Paeds · rheumatology-musculoskeletal-and-sports
Juvenile idiopathic arthritis
Also known as Juvenile rheumatoid arthritis · JIA · Juvenile chronic arthritis · Oligoarticular JIA · Polyarticular JIA · Enthesitis-related arthritis · Chronic anterior uveitis of childhood
Fellowship guide to juvenile idiopathic arthritis, the commonest rheumatic disease of childhood. Covers the ILAR classification with its seven categories, the dominance of the oligoarticular subtype, the chronic anterior uveitis that is silent and blinding and that drives the slit-lamp screening schedule, the methotrexate at ten to fifteen milligrams per square metre per week that is the anchor disease-modifying drug, the etanercept and adalimumab biologics that transformed refractory disease, the Wallace clinically inactive disease criteria and the treat-to-target TREAT trial, and the long-term remission and uveitis outcomes that frame the prognosis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old girl limps into the clinic with a knee that has been swollen for two months, stiffer in the morning and looser by recess. A six-year-old boy is found at the slit lamp to have quiet inflammation scarring his eye, three months into an oligoarticular course that never troubled him. Both have juvenile idiopathic arthritis, and both are the everyday face of the commonest rheumatic disease of childhood. Juvenile idiopathic arthritis is the arthritis of one or more joints that lasts for at least six weeks in a child under sixteen years of age, after every other cause is excluded. It is not one disease but a family of seven, unified by the chronic inflammatory arthritis and divided by the pattern, the serology and the extra-articular features, and the candidate who holds the unity and the diversity together holds the topic. [1][2]
The disease earns its gravity from two facts that the boards reward the candidate who carries. The first is the silent eye. The chronic anterior uveitis of JIA produces no pain, no redness and no visual complaint until the band keratopathy, the synechiae and the cataract have scarred the sight, and the only defence is the slit-lamp screening of the child at risk. The second is the long course. JIA is a chronic disease that stretches across the childhood and into the adult life, and the treatment has moved from the symptom control to the treat-to-target goal of the clinically inactive disease, driven by the methotrexate and transformed by the etanercept and adalimumab biologics. The candidate who can frame the disease as the treatable chronic illness, rather than the catalogue of subtypes, demonstrates the reasoning the boards reward. [2][3]
The clinical weight of the topic is concentrated in the classification, the uveitis and the therapeutics, because these are the three corners the examiner probes. The International League of Associations for Rheumatology classification sorts the children into the seven categories that guide the prognosis and the uveitis risk. The chronic anterior uveitis, commonest in the young antinuclear-antibody-positive child with oligoarticular disease, is the complication that changes the outcome and that drives the three-monthly slit-lamp. The methotrexate and the biologics are the drugs that turned JIA from a disease of deformity into a disease of remission, and the Wallace criteria and the TREAT trial are the evidence that anchors the treat-to-target care. [1][6]
Classification
The classification of juvenile idiopathic arthritis is the International League of Associations for Rheumatology, or ILAR, classification, and it is the framework that the boards probe most directly because it sorts the children into the seven categories that carry the prognosis, the uveitis risk and the treatment. The ILAR classification was published in its second revision, the Edmonton two-thousand-one revision, by Petty and the ILAR Task Force, and it requires the arthritis of at least six weeks in a child under sixteen with the other causes excluded, before the child is sorted into one of the categories. The exclusion criteria, which include the psoriatic arthritis in a parent, the ankylosing spondylitis or the enthesitis-related arthritis, the systemic lupus erythematosus and the inflammatory bowel disease, are the rules that keep the classification honest, and the undifferentiated category catches the child who fits none or more than one. [1][2]
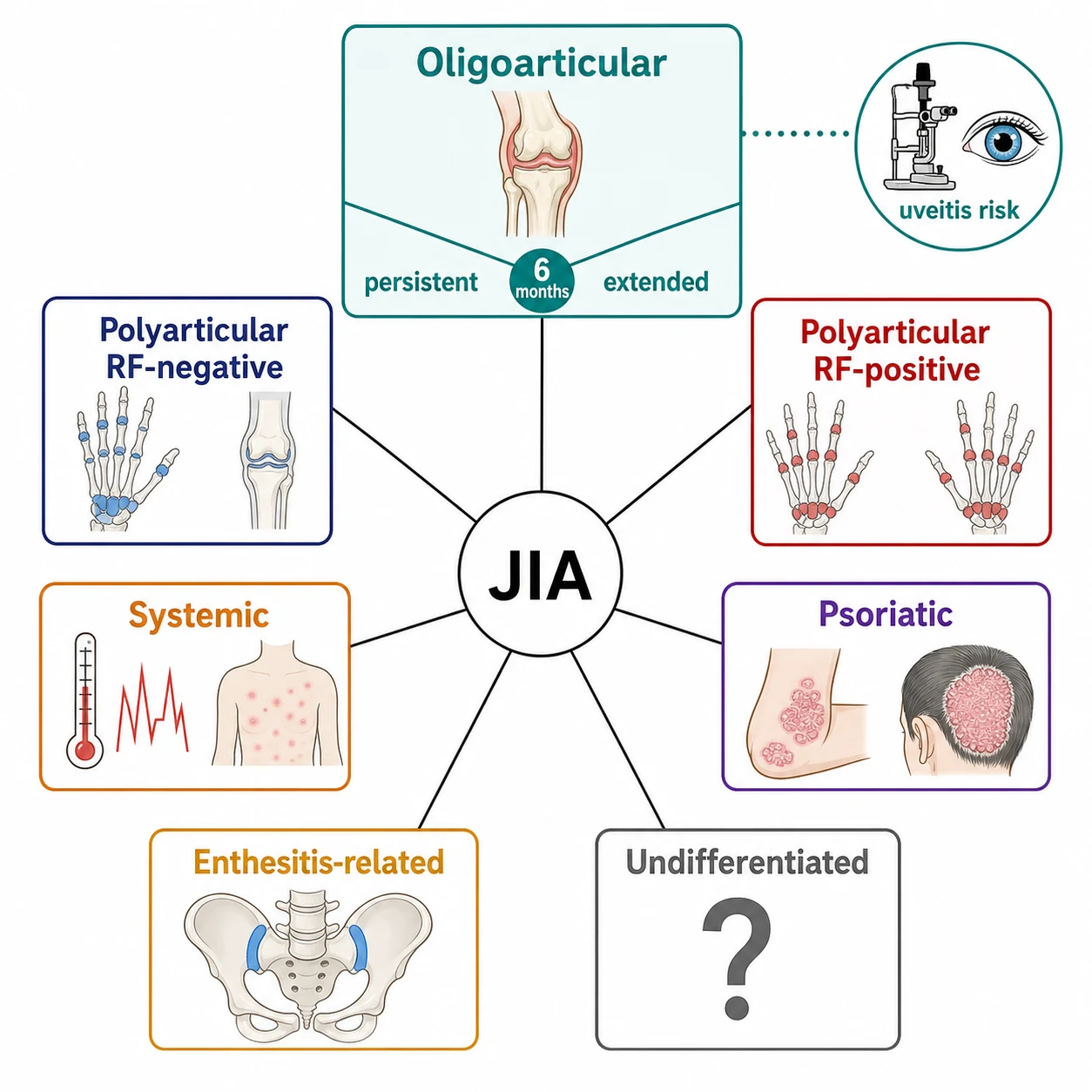
The seven categories, in the order the examiner expects, are the systemic, the oligoarticular, the polyarticular rheumatoid-factor negative, the polyarticular rheumatoid-factor positive, the psoriatic, the enthesitis-related and the undifferentiated. The oligoarticular, defined as the arthritis of one to four joints in the first six months, is the commonest category and accounts for roughly half to two-thirds of the cases, and it is the one that dominates the uveitis risk. The oligoarticular splits at the six-month mark into the persistent, where the disease stays in four joints or fewer, and the extended, where further joints become involved after the first six months, and this split is the prognostic fork the boards reward. The polyarticular rheumatoid-factor negative, the arthritis of five or more joints without the rheumatoid factor, is the next commonest and carries a moderate uveitis risk, while the polyarticular rheumatoid-factor positive, the childhood mirror of the adult rheumatoid disease, is the rarest and the most aggressive. [1][2]
Oligoarticular
one to four joints
- Commonest category, about half to two-thirds
- Young child, peak two to four years
- High chronic anterior uveitis risk
- Persistent versus extended split at six months
