Paeds · rheumatology-musculoskeletal-and-sports
Acute monoarthritis and septic arthritis
Also known as septic arthritis · pyogenic arthritis · suppurative arthritis · acute monoarthritis · hot joint · Kocher criteria
A fellowship approach to the child with an acutely hot, swollen joint: the Kocher clinical prediction rule that separates septic arthritis from transient synovitis, the urgent joint aspiration that confirms pus in the synovial fluid, the empiric intravenous antibiotics stratified by age and organism, and the surgical emergency that a septic hip represents because intracapsular pressure threatens the femoral head blood supply within hours.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A three-year-old boy is carried into the emergency department refusing to walk, holding his right hip flexed and externally rotated, with a fever of thirty-nine degrees and a knee that screams when anyone touches it; or a toddler presents with a swollen red ankle and a limp that came on over a day; or a neonate in the nursery is irritable and febrile with a swollen shoulder and will not move the arm. In each, the question is the same — is this joint infected, and if there is any doubt, aspirate it, drain the hip, and treat. [5] [1]
The five moves — Score, Sample, Scan, Strike, Sweep
Overview & Definition
Acute monoarthritis is inflammation of a single joint presenting over hours to days, and septic arthritis is the bacterial, pus-forming subset that is the orthopaedic and infectious-disease emergency within it. The two are framed together because the hot swollen joint is a single clinical problem whose first task is always the same — exclude infection — and because the other causes, from transient synovitis to juvenile idiopathic arthritis, reveal themselves only once sepsis has been ruled out. [1] [5]
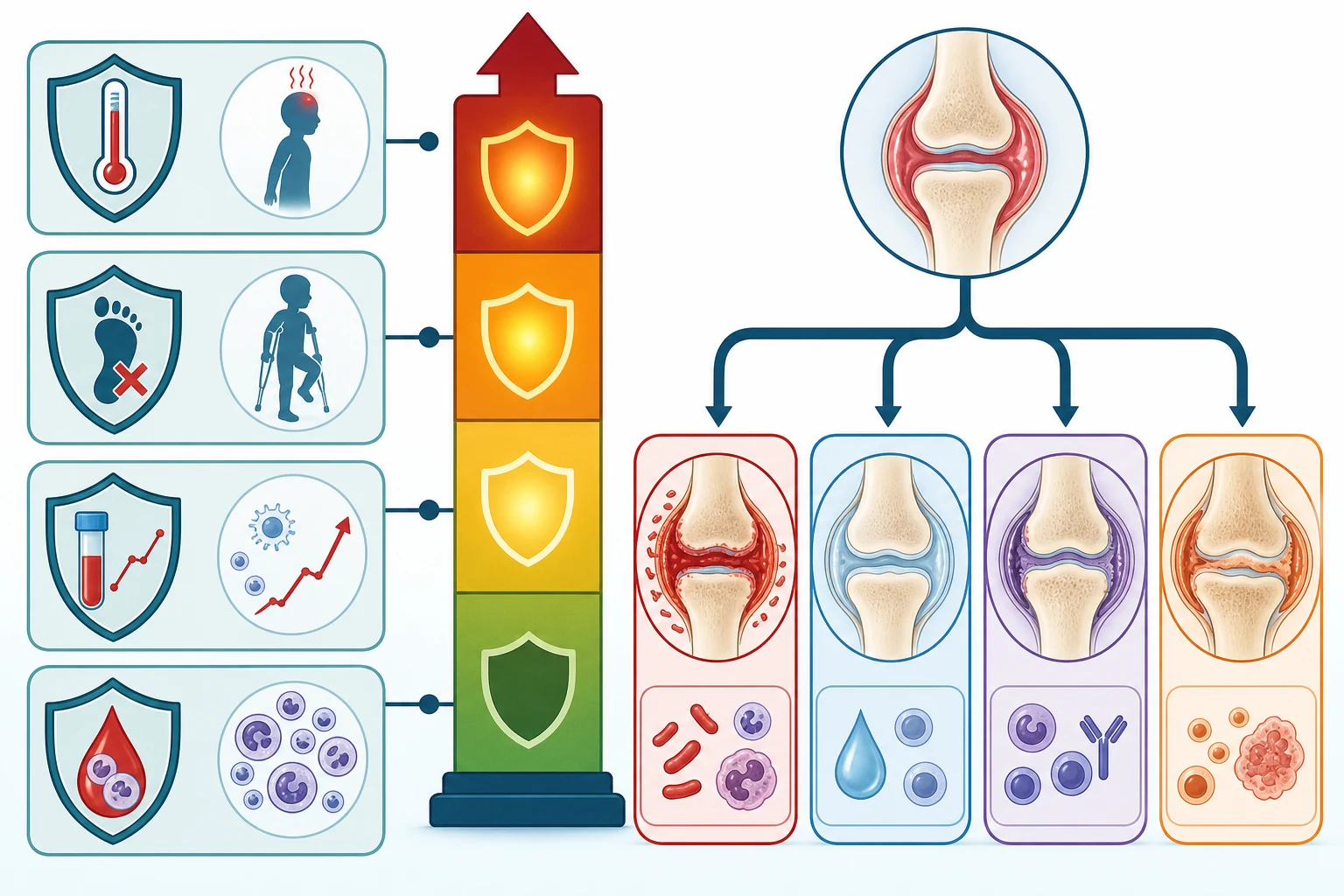
The fellowship framing rests on a single pathological truth. The synovium is a highly vascular membrane that produces the fluid lubricating the joint, and bacteria reach it most often by the haematogenous route, seeding the synovial membrane and multiplying within the synovial fluid where host defences and antibiotics penetrate poorly. The resulting neutrophilic inflammation raises the intra-articular pressure, erodes the articular cartilage, and — in the hip, where the capsule is tight and the femoral head blood supply is intracapsular — chokes the circulation to the epiphysis. This is why septic arthritis is measured in hours, not days. [9]
The clinical importance comes from what happens if the joint is drained late or treated inadequately. Permanent cartilage destruction, avascular necrosis of the femoral head, growth arrest with leg-length discrepancy, recurrent infection, and progression to chronic osteomyelitis are the sequelae of a delayed or partial response. In the neonate and the immunocompromised child the presentation is occult, multiple joints may be involved, and the diagnosis is even more easily missed — which is why a low threshold to aspirate any suspicious joint is the safeguard. [5] [6]
Classification
Classification of the acute monoarthritis rests on two axes — the probability of bacterial infection, which the Kocher clinical prediction rule estimates, and the synovial fluid analysis, which confirms it. The Kocher criteria were derived in 1999 from a retrospective study of children with an irritable hip, identifying four independent predictors of septic arthritis over transient synovitis, and they remain the taught framework for the probability of sepsis at the bedside. [1]
The four Kocher predictors are a history of fever above thirty-eight point five degrees Celsius, an inability to bear weight on the affected limb, an erythrocyte sedimentation rate above forty millimetres per hour, and a peripheral white blood cell count above twelve thousand per microlitre. The predicted probability of septic arthritis rises steeply with the number of predictors present — from below one per cent with none, to roughly three per cent with one, forty per cent with two, ninety-three per cent with three, and over ninety-nine per cent with all four — and a child with two or more predictors warrants urgent joint aspiration. [1] [2]
The Caird prospective study refined this framework by adding the C-reactive protein, which emerged as the single strongest independent predictor, with a cut-off of twenty milligrams per litre. The Caird study also offered an important calibration caveat — the original Kocher probabilities were derived retrospectively and may overestimate the true risk, so in Caird's prospective cohort the presence of four predictors carried a probability closer to sixty per cent rather than ninety-nine. The clinical message is that the Kocher criteria are a probability tool that sharpens suspicion, not a rule-out, and a reassuring score never overrides a septic-looking joint or a frankly purulent aspirate. [3] [4]
