Paeds · rheumatology-musculoskeletal-and-sports
Musculoskeletal examination and the limping child
Also known as pGALS · paediatric Gait Arms Legs Spine · pREMS · paediatric Regional Examination of the Musculoskeletal System · limping child · Kocher criteria · transient synovitis · Perthes disease · Legg-Calve-Perthes disease · slipped capital femoral epiphysis · SUFE · toddler fracture
A fellowship approach to the paediatric musculoskeletal examination and the limping child: pGALS as the bedside screen, pREMS as the regional deep-dive, and the age-stratified differential that turns a limp into a diagnosis — from transient synovitis to Perthes to slipped capital femoral epiphysis, anchored by the Kocher and Caird prediction rules that separate the irritable hip needing aspiration from the one that does not.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A four-year-old boy wakes with a limp and a sore left knee after a viral cold last week, he is afebrile, he walks with an antalgic gait but bears weight, and his hip has full passive range apart from some guarding — transient synovitis, the commonest cause of limp in this age. A three-year-old girl is febrile at 39 degrees, will not put her foot to the floor, holds her hip flexed and abducted, and has an ESR of 55 and a white cell count of 15,000 — septic arthritis, and the Kocher score is four. A twelve-year-old overweight boy presents with three weeks of vague knee pain and walks with external rotation of his leg — slipped capital femoral epiphysis, and the knee pain is referred from the hip. The task in each is to screen with pGALS, localise with pREMS, apply the prediction rule, and image before assuming the benign. [7] [8]
The five moves — Screen, Localise, Score, Image, Refer
Overview & Definition
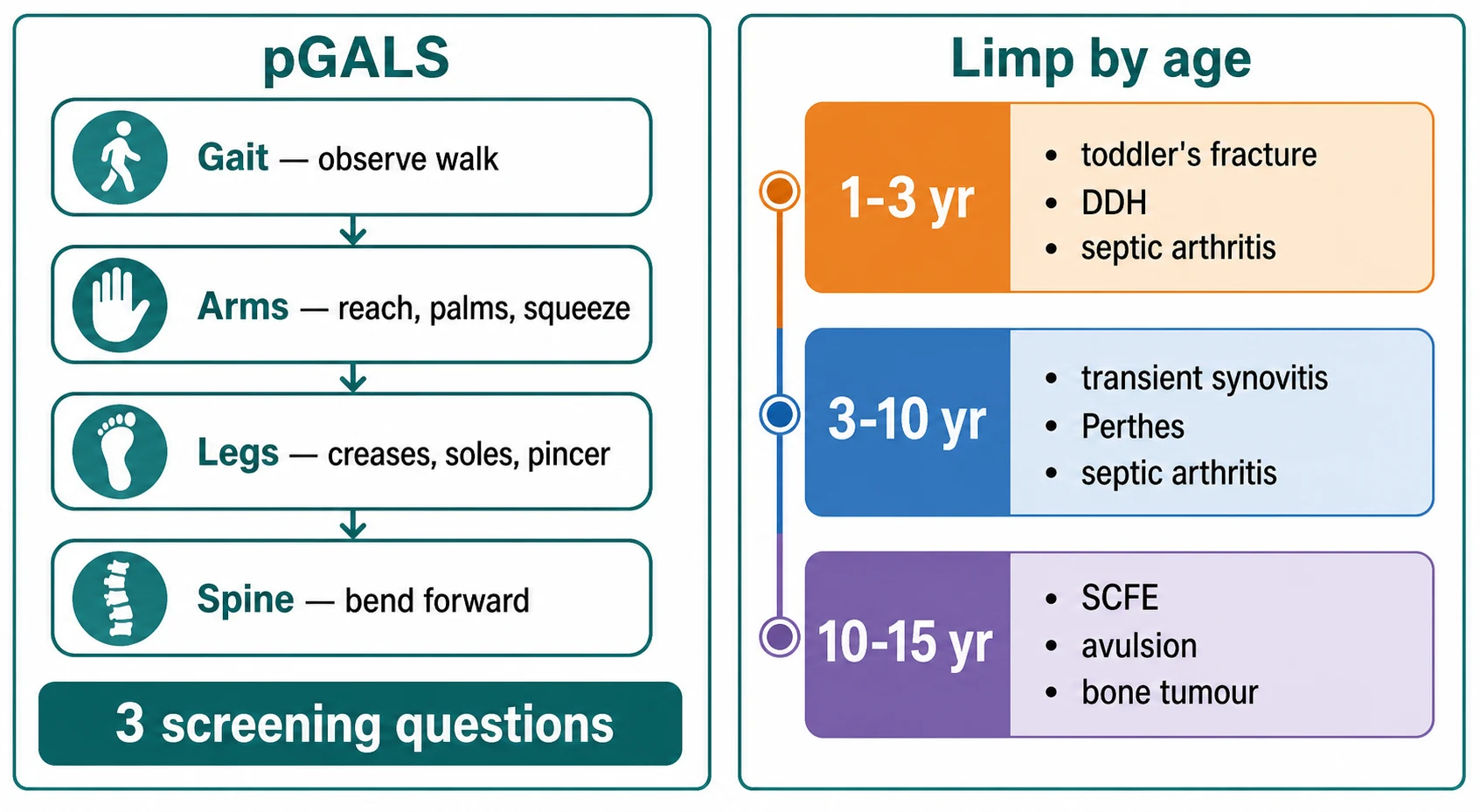
pGALS, the paediatric Gait Arms Legs Spine screen, is a simple, quick musculoskeletal examination adapted from the adult GALS screen for use in school-age children, and it is designed to be performed by any clinician, not only a rheumatologist. It takes two to three minutes, it begins with three screening questions, and it proceeds through a structured look at the gait, the arms, the legs, and the spine. The screen is not a diagnosis — it is a flag, and an abnormal finding prompts a more detailed regional examination. [1] [2]
The limping child is the presentation that tests the musculoskeletal screen most urgently, because a limp may be the only sign of a septic joint, a bone tumour, or an unrecognised fracture. A limp is defined as an asymmetrical gait pattern, and in the young child it often appears as a refusal to walk or a favouring of one leg rather than a complaint of pain. The fellowship task is to decide, rapidly and at the bedside, whether the limp is benign and self-limiting or whether it carries a red flag that demands urgent imaging, bloods, and orthopaedic review. [7] [9]
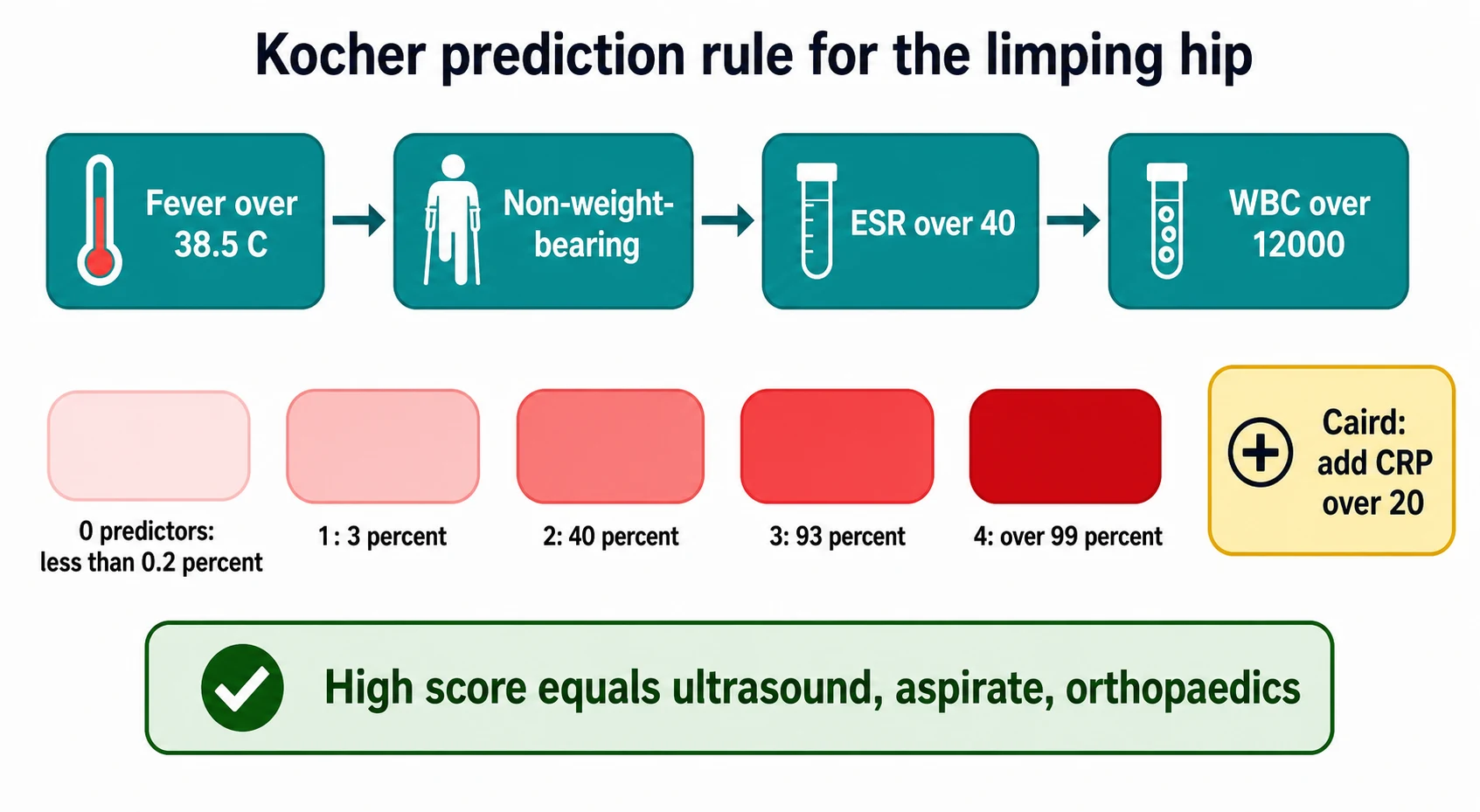
