Paeds · respiratory-sleep-and-airway
Upper-airway obstruction and stridor
Also known as Upper-airway obstruction and stridor · Paediatric stridor · Croup and stridor · Noisy breathing in children · Extrathoracic airway obstruction
Fellowship guide to upper-airway obstruction and stridor in children: how the flow phase of stridor localises the obstruction, why the small paediatric subglottis makes minor oedema catastrophic, the acute causes (croup, epiglottitis, bacterial tracheitis, foreign body, anaphylaxis, retropharyngeal abscess) and the chronic causes (laryngomalacia, subglottic stenosis, vocal-cord palsy), the Westley croup score, the do-not-distress principle, dexamethasone and nebulised adrenaline for croup, and the theatre-based approach to the critical airway.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A three-year-old who was well yesterday now barks like a seal, and every breath in makes a harsh crowing noise you can hear across the room. That sound is stridor, and it is the single most useful clue in the whole of paediatric airway medicine: it tells you the obstruction sits in the large upper airway, and its timing in the breath tells you roughly where. Upper-airway obstruction is any narrowing from the nose to the large intrathoracic airways that impedes the movement of air, and stridor is the harsh, monophonic sound turbulent flow makes as it squeezes past that narrowing. [1]
Stridor is a sign, not a diagnosis, and the whole skill lies in reading it. Inspiratory stridor points to an obstruction above or at the larynx, where the extrathoracic airway collapses inward on the negative pressure of inspiration. Expiratory stridor points below the thoracic inlet, where positive intrathoracic pressure narrows the airway in expiration. Biphasic stridor — heard on both phases — points to a fixed narrowing at or just below the vocal cords, classically the subglottis. Naming the phase, the time course and the child's overall stability is worth more than any single investigation. [1]
Classification
The most useful classification of stridor runs on two axes at once: where the obstruction sits and how quickly it came on. The anatomical axis uses the flow phase, because it maps directly onto the level of the lesion and therefore onto the differential. Supraglottic and glottic lesions give inspiratory stridor; a fixed subglottic narrowing gives biphasic stridor; a lower tracheal or bronchial lesion gives expiratory stridor or a monophonic wheeze. This single observation, made with a stethoscope and an ear at the bedside, narrows the diagnosis more than any imaging. [1] [10]
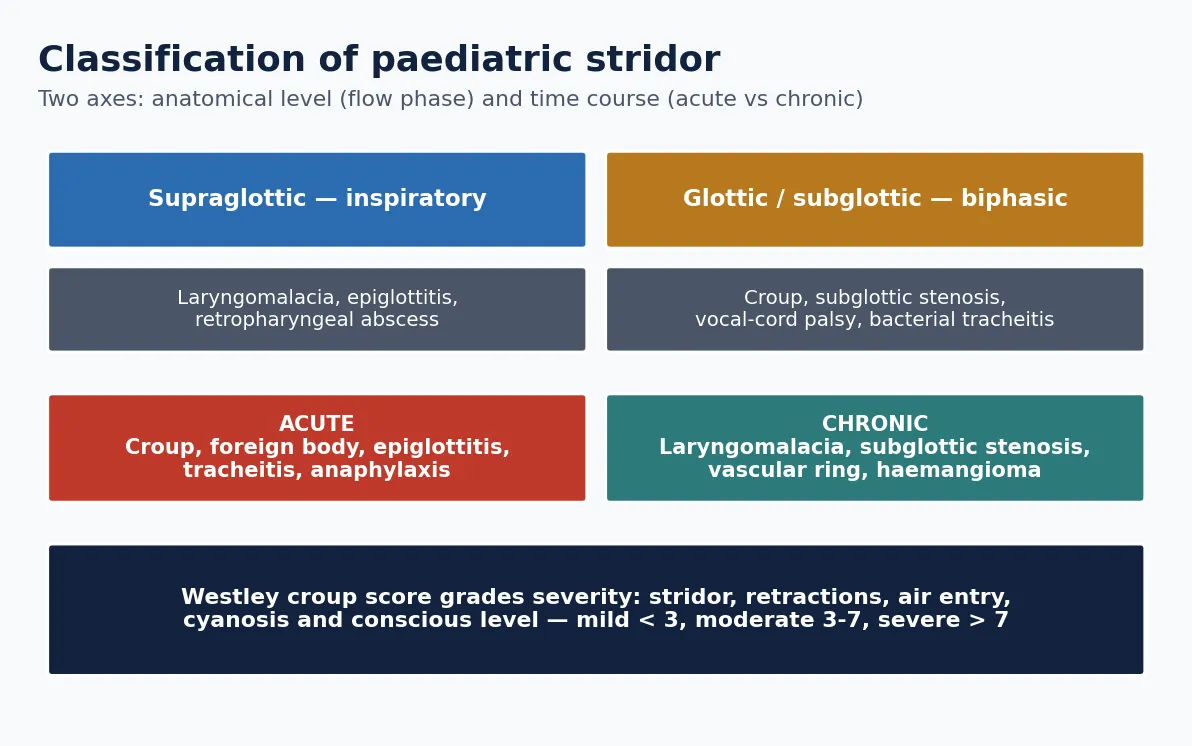
The time-course axis separates the acute from the chronic and reframes the whole assessment. Acute stridor developing over hours in a previously well child is usually infective (croup, epiglottitis, bacterial tracheitis, retropharyngeal abscess), inhaled (foreign body) or allergic (anaphylaxis with laryngeal oedema), and it is where the airway emergencies live. Chronic or recurrent stridor present for weeks to months is usually structural — laryngomalacia in the infant, subglottic stenosis after intubation, vocal-cord palsy, or a vascular ring — and is worked up electively with flexible laryngoscopy and imaging. [10] [9]
Epidemiology & Risk Factors
Croup is overwhelmingly the commonest cause of acute stridor in childhood, peaking in the second year of life and in the autumn and early winter, and caused most often by parainfluenza viruses. It affects boys slightly more than girls, recurs in a subset of children, and accounts for the great majority of children who present to an emergency department with a barking cough and stridor. The other acute infective causes are far rarer but far more dangerous per case. [1] [3]
