood-gas classification. Type 1 failure is hypoxaemic with a low or normal carbon dioxide, typical of lung-tissue disease and pneumonia. Type 2 failure is hypercapnic, typical of severe airway obstruction, pump failure, or a tiring child. A child in severe asthma or bronchiolitis who starts to retain carbon dioxide has crossed from type 1 into type 2, and that shift signals fatigue. [6] [8]
Epidemiology & Risk Factors
Respiratory problems are the single most common reason children present acutely and the most common pathway to cardiac arrest in childhood. Unlike adults, whose arrests are usually primary cardiac events, children almost always arrest because breathing or circulation failed first — so the child who is recognised and supported while still in respiratory distress rarely reaches an arrest at all. This is why early recognition changes outcomes. [8] [11]
Age shapes both frequency and vulnerability. Infants have the highest burden of acute respiratory illness, driven by bronchiolitis and viral lower-respiratory infection, and they decompensate fastest because of their small airways and limited reserve. Franklin and colleagues studied thousands of infants with bronchiolitis needing oxygen, a scale that reflects how common this presentation is. [2] [3]
Certain children carry higher risk of progressing to failure: former preterm infants with chronic lung disease, children with congenital heart disease, those with neuromuscular disease or complex disability, the immunocompromised, and children already dependent on respiratory technology such as home ventilation or tracheostomy. Each group has less reserve and a lower threshold for escalation. [6] [7]
Social and system factors matter too. Delayed presentation, incomplete immunisation, crowded housing, tobacco-smoke exposure, and remote location all increase severity at arrival and the time to definitive support. Indigenous children in Australia and New Zealand carry a disproportionate burden of severe respiratory infection, which reflects inequity rather than biology and demands a lower threshold for assessment and admission. [8] [12]
Pathophysiology
Children are built to fail their breathing faster than adults, and the reasons are structural. Their airways are small in radius, and because resistance to airflow rises steeply as a tube narrows, a few millimetres of mucosal oedema that an adult would shrug off can double or quadruple the work of breathing in an infant. This is why bronchiolitis and croup hit the youngest hardest. [3] [6]
The chest wall works against them. A young child's ribs are cartilaginous and horizontal, so instead of expanding the chest efficiently, hard inspiratory effort pulls the compliant wall inward as recession. Effort is spent on movement that does not translate into tidal volume, and the diaphragm — with fewer fatigue-resistant fibres than an adult's — tires quickly under that load. [1] [7]
Metabolic demand compounds the problem. Children consume more oxygen per kilogram than adults and hold less oxygen in reserve because their functional residual capacity is small relative to that demand. When breathing falters, saturations fall fast, and the buffer between "working hard" and "dangerously hypoxaemic" is short. [6] [8]
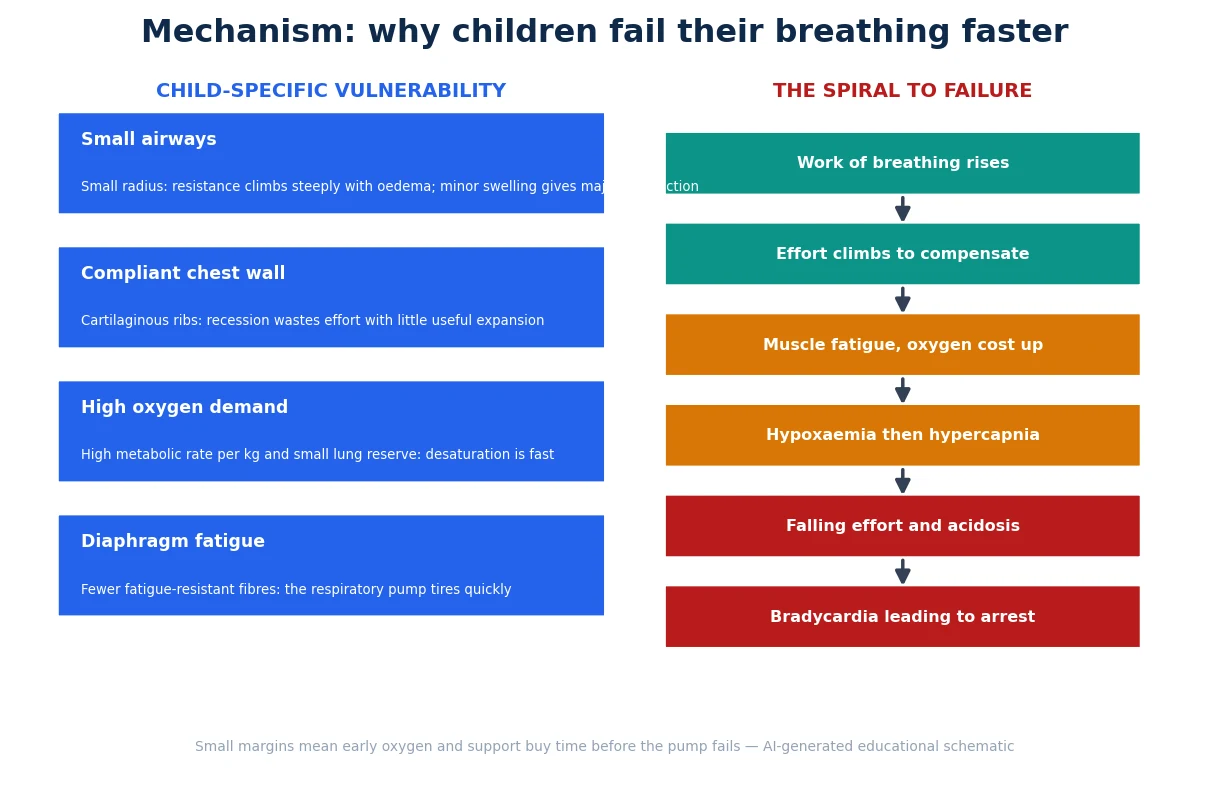
Put these together and you get the spiral to failure. Rising work of breathing compensates at first, but the muscle cost and oxygen consumption of that effort climb. As the child tires, alveolar ventilation falls, carbon dioxide rises, and hypoxaemia deepens. Acidosis and hypoxaemia then depress the myocardium and the respiratory drive, effort falls, and bradycardia announces an imminent hypoxic arrest. [6] [8]