The clinical importance comes from what an unrecognised septic hip does to a child. Bacterial infection of a joint destroys cartilage within hours to days, and a delayed aspiration leads to avascular necrosis, growth disturbance, and lifelong disability. The Kocher prediction algorithm, published in 1999 and validated in 2004, was built precisely to prevent this harm by turning four bedside and laboratory findings into a probability of sepsis that guides the decision to aspirate. [4] [5]
Classification
The musculoskeletal examination runs on two levels. pGALS is the screening level, designed to be quick and broad, and it is built on three questions followed by a head-to-toe look at the gait, the arms, the legs, and the spine. pREMS, the paediatric Regional Examination of the Musculoskeletal System, is the second level, and it is a detailed, region-by-region examination that is performed when pGALS flags an abnormality or when the history points to a specific region. [1] [3]
The limping child is classified along two axes that together drive the differential. The first axis is the presence or absence of pain: a painful limp points toward trauma, infection, or inflammation, while a painless limp points toward developmental dysplasia, a neurological cause, or a structural problem such as a leg-length discrepancy. The second axis is age, because the differential of a limp changes sharply with the developmental stage of the child. [7] [9]
The age axis is the single most useful classifier at the bedside. In the toddler, aged one to three years, the differential is dominated by developmental dysplasia of the hip, septic arthritis, osteomyelitis, the toddler's fracture, and the non-accidental injury that must never be missed. In the school-age child, aged three to ten years, transient synovitis is the commonest cause, followed by Perthes disease and septic arthritis. In the adolescent, aged ten to fifteen years, the slipped capital femoral epiphysis and the apophyseal avulsion fracture enter, alongside bone tumours that peak in this age band. [8] [7]
Epidemiology & Risk Factors
Limp is one of the commonest musculoskeletal presentations in paediatrics, and acute limp accounts for a significant proportion of paediatric emergency and primary care visits. The epidemiology study from Edinburgh found that the majority of limping children have a benign, self-limiting cause, with transient synovitis alone responsible for a large share of cases in the three-to-eight-year age band. The serious causes — septic arthritis, osteomyelitis, Perthes disease, and slipped capital femoral epiphysis — are individually less common but collectively demand the vigilance that this topic teaches. [9] [7]
The risk factors for a serious cause cluster around the age and the clinical picture. A child under three years carries a higher probability of serious disease than an older child, because the toddler cannot localise pain and because conditions such as osteomyelitis and septic arthritis are more aggressive in the young. A fever, a refusal to bear weight, and an elevated inflammatory marker are the individual risk factors that the Kocher rule combines into a probability. A high body mass index is the risk factor for slipped capital femoral epiphysis, and male sex and endocrine disorders such as hypothyroidism and growth hormone deficiency raise the risk further. [4] [7]
