Paeds · rheumatology-musculoskeletal-and-sports
Heat illness, exertional collapse and sudden death prevention
Also known as exertional heat illness · exertional heat stroke · exercise-associated collapse · heat exhaustion · cold water immersion · wet-bulb globe temperature · heat acclimatization · sudden cardiac arrest in young athletes · emergency action plan · cool first transport second
A fellowship approach to exertional heat illness, exercise-associated collapse, and the prevention of sudden death in the young athlete: the spectrum runs from exercise-associated muscle cramps and heat exhaustion to exertional heat stroke, and the central rule is that an athlete who collapses during exercise with altered mental status has exertional heat stroke until a rectal temperature proves otherwise — managed by cold-water immersion to below 39 degrees Celsius before transport — while a collapsed athlete without a pulse has sudden cardiac arrest demanding immediate CPR and defibrillation, and both emergencies are prevented by heat acclimatization, wet-bulb globe temperature activity modification, hydration discipline, and a rehearsed emergency action plan.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A sixteen-year-old cross-country runner collapses at the eight-kilometre mark of a hot August race, confused and combative, with hot dry skin and a rectal temperature of 41.2 degrees Celsius — exertional heat stroke, and the survival hinges on cold-water immersion begun within minutes. A fourteen-year-old football lineman slumps to the ground at the end of a full-contact two-a-day practice in heavy equipment, drowsy and vomiting, with a rectal temperature of 40.5 degrees Celsius — exertional heat stroke in the unacclimatised, heavily equipped athlete, the highest-risk combination the field knows. A seventeen-year-old collapses at the finish of a five-kilometre run, pale, dizzy, and sweaty but fully alert, with a normal core temperature — exercise-associated collapse from venous pooling, managed supine with the legs raised. And a fifteen-year-old basketball player slumps to the floor mid-drill without a pulse — sudden cardiac arrest, and the seconds to the defibrillator decide the outcome. [1] [12]
Cool first, transport second — the heat-stroke rule that saves lives
Overview & Definition
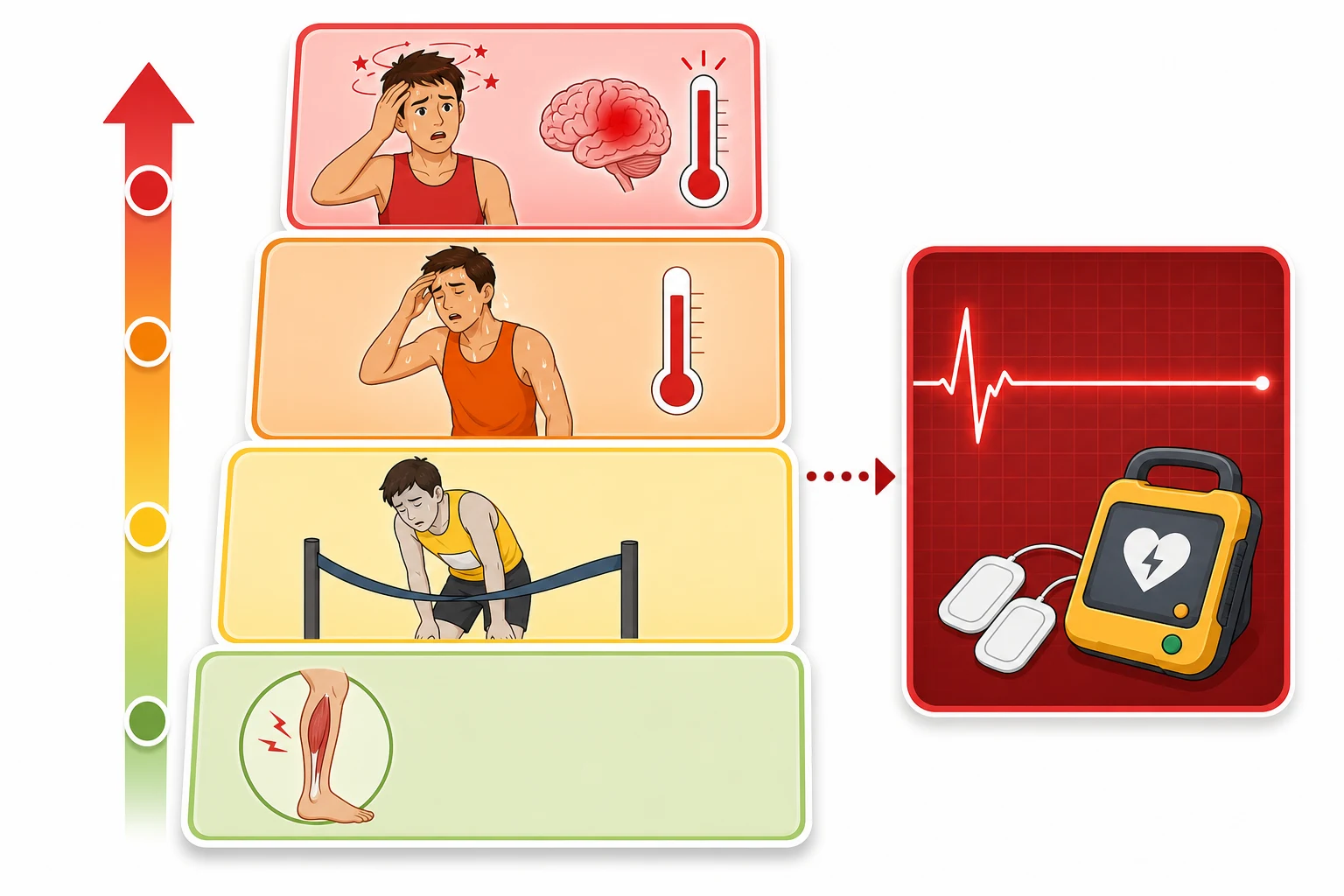
Exertional heat illness is the spectrum of illness that arises when the body's heat production during exercise outstrips its capacity to dissipate heat, and the young athlete is uniquely vulnerable because the paediatric thermoregulatory system generates more metabolic heat per kilogram and dissipates it less efficiently than the adult system. The National Athletic Trainers' Association position statement frames the spectrum as a continuum from exercise-associated muscle cramps and heat syncope through exertional heat exhaustion to exertional heat stroke, the life-threatening end. The fellowship candidate holds the spectrum in mind as a severity ladder, and the task at every collapse is to decide whether the athlete is at the benign end or the lethal end before the wrong treatment is given. [1]
The central concept is exertional heat stroke, defined as a core (rectal) temperature of 40 degrees Celsius (104 degrees Fahrenheit) or higher accompanied by central nervous system dysfunction. The central nervous system signs are the discriminator — confusion, aggression, irritability, ataxia, syncope, or loss of consciousness — and they distinguish heat stroke from heat exhaustion, which shares the high core temperature and the fatigue but preserves a normal mental state. The rectal temperature is the measurement that defines the diagnosis, and the field-side reliance on skin, tympanic, oral, or temporal readings is a documented cause of the missed diagnosis. The fellowship answer names the temperature threshold, the central nervous system criterion, and the rectal-temperature requirement aloud, because the examiner is testing whether the candidate would reach for the right measurement and the right treatment. [1] [2]
Exertional collapse is the parallel concept, and the term exercise-associated collapse describes the benign collapse that occurs when a runner stops and the calf-muscle pump ceases, allowing venous pooling and a transient drop in cerebral perfusion. The collapsed runner is pale, dizzy, and sweaty, the pulse is weak, and the mental state is preserved once supine; the management is rest with the legs elevated and oral rehydration. The collapse becomes dangerous when it is accompanied by central nervous system dysfunction, a very high or very low core temperature, or ongoing deterioration after the activity stops, because these features point to exertional heat stroke, exercise-associated hyponatraemia, or sudden cardiac arrest. The collapse pathway and the heat-stroke pathway meet at the point of collapse, and the skill is to separate them at the first assessment. [5]
Sudden cardiac arrest is the third collapse, and it is the leading medical cause of sudden death in young athletes. The athlete who collapses without a pulse, without breathing, or with seizure-like activity during or immediately after exertion has sudden cardiac arrest until a pulse is confirmed, and the treatment is immediate cardiopulmonary resuscitation and defibrillation. The prevention of sudden cardiac arrest rests on preparticipation screening, the recognition of warning symptoms, and the rehearsed emergency action plan that puts a defibrillator at the athlete's side within minutes. The fellowship answer treats exertional heat stroke and sudden cardiac arrest as the two survival-determining collapses and names the emergency action plan as the single intervention that links both. [9] [11]
