Paeds · rheumatology-musculoskeletal-and-sports
ANCA-associated and other childhood vasculitides
Also known as ANCA-associated vasculitis · Granulomatosis with polyangiitis · GPA · Wegener granulomatosis · Microscopic polyangiitis · MPA · Eosinophilic granulomatosis with polyangiitis · EGPA · Churg-Strauss syndrome · Takayasu arteritis · Childhood polyarteritis nodosa
Fellowship guide to ANCA-associated and other childhood vasculitides beyond IgA vasculitis. Covers the Chapel Hill 2012 vessel-size nomenclature that splits large-vessel Takayasu arteritis, medium-vessel Kawasaki disease and childhood polyarteritis nodosa, and small-vessel ANCA-associated disease. Details the three ANCA-associated vasculitides — granulomatosis with polyangiitis (PR3 or c-ANCA, destructive upper-airway and pulmonary-renal disease), microscopic polyangiitis (MPO or p-ANCA, necrotising glomerulonephritis and pulmonary capillaritis without granuloma), and eosinophilic granulomatosis with polyangiitis (asthma, eosinophilia, cardiac and nerve involvement). Reproduces the EULAR/PRINTO/PRES Ankara 2008 childhood GPA and Takayasu criteria, the SHARE recommendations, and the remission-induction regimens of rituximab or cyclophosphamide with glucocorticoids followed by maintenance therapy, alongside the Kawasaki cross-link of intravenous immunoglobulin and aspirin and the Takayasu pathway of glucocorticoids, biologics and revascularisation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A fourteen-year-old girl is brought in with a fortnight of epistaxis that will not stop, an ulcer on her nasal septum, a productive cough, and urine the colour of cola. She is pale and breathless. The nose is the clue, because the destruction is real — the bridge is starting to saddle, and the septum has a black-crusted ulcer. The chest radiograph shows two cavitating nodules, the urinalysis shows blood and protein with red-cell casts, and the creatinine is rising by the day. This is the pulmonary-renal syndrome of granulomatosis with polyangiitis, the prototypical ANCA-associated vasculitis, and it is one of the few diagnoses in paediatrics where a few days of delay costs the kidneys. [7][3]
The ANCA-associated vasculitides are a family of necrotising small-vessel vasculitides linked by a single mechanism: anti-neutrophil cytoplasmic antibodies that turn the neutrophil against the vessel wall. They are grouped into three diseases by their clinical face and their target antigen. Granulomatosis with polyangiitis, formerly Wegener granulomatosis, pairs granulomatous inflammation of the respiratory tract with the pulmonary-renal syndrome and a PR3 (cytoplasmic, c-ANCA) autoantibody. Microscopic polyangiitis drops the granuloma and keeps the necrotising glomerulonephritis and the pulmonary capillaritis, usually with an MPO (perinuclear, p-ANCA) autoantibody. Eosinophilic granulomatosis with polyangiitis, formerly Churg-Strauss syndrome, adds late-onset asthma and eosinophilia to the vasculitis, again usually MPO-positive. [3][6]
These three sit within the larger childhood vasculitis map defined by the 2012 Chapel Hill Consensus Conference, which sorts the vasculitides by the size of the vessel they injure. IgA vasculitis is the commonest and is covered in its own topic. This topic covers the rare but dangerous remainder: the ANCA-associated small-vessel diseases, the large-vessel Takayasu arteritis, and the medium-vessel diseases of Kawasaki disease and childhood polyarteritis nodosa that are the essential cross-links at the bedside. The naming matters, because the vessel size sets the organs at risk and the treatment. [3][8]
[6] [1]Classification
The classification that organises the whole topic is the vessel-size nomenclature agreed at the 2012 revised International Chapel Hill Consensus Conference. It groups the vasculitides by the predominant size of the vessel they injure, because the vessel size predicts the organs involved and the therapy. The large-vessel diseases involve the aorta and its major branches and include Takayasu arteritis. The medium-vessel diseases involve the main visceral arteries and their branches and include Kawasaki disease and childhood polyarteritis nodosa. The small-vessel diseases involve the arterioles, the capillaries and the venules, and they split into the ANCA-associated pauci-immune group and the immune-complex group that contains IgA vasculitis. [3]
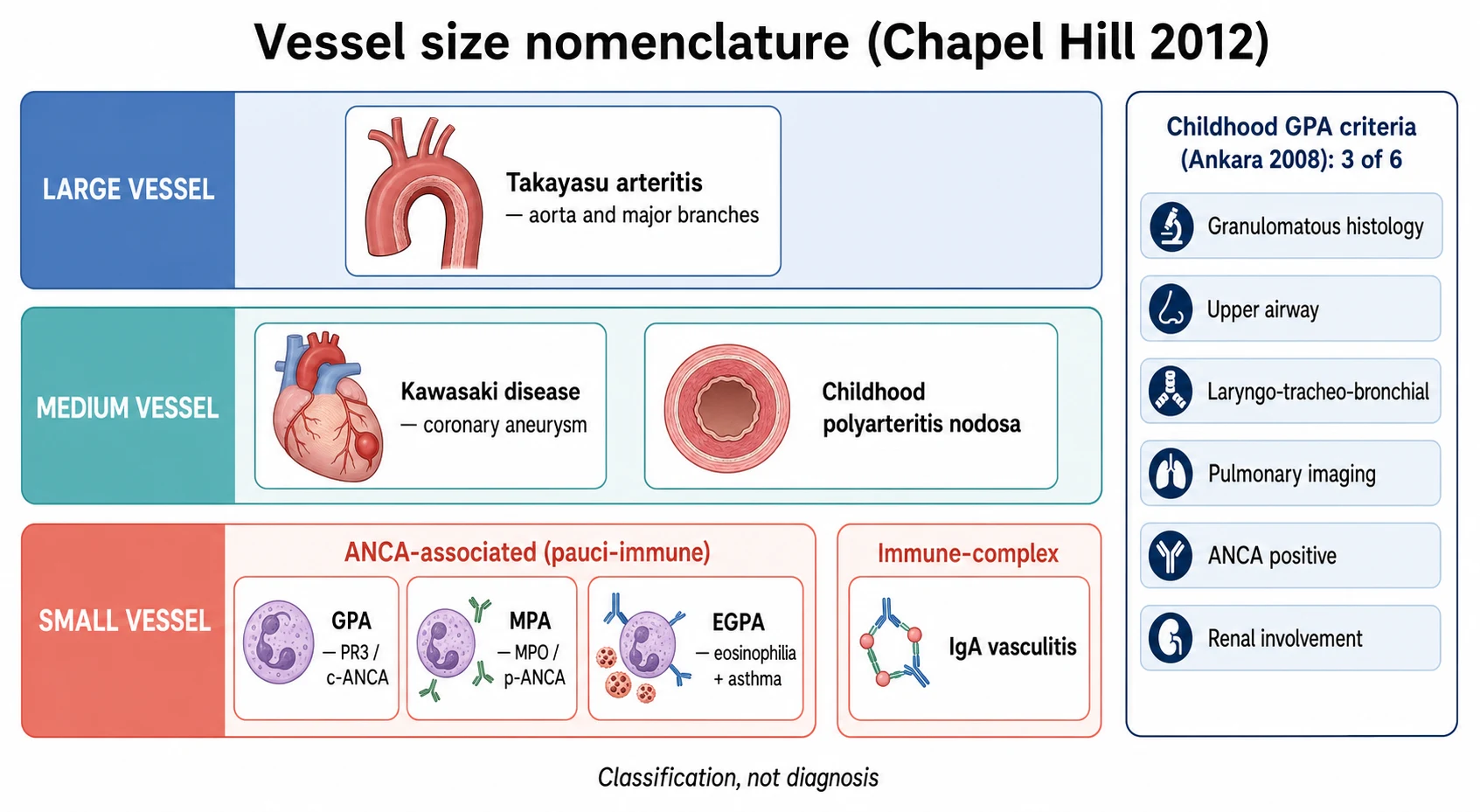
The small-vessel ANCA-associated group is the heart of this topic, and the discriminating axis is the autoantibody antigen and the presence of granuloma. Granulomatosis with polyangiitis is defined by granulomatous inflammation of the respiratory tract together with necrotising vasculitis and a PR3 autoantibody in most cases. Microscopic polyangiitis is defined by necrotising small-vessel vasculitis with few or no immune deposits and no granulomatous inflammation, usually with an MPO autoantibody. Eosinophilic granulomatosis with polyangiitis adds eosinophilia and asthma to the necrotising vasculitis and is MPO-positive in a minority. The shared histology is the pauci-immune pattern: fibrinoid necrosis of the vessel wall with little or no immunoglobulin deposition, which is what the term ANCA-associated implies. [3][10]
