Paeds · respiratory-sleep-and-airway
Spirometry and paediatric pulmonary-function testing
Also known as Spirometry and paediatric pulmonary-function testing · Paediatric lung function testing · Spirometry in children · Pulmonary function tests in children · Flow-volume loop interpretation · Bronchodilator reversibility testing
Fellowship guide to spirometry and pulmonary-function testing in children: how a forced blow into a spirometer generates the FEV1, FVC and their ratio and the flow-volume loop, how the ratio below the lower limit of normal defines obstruction and a low FVC with a preserved ratio raises restriction that lung volumes confirm, how bronchodilator responsiveness is measured and read, why the Global Lung Function Initiative reference equations and z-scores have replaced fixed cut-offs and percent-predicted, how quality is judged against ATS/ERS acceptability and repeatability standards, and how the whole result is interpreted in the child sitting in front of you rather than in isolation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child takes the deepest breath they can, seals their lips around a mouthpiece, and blasts the air out as hard and as long as they can manage. That single forced manoeuvre is spirometry, and from it come the three numbers that anchor almost every lung-function report: the total volume blown out, called the forced vital capacity or FVC; the volume blown out in the first second, the FEV1; and the ratio of the two, FEV1/FVC, which describes how quickly the lungs can empty. The machine also plots the effort as a flow-volume loop, whose shape tells the practised eye as much as the numbers. [1] [7]
Spirometry is only the most familiar member of a wider family of pulmonary-function tests. When spirometry cannot answer the question, the laboratory can measure absolute lung volumes to look for true restriction, the diffusing capacity to probe gas transfer, airway resistance by oscillometry, and airway responsiveness to a bronchodilator or a challenge agent. The purpose of all of them is the same — to turn a child's breathing into reproducible numbers that can be compared with healthy children of the same size and read over time. [2] [6]
Classification
The first fork in every interpretation is set by the FEV1/FVC ratio, because it separates the two great families of abnormality. When the ratio falls below the lower limit of normal for the child's size, the lungs are emptying too slowly and the pattern is obstructive — the picture of asthma, cystic fibrosis and other airway diseases. When the ratio is normal or high but the FVC is reduced, air is not being trapped but the lungs may be small or stiff, and the pattern is restrictive, though spirometry can only raise the suspicion. [6] [2]
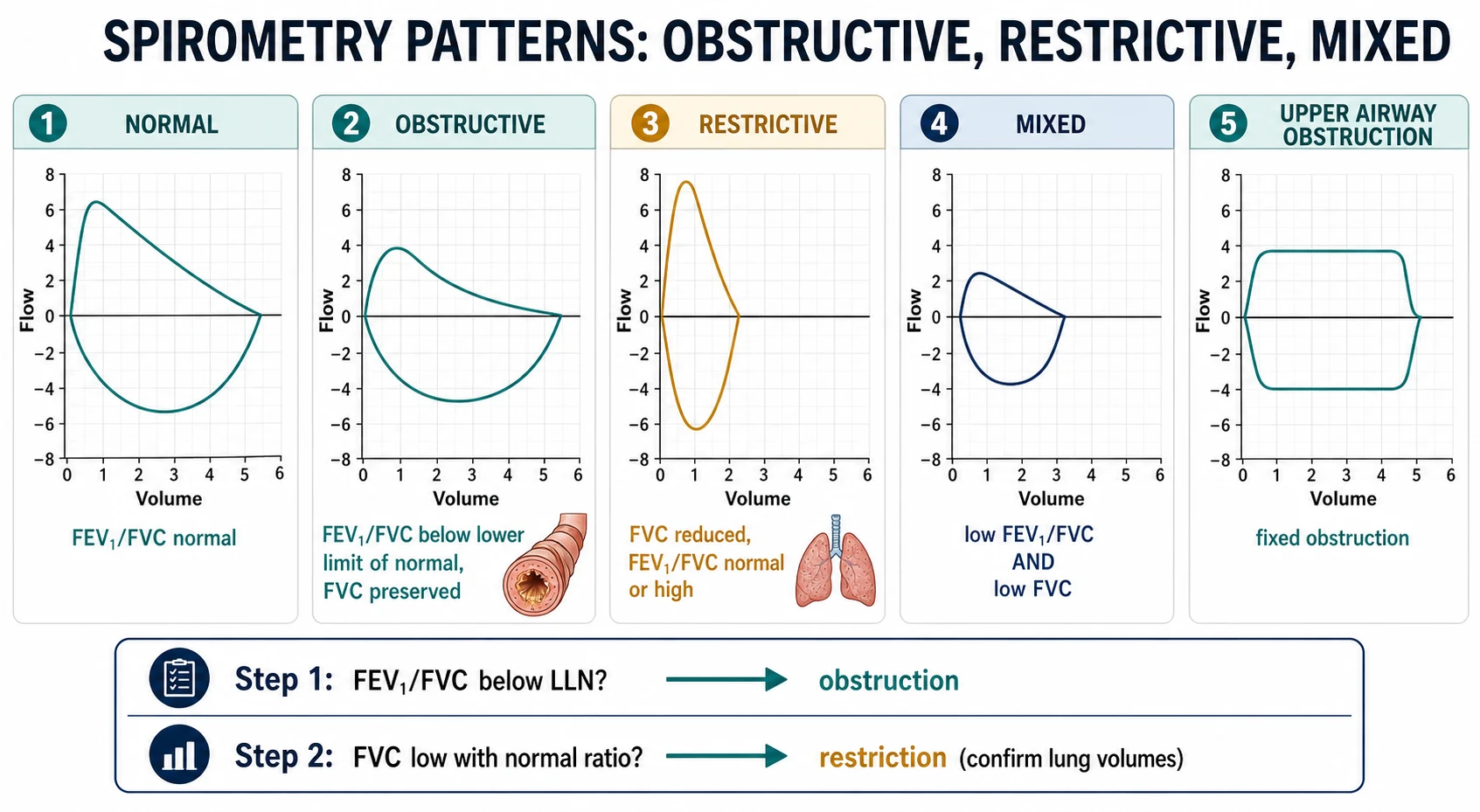
A third, mixed pattern shows both a low ratio and a low FVC, and it should prompt lung-volume measurement to disentangle how much of the reduced FVC is genuine restriction and how much is gas trapped behind obstructed airways. Beyond these, the flow-volume loop itself defines a distinctive category: a flattening of the inspiratory or expiratory limb into a plateau points to large- or upper-airway obstruction, such as a subglottic stenosis or a vascular ring, rather than to diffuse small-airway disease. [6] [2]
[6]Epidemiology & Risk Factors
