Paeds · rheumatology-musculoskeletal-and-sports
Bone pain and malignancy red flags
Also known as night pain · bone pain in children · leukaemia presenting as bone pain · childhood leukaemia mimicking arthritis · osteosarcoma · Ewing sarcoma · primary malignant bone tumour · metaphyseal lucent bands · leukaemic lines · Codman triangle · delayed cancer diagnosis in children · growing pains differential
A fellowship approach to paediatric bone pain and the red flags that signal malignancy: separating the child whose limb pain is benign growing pain or transient synovitis from the child harbouring leukaemia, osteosarcoma, or Ewing sarcoma. Anchored on the Cabral and Tucker and Jones multicentre studies that distinguish childhood leukaemia from juvenile idiopathic arthritis, the radiographic leukaemic lines of Tafaghodi, the epidemiology and survival of the primary bone tumours from SEER and EURAMOS-1, and the delayed-diagnosis lesson of George and Grimer that an unplanned excision or a missed night pain costs a child their prognosis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A six-year-old boy has three weeks of deep right thigh pain that now wakes him at two in the morning, he is tired and pale, and his mother has noticed some bruises — acute lymphoblastic leukaemia, and the limping child pathway must not stop at transient synovitis. A fifteen-year-old boy has two months of aching around the right knee that he attributes to football, then notices a firm lump on the distal thigh that is slowly growing — osteosarcoma, and the radiograph will show a mixed lytic and sclerotic lesion with a Codman triangle at the distal femur. A nine-year-old with pelvic pain, fever, and a soft tissue mass has been on two courses of oral antibiotics for a presumed infection — Ewing sarcoma, which is the great mimic of osteomyelitis. The shared skill is to treat persistent, progressive, or night-waking bone pain as malignancy until a full blood count, a film, and a radiograph say otherwise. [2] [4]
The night-pain rule — PERSISTENT, PROGRESSIVE, PAIN THAT WAKES
Overview & Definition
Bone pain in a child is a symptom, not a diagnosis, and the clinical question it poses is binary: is this a benign, self-limiting musculoskeletal pain, or is it the presenting feature of a malignancy? The benign causes dominate by far — growing pains, transient synovitis, minor trauma, stress and toddler fractures, benign hypermobility, and the apophysitides of the active child — and a confident registrar can reassure most families at the first visit. The danger is the small fraction that is leukaemia, osteosarcoma, Ewing sarcoma, metastatic neuroblastoma, or lymphoma, because these are the diagnoses that a delayed week or month measurably worsens. [1] [2]
The defining skill this topic teaches is the red-flag screen — the small set of historical, examination, and investigation features that reliably separate malignant from benign bone pain. The screen rests on three pillars. First, the pain pattern: benign pain is mechanical, bilateral, evening, and resolves with rest; malignant pain is focal, progressive, unrelieved by rest, and wakes the child from sleep. Second, the systemic search: fever, weight loss, fatigue, pallor, bruising, lymphadenopathy, and organomegaly are never part of growing pain. Third, the basic tests: a full blood count and film that reveals cytopenias or blasts, and a plain radiograph that reveals a destructive lesion, leukaemic lines, or a periosteal reaction. [1] [2] [3]
The reason this matters at fellowship level is that malignancy in children rarely announces itself with a flag. It hides inside the commonest complaint in paediatrics — a limb pain or a limp — and the same registrar who reassures the ninety-ninth child must not miss the hundredth. Cabral and Tucker showed, in a review of children referred to rheumatology clinics for rheumatic complaints, that those ultimately found to have malignancy had a recognisable cluster of red flags that was present but often not acted upon. The Jones multicentre case-control study then defined the discriminating features between childhood leukaemia and juvenile idiopathic arthritis with enough rigour to be used at the bedside. This page builds the clinical reasoning around those two studies and the primary bone tumour epidemiology that follows. [1] [2]
Classification
Classify a child's bone pain along two axes that together set the probability of malignancy. The first axis is the temporal pattern of the pain, and the second is the presence of systemic or examination red flags. The two axes interact — a focal, progressive pain with a normal examination still warrants bloods and a radiograph, whereas a bilateral evening pain in a completely well child with a normal examination does not.