The epidemiology of epiglottitis was transformed by the Haemophilus influenzae type b conjugate vaccine, which nearly eliminated the classic paediatric disease in immunised populations; residual cases now occur in the unimmunised, in vaccine failures and in older children and adults, and the mortality analyses show a shifting age distribution. Any assessment of a child with a toxic supraglottic picture must therefore include the immunisation history, because an unimmunised or under-immunised child returns epiglottitis to the differential. [6] [7]
The chronic and structural causes have their own demographics. Laryngomalacia is the commonest cause of chronic stridor in infancy, typically presenting in the first weeks of life and usually resolving by 18 to 24 months. Subglottic stenosis is most often acquired after prolonged neonatal intubation, so the risk factor is prematurity and a neonatal intensive care history. Foreign-body aspiration clusters in the one-to-three-year age group who explore with their mouths, with nuts, seeds and small toy parts the classic culprits. [10] [9]
Pathophysiology
The paediatric airway is not a small adult airway; it is a differently proportioned one, and that geometry is why minor swelling is catastrophic in a child but trivial in an adult. The narrowest fixed point in a young child is the subglottis, a complete cartilaginous ring, and the whole airway is smaller in absolute terms. Because resistance to laminar flow is inversely proportional to the fourth power of the radius, a single millimetre of circumferential mucosal oedema that barely narrows an adult trachea can halve the cross-sectional area of an infant subglottis and quadruple the resistance. [1] [8]
Once the airway narrows, flow becomes turbulent and audible as stridor, and the child recruits accessory muscles: nasal flaring, suprasternal and intercostal retractions, tracheal tug and a rising respiratory rate. This is compensation, and a child can sustain it for a surprisingly long time. The danger is that the noise and effort are the visible signs of that compensation, so their disappearance is ambiguous — it may mean the child is improving, or it may mean the child is exhausting and can no longer generate the effort to make the noise. [1]
Clinical Presentation
Croup presents with a prodrome of coryza followed by the unmistakable barking, seal-like cough, hoarse voice and inspiratory stridor, characteristically worse at night and worse when the child is upset. The child is usually not toxic and can swallow, which distinguishes croup from the supraglottic emergencies. Symptoms fluctuate, often frightening the family in the small hours and settling by the time they reach the department, and most cases are mild. [1] [2]
Epiglottitis presents in sharp contrast: a rapid onset over hours of high fever, a toxic appearance, drooling because swallowing is painful, a muffled hot-potato voice, and a child who sits forward and still, refusing to lie down. There is little or no cough. Bacterial tracheitis looks like severe croup that will not respond to adrenaline — a febrile, toxic child with brassy cough, stridor and rapid deterioration, caused by a bacterial infection producing thick purulent tracheal secretions and pseudomembranes. Retropharyngeal abscess presents with fever, neck stiffness or torticollis, drooling and a reluctance to move the neck. [6] [8] [11]