Whether a child can produce a usable test depends far more on age and coaching than on any disease. Most children can perform acceptable, repeatable spirometry from about six years of age, and many from five with skilled encouragement; below that, the forced manoeuvre is developmentally beyond them, which is why preschool testing needs adapted techniques and age-specific standards. Feasibility rises steadily through the school years, so the same request that fails in a four-year-old succeeds routinely in a nine-year-old. [5] [1]
The demand for testing is driven by the conditions it monitors, and in Australia and New Zealand that burden is unevenly shared. Asthma is the commonest reason a child meets a spirometer, and cystic fibrosis, bronchiectasis — including the high rates in Aboriginal, Torres Strait Islander and Māori and Pacific children — neuromuscular disease and chest-wall disorders all generate longitudinal testing. The children who most need reliable monitoring are often those with the least access to a laboratory, which shapes both the epidemiology and the equity of lung-function care. [4] [10]
The main risk factors are not for a disease but for a misleading test. A poorly coached or unwell child, a technician unfamiliar with children, equipment that is not calibrated, and — above all — the use of an inappropriate reference equation all threaten the validity of the result. Applying an adult fixed ratio, or a reference set that does not match the child's ancestry, systematically distorts interpretation and is a recognised source of both over- and under-diagnosis. [3] [8]
Pathophysiology
The physiology that makes spirometry work is the phenomenon of expiratory flow limitation. At the very start of a forced blow the flow depends on how hard the child pushes, so the sharp early peak of the flow-volume loop is effort-dependent. Within a fraction of a second, however, the rising pressure inside the chest compresses the airways at a point where the pressures inside and outside the airway are equal, and beyond that point extra effort no longer increases flow. The descending limb of the loop is therefore effort-independent and reflects the calibre and elastic properties of the airways themselves. [7] [1]
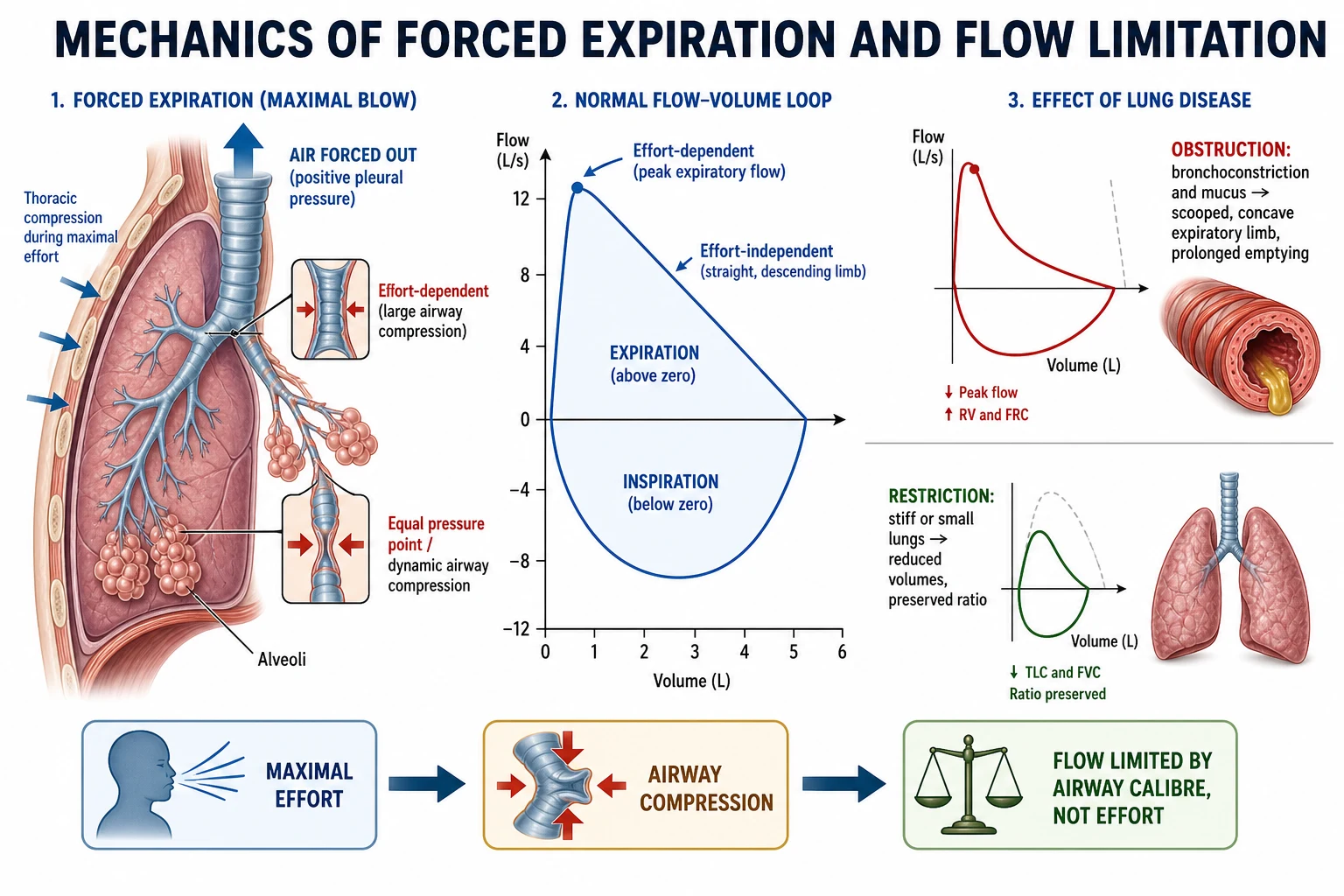
Obstruction acts on this effort-independent limb. When airways are narrowed by bronchoconstriction, mucosal swelling, secretions or scarring, the flow at any given lung volume falls and emptying is prolonged, so the FEV1 drops more than the FVC and the ratio falls; the expiratory limb of the loop becomes concave or scooped, the hallmark of small-airway disease. Because emptying is slow, air can be trapped behind closing airways, so the FVC measured by spirometry may itself fall even though the total lung capacity is normal or high. [6] [2]
Restriction works differently. Here the airways conduct air normally but the volume available to exhale is reduced, whether because the lungs are small, stiff, or compressed by a chest-wall or neuromuscular problem. Both FEV1 and FVC shrink in step, the ratio is preserved or high, and the loop keeps its normal shape at a smaller scale. Because spirometry cannot see the air left in the chest at the end of a breath, it cannot measure the total lung capacity, and so it can only suggest — never prove — that a small FVC is due to genuine restriction. [6] [9]
Clinical Presentation