[1]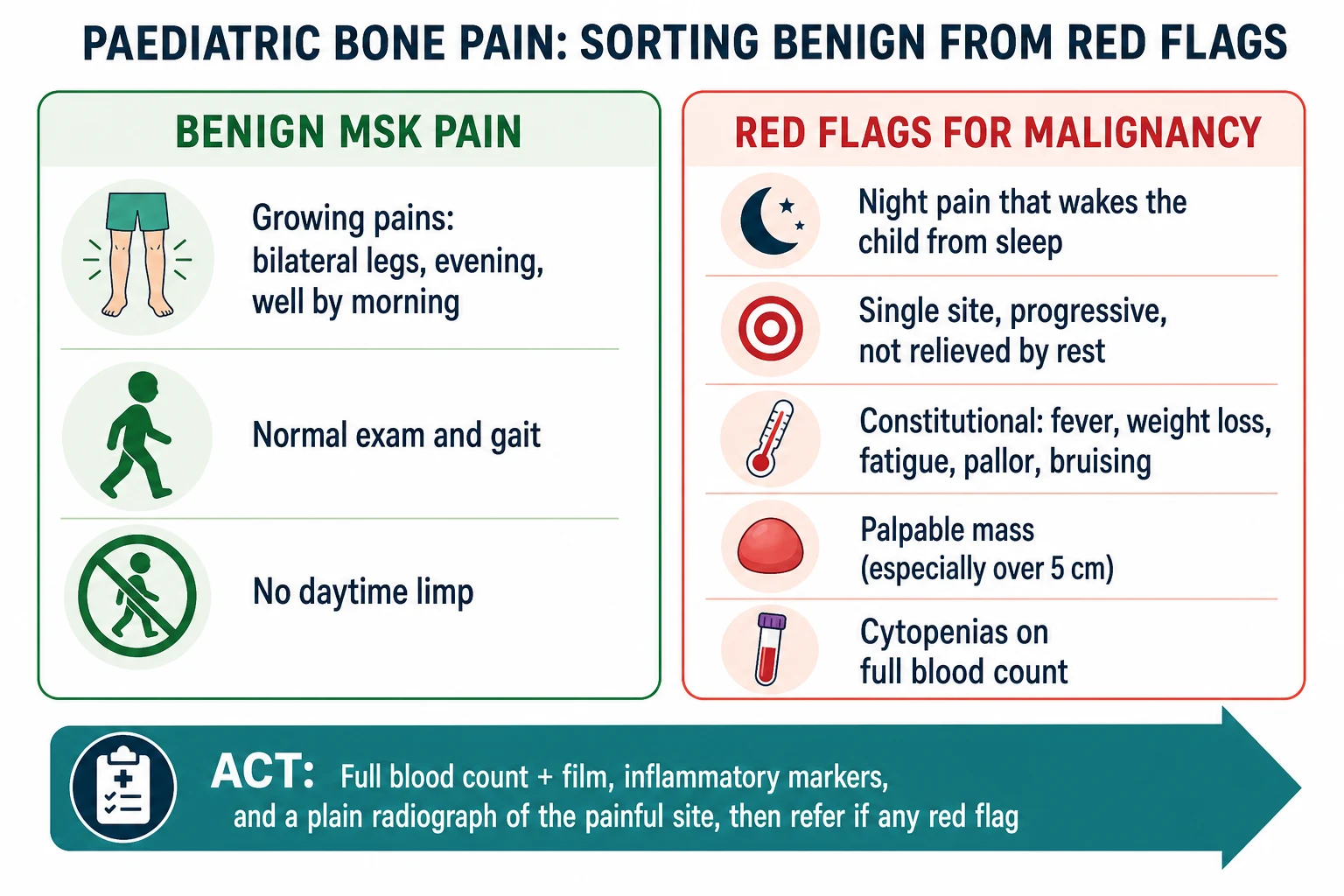
The benign panel is the home of growing pain and its cousins. Growing pain is intermittent, bilateral, predominantly in the calves and thighs, worse in the late afternoon and evening, and gone by morning, in a child who is entirely well between episodes and walks normally by day. Transient synovitis sits here too in the three-to-eight-year-old: a recent viral illness, an antalgic gait, a comfortable hip, low or no fever, and full recovery over days. Mechanical pains of the active child — Osgood-Schlatter at the tibial tubercle, Sever apophysitis at the heel, a stress fracture — are activity-related, focal, and resolve with rest. The unifying feature is that the pain respects the activity cycle and the child is well. [1]
Benign (growing pain pattern)
Red flag — leukaemia
Red flag — primary bone tumour
Red flag — metastatic or marrow
The malignant panel divides into three clinical syndromes that the rest of the page develops. Leukaemia is marrow disease that announces itself through bone pain and cytopenias, and it is the commonest malignancy to present this way. Primary bone tumours — osteosarcoma and Ewing sarcoma — are focal lesions of the bone itself, presenting with a single painful site and eventually a mass. Metastatic or multifocal malignancy — neuroblastoma in the young child, lymphoma, Langerhans cell histiocytosis — presents with systemic illness and multifocal or axial bone pain. The classification matters because each syndrome has a different first test, a different referral destination, and a different emergency. [2] [9]
Epidemiology & Risk Factors
The epidemiology of malignant bone pain is the epidemiology of childhood cancer seen through its commonest musculoskeletal door. Acute lymphoblastic leukaemia is the commonest childhood malignancy, and musculoskeletal symptoms bring roughly a fifth to a quarter of affected children to medical attention, often before the blood count has fully declared the disease. This is the population that drives the whole topic: a child whose leg pain is the first whisper of leukaemia, and whose arthritis-like presentation is the trap that delays diagnosis by weeks. [2] [4]
Osteosarcoma is the commonest primary malignant bone tumour of childhood and adolescence. Its incidence peaks in the second decade, during the adolescent growth spurt, and it favours the metabolically active metaphyses around the knee — the distal femur, the proximal tibia, and the proximal humerus. The SEER analysis by Mirabello and colleagues established the incidence and survival pattern across three decades, and it confirms the clinical teaching that an adolescent with persistent pain around the knee carries osteosarcoma until imaging says otherwise. Ewing sarcoma is the second commonest primary malignant bone tumour, with an incidence peaking slightly younger than osteosarcoma, and it differs in tending to the diaphysis of long bones and the axial skeleton, especially the pelvis. [5] [6] [9]
The risk factors for a missed malignancy are, paradoxically, the features that make a child look well. The pre-verbal toddler who cannot localise pain, the adolescent who attributes a knee ache to sport, the child whose initial blood count is near-normal, and the family given a reassuring label of growing pain or juvenile arthritis all carry the risk of diagnostic delay. George and Grimer, studying the early symptoms of bone and soft tissue sarcomas, found that many patients had symptoms for months before the diagnosis was made, and that the red flags — a palpable mass, night pain, and pain increasing in severity — were often present but not acted upon. The lesson for the general paediatrician is that a label given at the first visit must always carry a safety-net and a re-review, because the single most modifiable prognostic factor in paediatric bone malignancy is the interval between symptom onset and specialist referral. [8]
Pathophysiology
Understanding why malignancy causes bone pain turns the red flags from a list to be memorised into a mechanism to be reasoned with. The unifying principle is that bone is a rigid, closed compartment, and any expanding or infiltrating process inside it raises pressure, distends the richly innervated periosteum, and produces a pain that the child cannot relieve by shifting position. That is why malignant bone pain is progressive, focal, and characteristically nocturnal — it does not respect the activity cycle the way a sprain does.