Polyarticular RF-negative
five or more joints, RF negative
- Second commonest category
- Symmetric small and large joints
- Moderate uveitis risk
- Methotrexate responsive
Polyarticular RF-positive
five or more joints, RF positive
- Rarest category, under five percent
- Adolescent girl, adult-like rheumatoid disease
- Aggressive erosive course
- Low uveitis risk, high joint damage risk
Enthesitis-related
enthesitis plus arthritis
- Older boy, over six years
- Sacroiliitis, HLA-B27 positive
- Acute symptomatic uveitis, not chronic
- Ankylosing spondylitis precursor
The systemic category, the systemic juvenile idiopathic arthritis, is set apart by the quotidian fever, the salmon-pink rash and the extra-articular dominance, and it is the one that carries the macrophage activation syndrome. The psoriatic category requires the arthritis and the psoriasis, or two of the dactylitis, the nail pitting and the family history. The enthesitis-related category, the arthritis with the enthesitis or the sacroiliitis in the older child, often the human-leukocyte-antigen B27 positive boy, is the precursor of the ankylosing spondylitis, and it differs from the other categories in the acute symptomatic uveitis rather than the chronic silent uveitis. The undifferentiated category catches the child who fulfils none of the categories, or two or more of them, and it is the honest acknowledgement that the classification, however useful, does not capture every child. The systemic JIA is detailed in its own topic, because its biology, its macrophage activation syndrome and its interleukin-blocking biologics stand apart from the rest. [1][3]
Epidemiology & Risk Factors
Juvenile idiopathic arthritis is the commonest rheumatic disease of childhood, with an incidence of roughly ten to twenty per hundred thousand children per year and a prevalence of about one in a thousand children. The oligoarticular subtype dominates, the polyarticular subtypes follow, and the systemic and the rheumatoid-factor-positive categories are the rarest. The disease is slightly more common in girls than in boys, though the enthesitis-related category flips this and favours the boy. The age at onset is bimodal in some populations, with an early peak between one and three years that captures the oligoarticular disease and a later peak around the adolescence that captures the enthesitis-related and the polyarticular rheumatoid-factor-positive disease. The access to the paediatric rheumatology and the time to the diagnosis vary by the geography and the socioeconomic status, and the delay in the diagnosis is the equity issue that the candidate who names the social determinants demonstrates the breadth the boards reward. [2][12]
The genetic and the environmental risk factors are present but modest, and they matter because they shape the subtype. The human-leukocyte-antigen class one and two alleles confer the subtype susceptibility, with the human-leukocyte-antigen B27 linked to the enthesitis-related arthritis, the human-leukocyte-antigen A2 to the oligoarticular, and the shared epitope to the rheumatoid-factor-positive disease. The antinuclear antibody is the serological marker that flags the uveitis risk, present in roughly seventy percent of the oligoarticular and the polyarticular rheumatoid-factor-negative children, and its presence, with the young age and the subtype, is the combination that drives the slit-lamp screening. The environmental triggers, the infections and the microbiome, are suspected but unproven, and the candidate may name them as the active area of the research without overclaiming. [3][9]
The single most important risk-stratifying fact in the topic is the uveitis risk profile, because it is the fact that turns the chronic silent eye disease into a preventable cause of the blindness. The chronic anterior uveitis affects roughly ten to twenty percent of the children with the oligoarticular and the polyarticular rheumatoid-factor-negative JIA, and it is concentrated in the child who is young, antinuclear-antibody positive, oligoarticular and within the first four years of the disease. The Nordic cohort of Nordal and colleagues, and the eighteen-year outcome of Rypdal and colleagues, have mapped the incidence and the predictors, and they are the evidence base for the screening schedule. The candidate who can name the four risk factors, the young age, the antinuclear antibody, the oligoarticular subtype and the early disease, holds the screening logic. [9][10]
Pathophysiology
The pathophysiology of juvenile idiopathic arthritis is the dysregulated adaptive and innate immune response against the synovium, and it is the failure of the self-tolerance that drives the chronic inflammation of the joint and the eye. The synovial membrane, normally a thin lubricating layer, becomes hypertrophied and infiltrated by the activated T cells, the B cells and the macrophages, and the resulting pannus invades the cartilage and the bone. The cytokines, the tumour necrosis factor alpha and the interleukins, drive the inflammation, and they are the targets of the modern biologics that transformed the treatment. The candidate who can link the synovial pannus to the joint damage and the cytokines to the biologics demonstrates the mechanistic reasoning the boards reward. [3][2]
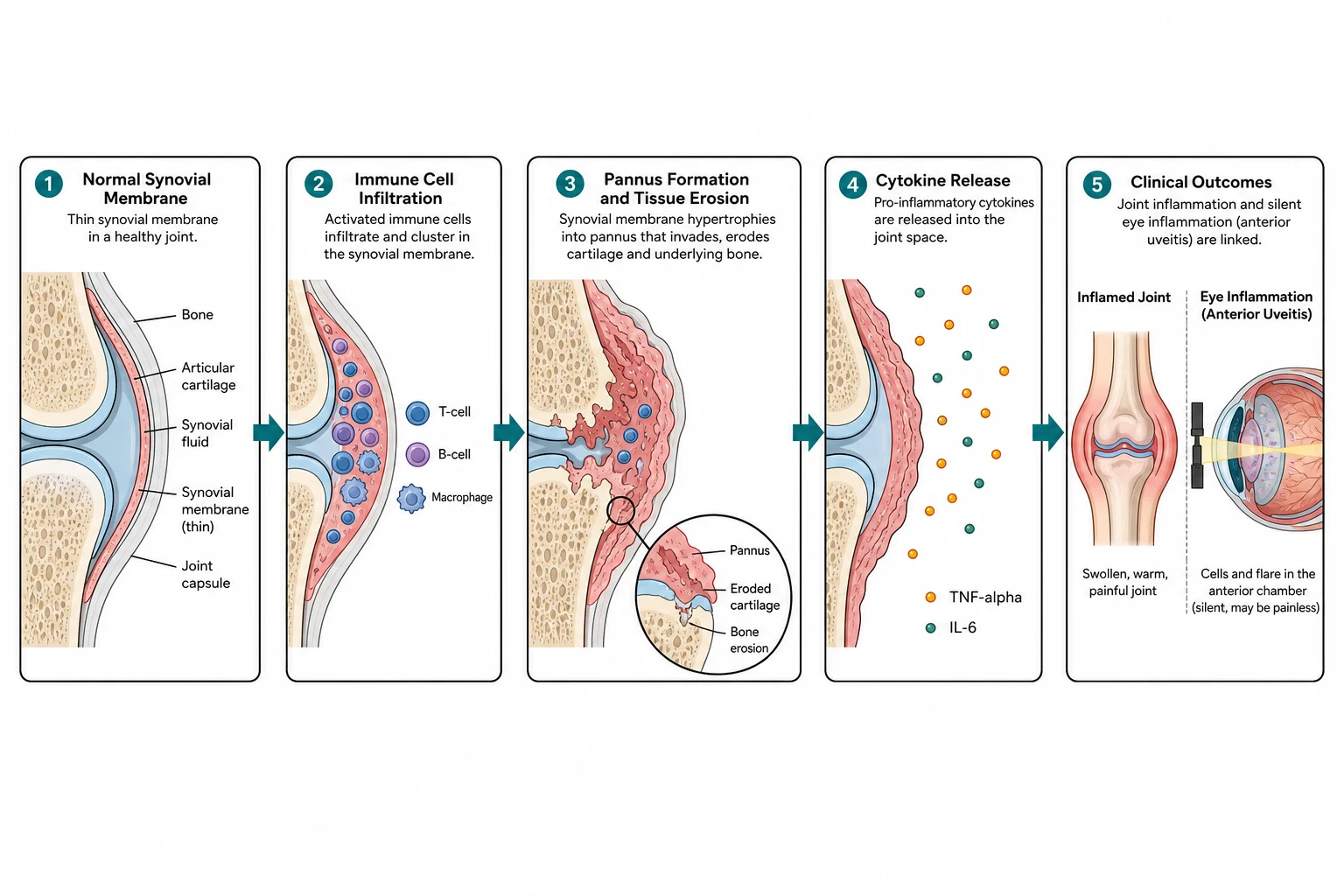