The inhaled foreign body has a bimodal story. There is often a witnessed choking episode in a toddler followed by stridor or a persistent monophonic wheeze; but the event may be unwitnessed, and the child can present days later with a persistent cough, focal wheeze or recurrent pneumonia. The chronic causes present differently again: laryngomalacia gives inspiratory stridor from the first weeks of life that worsens with feeding, crying and lying supine and improves when prone, in a thriving, non-toxic infant. [9] [10]
Differential Diagnosis
The first fork in the differential is acute versus chronic, because it separates the emergencies from the elective workups. In the acutely stridulous, previously well child, the differential is croup (by far the commonest), epiglottitis, bacterial tracheitis, inhaled foreign body, anaphylaxis with laryngeal oedema, and retropharyngeal or peritonsillar abscess. The discriminators are the presence of a barking cough and hoarse voice (croup), the toxic drooling forward-sitting picture (epiglottitis and deep-neck infection), a preceding choking episode (foreign body), and an allergen exposure with urticaria and angioedema (anaphylaxis). [1] [6] [9]
The critical must-not-miss diagnoses are the ones that kill quickly and are treated differently from croup. Epiglottitis and bacterial tracheitis both demand a controlled airway and must not be examined or distressed on the ward. An inhaled foreign body must be considered in any sudden stridor even without a witnessed event, because a delayed diagnosis leads to recurrent pneumonia and bronchiectasis. Anaphylaxis with airway involvement needs immediate intramuscular adrenaline, and its stridor will not respond to steroids alone. Missing any of these by anchoring on croup is the classic error. [6] [9] [8]
In the chronic or recurrent stridor of infancy, the differential is structural: laryngomalacia (the commonest, positional and improving prone), subglottic stenosis (usually post-intubation, biphasic and fixed), vocal-cord palsy (weak cry, aspiration), subglottic haemangioma (worsening over the first months, sometimes with a cutaneous haemangioma), and a vascular ring compressing the trachea and oesophagus. These are investigated with flexible awake laryngoscopy, and, when indicated, microlaryngobronchoscopy and cross-sectional imaging, rather than treated empirically. [10]
Clinical & Bedside Assessment
Assessment begins the moment you see the child, and the first judgement is stability, not diagnosis. From the doorway, read the work of breathing (retractions, tracheal tug, nasal flaring, respiratory rate), the effectiveness (air entry, chest movement, colour, oxygen saturation) and the effect on the child (conscious level, agitation or drowsiness, posture and ability to swallow secretions). A calm, pink child who is talking or babbling is compensating; a drowsy, pale or cyanosed child with reducing effort is decompensating and needs the airway team now. [1] [6]
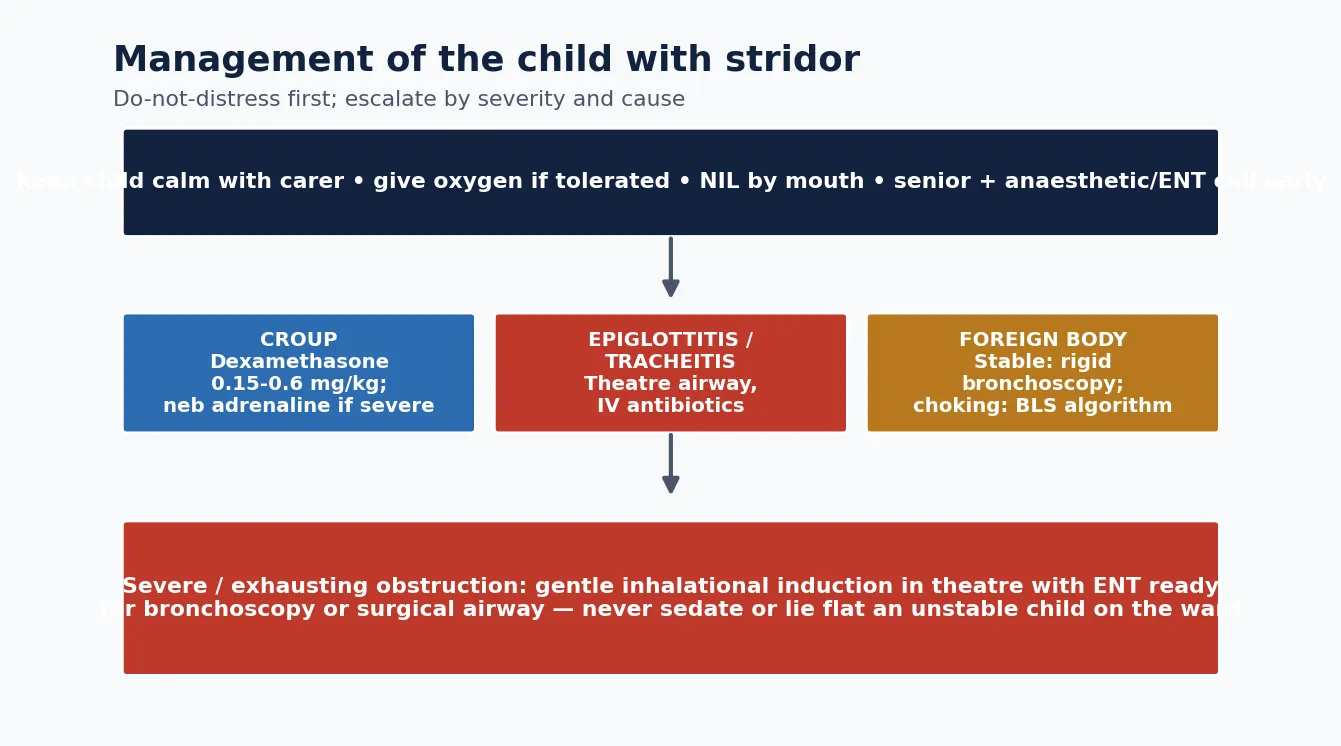
The do-not-distress principle governs everything that follows. Any procedure that upsets the child — lying them down, examining the throat with a spatula, taking blood, attempting cannulation, or separating them from the carer — can precipitate complete obstruction in a critical airway. Keep the child on the parent's lap in the position of comfort, give oxygen if it is tolerated without distress (blow-by if a mask is refused), and defer all non-essential interventions until the airway is either judged safe or secured. This restraint is the hallmark of the experienced clinician in a critical airway. [6] [1]