A parallel and complementary framework operates for the paediatric diseases, and it is the EULAR/PRINTO/PRES set agreed at Ankara in 2008 and published in 2010. It gives reproducible criteria for childhood granulomatosis with polyangiitis, childhood polyarteritis nodosa and childhood Takayasu arteritis. Childhood granulomatosis with polyangiitis is classified by three of six features: granulomatous histology, upper-airway involvement, laryngo-tracheo-bronchial involvement, pulmonary involvement on imaging, ANCA positivity, and renal involvement. Childhood Takayasu arteritis requires the mandatory angiographic abnormalities of the aorta and its branches, plus one of five features. The candidate who names both frameworks — Chapel Hill for the mechanism and PRINTO for the paediatric criteria — holds the classification. [1][2]
Epidemiology & Risk Factors
The ANCA-associated vasculitides are rare in children, and this rarity is itself the first point. The annual incidence of childhood-onset ANCA-associated vasculitis is roughly 1 to 2 per million children, and granulomatosis with polyangiitis is the commonest of the three, accounting for the majority of paediatric cases. The median age at onset in children is around twelve to fourteen years, and the diseases are rare before school age. There is a slight female or near-equal sex distribution in childhood granulomatosis with polyangiitis, in contrast to the male predominance seen in adults, and this difference is a small but examinable point. [6][7]
The risk factors cluster around a genetic susceptibility to the PR3 and MPO autoantibody response and an environmental trigger. The strongest genetic association of granulomatosis with polyangiitis is with the HLA-DP locus and the SERPINA1 gene that encodes alpha-1-antitrypsin, reflecting the PR3 antigen specificity, while microscopic polyangiitis and eosinophilic granulomatosis with polyangiitis associate more with HLA-DQ. The environmental triggers include silica and other airway irritants, chronic nasal carriage of Staphylococcus aureus, and certain drugs, of which the most important in paediatric practice is the propylthiouracil and the anti-thyroid drug class that can trigger an MPO-positive vasculitis. [6][7]
Takayasu arteritis carries a different epidemiology that the candidate should hold separately. It is a large-vessel vasculitis of the aorta and its main branches, and it is most common in adolescent girls and young women, with a striking predominance in East Asian, South Asian and Latin American populations. The childhood incidence is low, and the disease is uncommon before adolescence. Kawasaki disease, by contrast, is common, with an incidence of over 200 per 100,000 children under five in some East Asian populations, and it is covered in full in its own topic; the cross-link here is that Kawasaki is a medium-vessel, ANCA-negative disease, and the ANCA-positive child with a Kawasaki phenotype should redirect the diagnosis. [9][8]
Pathophysiology
The unifying mechanism of the ANCA-associated vasculitides is the anti-neutrophil cytoplasmic antibody turning the primed neutrophil against the vessel wall, and the cleanest way to hold it is as a five-step pipeline. The process begins with a priming event, usually an infection or an inflammatory stimulus, that brings the neutrophil granule proteins to the cell surface. The autoantibodies, directed against proteinase 3 in granulomatosis with polyangiitis or myeloperoxidase in microscopic polyangiitis and eosinophilic granulomatosis with polyangiitis, then bind these surface antigens. [3][10]
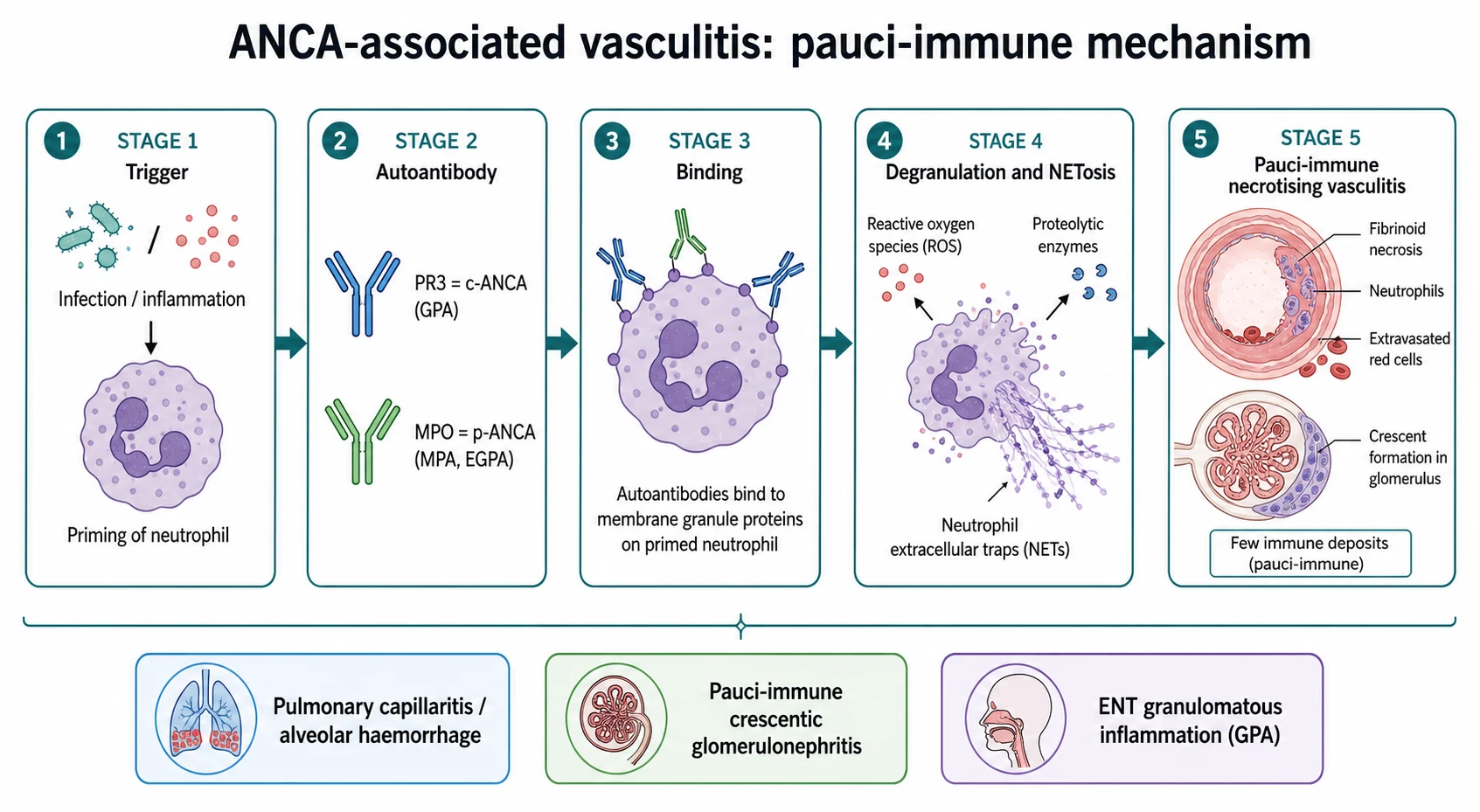
The bound antibody activates the neutrophil, which degranulates and releases its proteolytic enzymes and reactive oxygen species directly against the vessel wall. The neutrophil also undergoes NETosis, releasing neutrophil extracellular traps that deposit their histones and enzymes in the vessel wall and amplify the injury and the immune response. The result is the pauci-immune pattern: fibrinoid necrosis of the small-vessel wall, with little or no immunoglobulin deposition, accompanied by the crescent formation in the glomerulus when the kidney is involved. The pauci-immune label is the histological signature that separates the ANCA-associated diseases from the immune-complex small-vessel vasculitides such as IgA vasculitis. [3][10]
The clinical consequences follow the distribution of the small vessels and the antigen. The glomerular capillaries are injured in all three, producing the pauci-immune crescentic glomerulonephritis that is the renal emergency of the group. The pulmonary capillaries are injured in microscopic polyangiitis and granulomatosis with polyangiitis, producing the alveolar haemorrhage that, with the glomerulonephritis, forms the pulmonary-renal syndrome. The granulomatous inflammation of the upper and lower respiratory tract is the distinguishing feature of granulomatosis with polyangiitis, and the eosinophilic infiltration of the myocardium and the peripheral nerves is the distinguishing and dangerous feature of eosinophilic granulomatosis with polyangiitis. [3][7]
The large-vessel diseases operate by a different mechanism. Takayasu arteritis is a granulomatous vasculitis of the aorta and its main branches, driven by T-cell and macrophage infiltration of the vessel wall with granuloma formation, intimal proliferation and fibrosis that narrow the lumen and produce the pulse deficit and the ischaemia. Kawasaki disease is a medium-vessel vasculitis in which immune activation of the coronary and other medium-sized arteries produces the coronary aneurysm that defines its danger. Naming the mechanism by the vessel size is what lets the candidate predict the organ and the treatment. [9][8]
Clinical Presentation