Epidemiology & Risk Factors
Septic arthritis is uncommon but not rare, with an incidence of roughly one to two per ten thousand children per year, and it is the commonest cause of an acutely hot joint in a febrile child. The peak incidence sits in the young child under four years of age, driven by the dominance of Kingella kingae in this group, with a second contribution from Staphylococcus aureus across all ages. The knee and the hip are the most frequently involved joints, and the hip carries the highest stakes because of its tight capsule and intracapsular femoral head blood supply. [9] [7]
The organism changes with age, and this single fact drives the empiric antibiotic choice. Staphylococcus aureus is the overall commonest cause across childhood. In the neonate, group B streptococcus and Gram-negative bacilli such as Escherichia coli add to the S. aureus burden. In the infant and young child under four years, Kingella kingae rivals or exceeds S. aureus as the leading cause and is easily missed. In the older child and adolescent, S. aureus and Streptococcus pyogenes predominate, with Neisseria gonorrhoeae entering the differential in the sexually active adolescent. Special contexts shift the organism further — Salmonella in sickle cell disease, Pseudomonas after a puncture wound of the foot, and fungal or unusual organisms in the immunocompromised. [9] [8]
The risk factors that matter for the fellowship answer are those of impaired host defence and of bacteremic seeding. Indwelling central lines, recent instrumentation or surgery, immunocompromise, indwelling prosthetic material, chronic skin conditions such as eczema that breach the barrier, and concurrent or recent viral illness all raise the risk. In resource-limited settings the burden is far higher — Lavy's review of sub-Saharan African children documented septic arthritis presenting late, with multiple joints involved and a heavy burden of permanent disability — a reminder that access and timing, not biology, determine the outcome. [5] [6]
Pathophysiology
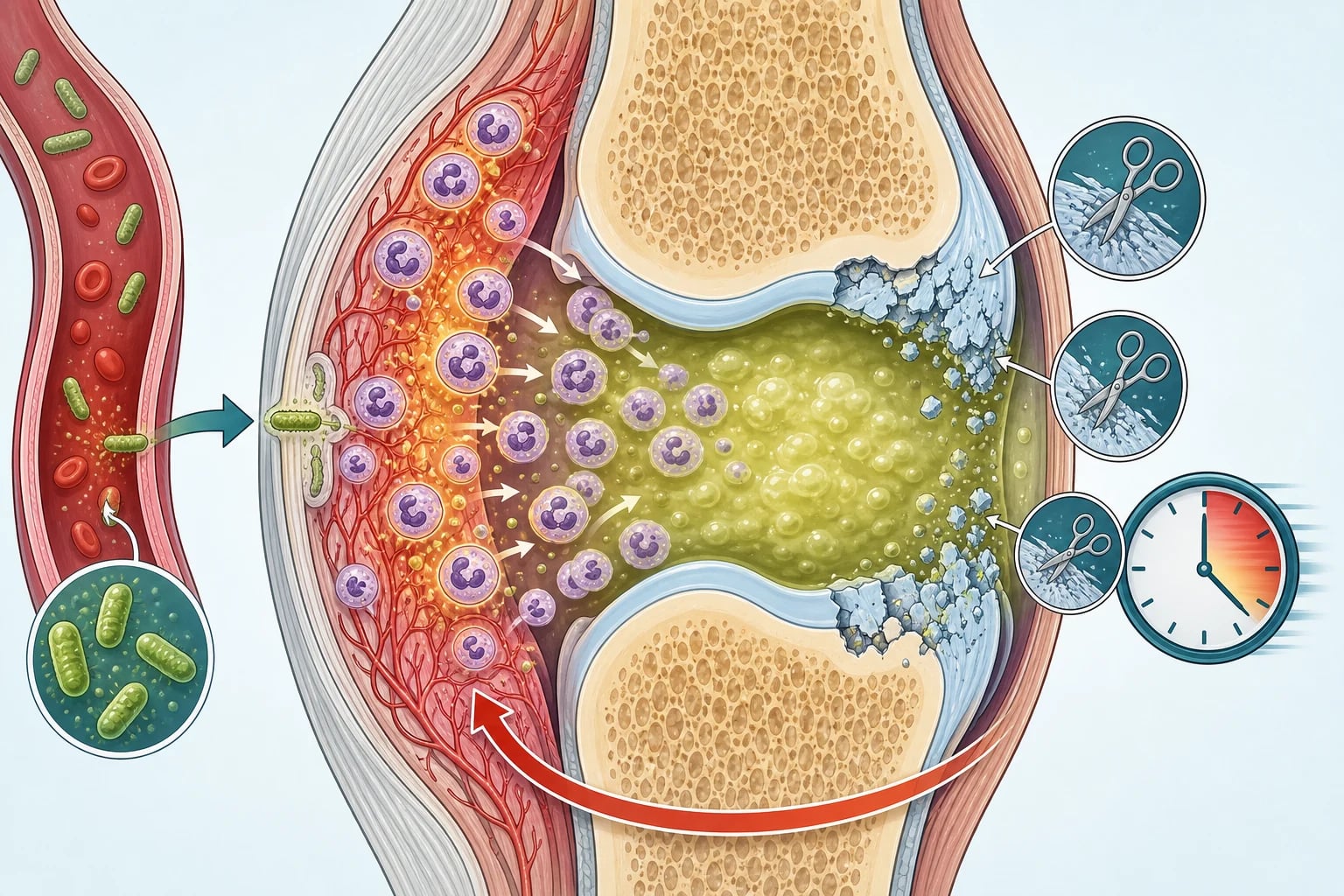
The pathophysiology begins with haematogenous seeding of the highly vascular synovial membrane. Bacteria circulating in the bloodstream lodge in the synovium, where the sluggish blood flow and the relatively low complement and opsonin activity of the synovial fluid create a sanctuary for multiplication. Once established, the bacteria multiply within the joint space, beyond the effective reach of circulating phagocytes, and the synovial fluid turns from a clear lubricant into a reservoir of pus. [9]
The inflammatory response is neutrophilic and destructive. The bacteria and their products activate the innate immune response, and neutrophils pour into the joint, releasing proteases and reactive oxygen species that degrade the proteoglycan matrix and the collagen network of the articular cartilage. Unlike the skin or the soft tissues, cartilage has almost no capacity to regenerate, so the destruction is cumulative and largely irreversible — which is the biological basis for the urgency of drainage. Cartilage loss begins within hours and is substantial within days, so every hour of pus under pressure is an hour of permanent joint damage. [4] [9]
The hip is the special case that defines the surgical emergency. The femoral head derives its blood supply largely from the medial circumflex femoral artery, whose retinacular branches traverse the joint capsule and are vulnerable to compression when the intracapsular pressure rises with pus. A septic hip therefore strangulates its own epiphysis, producing avascular necrosis of the femoral head, and because antibiotics reduce the bacterial load but do not decompress the capsule, the only intervention that protects the blood supply is surgical drainage. This is the reason the septic hip goes to theatre and the septic knee may sometimes be managed by aspiration or arthroscopy. [3]
The extension to osteomyelitis is the complication that broadens the management. The synovium reflects onto the metaphysis at the joint margin, and in the young child the metaphyseal blood supply communicates with the epiphyseal and synovial circulation, so an infection beginning in the joint can extend into the adjacent bone, and vice versa. This anatomical continuity is why septic arthritis and osteomyelitis coexist so often in children, and why imaging and treatment must consider both. [9] [10]
Clinical Presentation