The lung-tissue pathway has its own mechanism. In pneumonia and paediatric acute respiratory distress syndrome, inflammation and fluid flood the alveoli, collapse lung units, and create shunt — blood passing lung that cannot oxygenate it — which is why these children stay hypoxaemic despite high inspired oxygen and benefit from positive airway pressure to recruit lung. [6] [7]
Clinical Presentation
The end-of-bed picture usually tells you most of the story before you touch the child. In compensated distress you see a child who is alert but working: breathing fast, nostrils flaring, ribs and sternum drawing in, perhaps a soft grunt at the end of each breath as they hold their own airway pressure. Head-bobbing in an infant and tracheal tug in the neck are visible signs of hard accessory-muscle use. [1] [6]
The sound of the breathing localises the lesion. Stridor, loudest in inspiration with a hoarse or barking quality, points to the upper airway. Wheeze, prolonged and expiratory, points to the lower airways. Crackles and focal reduction in air entry point to the lung tissue. A silent chest in a child who is clearly struggling is ominous — it means too little air is moving to make any sound. [6] [8]
As failure approaches, the picture changes and often looks deceptively calmer. The respiratory rate slows, recession lessens, and the child becomes drowsy, agitated, or difficult to rouse. Colour turns pale, mottled, or cyanosed. In infants, feeding stops and apnoeas may appear. These "quieter" signs are the most dangerous in the whole topic. [1] [12]
Certain presentations declare a specific and urgent cause: drooling with a tripod posture and stridor suggests critical upper-airway obstruction; sudden distress in a previously well toddler suggests inhaled foreign body; urticaria and stridor after an exposure suggest anaphylaxis; and shallow, weak breathing in a floppy child suggests a pump or drive problem. Each redirects the immediate plan. [8] [6]
Differential Diagnosis
Localise first, then list causes within each compartment. [6] [7]
Upper airway (stridor, hoarse or barking voice): croup, bacterial tracheitis, epiglottitis, inhaled foreign body, retropharyngeal abscess, anaphylaxis, and — in infants — laryngomalacia decompensating with intercurrent illness. These threaten to occlude a small airway and must not be agitated. [8]
Lower airway (wheeze, prolonged expiration): acute asthma, viral-induced wheeze, and bronchiolitis dominate, with inhaled foreign body as the mimic that must not be missed when wheeze is focal or of sudden onset. [2] [10]
Lung tissue (crackles, focal signs, hypoxaemia): pneumonia, paediatric acute respiratory distress syndrome, pulmonary oedema from cardiac failure, pleural effusion or empyema, and aspiration. These cause shunt and hypoxaemia that responds better to positive pressure than to oxygen alone. [6]
Pump and drive (poor, shallow, irregular effort): neuromuscular weakness such as spinal muscular atrophy or Guillain–Barré syndrome, chest-wall or diaphragmatic problems, raised intracranial pressure or poisoning depressing central drive, and metabolic acidosis driving compensatory tachypnoea. Do not forget the non-respiratory causes of fast breathing: sepsis, diabetic ketoacidosis, and shock. [8] [9]
A febrile, tachypnoeic, poorly perfused child may be in respiratory failure, septic shock, or both, and the paediatric sepsis criteria remind us that respiratory dysfunction is a core organ-failure domain. Keep sepsis on the list whenever distress is out of proportion to the chest findings. [8] [9]