The musculoskeletal examination itself is underperformed in paediatric practice, and the underexamination is a risk factor for delayed diagnosis. The "cries from the joints" study documented that the musculoskeletal system is poorly examined in routine paediatric clerking, and children with juvenile idiopathic arthritis and other rheumatic diseases often experience long delays between symptom onset and specialist referral. pGALS was developed to close this gap, and its routine use is the safeguard against the missed examination. [10] [11]
Pathophysiology
The pathophysiology of the limping child is best understood by the tissue that is diseased, because each tissue produces a distinct clinical pattern. The joint, the bone, the growth plate, and the neuromuscular unit each generate their own limp, and the pREMS examination seeks the affected tissue through palpation, range of movement, and special tests. [3] [7]
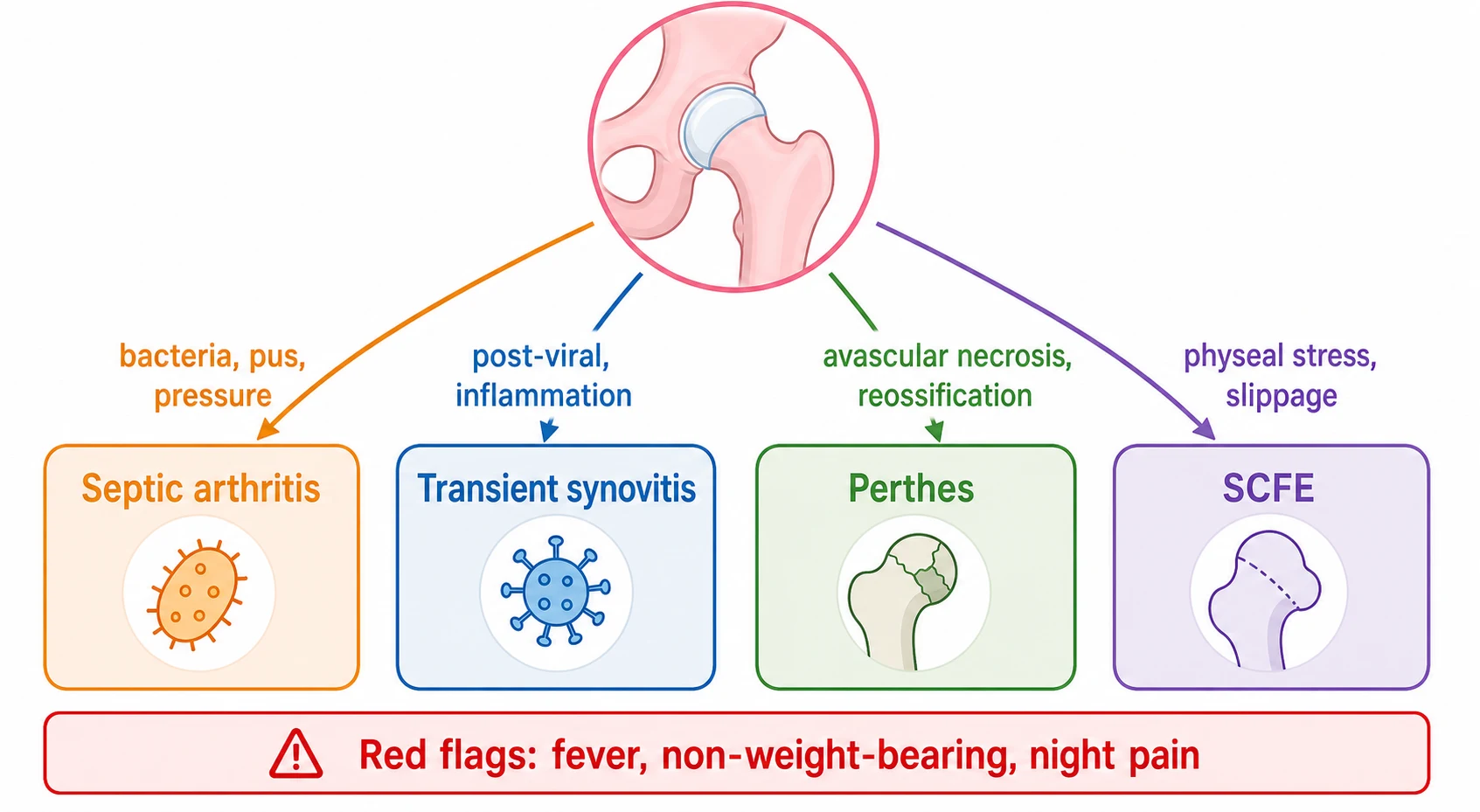
Septic arthritis is a bacterial infection of the synovial joint, most often caused by Staphylococcus aureus, and the pus under pressure destroys the articular cartilage and the blood supply to the femoral head within hours to days. The child holds the joint in the position of maximum capsular volume — flexion, abduction, and external rotation for the hip — and any movement is resisted. The pathophysiology is why this is a surgical emergency: the pus must be drained to save the joint, and every hour of delay compounds the damage. [4] [6]
Transient synovitis is a sterile, self-limiting inflammation of the synovium that often follows a viral upper respiratory infection, and it produces a reactive effusion without cartilage destruction. The child is usually afebrile or has a low-grade fever, bears weight with an antalgic gait, and recovers fully within one to two weeks. The pathophysiology is benign, but the clinical picture overlaps with septic arthritis, which is why the Kocher rule exists to separate the two. [4] [7]
Perthes disease is an idiopathic avascular necrosis of the capital femoral epiphysis, in which the blood supply to the growing femoral head is interrupted, the bone dies and fragments, and then reossifies over two to four years. The child is typically four to eight years, male, and presents with an insidious limp and pain that may be referred to the knee or the thigh. The pathophysiology is a cycle of necrosis, fragmentation, and reossification, and the management aims to contain the femoral head within the acetabulum while it remodels. [7] [9]
