Paeds · rheumatology-musculoskeletal-and-sports
Angular, rotational and gait variants
Also known as physiologic genu varum · physiologic bowlegs · physiologic genu valgum · knock knees · intoeing · in-toeing gait · metatarsus adductus · internal tibial torsion · femoral anteversion · pigeon-toed gait · torsional profile
A fellowship approach to the common physiologic variants of the growing lower limb — bow legs, knock knees, and intoeing — anchored by the Salenius and Vankka developmental curve, the Staheli rotational profile, and the skill of separating the symmetric, painless, age-appropriate variant that resolves spontaneously from the progressive, asymmetric, or painful limb that points to Blount disease, rickets, or a skeletal dysplasia.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A mother brings her two-year-old son because his legs are still bowed and he walks with his feet turning in — physiologic genu varum resolving into internal tibial torsion, two normal variants overlapping at the age where both are expected. A four-year-old girl is brought for knock knees so marked that her knees nearly touch when she walks — physiologic genu valgum at its peak, the age where it is most pronounced before it begins to resolve. An eight-year-old boy is referred because he still intoes and sits in a W — femoral anteversion nearing the end of its natural history. The task in each is to confirm the developmental age, to apply the rotational profile, and to separate the variant that resolves from the limb that does not. [1] [3]
The age-variant sequence — Bow, Knock, In
Overview & Definition
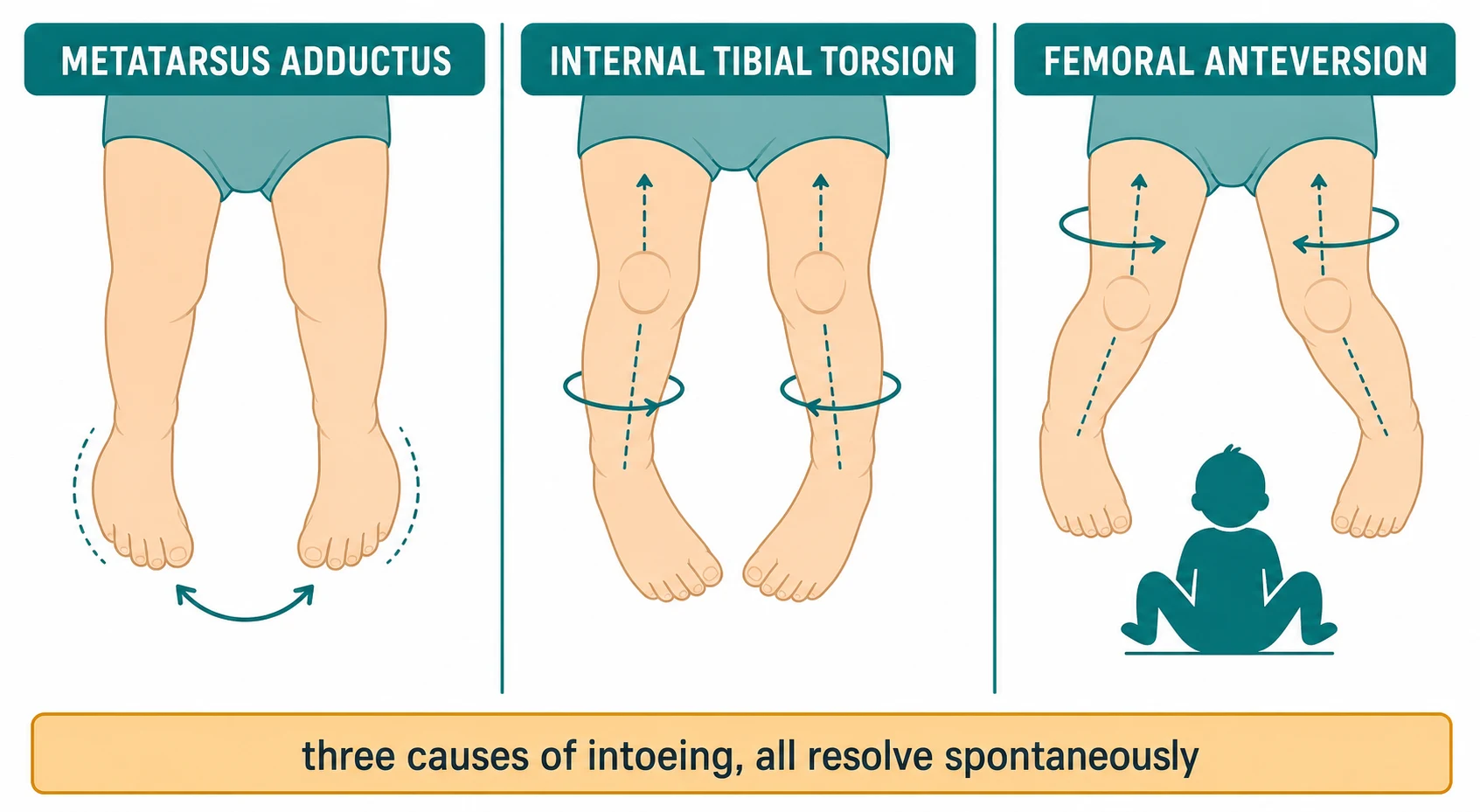
Angular, rotational, and gait variants are the common, painless, developmental patterns of the growing lower limb that a clinician sees in almost every well-child visit, and they are the patterns that most reliably separate the confident examiner from the one who over-investigates. The frontal-plane angular variants are bow legs, called physiologic genu varum, and knock knees, called physiologic genu valgum. The transverse-plane rotational variants are the three causes of intoeing: metatarsus adductus, internal tibial torsion, and femoral anteversion. Each has an expected age band, a benign natural history, and a small set of pathologic mimics that the assessment exists to catch. [3] [4]
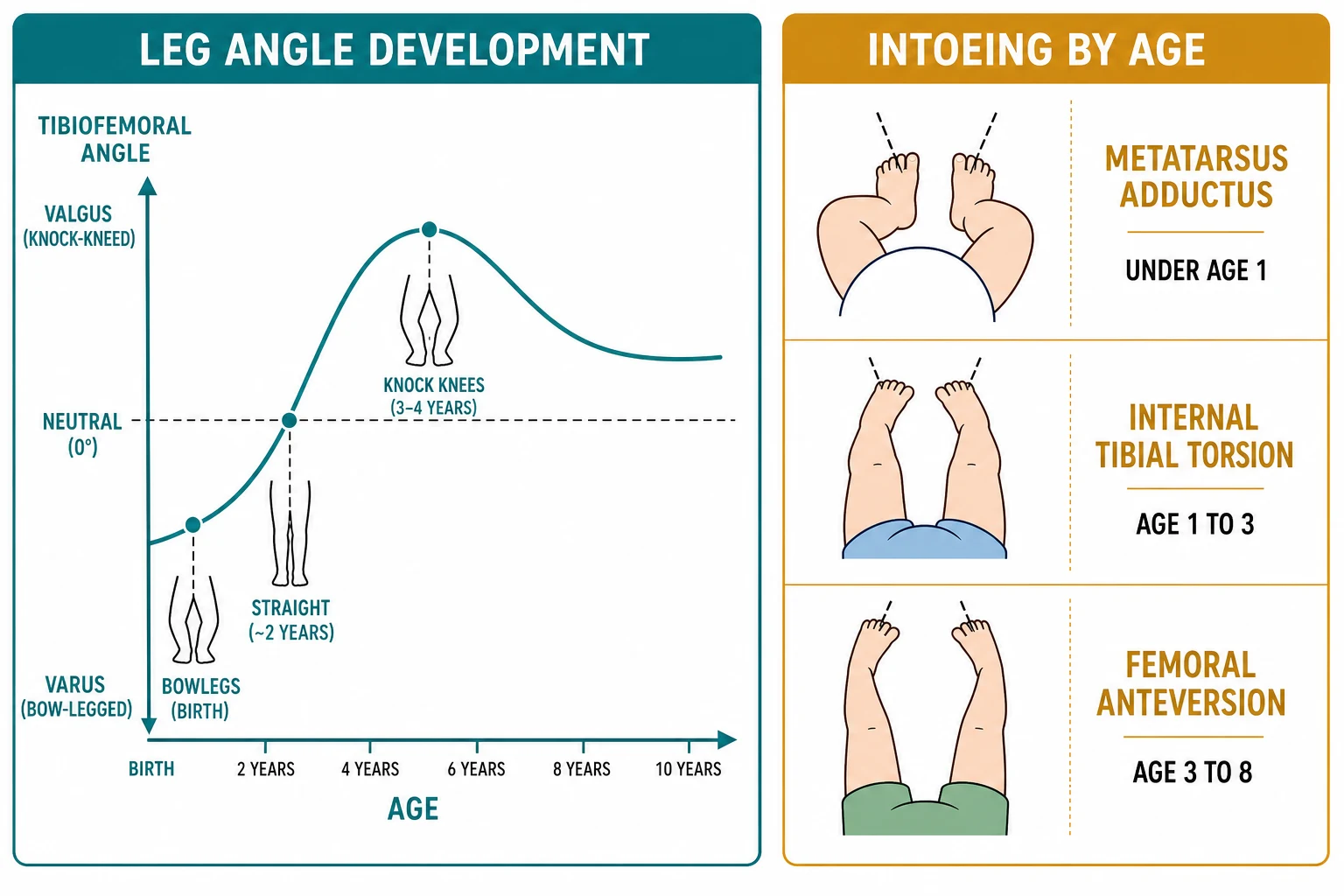
The unifying concept is the developmental curve. Salenius and Vankka measured the tibiofemoral angle in nearly fifteen hundred children and showed that the leg moves through a predictable arc from varus at birth to a peak valgus in the preschool years and back to a slight adult valgus by the early school-age years. A child seen at any point on this curve is showing a normal stage of growth, not a disease, and the clinician's job is to place the child on the curve and to confirm that the trajectory is the expected one. [1] [2]
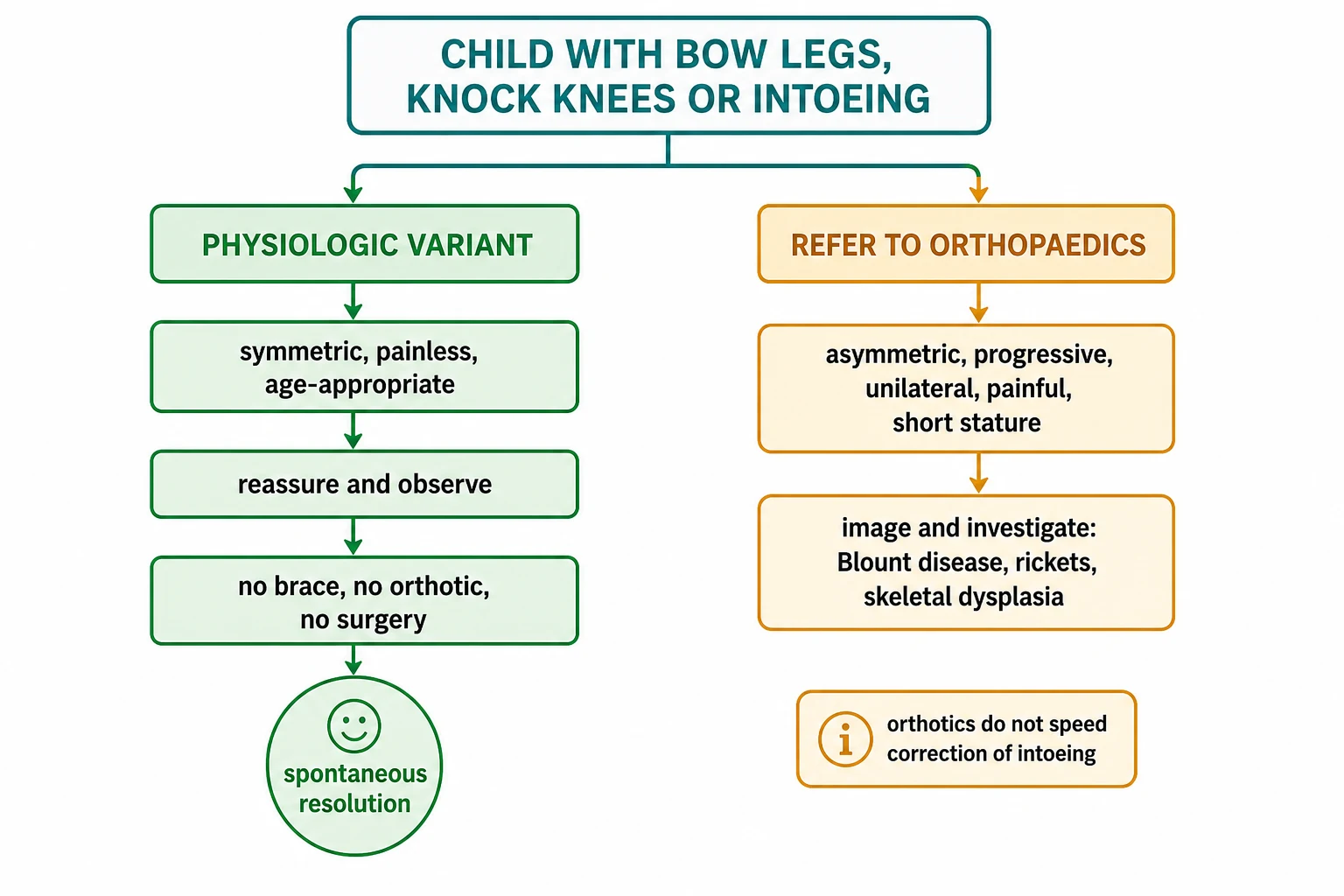
The clinical importance comes from what happens when the wrong label is applied. A child with a physiologic variant who is swept into braces, special shoes, and unnecessary imaging bears a cost in money, anxiety, and occasionally harm, while a child with Blount disease or rickets who is dismissed as a normal bowleg loses the window for the simple intervention that would have prevented a permanent deformity. The fellowship answer holds both risks at once and uses the developmental curve, the rotational profile, and the red-flag screen to place each child on the correct side of the line. [9] [11]
Classification
The variants are classified along two axes that together drive the assessment and the decision to observe or to refer. The first axis is the plane of the deformity: the frontal-plane angular variants change the angle between the thigh and the leg and produce bow legs and knock knees, while the transverse-plane rotational variants twist the limb around its long axis and produce intoeing. The second axis is the developmental age, because each variant belongs to an expected age band, and a finding outside its band is a reason to look harder. [3] [4]