Clinical & Bedside Assessment
1. First impression before you touch. Use a rapid triangle: appearance and interaction, work of breathing, and circulation to skin. A child who is quiet, floppy, or poorly interactive despite obvious illness is high-risk. This first glance decides how fast you move. [1] [12]
2. Threat gate. Ask immediately whether this is pre-arrest: apnoea or gasping, a silent chest, bradycardia, exhaustion, or hypoxaemia that does not lift with high-concentration oxygen. Any of these means call for help, open the airway, and support ventilation with a bag and mask now. [8]
3. Work, efficacy, and effect. Assess the work of breathing (rate, recession, flaring, grunting, accessory muscles), then its efficacy (air entry, chest expansion, oxygen saturation), then its effect on the child (heart rate, skin colour, and conscious state). Effect signs tell you whether the effort is winning. [1] [6]
4. Measure against age-normal ranges. Interpret respiratory and heart rate against the age-specific ranges Fleming and colleagues established across birth to 18 years, because a "normal" adult rate can be dangerously slow for an infant, and a falling rate in a sick child is a warning. [1]
5. Localise by sound. Stridor, wheeze, crackles, or a silent chest each point to a compartment and change the plan. Note the phase of the abnormal sound and whether it is present at rest. [6]
6. Targeted investigations at the bedside. Continuous pulse oximetry guides oxygen. A capillary or venous blood gas quantifies carbon dioxide and acidosis in the child who is failing, but never delay treatment to obtain one. Structured early-warning observations help teams recognise deterioration early. [8] [11]
7. Listen to the family. Parents who say their child is worse than the numbers suggest are frequently right; caregiver concern is independently associated with critical illness. Treat that concern as data and escalate your assessment rather than reassure on a single reading. [12]
Investigations
Investigations confirm severity, localise the cause, and guide escalation — they never replace the clinical decision to support a failing child. Continuous pulse oximetry is the first and most useful bedside test, and it should be interpreted against the target range for the underlying condition rather than a universal cut-off. [6] [8]
A blood gas is the key test in suspected failure. A rising carbon dioxide with a falling pH in a tiring child with asthma or bronchiolitis confirms type 2 failure and impending exhaustion. A normal or low carbon dioxide with severe hypoxaemia points to type 1 lung-tissue disease. Capillary or venous sampling is adequate for trend and carbon dioxide; do not delay resuscitation to obtain arterial access. [6] [8]
Chest imaging is directed, not routine. A chest radiograph helps when you suspect pneumonia, pneumothorax, effusion, foreign body, or paediatric acute respiratory distress syndrome, and PALICC-2 anchors the imaging and oxygenation criteria for that diagnosis. Point-of-care ultrasound increasingly supplements bedside assessment where expertise exists. [6]
Microbiology and bloods follow the suspected cause: viral respiratory panels in bronchiolitis, blood culture and inflammatory markers when sepsis or pneumonia is likely, and a full blood count and electrolytes in the sick child. In the child who is febrile and shocked, the sepsis pathway runs in parallel with respiratory support. [8] [9]
Escalation triggers to have in mind
Management — Resuscitation