The presentation is the child who will not move the joint. The affected joint is swollen, warm, tender, and held rigidly in the position of greatest capsular laxity — flexion, abduction, and external rotation for the hip, flexion for the knee — and any attempt to move it is resisted fiercely. The child is systemically unwell with a fever, irritability, and a refusal to bear weight or to use the limb, and the younger the child the more likely the presentation is non-localising, with a pseudoparalysed limb, sepsis, or inconsolable crying. [1] [5]
The joint distribution is dominated by the large weight-bearing joints. The knee is the most commonly involved joint overall, followed by the hip, with the ankle, elbow, shoulder, and wrist less frequent. Polyarticular involvement occurs in roughly ten per cent of children and is more common in the neonate, the immunocompromised, and in gonococcal or rheumatoid-driven disease — a child with two or more hot joints is not reassured by the count. The pain of a septic hip often refers to the knee, so any febrile child complaining of knee pain must have the hip examined and imaged, or the septic hip hiding behind a normal-looking knee will be missed. [5] [9]
Which reassuring-sounding stories must never close the search for sepsis? A child with a recent viral illness and a limp is not automatically transient synovitis — the Kocher criteria and the inflammatory markers, not the preceding virus, separate the two. A well-looking toddler with a mildly swollen knee is not safe because they look well — Kingella kingae produces a deceptively mild, low-fever picture and it is a real pathogen in the under-four. And a neonate who is simply irritable and not moving an arm is not colic — pseudoparalysis of a limb in a febrile neonate is septic arthritis or osteomyelitis until proven otherwise. [7] [5]
Differential Diagnosis
The differential diagnosis of the febrile limping child is broad, and the fellowship skill is to separate the bacterial joint from its mimics using the Kocher criteria, the inflammatory markers, and the synovial fluid. Transient synovitis is the commonest mimic and the one most easily confused with sepsis — it follows a viral illness, the child is afebrile or low-grade febrile, and the inflammatory markers are normal or minimally raised. The Kocher criteria and the synovial fluid cell count separate the two, and when the distinction remains unclear, the joint is aspirated. [1] [2]
Juvenile idiopathic arthritis enters the differential when the arthritis persists beyond six weeks, but it can present as an acute monoarthritis in the oligoarticular subtype, and a child with a swollen knee, a low-grade fever, and a raised antinuclear antibody may have either. The synovial fluid is inflammatory rather than septic — a cell count in the tens of thousands rather than above fifty thousand — and the response to non-steroidal anti-inflammatory drugs and the persistence beyond the acute window distinguish it. Reactive arthritis follows a gastrointestinal or genitourinary infection one to four weeks earlier, tends to be oligoarticular and asymmetric, and may include enthesitis and conjunctivitis. [9]
For the child presenting primarily with systemic upset, the differential includes osteomyelitis of the adjacent bone, cellulitis overlying a joint, deep vein thrombosis, a slipped capital femoral epiphysis in the older child, and a Perthes presentation in the young school-age child. A fracture or non-accidental injury must be considered in the limping toddler who will not bear weight. The ultrasound, the inflammatory markers, and the radiographs resolve most of these, and the joint aspiration settles the remainder. The single rule is that septic arthritis is excluded by a negative aspirate, not by the appearance of any mimic. [5] [1]
Clinical & Bedside Assessment
The recognition move is to treat every febrile child with a swollen joint or a refusal to bear weight as septic arthritis until proven otherwise, and to perform a full musculoskeletal and systemic examination. The history must establish the onset and pace of the swelling, the fever pattern, the ability to bear weight, any preceding illness, the immunisation status, and the background of immunocompromise or recent instrumentation — and in the young child, the history is often the observation that the limb is held still and the child will not use it. [1] [5]
The bedside examination must look, feel, move, and measure every joint. Look for swelling, erythema, and the posture of greatest comfort — the flexed, abducted, externally rotated hip, or the flexed knee. Feel for warmth, comparing with the contralateral joint, and for the boggy swelling of an effusion. Attempt gentle passive movement, expecting severe pain and a marked resistance at the end of the septic joint's limited range, and document the child's willingness to bear weight, because refusal to bear weight at all is a Kocher predictor. Examine the skin for a portal of entry, the adjacent limb for an osteomyelitic focus, and the child systemically for the stigmata of sepsis, endocarditis, and immunocompromise. [1] [3]