Classification
The classification of exertional heat illness is built on the severity of the heat load and the presence or absence of central nervous system dysfunction, and the National Athletic Trainers' Association position statement arranges the spectrum from the benign to the life-threatening. Exercise-associated muscle cramps are the painful, involuntary contractions of the exercising muscle that arise during or shortly after intense exercise in the heat, and they are managed by rest, stretching, and sodium and fluid replacement. Heat syncope is the brief fainting that occurs with prolonged standing or a sudden stop in the heat, and it reflects the venous pooling and the orthostatic drop that the exercise-associated collapse pathway explains. [1]
Exertional heat exhaustion is the inability to continue exercise in the heat because of cardiovascular insufficiency, and the athlete is tired, sweaty, and often mildly hyponatraemic or dehydrated, with a core temperature that may be raised but stays below the 40-degree threshold, and the mental state is preserved. The management is removal from the heat, rest in a cool environment, and oral or intravenous rehydration, and the athlete recovers within hours. The crucial distinction is the mental state and the core temperature, because the exhausted athlete who becomes confused or whose temperature climbs to 40 degrees has crossed into exertional heat stroke, and the management changes from rehydration to cold-water immersion. [1] [5]
Exertional heat stroke sits at the top of the ladder, and it carries the mortality that the lower rungs do not. The diagnosis needs the two features together — a core (rectal) temperature of 40 degrees Celsius or higher and central nervous system dysfunction — and the skin may be hot and dry or sweaty, because the old teaching that heat stroke is always dry is a myth that has cost lives. The classification is completed by the recognition that the central nervous system sign may be subtle at first — irritability, poor coordination, or an unusual tactical decision — and the experienced sideline clinician acts on the early sign, because the athlete who is allowed to continue exercising deteriorates rapidly. [1] [2]
Epidemiology & Risk Factors
Exertional heat illness is among the leading causes of preventable death in young athletes, and the epidemiology clusters the risk into a small number of identifiable factors that the prevention strategy targets. American high-school data show that exertional heat illness is commonest in the first weeks of the pre-season, in the heavily equipped sports of American football, and on the hot humid days that drive the wet-bulb globe temperature upward, and the deaths occur in the unacclimatised athlete pushed through a high-intensity session in heavy equipment. The fellowship candidate holds these clusters in mind, because the prevention is the targeted removal of the risk factor rather than a blanket restriction of all sport. [1] [8]
The intrinsic risk factors are the states that reduce the body's heat tolerance or its capacity to dissipate heat. The unacclimatised athlete, the athlete returning from illness with a residual fever or dehydration, the athlete with a low cardiovascular fitness, and the athlete with a history of a prior heat illness all carry a higher risk. Sickle cell trait raises the risk of exertional collapse and rhabdomyolysis in the heat, and certain medications and supplements — stimulants, antihistamines, and the attention-deficit medicines — impair thermoregulation. The obese athlete and the athlete in heavy protective equipment dissipate heat less efficiently, and the young child has a higher metabolic heat production per kilogram and a lower sweating capacity than the adult. [1] [7]
The extrinsic risk factors are the environmental and the organisational conditions. A high wet-bulb globe temperature, which combines the heat, the humidity, the radiant heat, and the wind, is the single most important environmental driver, because humidity limits the evaporation of sweat and the evaporation of sweat is the dominant route of heat loss in the exercising human. The lack of a heat-acclimatization protocol, the absence of wet-bulb globe temperature monitoring, the scheduling of intense sessions in the hottest part of the day, the restriction of fluids, and the absence of an on-site cooling tub and a rehearsed emergency action plan are the organisational failures that turn a preventable heat illness into a death. The fellowship answer names the environmental and the organisational risk factors together, because the policy intervention addresses them both. [6] [8]
Pathophysiology
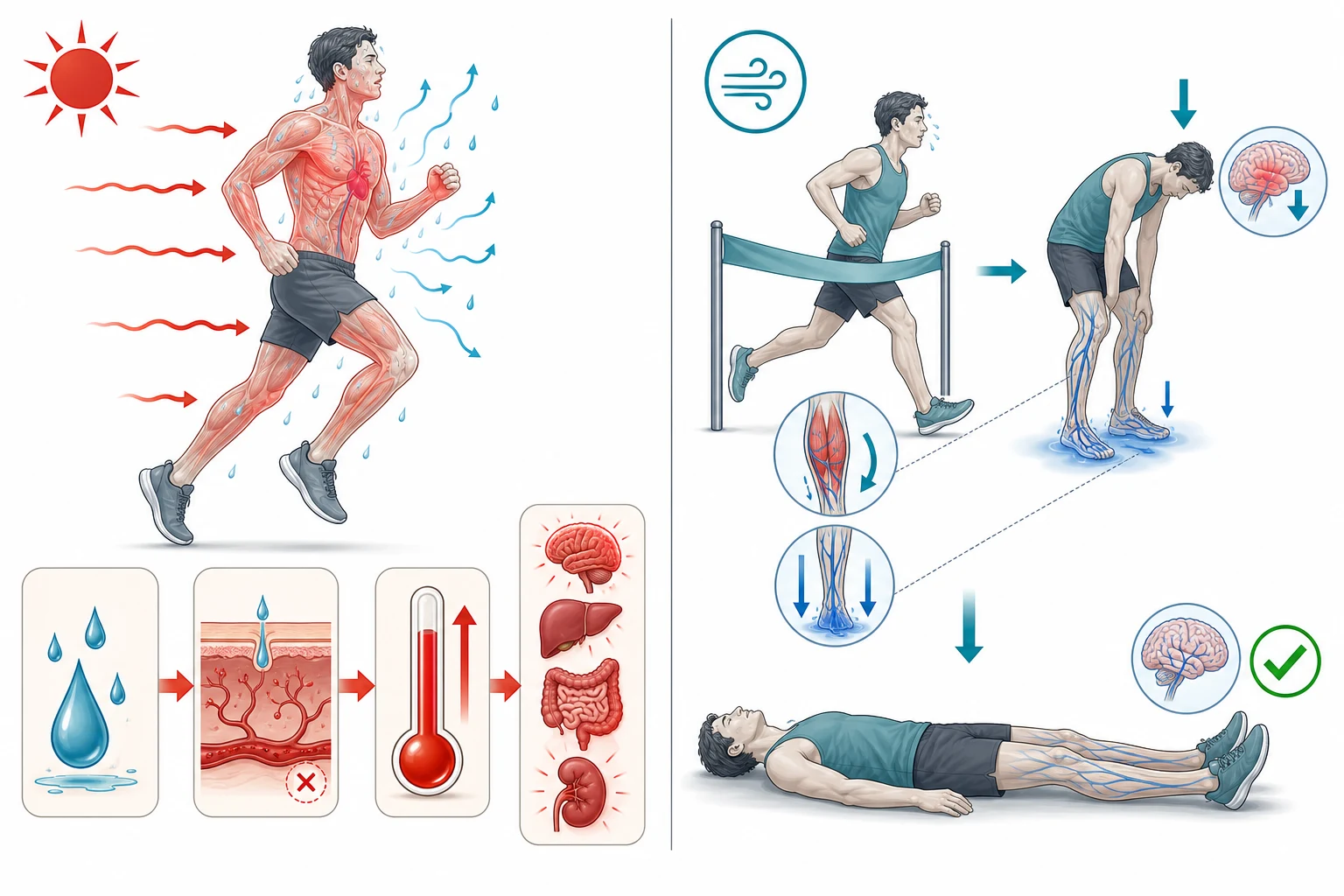
The pathophysiology of exertional heat illness is the imbalance between heat production and heat dissipation, and the exercising human is the mammal that generates the most heat per unit of time. During intense exercise, the metabolic heat production can raise the core temperature by roughly one degree Celsius every five minutes if the dissipation fails, and the dissipation rests on the cutaneous blood flow and the evaporation of sweat. The thermoregulatory centre in the hypothalamus drives the skin blood flow upward and the sweat rate upward as the core temperature rises, and the cardiovascular system supports both by raising the cardiac output and shunting blood to the skin. When the heat load exceeds the dissipation capacity, the core temperature climbs, and the cellular damage begins. [1] [2]