When the threat gate is breached, stop investigating and start supporting. Open the airway with positioning and suction, and in the child who is not breathing adequately, deliver bag-mask ventilation with high-concentration oxygen — effective bag-mask ventilation is the single most important intervention and often reverses a hypoxic bradycardia before any drug or tube. [8]
Give oxygen early to every hypoxaemic or severely distressed child while you decide on the next step; the child who stays hypoxaemic on high-concentration oxygen has significant shunt and needs positive pressure. Support circulation in parallel, because respiratory failure and shock frequently coexist, and treat sepsis on its own time-critical pathway when the picture fits. [8] [9]
Prepare for intubation and mechanical ventilation when non-invasive measures fail, when the child cannot protect their airway, or when exhaustion is overtaking effort. Anticipate that a child with a small functional residual capacity desaturates fast during laryngoscopy, so pre-oxygenate well and have a plan for the difficult paediatric airway. State the intent and sequence rather than inventing drug doses you cannot source, and call for senior and anaesthetic or intensive-care help early. [7] [8]
Management — Definitive & Stepwise
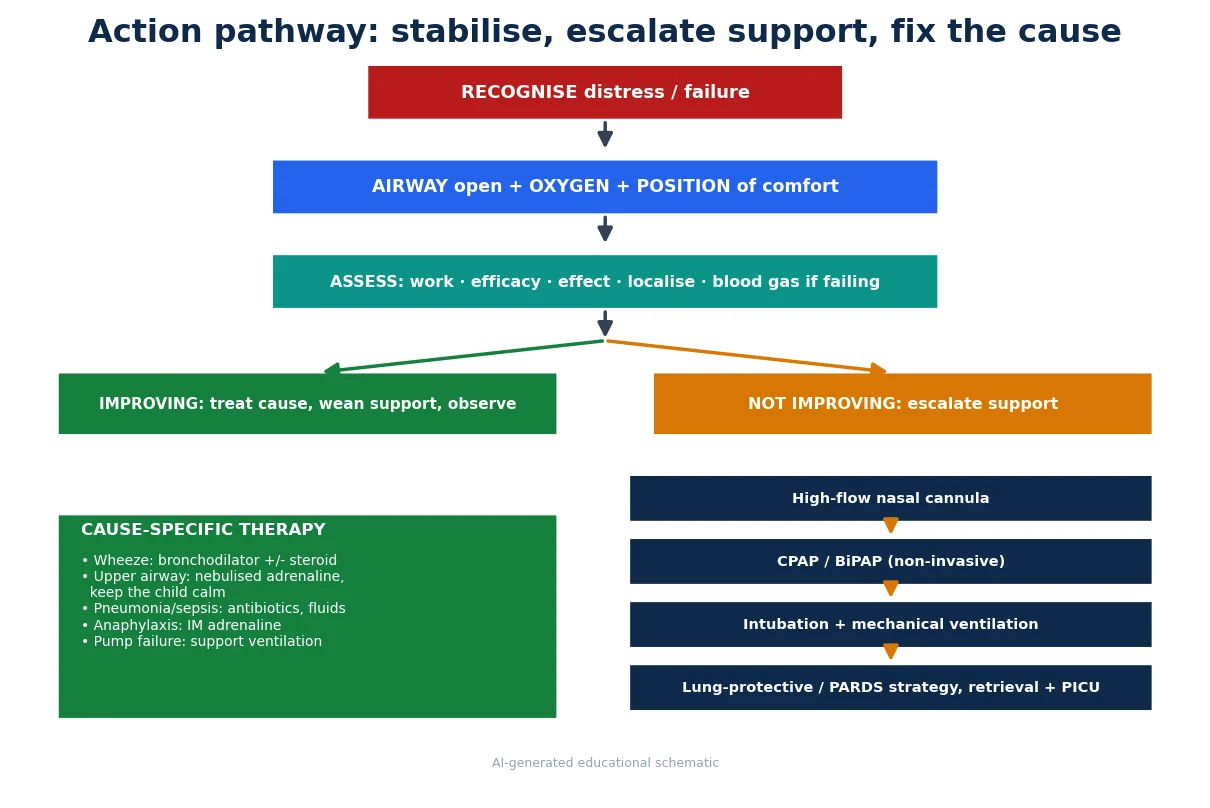
Step 1 — Open the airway and give oxygen. Position the child for comfort, keeping an anxious child with upper-airway obstruction calm on a parent's lap, and titrate oxygen to the target saturation for the condition. This first step buys time in every cause. [8]
Step 2 — Assess, localise, and decide the trajectory. Reassess work, efficacy, and effect after oxygen. A child who is improving gets cause-directed treatment, weaning, and observation. A child who is not improving climbs the support ladder. [1] [6]
Step 3 — High-flow nasal cannula. Heated, humidified high-flow oxygen is the usual first escalation for hypoxaemic infants and children, particularly in bronchiolitis. Franklin's trial showed high-flow reduces escalation of care compared with standard oxygen, and Kepreotes found similar benefit, though high-flow does not shorten the illness itself. It is a step on the ladder, not a cure. [2] [3]
Step 4 — Non-invasive ventilation (CPAP or BiPAP). When high-flow is not enough, continuous or bilevel positive pressure recruits lung and offloads the tiring pump. In young infants with bronchiolitis, the TRAMONTANE trial compared high-flow with nasal CPAP, and the FIRST-ABC trial compared high-flow with CPAP for acute illness in critical care; both inform how teams choose between modes rather than declaring one universally superior. [4] [5]
Step 5 — Intubation and lung-protective mechanical ventilation. When non-invasive support fails or the child cannot sustain or protect their breathing, intubate and ventilate. Use a lung-protective strategy with limited tidal volumes and appropriate positive end-expiratory pressure, following PEMVECC principles, and the PALICC-2 approach for paediatric acute respiratory distress syndrome. Escalate to retrieval and a paediatric intensive care unit when local capability is exceeded. [6] [7]
Step 6 — Treat the cause alongside the support. Bronchodilators and steroids for wheeze, with inhaled or intravenous magnesium sulfate considered in severe asthma; nebulised adrenaline and steroids for significant upper-airway obstruction; antibiotics and fluids for pneumonia and sepsis; and intramuscular adrenaline for anaphylaxis. Support keeps the child alive while cause-specific therapy fixes the problem. [10] [9]
Specific Subtypes & Scenarios
