Paeds · rheumatology-musculoskeletal-and-sports
Developmental dysplasia of the hip
Also known as DDH · congenital hip dislocation · congenital dislocation of the hip · CDH · hip dysplasia · Ortolani positive hip · Graf classification · Pavlik harness · acetabular dysplasia
A fellowship approach to developmental dysplasia of the hip: the Ortolani and Barlow manoeuvres in the newborn, the Graf ultrasound angles that grade the infant hip, the Pavlik harness that reduces it, and the late-presenting toddler whose painless limp and short leg declare a hip that screening missed.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A six-week-old girl born in the breech position has a soft clunk on the left Ortolani test, her ultrasound shows a Graf type III hip with an alpha angle of forty degrees, and a Pavlik harness is fitted and checked at three weeks to confirm reduction. A three-month-old boy with a normal newborn examination now has asymmetric thigh folds and limited left abduction, and his ultrasound reveals a shallow acetabulum with an alpha angle of fifty-two degrees, a Graf type IIb hip that has declared after the neonatal screen. A two-year-old girl who was never screened walks in with a painless left-sided limp, a short left leg, and a left hip that shifts upward and outward on the radiograph, a late-presenting dislocation that now needs an open reduction. The task in each is to screen at the right age, to image with the right modality, and to match the treatment to the age of the child. [2] [10]
The five moves of the dysplastic hip — Screen, Image, Grade, Harness, Refer
Overview & Definition
Developmental dysplasia of the hip describes a spectrum of abnormal development of the hip joint that is present at or soon after birth. At the mild end sits a capsular laxity that allows the femoral head to sublux, and at the severe end sits a fixed dislocation in which the head has migrated completely out of the acetabulum and come to rest against the ilium. The older name, congenital dislocation of the hip, has fallen from favour because the condition is not always present at birth and because the spectrum includes dysplasia without dislocation. [2]
The clinical importance of the condition comes from what an untreated dysplastic hip does to the adult. A shallow acetabulum and an unstable head fail to distribute load, the cartilage wears, and the joint develops osteoarthritis by the fourth or fifth decade. A dislocated hip that is never reduced leaves the child with a short leg, a limp, and a restricted, painful joint through childhood. The whole enterprise of newborn screening exists because the hip found and treated in the first months of life recovers almost completely, while the hip found in the toddler needs surgery and never quite returns to normal. [5] [10]
The fellowship candidate holds the condition as a time-sensitive problem. The neonate with a clunk is the prize, because a Pavlik harness worn for a few weeks will usually restore a normal hip. The infant with limited abduction is still salvageable with a harness or a closed reduction. The toddler with a limp has crossed into surgical territory, and the adolescent with residual dysplasia is managed to delay arthritis, not to cure it. The age at which the hip is found is the single strongest determinant of the outcome. [2] [11]
Classification
The dysplastic hip is classified by two complementary systems, and each owns a different age of the child. The Graf ultrasound classification grades the cartilaginous hip of the infant under six months, before the femoral head ossifies and becomes visible on a radiograph. The International Hip Dysplasia Institute radiographic classification grades the ossified hip of the older infant and child, once the head can be seen on a plain film. The fellowship candidate uses both, because they describe the same hip at different points in its maturation. [1] [6]
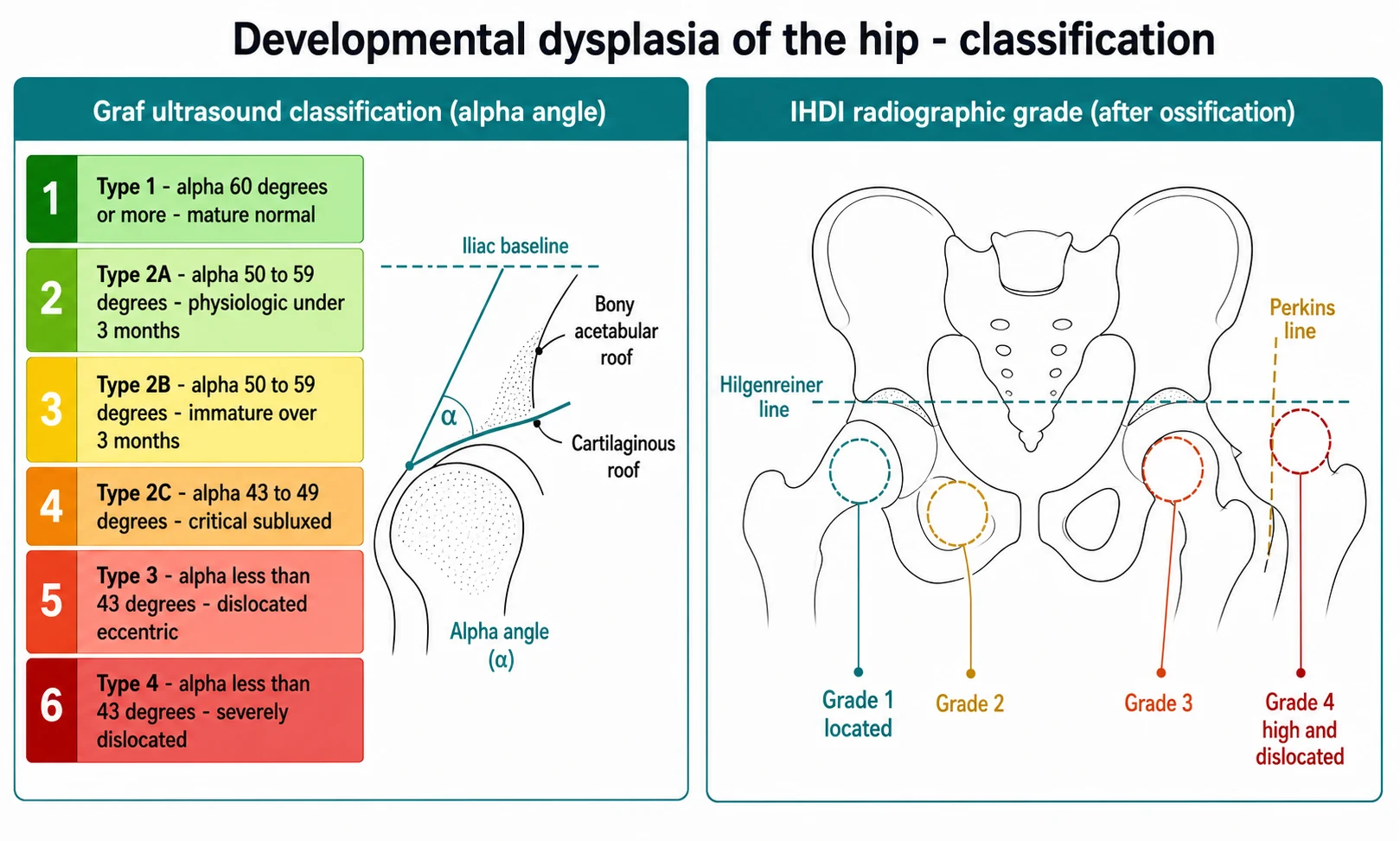
The Graf classification is built on the alpha angle, which measures the slope of the bony acetabular roof against the vertical iliac baseline on a coronal ultrasound. An alpha angle of sixty degrees or more marks a mature, normal hip, a Graf type I. An angle of fifty to fifty-nine degrees marks an immature hip, and the label splits by age: type IIa is the physiologic immaturity of a baby under three months that is expected to mature, while type IIb is the abnormal immaturity of a baby over three months that will not. An angle of forty-three to forty-nine degrees marks the critical zone, type IIc, where the head is still centred but the socket is shallow enough to sublux. An angle below forty-three degrees marks a dislocated hip, type III when eccentric and type IV when severely displaced. [1] [9]