The angular variants sit on the Salenius and Vankka curve. Physiologic genu varum is maximal at birth, with a tibiofemoral angle in the range of ten to fifteen degrees of varus, and it decreases through the second year to reach neutral around eighteen to twenty-four months. Physiologic genu valgum then develops, peaking at three to four years with an intermalleolar distance that may look striking, and it gradually resolves toward the adult valgus of five to seven degrees by seven to eight years. A child is placed on this curve by the age and the measured angle, and a trajectory that follows the curve is normal. [1] [2]
The rotational variants form their own ladder within the timeline, and the Staheli rotational profile is the tool that classifies them. Metatarsus adductus is a forefoot adductus of the infant, present at birth and resolving in the great majority within the first year or two. Internal tibial torsion is the commonest cause of intoeing in the toddler, peaking around the second year and resolving by four to five years. Femoral anteversion is the commonest cause of intoeing in the preschool and early school-age child, peaking around four to six years and resolving by eight to ten years. The foot progression angle ties the rotational profile to the gait that the family describes. [3] [5]
Epidemiology & Risk Factors
These variants are among the commonest reasons a family brings a child to the general paediatric clinic or the orthopaedic referral service, and their epidemiology is the epidemiology of normal growth. Nearly every infant is born with some bowing, and the knock-knee phase is so universal in the preschool years that it is regarded as a normal stage rather than a problem. The referral series of children sent to a paediatric orthopaedic centre for a diagnosis of intoeing confirmed that the great majority were physiologic variants needing no treatment, and the commonest error in the referral pathway was the over-use of corrective devices. [6] [4]
The risk factors for a physiologic variant are simply the age and the family history. A family history of bow legs, knock knees, or intoeing that resolved without treatment supports the physiologic label, because the inherited pattern of limb development tends to repeat across generations. Early walking does not cause intoeing, and the intrauterine packaging position shapes the newborn foot and the tibial torsion that then resolve with growth and weight-bearing. [3] [5]
The risk factors for a pathologic mimic cluster around the clinical picture and the background. Infantile Blount disease is more common in children who walk early, in children with obesity, and in some populations with a higher genetic predisposition, and it declares itself as a progressive asymmetric bowing after the first or second year. Rickets, whether nutritional from vitamin D deficiency or inherited, produces a symmetric bowing with short stature and the biochemical and radiographic signs of a disordered physis. Skeletal dysplasias and the focal bone lesions produce their own patterns, and the short stature, the asymmetry, or the dysmorphism is the clue that redirects the workup. [9] [11]
Pathophysiology
The pathophysiology of the physiologic variants is the pathophysiology of normal growth, and the mechanism in each is a controlled, symmetric remodelling of the growing bone. The newborn limb is packaged tightly in the uterus, and the resulting bowing and the inward torsion reflect the moulding of the soft cartilaginous bone rather than a structural defect. Once the child stands and walks, the mechanical load across the growth plates drives the remodelling, the varus resolves into neutral, and the limb then overshoots into a physiologic valgus before settling to the adult alignment. [1] [2]
The angular remodelling is driven by the growth plates at the distal femur and the proximal tibia, which respond to the load across them by growing asymmetrically until the mechanical axis is balanced. The Salenius and Vankka data showed that this remodelling is so reliable that even a severe early bowing or a marked knock-knee phase corrects without intervention in the typical child, and the natural-history follow-up confirmed that the spontaneous correction persists into adolescence. The growth plates do the work, and the clinician's task is to protect them from the unhelpful brace and the unnecessary surgery. [2] [3]