Which examination findings must never be dismissed? A child who holds the joint absolutely still, who screams when the joint is moved even a millimetre, has a septic joint until proven otherwise — the profound pseudoparalysis is the sign. A febrile child with a swollen knee and referred pain must have the hip examined and imaged, because the hip is hidden and the hip is dangerous. And a neonate who is not moving a limb, with or without fever, is a septic joint or a septic bone until imaging and aspiration exclude it — the younger and less communicative the child, the lower the threshold to image and aspirate. [5] [7]
Investigations
Joint aspiration is the single most important investigation, because the synovial fluid confirms or excludes the diagnosis and guides the antibiotic choice. The fluid is sent for a cell count and differential, a Gram stain, and culture, and in the young child it should be inoculated directly into blood-culture bottles to improve the yield of fastidious organisms such as Kingella kingae. A frankly purulent aspirate with a cell count above fifty thousand cells per microlitre and a neutrophil predominance is treated as septic arthritis regardless of the Gram stain, and a positive Gram stain or culture confirms the organism and narrows the therapy. The aspiration is therapeutic as well as diagnostic for the superficial joints, but it must precede the first antibiotic dose or the specimen is sterilised. [4] [7]
The blood tests frame the probability and the severity but do not confirm the diagnosis. A full blood count, an erythrocyte sedimentation rate, and a C-reactive protein provide the Kocher and Caird predictors and the baseline for tracking the response to treatment, with a CRP above twenty milligrams per litre a strong independent predictor of sepsis. Blood cultures are positive in roughly a third to a half of cases and provide an organism when the joint has already been drained or when aspiration is delayed, and they are drawn before the first antibiotic. The inflammatory markers are repeated to confirm the fall after forty-eight to seventy-two hours of appropriate therapy, and a CRP that does not fall prompts a search for persistent pus, an undrained focus, or resistant organism. [3] [4]
Imaging confirms the effusion and guides the tap, and it is essential for the deep joints that cannot be examined directly. Ultrasound is the first-line modality for the hip, detecting an effusion as a widened joint space and guiding the aspiration under real-time vision, and it is rapid, radiation-free, and available at the bedside. Plain radiographs exclude the mimics — a fracture, a slipped capital femoral epiphysis, a Perthes presentation, or a destructive bone lesion — and they may show soft-tissue swelling or joint-space widening in advanced sepsis. Magnetic resonance imaging is reserved for the child with suspected adjacent osteomyelitis, a complex or atypical presentation, or a poor response to treatment, because it defines the bone and soft-tissue extension that ultrasound cannot. [9] [5]
Management — Resuscitation
Resuscitation is the priority in the child who presents with sepsis or with a septic joint that has progressed to systemic upset. The airway, breathing, and circulation are assessed and supported, intravenous access is secured, and a fluid bolus of ten to twenty millilitres per kilogram of isotonic saline is given to the shocked child, repeated as guided by the clinical response. Analgesia is not optional — the joint is agonisingly painful — and intravenous morphine or a regional block allows the child to be examined, imaged, and aspirated humanely. [5] [9]
The cultures are drawn the moment access is secured. Blood cultures, the full blood count, the inflammatory markers, and the synovial fluid are all obtained before the first antibiotic, and the antibiotic is then started without further delay. In the well-looking child with a single hot joint and no sepsis, the resuscitation phase is brief and the pathway moves quickly to the definitive drainage and the targeted antibiotic, but the discipline of cultures-before-antibiotic holds in every case. [4] [1]
The septic hip is the resuscitation emergency that defines the urgency. A confirmed or strongly suspected septic hip is taken to theatre for arthrotomy and washout as soon as the team can be assembled, because the intracapsular pus threatens the femoral head blood supply with every hour it remains under pressure. The antibiotic and the analgesia are started, the cultures are drawn, and the child is moved to theatre — the drainage is part of the resuscitation, not a later step. [3] [6]
Management — Definitive & Stepwise