[5]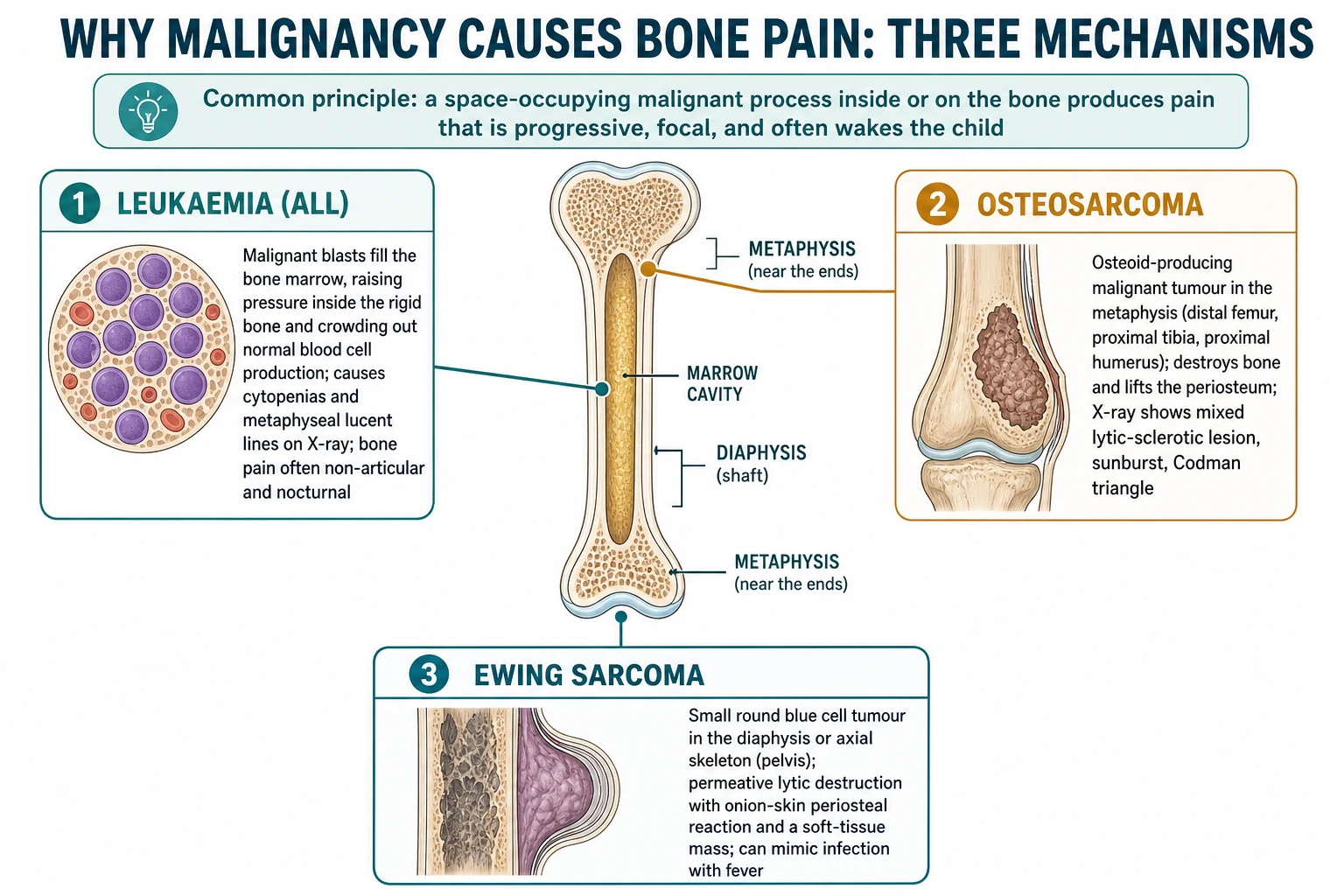
In leukaemia, malignant lymphoblasts fill the bone marrow and crowd out normal haematopoiesis. The expanding blast mass raises intramedullary pressure and distends the periosteum, producing a deep, often nocturnal bone pain that can precede the cytopenias by weeks. Because the marrow is the factory for all blood cell lines, the infiltration produces the triad that the clinic later detects: anaemia from red-cell crowding, thrombocytopenia from megakaryocyte loss, and a white cell count that may be high, low, or normal depending on the blast burden. The same infiltration thins the bone at the metabolically active metaphysis, producing the radiographic metaphyseal lucent bands known as leukaemic lines that Tafaghodi and colleagues identified as a discriminating plain-film sign between early leukaemia and juvenile idiopathic arthritis. [3] [4]
Osteosarcoma arises from the malignant osteoblast, the bone-forming cell, which is why the tumour produces its own disordered osteoid matrix. It grows in the metaphysis at the site of maximal adolescent growth, lifts and breaches the periosteum, and lays down new bone in a disorganised sunburst pattern; the elevated periosteum forms the Codman triangle at the tumour margin. The pain begins as activity-related ache at the favoured site and progresses to night pain as the tumour expands, and the eventual palpable mass is the tumour breaching the cortex into the soft tissues. [5]
Ewing sarcoma is a small round blue cell tumour driven by the EWSR1-FLI1 fusion of the t(11;22) translocation, and it differs from osteosarcoma in two clinically decisive ways. It tends to the diaphysis of long bones and the flat bones of the axial skeleton, especially the pelvis, rather than the metaphysis around the knee, and it produces a permeative, moth-eaten lytic destruction with an onion-skin or sunburst periosteal reaction and a disproportionate soft-tissue mass. Because it commonly presents with fever, a raised inflammatory response, and a tender swelling, it is the great mimic of osteomyelitis, and a child treated for presumed bone infection who does not improve is the classic delayed-diagnosis story. [9] [6]
Clinical Presentation
The clinical presentation of malignant bone pain is shaped by the underlying syndrome, but the red flags that should prompt investigation are common to all. Take the pain history first, because the pattern of the pain does more work than any single examination finding. Ask specifically whether the pain wakes the child from sleep, whether it is at one site or several, whether it is getting better or worse over weeks, and whether it responds to rest and simple analgesia. Night pain that wakes the child, focal pain at a single bony site, and progressive pain despite rest are the three historical features that move a child out of reassurance and into investigation. [1] [8]
The systemic history is the second screen, and it is where leukaemia most often declares itself. Ask about fever without an obvious source, unintentional weight loss, increasing fatigue and need for daytime sleeps, pallor noticed by relatives, easy bruising or prolonged bleeding, bone pain at multiple sites, and a recent change in exercise tolerance. Any of these alongside limb pain is never growing pain. Lymphadenopathy that is generalised or persistent, a distended abdomen from hepatosplenomegaly, and a waddling or regressing gait in a child who could previously walk are the examination correlates that confirm the systemic story. [2]
The examination of the painful site is the third screen, and it distinguishes a true arthritis from a non-articular bone pain. Palpate the limb carefully to localise the tenderness to the joint itself or to the bone shaft and metaphysis, because leukaemia and bone tumours cause non-articular bony tenderness whereas juvenile idiopathic arthritis causes a warm, swollen, tender joint. Look for a mass: a firm, deep, fixed swelling over a long bone, especially one that is enlarging or larger than five centimetres, is a sarcoma until proven otherwise. Compare both limbs for warmth, swelling, and muscle wasting, and always examine the abdomen for organomegaly, the nodes, and the skin for bruising and petechiae. [1] [2]
Two presentations deserve special vigilance because they are so easily mislabelled. The child with leukaemia who presents with a single swollen, painful joint can be indistinguishable from oligoarticular juvenile idiopathic arthritis at the first visit, and Needleman's description of childhood leukaemia mimicking arthritis remains the canonical warning — the discriminator is the cytopenia on the blood count and the non-articular bone tenderness on examination. The adolescent with osteosarcoma who attributes knee pain to sport is the other, and the trap closes when a firm mass appears weeks later. The safety-net for both is a scheduled re-review within two to four weeks and a clear instruction to return sooner if the pain progresses, wakes the child, or a mass appears. [4] [8]
