Paeds · rheumatology-musculoskeletal-and-sports
Common paediatric fractures and growth-plate injury
Also known as Salter-Harris classification · growth plate fracture · physeal injury · buckle fracture · torus fracture · greenstick fracture · supracondylar fracture · Gartland classification
A fellowship approach to the common fractures of children's long bones and the growth-plate injuries they carry: the Salter-Harris classification of physeal injury and its prognosis, the greenstick, buckle and plastic-bowing patterns that come from the pliable paediatric bone, the Gartland classification and emergency percutaneous pinning of the displaced supracondylar humerus fracture with lateral-entry pins, the soft-bandage evidence for the torus fracture, the remodelling potential that accepts certain malunion, and the growth-arrest complications of physeal injury.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A five-year-old falls off the monkey bars onto an outstretched hand and arrives with a swollen, S-shaped elbow held guarded and a hand that is pale and pulseless; or a toddler is brought in with a mildly sore wrist used normally, whose radiograph shows a tiny buckle of the dorsal distal radius cortex; or a non-walking infant presents not moving the leg and a radiograph shows a corner fracture at the distal femur. In each, the question is the same — what pattern is this, what does it threaten, and what is the right immobilisation. [7] [9]
The five patterns — Plate, Bend, Kink, Snap, Crush
Overview & Definition
A paediatric fracture is a break in a bone that is still growing, and the growth is what changes everything. The growth plate or physis is the cartilage layer at each end of a child's long bone, and it is weaker than the surrounding bone and ligament, so the forces that sprain or strain an adult instead fracture the child's growth plate. Because the bone is also more plastic and wrapped in a thicker periosteum, it bends, kinks and cracks in patterns that adult bone cannot reproduce. [1] [7]
The growth plate is the reason a child's fracture is a paediatric problem and not an orthopaedic aside. Injury to the physis can arrest growth, producing a leg-length discrepancy or an angular deformity months or years after the fracture has healed, and the pattern of the injury across the plate — captured by the Salter-Harris classification — predicts this risk. The fellowship skill is therefore not only to heal the bone but to read the growth plate and to follow the child long enough to catch a physeal bar. [1] [6]
The clinical importance comes from the handful of fractures that are not benign. The displaced supracondylar humerus fracture threatens the brachial artery and the nerves of the arm and is the commonest reason a child's hand becomes pulseless, and the high-energy physeal fracture of the distal femur or proximal tibia carries a high rate of growth arrest. Around these sit the common and forgiving fractures — the distal radius buckle, the greenstick forearm — which heal well and demand only the right immobilisation and a short follow-up. [7] [5]
Classification
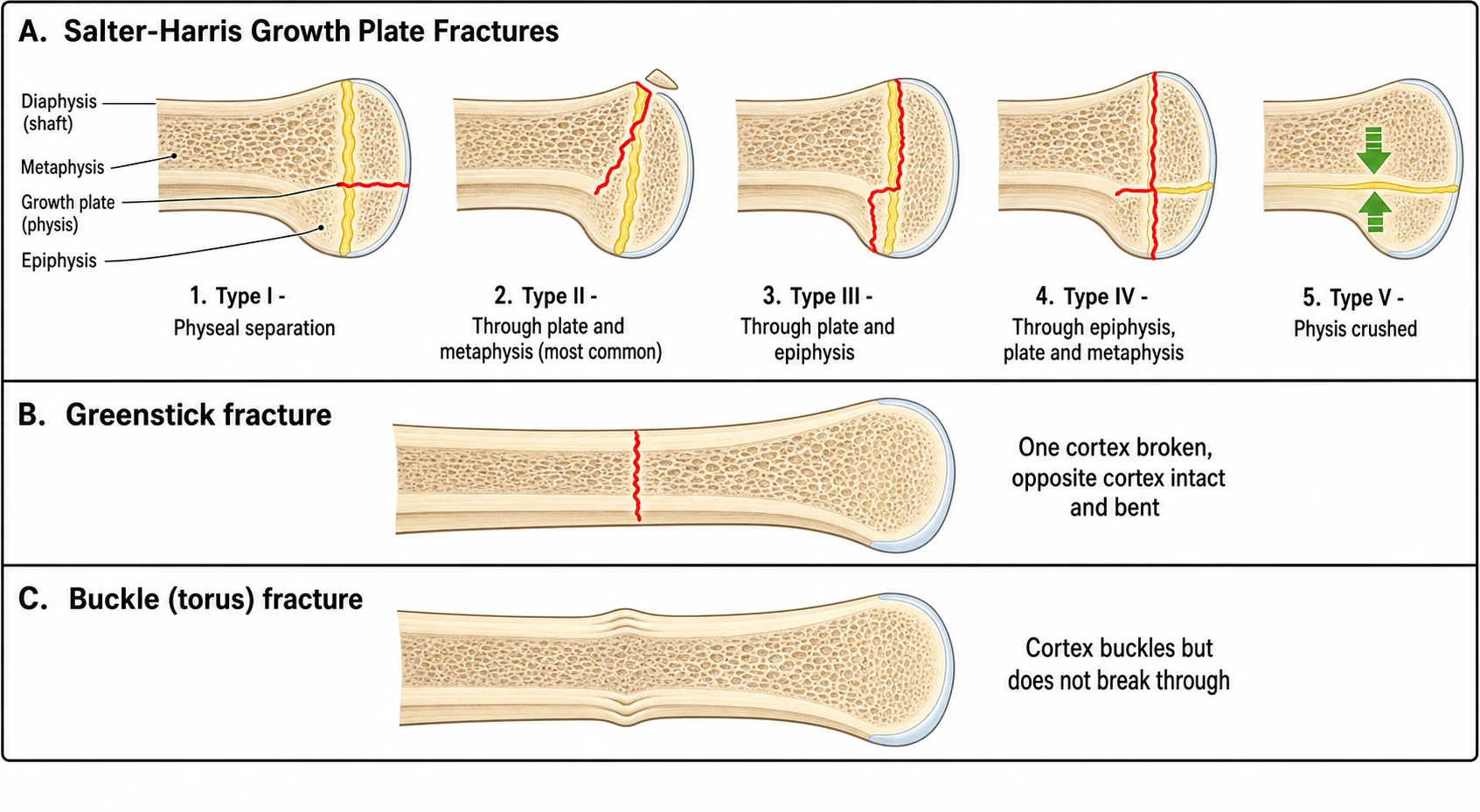
Classification rests on two things — whether the fracture crosses the growth plate, and how the pliable bone has failed. The Salter-Harris classification answers the first question, and it is the framework every fellowship candidate must reproduce. It describes five patterns of physeal injury, and the higher the type number, the worse the prognosis for growth. [1]
Type I is a clean separation of the epiphysis from the metaphysis entirely through the physis, with no bone fragment carried. It is common in infants and in the proximal femur, and it heals quickly because the growth-forming cells are usually spared. Type II is a fracture through the physis that exits through the metaphysis, carrying a small triangular metaphyseal fragment called the Thurston-Holland sign, and it is the commonest of all physeal injuries at roughly three-quarters of the total. The metaphyseal fragment is the radiographic signature, and the prognosis is good. [1] [7]