The cytokine biology is the bridge from the mechanism to the treatment, and the tumour necrosis factor alpha is the central node. The tumour necrosis factor alpha is produced by the activated macrophages and the T cells in the inflamed synovium, and it drives the recruitment of the further inflammatory cells, the osteoclast activation and the cartilage destruction. The etanercept, the soluble receptor that binds and neutralises the tumour necrosis factor alpha, was the first biologic to demonstrate the efficacy in the polyarticular JIA, in the landmark trial of Lovell and the Pediatric Rheumatology Collaborative Study Group, and it opened the biologic era. The adalimumab and the infliximab, the monoclonal antibodies against the tumour necrosis factor alpha, followed, and the systematic review of Horneff and colleagues confirmed the efficacy and the safety of the class. [5][11]
The chronic anterior uveitis is the second front of the dysregulation, and it shares the immune mechanism with the joint while it diverges in its silent course. The uveitis is the inflammation of the anterior uveal tract, the iris and the ciliary body, and it is driven by the same T-cell-mediated process that inflames the synovium. The uveitis produces no pain and no redness because the eye of the young child tolerates the low-grade inflammation without the alarm, and the only sign is the cells and the flare in the anterior chamber seen on the slit-lamp. The untreated chronic uveitis scars the eye through the band keratopathy, the posterior synechiae, the cataract and the glaucoma, and the eighteen-year Nordic outcome of Rypdal and colleagues showed that the visual outcomes have improved with the modern screening and treatment but that the burden persists. [9][10]
Clinical Presentation
The child with juvenile idiopathic arthritis presents most often through the swollen joint or the limp, and the pattern is the clue to the subtype. The oligoarticular child, the commonest, presents with a single swollen joint, most often the knee, that has been present for weeks to months, with the morning stiffness and the gelling that improve with the activity and the warmth. The child is otherwise well, afebrile, and the family doctor may have attributed the limp to the trauma or the transient synovitis, and the delay to the diagnosis is the rule rather than the exception. The examination shows the joint that is swollen, warm, slightly tender and restricted in the movement, with the muscle wasting and the flexion contracture in the chronic case, and the careful examination of all the joints finds the second affected joint that converts the diagnosis. [2][3]
The polyarticular child presents with the multiple swollen joints, often symmetric, involving the small joints of the hands and the feet alongside the large joints, and the morning stiffness is more pronounced and the function more impaired. The polyarticular rheumatoid-factor-positive adolescent girl may have the rheumatoid nodules, the vasculitis and the aggressive erosive disease that mirrors the adult rheumatoid arthritis, and she is the one who warrants the early and the aggressive treatment. The enthesitis-related older boy presents with the lower-limb arthritis and the enthesitis, the tenderness at the insertion of the tendon, and the sacroiliac pain, and he may give the family history of the ankylosing spondylitis. The psoriatic child presents with the arthritis and the dactylitis, the swollen digit that looks like a sausage, and the nail pitting. [1][2]
The extra-articular presentation is the chronic anterior uveitis, and it is the one that is silent and that demands the screening rather than the symptom. The uveitis is detected on the slit-lamp, not by the complaint, and the red flags of the established uveitis damage, the band keratopathy, the irregular pupil of the synechiae and the cataract, are the late signs that the screening is designed to prevent. The systemic JIA, with the quotidian fever and the salmon-pink rash, is the exception to the silent eye, and it is covered in its own topic. The candidate who can describe the joint pattern and then pivot to the silent eye demonstrates the breadth the boards reward. [8][10]
Methotrexate, the anchor disease-modifying drug
Dose
Ten to fifteen milligrams per square metre of body-surface area once weekly, with the typical range of ten to fifteen milligrams per square metre; the folic acid is one milligram daily or the equivalent the day after the dose
Differential Diagnosis
The differential diagnosis of the swollen joint in the child is broad, and the task is to separate the JIA from the dangerous mimics, the septic arthritis, the osteomyelitis, the malignancy and the reactive arthritis, before settling on the chronic diagnosis. The septic arthritis is the emergency that must not be missed, and the child is febrile, unwell, holding the joint rigid and refusing to bear weight, with the markedly raised inflammatory markers. The Kocher criteria, the fever, the inability to bear weight, the raised white-cell count and the raised erythrocyte sedimentation rate, are the bedside tool that probability-weights the septic arthritis, and the joint aspirate is the definitive test. The osteomyelitis may coexist or mimic, and the magnetic resonance imaging defines the extent. [2][3]
The reactive arthritis follows the infection, classically the enteric or the genitourinary, and it is the acute asymmetric oligoarthritis that resolves within weeks to months, distinguished from the JIA by the duration and the trigger. The post-streptococcal arthritis follows the streptococcal infection and is distinguished by the raised antistreptolysin titre and the shorter course. The Lyme arthritis, in the endemic regions, presents with the recurrent monoarthritis of the knee and the history of the tick exposure or the erythema migrans. The transient synovitis of the hip, the commonest cause of the limp in the young child, follows the viral infection, resolves within days to weeks and has the mild or the normal inflammatory markers. [2][12]