Granulomatosis with polyangiitis presents with the destructive upper-airway disease first, because this is where it most often declares itself. The child has persistent, often bloody, nasal discharge, oral and nasal ulcers, and a septal perforation that can progress to the saddle-nose deformity. Subglottic stenosis causes stridor and is particularly characteristic of the childhood disease. The pulmonary involvement shows as nodules that often cavitate, as fixed infiltrates, or as alveolar haemorrhage with haemoptysis and dyspnoea. The renal involvement is the pauci-immune crescentic glomerulonephritis, with haematuria, proteinuria, red-cell casts and a rising creatinine. The combination of any two of these systems, especially the airway and the kidney, is the clinical face of the disease. [7][1]
Microscopic polyangiitis presents with the necrotising small-vessel vasculitis without the granuloma, and the kidney and the lung dominate. The renal disease is the presenting feature in most children, as a rapidly progressive glomerulonephritis with haematuria, proteinuria and acute kidney injury. The pulmonary involvement is the pulmonary capillaritis and the alveolar haemorrhage, which together with the glomerulonephritis forms the pulmonary-renal syndrome. The upper airway is spared, which is the bedside point that separates microscopic polyangiitis from granulomatosis with polyangiitis, and a skin purpura and a mononeuritis multiplex may accompany the renal and pulmonary disease. [7][10]
[7] [10]Eosinophilic granulomatosis with polyangiitis presents in its three classic phases, and the phases are the teaching structure. The prodromal allergic phase is the late-onset asthma and the allergic rhinitis that may precede the vasculitis by years. The eosinophilic phase is the marked peripheral eosinophilia and the eosinophilic tissue infiltration of the lung, the gut and the heart. The vasculitic phase is the necrotising vasculitis that produces the mononeuritis multiplex and the other organ disease. The cardiac involvement, the eosinophilic myocarditis and the coronary vasculitis, is the leading cause of death, which is why every child with eosinophilic granulomatosis with polyangiitis needs a troponin and an echocardiogram. [5][6]
Takayasu arteritis presents with the ischaemic consequences of large-vessel narrowing, and the presentation is often subtle and delayed. The adolescent girl has claudication of the limbs, a pulse deficit, a blood-pressure discrepancy of more than 10 mmHg between the limbs, bruits over the subclavian, carotid or abdominal arteries, or unexplained hypertension. Systemic features of fever, weight loss and fatigue are common at onset and reflect the active inflammation of the vessel wall. The renal artery stenosis and the aortic coarctation contribute to the hypertension, and the pulse deficit and the bruit are the bedside signs the candidate must actively seek. [9][6]
The Kawasaki disease cross-link is essential, because Kawasaki is the disease most often confused with the ANCA-associated vasculitides and it is treated very differently. Kawasaki disease presents with fever for five days or more, a polymorphous rash, conjunctival injection, oral changes, and extremity changes, and it threatens the coronary arteries with aneurysms. It is a medium-vessel, ANCA-negative disease, and the ANCA-positive child with a Kawasaki phenotype almost never has Kawasaki disease — this redirects the workup to the ANCA-associated vasculitides or to an alternative diagnosis. The treatment of Kawasaki is intravenous immunoglobulin and aspirin, not rituximab or cyclophosphamide, and the coronary surveillance is the long-term task. [8][11]
Differential Diagnosis
The first differential is the life-threatening one, and it sits within the pulmonary-renal syndrome itself. A child with haemoptysis and a rising creatinine has granulomatosis with polyangiitis, microscopic polyangiitis, anti-glomerular basement membrane disease, or a lupus nephritis with pulmonary haemorrhage until proven otherwise. Anti-glomerular basement membrane disease, Goodpasture syndrome, is separated by the anti-GBM antibody and the linear immunoglobulin G deposition on the renal biopsy, in contrast to the pauci-immune pattern and the ANCA of the vasculitides. Lupus nephritis is separated by the positive antinuclear antibody, the double-stranded DNA, the low complement, and the full-thickness immune-complex deposition on the biopsy. [7][10]
The destructive upper-airway disease has its own differential that the viva may probe. Recurrent or chronic bacterial sinusitis, a sinonasal lymphoma, a cocaine-induced midline destruction, and the natural killer or T-cell lymphoma of the nose can all mimic the destructive upper-airway disease of granulomatosis with polyangiitis. The discriminating tests are the PR3 (c-ANCA), the biopsy for the granuloma and the lymphoma, and the imaging. The cocaine-induced midline destruction is a particular trap, because it can produce a positive ANCA and a destructive nose, and the history is the discriminator; it does not need the cyclophosphamide. [6][7]
The medium- and large-vessel diseases carry their own differentials. Kawasaki disease is separated from the other febrile rashes of childhood by its five-day fever and its constellation of features, and from the ANCA-associated vasculitides by its ANCA negativity and its medium-vessel distribution. Childhood polyarteritis nodosa presents with fever, weight loss, livedo reticularis, tender nodules, myalgia, peripheral neuropathy and hypertension, with angiographic micro-aneurysms in the medium-sized arteries of the kidney and the gut. Takayasu arteritis is separated from the other causes of hypertension and pulse deficit in the adolescent, including coarctation of the aorta and the fibromuscular dysplasia, by the angiographic skip lesions of the aorta and its branches and the systemic inflammation at onset. [9][8]