Slipped capital femoral epiphysis is a failure of the proximal femoral growth plate under shear load, in which the epiphysis slips posteriorly and inferiorly relative to the metaphysis. The child is typically an overweight adolescent, and the slip may be stable — the child walks with an external rotation gait and chronic pain — or unstable, presenting after an acute fall with an inability to bear weight. The pathophysiology is mechanical and sometimes endocrine, and the management is urgent surgical fixation to prevent further slippage and avascular necrosis. [7] [8]
Clinical Presentation
The presentation of the limping child is shaped by the age, and the fellowship candidate must hold the age-stratified differential in mind from the moment the child walks into the room. The toddler, aged one to three years, may present not with a limp but with a refusal to walk or a regression from walking to crawling, and the differential includes developmental dysplasia of the hip, septic arthritis, osteomyelitis, the toddler's fracture, and non-accidental injury. A fever, a toxic appearance, or a refusal to bear any weight in this age group is a red flag that demands urgent workup. [8] [9]
The school-age child, aged three to ten years, most often presents with an acute or subacute limp and an irritable hip. Transient synovitis is the commonest cause, presenting one to two weeks after a viral illness, with an afebrile or low-grade febrile child who walks with an antalgic gait but still bears weight, holds the hip in slight flexion and external rotation, and has a slightly restricted range of movement. Perthes disease presents more insidiously, with a limp and pain that has built over weeks, and the child may be pain-free at rest. Septic arthritis presents acutely, with fever, toxicity, and an absolute refusal to bear weight. [7] [4]
The adolescent, aged ten to fifteen years, presents with a different set of diagnoses. Slipped capital femoral epiphysis presents with hip, thigh, or knee pain and an external rotation gait, and the pain may be chronic and stable or acute and unstable after a fall. Apophyseal avulsion fractures occur in the athletic adolescent after a sudden sprint or jump, with pain at the anterior superior iliac spine, the anterior inferior iliac spine, or the ischial tuberosity. Bone tumours — osteosarcoma and Ewing sarcoma — peak in this age band and present with progressive, unrelenting pain, often worse at night and unrelated to activity, with a palpable mass in a minority. [7] [8]
The juvenile idiopathic arthritis presentation is the one that pGALS catches and the limp alone may miss. A child with oligoarticular juvenile idiopathic arthritis may present with a chronic limp, morning stiffness lasting more than thirty minutes that improves with activity, a single swollen knee, and a normal or near-normal general examination. The uveitis that accompanies oligoarticular disease is silent and sight-threatening, which is why every child with a swollen joint receives a slit-lamp examination regardless of the limp. [3] [11]
Which reassuring-sounding stories must never close the search for serious disease? A child with transient synovitis may also have a fever, and the Kocher score, not the diagnosis, decides the management. A child with referred knee pain may have a hip problem, and a normal knee examination demands a hip examination and a hip radiograph. And a child with a chronic, painless limp may have a bone tumour or an early Perthes that only the radiograph reveals. [7] [9]