Juvenile idiopathic arthritis
chronic, six weeks
- More than six weeks, afebrile
- Morning stiffness, improves with activity
- Normal or mildly raised inflammatory markers
- Slit-lamp for the silent uveitis
Septic arthritis
emergency
- Fever, unwell, refusing to bear weight
- Markedly raised inflammatory markers
- Kocher criteria to probability-weight
- Joint aspirate and urgent washout
Reactive arthritis
post-infectious
- One to six weeks after infection
- Acute asymmetric oligoarthritis
- Resolves within weeks to months
- Trigger the enteric or genitourinary
The malignancy is the mimic that the examiner probes, and the leukaemia and the bone tumour must be excluded in the child with the atypical presentation. The leukaemia may present with the bone pain and the joint pain that mimics the JIA, and the pallor, the bruising, the hepatosplenomegaly and the cytopenias, with the blast cells on the blood film, are the clues. The pain that is disproportionate to the examination, the night pain, the weight loss and the constitutional symptoms are the red flags that demand the further imaging and the marrow. The connective tissue diseases, the systemic lupus erythematosus and the juvenile dermatomyositis, may present with the arthritis, and the malar rash, the Gottron papules and the multi-organ involvement distinguish them. [2][12]
Clinical & Bedside Assessment
The bedside assessment of the child with the suspected juvenile idiopathic arthritis begins with the general inspection and the growth, because the failure to thrive and the anaemia of the chronic disease are the clues to the severity. The child is examined for the fever and the rash, because the quotidian fever and the salmon-pink rash of the systemic JIA are the exception that changes the pathway. The pGALS, the paediatric Gait Arms Legs Spine screening, is the musculoskeletal screen that catches the child who needs the full examination, and the candidate who can perform it demonstrates the skill the boards reward. The vital signs, the height and the weight, and the pubertal stage complete the baseline. [2][3]
The joint examination is the centrepiece, and the look-feel-move-measure approach across all the joints is the method. The swollen joint is characterised by the warmth, the effusion, the synovial thickening, the tenderness and the restricted movement, and the comparison with the other side confirms the asymmetry. The child is examined for the flexion contractures, the muscle wasting and the leg-length inequality, because the long-standing knee arthritis causes the overgrowth of the affected limb from the hyperaemia and the resulting discrepancy. The enthesitis is sought at the insertion of the Achilles tendon, the plantar fascia and the patellar tendon, and the sacroiliac joints are stressed. The temporomandibular joint, often missed, is examined for the limited mouth opening and the micrognathia, and the cervical spine is examined for the limited rotation and extension. [2][12]
The eye examination is the non-negotiable third leg, and the slit-lamp is the tool that detects the silent uveitis. The child is referred to the ophthalmology for the slit-lamp examination at the diagnosis, and the screening schedule is set by the risk profile. The high-risk child, the oligoarticular or the polyarticular rheumatoid-factor-negative child who is antinuclear-antibody positive and under seven at onset, within the first four years of the disease, is screened every three months. The moderate-risk child is screened every six to twelve months, and the low-risk child every six to twelve months for the longer duration. The candidate who can recite the high-risk profile and the three-monthly interval is the one who passes the uveitis question. [8][9]
Investigations
The investigation of the child with the suspected juvenile idiopathic arthritis is the workup that confirms the chronicity and excludes the mimics, because there is no single diagnostic test for the JIA. The full blood count may show the mild anaemia and the thrombocytosis of the chronic inflammation, and the leukaemia is excluded by the absence of the blasts and the cytopenias. The inflammatory markers, the C-reactive protein and the erythrocyte sedimentation rate, are normal or mildly raised in the oligoarticular disease and more raised in the polyarticular and the systemic disease, and they are the baseline for the disease activity and the response. The liver and the renal function are the baseline before the methotrexate. [2][4]
The serology is the antinuclear antibody and the rheumatoid factor, and they are the tests that subtype the disease and the uveitis risk rather than the ones that confirm it. The antinuclear antibody is positive in roughly seventy percent of the oligoarticular and the polyarticular rheumatoid-factor-negative children, and its presence, with the young age and the subtype, flags the uveitis risk that drives the three-monthly slit-lamp. The rheumatoid factor is positive in the polyarticular rheumatoid-factor-positive category, the rare and the aggressive adolescent disease, and it is otherwise negative. The human-leukocyte-antigen B27 is tested when the enthesitis-related arthritis is suspected, and it is positive in the older boy with the sacroiliitis. The candidate who understands that these tests subtype rather than diagnose is the one who avoids the trap of the negative antinuclear antibody in the oligoarticular child. [1][9]