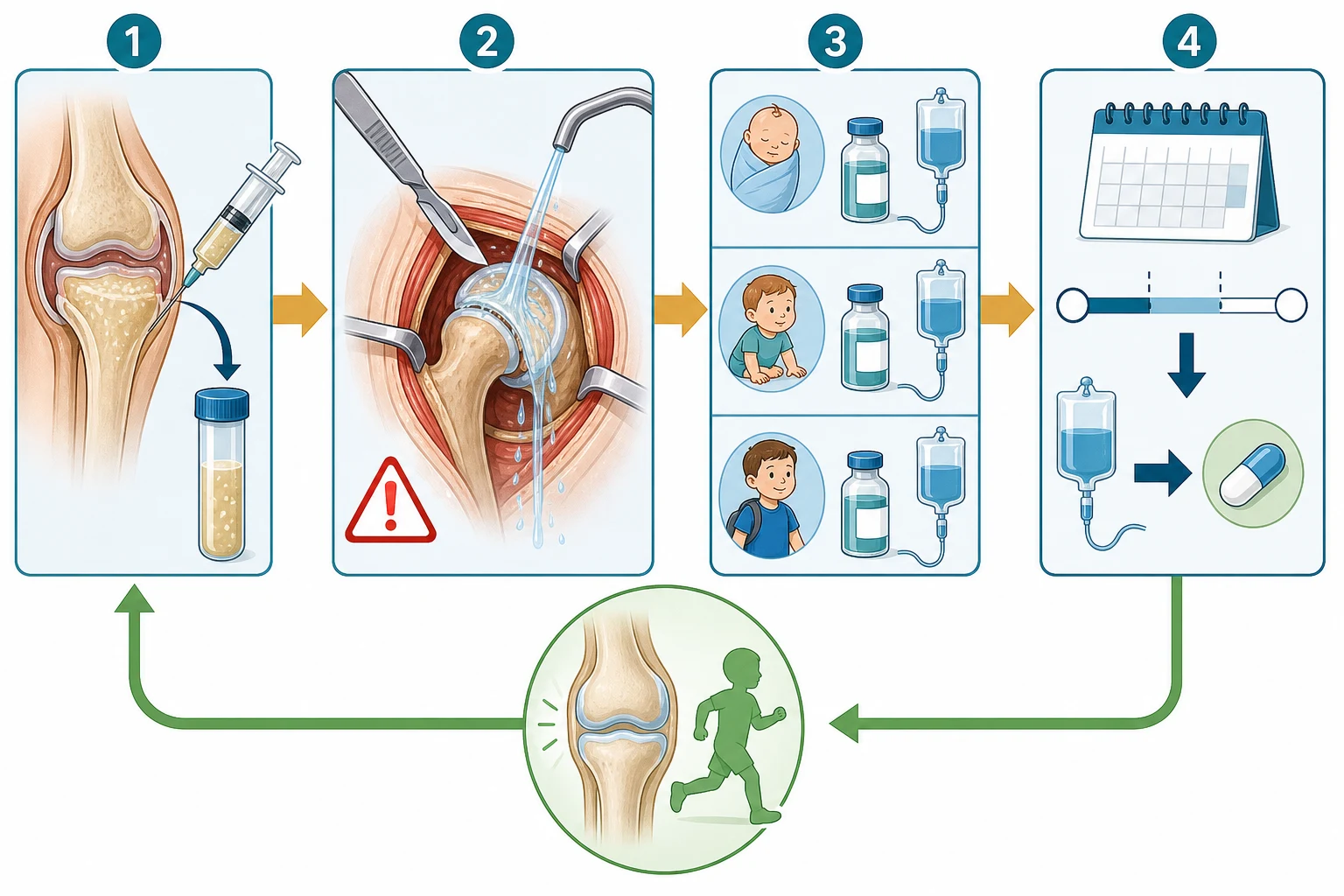
The definitive management combines drainage, empiric antibiotics, and targeted therapy guided by the organism, and the order is cultures first, then drainage, then antibiotic. Drainage relieves the pressure that destroys cartilage and the femoral head, and it provides the diagnostic specimen. The septic hip is drained surgically by arthrotomy and washout, and it is the non-negotiable surgical emergency of the disease. The knee and other large joints may be managed by arthroscopic washout or by serial needle aspiration, and the Malawian randomised trial of septic shoulder in children showed that needle aspiration was as effective as open arthrotomy for that joint — but the hip is never left to aspiration alone. [6] [3]
The empiric antibiotic is chosen to cover the likely organism by age, and it is given intravenously the moment the cultures are drawn. Staphylococcus aureus is covered in every child with intravenous flucloxacillin, given as twelve point five to twenty-five milligrams per kilogram every six hours, up to fifty milligrams per kilogram every six hours in severe infection. In the neonate under one month, gentamicin is added to flucloxacillin to cover group B streptococcus and Gram-negative bacilli, or cefotaxime replaces the gentamicin for broad Gram-negative cover. In the infant and young child under four years, a third-generation cephalosporin such as cefotaxime or ceftriaxone is added to flucloxacillin to cover Kingella kingae, with ceftriaxone given as fifty to eighty milligrams per kilogram once daily. In the older child over five years, flucloxacillin alone covers the dominant S. aureus and S. pyogenes, and where community-acquired meticillin-resistant S. aureus is prevalent, vancomycin or clindamycin is added. [9] [8]
The targeted therapy narrows the antibiotic once the organism and its sensitivities are known, and it streamlines the broad empiric cover to a single agent, the core of antimicrobial stewardship. The total duration of intravenous and oral therapy is three to four weeks for septic arthritis, with the intravenous component continued until the child is afebrile, clinically improved, and the inflammatory markers are falling — typically ten to fourteen days — followed by an oral step-down to complete the course at high oral bioavailability. The transition from intravenous to oral is made once the child is improving and the organism is sensitive to an oral agent, and the CRP and the clinical examination are tracked to confirm the response, with a rising or plateauing CRP prompting a search for persistent pus or resistant organism. [9] [10]
Specific Subtypes & Scenarios
Kingella kingae is the subtype that defines the under-four age group and that is most easily missed. It is a fastidious Gram-negative bacillus that colonises the oropharynx of young children and seeds the bloodstream to produce osteoarticular infections, and it is the commonest cause of septic arthritis in children between six months and four years. Its presentation is deceptively mild — a low or absent fever, modestly raised inflammatory markers, and a clinical picture that overlaps with transient synovitis — and it grows poorly on routine solid media, so standard cultures are often negative. The diagnosis is made by inoculating the synovial fluid into blood-culture bottles or by detecting the organism with a polymerase chain reaction assay, and Ceroni showed that an oropharyngeal swab PCR detects the organism in the carrier child with an osteoarticular infection. Kingella kingae is usually sensitive to beta-lactams, and a third-generation cephalosporin is the empiric cover of choice in the under-four. [7] [8]
Neonatal septic arthritis is the subtype that is hardest to recognise. The neonate presents with sepsis, irritability, or a pseudoparalysed limb rather than a localised hot joint, and multiple joints may be involved because the metaphyseal and synovial circulations communicate across the growth plate in this age group. The organisms reflect the neonatal bacteriology — Staphylococcus aureus, group B streptococcus, and Gram-negative bacilli — and the threshold to image and aspirate any suspicious joint is at its lowest. The outcome is often poor because the diagnosis is delayed and the growing joint is exquisitely vulnerable, so a febrile or irritable neonate with a limb held still is imaged and aspirated without hesitation. [5] [9]
The septic hip is the subtype that defines the surgical emergency. The intracapsular pressure of a pus-filled hip joint compresses the retinacular vessels supplying the femoral head, and avascular necrosis follows within hours to days, producing a permanent, crippling deformity. The hip is therefore drained by arthrotomy and washout, not managed by aspiration alone, and the urgency is measured against the femoral head blood supply, not the convenience of the theatre list. A confirmed septic hip goes to theatre as soon as the team can assemble, and the antibiotic and the analgesia are continued through the drainage. [3] [6]