Differential Diagnosis
The differential diagnosis of the limp is driven by age and by the presence of pain. In the toddler, developmental dysplasia of the hip presents as a painless limp or a leg-length discrepancy, detected by the Galeazzi test with the knees flexed and by limited hip abduction, and it is confirmed by ultrasound in the infant and radiograph in the older child. Septic arthritis and osteomyelitis present with fever and refusal to bear weight, the toddler's fracture is a non-displaced spiral tibial fracture detected on radiograph, and non-accidental injury must be considered when the history is inconsistent or the fracture pattern is unexpected. [9] [8]
In the school-age child, the differential of the irritable hip is the fellowship centrepiece. Transient synovitis, Perthes disease, and septic arthritis share the same presenting complaint — a limp and a painful hip — and they are separated by the Kocher score, the temperature, the inflammatory markers, and the imaging. Juvenile idiopathic arthritis enters when the limp is chronic, when there is morning stiffness, when more than one joint is involved, or when the pGALS screen reveals abnormalities beyond the hip. A stress fracture, a discitis in the younger child, and a transient synovitis that fails to resolve are the further considerations. [4] [7]
In the adolescent, the differential broadens to the slipped capital femoral epiphysis, the apophyseal avulsion fracture, and the bone tumour. Slipped capital femoral epiphysis is separated from transient synovitis and Perthes by the age and the external rotation gait, and it is confirmed by a frog-lateral radiograph of both hips. A bone tumour is suspected when the pain is constant, nocturnal, and unrelated to activity, and it is confirmed by radiograph and magnetic resonance imaging. Avascular necrosis from steroid use, sickle cell disease, or trauma is a further consideration in the right clinical context. [7] [9]
The treatable mimics must not be missed. A testicular torsion or an inguinal hernia may present as a limp in a boy who guards the groin, and an intra-abdominal pathology such as appendicitis or psoas abscess may refer pain to the hip. A neurological cause — a cerebral palsy hemiplegia, a muscular dystrophy, or a spinal cord lesion — produces a painless, patterned gait abnormality that the neurological examination reveals. The pGALS and pREMS examination, combined with a focused neurological screen, is the safeguard against these missed diagnoses. [8] [3]
Clinical & Bedside Assessment
The bedside assessment begins with pGALS, and the screen starts before the child is on the couch. Watch the child walk into the room, because the gait is the first and often the most informative examination. An antalgic gait shortens the stance phase on the painful side, a Trendelenburg gait drops the contralateral pelvis from hip abductor weakness, and an external rotation gait with a foot progression angle that has acutely changed suggests a slipped capital femoral epiphysis. [1] [2]