At the cellular level, the high core temperature damages the membranes, the enzymes, and the cytoskeleton of the gut, the liver, the kidney, and the brain, and the damage is both direct and ischaemic. The splanchnic vasoconstriction that diverts blood to the exercising muscle and the skin compromises the gut barrier, and the endotoxaemia and the systemic inflammatory response that follow drive a cascade that resembles septic shock. The coagulation system activates, the platelets and the clotting factors are consumed, and the disseminated intravascular coagulation, the acute kidney injury from the rhabdomyolysis, and the hepatic failure compound the encephalopathy. The central nervous system dysfunction reflects the direct thermal injury of the cerebellum and the cortex, and it is the organ system whose failure defines the clinical picture. [1] [9]
The pathophysiology of exercise-associated collapse is different and benign. When the runner stops, the sudden cessation of the calf-muscle pump and the persistent peripheral vasodilation allow the blood to pool in the legs, the venous return and the cardiac output drop, and the cerebral perfusion falls transiently. The athlete faints, but once horizontal the venous return is restored and the mental state clears within seconds to minutes. The collapse is a haemodynamic event, not a thermal one, and the rectal temperature is normal or only mildly raised. The pathophysiology explains the treatment — the supine position with the legs elevated restores the venous return — and it explains why the collapse is self-limiting unless an additional pathology, such as heat stroke or hyponatraemia, is present. [5]
Clinical Presentation
The presentation of exertional heat stroke is the athlete who collapses or falters during exercise in the heat with a change in the mental state, and the change may be subtle before it is dramatic. The early signs are the irritability, the poor coordination, the unusual tactical decision, and the stumbling that the attentive coach or athletic trainer notices as uncharacteristic for the athlete. The progression is rapid — confusion, aggression, ataxia, vomiting, and the loss of consciousness — and the skin is hot, though it may be dry or wet with sweat. The fellowship skill is to act on the early sign, because the athlete who is told to run it off deteriorates, and the early cold-water immersion is the difference between a full recovery and a death. [1] [2]
The presentation of exertional heat exhaustion is the athlete who is struggling to keep up, sweating profusely, pale, dizzy, and headachy, but with a preserved mental state and a core temperature below the 40-degree threshold. The athlete may have cramps, nausea, and a tachycardia, and the symptoms ease with rest in a cool environment and rehydration. The danger is the athlete who is pushed back into the session, because the borderline exhaustion can tip into heat stroke as the heat load continues. The decision to remove the athlete from the heat and to assess the rectal temperature is the safeguard, and the athlete whose mental state or temperature crosses the line is managed as heat stroke. [1] [5]
The presentation of exercise-associated collapse is the runner who slumps at or just after the finish line, pale, sweaty, and pulse-weak, with a preserved mental state that clears once the athlete is horizontal. The rectal temperature is normal or only mildly raised, the pulse recovers, and the athlete feels better within minutes of rest with the legs elevated. The features that redirect the assessment away from the benign collapse are the persistent altered mental state, the very high or very low core temperature, the ongoing deterioration after the activity stops, the seizures, and the vomiting — because these point to exertional heat stroke, exercise-associated hyponatraemia, or sudden cardiac arrest. The collapse is managed by the protocol, and the red flags are sought at the same assessment. [5]
The presentation of sudden cardiac arrest is the athlete who collapses during or immediately after exertion without a pulse, without breathing, or with brief seizure-like activity from cerebral hypoperfusion, and it is the collapse that is missed when the seizure-like activity is mistaken for a convulsion. The athlete may have had warning symptoms in the weeks before — exertional chest pain, exertional syncope, palpitations, or a family history of sudden death — and the preparticipation screen is the safeguard that catches the structural and the electrical cardiac disease. The collapsed athlete without a pulse is managed by the cardiac arrest protocol, and the defibrillator is the treatment that determines the survival. [9] [12]
Differential Diagnosis
The differential diagnosis of the exertional collapse is the short list that the field-side assessment separates, and the skill is to run the list in the order of the life threat. The first fork is the pulse — the athlete without a pulse has sudden cardiac arrest and the start of cardiopulmonary resuscitation. The athlete with a pulse and an altered mental state has exertional heat stroke until the rectal temperature proves otherwise, and the high temperature with the central nervous system sign confirms it. The athlete with a pulse, a preserved mental state, and a normal temperature has exercise-associated collapse, and the management is conservative. [1] [5]