Infant with bronchiolitis and hypoxaemia. Oxygen to target, minimal handling, and high-flow nasal cannula as the usual escalation, with CPAP if high-flow fails. High-flow reduces treatment escalation but does not shorten the disease. [2] [3]
Child in acute severe asthma. Oxygen, inhaled bronchodilators, and systemic steroids, with escalation to intravenous therapy and magnesium sulfate for severe or life-threatening attacks. A rising carbon dioxide is a warning of fatigue, not a reassurance. [10]
Child with stridor and critical upper-airway obstruction. Keep the child calm and undisturbed, give oxygen and nebulised adrenaline, and involve senior airway help early; distressing the child can precipitate complete obstruction. [8]
Child with pneumonia and refractory hypoxaemia. Suspect shunt from consolidation or evolving paediatric acute respiratory distress syndrome; positive airway pressure recruits lung, and PALICC-2 guides diagnosis and ventilation. [6]
Floppy child with weak, shallow breathing. Think neuromuscular disease or depressed central drive; the pump is failing, so support ventilation and look for the underlying cause rather than expecting bronchodilators to help. [7]
Febrile, shocked, tachypnoeic child. Run the sepsis and respiratory pathways together; respiratory dysfunction is a core organ-failure domain in the paediatric sepsis criteria and the 2020 Surviving Sepsis Campaign paediatric guidelines. [8] [9]
Technology-dependent child (home ventilation or tracheostomy). First exclude a blocked or displaced tube or circuit, follow the family's emergency plan, and treat the intercurrent illness; parents and carers often read deterioration earliest. [7] [12]
Complications & Pitfalls
- Mistaking a falling respiratory rate and reducing effort for recovery when it signals exhaustion. [1]
- Waiting for a blood gas before treating an obviously failing child. [8]
- Distressing a child with critical upper-airway obstruction by lying them flat or examining the throat. [8]
- Treating focal or sudden-onset wheeze as asthma and missing an inhaled foreign body. [10]
- Assuming oxygen alone will fix hypoxaemia that is due to shunt and needs positive pressure. [6]
- Forgetting that sepsis, acidosis, and shock cause tachypnoea without primary lung disease. [9]
- Under-recognising deterioration in a child on a busy ward without structured early-warning observations. [11]
- Dismissing a caregiver's concern that the child is worse than the numbers suggest. [12]
Prognosis & Disposition
Most children in respiratory distress recover fully with oxygen, cause-specific treatment, and time, and the majority of infants with bronchiolitis or children with asthma who are recognised and supported early do well. The prognosis worsens sharply once true failure and hypoxic arrest occur, which is exactly why early recognition and stepwise escalation matter so much. [2] [8]
Disposition is capability-matched. A child improving on low-flow oxygen with a treatable cause can be managed on a ward with clear escalation criteria and structured observations. A child needing high-flow or non-invasive support needs a high-dependency environment, and a child who is intubated or has refractory hypoxaemia needs a paediatric intensive care unit, reached by retrieval if necessary. [5] [6]
Structured early-warning systems and clear review triggers reduce missed deterioration on the ward, and a documented plan of what to watch for and when to call helps the whole team respond in time. Handover should transfer the problem, the trajectory, the current support, and the residual risk. [11] [12]
Special Populations