Spirometry does not present with symptoms; it presents as a report, and learning to read that report is the clinical skill. The obstructive report shows a reduced FEV1/FVC ratio and a scooped expiratory loop, and it belongs to the child with wheeze, cough or breathlessness whose airways are narrowed — most often in asthma, where the test may also reveal reversibility after a bronchodilator. The magnitude of the fall in FEV1, expressed against the child's own predicted value, grades how severe the obstruction is at that moment. [10] [6]
The restrictive-pattern report shows a reduced FVC with a preserved ratio and a small but normally shaped loop, and it accompanies the child with a stiff or small lung, a deformed chest wall, or weak respiratory muscles. Here the practitioner's task is to recognise that spirometry has only raised a possibility and to arrange the lung-volume study that confirms or refutes it. A flattened loop, by contrast, is the presentation of large-airway or upper-airway obstruction and points the assessment toward the trachea and larynx. [6] [2]
[6]A crucial part of the presentation is the normal test in a symptomatic child. Lung function is often entirely normal between episodes of asthma or exercise-induced symptoms, so a normal spirometry can never exclude these diagnoses; it simply means the airways are open at that moment. The correct response to a normal test in a symptomatic child is to consider reversibility testing on a different day or a bronchial challenge, not to reassure the family that nothing is wrong. [10] [12]
Differential Diagnosis
The differential in spirometry is the differential of the abnormal pattern itself. A low FEV1/FVC ratio means airflow obstruction, and the differential then spans asthma, cystic fibrosis, bronchiectasis, post-infectious bronchiolitis obliterans and, rarely, congenital airway disease; the history, the bronchodilator response and the wider workup separate them. What matters at the level of the test is to confirm the obstruction is real by checking that the effort was maximal and the FVC fully exhaled, because an early stop mimics both a low ratio and a low FVC. [6] [1]
The more treacherous differential surrounds the reduced FVC. Far more often than true restriction, a low FVC reflects submaximal effort, an early termination of the blow, or air trapped behind obstructed airways so that the child simply cannot get it all out in the time available. Distinguishing genuine restriction from these artefacts and from obstruction-with-trapping is precisely why a reduced FVC on spirometry mandates lung-volume measurement rather than a diagnostic label. [2] [9]
The flattened flow-volume loop generates its own differential of fixed and variable large-airway lesions — subglottic stenosis, an external vascular ring, an intraluminal mass, tracheomalacia or vocal-cord dysfunction — distinguished by whether the inspiratory limb, the expiratory limb, or both are affected. Recognising that the loop shape, rather than the FEV1 and FVC alone, is abnormal is what redirects the assessment away from asthma and toward imaging and endoscopy of the central airway. [6] [2]
Clinical & Bedside Assessment
Good spirometry begins before the child blows. The technician measures standing height accurately, because the reference values depend heavily on it, records age, sex and ancestry, and checks that the child has withheld bronchodilators for the appropriate interval if reversibility is being assessed. The manoeuvre is then demonstrated and coached with energy and, for younger children, with incentive animations that turn the forced blow into a game of blowing out candles or knocking down a target. [1] [8]