Exercise-associated hyponatraemia is the mimic that demands the same vigilance as heat stroke. The endurance athlete who drinks far more water than the sweat loss loses develops a dilutional hyponatraemia, and the presentation is a collapse with confusion, nausea, vomiting, and seizures, sometimes with a normal or low core temperature. The clue is the weight gain from the overhydration and the onset hours into a long event, and the management is fluid restriction and the hypertonic saline in the severe case, never the free-water rehydration that worsens the hyponatraemia. The fellowship answer names the hyponatraemia as the collapse that cooling does not fix and overhydration causes. [5]
Exertional rhabdomyolysis is the muscle breakdown that accompanies intense exercise in the heat, and it presents with severe muscle pain, weakness, and the dark cola-coloured urine of the myoglobinuria, sometimes hours after the event. The sickle-cell crisis in the athlete with sickle cell trait presents with the acute pain and the rhabdomyolysis in the heat, and it is a differential that the screening history raises. The hypoglycaemia, the asthma, the anaphylaxis, and the exertional syncope of the structural cardiac disease round out the differential, and the field-side assessment seeks the cause that the rectal temperature and the pulse do not explain. The fellowship skill is to hold the collapse as a diagnosis to be separated, not a single entity to be named. [9]
Clinical & Bedside Assessment
The bedside assessment of the exertional collapse is the field-side protocol, and it begins the moment the athlete hits the ground. The first move is the safety and the responsiveness check, and the second is the pulse and the breathing check, because the athlete without a pulse has sudden cardiac arrest and the immediate start of the cardiopulmonary resuscitation. The airway is opened, the breathing is assessed, and the defibrillator is called for as soon as the arrest is recognised, because the minutes to the shock determine the survival. The athlete with a pulse moves to the heat-illness assessment, and the time from the collapse to the rectal temperature is measured in seconds, not minutes. [1] [10]
The history is gathered from the coach, the teammates, and the observers as the cooling begins. The sport, the environmental conditions, the duration and the intensity of the exercise, the equipment worn, and the acclimatization status frame the risk. The recent illness, the fever, the medication and the supplement use, the hydration, and the prior history of heat illness are sought, because each raises the probability of the heat stroke. The warning symptoms in the days before — the chest pain, the syncope, and the palpitations — are sought when the cardiac arrest is the presentation, because they point to the underlying structural or the electrical disease. [1] [6]
The examination is focused on the mental state, the rectal temperature, the pulse, the hydration, and the skin. The mental state is assessed for the confusion, the aggression, the ataxia, and the level of consciousness, because the central nervous system sign is the discriminator. The rectal temperature is taken with a rectal thermistor, because the tympanic, the oral, the temporal, and the skin measurements are unreliable in the exercising athlete and their use is a documented cause of the missed diagnosis. The pulse, the blood pressure, the respiratory rate, and the skin temperature and the moisture complete the assessment, and the athlete who meets the heat-stroke criteria moves directly to the cold-water immersion. [1] [2]
Which findings must never be dismissed? The athlete who collapses and has a rectal temperature of 40 degrees Celsius or higher with a central nervous system sign has exertional heat stroke, and the immersion begins at once. The athlete who collapses without a pulse has sudden cardiac arrest, and the resuscitation begins at once. And the athlete who deteriorates after the collapse, who fails to clear once supine, or who seizes has a serious diagnosis and not a simple collapse. The field-side protocol is the safeguard, and the rectal temperature and the pulse check are the two moves that the protocol never skips. [1] [5]
Investigations
The investigation of the exertional heat illness is the rectal temperature, taken at the field side, because the rectal thermistor is the only valid measure of the core temperature in the exercising athlete. The tympanic, the oral, the temporal, and the skin measurements underestimate the core temperature and their use to exclude the heat stroke is the error that has cost lives, and the fellowship answer states the rectal-temperature requirement aloud. The ingestible thermistor pill is an alternative in the research and the elite setting, and the oesophageal probe is used in the hospital, but the rectal measurement is the field standard. [1] [3]
The blood tests are taken in the hospital after the cooling has begun, because the cooling is never delayed for the bloods. The full blood count, the electrolytes including the sodium, the urea and the creatinine, the creatine kinase, the liver function tests, and the coagulation profile frame the severity and the complications. The sodium distinguishes the heat stroke from the exercise-associated hyponatraemia, the creatine kinase and the creatinine frame the rhabdomyolysis and the acute kidney injury, the liver function tests frame the hepatic injury that is a hallmark of the heat stroke, and the coagulation profile frames the disseminated intravascular coagulation. The blood gas shows the metabolic acidosis and the lactate, and the troponin is taken when the cardiac involvement is suspected. [1] [9]