Clinical & Bedside Assessment
Begin with the sick-or-well assessment, because the pulmonary-renal syndrome is the emergency that drives the tempo. The child with haemoptysis, dyspnoea and a rising creatinine is managed as the medical emergency, with the oxygen, the fluid balance, the urgent ANCA and the renal review, and the early induction therapy. The well-looking child with the chronic destructive upper-airway disease still needs the structured assessment, because the renal involvement can be silent and the creatinine can be climbing. [6][10]
The focused examination is built around the vessel size and the systems at risk. For the small-vessel ANCA-associated diseases, examine the upper airway for the crusting, the ulcers, the septal perforation and the saddle-nose deformity, and listen for the stridor of the subglottic stenosis. Examine the chest for the crackles and the consolidation of the alveolar haemorrhage, and perform the urinalysis for the blood and the protein that signal the glomerulonephritis. Examine the skin for the palpable purpura and the nodules, and the nervous system for the mononeuritis multiplex that is the signature of the eosinophilic and the microscopic diseases. [7][5]
For Takayasu arteritis, the examination is the four-limb blood pressure and the pulse assessment, and this is where the diagnosis is most often made or missed. Measure the blood pressure in all four limbs, feeling for the pulse deficit and the discrepancy of more than 10 mmHg between the limbs, and auscultate for the bruits over the subclavian, the carotid, the abdominal and the renal arteries. The absent or the weak pulse, the bruit and the unexplained hypertension in the adolescent girl are the bedside signs that demand the angiography. Do not attribute the hypertension of Takayasu to the essential or the renal causes until the large vessels have been examined. [9][6]
[9] [6]For the Kawasaki cross-link, the examination is the classic five-feature set of the prolonged fever, the conjunctival injection, the oral changes, the extremity changes and the polymorphous rash. The candidate should be able to state aloud that the Kawasaki phenotype with a positive ANCA is not Kawasaki disease and that the coronary aneurysm is the danger to exclude by the echocardiography. The synthesis is the problem representation, and the examiner listens for the vessel size, the systems involved, the ANCA result and the urgency in a single sentence. [8][11]
Investigations
The diagnosis rests on the autoantibody, the histology and the imaging, anchored by the clinical pattern. The anti-neutrophil cytoplasmic antibody is tested by the immunofluorescence and the enzyme-linked immunosorbent assay for the PR3 and the MPO antigens, and the antigen-specific assay is the more reliable of the two. The cytoplasmic pattern (c-ANCA) with the PR3 specificity points to the granulomatosis with polyangiitis, and the perinuclear pattern (p-ANCA) with the MPO specificity points to the microscopic polyangiitis and the eosinophilic granulomatosis with polyangiitis. A negative ANCA does not exclude the disease, because a minority of the biopsy-proven cases are ANCA-negative. [6][7]
The histology confirms the pauci-immune pattern and excludes the mimics. The renal biopsy shows the necrotising and crescentic glomerulonephritis with little or no immunoglobulin deposition, which separates the ANCA-associated disease from the immune-complex diseases and the anti-glomerular basement membrane disease. The upper-airway or the lung biopsy shows the necrotising granulomatous inflammation that is the defining feature of the granulomatosis with polyangiitis. The biopsy is not always needed when the clinical and the serological picture is classic, but it is performed when the diagnosis is uncertain or the mimics are in play. [10][7]
The laboratory panel grades the organ involvement and the activity. The full blood count may show the eosinophilia of the eosinophilic granulomatosis with polyangiitis or the anaemia of the chronic disease, and the urinalysis, the urine protein-to-creatinine ratio and the serum creatinine quantify the renal involvement. The acute-phase reactants, the C-reactive protein and the erythrocyte sedimentation rate are raised in the active disease and the Takayasu arteritis. The troponin and the echocardiogram are essential in the eosinophilic granulomatosis with polyangiitis to detect the eosinophilic myocarditis, and the echocardiogram is essential in the Kawasaki disease to detect the coronary aneurysm. [5][6]
The imaging is directed by the vessel size. The chest radiograph and the high-resolution computed tomography show the nodules, the cavities and the alveolar haemorrhage of the granulomatosis with polyangiitis and the microscopic polyangiitis. The computed tomography or the magnetic resonance angiography of the sinuses and the chest grades the upper-airway and the pulmonary disease. The angiography, by the conventional, the computed tomography or the magnetic resonance method, is the mandatory test for the Takayasu arteritis, showing the segmental wall thickening, the stenosis, the occlusion and the aneurysms of the aorta and its branches in the skip-lesion distribution. [9][6]
Management — Resuscitation