The International Hip Dysplasia Institute classification grades the position of the ossified femoral head against two reference lines on an anteroposterior pelvis radiograph. Hilgenreiner's line runs horizontally through the triradiate cartilages, and Perkins's line drops vertically from the lateral edge of the acetabulum, perpendicular to Hilgenreiner's line. A normal head sits in the inner lower quadrant below Hilgenreiner's line and medial to Perkins's line, a grade I hip. Grades II, III, and IV describe a head that migrates progressively upward and lateral, and a grade IV head rides high against the ilium. The acetabular index, measured from Hilgenreiner's line to the sloping acetabular roof, sits below twenty-five degrees in a normal infant and above thirty degrees in a dysplastic one. [6] [2]
Epidemiology & Risk Factors
Developmental dysplasia of the hip is one of the commonest musculoskeletal conditions of infancy, and its reported incidence depends on how it is counted. Clinical instability at birth is found in roughly one to two per thousand live births, while sonographic dysplasia, which includes milder forms, is far commoner and is reported in the range of several per hundred. The gap between the two figures is the essence of the condition: many dysplastic hips are sonographically abnormal but clinically silent, and most mature on their own without treatment. [3] [4]
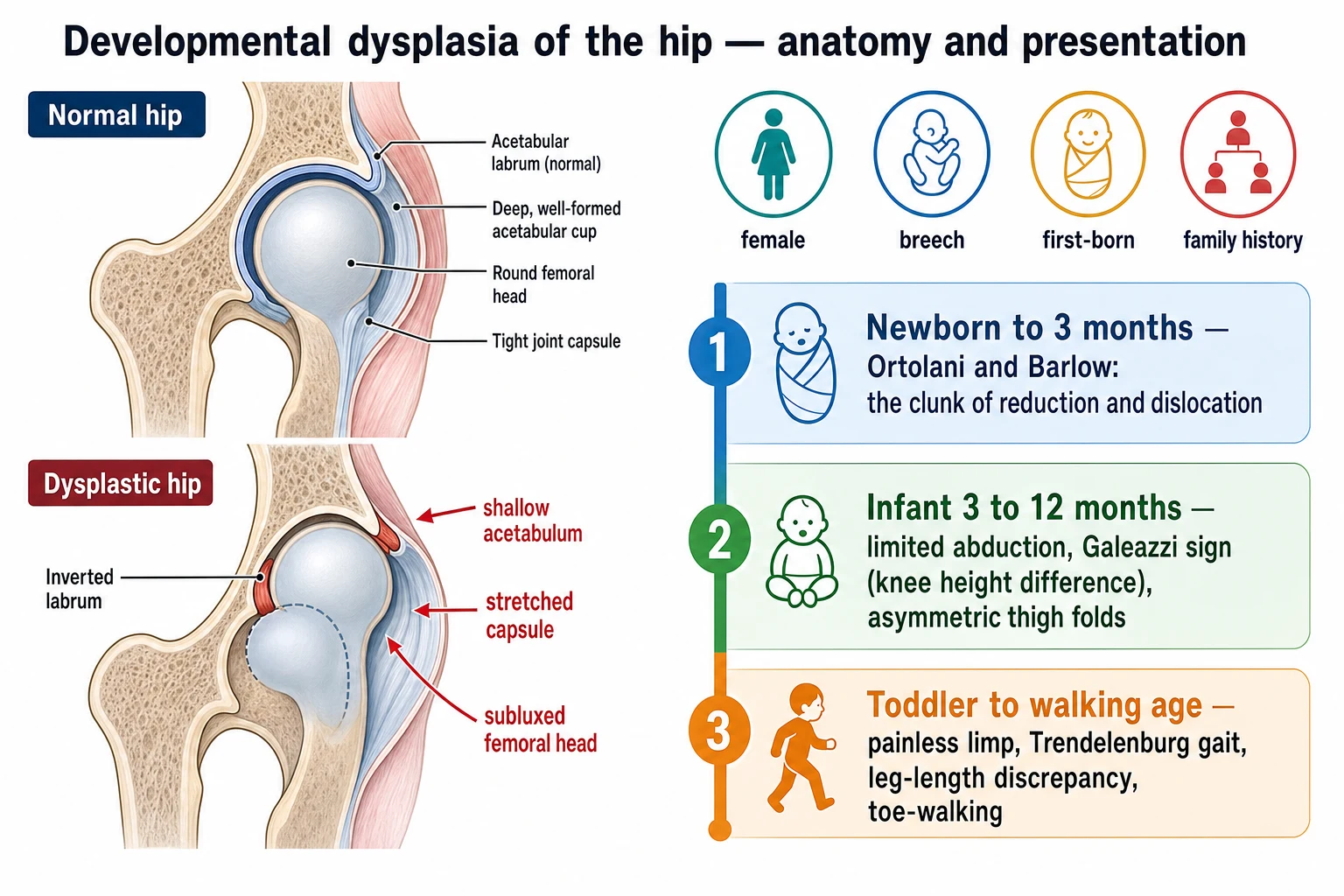
The risk factors cluster around the mechanical environment of the womb and the genetic background of the child. A baby in the breech position, especially after thirty-four weeks of gestation, has had the hips held flexed against a stretched capsule, and the risk is high enough that current selective-screening guidance mandates an ultrasound for every breech baby regardless of sex. A first-born child has been compressed by a primigravid uterus and abdominal wall, and a family history in a first-degree relative raises the risk further. Girls are affected roughly four to eight times more often than boys, a difference attributed in part to maternal relaxin crossing the placenta and loosening the female infant's ligaments. [5] [2]
Several further factors complete the bedside assessment. Oligohydramnios reduces the space available for the fetus and forces the hips into flexion, and postural foot deformities such as metatarsus adductus and congenital torticollis travel with dysplasia often enough that their presence lowers the threshold for ultrasound. The left hip is affected more often than the right, because most fetuses lie in the left occiput anterior position with the left hip pressed against the maternal sacrum. Swaddling with the legs held extended and adducted is a modifiable postnatal risk factor, and counselling families on hip-safe swaddling, with the legs free to flex and abduct, is part of prevention. [2] [5]
Pathophysiology
The pathophysiology of developmental dysplasia of the hip is a disorder of the ball-and-socket relationship, and the fellowship candidate understands it as a mechanical sequence that begins with laxity and ends with dislocation. A normal hip has a deep acetabulum that cradles a round femoral head, and the two grow together under the stimulus of reciprocal contact. When the capsule is lax or the acetabulum is shallow, the head is no longer held firmly, the reciprocal stimulus is lost, and the socket grows even shallower as the head drifts upward and outward. [2]
The early lesion is capsular laxity, and it is the state that the Ortolani and Barlow tests detect. The head can be pushed out of the socket and pushed back in, and at this stage the acetabulum and the head are still essentially normal in shape. If the laxity resolves, as it does in most babies, the hip matures normally. If the laxity persists, the head spends more time subluxed than seated, the acetabular rim flattens under the uneven load, and the labrum inverts and is pushed into the joint. The hip moves from laxity to dysplasia to subluxation, and each step deepens the structural abnormality. [1] [2]
The late lesion is a fixed dislocation. The head has migrated fully out of the acetabulum and rests against the ilium, the capsule stretches and narrows into an hourglass shape that traps the head outside, the psoas and adductor muscles tighten and pull the head upward, and the acetabulum fills with fibro-fatty tissue known as pulvinar. At this stage the hip cannot be reduced by manipulation alone, the soft tissues have remodelled around the dislocation, and an open operation is needed to clear the obstruction and bring the head back into the socket. The pathology explains why a late hip needs surgery and an early hip does not. [10]
Clinical Presentation