The electrocardiogram and the cardiac assessment are taken when the collapse is a cardiac arrest or when the warning symptoms point to the structural or the electrical disease. The electrocardiogram seeks the ischaemia, the channelopathy, and the cardiomyopathy pattern, and the echocardiogram seeks the hypertrophic cardiomyopathy, the arrhythmogenic right-ventricular cardiomyopathy, and the anomalous coronary artery. The preparticipation screening with the history, the examination, and the selected electrocardiogram is the safeguard that catches the cardiac disease before the arrest, and the emergency action plan is the safeguard that puts the defibrillator at the side of the athlete when the arrest occurs. [9] [11]
Management — Resuscitation
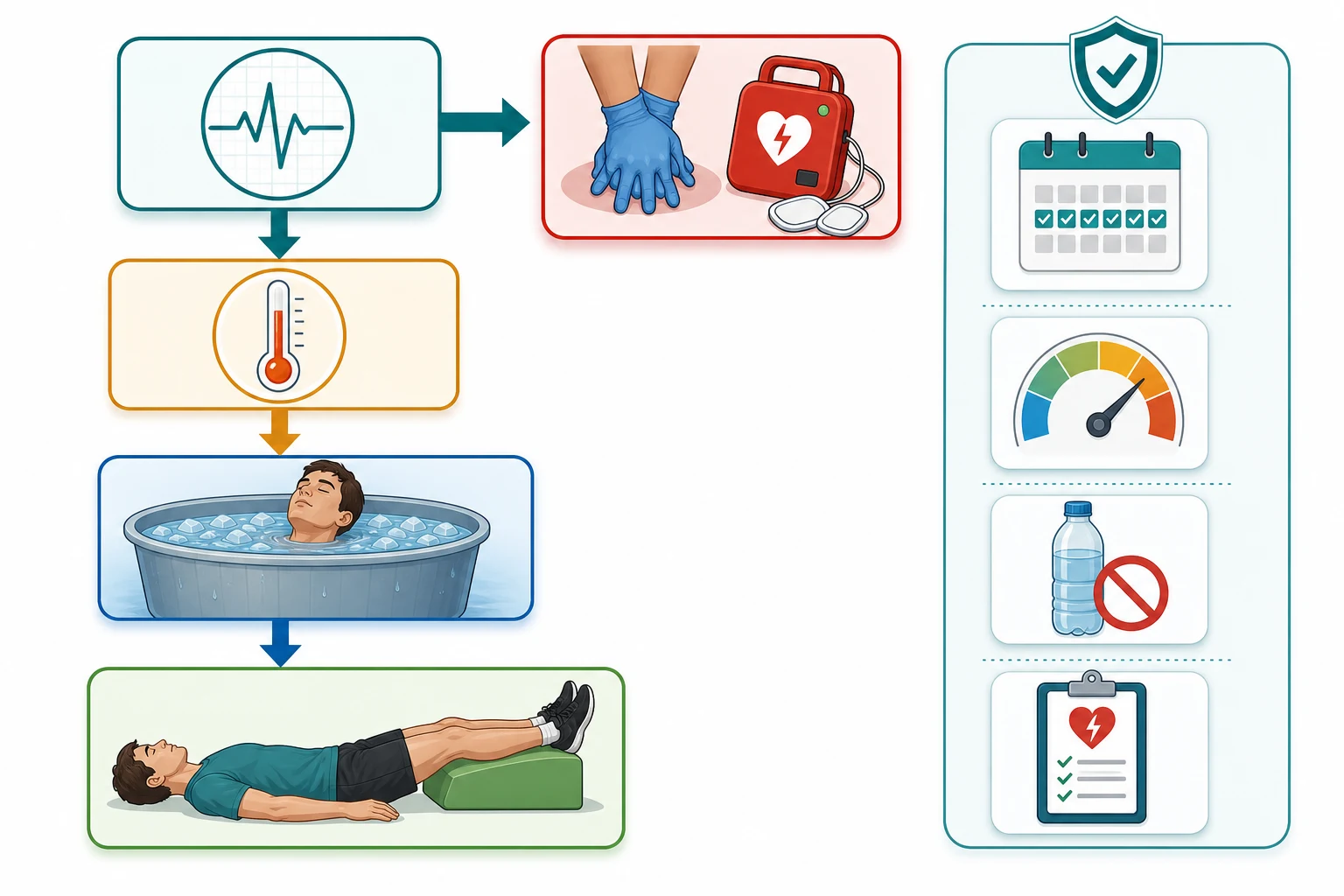
The resuscitation of the collapsed athlete begins with the pulse check, because the athlete without a pulse has sudden cardiac arrest and the immediate start of the cardiopulmonary resuscitation. The high-quality chest compressions begin at once, the defibrillator is called for, and the shock is delivered as soon as the device is ready, because the survival from the cardiac arrest falls by roughly ten per cent for every minute without the defibrillation and the early shock is the single most powerful intervention. The airway is managed, the oxygen is given, and the emergency services are called, and the rehearsed emergency action plan directs the team to the defibrillator and the evacuation. [10] [12]
The resuscitation of the exertional heat stroke is the rapid cooling, and the treatment of choice is the cold-water immersion. The athlete is immersed to the neck in a tub of cold water at 2 to 15 degrees Celsius, the water is stirred continuously to maintain the gradient, and the rectal temperature is monitored throughout. The cooling rate of the cold-water immersion is approximately 0.15 to 0.35 degrees Celsius per minute, the fastest of any field method, and the goal is a rectal temperature below 39 degrees Celsius (around 102 degrees Fahrenheit) before the transport is arranged. The mantra is cool first, transport second, because the survival approaches one hundred per cent when the cooling begins within minutes and the mortality rises sharply when it is delayed. [2] [3]
When the immersion tub is not available, the tarp-assisted cooling method is an effective alternative that uses the athlete's own tarp or a flat sheet to create a makeshift tub, filled with ice and water and stirred continuously, and the rotating ice-water towels and the evaporative cooling with the fanning and the misting are the field alternatives that achieve a slower but useful cooling rate. Dousing with cold water, removing the heavy equipment, and moving the athlete to the shade are the immediate moves while the cooling method is prepared, and the cooling is never delayed for the transport. The dantrolene is not recommended, because the evidence does not support its use in the exertional heat stroke, unlike the malignant hyperthermia. [1] [4]
The airway, the breathing, and the circulation are supported throughout the cooling, and the vomiting is anticipated and the airway protected. The intravenous fluids are given for the hypotension and the dehydration, and the electrolytes, particularly the sodium, are checked and corrected. The seizure is treated with the benzodiazepine, and the shivering is suppressed because it generates heat and slows the cooling. The athlete is transported to the hospital after the temperature is controlled, because the heat stroke causes the multi-organ injury that the hospital monitoring and the support address. [1] [9]
Management — Definitive & Stepwise
The definitive management of the exertional collapse is rest in the supine position with the legs elevated and the oral rehydration, and the athlete recovers within minutes. The oral fluids are given as the athlete tolerates them, the vital signs and the mental state are monitored, and the rectal temperature is taken to exclude the heat stroke. The athlete who fails to recover, whose mental state does not clear, or whose temperature is raised is reassessed for the heat stroke or the hyponatraemia and managed accordingly. The return to the activity is gradual, and the athlete is observed for the delayed deterioration. [5]
The definitive management of the exertional heat exhaustion is removal from the heat, rest in a cool environment, and the oral or the intravenous rehydration, and the athlete recovers within hours. The rectal temperature is taken to confirm that the heat stroke is not present, and the electrolytes are checked when the sodium disturbance is suspected. The return to the sport is guided by the recovery and the correction of the risk factors, and the athlete is educated on the hydration, the acclimatization, and the recognition of the early signs. [1]
The definitive management of the exertional heat stroke is the cold-water immersion followed by the hospital monitoring for the multi-organ injury. The athlete is admitted for the observation of the hepatic, the renal, the coagulation, and the neurological complications, and the support is given as the picture demands. The return to the sport after the heat stroke is a graded process that begins only after the full clinical and the biochemical recovery, and it follows the return-to-activity progression that the position statement frames — the rest, the gradual re-acclimatization, the monitored return to the activity, and the clearance by the medical team. [1] [2]
The four pillars of prevention and the field-side rule
Specific Subtypes & Scenarios