Type III runs through the physis and then turns across the epiphysis into the joint, so it is intra-articular and needs an anatomic reduction to restore the joint surface. Type IV crosses the epiphysis, the physis and the metaphysis in one line, and because the fracture crosses the whole growth plate it carries the highest risk of growth arrest and demands anatomic reduction and often internal fixation. Type V is a compression or crush injury of the physis with no visible fracture line, so the initial radiograph looks normal and the diagnosis is made in retrospect when growth arrest appears weeks to months later. [1] [6]
Epidemiology & Risk Factors
Fractures are among the commonest reasons a child presents to emergency care, and the upper limb carries the bulk of the burden. The distal radius — through its buckle, greenstick and complete-transverse patterns — is the single most frequently fractured bone in childhood, followed by the distal forearm as a whole and then the supracondylar humerus. The peak incidence sits in the school-age years, when children climb, jump and fall onto the outstretched hand. [7] [2]
The supracondylar humerus fracture peaks between five and eight years of age and carries the highest stakes of any common paediatric fracture, because it sits at the elbow where the brachial artery and the median, radial and anterior interosseous nerves are stretched across the sharp anterior metaphysis when the distal fragment displaces posteriorly. It is the commonest reason a child's hand becomes pulseless after a fracture, and it carries the highest nerve-injury and compartment-syndrome risk of any paediatric injury. [5] [10]
The risk of growth arrest rises with the Salter-Harris type and with the energy and the site. The distal radius physeal fracture is common but low-risk, whereas the high-energy distal femoral and proximal tibial physeal fractures that occur in adolescents near the growth spurt carry growth-arrest rates that demand long surveillance. The high type number, the joint involvement, and the violent mechanism are the markers of the fracture that will not simply heal and be forgotten. [1] [6]
A separate and crucial risk marker is the child who should not have the fracture. The classic metaphyseal lesion of inflicted injury, the femoral fracture in the non-walking infant, and fractures of different ages in the same child demand a safeguarding assessment rather than a cast. Kleinman showed that the classic metaphyseal lesion is far more prevalent in infants at high risk for abuse than in those at low risk, and it is the radiographic signature of inflicted skeletal injury. [9]
Pathophysiology
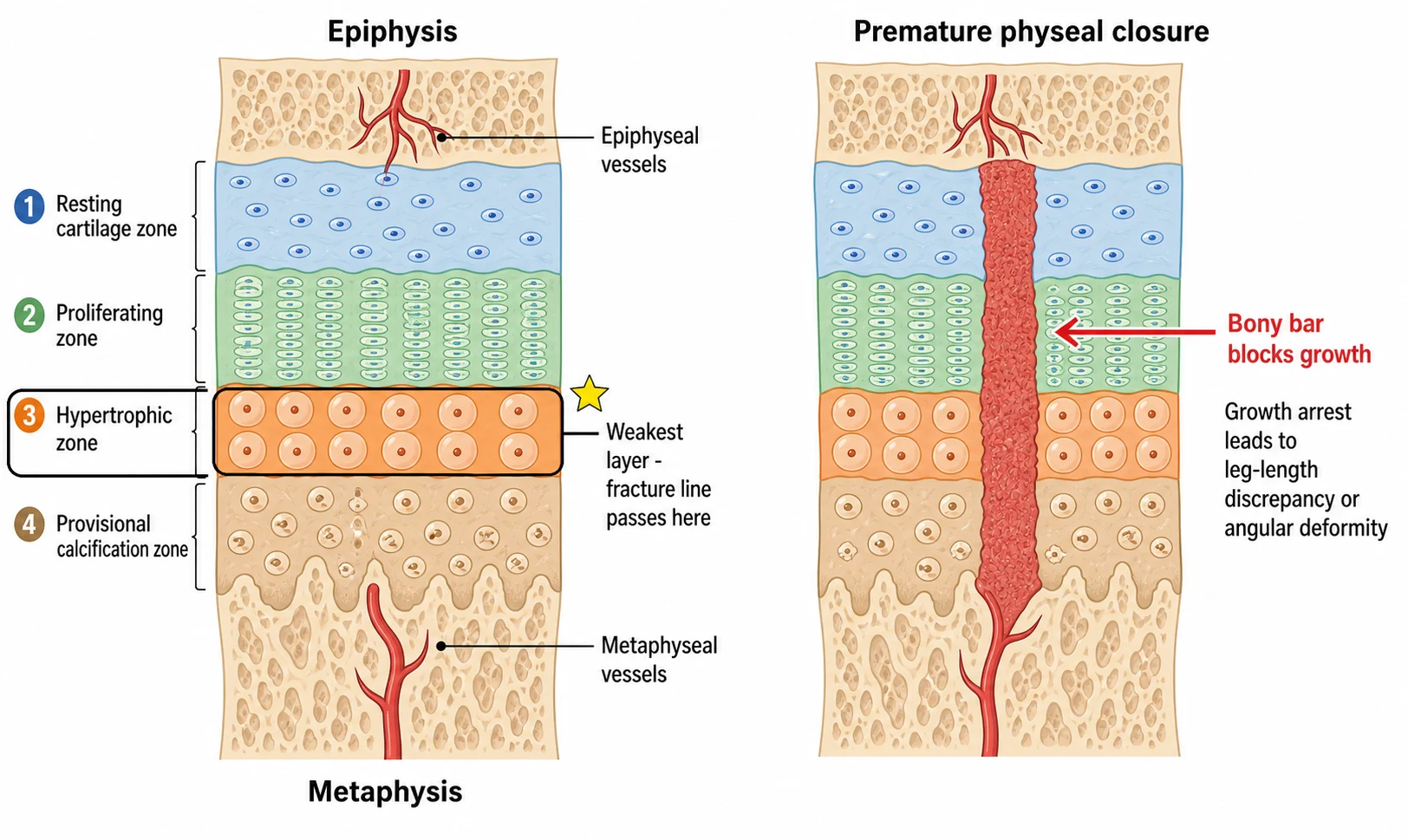
The growth plate is a layered cartilage sandwich, and its layered anatomy explains both why it breaks and why it usually keeps growing. From the epiphysis toward the metaphysis it runs through a resting cartilage zone, a proliferating zone where the future bone length is generated, a hypertrophic zone of enlarged maturing cartilage cells, and a provisional-calcification zone where the cartilage prepares to turn into bone. [1]
The hypertrophic zone is the weakest layer, and this single fact is the key to the physeal fracture. The forces of injury drive the fracture line through this weak layer, separating the epiphysis and its resting and proliferating zones from the metaphysis, and because the growth-forming cells in the resting and proliferating zones stay with the epiphysis, growth usually continues after healing. This is why most Salter-Harris I and II fractures heal without growth disturbance. [1] [6]
The growth arrest happens when the fracture crosses or crushes the whole plate and destroys the growth-forming cells or their blood supply. In a Salter-Harris IV the fracture line runs through the epiphysis, across the full thickness of the physis and out through the metaphysis, and the healing bone can bridge the plate to form a bony bar that tethers growth. A peripheral bar causes an angular deformity as one side of the plate stops while the other keeps growing, and a central bar causes shortening as the whole plate is anchored. The bar is the complication that declares itself late. [6] [1]