The first action is the recognition and the stabilisation of the pulmonary-renal syndrome, because this is the emergency that drives the outcome. The child with the alveolar haemorrhage receives the oxygen and the ventilatory support, and the child with the acute kidney injury receives the fluid and the electrolyte management and the renal review, with the dialysis for the refractory or the severe presentation. The induction therapy is started early, often before the biopsy, because the untreated pauci-immune crescentic glomerulonephritis can destroy the kidneys within days, and the cost of the early immunosuppression in the confirmed case is small against the cost of the delayed treatment. [6][10]
The first steps in the child with suspected ANCA-associated vasculitis
Stabilise the pulmonary-renal syndrome: oxygen for the alveolar haemorrhage, fluid and electrolyte management for the acute kidney injury, and renal review with dialysis for the refractory case
Send the urgent ANCA with the immunofluorescence and the PR3 and MPO enzyme-linked immunosorbent assay, the urinalysis, the creatinine, the troponin and the acute-phase reactants
Confirm the histology where feasible: the renal biopsy for the crescentic glomerulonephritis, the upper-airway or lung biopsy for the granuloma, to grade the injury and exclude the mimics
Start the remission induction for the organ or life-threatening disease with rituximab or cyclophosphamide plus glucocorticoids, in consultation with the paediatric rheumatology and nephrology
Exclude and treat the infection, the electrolyte and the acid-base disturbance, and counsel the family on the diagnosis, the immunosuppression and the long-term surveillance
The child with the severe eosinophilic granulomatosis with polyangiitis, especially with the eosinophilic myocarditis, is the second emergency, and the high-dose glucocorticoid is the first-line treatment. The echocardiography and the troponin are performed urgently, and the heart failure is managed by the cardiology. The child with the active Takayasu arteritis and the critical stenosis, especially of the renal or the carotid arteries, is managed for the hypertension and the ischaemia, with the glucocorticoid for the active inflammation and the revascularisation for the critical narrowing once the inflammation is controlled. [5][9]
Management — Definitive & Stepwise
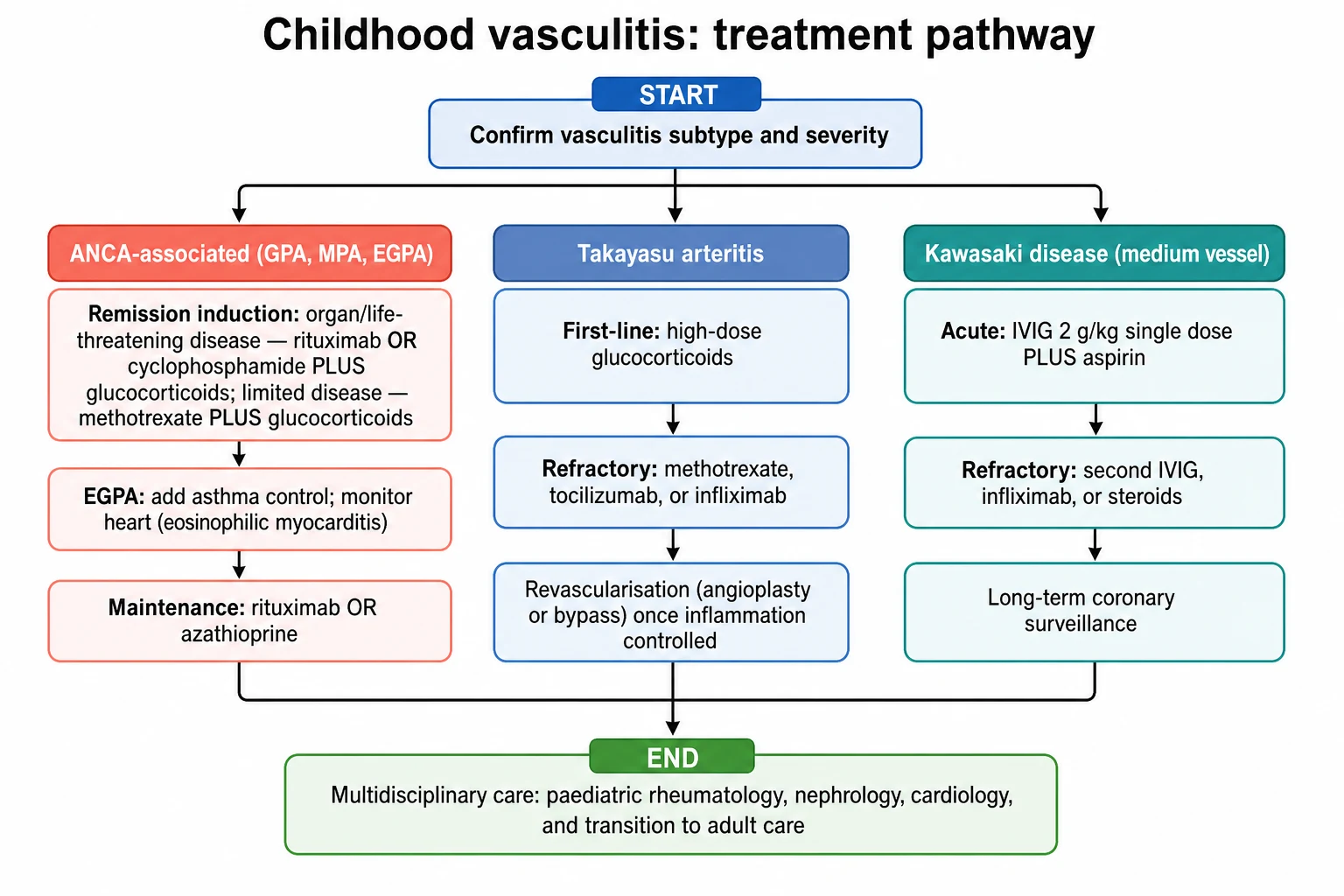
The definitive management of the ANCA-associated vasculitides is the remission-induction and the maintenance framework, and the cleanest way to hold it is as a ladder from the limited to the severe. At the top is the remission induction for the organ or life-threatening disease, which is rituximab or cyclophosphamide with the glucocorticoids. Below that is the limited-disease pathway of the methotrexate with the glucocorticoids. Below that is the maintenance therapy that prevents the relapse, and at the bottom is the long-term surveillance for the renal, the cardiac and the infection risk. [6][4]
[6] [8]For the organ or life-threatening ANCA-associated vasculitides, the remission induction is rituximab or cyclophosphamide with the glucocorticoids. Rituximab, at 375 milligrams per square metre per week for four weeks, depletes the B cells that produce the ANCA, and the cyclophosphamide, given as the intravenous pulse at 15 milligrams per kilogram or the oral dose at 2 milligrams per kilogram per day, suppresses the cellular immune response. The glucocorticoid, as the methylprednisolone pulse followed by the prednisolone at 1 to 2 milligrams per kilogram per day, controls the acute inflammation. The choice between rituximab and cyclophosphamide is guided by the phenotype, the fertility, the infection risk and the local protocol, and the rituximab is increasingly the first choice for the relapsing PR3-positive disease. [6][4]
Remission induction for ANCA-associated vasculitis
For the limited, non-organ-threatening granulomatosis with polyangiitis confined to the upper airway, the methotrexate at 15 to 25 milligrams per week with the glucocorticoids is an alternative to the cyclophosphamide, and it spares the cyclophosphamide toxicity. The eosinophilic granulomatosis with polyangiitis is treated with the glucocorticoids as the foundation, with the methotrexate, the mepolizumab (the anti-interleukin-5 biologic for the eosinophilic and the asthma phenotype) or the cyclophosphamide added for the organ or life-threatening disease or the refractory course. The plasma exchange is reserved for the severe renal failure or the alveolar haemorrhage, where its role remains debated and it is used selectively under the specialist guidance. [5][6]
The maintenance therapy prevents the relapse after the remission, and the disease is relapsing by nature, especially the PR3-positive granulomatosis with polyangiitis. The maintenance is the rituximab, given as the repeat infusion every six months, or the azathioprine at 1.5 to 2.5 milligrams per kilogram per day, continued for at least 18 to 24 months. The maintenance is essential because the relapse carries the risk of the further organ damage, and the candidate who names the induction and the maintenance in the same answer holds the framework. The trimethoprim-sulfamethoxazole has a limited role for the upper-airway disease, aimed at the Staphylococcus aureus carriage, and it is not a substitute for the immunosuppression. [6][4]
Takayasu arteritis is managed by a different pathway, because it is a large-vessel disease. The first-line therapy is the high-dose glucocorticoid, as the prednisolone at 1 to 2 milligrams per kilogram per day, tapered over months with the clinical and the inflammatory response. The refractory or the relapsing disease is treated with the methotrexate, the tocilizumab (the anti-interleukin-6 biologic) or the infliximab (the anti-tumour necrosis factor biologic), and the angioplasty or the surgical bypass is performed for the critical stenosis, especially of the renal or the carotid arteries, once the inflammation is controlled. The revascularisation in the active inflammation carries a high restenosis rate, which is why the inflammation is treated first. [9][6]