Once stability is established and the airway is judged safe, a focused history and examination follow: the time course, the barking cough and voice quality, fever and toxicity, any choking episode, immunisation status, feeding and positional pattern in an infant, and a birth and intubation history for the chronic presentations. The examination confirms the flow phase of the stridor, the air entry and any focal findings, but in the unstable child the examination is deliberately minimal and the priority is the airway. [1] [10]
Investigations
The single most important point about investigating the acute critical airway is that investigation must never precede airway safety. In a child with suspected epiglottitis or a critical obstruction, there is no blood test, throat swab or radiograph worth the risk of distressing the child; the airway is secured first, in theatre, and the investigations follow under controlled conditions. Croup, by contrast, is a clinical diagnosis that needs no investigation at all in the typical case — the barking cough, hoarse voice and inspiratory stridor in a non-toxic child are enough. [1] [6]
When imaging is safe and indicated, it is targeted. A lateral neck radiograph may show the thumbprint sign of a swollen epiglottis or the widened prevertebral soft tissues of a retropharyngeal abscess, and the classic subglottic steeple sign of croup, but radiographs are neither sensitive nor necessary for croup and must never delay treatment or endanger the airway. Contrast-enhanced computed tomography of the neck defines a deep-neck abscess and guides drainage once the airway is safe. [11] [6]
For the inhaled foreign body, the crucial teaching point is that a normal chest radiograph does not exclude it: most aspirated objects are radiolucent, and the film may show only subtle air trapping, or be entirely normal. A convincing history of choking is itself an indication for rigid bronchoscopy, which is both the diagnostic and the therapeutic procedure. For chronic stridor, flexible awake laryngoscopy is the key investigation, identifying laryngomalacia and vocal-cord movement, supplemented by microlaryngobronchoscopy and cross-sectional imaging for structural and vascular lesions. [9] [10]
Management — Resuscitation
The resuscitation of a child with a critical upper-airway obstruction is a controlled, unhurried, senior-led process, not a scramble. The moment a critical airway is suspected, call for the most senior available anaesthetist and ENT surgeon and move toward theatre. Keep the child calm and undisturbed in the position of comfort with the carer, deliver oxygen in whatever way is tolerated, and prepare for a gas induction. Do not attempt intravenous access, throat examination or awake laryngoscopy in a child with suspected epiglottitis, because distress can precipitate complete obstruction. [6] [1]
The definitive rescue for the severe or exhausting obstruction is a gentle inhalational (gas) induction of anaesthesia in theatre, maintaining spontaneous breathing, with the ENT surgeon scrubbed and ready to perform rigid bronchoscopy or a surgical airway if intubation fails. Nebulised adrenaline buys time in severe croup and in laryngeal oedema by reducing mucosal swelling, and it is given while the definitive plan is organised. For anaphylaxis with airway involvement, intramuscular adrenaline is the immediate treatment and must not be delayed for steroids or antihistamines. [4] [5]
Nebulised adrenaline (severe croup or laryngeal oedema)
Loading dose
0.5 mL/kg of 1:1000 adrenaline (maximum 5 mL) nebulised
Maintenance dose
Repeat as needed for recurrent severe obstruction with cardiac monitoring