The imaging is the ultrasound and the magnetic resonance imaging, and they are the tools that confirm the synovitis and detect the subclinical disease. The ultrasound detects the synovial hypertrophy and the effusion, and it is useful for the joint that is difficult to examine, like the hip. The magnetic resonance imaging with the contrast is the gold standard for the synovitis and the early cartilage damage, and it is the imaging for the sacroiliitis of the enthesitis-related arthritis, which may be clinically silent. The radiograph is the late test, because the erosions and the joint-space narrowing are the signs of the established damage that the modern treatment is designed to prevent. The slit-lamp remains the eye test, and it is the investigation that is done at the diagnosis and on the schedule, not on the symptom. [2][8]
The uveitis screening schedule at the diagnosis
Refer every child newly diagnosed with juvenile idiopathic arthritis for the baseline slit-lamp examination
The uveitis may precede or accompany the arthritis and is silent
Assign the risk profile from the subtype, the antinuclear antibody and the age at onset
High risk is oligoarticular or RF-negative polyarticular, ANA positive, onset under seven
Screen the high-risk child every three months for the first four years
The window of the highest uveitis incidence is the first four years
Screen the moderate-risk child every six to twelve months
Lower risk, longer interval, individualised with the ophthalmology
Continue the screening for the duration set by the risk, even in the clinically inactive joint disease
The uveitis may flare independent of the joint disease
Management — Resuscitation
The resuscitation of the child with the juvenile idiopathic arthritis is governed by the principle that the dangerous mimics and the acute complications are addressed before the chronic disease is settled. The child with the swollen joint and the fever is the septic arthritis until proven otherwise, and the Kocher criteria, the blood cultures and the joint aspirate are obtained, with the urgent orthopaedic washout if the septic arthritis is confirmed. The child with the systemic JIA and the high fever, the rash and the hepatosplenomegaly is the macrophage activation syndrome until proven otherwise, and the ferritin, the fibrinogen and the coagulation are the tests, and the management is detailed in the systemic JIA topic. [2][3]
The child with the established JIA on the methotrexate who presents with the fever and the neutropenia is the marrow suppression, and the management is the cessation of the methotrexate, the broad-spectrum antibiotics and the supportive care. The child with the vomiting and the lethargy and the rising transaminase is the hepatotoxicity, and the methotrexate is held and the liver function monitored. The child on the biologic who develops the fever is the serious infection until proven otherwise, because the tumour necrosis factor blockade masks the signs of the infection, and the empiric broad-spectrum antibiotics are begun before the cultures return. The varicella exposure in the child on the biologic or the methotrexate warrants the urgent varicella-zoster immunoglobulin, because the live vaccine is contraindicated and the primary varicella can be severe. [4][11]
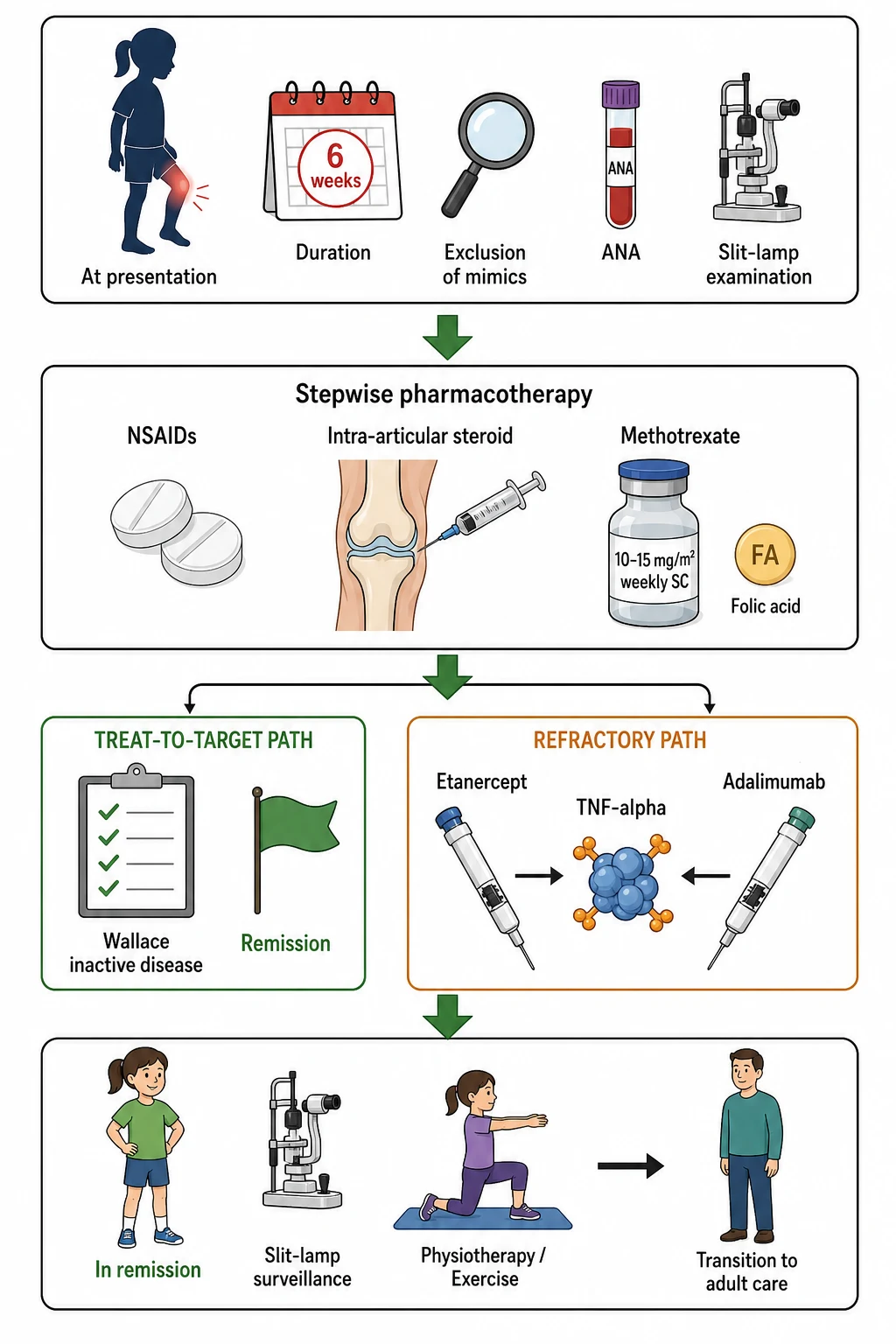
The intra-articular corticosteroid injection is the bridge that settles the inflamed joint while the disease-modifying drug takes effect, and it is the resuscitation of the single active joint. The triamcinolone hexacetonide is the preferred preparation for the longer duration, and the injection, under the sedation or the anaesthesia and often with the ultrasound guidance, settles the majority of the injected joints within weeks. The intra-articular injection is particularly useful in the oligoarticular disease, where it may be the only treatment needed, and in the child with the contracture, where the injection precedes the physiotherapy. [2][3]
Management — Definitive & Stepwise
The definitive treatment of juvenile idiopathic arthritis is stepwise and treat-to-target, and the goal is the clinically inactive disease measured by the Wallace criteria. The first step is the non-steroidal anti-inflammatory drugs and the intra-articular corticosteroid injection, and these are sufficient for many of the oligoarticular children. The second step is the methotrexate, the anchor disease-modifying drug, given at ten to fifteen milligrams per square metre once weekly, subcutaneously for the better bioavailability, with the folic acid to reduce the mucosal and the hepatic toxicity. The landmark trial of Giannini and the Pediatric Rheumatology Collaborative Study Group, in two-thousand-and-ninety-two, established the methotrexate in the resistant disease, and it has been the foundation of the treatment ever since. The methotrexate takes six to eight weeks to work, and the candidate who counsels the family on the delayed onset avoids the premature discontinuation. [4][2]
The third step is the biologic, and the tumour necrosis factor inhibitors are the first-line biologics for the disease that has not responded to the methotrexate. The etanercept, at zero point eight milligrams per kilogram once weekly to a maximum of fifty milligrams, was the first biologic to demonstrate the efficacy in the polyarticular JIA, in the landmark trial of Lovell and the Pediatric Rheumatology Collaborative Study Group in two-thousand, and it opened the biologic era. The adalimumab, at twenty-four milligrams per square metre every two weeks to a maximum of forty milligrams, given with the methotrexate, is the other first-line tumour necrosis factor inhibitor, and it has the added benefit for the uveitis. The systematic review of Horneff and colleagues confirmed the efficacy and the safety of the tumour necrosis factor inhibitor class, and the biologics have transformed the prognosis of the refractory disease. [5][11]