The child with an underlying rheumatic disease or immunocompromise is the subtype where the differential widens and the organism list extends. A child on biological therapy for juvenile idiopathic arthritis may present with an infected joint alongside a disease flare, and the two are separated only by the synovial fluid. The immunocompromised child may be infected with unusual or fungal organisms, and the threshold for a synovial biopsy and extended cultures is lower. In each, the discipline is the same — aspirate, culture, drain, treat — but the organism list is broader and the clinical judgement is sharper. [9] [10]
Complications & Pitfalls
The complications of delayed or incomplete treatment are permanent and crippling. Articular cartilage destruction produces a stiff, painful joint with reduced range and early osteoarthritis. Avascular necrosis of the femoral head, the feared complication of the septic hip, produces a deformed head, a leg-length discrepancy, and a limp that persists for life. Growth arrest from damage to the physis produces a progressive leg-length discrepancy or angular deformity, and the younger the child, the greater the growth remaining and the greater the deformity. Progression to chronic osteomyelitis, recurrent sepsis, and the rare but real risk of death from overwhelming sepsis complete the burden. [5] [6]
The pitfall of reassurance is the commonest and the deadliest error. A febrile child with a limp is sent home with a diagnosis of transient synovitis, the Kocher criteria are not applied, the inflammatory markers are not measured, and the joint is not aspirated, and the child returns days later with a destroyed hip. The safeguard is the discipline of treating every febrile child with a swollen joint as septic until excluded, applying the Kocher and Caird criteria, and aspirating when the probability is two or more predictors or when the clinical picture is septic regardless of the score. The pitfall of over-investigation is less harmful but real — aspirating every irritable hip — and the criteria and the clinical judgement temper it. [1] [3]
The pitfall of the antibiotic-before-culture is the error that robs the team of the organism. An antibiotic given before the blood cultures and the joint aspiration sterilises the specimens and forces days of blind, broad-spectrum therapy, with all the harms of prolonged intravenous access, extended hospital stay, and antimicrobial resistance. The safeguard is the discipline of cultures-first, always, and in the deteriorating child the cultures are drawn and the aspiration done immediately before the antibiotic. The pitfall of the missed Kingella kingae is the child with a mild, culture-negative septic arthritis treated inadequately because the organism was not sought in the blood-culture bottle or by PCR. [4] [7]
The pitfall of the aspiration-only hip is the surgical error that costs the femoral head. A septic hip managed by needle aspiration alone, without arthrotomy and washout, does not decompress the intracapsular pressure reliably and does not remove the organised pus and the synovial debris, so the blood supply remains threatened and the head is lost. The safeguard is the rule that the septic hip is drained surgically, and the knee and other large joints may be managed by arthroscopic washout or serial aspiration. [6] [3]
Prognosis & Disposition
The prognosis of septic arthritis treated promptly and appropriately is good, with most children recovering full joint function if the joint is drained within twenty-four to forty-eight hours of onset and the organism is sensitive to the chosen antibiotic. The prognosis worsens with every day of delay, and the septic hip drained after forty-eight to seventy-two hours carries a substantial risk of avascular necrosis and permanent deformity. The CRP that falls by half within the first week is a favourable prognostic sign, and a CRP that plateaus or rises prompts a search for persistent pus, an undrained focus, or a resistant organism. [1] [3]
The long-term outlook depends on the joint and the age. The hip carries the worst prognosis because of the avascular necrosis risk, and the young child carries the greatest burden of growth-related deformity because of the years of growth remaining. The knee and the other large joints, drained early and treated appropriately, generally recover well. The child is followed until the joint is painless and mobile, the inflammatory markers have normalised, and the radiographs show no evidence of avascular necrosis or growth arrest — a follow-up of months to years for the hip, and weeks to months for the other joints. [5] [6]