The heavily equipped pre-season football lineman is the scenario that defines the high-risk heat-stroke presentation. The athlete trains in the hottest weeks of the summer, in the heavy helmet and the shoulder pads that impair the heat dissipation, in the first days of the pre-season when the acclimatization is incomplete. The collapse with the confusion and the rectal temperature above 40 degrees Celsius is the presentation, and the management is the immediate cold-water immersion. The prevention is the fourteen-day acclimatization protocol, the restriction of the equipment in the early days, the modification of the session by the wet-bulb globe temperature, and the unrestricted access to the fluids. [6] [8]
The distance runner who collapses at the finish is the scenario that defines the exercise-associated collapse and the exercise-associated hyponatraemia. The runner who slumps, pale and sweaty but alert, with a normal temperature has the exercise-associated collapse, managed supine with the legs raised. The runner who is confused, seizing, or vomiting, with a normal or low temperature and a weight gain from the overhydration, has the exercise-associated hyponatraemia, managed with the fluid restriction and the hypertonic saline. The runner who collapses with the high temperature and the altered mental state has the exertional heat stroke, managed with the cold-water immersion. The marathon medical tent separates the three at the finish line. [5] [3]
The young athlete who collapses without a pulse is the scenario that defines the sudden cardiac arrest. The athlete may have had the warning symptoms — the exertional chest pain, the exertional syncope, the palpitations, or the family history of the sudden death — and the underlying disease is often the hypertrophic cardiomyopathy, the arrhythmogenic right-ventricular cardiomyopathy, the anomalous coronary artery, or the channelopathy. The management is the immediate cardiopulmonary resuscitation and the early defibrillation, and the prevention is the preparticipation screening and the rehearsed emergency action plan that puts the defibrillator at the side of the athlete within minutes. [9] [12]
The younger child in the school sports day is the scenario that demands the paediatric vigilance, because the child has the higher metabolic heat production per kilogram and the lower sweating capacity than the adult, and the child may not recognise or report the early signs. The acclimatization, the hydration, the session modification in the heat, and the attentive supervision are the prevention, and the rectal temperature and the cold-water immersion are the management of the heat stroke. The child with the special needs and the limited communication is the scenario that lowers the threshold for the active assessment, because the early sign is the change from the baseline rather than the verbal report. [1] [7]
Complications & Pitfalls
The complications of the exertional heat stroke span the organ systems and they are the source of the mortality. The hepatic injury presents with the raised transaminases and the jaundice, the acute kidney injury arises from the rhabdomyolysis and the direct thermal injury, and the coagulopathy ranges from the thrombocytopenia to the disseminated intravascular coagulation. The neurological injury ranges from the transient encephalopathy to the persistent cerebellar and the cognitive deficits, and the multi-organ failure is the terminal pathway. The complication rate and the mortality rise steeply with the delay in the cooling, and the rapid cold-water immersion is the intervention that prevents the complications. [1] [9]
The pitfall of the missed diagnosis is the deadliest error. The athlete who collapses and is assumed to have a simple collapse, and who is sent to the medical tent without the rectal temperature, has the heat stroke missed until the deterioration makes it obvious, and the delay narrows the survival. The reliance on the tympanic, the oral, or the skin temperature to exclude the heat stroke is the related error, and the safeguard is the rectal thermistor at every collapse. The pitfall of the athlete told to run it off is the organisational error that the acclimatization protocol and the sideline vigilance address, and the safeguard is the empowered athletic trainer and the coach who removes the struggling athlete. [1] [2]
The pitfall of the transport before the cooling is the error that the cool-first-transport-second rule addresses. The athlete who is moved to the ambulance before the temperature is controlled continues to cook, and the mortality rises with the delay. The safeguard is the field-side cold-water immersion, begun at the collapse and continued until the rectal temperature is below 39 degrees Celsius, and the transport arranged only after the temperature is controlled. The pitfall of the free-water rehydration in the hyponatraemia is the error that worsens the sodium, and the safeguard is the fluid restriction and the sodium check. [3] [5]
The pitfall of the unprepared venue is the error that the emergency action plan addresses. The venue without a cold-water immersion tub, without a defibrillator within minutes, and without a rehearsed team loses the time that the survival demands, and the safeguard is the written, rehearsed, and reviewed plan. The fellowship answer frames the emergency action plan as the single intervention that links the heat stroke and the cardiac arrest, because the prepared venue survives both and the unprepared venue loses both. [10] [11]
Prognosis & Disposition