The torsional variants remould by a related mechanism, and each has its own site of correction. Metatarsus adductus corrects as the foot grows and the abductor muscles pull the forefoot outward, so a flexible forefoot that can be abducted past the midline resolves in roughly nine in ten infants without treatment. Internal tibial torsion corrects as the tibia derotates with growth and with the rotation imposed by walking and by sitting cross-legged, and the thigh-foot angle normalises by the early school-age years. Femoral anteversion corrects as the femoral neck derotates with growth, the medial hip rotation decreases, and the gait straightens by the end of the first decade. [4] [5]
The pathophysiology of the pathologic mimics is different in kind. In Blount disease, the medial proximal tibial growth plate is overloaded and fails, the medial cortex collapses, and the tibia angulates into a progressive varus that the growth plate cannot correct. In rickets, the unmineralised physis widens and the load across it bows the bone symmetrically, and the metabolic defect drives the deformity until the biochemistry is corrected. The fellowship skill is to recognise that a deformity driven by a failing growth plate or a metabolic defect does not sit on the developmental curve and does not resolve on its own. [9] [11]
Clinical Presentation
The presentation is driven by what the family sees, and the chief complaint is almost always the shape of the legs, the direction of the feet, or an unusual gait rather than a symptom of illness. The infant with metatarsus adductus is brought because the front of the foot turns inward and the outer border is curved. The toddler with internal tibial torsion is brought because the feet point inward on walking, the child trips, or the shoes wear unevenly. The preschool child with femoral anteversion is brought because the intoeing persists, the child sits in a W, or the family is anxious about the appearance and the teasing. [4] [6]
The presentation of the angular variants is the visible shape. The bowlegged toddler stands with the ankles apart and the knees close or touching, and the knock-kneed preschool child stands with the knees touching and the ankles apart. Neither child is in pain, and neither has a limp or a refusal to walk. The onset is gradual and noticed by the family, and the trajectory tracks the developmental curve. A child who is painful, who limps, or who has a sudden change is not showing a physiologic variant and is assessed for a different cause. [3] [4]
The presentation of the pathologic mimic differs in the details that the history must elicit. A child with Blount disease has a bowing that continues to worsen after the age when the physiologic varus should be resolving, and the bowing may be more marked on one side. A child with rickets has a symmetric bowing with a short stature, a delayed walking, and a dietary or a sunlight history that points to the vitamin D deficiency. A child with a skeletal dysplasia has a disproportionate short stature, a family history, and often other skeletal features. The history is built to find these clues. [9] [11]
Differential Diagnosis
The differential diagnosis of bow legs is the fork between physiologic genu varum and the pathologic bowing, and the age and the trajectory decide it. Physiologic genu varum is the normal bowing of the infant and the early toddler, and it improves through the second year. Infantile Blount disease is the progressive, often asymmetric bowing that appears or worsens after the first year in an early walker with risk factors, and the proximal tibial metaphyseal-diaphyseal angle above about eleven degrees on the radiograph supports the diagnosis. [9] [3]
Rickets, both nutritional and inherited, is the metabolic cause of symmetric bowing, and it presents with short stature, a widening of the wrists and the ankles, frontal bossing, and the radiographic widening and cupping of the growth plates. The focal causes — a post-traumatic tibial bowing, a fibrocartilaginous dysplasia, a bone lesion in neurofibromatosis, or an Ollier enchondromatosis — produce an asymmetric or a focal bowing that the imaging reveals. The fellowship answer names the physiologic variant, screens for Blount and rickets, and reserves the focal diagnosis for the radiograph. [11] [9]