The forced expiratory manoeuvre itself has a defined anatomy that the assessor watches for in real time: a maximal inspiration to full lungs, a sharp explosive start with no hesitation, a blast that continues smoothly without coughing or a second breath, and an expiration prolonged until the child can give no more. The technician judges each effort against the ATS/ERS acceptability criteria as it happens, coaching the child to a better attempt rather than simply collecting whatever comes. [1] [7]
Performing and judging a paediatric forced expiratory manoeuvre
Measure standing height and record age, sex and ancestry, since these drive the reference values
Demonstrate and coach the manoeuvre, using incentive displays for younger children
Have the child inhale fully to total lung capacity with no pause before blowing
Coach a sharp, explosive start with minimal back-extrapolated volume and no hesitation
Encourage a smooth, cough-free blast prolonged to a clear end-of-test plateau
Judge each effort against ATS/ERS acceptability, and collect enough efforts for repeatability
Acceptability and repeatability are then formalised. An acceptable effort has a good start with a small back-extrapolated volume, no cough in the first second, no early termination and no leak or obstructed mouthpiece; repeatability requires that the two largest values for FVC and for FEV1 agree closely, within a defined margin that is tighter for small children. Only when these standards are met should the values be reported, and modern reports grade the quality explicitly so the reader knows how much to trust the numbers. [1] [8]
Investigations
Spirometry is the first investigation, and it is often extended in the same visit by bronchodilator reversibility testing. Baseline spirometry is followed by an inhaled bronchodilator, and spirometry is repeated after a short interval to see whether the obstruction improves; a meaningful increase supports variable airflow obstruction and, in the right context, asthma. The 2022 interpretive standard expresses a significant response as a change in FEV1 or FVC of more than ten percent of the predicted value, a definition designed to be fairer across body sizes than the older threshold of a twelve-percent rise from the child's own baseline. [2] [10]
Salbutamol (bronchodilator reversibility testing)
Loading dose
Give 400 micrograms of salbutamol (for example four separate actuations of a 100-microgram metered-dose inhaler, each inhaled through a spacer) after baseline spirometry
Maintenance dose
Repeat spirometry 10 to 15 minutes later and compare; a rise in FEV1 or FVC of more than ten percent of predicted is a significant bronchodilator response under the 2022 standard
When spirometry raises restriction or cannot explain the picture, the laboratory adds static lung volumes measured by body plethysmography or gas dilution, which quantify the total lung capacity and residual volume and so confirm or refute true restriction and reveal hyperinflation and air trapping. The diffusing capacity for carbon monoxide probes the gas-exchange surface, and airway responsiveness can be formally tested with a bronchial challenge when reversibility is equivocal but the suspicion of asthma remains. [9] [6]
[6]The interpretation of every one of these tests now rests on the Global Lung Function Initiative reference equations, which convert a raw value into a z-score against healthy people of the same age, height, sex and ethnicity. A z-score expresses how many standard deviations the child sits from the predicted mean, and the lower limit of normal is set at the fifth percentile, a z-score of about minus 1.64. Oscillometry offers a tidal-breathing alternative in children too young for a forced manoeuvre, and it correlates usefully with spirometry in wheezy children. [3] [11]