The prognosis of the exertional heat stroke is excellent when the cold-water immersion begins within minutes, and the survival approaches one hundred per cent in the Falmouth Road Race series where the rapid cooling was the standard. The prognosis worsens with the delay in the cooling, and the multi-organ injury and the mortality rise steeply when the time from the collapse to the immersion exceeds the first half-hour. The athlete who is cooled rapidly and monitored for the complications generally recovers fully, and the persistent neurological deficit is the feared but uncommon outcome of the rapid cooling. [3] [2]
The prognosis of the exercise-associated collapse is excellent, and the athlete recovers within minutes of the supine rest and the oral rehydration. The prognosis worsens only when an additional pathology is missed, and the safeguard is the rectal temperature and the sodium check at the assessment. The prognosis of the exertional heat exhaustion is excellent, and the athlete recovers within hours of the rest and the rehydration, with the return to the sport guided by the recovery and the correction of the risk factors. [1] [5]
The prognosis of the sudden cardiac arrest is poor overall, and it depends on the minutes to the defibrillation. The survival from the exercise-related sudden cardiac arrest in the young athlete is highest when the collapse is witnessed, the cardiopulmonary resuscitation begins immediately, and the defibrillation occurs within the first minutes, and the rehearsed emergency action plan with the accessible defibrillator is the intervention that improves the survival. The fellowship answer frames the prognosis as time-dependent and the prevention as the venue and the policy. [12] [10]
The disposition is shared between the team physician or the athletic trainer at the field side, the emergency services and the emergency department for the heat stroke and the cardiac arrest, and the paediatrician or the sports-medicine physician for the return-to-play and the prevention. The field-side team owns the recognition, the rectal temperature, the cold-water immersion, and the defibrillation, the emergency department owns the hospital monitoring and the complication management, and the paediatrician owns the preparticipation screening, the heat-acclimatization policy, and the return-to-play progression. [1] [11]
Special Populations
The younger child and the child with the special needs demand the adapted assessment. The child has the higher metabolic heat production per kilogram and the lower sweating capacity than the adult, and the child may not recognise or report the early signs of the heat illness. The child with the developmental disability or the limited communication presents with the change from the baseline rather than the verbal report, and the threshold for the active assessment and the rectal temperature is lower. The session modification in the heat, the attentive supervision, and the empowered adult who removes the struggling child are the safeguards. [1] [7]
The Indigenous, the remote, and the socioeconomically disadvantaged young athletes face the additional burdens of the climate and the access. The remote and the tropical communities train in the high wet-bulb globe temperature for much of the year, and the distance to the defibrillator and the emergency care raises the stakes of the heat stroke and the cardiac arrest. The lack of the athletic trainer, the cooling tub, and the rehearsed emergency action plan at the community venue is the equity gap that the policy and the funding address, and the fellowship answer acknowledges the disparity and builds the local capacity. [8] [11]
The migrant and the refugee young athlete may carry the undiagnosed cardiac condition, the sickle cell trait, or the chronic illness that raises the risk of the exertional collapse, and the preparticipation assessment is the safeguard that catches it. The athlete with the attention-deficit disorder on the stimulant medication and the athlete on the antihistamine carry the impaired thermoregulation, and the session modification and the hydration are adjusted. The young athlete with the prior heat illness carries the higher risk of the recurrence, and the acclimatization and the monitoring are intensified. [1] [9]
Evidence, Guidelines & Regional Differences
The evidence base for the exertional heat illness rests on the National Athletic Trainers' Association position statement, which frames the spectrum, the rectal-temperature diagnosis, the cool-first-transport-second rule, and the prevention pillars. The Casa review established the cold-water immersion as the gold standard for the treatment, and the DeMartini Falmouth Road Race study demonstrated the near-complete survival when the rapid cooling was the standard, with the cooling rate of the immersion exceeding the alternative methods. The Pryor tarp-assisted cooling study extended the evidence to the field method that uses the ice and the water in the makeshift tub, and the Asplund review framed the exercise-associated collapse and its separation from the heat stroke and the hyponatraemia. [1] [3]
The evidence for the prevention rests on the heat-acclimatization and the activity-modification studies. The Casa inter-association task force established the fourteen-day preseason heat-acclimatization guidelines for the secondary-school athletics, and the Adams roundtable updated the consensus on the heat safety and the acclimatization in the school athlete. The Cooper Georgia heat-policy study demonstrated the data-driven revision of the practice policy by the wet-bulb globe temperature and its effect on the exertional heat illness, and it frames the wet-bulb globe temperature as the environmental tool that drives the activity modification. [6] [8]