The differential diagnosis of intoeing is the ladder of the three physiologic causes and the small set of pathologic mimics. Metatarsus adductus is separated from a clubfoot by the flexible hindfoot and the normal ankle dorsiflexion, and from a metatarsus primus varus by the lateral forefoot curve. Internal tibial torsion and femoral anteversion are separated from each other by the rotational profile, and both are separated from a pathologic cause by the symmetry, the absence of pain, and the normal hip examination that excludes a neuromuscular or a hip-driven intoeing. The referral series confirmed that the great majority of intoeing referred to a specialist centre was physiologic. [5] [6]
Clinical & Bedside Assessment
The assessment begins with the gait and the general inspection, performed with the child barefoot and in shorts so the whole limb is visible. Watch the child walk, run, and sit, because the intoeing that the family describes is best seen in the corridor, and the W-sitting reveals the femoral anteversion. Inspect the standing alignment from the front for the varus of the bowleg or the valgus of the knock knee, and inspect from behind for any asymmetry of the leg creases, the foot shape, or the limb length. [3] [4]
The angular measurement is the intercondylar and the intermalleolar distance. Measure the bowlegs with the child lying supine and the ankles touching, recording the intercondylar distance at the knees, and measure the knock knees with the knees touching, recording the intermalleolar distance at the ankles. These distances place the child on the curve and provide the baseline for the follow-up, and a photograph with the knees facing forward and the patellae aligned is a useful adjunct that the family can repeat at home. [4] [2]
The rotational profile is performed with the child prone, and it is the set of measurements that locates an intoeing on the limb. The foot progression angle relates the foot axis to the line of progression. The medial and the lateral rotation of the hip, measured with the pelvis flat and the knee flexed, reveal the femoral anteversion through an increased medial rotation. The thigh-foot angle, measured with the knee flexed and the foot hanging, reveals the tibial torsion, and a negative angle points to internal tibial torsion. The shape of the foot, with the curved lateral border and the heel bisector, reveals the metatarsus adductus. [3] [5]
Which findings must never be dismissed? An asymmetry, a progression, a pain, or a finding in the wrong age band redirects the assessment from reassurance to investigation. A short stature, a dysmorphism, or a delayed walking raises the metabolic or the dysplasia question. The hip examination is performed on every child, because an unrecognized hip problem can present as a gait change, and the neurological examination of the lower limbs excludes a neuromuscular cause of the apparent torsion. [4] [11]
Investigations
The investigation of the physiologic variant is the history and the examination, because the diagnosis is clinical and the imaging is avoided. A child whose variant sits on the developmental curve, is symmetric and painless, and carries no red flag needs no radiograph, no blood test, and no referral, and the imaging in this setting exposes the child to radiation and the family to anxiety without changing the management. The investigation is reserved for the child in whom a pathologic cause is suspected. [3] [4]
A single anteroposterior radiograph of the lower limbs, weight-bearing and with the patellae facing forward, is the first-line imaging when a pathologic bowing is suspected, and it is taken when the child is old enough to stand and the bowing is asymmetric, progressive, or in the wrong age band. The radiograph reveals the metaphyseal-diaphyseal angle of the proximal tibia, the medial beaking and the fragmentation of Blount disease, and the widened, cupped, and frayed physes of rickets, and it frames the mechanical axis that the varus or the valgus disrupts. [9] [3]
Bloods are taken when rickets is in the differential. The serum calcium, phosphate, alkaline phosphatase, parathyroid hormone, and vitamin D level frame the metabolic bone disease, and the pattern of a low or a normal calcium with a low phosphate and a high alkaline phosphatase supports the nutritional deficiency. The biochemistry is interpreted with the radiograph, because the two together confirm the rickets and separate it from the inherited forms. A child with a confirmed metabolic bone disease is referred to the endocrine team alongside the orthopaedic assessment. [11] [4]