The principle that unifies airway resuscitation is that the acute measures buy time to reach the definitive intervention safely. Adrenaline and steroids in croup, intramuscular adrenaline in anaphylaxis, and oxygen and calm in every case are bridges to a stable airway or to theatre. The single most dangerous decision is to sedate, cannulate, lie flat or examine the throat of an unstable child on the ward instead of taking them to a controlled environment with the airway team assembled. [6] [1]
Immediate management of the child with a critical airway
Recognise the critical airway: toxic, drooling, tripod, drowsy, silent chest or falling effort
Do not distress: keep the child with the carer in the position of comfort, no throat exam, no cannulation
Call the most senior anaesthetist and ENT surgeon and move toward theatre
Give oxygen in whatever form is tolerated; give nebulised adrenaline for severe croup or laryngeal oedema
Give intramuscular adrenaline immediately if anaphylaxis is suspected
Secure the airway by gentle inhalational induction in theatre with ENT ready for bronchoscopy or surgical airway
Investigate and give antibiotics only once the airway is safe
Management — Definitive & Stepwise
The definitive management of croup is corticosteroid, and this is the highest-yield fact in the topic. A single dose of dexamethasone reduces the severity and duration of symptoms, the rate of return visits and the need for admission and adrenaline across the whole severity spectrum, including mild croup. The Cochrane review of glucocorticoids for croup and the randomised trial of dexamethasone for mild croup established this benefit, and dexamethasone is given to essentially every child who presents with croup. [3] [2]
Dexamethasone (croup, all severities)
Loading dose
0.15 to 0.6 mg/kg orally as a single dose (commonly 0.15 mg/kg)
Maintenance dose
Usually a single dose; a second dose may be given the next day in severe cases
For the acute infective airway obstructions other than croup, the definitive treatment pairs a secured airway with cause-specific therapy. Epiglottitis is treated with a controlled airway followed by intravenous third-generation cephalosporin antibiotics, and the child is typically extubated within a few days as the swelling settles. Bacterial tracheitis needs airway endoscopy to clear the purulent secretions and pseudomembranes, intubation in most cases, and intravenous antistaphylococcal and broad-spectrum antibiotics. A retropharyngeal abscess is treated with intravenous antibiotics and surgical drainage once the airway is safe. [6] [8] [11]
[6] [8] [9]The inhaled foreign body is removed by rigid bronchoscopy under general anaesthesia, which is both diagnostic and therapeutic and is undertaken urgently once the diagnosis is suspected on history. The chronic structural causes are managed on their own timelines: laryngomalacia is observed and usually resolves, with supraglottoplasty reserved for the minority with severe obstruction, failure to thrive or apnoea; subglottic stenosis is managed by dilatation or laryngotracheal reconstruction; and a vascular ring is divided surgically when it causes significant symptoms. [9] [10]
Specific Subtypes & Scenarios
Croup (laryngotracheobronchitis) is the archetype and the one an examiner expects in full. It is a viral (usually parainfluenza) inflammation of the subglottis presenting with a barking cough, hoarse voice and inspiratory stridor in a non-toxic child, graded by the Westley score, and treated with a single dose of dexamethasone for all severities plus nebulised adrenaline for severe obstruction. Most children are managed at home or with a short observation; a child needing repeated adrenaline is admitted, and intubation is rarely required. The evidence base — the Cochrane glucocorticoid review, the mild-croup dexamethasone trial, and the adrenaline data — is the part examiners probe. [1] [3] [4]