Former preterm infants with chronic lung disease: less reserve, quicker desaturation, and a lower threshold for oxygen and escalation during intercurrent viral illness. [6]
Children with neuromuscular disease or complex disability: pump failure dominates, cough is weak, and secretions accumulate; support ventilation and airway clearance rather than expecting bronchodilators to help. [7]
Immunocompromised children: broaden the differential for the cause of respiratory failure and involve seniors early, because deterioration can be rapid and atypical. [8]
Technology-dependent children (home ventilation, tracheostomy): always exclude a tube or circuit problem first, and use the family's individualised emergency plan. [7]
Indigenous, rural, and remote families: higher burden of severe respiratory infection and longer transfer times mean a lower threshold for assessment, early retrieval activation, and culturally safe, family-centred care. [12]
Evidence, Guidelines & Regional Differences
Fleming and colleagues provide the age-specific respiratory and heart rate ranges that underpin every bedside judgement about whether a child's breathing is fast, normal, or ominously slow. [1]
The high-flow evidence base is now substantial. Franklin's large trial and Kepreotes' study established that high-flow nasal cannula reduces escalation of care in bronchiolitis without shortening the illness, positioning it as an early rung on the escalation ladder rather than a disease-modifying therapy. [2] [3]
How to choose between high-flow and CPAP is still being defined. The TRAMONTANE trial compared high-flow with nasal CPAP in young infants with bronchiolitis, and the FIRST-ABC trials compared high-flow with CPAP for acutely ill children in critical care, giving teams evidence to weigh comfort, failure rates, and resource use rather than a single mandated mode. [4] [5]
For the sickest lungs, PALICC-2 sets the contemporary definition and management of paediatric acute respiratory distress syndrome, and PEMVECC provides consensus principles for lung-protective mechanical ventilation in children. The paediatric sepsis criteria and the 2020 Surviving Sepsis Campaign paediatric guidelines frame respiratory dysfunction within organ failure and time-critical care. [6] [7] [8] [9]
In acute asthma, the Cochrane review of inhaled magnesium sulfate reflects the ongoing evaluation of adjuncts for severe attacks, and Parshuram's EPOCH trial tempered expectations that a single early-warning score alone reduces mortality, reminding us that recognition systems work only within a responsive team. [10] [11]
Australian and New Zealand practice follows ANZCOR paediatric advanced life support and widely used local guidelines such as those from the Royal Children's Hospital Melbourne, with strong rural and remote retrieval systems that shape time-to-support for the failing child. Care for Aboriginal and Torres Strait Islander, Māori, and Pasifika families must be culturally safe and family-centred, with a lower threshold for assessment given the higher burden of severe respiratory infection. [8] [12]
UK practice follows APLS structured assessment and NICE and BTS respiratory guidance, with paediatric early-warning scores embedded in ward observation. High-flow and non-invasive support are widely used, with escalation to regional paediatric intensive care and retrieval teams. [1] [11]
US practice follows PALS and AAP respiratory guidance, with high-flow nasal cannula and non-invasive ventilation established in emergency departments and wards and PALICC-2 informing paediatric acute respiratory distress syndrome care in intensive care. [2] [6]