Management — Resuscitation
Resuscitation is not the task in the child with a physiologic variant, because these are painless, well children with no threat to life or limb, and the encounter is an outpatient or a well-child encounter. The rare exception is the child who is referred with a suspected acute limb problem that turns out to have a serious underlying cause, and in whom the priority is the recognition of the red flag and the arrangement of the imaging and the referral rather than any bedside manoeuvre. The harm in this topic is the harm of omission — the missed Blount or rickets — and it is prevented by the assessment, not by a resuscitation step. [9] [11]
The child with a suspected metabolic bone disease and a hypocalcaemic complication, such as a seizure or a cardiac arrhythmia, is the rare emergency that the rickets assessment may surface, and the priority is the recognition of the low calcium and the urgent biochemical correction alongside the paediatric and the endocrine teams. This is uncommon, but the fellowship candidate holds it as the one situation in this topic where the acute stabilisation precedes the developmental reassurance. [11] [4]
Management — Definitive & Stepwise
The definitive management of the physiologic variant is observation, reassurance, and a safety-net, and the evidence is clear that no device speeds the correction. The family is counselled on the developmental curve, the expected timeline, and the natural history, and the child is reviewed at the interval that matches the variant — six to twelve months for the angular variant, and annually for the femoral anteversion until it resolves. The reassurance is the treatment, and the photograph and the measurement at each visit document the trajectory. [2] [6]
The definitive management of metatarsus adductus is guided by the flexibility. The flexible forefoot, which the examiner can abduct past the midline, resolves without treatment in the great majority of infants, and the family is taught gentle passive stretching. The rigid or the partially correctable forefoot, which cannot be abducted to the midline, is referred for serial casting in the first year, and the rare resistant case is considered for a foot orthosis or a rare surgical release. The flexible-rigid distinction is the decision point that separates the reassured from the referred. [3] [4]
The definitive management of internal tibial torsion and femoral anteversion is observation, because both resolve with growth, and the orthotic and the special-shoe literature confirms that these devices do not improve the outcome. The Denis Browne bar, the twister cables, and the wedged shoes were once common, and the contemporary evidence reserves them for the rare, severe, persistent case in the older child, and even there their benefit is marginal. The surgical derotation osteotomy is reserved for the rare child older than about eight to ten years with a severe, persistent torsion that causes a functional or a cosmetic problem, and the decision is made with the orthopaedic team. [8] [3]
The three variants and their first management
Specific Subtypes & Scenarios
Physiologic genu varum is the subtype that defines the bowlegged infant and toddler. The child is born with a tibiofemoral angle in the range of ten to fifteen degrees of varus, the bowing is symmetric and painless, and the angle decreases through the second year to reach neutral by eighteen to twenty-four months. The family is reassured with the curve, the child is reviewed at six to twelve months, and a bowing that is still increasing after two years, or that is asymmetric, is referred for the radiograph that excludes Blount disease. [1] [9]
Physiologic genu valgum is the subtype that defines the knock-kneed preschool child. The valgus develops after the second year, peaks at three to four years with an intermalleolar distance that may look striking, and resolves toward the adult valgus by seven to eight years. The family is reassured, the distance is measured and recorded, and a knock knee that is severe, progressive after four years, or persistent beyond seven years is referred for the measurement and the imaging that guide the orthopaedic decision. [2] [3]