Differential Diagnosis
The differential of persistent paediatric bone pain splits into the dangerous diagnoses this topic exists to catch and the benign diagnoses that dominate by number. The dangerous differentials are leukaemia, osteosarcoma, Ewing sarcoma, metastatic neuroblastoma in the young child, lymphoma, and Langerhans cell histiocytosis, and the mimic that sits among them is osteomyelitis, which shares night pain, fever, a raised inflammatory response, and a lytic radiograph with malignancy. [1] [9]
Osteomyelitis
Juvenile idiopathic arthritis
Growing pains
Stress or toddler fracture
Resolving the differential rests on the same three pillars — the pain pattern, the systemic search, and the basic tests. Leukaemia resolves on the full blood count and film that reveals cytopenias or blasts, confirmed by marrow aspirate; juvenile idiopathic arthritis resolves on the presence of true arthritis lasting six weeks with a normal blood count; osteomyelitis resolves on the fever, the high inflammatory markers, the positive blood culture, and the dramatic response to antibiotics within days. The bone tumours resolve on the plain radiograph, which shows a destructive, permeative lesion with the characteristic periosteal signatures, and then on magnetic resonance imaging and specialist biopsy. [3] [8]
Two diagnostic traps deserve naming because they recur in examinations. The first is labelling a child with monoarticular arthritis when the underlying diagnosis is leukaemia — the cytopenia was missed or not sought, and the joint pain was in fact referred from a leukaemic metaphyseal lesion. The second is treating a Ewing sarcoma of the pelvis as osteomyelitis through several courses of antibiotics, because both produce fever, pain, and a soft-tissue mass. The defence against both is the same: any bone pain that is persistent, progressive, or nocturnal gets a full blood count and film, inflammatory markers, and a radiograph of the painful site, and any child who does not improve as expected gets re-imaged and reconsidered. [4] [9]
Clinical & Bedside Assessment
The bedside assessment of a child with bone pain is built to answer one question: does this pain need investigation today? Run it in three layers — the pain history, the systemic search, and the focused musculoskeletal and general examination — and let the layers accumulate into a decision.
[1]For the pain history, use the child and the parent as separate witnesses. Ask the parent whether the child has been limping, refusing to walk, or regressing from walking to crawling, and ask the child to point with one finger to where it hurts, because a single-finger localisation to bone is far more concerning than a vague swept-hand indication of a limb. Establish the temporal pattern with three direct questions: does the pain wake the child from sleep, is it at one site or several, and is it getting better or worse over the weeks. A pain that wakes the child, that sits at one bony point, and that is worsening is malignant until the basic tests say otherwise. [1] [8]
For the systemic search, screen for the constitutional features of marrow disease and disseminated malignancy. Ask directly about fever, weight loss, fatigue, pallor, bruising, gum or nose bleeding, and bone pain at sites other than the one presented. Examine the nodes in all five regions, palpate the abdomen for hepatosplenomegaly, and inspect the skin for bruising and petechiae. Generalised lymphadenopathy, an enlarged liver or spleen, and unexplained bruising alongside limb pain are each alone sufficient to request a full blood count and film the same day. [2]
For the musculoskeletal examination, expose both limbs fully and compare. Look for asymmetry, swelling, muscle wasting, and a visible mass, and ask the child to walk so that an antalgic or altered gait is observed. Palpate to localise the tenderness precisely — over the joint line, which favours arthritis, or over the bone shaft and metaphysis, which favours leukaemia, osteomyelitis, or a bone tumour. Feel for warmth and effusion at the joints, measure the range of movement of the nearest joint, and palpate along the entire length of the painful bone for a mass. A firm, deep, fixed mass over a long bone is the examination finding that demands imaging and referral the same day, and a tender warm joint with full active movement elsewhere is the finding that allows measured reassurance with a safety-net. [1] [2]
Investigations
The investigation of suspected malignant bone pain begins with two cheap, fast, high-yield tests that every general paediatrician can order today: a full blood count and film, and a plain radiograph of the painful site in two views. These two tests, read together, resolve most of the dangerous differentials at the first visit and direct the child to the right specialist.