The Kawasaki disease cross-link is treated with the intravenous immunoglobulin and the aspirin, and this is the treatment the candidate must not confuse with the ANCA-associated therapy. The intravenous immunoglobulin is given at 2 grams per kilogram as a single infusion, with the aspirin at 30 to 50 milligrams per kilogram per day in the acute phase reduced to the antiplatelet dose of 3 to 5 milligrams per kilogram per day. The refractory Kawasaki disease is treated with the second intravenous immunoglobulin, the infliximab or the glucocorticoid, and the coronary surveillance by the echocardiography is the long-term task. [8][11]
Specific Subtypes & Scenarios
The child with the rapidly progressive glomerulonephritis is the subtype that the viva most often presents, because it is the renal emergency. The biopsy shows the crescentic, necrotising, pauci-immune glomerulonephritis, and the management is the urgent induction with the rituximab or the cyclophosphamide and the glucocorticoids, in partnership with the paediatric nephrology. The plasma exchange is considered for the severe presentation with the creatinine above the dialysis threshold or the alveolar haemorrhage. The candidate who names the urgency, the biopsy, the induction and the nephrology partnership holds the renal subtype. [10][6]
The child with the subglottic stenosis is the subtype that tests the candidate on the airway interface. The subglottic stenosis is particularly characteristic of the childhood granulomatosis with polyangiitis, and it may require the intralesional glucocorticoid and the endoscopic dilation alongside the systemic immunosuppression. The airway compromise is the surgical and the intensive-care interface, and the systemic disease is the rheumatology interface, and both run together. The candidate should name the dual approach and the risk that the airway disease can be the most refractory feature of the disease. [7][6]
The child with the eosinophilic granulomatosis with polyangiitis and the cardiac involvement is the subtype that carries the highest mortality, and it tests the candidate on the cardiac interface. The eosinophilic myocarditis and the coronary vasculitis present with the heart failure and the arrhythmia, and the troponin and the echocardiography are the essential tests. The management is the high-dose glucocorticoid and the early cyclophosphamide for the severe cardiac disease, and the heart failure is managed by the cardiology. The candidate who names the cardiac monitoring and the cardiac mortality holds the dangerous subtype. [5][6]
The adolescent with the Takayasu arteritis and the hypertension is the subtype that tests the candidate on the vascular interface. The hypertension is often driven by the renal artery stenosis or the aortic coarctation, and the angiography defines the anatomy. The glucocorticoid controls the active inflammation, and the revascularisation, by the angioplasty or the bypass, addresses the critical stenosis once the inflammation is controlled. The biologic, the tocilizumab or the infliximab, is added for the refractory or the relapsing disease, and the transition to the adult rheumatology and the vascular service is planned for the adolescent. [9][6]
Complications & Pitfalls
The acute complications are the alveolar haemorrhage, the rapidly progressive glomerulonephritis, the eosinophilic myocarditis and the airway compromise. The alveolar haemorrhage and the glomerulonephritis form the pulmonary-renal syndrome that is the emergency of the group, and the myocarditis is the leading cause of death in the eosinophilic granulomatosis with polyangiitis. The airway compromise, especially the subglottic stenosis, can require the intubation and the surgical intervention. These are the complications that drive the induction and the intensive care, and the candidate who names them in the order of their danger shows the judgement. [7][5]
The long-term complications are the chronic kidney disease and the end-stage renal failure, the coronary aneurysm and the ischaemic heart disease, and the vascular stenosis and the claudication. The chronic kidney disease follows the crescentic glomerulonephritis, concentrated in those with the severe or the relapsing renal disease, and the end-stage renal failure is the worst renal outcome. The coronary aneurysm follows the Kawasaki disease, and the vascular stenosis and the hypertension follow the Takayasu arteritis. The relapsing course, especially of the PR3-positive granulomatosis with polyangiitis, drives the cumulative damage, which is why the maintenance therapy and the surveillance are essential. [10][9]
Cabral 2016 ARChiVe: the paediatric phenotype of GPA and MPA
Population: Children with microscopic polyangiitis and granulomatosis with polyangiitis
Key finding
The childhood vasculitis cohort study compared 48 children with microscopic polyangiitis to 183 children with granulomatosis with polyangiitis. The granulomatosis with polyangiitis children had more upper-airway and pulmonary disease, and both diseases shared the necrotising glomerulonephritis. The study established that the paediatric phenotype differs from the adult, with more upper-airway and subglottic disease and less of the classic adult comorbidity, and it underpins the paediatric approach to the induction and the maintenance.