Epiglottitis and bacterial tracheitis are the toxic airway emergencies. Epiglottitis is now rare because of Hib vaccination but must be recalled in the unimmunised or under-immunised child and in older patients; the picture is rapid-onset fever, drooling, a muffled voice and a forward-sitting posture, and the management is a controlled airway plus cephalosporin. Bacterial tracheitis is the great mimic of severe croup that fails to respond to adrenaline — a toxic, febrile child with copious purulent tracheal secretions needing endoscopy, intubation and antibiotics — and it is an increasingly recognised cause of the croup-like child who deteriorates. [6] [7] [8] [12]
Across Australia, New Zealand and the United Kingdom, croup is managed to a common standard: oral dexamethasone for all severities, nebulised adrenaline with observation for severe obstruction, and clear discharge safety-netting for the fluctuating night-time course. The critical airway is managed within a networked model — the do-not-distress principle, early senior anaesthetic and ENT involvement, gas induction in theatre, and retrieval of the child in a rural or remote setting to a centre with paediatric airway expertise. Hib immunisation coverage keeps epiglottitis rare, and immunisation status is checked in every under-immunised or unusually presenting child. [1] [6]
The inhaled foreign body and laryngomalacia complete the high-yield scenarios. The foreign body is suspected on a choking history even with a normal chest radiograph, and it is removed by rigid bronchoscopy; the danger is a delayed or missed diagnosis leading to recurrent pneumonia. Laryngomalacia is the reassuring counterpoint — the commonest chronic infant stridor, inspiratory and positional, in a thriving baby, usually resolving by two years and needing only rare surgical intervention for severe disease. Recognising which stridor is dangerous and which is benign is the essence of the topic. [9] [10]
Complications & Pitfalls
The complications of upper-airway obstruction follow from the airway itself and from the specific causes. Complete obstruction leading to hypoxic respiratory arrest is the feared outcome of any critical airway that is mishandled or under-recognised. A missed inhaled foreign body causes recurrent or persistent pneumonia, atelectasis and, over time, bronchiectasis. Bacterial tracheitis and deep-neck abscesses can extend to mediastinitis or septic complications. Prolonged intubation, whether for airway disease or in the neonatal period, is itself the commonest cause of acquired subglottic stenosis. [9] [8] [11]
The pitfalls are mostly failures of recognition and of restraint. The first is anchoring on croup and missing the toxic child with epiglottitis, bacterial tracheitis or a deep-neck infection. The second is distressing a critical airway — examining the throat, lying the child flat, forcing a mask or attempting cannulation — and precipitating complete obstruction. The third is misreading exhaustion as improvement when the chest goes quiet. The fourth is excluding an inhaled foreign body on the basis of a normal chest radiograph. [6] [1] [9]
Prognosis & Disposition
The prognosis of the common causes is excellent when they are correctly recognised and managed. Croup is self-limiting, resolves over a few days, and with dexamethasone the great majority of children are managed at home or after a short observation, with intubation rarely required. Laryngomalacia resolves spontaneously in the large majority by 18 to 24 months, needing only reassurance and growth monitoring. The reassuring, common diagnoses therefore carry a very good outlook once the dangerous mimics have been excluded. [1] [10]