[2]The full blood count and film is the single most important test for leukaemia, and its absence is the commonest reason the diagnosis is delayed. Look for the cytopenias of marrow infiltration — anaemia, thrombocytopenia, and a low or high white cell count — and specifically request a film to be examined for blasts, because an early leukaemia can hide in a near-normal count and declare itself only on the film. Add a lactate dehydrogenase, which reflects cell turnover and tumour burden and is elevated in leukaemia, lymphoma, and Ewing sarcoma, an erythrocyte sedimentation rate and C-reactive protein to gauge inflammation and infection, a urate as a baseline before any tumour lysis risk, and renal and liver function as a baseline for later chemotherapy. [2] [3]
| Test | What it shows | Red-flag result |
|---|---|---|
| Full blood count and film | Marrow cell lines and blasts | Cytopenias or blasts on the film |
| ESR and CRP | Inflammation, infection, malignancy | Markedly raised without an infection source |
| Lactate dehydrogenase | Cell turnover, tumour burden | Elevated in leukaemia, lymphoma, Ewing sarcoma |
| Plain radiograph (two views) | Bone destruction, periosteal reaction | Destructive lesion, Codman triangle, onion-skin, leukaemic lines |
| Magnetic resonance imaging | Marrow and soft-tissue extent, mass | Tumour with soft-tissue component, marrow oedema |
The plain radiograph is the test that names a primary bone tumour, and its features must be read deliberately. Osteosarcoma shows a destructive, mixed lytic and sclerotic lesion in the metaphysis around the knee, with new bone in a sunburst pattern and a Codman triangle where the periosteum is lifted at the tumour edge. Ewing sarcoma shows a permeative, moth-eaten lytic lesion in the diaphysis or pelvis, with an onion-skin or sunburst periosteal reaction and a soft-tissue mass out of proportion to the bone change. Leukaemia shows diffuse osteopenia, periosteal reaction, and the metaphyseal lucent bands known as leukaemic lines, which Tafaghodi and colleagues identified as a discriminating sign between early leukaemia and juvenile idiopathic arthritis. A normal radiograph does not exclude a tumour, because an early marrow lesion can hide behind normal cortical bone — a child with high suspicion and a normal film needs magnetic resonance imaging. [3] [9]
Magnetic resonance imaging is the imaging of choice once a tumour or osteomyelitis is suspected, because it defines the intramedullary extent, the soft-tissue mass, the skip lesions, and the relationship to the neurovascular bundle and growth plate. It is the staging baseline that a specialist sarcoma centre builds the surgical plan on. Computed tomography of the chest, a bone scan or whole-body imaging, and a biopsy follow in the specialist centre, and the biopsy is always performed by the team that will treat the tumour — never by a general surgeon or in a peripheral hospital, because an unplanned excision contaminates tissue planes and worsens the prognosis. [8] [7]
Management — Resuscitation
Resuscitation in malignant bone pain is rarely about circulation and airway, and almost always about two surgical and oncological emergencies that a general paediatrician must recognise before referral: pathological fracture and spinal cord compression. Both can declare themselves at presentation, and both change the urgency and the mode of the referral.
[8]A child with a destructive bone lesion is at risk of pathological fracture through structurally weakened bone, and a fracture through a sarcoma is a surgical and oncological catastrophe that changes the operation from limb-sparing to amputation in some cases. Protect the limb immediately with a splint, make the child non-weight-bearing, and arrange urgent transfer to a specialist sarcoma centre. Do not reduce or internally fix a pathological fracture outside the treating team, because the operation contaminates the tumour and compromises the later resection. [8]
The systemic emergency of leukaemia at presentation is tumour lysis and the consequences of profound cytopenias, and both fall to the paediatric oncology service once suspected. A child with a high white cell count or a high tumour burden is at risk of tumour lysis when treatment begins, and a child with severe thrombocytopenia or neutropenia is at risk of bleeding and infection. The general paediatrician's role at this stage is to recognise the likely leukaemia on the blood count and film, begin intravenous fluids, avoid intramuscular injections and rectal procedures in the thrombocytopenic child, and transfer urgently to the oncology centre for confirmation by marrow aspirate and the start of protocol therapy. [2] [4]
Management — Definitive & Stepwise
The definitive management of malignant bone pain is, with few exceptions, the management of the underlying malignancy, and it is delivered in a specialist paediatric oncology or sarcoma centre. The general paediatrician's role is to recognise, to investigate, to refer correctly, and to avoid the iatrogenic harm of an unplanned procedure — and then to support the child and family through treatment. The pathway runs in four steps.