The thicker and more biologically active periosteum of the child explains the pliable-bone patterns. Because the paediatric bone is more plastic, it bends before it breaks, producing the plastic bowing deformity and the buckle or torus kink; and because the periosteum is thick and tears on only one side, a greenstick fracture leaves one cortex intact. The intact periosteum on the compression side is what holds a greenstick fracture together and what can cause it to re-angulate in the cast if the cortex is not completed. [7]
Clinical Presentation
The child with a fracture presents with pain, swelling and a refusal to use the limb, and the pattern of presentation follows the pattern of the fracture. The buckle fracture of the distal radius presents subtly — a low-energy fall, mild local tenderness over the dorsal distal radius, and a child who is often still using the hand, sometimes days after the injury, so it is easily under-called as a sprain. [7] [2]
The greenstick fracture presents with an angulated, painful forearm after a fall, and the plastic bowing deformity presents as a gentle bend of a long bone with no focal point of pain. The displaced supracondylar fracture presents with a swollen, S-deformed elbow held guarded, severe pain, a refusal to move, and the child cradling the arm. The supracondylar is the fracture that can threaten the hand, and the presentation includes the five signs of vascular compromise — pallor, pulselessness, paraesthesia, paralysis and a perishing cold hand. [5] [10]
Which reassuring-sounding stories must never close the fracture search? A toddler who has stopped walking or crawling may carry a toddler's fracture of the distal tibia or an inflicted injury rather than a minor sprain. An infant who will not move an arm after a reported pull may have a physeal injury of the distal humerus rather than a pulled elbow, especially if the elbow is swollen. And any fracture in a non-mobile infant, or a fracture inconsistent with the offered mechanism, opens the safeguarding pathway rather than the plaster room. [9] [7]
Differential Diagnosis
The differential diagnosis begins by separating the pliable-bone patterns from one another, because each leads to a different management. The buckle fracture shows a cortex that crumples without breaking through and is inherently stable, whereas the greenstick shows one cortex broken and one intact and the complete transverse fracture shows both cortices disrupted. The radiograph, with two orthogonal views, separates them, and the stability of the buckle is what permits a soft bandage. [7] [2]
For the swollen elbow, the differential includes the displaced supracondylar fracture, the lateral condyle fracture, the medial epicondyle avulsion, the transphyseal distal humerus fracture of the infant, the pulled elbow or nursemaid's elbow, a septic arthritis, and an osteomyelitis. The anterior humeral line and the radiocapitellar line on the lateral radiograph detect the subtle supracondylar, and the posterior fat-pad sign flags an occult intra-articular elbow fracture that is not yet visible. The younger the child, the more a transphyseal separation mimics a dislocation and the more septic arthritis enters the differential. [5] [10]
When the pattern does not fit the offered mechanism, the differential turns to inflicted injury. The classic metaphyseal lesion — the corner or bucket-handle fracture at the distal femur or the proximal or distal tibia in a non-mobile infant — the femoral fracture in a non-walker, rib fractures, and multiple fractures of different ages together demand a safeguarding workup. The radiograph is read not only for the fracture but for the fracture's plausibility. [9]
Clinical & Bedside Assessment
The assessment is look, feel, move, and neurovascular. Look for the deformity, the swelling, the bruising, and any open wound where bone may have pierced the skin. Feel for the point of maximal tenderness, the crepitus, and the compartments — a tense, firm, painful forearm compartment is compartment syndrome until proven otherwise. Move gently and only enough to establish the range, because forcing a displaced fracture hurts the child and may injure the neurovascular structures. [5] [7]