Management — Resuscitation
Spirometry is a safe test, but the forced manoeuvre and the challenges built around it can occasionally provoke trouble, and the laboratory must be prepared to respond. The most important acute event is bronchospasm — a child with reactive airways can wheeze and desaturate after repeated maximal efforts or, more so, after a bronchial challenge — and the response is to stop testing, sit the child up, give inhaled salbutamol and oxygen if needed, and treat a significant fall as an acute asthma exacerbation rather than a testing hiccup. [1] [10]
The other events are mechanical and self-limiting. Repeated maximal expirations can cause light-headedness or, rarely, cough syncope, so a child who feels faint should be allowed to sit and recover before another attempt, and testing should pause. Recognising the small number of genuine contraindications, and having salbutamol, a spacer and oxygen to hand, converts these events from emergencies into managed incidents and is the resuscitation-level skill the setting demands. [1] [7]
Management — Definitive & Stepwise
The definitive management of a spirometry result is its correct interpretation, and that follows a fixed order every time. Quality comes first: confirm the effort was acceptable and repeatable, because an unacceptable test is not interpreted at all but repeated. Next comes the FEV1/FVC ratio, read against the lower limit of normal to decide whether obstruction is present. Then the FVC is examined, and a reduction with a preserved ratio triggers lung-volume measurement before restriction is accepted. [2] [6]
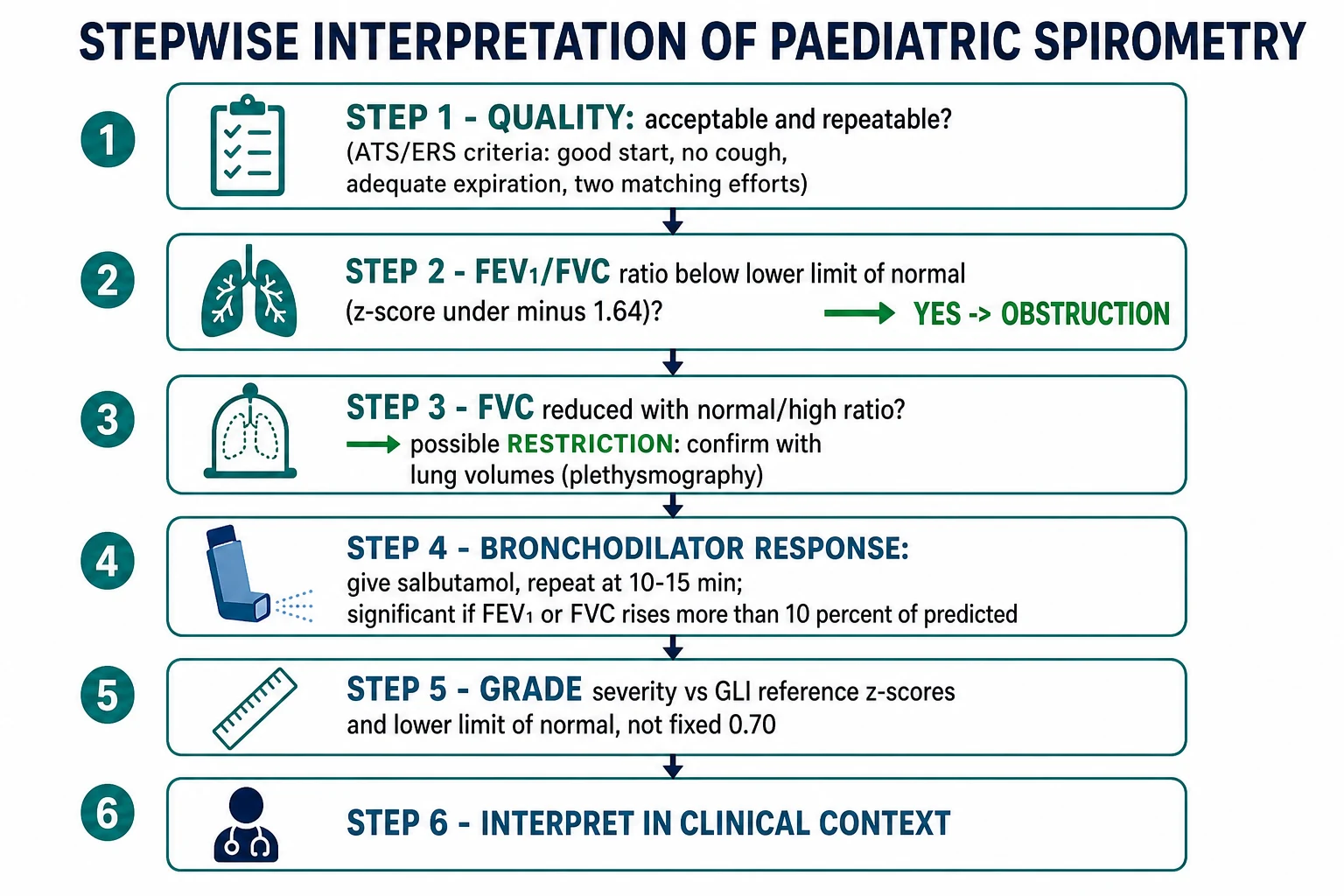
With the pattern established, severity is graded not by fixed percentages but by how far the FEV1 sits below predicted on the z-score scale, and reversibility is judged by the response to a bronchodilator. Crucially, the numbers are then placed against the child's own previous tests, because a value still within the normal range can represent a real decline from that child's personal best, and a longitudinal fall can matter more than a single cross-sectional result. This is the essence of monitoring in cystic fibrosis and chronic asthma. [2] [4]
Stepwise interpretation of a paediatric spirometry report
Confirm acceptability and repeatability; if the test is unacceptable, repeat rather than interpret
Read the FEV1/FVC ratio against the lower limit of normal — below it means obstruction
Examine the FVC; a reduction with a normal ratio prompts lung-volume testing for restriction
Assess bronchodilator response: a rise in FEV1 or FVC over ten percent of predicted is significant
Grade severity by the FEV1 z-score against GLI reference values, not a fixed cut-off
Compare with the child's own prior results to detect a real decline over time
Integrate the whole result with the history, examination and clinical question
The final and indispensable step is clinical integration. A spirometry result is a measurement, not a diagnosis, and its meaning comes only from the child in front of you — their symptoms, their examination, their trajectory and the question the test was meant to answer. The definitive management of the result is to use it to confirm, refute or grade a clinical hypothesis and to guide treatment, never to treat the number in isolation. [6] [12]