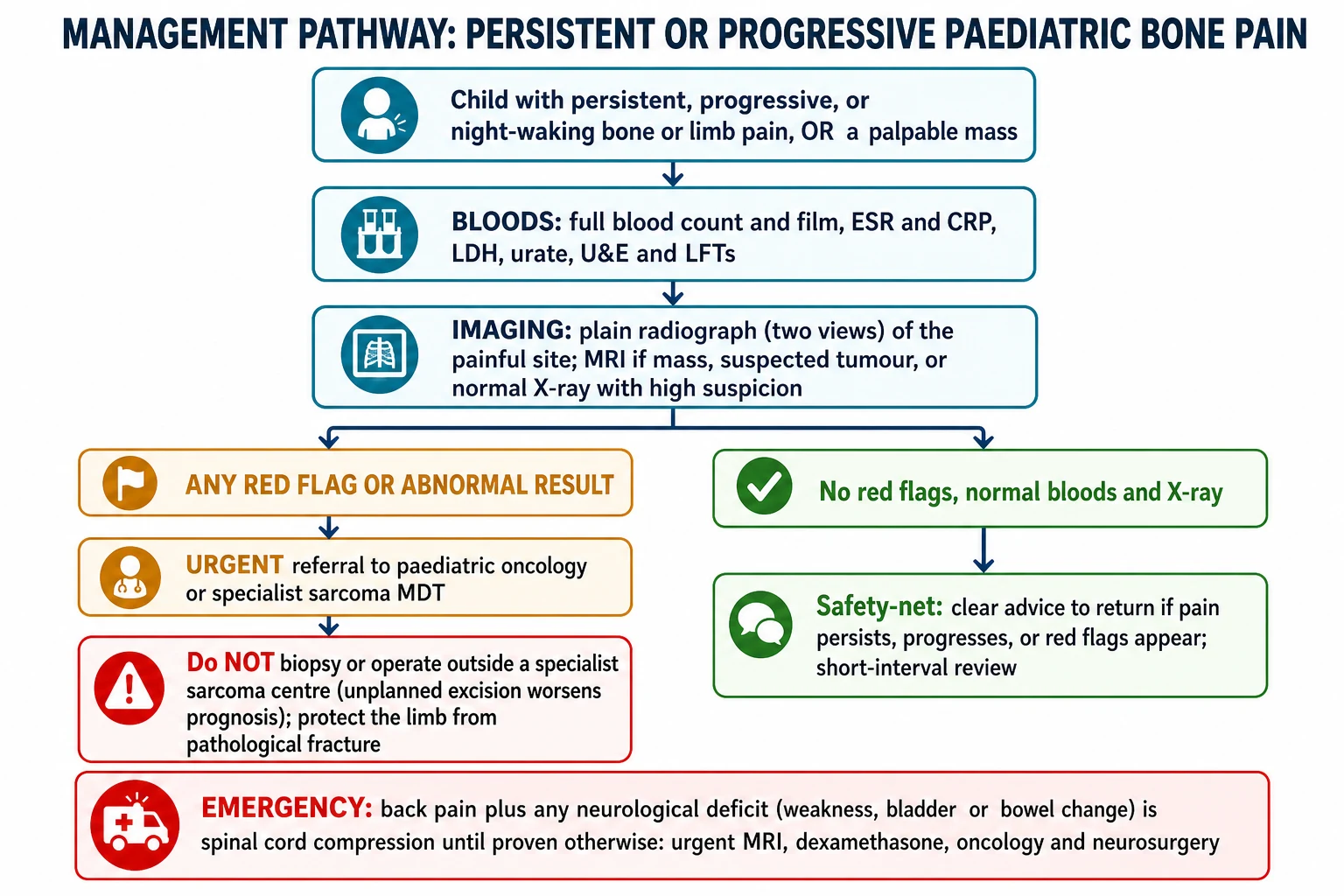
[8]Take a focused pain history and systemic search, and examine to localise the pain to bone or joint and to find a mass, organomegaly, or bruising.
Order the same-day basic bundle: full blood count and film, erythrocyte sedimentation rate and C-reactive protein, lactate dehydrogenase, urate, and renal and liver function.
Image the painful site with a two-view plain radiograph; arrange magnetic resonance imaging if a mass or tumour is suspected or if the radiograph is normal but suspicion remains.
If any red flag or abnormal result is present, refer urgently to paediatric oncology or a specialist sarcoma centre; never biopsy or operate on a suspected tumour outside that centre.
For suspected leukaemia, the child is referred urgently to paediatric oncology for a bone marrow aspirate and trephine with morphology, flow cytometry, and cytogenetics, which confirm the diagnosis and risk-stratify the disease. Definitive treatment is risk-stratified multi-agent chemotherapy delivered under a national or international protocol, with induction, consolidation, and maintenance phases, and central nervous system-directed therapy. The general paediatrician supports the family, monitors for infection and treatment toxicity, and coordinates the long surveillance of late effects. [2]
For osteosarcoma, the standard of care established by EURAMOS-1 and its predecessors is neoadjuvant chemotherapy followed by wide surgical resection and then adjuvant chemotherapy. The chemotherapy backbone is MAP — high-dose methotrexate, doxorubicin, and cisplatin — and the strongest prognostic factor is the histological response of the resected tumour, with a good response defined as at least ninety per cent tumour necrosis. Smeland and colleagues reported the EURAMOS-1 survival outcomes in over two thousand patients, and Marina and colleagues showed in a randomised trial that escalating from MAP to MAPIE by adding ifosfamide and etoposide did not rescue poor responders, confirming that the response to neoadjuvant chemotherapy is both prognostic and currently non-modifiable. The lesson for the candidate is that the outcome is set largely by the biology of the tumour and the completeness of the surgery, which is why early recognition and correct referral — not later rescue — determine prognosis. [7] [10]
For Ewing sarcoma, definitive treatment combines multi-agent chemotherapy with local control by surgery or radiotherapy, delivered in a specialist centre. The regimen is built around the VDC and IE backbones — vincristine, doxorubicin, and cyclophosphamide alternating with ifosfamide and etoposide — and the response to chemotherapy and the completeness of local control again set the prognosis. Because Ewing sarcoma is radiosensitive, radiotherapy has a role where complete surgical resection is not possible, particularly in the pelvis and axial skeleton. [6] [9]
Specific Subtypes & Scenarios
Each malignant syndrome that presents with bone pain has a recognisable clinical archetype that the fellowship examination rewards. Holding these archetypes lets a candidate move from the history to the probable diagnosis to the first test in one step.