The presentation of developmental dysplasia of the hip is shaped entirely by the age at which the child is examined, because the hip that produces a clunk in the newborn produces only a stiff hip in the infant and a limp in the toddler. The fellowship candidate holds the age-stratified presentation in mind from the first moment the child is in the room. [2] [5]
The newborn, examined in the first days and weeks of life, is screened with the Ortolani and Barlow manoeuvres. The Ortolani test is performed with the baby supine and relaxed, the hips flexed to ninety degrees and the knees held in the examiner's hands. The hips are gently abducted while the examiner lifts the greater trochanters forward, and a dislocated head sliding back into the acetabulum produces the clunk of reduction. The Barlow test is the provocative complement: with the hips flexed and adducted, the examiner pushes the femur gently backward and outward, and an unstable head sliding out of the socket produces the clunk of dislocation. A positive test is felt in the examiner's hands more than it is heard, and it is the sign of true instability. [2] [5]
The infant beyond three months presents differently, because the soft tissues have tightened around the displaced head and the clunk can no longer be provoked. The hip now declares itself through limited abduction, which is the single most reliable sign in this age group, and the loss is often asymmetric, with the affected hip abducting less than the normal side. The Galeazzi or Allis test, performed with the hips and knees flexed and the feet flat on the couch, reveals a knee at different heights when the femur has been displaced upward, and asymmetric thigh and gluteal folds often accompany it. The Ortolani and Barlow tests become negative as the dislocation fixes, and the candidate who relies on them alone will miss the older infant. [2]
The toddler and the walking-age child present with the gait of a dislocated hip. The affected leg is short, because the femoral head has migrated upward, and the child walks with a painless limp, dropping the contralateral pelvis in a Trendelenburg pattern from abductor weakness. Many toe-walk on the short side to compensate for the leg-length difference, and bilateral dislocations produce a waddling, hyperlordotic gait rather than a limp. The diagnosis is confirmed on a plain anteroposterior pelvis radiograph, which shows the femoral head riding high and lateral to Perkins's line above a shallow acetabulum. [10]
Differential Diagnosis
The differential diagnosis of an abnormal infant hip examination is short, but each entry changes the management. The first task is to separate the true instability of dysplasia from the benign soft-tissue click, and the distinction rests on the quality of the finding: a clunk that relocates or dislocates the head is abnormal, while a click that neither moves the head nor persists with instability is benign. The risk-factor assessment guides the threshold for imaging a click, because a click in a breech baby with a family history is worked up, while a click in a low-risk baby with a stable hip is observed. [5]
A proximal focal femoral deficiency and a congenital coxa vara may mimic a short leg and an asymmetric fold, but the hip joint itself is stable and the radiograph shows the abnormal femur rather than a dislocated head. A teratologic dislocation, seen with arthrogryposis, myelodysplasia, or Larsen syndrome, is a fixed dislocation present at birth with a rigid hip and other joint contractures, and it is not managed with a Pavlik harness because the pathology is structural rather than lax. Septic arthritis of the infant hip produces a febrile, irritable child who holds the hip rigidly and refuses to move it, and it is distinguished from dysplasia by the fever, the inflammatory markers, and the ultrasound effusion. [2]
The older child with a limp carries the broader differential of the limping child, and the fellowship candidate keeps developmental dysplasia on the list alongside transient synovitis, Perthes disease, slipped capital femoral epiphysis, and septic arthritis. The painless, chronic, afebrile limp with a short leg points toward dysplasia, while the painful, febrile, acute limp points toward infection. A pelvis radiograph separates the structural causes, and the age of the child guides the suspicion: dysplasia in the toddler, Perthes in the young school-age child, and slipped capital femoral epiphysis in the adolescent. [2] [10]
Clinical & Bedside Assessment
The bedside assessment begins with the newborn hip examination, performed on a calm, relaxed baby, because a crying baby tightens the muscles and masks the instability. The baby is laid supine on a firm surface, and the examiner warms the hands before placing them on the child. Both hips are examined together, with the hips and knees flexed to ninety degrees and the examiner's thumbs on the inner thighs and the fingers over the greater trochanters. [2] [5]