The disposition is shared between the general paediatrician, who owns the recognition and the initial cultures and antibiotic, the orthopaedic surgeon, who owns the drainage of the hip and the surgical washout, and the infectious diseases and microbiology team, who own the organism identification and the antimicrobial stewardship. The child is admitted for the intravenous therapy and the surgical drainage, and the step-down to oral and the outpatient follow-up are coordinated by the paediatrician once the child is improving. The family is counselled on the diagnosis, the duration of therapy, the signs of recurrence, and the importance of completing the course and attending the follow-up imaging. [9] [10]
Special Populations
Neonates are the population in whom the disease is hardest to recognise and the outcome the worst. The presentation is sepsis, irritability, or a pseudoparalysed limb rather than a localised hot joint, multiple joints may be involved, and the diagnosis is often delayed. The organisms reflect the neonatal bacteriology — Staphylococcus aureus, group B streptococcus, Gram-negative bacilli, and occasionally Candida — and the empiric cover is flucloxacillin plus gentamicin or cefotaxime. The threshold to image and aspirate any suspicious joint is at its lowest in the neonate, because the growing joint is exquisitely vulnerable and the cost of delay is a lifetime of deformity. [5] [9]
Immunocompromised children are the population where the organism list extends and the clinical judgement sharpens. A child on chemotherapy, on biological therapy, or with a primary immunodeficiency may be infected with unusual or opportunistic organisms, and the threshold for a synovial biopsy and extended cultures including fungal and mycobacterial media is lower. The empirical cover is broadened, the infectious diseases team is involved early, and the distinction between an infected joint and a disease flare is made by the synovial fluid, not by the appearance. [9] [10]
Children in resource-limited settings bear the heaviest burden and the worst outcomes. Lavy's review of sub-Saharan African children documented septic arthritis presenting late, with multiple joints involved, a heavy burden of permanent disability, and limited access to imaging, surgery, and antibiotics. The Malawian randomised trial of aspiration versus arthrotomy for the septic shoulder showed that needle aspiration — cheap, available, and safe — was as effective as open surgery for that joint, and it offers a pragmatic drainage option where theatre access is limited. The fellowship answer acknowledges that access and timing, not biology, determine the outcome, and it advocates for the capacity to drain and to treat that prevents the disability. [5] [6]
Indigenous and socioeconomically disadvantaged children are over-represented in the burden of late-presenting septic arthritis, through the same pathways of crowding, limited primary care access, and delayed presentation that drive other infectious diseases of inequity. The recognition and the early drainage that protect the joint depend on access to care, and the fellowship answer frames the disease as one in which the social determinants shape the outcome as much as the organism. [5] [9]
Evidence, Guidelines & Regional Differences
The Kocher clinical prediction rule, derived in 1999 from a retrospective cohort at Boston Children's Hospital, is the taught framework for the probability of septic arthritis of the hip in children, identifying the four predictors and the rising probability with each. The 2004 validation by Kocher, Mandiga, and colleagues confirmed the discriminant performance in a separate cohort, and the 2006 prospective study by Caird, Flynn, and colleagues added the C-reactive protein and provided the important calibration caveat that the original probabilities may overestimate the true risk. These three papers frame the bedside decision of when to aspirate. [1] [2] [3]
The modern evidence-based reviews guide the empiric antibiotic and the duration. The 2020 narrative review by Autore, Bernardi, and Esposito summarised the recent recommendations for the diagnosis and the appropriate anti-infective therapy of acute bone and joint infections in children, emphasising the age-stratified organism list, the role of Kingella kingae, and the shorter intravenous durations enabled by early oral step-down. The 2025 antimicrobial stewardship study by Font and colleagues demonstrated that a structured stewardship programme shortened the intravenous duration and broadened the oral step-down without compromising the outcome, and it informs the contemporary practice of shorter, narrower courses. [9] [10]