The neurovascular examination is the move that is never skipped and always documented before and after any reduction. Feel the radial, ulnar and brachial pulses and the capillary refill, and test the radial, ulnar and median nerves by sensation and by motor action. The anterior interosseous nerve is tested by asking the child to make an OK sign with thumb and index finger — flexion at the thumb interphalangeal and index distal interphalangeal joints — and its palsy, the commonest nerve injury of the extension supracondylar, is missed unless it is sought. [10] [5]
Which examination findings must never be dismissed? A pulseless, pale, cold hand is a vascular emergency that needs immediate reduction and often brachial artery exploration. A tense, painful forearm that hurts on passive finger extension is compartment syndrome, which can develop even after an apparently successful supracondylar reduction and which costs the forearm if not released. And pain that is out of proportion to the fracture, or analgesia that stops working, is the bedside signal of a worsening limb that overrides any reassuring radiograph. [5]
Investigations
Two orthogonal radiographs — an anteropasterior and a lateral — are required for every suspected paediatric fracture, centred on the joint and including the joint above and below where relevant. The suspected buckle of the distal radius is sometimes visible only on the lateral view as a subtle kink of the dorsal cortex, so a single anteropasterior view does not exclude it. The elbow radiograph is read for the anterior humeral line, the radiocapitellar line, and the posterior fat-pad sign, which together catch the occult supracondylar and lateral condyle fracture. [5] [7]
Computed tomography is reserved for the intra-articular Salter-Harris III and IV fractures where the joint surface and the displacement must be defined before an anatomic reduction, and magnetic resonance imaging is used when an occult fracture is strongly suspected and the radiograph is normal, or to map a physeal bar that is suspected on follow-up. Ultrasound has a limited role, mainly in the infant where the unossified epiphysis is cartilage and a transphyseal separation or a septic hip must be distinguished. [1] [6]
The follow-up radiograph is itself an investigation, because the growth-plate injury declares its late complication only on the films taken weeks to months after the fracture heals. A physeal bar, an asymmetric growth plate, or a developing angular deformity appears on the surveillance radiograph, and the child with a high-risk physeal fracture — a Salter-Harris IV, a high-energy distal femoral or proximal tibial injury — is followed until growth is complete or a bar is excluded. [6] [1]
Management — Resuscitation
Resuscitation begins with the limb, because the threatened hand is the time-critical problem in the displaced supracondylar fracture. Analgesia is given, the limb is splinted in a position of safety, and the neurovascular status is assessed and documented before and after any manipulation. The hard signs of vascular injury — a pulseless, pale, cold hand — demand immediate reduction of the fracture, because restoring alignment often restores the pulse, and a hand that remains pulseless and white after reduction is taken to theatre for exploration of the brachial artery. [5]
The pulseless but well-perfused, pink hand is managed differently from the pulseless white hand, and this distinction is a fellowship favourite. The pink, perfused hand with an absent pulse after a satisfactory reduction may be observed, because the collateral circulation is intact and the spasm often settles; the white, poorly perfused hand is an emergency that will not wait. In either case the reduction is performed first, and the decision to explore follows the perfusion, not the pulse alone. [5] [10]
Procedural pain control and sedation allow the child to be reduced humanely, whether with a haematoma block, nitrous oxide, or a procedural-sedation protocol appropriate to the child and the setting. Open fractures are covered with a sterile dressing, intravenous antibiotics are given, and tetanus status is checked. The child with a neurovascularly threatened fracture in a remote setting is splinted, given analgesia, and retrieved to a centre with paediatric orthopaedic capability, because the threatened hand is measured against the clock, not the distance. [5] [7]