The Ortolani test is the test of reduction. The hips are abducted gently, one at a time or together, while the fingers lift the greater trochanters forward toward the acetabulum. A dislocated head that clunks back into the socket is a positive Ortolani, and it is felt as a distinct shift, not a soft sound. The Barlow test is the test of provocation, performed after the Ortolani: the hip is adducted across the midline while the examiner pushes the femur gently backward, and a head that clunks out of the socket is a positive Barlow. Both tests are most reliable in the first six weeks of life, and they become negative as the soft tissues tighten and the dislocation fixes. [5] [2]
Beyond the neonatal period, the assessment shifts to the signs of an established dysplasia. Abduction is tested with the hip flexed, and a loss of abduction, particularly when asymmetric, is the single most reliable sign in the infant. The Galeazzi test compares the knee heights with the hips flexed and the feet flat, and a lower knee on the affected side signals a proximal migration of the femur. The skin folds of the thigh and groin are inspected for asymmetry, though asymmetric folds alone are neither sensitive nor specific and must be read with the rest of the examination. Leg length is compared from the anterior superior iliac spine to the medial malleolus, and a Trendelenburg test is performed in the walking child. [2]
Which findings must never be dismissed? A positive Ortolani or Barlow in any baby is a clunk of true instability that demands ultrasound and orthopaedic review, regardless of the risk factors. A loss of abduction in an infant beyond three months is an established dysplasia until imaging proves otherwise. And a painless limp with a short leg in a toddler is a late-presenting dislocation that demands a pelvis radiograph the same day, because each month of delay narrows the surgical options and worsens the long-term outcome. [10] [5]
Investigations
The investigation of developmental dysplasia of the hip is chosen by the age of the child and the state of the femoral head. In the infant under six months, before the femoral head ossifies, the hip is imaged with ultrasound, because ultrasound sees the cartilaginous head and the acetabular roof that the radiograph cannot. In the older infant and child, once the head ossifies, the plain anteroposterior pelvis radiograph becomes the investigation of choice, because ultrasound loses its window once the bone appears. [1] [2]
The hip ultrasound is performed by a trained sonographer using the Graf technique, with the baby relaxed and the probe placed coronally over the lateral hip. The alpha angle of the bony acetabular roof is measured against the vertical iliac baseline, and the beta angle of the cartilaginous roof is measured as a secondary guide. The alpha angle is the load-bearing value: sixty degrees or more is normal, fifty to fifty-nine degrees is immature, forty-three to forty-nine degrees is critical, and below forty-three degrees is dislocated. The ultrasound is also used to confirm the reduction of a hip held in a Pavlik harness, because a harness that looks well placed can still hold the head displaced posteriorly. [1] [9]
The plain radiograph is the investigation of the older infant and the walking child. The anteroposterior pelvis view shows the ossified femoral head in relation to Hilgenreiner's and Perkins's lines, the slope of the acetabular roof as the acetabular index, and the integrity of Shenton's line, the smooth arc that runs from the inferior pubic ramus up the femoral neck and breaks when the head is displaced. The acetabular index sits below twenty-five degrees in a normal infant and rises above thirty degrees in a dysplastic one, and the International Hip Dysplasia Institute grade locates the head in one of four positions of increasing displacement. Magnetic resonance imaging is reserved for the assessment of reduction in difficult cases and for the cartilage that the radiograph cannot see. [6] [2]
Management — Resuscitation
Resuscitation is rarely the primary concern in developmental dysplasia of the hip, because the condition is not immediately life-threatening and most babies are well. The priority at the first encounter is the accurate diagnosis, the risk stratification, and the timely referral, because the harm of the condition is the slow destruction of the joint over months and years rather than an acute collapse. The general paediatrician's resuscitation role is to recognise the clunk, image the hip, and refer to the orthopaedic team before the window for non-operative treatment closes. [2] [11]