Specific Subtypes & Scenarios
Preschool spirometry is the scenario that most tests judgement, because children under six often cannot sustain the full second of forced expiration that the adult FEV1 assumes. The ATS/ERS preschool statement adapts the standards for this age — accepting shorter expiratory times and reporting values such as the FEV in half or three-quarters of a second — and it endorses tidal-breathing techniques like oscillometry and the interrupter resistance when a forced manoeuvre is impossible. The goal is a valid measurement appropriate to the child's development, not a failed attempt at an adult test. [5] [11]
The asthma-monitoring scenario is the everyday one. Spirometry with reversibility supports the diagnosis when it shows variable obstruction, contributes to grading severity and control, and tracks the child over years, though guidelines stress that a normal or non-reversible test never excludes asthma in a symptomatic child. In cystic fibrosis and bronchiectasis the same test is used longitudinally to detect decline early, which is why a fall from a child's personal best matters even when the absolute value looks acceptable. [10] [4]
[6]Neuromuscular disease gives a restrictive scenario with its own refinements: a falling FVC tracks progressive respiratory-muscle weakness, and comparing the FVC sitting and lying flat unmasks diaphragm weakness, which drops the supine value markedly. And the upper-airway scenario — the child with fixed or variable central-airway obstruction — is recognised not from the FEV1 and FVC but from the shape of the full inspiratory-and-expiratory loop, a reminder to inspect the loop and not only the table of numbers. [6] [2]
Complications & Pitfalls
The pitfalls of spirometry are almost all interpretive, and the first is applying adult rules to growing lungs. Using a fixed FEV1/FVC below 0.70 to define obstruction, or leaning on percent-predicted with an arbitrary eighty-percent cut-off, systematically over-diagnoses restriction and under-diagnoses obstruction in children, whose normal ratios are higher than adults' and change with growth. The z-score against the Global Lung Function Initiative equations avoids this, and abandoning fixed cut-offs is one of the most important shifts in modern interpretation. [2] [3]
The second cluster of pitfalls is about quality and effort. A submaximal blow, an early stop, a cough or a leak produces numbers that imitate disease, and reporting them without the quality grade invites error; the antidote is the discipline of acceptability and repeatability and an explicit statement of test quality on the report. Reading a reduced FVC as restriction without lung volumes, and misreading air trapping as restriction, belong to the same family of avoidable mistakes. [1] [8]
The third pitfall is choosing the wrong reference population. The Global Lung Function Initiative provides ethnicity-specific equations and a composite 'other' equation, and using a set that does not match a child's ancestry shifts every z-score and can create or hide abnormality. Awareness that reference choice is a clinical decision, not a default, and caution in applying equations to populations they were not derived from, guard against a subtle but systematic error. [3] [4]
Prognosis & Disposition