The dangerous causes carry a good prognosis too, but only if the airway is secured in time. Epiglottitis and bacterial tracheitis have low mortality in the modern era of controlled airway management and antibiotics, but both are lethal if the airway is lost; the mortality trend analyses underline that outcome depends on timely recognition and airway control. A promptly removed foreign body does well, whereas a missed one leads to chronic suppurative lung disease. Acquired subglottic stenosis may need staged reconstructive surgery. [6] [8] [9]
Disposition follows severity and cause. A child with mild croup who is comfortable after dexamethasone is discharged with clear safety-netting about the fluctuating night-time course and the signs that warrant return. A child with moderate-to-severe croup, or one who needs repeated adrenaline, is admitted for observation. A child with a critical or toxic airway is managed in theatre and then in a paediatric intensive care unit, and a rural or remote child with a threatened airway is retrieved to a centre with paediatric airway expertise. [1] [6]
Special Populations
The child with a pre-existing narrow or abnormal airway is the first special population. A child with subglottic stenosis, a repaired tracheo-oesophageal fistula, Down syndrome (with its narrower airway and hypotonia) or a craniofacial syndrome has less reserve, so a minor intercurrent croup can precipitate a disproportionate obstruction. These children warrant a lower threshold for admission and early involvement of their existing airway team. [10] [8]
The technology-dependent child with a tracheostomy is the second. In these children the differential for acute deterioration includes tube blockage, displacement and tracheostomy-associated infection, and the first response to respiratory distress is to assess and, if needed, change the tracheostomy tube. Bacterial tracheitis and tracheobronchitis are recognised problems in children with long-term artificial airways, and families are trained in emergency tube management. [8] [12]
The under-immunised or unimmunised child is the third. Falling or incomplete Haemophilus influenzae type b coverage returns epiglottitis to the differential, and the immunisation history must be sought in any child with a toxic supraglottic picture. This has particular relevance for migrant, refugee and other under-served populations, and for communities with lower vaccination uptake, where clinicians must keep the vaccine-preventable airway emergencies in mind. [7] [6]
The rural or remote child is the fourth. Distance from paediatric airway expertise means the local team must recognise the critical airway, apply the do-not-distress principle, give the time-buying treatments (dexamethasone, nebulised adrenaline, intramuscular adrenaline for anaphylaxis), and involve the retrieval service early, so that a threatened airway is stabilised and transferred before it is lost. [1] [4]
Evidence, Guidelines & Regional Differences
The evidence base for croup is unusually strong and is the centrepiece of the topic. The Cochrane review of glucocorticoids for croup established that a single dose of corticosteroid reduces symptom severity, return visits and the need for admission and adrenaline, and the randomised trial of dexamethasone for mild croup extended this benefit to the mildest cases, which is why dexamethasone is now given across the whole severity spectrum. The Cochrane review of nebulised epinephrine confirmed its role in providing rapid, temporary relief in severe croup, and the historical Westley study gave us the severity score that still grades croup at the bedside. [3] [2] [4] [5]