The evidence for the sudden cardiac arrest rests on the Casa preventing-sudden-death position statement, the Drezner inter-association task force on the emergency preparedness, and the Pelto emergency-action-plan design paper, which frame the rehearsed plan and the accessible defibrillator as the survival intervention. The Drezner survival study reported the outcomes of the exercise-related sudden cardiac arrest in the young athlete and framed the gap between the current and the achievable survival, and it anchors the drive for the better screening and the faster defibrillation. [9] [12]
The regional differences are real and they shape the prevention. The Australian and the New Zealand summer sports — the cricket, the Australian-rules football, the athletics, and the distance running — train in the high wet-bulb globe temperature, and the regional policies vary in the threshold and the modification. The North American pre-season football policy is the most studied, and the wet-bulb globe temperature thresholds and the acclimatization protocols are the most codified. The fellowship answer names the local policy and the regional climate, because the prevention is the adaptation of the universal principles to the local conditions, and the rehearsed emergency action plan is the constant across the regions. [8] [11]
Exam Pearls
The fellowship answer turns on five facts. The athlete who collapses during exercise with the altered mental state and the rectal temperature of 40 degrees Celsius or higher has the exertional heat stroke, and the treatment is the cold-water immersion to below 39 degrees Celsius before the transport. The rectal temperature is the only valid field measure, and the tympanic, the oral, and the skin measurements do not exclude the diagnosis. The collapse with the preserved mental state and the normal temperature is the exercise-associated collapse, managed supine with the legs raised. The collapse without a pulse is the sudden cardiac arrest, managed with the immediate resuscitation and the defibrillation. And the prevention rests on the heat acclimatization, the wet-bulb globe temperature modification, the hydration without the overhydration, and the rehearsed emergency action plan. [1] [2]
The examiner probes three traps. The first is the collapse assumed to be benign and sent to the tent without the rectal temperature — the heat stroke is missed until the deterioration, and the rectal thermistor is the safeguard. The second is the transport before the cooling — the athlete continues to cook in the ambulance, and the cool-first-transport-second rule is the safeguard. The third is the free-water rehydration in the hyponatraemia — the sodium worsens, and the fluid restriction and the sodium check are the safeguard. [1] [5]
The examiner rewards the candidate who frames the collapse as a protocol to be run in the order of the life threat — the pulse check, the rectal temperature, and the matching treatment — and who names the prevention pillars and the emergency action plan. A candidate who shows the rectal-temperature requirement, the cool-first-transport-second rule, and the integration of the heat stroke and the cardiac arrest into a single prepared venue demonstrates the systems thinking that the fellowship demands. [1] [10]
References
- [1]Casa DJ, DeMartini JK, Bergeron MF, Csillan D, Eichner ER, Lopez RM, et al. National Athletic Trainers' Association Position Statement: Exertional Heat Illnesses. J Athl Train, 2015.PMID 26381473
- [2]Casa DJ, McDermott BP, Lee EC, Yeargin SW, Armstrong LE, Maresh CM. Cold water immersion: the gold standard for exertional heatstroke treatment. Exerc Sport Sci Rev, 2007.PMID 17620933
- [3]Demartini JK, Casa DJ, Stearns R, Belval L, Crago A, Davis R, et al. Effectiveness of cold water immersion in the treatment of exertional heat stroke at the Falmouth Road Race. Med Sci Sports Exerc, 2015.PMID 24983342
- [4]Pryor RR, Haboian K, Fitts T, Stooks JJ. Tarp-Assisted Cooling for Exertional Heat Stroke Treatment in Wildland Firefighting. Wilderness Environ Med, 2023.PMID 37748988
- [5]Asplund CA, O'Connor FG, Noakes TD. Exercise-associated collapse: an evidence-based review and primer for clinicians. Br J Sports Med, 2011.PMID 21948122
- [6]Casa DJ, Csillan D, Inter-Association Task Force for Preseason Secondary School Athletics Participants, Armstrong LE, Baker LB, Bergeron MF, et al. Preseason heat-acclimatization guidelines for secondary school athletics. J Athl Train, 2009.PMID 19478834
- [7]Adams WM, Hosokawa Y, Casa DJ, Periard JD, Racinais S, Wingo JE, et al. Roundtable on Preseason Heat Safety in Secondary School Athletics: Heat Acclimatization. J Athl Train, 2021.PMID 33878177
- [8]Cooper ER, Grundstein AJ, Miles JD, Ferrara MS, Curry P, Casa DJ, et al. Heat Policy Revision for Georgia High School Football Practices Based on Data-Driven Research. J Athl Train, 2020.PMID 32559286
- [9]Casa DJ, Guskiewicz KM, Anderson SA, Courson RW, Heck JF, Jimenez CC, et al. National athletic trainers' association position statement: preventing sudden death in sports. J Athl Train, 2012.PMID 22488236
- [10]Drezner JA, Courson RW, Roberts WO, Mosesso VN, Link MS, Maron BJ. Inter-association Task Force recommendations on emergency preparedness and management of sudden cardiac arrest in high school and college athletic programs: a consensus statement. J Athl Train, 2007.PMID 17597956
- [11]Pelto HF, Drezner JA. Design and Implementation of an Emergency Action Plan for Sudden Cardiac Arrest in Sport. J Cardiovasc Transl Res, 2020.PMID 32300931
- [12]Drezner JA, Peterson DF, Siebert DM, Thomas LC, Lopez-Anderson M, Suchsland MZ, et al. Survival After Exercise-Related Sudden Cardiac Arrest in Young Athletes: Can We Do Better? Sports Health, 2019.PMID 30204540