Management — Definitive & Stepwise
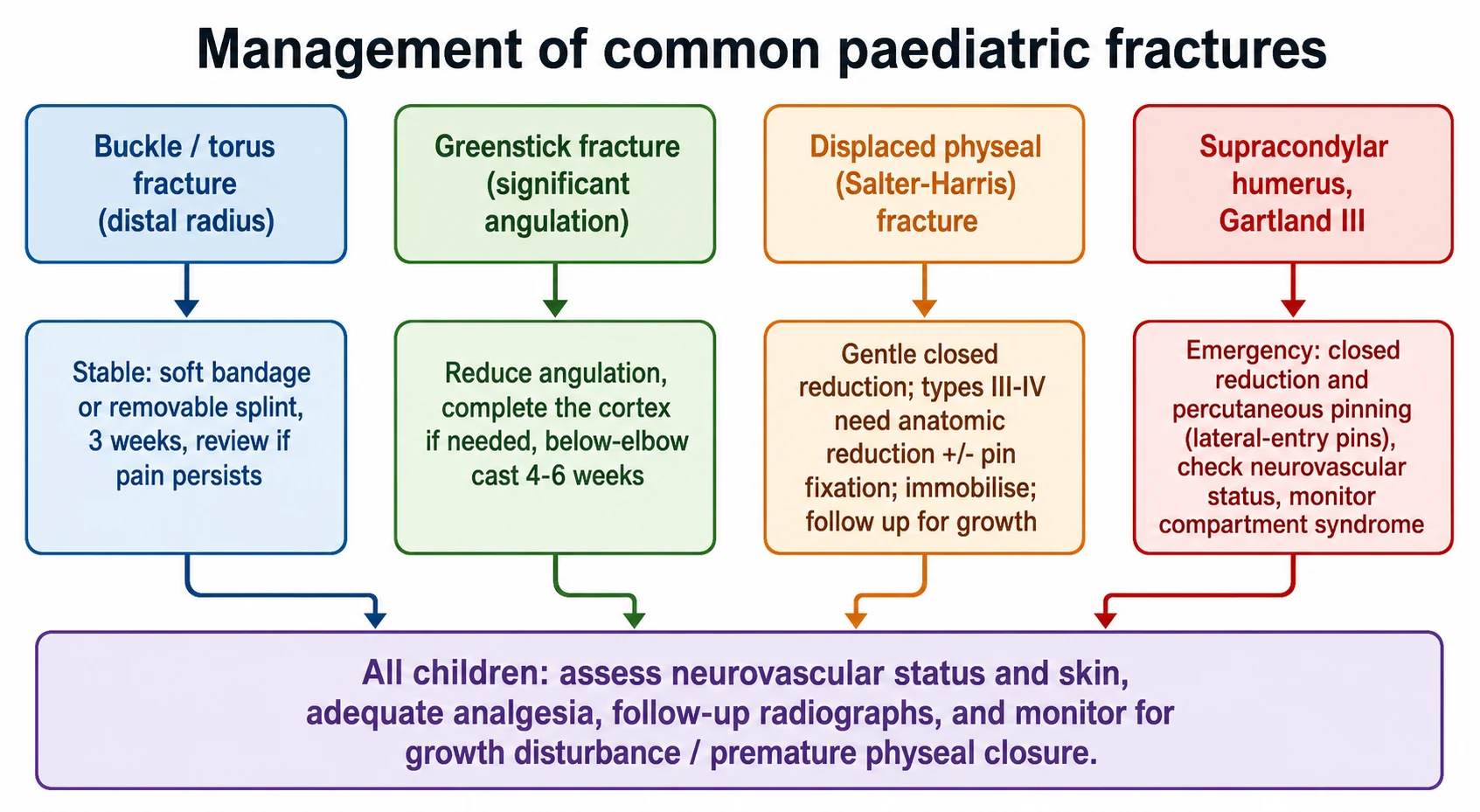
The definitive management follows the pattern, and the pattern follows the growth plate. The buckle or torus fracture of the distal radius is inherently stable and never displaces, so it is managed with a soft bandage or a removable splint for around three weeks, supported by the FORCE equivalence trial which showed that offering a bandage was no worse than rigid immobilisation and gave children better function and less pain, and by a systematic review confirming bandage or splint over a cast. [3] [2]
The angulated greenstick fracture is reduced and held in a below-elbow cast, and the intact cortex on the compression side may be gently completed to prevent re-angulation within the cast. The Salter-Harris I and II physeal fractures are managed by gentle closed reduction and immobilisation, taking care not to repeatedly force the physis, because repeated manipulation injures the growth plate further. The Salter-Harris III and IV fractures are intra-articular or cross the whole plate, so they need an anatomic reduction — often open with internal fixation — to restore the joint surface and to minimise growth arrest. [1] [7]
The Gartland III supracondylar fracture is managed by emergency closed reduction and percutaneous pinning, and the pin configuration is the fellowship detail that protects the ulnar nerve. Crossed pins, with one passed down the medial column, risk transfixing the ulnar nerve as it crosses the medial epicondyle, and the meta-analysis of randomised trials and the Skaggs pin-placement study showed that lateral-entry pin configurations reduce the iatrogenic ulnar nerve injury rate while maintaining fixation stability. Two or three divergent lateral pins are therefore the taught configuration for the unstable supracondylar. [4] [5]
Specific Subtypes & Scenarios
The distal radius buckle or torus fracture is the commonest and the most benign of the paediatric fractures, and it runs a short, forgiving course. A low-energy fall produces a crumpling of the dorsal cortex, the child has mild pain, and the fracture heals within three weeks. The FORCE trial settled the long debate about rigid casting by showing that a soft bandage was no worse than a cast and was better tolerated, and contemporary practice immobilises the buckle lightly and reviews only if pain persists. [3] [2]
The supracondylar humerus fracture is the subtype that carries the highest stakes. Classified by Gartland — type I undisplaced, type II displaced with the posterior cortex intact, type III fully displaced with no cortical contact — the type III is the emergency that goes to theatre for closed reduction and percutaneous pinning. The anterior interosseous nerve is the commonest nerve injured in the extension pattern, and the brachial artery is the vessel at risk, so the neurovascular examination before and after reduction is the safeguard. [5] [10]
The toddler's fracture is the subtype of the limping child. It is a non-displaced spiral fracture of the distal tibia in a child between nine months and three years who is ambulatory, produced by a low-energy twist, and it presents as an acute limp or a refusal to bear weight. The radiograph may be subtle or initially normal, and the fracture is managed with a splint or cast and heals well, with the safeguarding assessment reserved for the child whose history does not fit or who is not yet walking. [7]
The classic metaphyseal lesion is the subtype of inflicted injury. It appears as a corner or bucket-handle fracture at the distal femur or the proximal or distal tibia in the non-mobile infant, and it is produced by shearing or twisting of the fragile metaphysis. Kleinman demonstrated that it is far more prevalent in infants at high risk for abuse than in those at low risk, and it is the radiographic signature that takes the child out of the plaster room and into the safeguarding pathway, alongside the femoral fracture in a non-walker and fractures of different ages. [9]