The epiglottitis and structural-airway literature frames the rarer causes. The analysis of United States epiglottitis mortality trends and the Hib vaccine-failure survey together explain the transformation of epiglottitis into a rare disease and its residual occurrence in the unimmunised and in older patients. The laryngomalacia review summarises the modern approach to the commonest chronic infant stridor, the foreign-body review sets out the diagnosis and endoscopic management of the inhaled foreign body, and the bacterial-tracheitis literature establishes it as the toxic mimic of severe croup that needs endoscopy and antibiotics. [6] [7] [10] [9] [8]
Across ANZ, the United Kingdom, Europe and North America the core is uniform: dexamethasone for all croup, nebulised adrenaline for severe obstruction, the do-not-distress principle for the critical airway, and early senior anaesthetic and ENT involvement with a theatre-based gas induction. What varies is the local airway-escalation pathway, the retrieval arrangements for rural and remote children, and the residual burden of epiglottitis, which tracks Hib immunisation coverage. The unifying message is to recognise the dangerous airway early, avoid distressing it, and secure it in a controlled environment. [1] [6]
Exam Pearls
Approach to the child with stridor — 'STRIDOR'
References
- [1]Bjornson CL; Johnson DW Croup. Lancet, 2008.PMID 18295000
- [2]Bjornson CL; Klassen TP; Williamson J; Brant R; Mitton C; Plint A; Bulloch B; Evered L; Johnson DW; Pediatric Emergency Research Canada Network A randomized trial of a single dose of oral dexamethasone for mild croup. N Engl J Med, 2004.PMID 15385657
- [3]Russell KF; Liang Y; O'Gorman K; Johnson DW; Klassen TP Glucocorticoids for croup. Cochrane Database Syst Rev, 2011.PMID 21249651
- [4]Bjornson C; Russell K; Vandermeer B; Klassen TP; Johnson DW Nebulized epinephrine for croup in children. Cochrane Database Syst Rev, 2013.PMID 24114291
- [5]Westley CR; Cotton EK; Brooks JG Nebulized racemic epinephrine by IPPB for the treatment of croup: a double-blind study. Am J Dis Child, 1978.PMID 347921
- [6]Allen M; Meraj TS; Oska S; Spillinger A; Folbe AJ; Cramer JD Acute epiglottitis: Analysis of U.S. mortality trends from 1979 to 2017. Am J Otolaryngol, 2021.PMID 33429180
- [7]Marques JG; Inácio Cunha FM; Bajanca-Lavado MP; Portuguese Study Group on Haemophilus influenzae Invasive Disease in Children Haemophilus influenzae Type b Vaccine Failure in Portugal: A Nationwide Multicenter Pediatric Survey. Pediatr Infect Dis J, 2023.PMID 37406244
- [8]Eckel HE; Widemann B; Damm M; Roth B Airway endoscopy in the diagnosis and treatment of bacterial tracheitis in children. Int J Pediatr Otorhinolaryngol, 1993.PMID 8258482
- [9]Salih AM; Alfaki M; Alam-Elhuda DM Airway foreign bodies: A critical review for a common pediatric emergency. World J Emerg Med, 2016.PMID 27006731
- [10]Thorne MC; Garetz SL Laryngomalacia: Review and Summary of Current Clinical Practice in 2015. Paediatr Respir Rev, 2016.PMID 25802018
- [11]Suchecki M; Wolniewicz M; Jędrychowski J; Zawadzka-Głos L Retropharyngeal and parapharyngeal abscesses in children - a 9.5-year retrospective single-center analysis followed by literature review. Otolaryngol Pol, 2026.PMID 42417448
- [12]Gipsman A; Prero M; Toltzis P Tracheobronchitis in children with tracheostomy tubes: Overview of a challenging problem. Pediatr Pulmonol, 2022.PMID 34981895