Metatarsus adductus is the intoeing of the infant, and the flexibility is the key. The forefoot is adducted, the lateral border is curved, and the heel bisector points medial to the second toe. The flexible forefoot resolves without treatment in the great majority, the rigid forefoot is cast in the first year, and the rare resistant case is referred to the paediatric orthopaedic foot service. The condition is distinguished from the clubfoot by the flexible hindfoot and the normal ankle dorsiflexion, and the distinction is made at the bedside. [3] [4]
Infantile Blount disease is the pathologic subtype that the bowleg assessment exists to catch. The child, often an early walker with risk factors, develops a progressive and often asymmetric bowing after the first or second year, and the radiograph reveals the proximal tibial metaphyseal-diaphyseal angle above about eleven degrees, the medial beaking, and the fragmentation of the medial growth plate. The early disease may be braced, the progressive disease is treated with an osteotomy, and the adult-function follow-up confirms that the childhood deformity leaves a lasting burden when it is treated late. [9] [10]
Complications & Pitfalls
The complications of this topic are the harms on both sides of the line. The harm of over-treatment is the brace, the special shoe, and the unnecessary imaging applied to a physiologic variant, and it costs the family money and anxiety, it exposes the child to radiation, and it occasionally applies a device that is uncomfortable or that interferes with play. The contemporary orthotic literature confirms that these devices do not speed the correction of intoeing, and the stewardship of the consultation is to remove them from the management of the typical child. [8] [6]
The harm of under-treatment is the missed Blount disease or the missed rickets. A child with a progressive bowing that is dismissed as a normal bowleg loses the window for the brace or the early osteotomy that would have prevented a permanent deformity, and the adult-function study of Blount disease confirmed the lasting burden of the late-treated case. The safeguard is the red-flag screen applied to every child, the recognition that a bowing in the wrong age band or with an asymmetry is not physiologic, and the weight-bearing radiograph taken when the suspicion is raised. [9] [10]
The pitfall of the reassuring label is the error that the red-flag screen prevents. A child with a metabolic bone disease who is reassured as a normal bowleg continues to bow while the vitamin D deficiency goes untreated, and the safeguard is the short-stature check, the dietary history, and the biochemistry that the rickets suspicion triggers. The pitfall of the missed hip or neurological cause of an apparent intoeing is the related error, and the safeguard is the hip and the lower-limb neurological examination performed on every child with a torsional complaint. [11] [4]
Prognosis & Disposition
The prognosis of the physiologic variants is excellent, and the resolution is the rule. Physiologic genu varum resolves to neutral by the second year, physiologic genu valgum resolves to the adult valgus by seven to eight years, and the three causes of intoeing resolve on their age-appropriate timelines — metatarsus adductus in infancy, internal tibial torsion by four to five years, and femoral anteversion by eight to ten years. A child placed on the curve and observed resolves without treatment in the great majority, and the residual adult alignment is the slight valgus that is normal. [2] [7]
The prognosis of the pathologic mimics depends on the early recognition and the cause. Infantile Blount disease treated early, with a brace in the early lesion and an osteotomy in the progressive lesion, has a better outcome than the late-treated case, and the adult-function study confirmed that the childhood deformity leaves a lasting burden when it is treated late. Rickets treated with the correction of the metabolic defect halts the bowing and allows the growth plate to remodel, and the residual deformity is determined by the severity and the age at treatment. [10] [11]