The high-energy distal femoral and proximal tibial physeal fractures of the adolescent are the subtypes that threaten growth. Occurring near the growth spurt and produced by violent mechanisms such as a motor-vehicle impact or a sporting collision, they cross the whole growth plate and carry growth-arrest rates that demand orthopaedic reduction, internal fixation, and surveillance until growth is complete, because the bony bar that forms across the plate can produce a leg-length discrepancy or an angular deformity years after the injury. [6] [1]
Complications & Pitfalls
The complications of the paediatric fracture fall into the immediate and the late. The immediate complications are the vascular compromise of the supracondylar fracture, the nerve injuries, and the compartment syndrome that can develop after an elbow injury even when the reduction looks good on the radiograph. The late complications are the growth arrest and the physeal bar, the malunion, and the stiffness of a joint held too long in a cast. [5] [6]
The pitfall of treating the paediatric fracture like an adult fracture is the overarching error. Over-immobilising the inherently stable buckle fracture in a rigid cast, when the FORCE trial showed a soft bandage to be no worse, is the common over-treatment. Missing the threatened hand of the supracondylar, or sending the pulseless white hand to the ward, is the dangerous under-treatment. And forgetting the growth plate — failing to follow up a Salter-Harris IV or a high-energy distal femoral physeal injury — is the error that declares itself as a leg-length discrepancy months later. [3] [6]
The pitfall of iatrogenic ulnar nerve injury is the surgical error specific to the supracondylar. A medial pin passed down the humeral column can transfix the ulnar nerve as it crosses the medial epicondyle, and the meta-analysis and the pin-placement study showed that lateral-entry pin configurations avoid this while maintaining fixation. The safeguard is the taught preference for two or three divergent lateral pins, reserving a medial pin only when lateral fixation is insufficient and placing it through a small incision to visualise the nerve. [4] [5]
The pitfall of the missed physeal bar is the late error. A growth-plate injury that looks healed on the early follow-up film can still arrest growth, because the bar forms as the fracture heals, and the first sign is an asymmetric growth plate or a developing angular deformity on the surveillance radiograph. The safeguard is the follow-up schedule matched to the risk — a short review for the low-risk distal radius physeal fracture, and surveillance to growth completion for the high-risk distal femoral and proximal tibial injury. [6] [1]
Prognosis & Disposition
The prognosis of the paediatric fracture generally favours healing and remodelling, and this is the single most reassuring difference from the adult. The growing bone remodels an acceptable malunion, especially when the fracture is near the physis, when the angulation lies in the plane of motion of the adjacent joint, and when the child is young with more growth remaining. Price showed that malunited forearm fractures in children remodel substantially, and the teaching is that the younger the child and the closer the fracture to the growth plate, the more the bone will correct itself. [8] [11]
The prognosis worsens predictably with the growth-plate risk. The distal radius physeal fracture heals with a low rate of arrest, but the Salter-Harris IV that crosses the whole plate, and the high-energy distal femoral and proximal tibial physeal fractures of the adolescent, carry the highest growth-arrest rates and the longest burden of deformity. The follow-up is therefore risk-stratified — weeks for the buckle, months for the distal radius physeal fracture, and until growth completion for the high-risk sites — and the physeal bar that appears on the surveillance film is the complication that re-engages the orthopaedic team. [6] [1]