The regional differences are modest in the framework but real in the organism list and the access. The Kocher criteria and the drainage principles apply globally, but the prevalence of community-acquired meticillin-resistant Staphylococcus aureus varies by region and shapes the empiric cover, with vancomycin or clindamycin added where the prevalence is high. The access to imaging, theatre, and antibiotics shapes the outcome more than the biology, and the resource-limited experience documented by Lavy and by Smith and colleagues offers pragmatic drainage options for the settings where open surgery is not available. The NICE guidance for the United Kingdom and the stewardship-informed practice for Australia and New Zealand frame the empiric cover and the durations for the fellowship answer. [5] [6]
Exam Pearls
The fellowship answer turns on five numbers. The Kocher predictors are a fever above thirty-eight point five, an inability to bear weight, an erythrocyte sedimentation rate above forty, and a white cell count above twelve thousand, with the Caird addition of a C-reactive protein above twenty. The synovial fluid cell count above fifty thousand with a neutrophil predominance supports sepsis, though no single threshold is absolute. The empiric antibiotic covers Staphylococcus aureus with flucloxacillin in every child, adds a third-generation cephalosporin for Kingella kingae in the under-four, and the total duration is three to four weeks with an oral step-down once the child improves. And the septic hip is always drained surgically by arthrotomy and washout. [1] [3]
The examiner probes three traps. The first is the febrile limping child sent home as transient synovitis — the Kocher criteria and the inflammatory markers separate the two, and the joint is aspirated when the probability is two or more predictors. The second is the culture-negative septic arthritis of the under-four — Kingella kingae is sought in the blood-culture bottle and by the oropharyngeal PCR, and a third-generation cephalosporin is the empiric cover. The third is the septic hip managed by aspiration alone — the intracapsular pus threatens the femoral head, and the hip is drained surgically. [1] [7]
The examiner rewards the candidate who frames the disease around the urgency and the stewardship. Cartilage destruction begins within hours, the femoral head blood supply fails under intracapsular pressure, and the drainage is measured against these clocks, not the theatre list. The cultures precede the antibiotic, the empiric cover narrows to the organism, and the intravenous duration shortens to the clinical and biochemical improvement — the discipline of antimicrobial stewardship that protects the child and the community. A candidate who shows this awareness demonstrates the systems thinking that the fellowship demands. [9] [10]
The four Kocher predictors — FEWW
References
- [1]Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction algorithm. J Bone Joint Surg Am, 1999.PMID 10608376
- [2]Kocher MS, Mandiga R, Zurakowski D, Barnewolt C, Kasser JR. Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am, 2004.PMID 15292409
- [3]Caird MS, Flynn JM, Leung YL, Millman JE, D'Italia JG, Dormans JP. Factors distinguishing septic arthritis from transient synovitis of the hip in children. A prospective study. J Bone Joint Surg Am, 2006.PMID 16757758
- [4]Li SF, Cassidy C, Chang C, Gharib S, Torres J. Diagnostic utility of laboratory tests in septic arthritis. Emerg Med J, 2007.PMID 17251607
- [5]Lavy CB. Septic arthritis in Western and sub-Saharan African children - a review. Int Orthop, 2007.PMID 16741731
- [6]Smith SP, Thyoka M, Lavy CB, Pitani A. Septic arthritis of the shoulder in children in Malawi. A randomised, prospective study of aspiration versus arthrotomy and washout. J Bone Joint Surg Br, 2002.PMID 12463664
- [7]Ceroni D, Dubois-Ferriere V, Cherkaoui A, Gesuele R, Combescure C, Lamah L, Manzano S, Hibbs J, Schrenzel J. Detection of Kingella kingae osteoarticular infections in children by oropharyngeal swab PCR. Pediatrics, 2013.PMID 23248230
- [8]Yagupsky P. Diagnosing Kingella kingae in Pediatric Chest Wall Infections. Pediatr Infect Dis J, 2023.PMID 36729685
- [9]Autore G, Bernardi L, Esposito S. Update on Acute Bone and Joint Infections in Paediatrics: A Narrative Review on the Most Recent Evidence-Based Recommendations and Appropriate Antinfective Therapy. Antibiotics (Basel), 2020.PMID 32781552
- [10]Font A, Aguera M, Rios-Barnes M, Gamell A, Moreno-Romo D, Lopez-Ramos MG, Monsonis M, Fumado V, Simo-Nebot S, Fontecha CG, Fortuny C, Echeverria-Esnal D, Noguera-Julian A, Velasco-Arnaiz E. Impact of paediatric antimicrobial stewardship program in haematogenous bone and joint infections. Eur J Pediatr, 2025.PMID 40527966