Canadian paediatric practice aligns with PALS and CPS guidance, with the RCPSC EPAs anchoring recognition of the deteriorating child and communication with families, and provincial retrieval systems supporting rural and remote transfer. [8] [9]
Exam Pearls
- Respiratory distress and failure are one continuum; the trend in effort matters more than any single number. [1]
- A falling respiratory rate and reducing effort without improvement mean exhaustion and impending arrest, not recovery. [8]
- Type 1 failure is hypoxaemic; type 2 is hypercapnic; a tiring obstructed child slides from type 1 into type 2. [6]
- Localise by sound: stridor is upper airway, wheeze is lower airway, crackles are lung tissue, poor effort is pump or drive. [6]
- Effective bag-mask ventilation reverses most paediatric hypoxic bradycardias before any drug. [8]
- High-flow nasal cannula reduces escalation in bronchiolitis but does not shorten the illness. [2] [3]
- Positive airway pressure, not more oxygen, treats hypoxaemia driven by shunt in pneumonia and PARDS. [6]
- A silent chest in a working child means too little air is moving to make a sound. [8]
- Caregiver concern is independently associated with critical illness — treat it as data. [12]
One-line viva opener
"I treat distress and failure as a continuum: I clear the pre-arrest threat gate first, give oxygen, and read the trend in the child's effort. If effort is rising they are compensating; if it is falling with a quieter chest and a drowsier child they are failing, and I escalate through high-flow, non-invasive support, and intubation while I localise and treat the cause." [1] [6] [8]
References
- [1]Fleming S Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet, 2011.PMID 21411136
- [2]Franklin D A Randomized Trial of High-Flow Oxygen Therapy in Infants with Bronchiolitis. N Engl J Med, 2018.PMID 29562151
- [3]Kepreotes E High-flow warm humidified oxygen versus standard low-flow nasal cannula oxygen for moderate bronchiolitis (HFWHO RCT): an open, phase 4, randomised controlled trial. Lancet, 2017.PMID 28161016
- [4]Milési C High flow nasal cannula (HFNC) versus nasal continuous positive airway pressure (nCPAP) for the initial respiratory management of acute viral bronchiolitis in young infants: a multicenter randomized controlled trial (TRAMONTANE study). Intensive Care Med, 2017.PMID 28124736
- [5]Ramnarayan P Effect of High-Flow Nasal Cannula Therapy vs Continuous Positive Airway Pressure Therapy on Liberation From Respiratory Support in Acutely Ill Children Admitted to Pediatric Critical Care Units: A Randomized Clinical Trial. JAMA, 2022.PMID 35707984
- [6]Emeriaud G Executive Summary of the Second International Guidelines for the Diagnosis and Management of Pediatric Acute Respiratory Distress Syndrome (PALICC-2). Pediatr Crit Care Med, 2023.PMID 36661420
- [7]Kneyber MCJ Recommendations for mechanical ventilation of critically ill children from the Paediatric Mechanical Ventilation Consensus Conference (PEMVECC). Intensive Care Med, 2017.PMID 28936698
- [8]Schlapbach LJ International Consensus Criteria for Pediatric Sepsis and Septic Shock. JAMA, 2024.PMID 38245889
- [9]Weiss SL Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026. Pediatr Crit Care Med, 2026.PMID 41869844
- [10]Knightly R Inhaled magnesium sulfate in the treatment of acute asthma. Cochrane Database Syst Rev, 2017.PMID 29182799
- [11]Parshuram CS Effect of a Pediatric Early Warning System on All-Cause Mortality in Hospitalized Pediatric Patients: The EPOCH Randomized Clinical Trial. JAMA, 2018.PMID 29486493
- [12]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. Lancet Child Adolesc Health, 2025.PMID 40451224