The principal pitfall is the delay in the diagnosis and the induction in the pulmonary-renal syndrome, because the untreated pauci-immune crescentic glomerulonephritis can destroy the kidneys within days. The child who is treated as the infection or the asthma, while the creatinine climbs, is the child whose kidneys are lost. The second pitfall is the over-reliance on the ANCA, because a minority of the biopsy-proven cases are ANCA-negative and a positive ANCA can occur in the other diseases and the infections, so the ANCA is read in the context of the clinical picture and the histology. The third pitfall is the confusion of the Kawasaki disease with the ANCA-associated vasculitis, which leads to the wrong treatment. [6][8]
The fourth pitfall is the failure to examine the four limbs in the adolescent with the hypertension, which misses the Takayasu arteritis. The fifth is the failure to monitor the eosinophilic myocarditis in the eosinophilic granulomatosis with polyangiitis, which misses the leading cause of death. The sixth is the failure to maintain the maintenance therapy, which courts the relapse and the cumulative damage. The seventh is the failure to screen and prevent the infection and the glucocorticoid toxicity during the immunosuppression, including the Pneumocystis prophylaxis, the bone health and the vaccination. [9][6]
Prognosis & Disposition
The prognosis of the ANCA-associated vasculitides has improved markedly with the rituximab and the cyclophosphamide era, and the great majority of the children with the organ or life-threatening disease achieve the remission with the prompt induction. The survival in the modern paediatric cohorts exceeds 90 per cent at five years, and the renal prognosis is set by the severity and the promptness of the treatment of the crescentic glomerulonephritis. The relapsing course, especially of the PR3-positive granulomatosis with polyangiitis, is the pattern that drives the maintenance and the surveillance, and the relapse rate is substantial without the maintenance. [6][10]
The prognosis of the eosinophilic granulomatosis with polyangiitis is set by the cardiac involvement, and the eosinophilic myocarditis and the coronary vasculitis are the leading causes of death. The cardiac prognosis is improved by the early high-dose glucocorticoid and the surveillance, and the asthma and the eosinophilia often persist and require the long-term management. The neuropathy of the mononeuritis multiplex is often slow to recover and may leave the residual deficit, which is part of the counselling. [5][6]
The prognosis of the Takayasu arteritis is set by the vascular damage, the hypertension and the ischaemic complications, and the disease is chronic and relapsing over the years. The early glucocorticoid and the biologic control the inflammation, and the revascularisation addresses the critical stenosis, but the restenosis and the progression are common, and the long-term surveillance and the transition to the adult care are essential. The hypertension and the renal artery involvement carry the renal and the cardiovascular risk over the lifespan. [9][6]
The disposition follows the severity and the subtype. The child with the pulmonary-renal syndrome or the eosinophilic myocarditis is admitted to the paediatric intensive care or the high-dependency unit for the induction and the organ support. The child with the active Takayasu and the critical stenosis is admitted for the blood-pressure control and the early revascularisation assessment. The child with the limited, stable disease is managed in the day-care or the outpatient setting, under the shared care of the paediatric rheumatology, the nephrology and the cardiology, with the transition to the adult care planned for the adolescent. [6][9]
Special Populations
The adolescent with the ANCA-associated vasculitis or the Takayasu arteritis is the population that tests the transition, because the disease is chronic and the immunosuppression is long-term. The adolescent is engaged directly in the adherence to the maintenance, the contraception during the teratogenic immunosuppression, the bone health during the glucocorticoid, and the transition to the adult rheumatology and nephrology. The failure mode in this age group is the loss to the follow-up and the relapse, which is why the structured transition and the adolescent-friendly care are essential. [6][9]
The child from the East Asian, the South Asian or the Latin American population carries a higher risk of the Takayasu arteritis and, for the Kawasaki disease, a higher incidence, and the cultural and the linguistic adaptation of the counselling is part of the care. The child from the socioeconomic disadvantage or the rural and the remote setting needs the access to the specialist rheumatology and nephrology services adapted to the distance, with the telehealth and the shared care with the local general paediatrician, because the delayed access to the induction and the maintenance is the barrier that worsens the outcome. [9][6]
[6] [9]The Indigenous populations of Australia and Aotearoa New Zealand carry a higher burden of the post-infectious and the inflammatory diseases, including the rheumatic fever and the glomerulonephritis, and the access to the specialist vasculitis care and the cultural safety are part of the management. The child with the comorbidity, including the chronic kidney disease or the immunocompromise, needs the tailored immunosuppression that balances the disease control against the infection and the drug-toxicity risk. The candidate who names the population and the access in the answer shows the breadth of the practice. [6][9]
Evidence, Guidelines & Regional Differences
The evidence base is anchored by the classification frameworks and the cohort and trial data. The EULAR/PRINTO/PRES Ankara 2008 criteria, published in 2010 by Ozen and colleagues in Part II and Ruperto and colleagues in Part I, give the paediatric classification for the childhood granulomatosis with polyangiitis, the childhood polyarteritis nodosa and the childhood Takayasu arteritis, validated with the high sensitivity and specificity in the PRINTO cohort. The Chapel Hill 2012 nomenclature, published by Jennette and colleagues in 2013, gives the vessel-size framework that unifies the vasculitides by the mechanism and the organ. [1][2][3]
The 2022 American College of Rheumatology and European Alliance classification criteria, published by Robson and colleagues for the granulomatosis with polyangiitis and Grayson and colleagues for the eosinophilic granulomatosis with polyangiitis, provide the contemporary classification validated against the vasculitis cohorts. The European consensus SHARE recommendations of de Graeff and colleagues in 2019 provide the contemporary framework for the diagnosis and the treatment of the rare paediatric vasculitides, and they are the primary reference for the induction and the maintenance in the children. The childhood cohort data of Cabral and colleagues in 2016 established the paediatric phenotype of the granulomatosis and the microscopic polyangiitis. [4][5][6][7]
The Kawasaki cross-link is anchored by the American Heart Association scientific statement of McCrindle and colleagues in 2017 and the SHARE Kawasaki recommendations of de Graeff and colleagues in 2019, which give the intravenous immunoglobulin and aspirin framework and the coronary surveillance. The Takayasu evidence rests on the cohort study of Brunner and colleagues in 2010 and the SHARE recommendations, which give the glucocorticoid, the biologic and the revascularisation framework. The renal review of Pop and colleagues in 2026 synthesises the renal involvement and the management of the paediatric small-vessel vasculitis. [8][9][10][11]
In Australia and Aotearoa New Zealand, the ANCA-associated vasculitides and the Takayasu arteritis are managed in the tertiary paediatric rheumatology services, in partnership with the nephrology and the cardiology, under the protocols aligned with the Chapel Hill 2012 nomenclature, the Ankara 2008 criteria and the SHARE recommendations. The remission induction is rituximab or cyclophosphamide with the glucocorticoids for the organ or life-threatening disease, and the maintenance is the rituximab or the azathioprine. The Kawasaki disease is treated with the intravenous immunoglobulin and aspirin. The Takayasu arteritis is treated with the glucocorticoids and the biologic, with the revascularisation for the critical stenosis. The transition to the adult rheumatology and nephrology is the long-term task.