[2]Leukaemia (ALL) archetype
Osteosarcoma archetype
Ewing sarcoma archetype
Metastatic neuroblastoma archetype
The scenario that most often appears in written and oral examinations is the child with a single swollen joint labelled as juvenile idiopathic arthritis who turns out to have leukaemia. The discriminating features from the Jones multicentre case-control study are the absence of morning stiffness, the presence of non-articular bone pain, nocturnal pain, constitutional symptoms, lymphadenopathy or organomegaly, and a cytopenia on the blood count — in particular, a platelet count that is low rather than the reactive thrombocytosis of true juvenile arthritis. The teaching point is that a child with a "monoarthritis" and any of these features gets a full blood count and film before the label of juvenile idiopathic arthritis is written. [2] [4]
The second recurring scenario is the adolescent athlete with persistent knee pain and an eventual mass. This child is at the peak age and site for osteosarcoma, and the error is to treat the pain as a sports injury through several weeks of physiotherapy while the mass declares itself. The teaching point is that persistent pain around the knee in an adolescent — pain that does not settle with rest, that wakes the child, or that is accompanied by a mass — gets a plain radiograph, and a destructive lesion with a Codman triangle ends the sports-injury label and begins the sarcoma pathway. [5] [8]
Complications & Pitfalls
The complications of malignant bone pain are the complications of a missed or mishandled diagnosis, because the disease itself, once referred, is managed by a specialist team. Three pitfalls recur in practice and in examinations, and each is preventable.
[8]The first pitfall is diagnostic delay from premature reassurance. The child is given a label of growing pain, viral synovitis, or juvenile arthritis at the first visit, the red flags in the history and examination are not acted upon, and the diagnosis is made weeks or months later when a mass appears, a cytopenia is found, or a pathological fracture occurs. George and Grimer showed that many sarcoma patients had symptoms for months before diagnosis, and that the red flags were often present but not investigated. The defence is the structured red-flag screen, the same-day basic tests for any child with persistent, progressive, or nocturnal pain, and a scheduled re-review with an explicit safety-net. [8] [1]
The second pitfall is the unplanned procedure on an unrecognised tumour. A child with a destructive lesion is referred to an orthopaedic service that performs a biopsy or curettage without knowing it is a sarcoma, or a pathological fracture is internally fixed without recognising the underlying tumour. Each contaminates the field and worsens the prognosis. The defence is to treat any destructive, permeative, or sunburst bone lesion as a tumour until proven otherwise, and to refer before any procedure. [8]
The third pitfall is missing spinal cord compression. Back pain in a child is uncommon enough to warrant attention, and back pain with any neurological deficit is an emergency that must not wait for a routine outpatient pathway. The defence is to ask every child with back or limb pain about weakness, gait change, and bladder and bowel function, to examine the neurological system, and to treat any deficit as cord compression with dexamethasone and urgent magnetic resonance imaging until proven otherwise. [9]
Prognosis & Disposition
The prognosis of paediatric malignancy that presents with bone pain is set largely by the biology of the tumour, the stage at diagnosis, and the completeness of surgical resection — and the one of these that the general paediatrician influences is the stage at diagnosis, through early recognition and correct referral. For osteosarcoma, the EURAMOS-1 cohort reported by Smeland and colleagues showed that localised disease carries around seventy per cent five-year survival, whereas metastatic disease falls below thirty per cent, and that the histological response to neoadjuvant chemotherapy — at least ninety per cent necrosis defining a good responder — is the strongest predictor. [7] [5]
For Ewing sarcoma, survival has improved over the three decades captured by the SEER analysis of Esiashvili and colleagues, with localised disease doing substantially better than metastatic disease, and the prognosis set by the response to chemotherapy and the completeness of local control. For childhood leukaemia, the prognosis has been transformed by risk-stratified multi-agent chemotherapy, and the children whose diagnosis is delayed are those who present atypically through bone pain and whose early cytopenias are missed — the very population this topic trains the general paediatrician to recognise. [6] [2]
Severity
Metastatic at presentation
under 30 per cent
The disposition from the general paediatric setting is therefore defined by the suspicion level. A child with any red flag or abnormal basic test is referred urgently — within days — to paediatric oncology or a specialist sarcoma centre, with the imaging and bloods sent ahead. A child with persistent pain but no red flags and normal basic tests is discharged with a written safety-net and a scheduled re-review in two to four weeks, with an instruction to return sooner if the pain progresses, wakes the child, or a mass appears. The disposition is never "discharge with no plan", because the safety-net is the last defence against the diagnostic-delay pitfall. [8]
Special Populations
The pre-verbal toddler and the adolescent are the two populations in whom malignant bone pain is most often missed, and each is missed for a different reason that the examination tests. The toddler cannot localise pain, refuses to walk or regresses from walking to crawling, and may simply be irritable or off feeds, so the presentation is non-specific and the differential is wide — from toddler fracture and septic arthritis to neuroblastoma and leukaemia. A toddler who will not bear weight, or who is systemically unwell with limb pain, gets the same basic bundle of bloods and imaging and the same red-flag vigilance as the verbal child. [1]
The adolescent attributes pain to sport and growth, minimises symptoms to avoid losing a place in a team, and may not disclose a mass until it is large. Persistent pain around the knee or shoulder in an adolescent is osteosarcoma until a radiograph says otherwise, and the general paediatrician must resist the shared temptation to label it a sports injury. The adolescent also needs developmentally appropriate communication — honest information about the concern and the need for imaging, involvement in decisions, and attention to the psychosocial impact of a potential cancer diagnosis on identity, schooling, and peer relationships. [5] [8]
Children with complex chronic conditions, immunocompromise, and existing haematological or oncological disease form a third population in whom bone pain has a raised prior probability of malignancy or its complications, and in whom the threshold to investigate is lower still. Aboriginal and Torres Strait Islander children, migrant and refugee families, and children in socioeconomically disadvantaged circumstances face higher rates of delayed presentation and reduced access to imaging and specialist review, and the general paediatrician must lower the threshold to investigate, use interpreter services, and ensure the referral is received and acted upon. [2]
Evidence, Guidelines & Regional Differences
The evidence base for distinguishing malignant from benign paediatric bone pain rests on two foundational clinical studies and the epidemiology of the primary bone tumours. Cabral and Tucker reviewed the children referred to rheumatology clinics whose ultimate diagnosis was malignancy, and defined the red-flag cluster that should trigger investigation. Jones and colleagues then ran the multicentre case-control study that formally compared children with childhood leukaemia against those with juvenile rheumatoid arthritis, and identified the discriminating clinical and laboratory features — non-articular bone pain, the absence of morning stiffness, nocturnal pain, constitutional symptoms, and cytopenias. Tafaghodi and colleagues added the radiographic discriminator of the metaphyseal lucent lines. [1] [2] [3]
For the primary bone tumours, the SEER analyses by Mirabello for osteosarcoma and Esiashvili for Ewing sarcoma provide the population incidence and survival data, the EURAMOS-1 outcomes reported by Smeland and the randomised comparison by Marina provide the modern treatment and prognostic framework for osteosarcoma, and Choi and colleagues provide the clinical and pathological review of Ewing sarcoma. George and Grimer contribute the delayed-diagnosis evidence that frames the central preventable harm. Together these ten sources carry every claim in this page, and each is verified against its live PubMed record. [5] [6] [7] [9] [10]
In Australia and Aotearoa New Zealand, suspected childhood malignancy is referred to the state or regional paediatric oncology service through the Australian and New Zealand Children's Haematology and Oncology Group network, and suspected primary bone sarcoma is referred to a specialist sarcoma multidisciplinary team at a tertiary children's hospital. A two-view plain radiograph of any painful bony site is available in primary and rural settings and is the recommended first investigation; magnetic resonance imaging and staging are arranged by the receiving centre.