The disposition is shared between the general paediatrician, the paediatric orthopaedic surgeon, and the endocrine team. The general paediatrician owns the initial assessment, the placement on the developmental curve, the rotational profile, and the safety-net review of the physiologic variant. The paediatric orthopaedic surgeon owns the Blount disease, the severe or the persistent knock knee, and the rare severe persistent torsion that needs a derotational osteotomy. The endocrine team owns the metabolic bone disease. The fellowship answer names the right specialist for the right diagnosis and never holds a child with a red flag in the observe-and-reassure pathway. [9] [11]
Special Populations
Children with developmental disability and neuromuscular conditions present particular challenges in the lower-limb assessment. A child with cerebral palsy or a myelomeningocele may have a torsional or an angular deformity driven by the muscle imbalance rather than by the normal growth, and the developmental curve does not apply in the same way. The threshold for the orthopaedic referral is lower, and the assessment is integrated with the physiotherapy and the orthotic service that the neurodisability team coordinates. [3] [4]
Indigenous, remote, and socioeconomically disadvantaged children face the additional burden of the rickets risk. Nutritional rickets remains more common in children with a dark skin, a restricted diet, and a low sunlight exposure, and the remote and the disadvantaged settings carry a higher prevalence of the vitamin D deficiency that drives the symmetric bowing. The dietary and the sunlight history is taken with this in mind, the biochemistry is checked when the suspicion is raised, and the public-health vitamin D supplementation is the population-level intervention that the fellowship answer acknowledges. [11] [4]
The newly arrived migrant or refugee child may have an undocumented history and a higher prevalence of the nutritional and the inherited bone disease, and the workup considers the metabolic cause in the child with a symmetric bowing and a short stature. The family may carry a strong cultural expectation of treatment, and the counselling that explains the natural history of the physiologic variant is delivered with the interpreter and the cultural respect that the encounter demands. The fellowship candidate does not close the lower-limb assessment at the alignment measurement. [11] [3]
Evidence, Guidelines & Regional Differences
The evidence base for the physiologic variants rests on the developmental-curve studies of Salenius and Vankka. The 1975 paper measured the tibiofemoral angle in nearly fifteen hundred children and established the arc from varus at birth through peak valgus at three to four years to the adult valgus by seven to eight, and the 1982 follow-up confirmed that even the severe early deformity corrects spontaneously in the typical child. These studies frame the fellowship task: place the child on the curve, confirm the trajectory, and observe the physiologic variant. [1] [2]
The evidence for the torsional variants and their natural history rests on the clinical reviews of Bruce, Sass and Hassan, and Kahf. The Bruce review framed the torsional and the angular deformities around the rotational profile, the Am Fam Physician paper translated the assessment for the primary-care setting, and the Kahf review set out the approach to the paediatric rotational limb deformity. The Staheli group contributed the evidence that intoeing does not impair the athletic function, with the sprinting study showing that the intoeing child runs as well as the non-intoeing child. [3] [7]
The evidence for the over-treatment of intoeing rests on the referral series and the orthotic evaluation. The Faulks series of children referred to a paediatric orthopaedic centre for intoeing confirmed that the great majority were physiologic and that the commonest error was the over-use of corrective devices, and the recent orthotic evaluation found no benefit of the orthoses in the in-toeing or the out-toeing gait. The evidence for Blount disease rests on the StatPearls review and the Makarov adult-function study, which confirmed the lasting burden of the late-treated deformity, and the rickets position statement frames the metabolic management. [6] [8]