The exception is the older infant or child who presents for a closed or open reduction and needs a general anaesthetic. These children undergo a pre-operative assessment, the hip is imaged to plan the operation, and the family is counselled on the procedure, the spica cast, and the rehabilitation. Pain is controlled with simple analgesia and regional techniques as appropriate, and the child is prepared for a period of immobilisation that follows the reduction. The resuscitation principle here is the safe conduct of an elective operation, with attention to the airway, the fasting status, and the consent. [10]
The child with an associated syndrome or neuromuscular condition, such as arthrogryposis or myelodysplasia, may have a teratologic dislocation that behaves differently from the classic developmental form, and the management is individualised with the orthopaedic and paediatric teams together. These children are not managed with a Pavlik harness, because the dislocation is structural and rigid, and the workup includes the identification and stabilisation of the underlying condition before the hip is addressed. [2]
Management — Definitive & Stepwise
The definitive management of developmental dysplasia of the hip is a stepwise ladder that climbs with the age of the child, and the step chosen at each age reflects how much the soft tissues have remodelled around the displacement. The infant under six months is managed with a Pavlik harness, the older infant with a closed reduction and a spica cast, the toddler with an open reduction, and the adolescent with residual dysplasia with a pelvic osteotomy. [2] [7]
The Pavlik harness is the first step and the foundation of non-operative management. It is a soft, dynamic splint that holds the hips flexed to about one hundred degrees and abducted to about fifty degrees, a position that points the femoral head toward the acetabulum and allows it to reduce under the pull of its own muscles. It is worn for twenty-three hours a day, and the reduction is confirmed with an ultrasound at three weeks. A hip that has reduced is kept in the harness for a total of six to twelve weeks until the acetabulum matures, while a hip that has not reduced by three weeks is taken out of the harness, because continued forced abduction against a dislocated head causes avascular necrosis. The Pavlik harness succeeds in the great majority of reducible dysplastic hips detected under six months, including many Graf type III and IV hips when applied correctly. [7] [8]
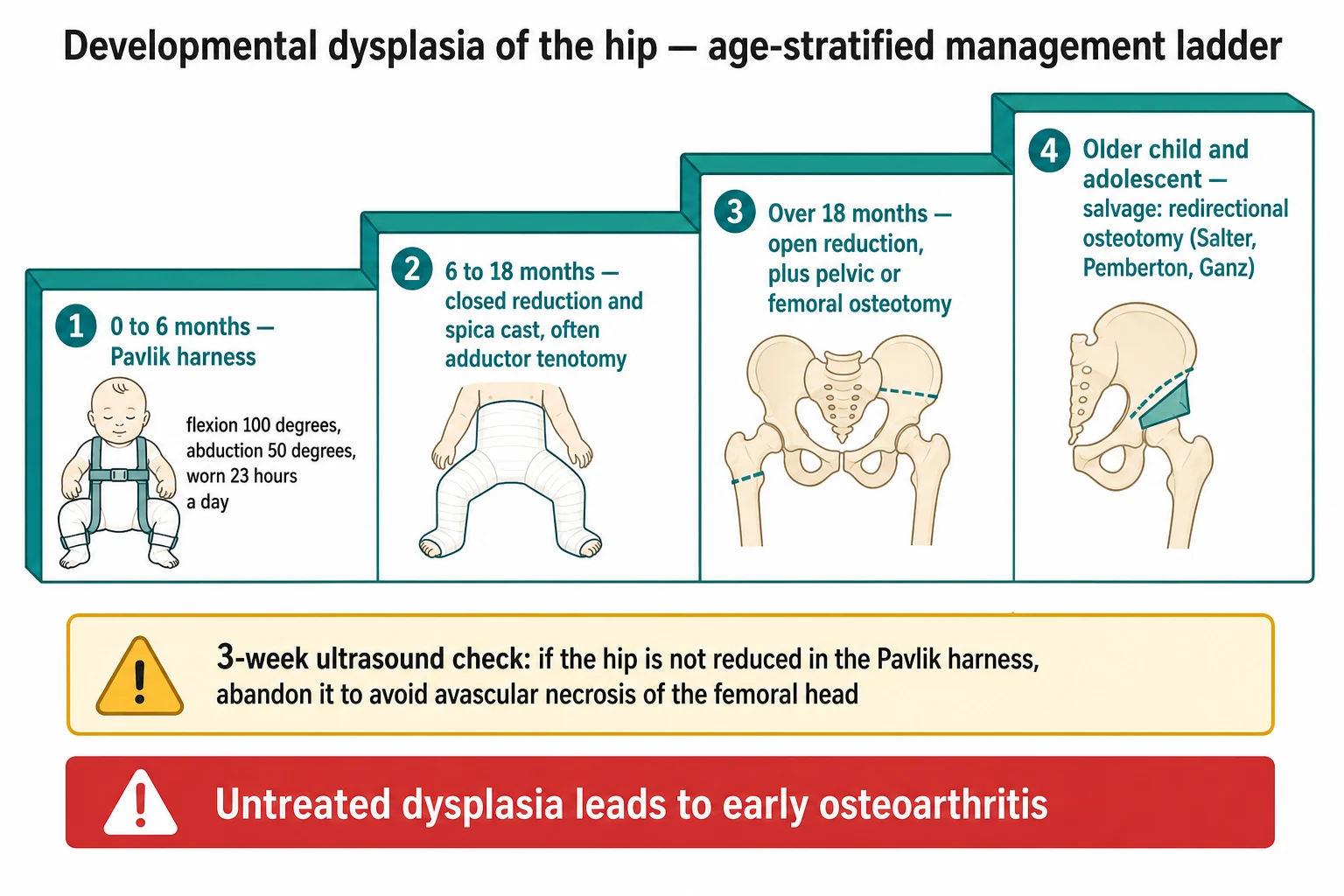
The second step is the closed reduction with a spica cast, reserved for the infant in whom the Pavlik harness has failed or who presents between six and eighteen months. Under anaesthetic, the hip is manipulated back into the acetabulum, often after a period of traction and an adductor tenotomy to release the tight muscles, and a spica cast holds the reduced position for around three months. An arthrogram, with dye injected into the joint, confirms that the head is deeply seated and stable. The closed reduction is preferred over an open operation when it can be achieved without excessive pressure on the head, because pressure, like forced abduction in the harness, risks avascular necrosis. [2] [10]
The third step is the open reduction, reserved for the child over eighteen months or the hip that cannot be reduced closed. The surgeon clears the obstructing soft tissue, the inverted labrum and the pulvinar, from the acetabulum, brings the head back into the socket, and tightens the capsule. A pelvic osteotomy, such as a Salter or Pemberton, may be added to redirect the shallow acetabulum over the head, and a femoral osteotomy may correct a valgus or anteverted neck. The older the child at open reduction, the less complete the remodelling and the greater the risk of residual dysplasia and stiffness. [10]
The fourth step, for the older child and adolescent with residual acetabular dysplasia, is a redirectional pelvic osteotomy such as the Ganz periacetabular osteotomy, which reorientates the socket to cover the head and delay the onset of arthritis. At this stage the joint is preserved rather than cured, and the goal is to postpone the need for a total hip replacement into late adulthood rather than to restore a normal hip. [10]
The four steps of the management ladder
Specific Subtypes & Scenarios
The breech-presenting infant is the highest-yield scenario for early detection, because the mechanical environment of the breech position stretches the capsule and flattens the acetabular roof. Current selective-screening guidance, mindful of the high miss rate of the clinical examination alone, recommends an ultrasound of the hips for every breech baby, regardless of sex, by six weeks of age. A baby with a first-degree family history of dysplasia is offered the same selective ultrasound, because the genetic contribution roughly doubles the risk. The fellowship candidate treats the breech baby and the family-history baby as pre-selected for imaging, and the clinical examination becomes a safeguard rather than the sole screen. [5] [3]