The disposition is shared between the general paediatrician and emergency clinician, who own the recognition, the splinting and the safeguarding assessment, and the orthopaedic surgeon, who owns the reduction, the pinning and the growth-arrest management. The child with a common fracture is managed and discharged with clear safety-netting advice on cast care and return precautions, and the child with a high-risk or inflicted-injury pattern is referred onward to orthopaedics and, where indicated, to the safeguarding team. [7] [9]
Special Populations
The non-mobile infant with a femoral fracture or a classic metaphyseal lesion enters the safeguarding pathway, because these patterns are inflicted injury until proven otherwise. The absent or inconsistent history, the fracture that does not fit the offered mechanism, and the presence of other injuries of different ages together demand a full safeguarding workup — a skeletal survey, a child-protection referral, and the involvement of the social-paediatrics team — rather than a cast alone. The fracture is treated, but the cause is investigated. [9]
The adolescent at the growth spurt carries the highest growth-arrest risk for the high-energy distal femoral and proximal tibial physeal fractures, because the growth plate is nearing closure and a violent mechanism can cross the whole plate. These injuries demand orthopaedic reduction, internal fixation, and surveillance to growth completion, and the leg-length discrepancy or angular deformity that a physeal bar produces is managed with epiphysiodesis, bar resection, or osteotomy depending on the site and the growth remaining. [6] [1]
The child with a bleeding disorder, osteogenesis imperfecta, or another bone fragility syndrome presents with recurrent or low-trauma fractures, and the fellowship task is to distinguish the disease from inflicted injury and to manage both appropriately. A careful family and fracture history, the pattern of the fractures, the presence of blue sclerae or other stigmata, and the safeguarding assessment together separate the brittle-bone disease from the inflicted injury, and both pathways may need to run in parallel. [9] [7]
The child in a remote or rural setting needs the threatened-limb fracture recognised, splinted and retrieved safely. Telehealth orthopaedic advice guides the reduction and the decision to transfer, and the pulseless hand or the compartment syndrome is retrieved urgently to a centre with paediatric orthopaedic and theatre capability, because the time-critical injury is measured against the vascular clock. The common buckle fracture is managed locally with a soft bandage and a clear return precaution. [5] [3]
Evidence, Guidelines & Regional Differences
The Salter-Harris classification, published in 1963, remains the taught framework for growth-plate injury, and the Peterson physeal classification of 1994 refined it by adding further patterns — including the partial physeal-loss variant — that capture injuries the original five types miss. The two classifications agree that the growth plate is the prognostic organ and that the higher-energy, whole-plate-crossing injury carries the growth-arrest risk, and the fellowship candidate is expected to reproduce the Salter-Harris five and to know that Peterson extended them. [1]
The modern evidence has reshaped two areas of practice. The FORCE equivalence trial settled the buckle-fracture immobilisation debate by showing that a soft bandage was no worse than a rigid cast and gave children better function and less pain, and a systematic review and meta-analysis confirmed the bandage or splint over the cast. The lateral-entry versus crossed-pinning question for the supracondylar was settled by a meta-analysis of randomised trials and the Skaggs pin-placement study, which together showed that lateral pins reduce the iatrogenic ulnar nerve injury rate while maintaining fixation. [3] [4]
The remodelling evidence frames the acceptable malunion. Price showed that malunited forearm fractures in children remodel substantially, and Jeroense confirmed that the malunion of the distal radius in children remodels in the plane of joint motion, especially in the younger child. The teaching that follows is that the younger the child and the closer the fracture to the physis, the more malunion is accepted, and that bayonet apposition and moderate angulation remodel in the young forearm. [8] [11]