The three pGALS screening questions are asked of the child or the parent. Do you have any pain or stiffness in your muscles, joints, or back? Can you dress yourself without any difficulty? And can you walk up and down stairs without any difficulty? A positive answer to any question, or an abnormal finding on the examination that follows, prompts the five additional questions and the regional examination. The screening questions are sensitive for musculoskeletal disease, and they are the gateway to the pREMS deep-dive. [1] [10]
The pGALS examination proceeds through gait, arms, legs, and spine. The gait is observed for symmetry, foot drop, and limping. The arms are screened by asking the child to reach up with palms forward, put hands behind the head and then behind the back, and by squeezing the metacarpophalangeal joints — the prayer and reverse-prayer positions detect wrist and elbow limitation. The legs are screened by looking at the soles, the calf bulk, and the skin creases, feeling for warmth and effusion at the knees, and moving the hips, knees, and ankles. The spine is screened by inspecting from behind, palpating for tenderness, and asking the child to bend forward — the Adams forward bend test reveals a scoliosis. [1] [3]
When pGALS is abnormal, the pREMS regional examination is performed on the affected region. For the lower limb, the hip is examined for range of movement — flexion, abduction, internal and external rotation — with the child supine, and a loss of internal rotation and abduction is an early sign of a hip effusion or a slipped epiphysis. The knee is examined for effusion with the patellar tap and the bulge sign, and the ankle and foot are examined for swelling and deformity. The spine is examined regionally for tenderness, range of movement, and neurological signs, including a careful lower-limb neurological examination when a spinal cause is suspected. [3] [2]
Which findings must never be dismissed? A child who holds the hip in flexion, abduction, and external rotation and resists any movement has an irritable hip that demands the Kocher score, bloods, and an ultrasound. A child with a palpable mass, night pain, or systemic symptoms has a possible malignancy that demands urgent imaging and a paediatric oncology referral. And a child with a regression of motor milestones, a change in gait pattern, or new neurological signs has a neurological or neuromuscular cause that demands a careful neurological examination and specialist referral. [8] [7]
Investigations
The investigation of the limping child is guided by the clinical picture and the Kocher score. Bloods are taken when an infection or an inflammatory condition is suspected: a full blood count, a C-reactive protein, and an erythrocyte sedimentation rate. The C-reactive protein is the strongest individual predictor of septic arthritis in the Caird study, and an ESR above 40 is a Kocher criterion. Blood cultures are taken when the child is febrile, and a viral screen may support transient synovitis but does not rule out sepsis. [4] [6]