The value of spirometry lies less in any single result than in the trajectory it reveals over time, and this is where it most changes outcomes. In cystic fibrosis, asthma and other chronic lung diseases, serial FEV1 tracks the course of disease, flags decline that precedes symptoms, and guides escalation of treatment; a result that has fallen from a child's own personal best carries prognostic weight even when it remains inside the population's normal range. Longitudinal testing, not one-off measurement, is what informs prognosis. [4] [2]
Disposition after a test is set by the pattern and the clinical picture together. A normal, good-quality test in a child whose symptoms are mild and explained needs only routine follow-up; a clearly obstructive test with reversibility supports an asthma pathway and its controller treatment; and an unexplained restrictive pattern, a flattened loop, or an unexpected decline warrants referral to a paediatric respiratory service for lung volumes, imaging or endoscopy. The test rarely stands alone in deciding disposition, but it sharpens every such decision. [6] [12]
Special Populations
Ethnicity and the choice of reference equation form the most important special-population issue in paediatric lung function, and it is a live one in Australia and New Zealand. The Global Lung Function Initiative derived equations for several ancestral groups and a composite 'other' category, but these do not perfectly represent every population, including Aboriginal, Torres Strait Islander, Māori and Pacific children, so a value read against a mismatched reference can misclassify a child. Interpreting with awareness of this limitation, and avoiding treatment decisions driven by a reference artefact, is essential to equitable care. [3] [4]
Socioeconomically disadvantaged and remote-dwelling children face a different barrier: access. The chronic lung diseases that most need longitudinal spirometry — bronchiectasis above all — fall heavily on these communities, yet laboratory testing is concentrated in cities. Bringing testing closer through spirometry in primary care with quality assurance, telehealth-supported interpretation, and outreach clinics matters more to these children's outcomes than any refinement of interpretation, and it is where the equity gap in lung-function care is widest. [4] [10]
Children who cannot perform the forced manoeuvre — the very young, and those with intellectual disability or neuromuscular weakness — need adapted approaches rather than repeated failed attempts. Oscillometry and other tidal-breathing techniques give useful information without a forced effort, and in progressive neuromuscular disease the trend in FVC, including the sitting-to-supine fall, guides respiratory support even when a single value is imperfect. The principle is to measure what the child can reliably do and to track it over time. [5] [11]
Evidence, Guidelines & Regional Differences
The technical foundations are set by the American Thoracic Society and European Respiratory Society. The 2019 spirometry standardisation update (Graham 2019), building on the earlier 2005 statement (Miller 2005), defines how the test is performed and what makes an effort acceptable and repeatable; the standardised reporting statement (Culver 2017) sets out how results, including z-scores and quality grades, should be presented. Interpretation is governed by the 2022 interpretive-strategies standard (Stanojevic 2022), which updates the earlier framework (Pellegrino 2005) and moves the field decisively toward z-scores and away from fixed cut-offs. [1] [2] [8]