The Graf type IIa hip is the scenario that teaches patience, because it is the physiologic immaturity of a baby under three months that is expected to mature on its own. The alpha angle sits between fifty and fifty-nine degrees, and the management is observation with a repeat ultrasound at six weeks, because most of these hips mature into a normal type I without treatment. The decision to splint a type IIa hip rests on the stability of the hip on dynamic ultrasound and on the trend of the alpha angle over time, and over-treatment with a harness exposes a hip that would have matured anyway to a small but real risk of avascular necrosis. [9] [11]
The late-presenting toddler is the scenario that exposes the limits of screening. A child who slipped through the newborn screen, or who was never screened, walks in at two or three years of age with a painless limp, a short leg, and a hip that has been dislocated for as long as it has been weight-bearing. The radiograph shows the femoral head riding high against the ilium above a shallow, empty acetabulum, and the management is an open reduction with the soft-tissue clearance and the osteotomies described above. The outcome is guarded, because the acetabulum and the head have remodelled around the dislocation and never fully recover, and the hip is at lifelong risk of stiffness and arthritis. [10] [5]
The bilateral dislocation is the scenario that is easy to miss, because the symmetry of the findings hides the abnormality. Both hips are limited in abduction, the Galeazzi test is symmetrically negative because both legs are shortened equally, and the child walks with a waddling, hyperlordotic gait rather than a unilateral limp. The fellowship candidate examines both hips, images both when either is abnormal, and remembers that a symmetric examination is not necessarily a normal one. [2] [10]
Complications & Pitfalls
The complications of developmental dysplasia of the hip are the complications of the untreated disease and the complications of its treatment, and the fellowship candidate holds both in balance. The untreated dislocation leaves the child with a short leg, a limp, a restricted and painful joint, and an early osteoarthritis that declares in the fourth or fifth decade. The dysplastic hip that is reduced but incompletely remodeled carries a lifelong risk of residual acetabular dysplasia and progressive arthritis. [10] [2]
Avascular necrosis of the femoral head is the most feared complication of treatment, and it is caused by the very manoeuvres that reduce the hip. Forced abduction in a Pavlik harness, excessive pressure during a closed reduction, and the dissection of an open operation all compromise the tenuous blood supply to the growing head, and the result is a flattened, fragmented head that grows into a deformed, arthritic joint. The prevention is the gentle reduction confirmed by imaging, the abandonment of a harness that has not reduced the hip within three weeks, and the avoidance of extreme abduction positions. [7] [8]
The pitfall of the over-called click is the error that exposes a normal hip to unnecessary treatment. A benign soft-tissue click in a low-risk baby is read as instability, the baby is placed in a harness, and a hip that would have matured normally is exposed to the small risk of avascular necrosis for no benefit. The safeguard is the careful distinction between the clunk that moves the head and the click that does not, the disciplined use of ultrasound to confirm a true dysplasia, and the observation of the low-risk type IIa hip that is expected to mature. [5] [11]
The pitfall of the missed late presentation is the error that denies a child the chance of a simpler cure. A toddler with a painless limp is discharged without a hip radiograph, the dislocation progresses, and the child returns at an age when only an open operation with a guarded outcome is possible. The safeguard is the rule that every toddler with a painless limp and a short leg receives a pelvis radiograph, because the late-presenting dislocation is found on the film and not on the examination alone. [10]
Prognosis & Disposition
The prognosis of developmental dysplasia of the hip is excellent when the condition is detected and treated in the first months of life. A hip reduced in a Pavlik harness before six months, and confirmed reduced at the three-week ultrasound, recovers almost completely, and the child grows up with a normal hip and a normal gait. The acetabulum matures under the stimulus of the seated head, the capsule tightens, and the long-term risk of arthritis falls close to that of the general population. [7] [2]