The treatment journey of polyarticular juvenile idiopathic arthritis
The treat-to-target framework is the modern principle that unifies the stepwise care, and it is the evidence the boards reward. The Wallace clinically inactive disease criteria, validated by Wallace and the colleagues through the OMERACT filter in two-thousand-and-six, define the inactive disease as no joints with active arthritis, no systemic features, the normal physician and parent global scores, and the normal inflammatory markers. The TREAT trial of Wallace and the colleagues, in two-thousand-and-twelve, tested the early aggressive therapy in the polyarticular JIA and showed that the early methotrexate with the etanercept could achieve the clinically inactive disease in a substantial proportion. The candidate who can name the Wallace criteria and the treat-to-target goal demonstrates the modern reasoning. [6][7]
Specific Subtypes & Scenarios
The oligoarticular juvenile idiopathic arthritis is the commonest and the most testable subtype, and it is the scenario that ties together the joint disease, the uveitis risk and the methotrexate. The oligoarticular child presents with one to four joints in the first six months, most often the knee, and the persistent-versus-extended split at the six-month mark is the prognostic fork. The persistent oligoarticular disease, where the disease stays in four joints or fewer, carries the better prognosis and may need only the intra-articular injection. The extended oligoarticular disease, where further joints become involved after six months, carries the worse prognosis and warrants the methotrexate and the closer surveillance. The uveitis risk is the highest in this subtype, and the three-monthly slit-lamp is the non-negotiable for the high-risk child. [1][9]
The polyarticular rheumatoid-factor-negative juvenile idiopathic arthritis is the second commonest subtype, and it is the scenario that demonstrates the methotrexate responsiveness and the moderate uveitis risk. The polyarticular rheumatoid-factor-negative child presents with five or more joints, often symmetric, and the methotrexate is the first disease-modifying drug, with the biologic for the refractory disease. The polyarticular rheumatoid-factor-positive adolescent girl is the rare and the aggressive subtype, and she warrants the early and the aggressive treatment with the methotrexate and the biologic, because the erosive disease mirrors the adult rheumatoid arthritis. [2][11]
The seven ILAR categories in order
The enthesitis-related juvenile idiopathic arthritis is the older-child subtype, often the human-leukocyte-antigen B27 positive boy, and it is the precursor of the ankylosing spondylitis. The enthesitis-related child presents with the lower-limb arthritis and the enthesitis, and the sacroiliitis may be silent and detected only on the magnetic resonance imaging. The uveitis of the enthesitis-related arthritis differs from the rest, because it is the acute symptomatic uveitis with the pain and the redness rather than the chronic silent uveitis, and the screening logic differs. The treatment includes the sulfasalazine and the tumour necrosis factor inhibitors, and the candidate who distinguishes the acute from the chronic uveitis demonstrates the depth the boards reward. [1][2]
The uveitis is the scenario that crosses all the subtypes, and it is the one that the examiner probes most directly. The chronic anterior uveitis is concentrated in the oligoarticular and the polyarticular rheumatoid-factor-negative child who is young and antinuclear-antibody positive, and it is detected on the slit-lamp. The management of the uveitis, guided by the SHARE initiative consensus of Constantin and the colleagues, begins with the topical corticosteroid and the mydriatic, and escalates to the methotrexate for the steroid-sparing and the anti-tumour-necrosis-factor, particularly the adalimumab, for the resistant disease. The candidate who can recite the topical corticosteroid, the methotrexate and the adalimumab holds the uveitis management. [8][10]
Complications & Pitfalls
The complications of the juvenile idiopathic arthritis divide into the joint-related, the eye-related and the treatment-related, and the candidate who holds all three together manages the child across the years. The joint-related complications are the flexion contracture, the muscle wasting, the leg-length inequality from the overgrowth of the affected limb, the growth disturbance and the temporomandibular and the cervical involvement. The eye-related complications are the band keratopathy, the posterior synechiae, the cataract, the glaucoma and the visual loss of the untreated chronic uveitis. The treatment-related complications are the methotrexate intolerance and toxicity, the biologic infections and the injection reactions, and the corticosteroid burden. [2][10]
The leg-length inequality is the classic joint complication of the unilateral knee arthritis, and it is the one the examiner probes. The inflamed knee causes the hyperaemia that stimulates the growth plate of the affected limb, and the overgrowth produces the longer leg and the resulting pelvic tilt and the compensatory scoliosis. The management is the shoe raise and the attention to the joint control, and the severe cases may need the epiphysiodesis. The temporomandibular joint involvement causes the micrognathia and the malocclusion, and the cervical involvement causes the limited rotation and the risk of the atlantoaxial instability, and both demand the surveillance. [2][12]