[5]Exam Pearls
The high-yield facts for this topic are the discriminating features and the radiographic signatures, because these are what a written stem or a viva probes. Hold the leukaemia-versus-juvenile-idiopathic-arthritis distinction from the Jones study as a single sentence: true arthritis with morning stiffness and a reactive thrombocytosis favours juvenile idiopathic arthritis, whereas non-articular bone pain, night pain, constitutional features, and a cytopenia favour leukaemia. [2]
Hold the three radiographic signatures by tumour and site. Leukaemia produces diffuse osteopenia and metaphyseal lucent lines. Osteosarcoma produces a mixed lytic and sclerotic metaphyseal lesion around the knee with a sunburst periosteal reaction and a Codman triangle. Ewing sarcoma produces a permeative diaphyseal or pelvic lytic lesion with an onion-skin periosteal reaction and a soft-tissue mass, and it is the great mimic of osteomyelitis. [3] [9]
EURAMOS-1 (Smeland 2019; Marina 2016)
Population: Over 2000 patients with high-grade resectable osteosarcoma
Key finding
Good histological response (at least ninety per cent necrosis) was the strongest prognostic factor; escalating to MAPIE did not improve the outcome of poor responders
Hold the two most preventable errors: the delayed diagnosis from premature reassurance, and the unplanned excision of an unrecognised tumour. The defence against the first is the structured red-flag screen and the same-day basic tests for any persistent, progressive, or nocturnal pain. The defence against the second is to treat any destructive or sunburst bone lesion as a tumour until proven otherwise and to refer before any procedure. The emergency that must never be missed is back pain with neurological deficit, which is spinal cord compression until urgent magnetic resonance imaging says otherwise. [8] [7]
Finally, remember that night pain is the pivot of the whole topic. Night pain that wakes a child from sleep is shared by malignancy and osteomyelitis and only weakly by growing pain, and it is the single feature that most reliably converts a likely-benign pain into one that needs bloods and a radiograph the same day. A child sent home with a diagnosis of growing pain must always carry a safety-net and a re-review, because the hundredth child is the one the diagnosis depends upon. [1] [4]
References
- [1]Cabral DA, Tucker LB. Malignancies in children who initially present with rheumatic complaints. Journal of Pediatrics, 1999.PMID 9880449
- [2]Jones OY, Spencer CH, Bowyer SL, Dent PB, Gottlieb BS, Rabinovich CE. A multicenter case-control study on predictive factors distinguishing childhood leukemia from juvenile rheumatoid arthritis. Pediatrics, 2006.PMID 16651289
- [3]Tafaghodi F, Aghighi Y, Rokni Yazdi H, Shakiba M, Adibi A. Predictive plain X-ray findings in distinguishing early stage acute lymphoblastic leukemia from juvenile idiopathic arthritis. Clinical Rheumatology, 2009.PMID 19621208
- [4]Needleman M. Childhood leukemia mimicking arthritis. Journal of the American Board of Family Practice, 1996.PMID 8770811
- [5]Mirabello L, Troisi RJ, Savage SA. Osteosarcoma incidence and survival rates from 1973 to 2004: data from the Surveillance, Epidemiology, and End Results Program. Cancer, 2009.PMID 19197972
- [6]Esiashvili N, Goodman M, Marcus RB Jr. Changes in incidence and survival of Ewing sarcoma patients over the past 3 decades: Surveillance Epidemiology and End Results data. Journal of Pediatric Hematology and Oncology, 2008.PMID 18525458
- [7]Smeland S, Bielack SS, Whelan J, Bernstein M, Hogendoorn P, Krailo MD, et al. Survival and prognosis with osteosarcoma: outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteograsarcoma Study) cohort. European Journal of Cancer, 2019.PMID 30685685
- [8]George A, Grimer R. Early symptoms of bone and soft tissue sarcomas: could they be diagnosed earlier? Annals of the Royal College of Surgeons of England, 2012.PMID 22613305
- [9]Choi EY, Gardner JM, Lucas DR, McHugh JB, Patel RM. Ewing sarcoma. Seminars in Diagnostic Pathology, 2014.PMID 24680181
- [10]Marina NM, Smeland S, Bielack SS, Bernstein M, Jovic G, Krailo MD, et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): an open-label, international, randomised controlled trial. Lancet Oncology, 2016.PMID 27569442