The regional differences are modest but real. The prevalence of nutritional rickets varies with the skin pigmentation, the diet, the sunlight, and the latitude, and the threshold for the vitamin D check is set by the local epidemiology. The thresholds for the Blount bracing and the osteotomy, and for the rare derotational osteotomy of the persistent torsion, are broadly consistent across the regions and are set by the paediatric orthopaedic team. The fellowship answer names the local guideline and the local epidemiology without pretending that a single algorithm resolves every consultation. [11] [9]
Exam Pearls
The fellowship answer turns on five facts. Most bow legs, knock knees, and intoeing in young children are normal developmental variants that resolve spontaneously. The Salenius and Vankka curve runs from varus at birth through peak valgus at three to four years to the adult valgus by seven to eight. The three causes of intoeing march through the age bands in order — metatarsus adductus in the infant, internal tibial torsion in the toddler, and femoral anteversion in the older child. No brace, special shoe, or orthotic speeds the correction of intoeing. And the red flags — progressive, asymmetric, unilateral, painful, or in the wrong age band — move the child off the developmental curve and into the investigative pathway for Blount disease, rickets, or a skeletal dysplasia. [1] [8]
The examiner probes three traps. The first is the over-treated intoeing — a child placed in a brace or a special shoe that the evidence does not support, and the safeguard is the knowledge that the devices do not speed the correction. The second is the missed Blount disease — a progressive bowing dismissed as a normal bowleg, and the safeguard is the recognition that a bowing in the wrong age band, with an asymmetry or a proximal tibial angle above about eleven degrees, is referred for the radiograph. The third is the missed rickets — a symmetric bowing with a short stature dismissed as a normal variant, and the safeguard is the dietary history, the short-stature check, and the biochemistry. [9] [11]
The examiner rewards the candidate who frames the lower-limb variant as a developmental-reasoning exercise rather than a list. The child is placed on the developmental curve, the rotational profile is performed, the red-flag screen is run, the physiologic variant is observed and reassured, and the pathologic mimic is referred. A candidate who shows this safety and this stewardship — the confident reassurance and the vigilant screen — demonstrates the systems thinking that the fellowship demands. [1] [3]
References
- [1]Salenius P, Vankka E. The development of the tibiofemoral angle in children. J Bone Joint Surg Am, 1975.PMID 1112851
- [2]Vankka E, Salenius P. Spontaneous correction of severe tibiofemoral deformity in growing children. Acta Orthop Scand, 1982.PMID 7102273
- [3]Bruce RW Jr. Torsional and angular deformities. Pediatr Clin North Am, 1996.PMID 8692584
- [4]Sass P, Hassan G. Lower extremity abnormalities in children. Am Fam Physician, 2003.PMID 12924829
- [5]Kahf H, Kesbeh Y, van Baarsel E, Patel V. Approach to pediatric rotational limb deformities. Orthopedic Reviews, 2019.PMID 31579218
- [6]Faulks S, Brown K, Birch JG. Spectrum of Diagnosis and Disposition of Patients Referred to a Pediatric Orthopaedic Center for a Diagnosis of Intoeing. J Pediatr Orthop, 2017.PMID 28471818
- [7]Fuchs R, Staheli LT. Sprinting and intoeing. J Pediatr Orthop, 1996.PMID 8784703
- [8]Bollepalli H, White CJK, Kodra JD, Liu XC. An Evaluation of Orthotics on In-Toeing or Out-Toeing Gait. Healthcare (Basel), 2025.PMID 40077093
- [9]Shah S, Taqi M, De Leucio A. Blount Disease. StatPearls Publishing, 2026.PMID 32809758
- [10]Makarov MR, Polk JL, Shivers CR, Jo CH. Clinical and Radiographic Assessment of Adult Function After Blount Disease in Childhood: An Exercise in Futility. J Pediatr Orthop, 2023.PMID 37493033
- [11]Baroncelli GI, Comberiati P, Aversa T, Baronio F. Diagnosis, treatment, and management of rickets: a position statement from the Bone and Mineral Metabolism Group of the Italian Society of Pediatric Endocrinology and Diabetology. Front Endocrinol (Lausanne), 2024.PMID 38706696