The prognosis worsens as the age at detection rises. A hip reduced by closed reduction between six and eighteen months does well in most children, though a minority develop residual dysplasia or avascular necrosis that declare over the growing years. A hip reduced by open reduction over eighteen months has a guarded outcome, because the remodelling is incomplete and the joint is at lifelong risk of stiffness and arthritis. The late-presenting dislocation carries the poorest prognosis, and many of these children need further operations through childhood and a hip replacement in early or middle adulthood. [10]
The disposition is shared between the general paediatrician, the paediatric orthopaedic surgeon, and the sonographer. The general paediatrician owns the newborn screen, the risk-factor assessment, the timely ultrasound, and the referral. The paediatric orthopaedic surgeon owns the harness, the reductions, and the osteotomies. The sonographer owns the Graf measurement and the confirmation of reduction. The fellowship answer names the right specialist for the right stage and never holds a clunk in the outpatient clinic when the orthopaedic pathway is indicated. [11] [2]
Special Populations
Children in remote and Indigenous communities face the additional burdens of access and equity in the detection of dysplasia. The distance to a trained sonographer and a paediatric orthopaedic service delays the ultrasound and the referral, and the late-presenting dislocation is over-represented in these settings. The fellowship answer builds the rapid-referral pathways that close the gap, with a low threshold for imaging and a clear route from the remote clinic to the regional orthopaedic service, because the harm of the late detection falls hardest on the child furthest from the centre. [10] [5]
The newly arrived migrant or refugee infant may carry an undocumented history of screening, and the workup may need to begin from first principles. A reliable hip examination and a timely ultrasound are offered regardless of the prior history, because a missed dysplasia in a displaced child is a preventable harm. The candidate takes the time to establish the risk factors, the family history, and the birth history, and arranges the imaging that the prior setting may not have provided. [3]
Children with developmental disability and neuromuscular conditions may carry a teratologic rather than a developmental dislocation, and the management differs from the classic pathway. A child with arthrogryposis, myelodysplasia, or cerebral palsy may have a rigid, structural dislocation that does not respond to a Pavlik harness, and the workup includes the identification and the stabilisation of the underlying condition. The threshold for orthopaedic referral is low, because these hips behave differently and the treatment is individualised to the child's overall prognosis and function. [2]
Evidence, Guidelines & Regional Differences
The evidence base for screening developmental dysplasia of the hip is the battleground of the field, because no trial has ever proven that universal screening changes the long-term outcome, and the regional practice reflects the local reading of the evidence. The systematic review prepared for the United States Preventive Services Task Force in 2006 concluded that the evidence was insufficient to recommend universal screening, and the Task Force left the decision to the clinician and the family. The Cochrane review of screening programmes in newborn infants found no randomised evidence that any single screening strategy reduced the late presentation or the need for surgery. [3] [4]
The regional differences are real and consequential. Austria and Germany operate a universal ultrasound screening programme, with a Graf scan offered to every baby at around four to six weeks, and the reported rates of late presentation and open operation fell after its introduction. The United Kingdom operates a selective strategy, with a clinical newborn examination for every baby and a selective ultrasound reserved for the breech baby and the family-history baby, and the rates of late presentation have not fallen to the same degree, a finding attributed to the imperfect sensitivity of the clinical examination. The Perry and Paton critique framed the problem sharply, asking whether the current screening is fit for purpose when the click is over-investigated and the clunk is sometimes missed. [5] [3]
The evidence for the Pavlik harness rests on the systematic review of the method and on the cohorts of Graf type III and IV hips treated by Pavlik, which show that the harness succeeds in a high proportion of reducible dislocated hips when it is applied correctly and monitored at three weeks. The Cochrane review of splinting in children under six months, updated in 2022, noted the limited randomised evidence and the reliance on observational data, and it called for trials that compare the harness with watchful waiting and with alternative splints. [7] [11]