The classic diagnostic pitfalls are the ones the examiner probes, because they are the points where the diagnosis is missed or the harm is done. The swollen knee attributed to the trauma or the transient synovitis in the child who has had it for weeks is the error that delays the oligoarticular diagnosis. The failure to perform the slit-lamp at the diagnosis in the young antinuclear-antibody-positive child is the error that allows the uveitis to scar the eye. The swollen joint in the febrile unwell child attributed to the JIA rather than the septic arthritis is the error that delays the washout and risks the joint destruction. The methotrexate intolerance attributed to the non-compliance rather than the nausea is the error that stops the effective drug. [2][9]
Prognosis & Disposition
The prognosis of the juvenile idiopathic arthritis has improved markedly with the methotrexate and the biologics, and the modern goal is the sustained clinically inactive disease and the remission. The systematic review of Shoop-Worrall and the colleagues showed that the remission, defined by the Wallace criteria, is achieved by a substantial minority, with the variation by the subtype and the treatment. The oligoarticular disease carries the best prognosis, with many children achieving the inactive disease with the intra-articular injection alone, and the polyarticular rheumatoid-factor-positive disease carries the worst. The enthesitis-related disease may progress to the ankylosing spondylitis in the adult life. The candidate who can give the subtype-specific prognosis demonstrates the reasoning the boards reward. [12][7]
The uveitis prognosis has improved with the screening and the modern treatment, but the burden persists. The eighteen-year Nordic outcome of Rypdal and the colleagues showed that the visual acuity outcomes have improved, with the fewer children developing the visual impairment, but that the chronic uveitis continues to affect a substantial proportion, and that the risk of the complications like the cataract and the glaucoma persists. The early detection, the early methotrexate and the anti-tumour-necrosis-factor for the resistant disease are the reasons for the improvement, and the ongoing screening is the reason it is sustained. [10][8]
The disposition of the child is the specialist paediatric rheumatology centre, because the diagnosis, the classification, the treat-to-target care and the uveitis surveillance demand the multidisciplinary team. The team includes the paediatric rheumatologist, the ophthalmologist, the physiotherapist, the occupational therapist, the specialist nurse, the psychologist, the social worker and the school liaison. The child with the uveitis is managed jointly with the ophthalmology, and the child on the biologic is monitored for the infections and the response. The transition to the adult rheumatology, planned from the mid-adolescence, is the step that maintains the continuity of the care across the years. [2][12]
Special Populations
The adolescent with the juvenile idiopathic arthritis is the patient in whom the transition and the adherence are the primary concerns, because the chronic disease meets the developmental stage. The adolescence is the time of the pubertal growth, the identity formation and the risk-taking, and the chronic disease and the methotrexate challenge the adherence and the self-image. The transition to the adult rheumatology, planned and staged from the mid-adolescence, is the step that maintains the care and prevents the loss to the follow-up. The sexual health, the teratogenicity of the methotrexate and the pregnancy planning are the conversations that the candidate who addresses the adolescence demonstrates the breadth. [2][12]
The indigenous, the remote and the migrant or the refugee populations carry the additional burden of the access and the equity. The distance to the specialist paediatric rheumatology, the cultural and the language barriers, and the competing priorities of the socioeconomic disadvantage delay the diagnosis and the treatment. The telehealth and the outreach clinics, the cultural safety and the interpreter services, and the social work and the travel support are the measures that narrow the gap. The candidate who acknowledges the social determinants and names the equity measures demonstrates the breadth the boards reward. [2][12]
The child with the uveitis is the patient in whom the multidisciplinary care and the long-term surveillance are the primary concerns, because the eye disease may flare independent of the joint disease and may persist into the adult life. The child with the chronic uveitis needs the ongoing slit-lamp, the topical and the systemic treatment, and the surveillance for the cataract and the glaucoma, and the family is counselled on the chronic course. The child with the enthesitis-related arthritis and the human-leukocyte-antigen B27 needs the surveillance for the progression to the ankylosing spondylitis, and the acute symptomatic uveitis is the one that presents with the pain and the redness and that is managed as the emergency. [8][10]
Evidence, Guidelines & Regional Differences
The landmark evidence for the juvenile idiopathic arthritis is the body of the classification, the methotrexate and the biologic trials that have refined the diagnosis and the treatment. The International League of Associations for Rheumatology classification of Petty and the ILAR Task Force, published in two-thousand-and-four, established the seven categories that have been the international standard, and it has harmonised the diagnosis across the regions. The methotrexate trial of Giannini and the Pediatric Rheumatology Collaborative Study Group, published in two-thousand-and-ninety-two, established the methotrexate in the resistant disease, and it remains the foundation. The etanercept trial of Lovell, published in two-thousand, opened the biologic era, and the systematic review of Horneff confirmed the efficacy and the safety of the tumour necrosis factor inhibitor class. [1][11]