The regional differences are modest, because the consensus is international, but the access to the tertiary paediatric rheumatology and nephrology is the variable that matters in the rural and the remote practice, and the telehealth and the shared care are the adaptations. The live controversy is the role of the plasma exchange in the severe renal and the alveolar haemorrhage, where the evidence is debated and the practice varies, and the choice between the rituximab and the cyclophosphamide for the induction, which is guided by the phenotype and the local protocol. The candidate who names the controversy and the consensus in the same answer shows the balance. [6][10]
Exam Pearls
The ANCA-associated vasculitides are rare, necrotising small-vessel vasculitides driven by the PR3 or MPO anti-neutrophil cytoplasmic antibodies, classified by the Chapel Hill 2012 vessel-size nomenclature and the EULAR/PRINTO/PRES Ankara 2008 childhood criteria. Granulomatosis with polyangiitis is the PR3-positive, c-ANCA-positive disease with the destructive upper-airway and the pulmonary-renal disease, classified in the child by three of the six Ankara features. Microscopic polyangiitis is the MPO-positive, p-ANCA-positive disease with the necrotising glomerulonephritis and the pulmonary capillaritis but no granuloma. Eosinophilic granulomatosis with polyangiitis adds the asthma, the eosinophilia and the cardiac and the nerve involvement. [3][1]
ANCA
The organ or life-threatening disease is treated with the remission induction of the rituximab at 375 milligrams per square metre per week for four weeks, or the cyclophosphamide, plus the glucocorticoids, followed by the maintenance of the rituximab or the azathioprine for at least 18 to 24 months. The pulmonary-renal syndrome is the emergency, and the untreated pauci-immune crescentic glomerulonephritis can destroy the kidneys within days. The eosinophilic granulomatosis with polyangiitis needs the troponin and the echocardiogram for the eosinophilic myocarditis, the leading cause of death. The candidate who names the induction, the maintenance and the surveillance holds the management. [6][5]
Takayasu arteritis is the large-vessel disease of the adolescent girl, with the absent pulse, the blood-pressure discrepancy, the bruit and the unexplained hypertension, and the angiographic skip lesions are mandatory for the diagnosis. The treatment is the high-dose glucocorticoid, with the biologic for the refractory disease and the revascularisation for the critical stenosis once the inflammation is controlled. The Kawasaki disease cross-link is the medium-vessel, ANCA-negative disease treated with the intravenous immunoglobulin at 2 grams per kilogram and the aspirin, and the coronary surveillance is the long-term task. [9][8]
[7] [10] [6] [9]References
- [1]Ozen S, Pistorio A, Iusan SM, et al EULAR/PRINTO/PRES criteria for Henoch-Schonlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: Ankara 2008. Part II: Final classification criteria. Ann Rheum Dis, 2010.PMID 20413568
- [2]Ruperto N, Ozen S, Pistorio A, et al EULAR/PRINTO/PRES criteria for Henoch-Schonlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: Ankara 2008. Part I: Overall methodology and clinical characterisation. Ann Rheum Dis, 2010.PMID 20388738
- [3]Jennette JC, Falk RJ, Bacon PA, et al 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum, 2013.PMID 23045170
- [4]Robson JC, Grayson PC, Ponte C, et al 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Granulomatosis With Polyangiitis. Arthritis Rheumatol, 2022.PMID 35106964
- [5]Grayson PC, Ponte C, Suppiah R, et al 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis With Polyangiitis. Arthritis Rheumatol, 2022.PMID 35106968
- [6]de Graeff N, Groot N, Brogan P, et al European consensus-based recommendations for the diagnosis and treatment of rare paediatric vasculitides - the SHARE initiative. Rheumatology (Oxford), 2019.PMID 30535249
- [7]Cabral DA, Canter DL, Muscal E, et al Comparing Presenting Clinical Features in 48 Children With Microscopic Polyangiitis to 183 Children Who Have Granulomatosis With Polyangiitis (Wegener's): An ARChiVe Cohort Study. Arthritis Rheumatol, 2016.PMID 27111558
- [8]McCrindle BW, Rowley AH, Newburger JW, et al Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association. Circulation, 2017.PMID 28356445
- [9]Brunner J, Feldman BM, Tyrrell PN, et al Takayasu arteritis in children and adolescents. Rheumatology (Oxford), 2010.PMID 20562196
- [10]Pop AA, Bot Rachisan AL, Botan E, et al Renal Involvement in Pediatric Small-Vessel Vasculitis: A Comprehensive Review of Clinical Impact, Diagnosis, and Management. Med Sci (Basel), 2026.PMID 42346872
- [11]de Graeff N, Groot N, Ozen S, et al European consensus-based recommendations for the diagnosis and treatment of Kawasaki disease - the SHARE initiative. Rheumatology (Oxford), 2019.PMID 30535127