The controversies are few but genuine. The threshold for splinting a Graf type IIa hip, the role of the adductor tenotomy in the closed reduction, and the decision to perform a pelvic osteotomy at the time of the open reduction are the judgement calls that the fellowship answer names without pretending that a single algorithm resolves them. The general paediatrician applies the evidence, recognises the uncertainty, and involves the orthopaedic team when the decision sits at the margin. [9] [2]
Exam Pearls
The fellowship answer turns on five facts. Developmental dysplasia of the hip is a spectrum from neonatal laxity to fixed dislocation, and the Ortolani and Barlow tests detect the early, reducible form. The Graf alpha angle grades the infant hip: sixty degrees or more is normal, below forty-three degrees is dislocated, and the type sets the treatment. The Pavlik harness reduces most hips under six months, and the three-week ultrasound confirms it. The hip unreduced at three weeks must come out of the harness to avoid avascular necrosis. And the late-presenting toddler with a painless limp and a short leg needs a pelvis radiograph, because the film, not the examination, makes the diagnosis. [2] [7]
The examiner probes three traps. The first is the clunk that is dismissed as a click, the benign soft-tissue finding that neither relocates nor dislocates the head, and the safeguard is the quality of the finding felt in the hands. The second is the type IIa hip that is splinted unnecessarily, the physiologic immaturity that would have matured, and the safeguard is the repeat ultrasound and the trend of the alpha angle. The third is the harness that is continued past three weeks in a hip that has not reduced, the forced abduction that causes avascular necrosis, and the safeguard is the ultrasound that confirms the reduction or prompts the abandonment. [5] [8]
The examiner rewards the candidate who frames the condition as a time-sensitive problem. The newborn is screened, the at-risk infant is imaged, the dysplastic hip is graded and matched to the age, and the right step of the ladder is chosen at the right time. The family is counselled on hip-safe swaddling, the harness is monitored, and the late presentation is caught on the radiograph. A candidate who shows this sequence demonstrates the systems thinking that the fellowship demands. [10] [11]
References
- [1]Graf R. The diagnosis of congenital hip-joint dislocation by the ultrasonic Combound treatment. Archives of Orthopaedic and Traumatic Surgery, 1980.PMID 7458597
- [2]Guille JT, Pizzutillo PD, MacEwen GD. Development dysplasia of the hip from birth to six months. Journal of the American Academy of Orthopaedic Surgeons, 2000.PMID 10951112
- [3]Shipman SA, Helfand M, Moyer VA, Yawn BP. Screening for developmental dysplasia of the hip: a systematic literature review for the US Preventive Services Task Force. Pediatrics, 2006.PMID 16510634
- [4]Shorter D, Hong T, Osborn DA. Screening programmes for developmental dysplasia of the hip in newborn infants. Cochrane Database of Systematic Reviews, 2011.PMID 21901691
- [5]Perry DC, Paton RW. Knowing your click from your clunk: is the current screening for developmental dysplasia of the hip fit for purpose? The Bone and Joint Journal, 2019.PMID 30813794
- [6]Narayanan U, Mulpuri K, Sankar WN, Clarke NM, Hosalkar H, Price CT, et al. Reliability of a New Radiographic Classification for Developmental Dysplasia of the Hip. Journal of Pediatric Orthopaedics, 2015.PMID 25264556
- [7]Tibrewal S, Gulati V, Ramachandran M. The Pavlik method: a systematic review of current concepts. Journal of Pediatric Orthopaedics Part B, 2013.PMID 23995089
- [8]Peled E, Bialik V, Katzman A, Eidelman M, Norman D. Treatment of Graf's ultrasound class III and IV hips using Pavlik's method. Clinical Orthopaedics and Related Research, 2008.PMID 18288557
- [9]Bilgili F, Saglam Y, Goksan SB, Hurmeydan OM, Birisik F, Demirel M. Treatment of Graf Type IIa Hip Dysplasia: A Cut-off Value for Decision Making. Balkan Medical Journal, 2018.PMID 29966996
- [10]Terjesen T, Horn J. Have Changes in Treatment of Late-detected Developmental Dysplasia of the Hip During the Last Decades Led to Better Radiographic Outcome? Clinical Orthopaedics and Related Research, 2016.PMID 26290341
- [11]Dwan K, Kirkham J, Paton RW, Morley E, Newton AW, Perry DC. Splinting for the non-operative management of developmental dysplasia of the hip (DDH) in children under six months of age. Cochrane Database of Systematic Reviews, 2022.PMID 36214650