The treat-to-target evidence is the TREAT trial of Wallace and the colleagues, published in two-thousand-and-twelve, which tested the early aggressive therapy in the polyarticular JIA and shaped the modern goal of the clinically inactive disease. The Wallace clinically inactive disease criteria, validated through the OMERACT filter in two-thousand-and-six, are the measure of the inactive disease and the remission, and they are the foundation of the treat-to-target care. The SHARE initiative consensus of Constantin and the colleagues, published in two-thousand-and-eighteen, established the evidence-based recommendations for the uveitis management, and it harmonised the approach across the regions. [6][8]
The uveitis screening schedule is broadly consistent across the regions, with the three-monthly slit-lamp for the high-risk child, though the duration of the screening and the intervals for the lower-risk child vary. The biologics are available across the high-income regions, with the etanercept and the adalimumab as the first-line tumour necrosis factor inhibitors, though the access varies by the funding and the geography. The Nordic cohort studies of Nordal and Rypdal have provided the population-based evidence on the uveitis incidence, the predictors and the long-term outcomes, and they have shaped the screening and the management. The candidate who acknowledges the regional variation and the evidence base demonstrates the breadth the boards reward.
[9][10]The controversies are the ones that the candidate can discuss without pretending to resolve them. The optimal duration of the methotrexate after the inactive disease, the role of the methotrexate in the enthesitis-related arthritis, the choice between the etanercept and the adalimumab, and the role of the newer biologics like the tocilizumab and the canakinumab in the non-systemic disease are the open questions. The stratification of the uveitis risk by the biomarkers beyond the antinuclear antibody, and the role of the methotrexate for the uveitis prevention, are the active areas of the research. The precision medicine approaches, targeting the cytokine profile and the genetics, are the emerging therapies that the candidate may name as the future direction. [3][11]
Exam Pearls
The high-yield facts for the examination are the ones that the examiner probes and that the candidate must carry without hesitation. The six-week duration and the under-sixteen age, the seven ILAR categories with the oligoarticular dominance, the persistent-versus-extended split at six months, the chronic anterior uveitis and its silent course, the young-antinuclear-antibody-positive risk profile and the three-monthly slit-lamp, the methotrexate at ten to fifteen milligrams per square metre weekly, and the etanercept and the adalimumab are the core of the topic. The Wallace criteria, the treat-to-target goal, and the septic-arthritis mimic are the clinical reasoning the boards reward. [1][2]
The uveitis is the single most testable complication in the topic, and the principle is simple and absolute. The child who is young, antinuclear-antibody positive, oligoarticular and within the first four years of the disease is the high-risk child, and the three-monthly slit-lamp screening is the non-negotiable defence against the silent scarring. The candidate who carries this single fact, alongside the methotrexate and the biologics, holds the topic that the boards reward. [8][9]
References
- [1]Petty RE, Southwood TR, Manners P, et al International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001 J Rheumatol, 2004.PMID 14760812
- [2]Ravelli A, Martini A Juvenile idiopathic arthritis Lancet, 2007.PMID 17336654
- [3]Giancane G, Alongi A, Ravelli A Update on the pathogenesis and treatment of juvenile idiopathic arthritis Curr Opin Rheumatol, 2017.PMID 28538013
- [4]Giannini EH, Brewer EJ, Kuzmina N, et al Methotrexate in resistant juvenile rheumatoid arthritis. Results of the U.S.A.-U.S.S.R. double-blind, placebo-controlled trial N Engl J Med, 1992.PMID 1549149
- [5]Lovell DJ, Giannini EH, Reiff A, et al Etanercept in children with polyarticular juvenile rheumatoid arthritis N Engl J Med, 2000.PMID 10717011
- [6]Wallace CA, Giannini EH, Spalding SJ, et al Trial of early aggressive therapy in polyarticular juvenile idiopathic arthritis Arthritis Rheum, 2012.PMID 22183975
- [7]Wallace CA, Ruperto N, Giannini E Preliminary criteria for clinical remission for select categories of juvenile idiopathic arthritis using the OMERACT filter J Rheumatol, 2006.PMID 16482643
- [8]Constantin T, Foeldvari I, Anton J, et al Consensus-based recommendations for the management of uveitis associated with juvenile idiopathic arthritis: the SHARE initiative Ann Rheum Dis, 2018.PMID 29592918
- [9]Nordal EB, Foster CS, Ahmed AR, et al Incidence and predictors of uveitis in juvenile idiopathic arthritis in a Nordic long-term cohort study Pediatr Rheumatol Online J, 2017.PMID 28821293
- [10]Rypdal V, Gjerstad IJ, Sanner H, et al Uveitis in juvenile idiopathic arthritis: 18-year outcome in the population-based Nordic cohort study Ophthalmology, 2021.PMID 32866542
- [11]Horneff G, Schulz AC, Klotsche J, et al Efficacy and safety of TNF inhibitors in the treatment of juvenile idiopathic arthritis: a systematic literature review Pediatr Rheumatol Online J, 2023.PMID 36829225
- [12]Shoop-Worrall SJW, Hyrich K, Thursz M, et al How common is remission in juvenile idiopathic arthritis: a systematic review Semin Arthritis Rheum, 2017.PMID 28625712