The regional differences are modest but real. The AAOS and the Royal Children's Hospital Melbourne frame the common-fracture management and the immobilisation guidance, and the contemporary ANZ and UK practice now favours the soft bandage for the buckle fracture after the FORCE trial, whereas practice in some regions still defaults to a below-elbow cast. The supracondylar pin configuration is taught as lateral-entry in most paediatric orthopaedic units, with regional variation in the use of a medial pin when lateral fixation is insufficient. [3] [2]
Exam Pearls
The fellowship answer turns on a handful of patterns and numbers. Salter-Harris type II is the commonest physeal injury at roughly three-quarters of the total, type IV crosses the whole plate and carries the highest growth-arrest risk, and type V is the crush injury with the normal initial radiograph that arrests growth late. The Gartland III supracondylar goes to theatre for emergency closed reduction and percutaneous pinning, and the anterior interosseous nerve — tested by the OK sign — is the commonest nerve injured in the extension type. [1] [5]
The examiner probes three traps. The first is the type V with the normal radiograph that later arrests growth — the physis is followed up, not dismissed. The second is the Gartland III managed in a cast without pinning — the unstable supracondylar displaces and threatens the hand. The third is the torus fracture over-immobilised in a rigid cast when the FORCE trial showed a soft bandage to be no worse. A candidate who names these three traps and their safeguards demonstrates the pattern-level thinking the fellowship rewards. [3] [6]
The examiner rewards the candidate who frames the paediatric fracture around the growth plate, the remodelling potential, and the safeguarding duty. The bone grows because of the physis, the fracture is read through the physis, and the child is followed because of the physis; the malunion is accepted because the bone remodels; and the fracture in the non-walking infant or with the classic metaphyseal lesion is investigated, not just cast. This three-part framing — growth, remodelling, safeguarding — is the fellowship answer in miniature. [1] [9]
The Salter-Harris types — SALTR
References
- [1]Peterson HA. Physeal fractures: Part 3. Classification. J Pediatr Orthop, 1994.PMID 8077424
- [2]Pakarinen O, Saarinen AJ, Ponkilainen VT, Uimonen M, Helenius I, Kuitunen I. Soft bandage, splint or cast as the treatment of distal forearm torus fracture in children: a systematic review and meta-analysis. Sci Rep, 2024.PMID 39251716
- [3]Perry DC, Achten J, Knight R, Dutton SJ, Dritsaki M, Mason JM, Appelbe DE, Roland DT, Messahel S, Widnall J, Gibson P, Costa ML. Offer of a bandage versus rigid immobilisation in 4- to 15-year-olds with distal radius torus fractures: the FORCE equivalence RCT. Health Technol Assess, 2022.PMID 35904496
- [4]Kwok SM, Clayworth C, Nara N. Lateral versus cross pinning in paediatric supracondylar humerus fractures: a meta-analysis of randomized control trials. ANZ J Surg, 2021.PMID 33792121
- [5]Skaggs DL, Hale JM, Bassett J, Kaminsky C, Kay RM, Tolo VT. Operative treatment of supracondylar fractures of the humerus in children. The consequences of pin placement. J Bone Joint Surg Am, 2001.PMID 11379744
- [6]Peterson HA, Shaughnessy WJ, Stans AA. Physeal bar equivalent. J Pediatr Orthop B, 2017.PMID 27748675
- [7]Noonan KJ, Price CT. Forearm and distal radius fractures in children. J Am Acad Orthop Surg, 1998.PMID 9689186
- [8]Price CT, Scott DS, Kurzner ME, Flynn JC. Malunited forearm fractures in children. J Pediatr Orthop, 1990.PMID 2250053
- [9]Kleinman PK, Perez-Rossello JM, Newton AW, Feldman HA, Kleinman PL. Prevalence of the classic metaphyseal lesion in infants at low versus high risk for abuse. AJR Am J Roentgenol, 2011.PMID 21940592
- [10]Cramer KE, Green NE, Devito DP. Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop, 1993.PMID 8370784
- [11]Jeroense KT, America T, Witbreuk MM, van der Sluijs JA. Malunion of distal radius fractures in children. Acta Orthop, 2015.PMID 25355309