The reference values themselves come from the Global Lung Function Initiative. The 2012 multi-ethnic spirometry equations (Quanjer 2012) provide the age, height, sex and ethnicity-specific predictions now recommended worldwide, and their adoption measurably changed how many children are classified as abnormal (Stanojevic 2014); a companion standard extends reference values to static lung volumes (Hall 2021). For young children, the ATS/ERS preschool statement (Beydon 2007) adapts the whole approach, and oscillometry (Gunawardana 2023) offers a tidal-breathing alternative. [3] [9] [5]
The clinical framing is provided by the asthma guidelines. The European Respiratory Society guideline on diagnosing asthma in children (Gaillard 2021) and the Global Initiative for Asthma strategy (Levy 2023) both place spirometry with reversibility within a diagnostic algorithm while insisting that a normal test cannot exclude asthma. Regional differences are of resource and access rather than principle: the standards are near-universal, but the availability of laboratories, the fit of reference equations to local populations, and the reach of testing into remote and disadvantaged communities vary widely. [10] [12]
Exam Pearls
Interpreting spirometry in order — 'QROB-ZI'
References
- [1]Graham BL; Steenbruggen I; Miller MR; Barjaktarevic IZ; Cooper BG; Hall GL; et al Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med, 2019.PMID 31613151
- [2]Stanojevic S; Kaminsky DA; Miller MR; Thompson B; Aliverti A; Barjaktarevic I; et al ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J, 2022.PMID 34949706
- [3]Quanjer PH; Stanojevic S; Cole TJ; Baur X; Hall GL; Culver BH; et al Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J, 2012.PMID 22743675
- [4]Stanojevic S; Stocks J; Bountziouka V; Aurora P; Kirkby J; Bourke S; et al The impact of switching to the new global lung function initiative equations on spirometry results in the UK CF registry. J Cyst Fibros, 2014.PMID 24332996
- [5]Beydon N; Davis SD; Lombardi E; Allen JL; Arets HG; Aurora P; et al An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am J Respir Crit Care Med, 2007.PMID 17545458
- [6]Pellegrino R; Viegi G; Brusasco V; Crapo RO; Burgos F; Casaburi R; et al Interpretative strategies for lung function tests. Eur Respir J, 2005.PMID 16264058
- [7]Miller MR; Hankinson J; Brusasco V; Burgos F; Casaburi R; Coates A; et al Standardisation of spirometry. Eur Respir J, 2005.PMID 16055882
- [8]Culver BH; Graham BL; Coates AL; Wanger J; Berry CE; Clarke PK; et al Recommendations for a Standardized Pulmonary Function Report. An Official American Thoracic Society Technical Statement. Am J Respir Crit Care Med, 2017.PMID 29192835
- [9]Hall GL; Filipow N; Ruppel G; Okitika T; Thompson B; Kirkby J; et al Official ERS technical standard: Global Lung Function Initiative reference values for static lung volumes in individuals of European ancestry. Eur Respir J, 2021.PMID 33707167
- [10]Gaillard EA; Kuehni CE; Turner S; Goutaki M; Holden KA; de Jong CCM; et al European Respiratory Society clinical practice guidelines for the diagnosis of asthma in children aged 5-16 years. Eur Respir J, 2021.PMID 33863747
- [11]Gunawardana S; Tuazon M; Wheatley L; Vyas B; Douglas C; Alahmadi F; et al Airwave oscillometry and spirometry in children with asthma or wheeze. J Asthma, 2023.PMID 36218195
- [12]Levy ML; Bacharier LB; Bateman E; Boulet LP; Brightling C; Buhl R; et al Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Prim Care Respir Med, 2023.PMID 36754956