Imaging is selected by the suspected diagnosis. A plain radiograph of the hip and the femur is the first-line imaging for a painful limp, and it may reveal a fracture, a Perthes with widening and irregularity of the joint space and later flattening of the epiphysis, or a slipped capital femoral epiphysis with a widened and displaced physis on the frog-lateral view. An ultrasound of the hip detects a joint effusion and guides aspiration, and it is the key investigation when the Kocher score is intermediate or high. A magnetic resonance imaging is requested when osteomyelitis, a bone tumour, or an atypical infection is suspected, because it reveals bone marrow oedema and soft-tissue extension that the radiograph misses. [7] [5]
Joint aspiration is both diagnostic and therapeutic when septic arthritis is suspected. The aspirate is sent for gram stain, culture, cell count, and crystal analysis, and a white cell count in the synovial fluid above 50,000 per cubic millimetre with a neutrophil predominance strongly supports septic arthritis. The aspiration is performed under ultrasound guidance by an experienced operator, and the orthopaedic team is involved before the needle is placed, because a confirmed septic hip is washed out in theatre. [4] [6]
Management — Resuscitation
Resuscitation is rarely the primary need in the limping child, because most causes are not immediately life-threatening. The exception is the child with septic arthritis who is toxic and septicaemic, in whom the priority is airway, breathing, and circulation, followed by intravenous access, fluid resuscitation if shocked, and empirical intravenous antibiotics after blood cultures. The septic joint is a surgical emergency, and the orthopaedic team is involved at the same time as the resuscitation, not after it. [4] [7]
The child with suspected septic arthritis receives empirical intravenous antibiotics that cover the common organisms once the joint has been aspirated or washed out. Staphylococcus aureus is the commonest organism across all age groups, and Kingella kingae is an important cause in children under four years, often with a milder presentation. The choice of antibiotic follows local guidelines and is guided by the culture result, and the duration is typically two to three weeks intravenously and then orally. [7] [8]
The child with a stable slipped capital femoral epiphysis, an unstable slip, or a suspected bone tumour is managed as an urgent orthopaedic admission, and the general paediatrician's role is to make the diagnosis, arrange the imaging, control the pain, and refer. The limb is kept non-weight-bearing, and the child is prepared for surgical fixation or biopsy. The resuscitation principle is that the diagnosis is made before the deterioration, and the harm is prevented by the early referral. [8] [7]
Management — Definitive & Stepwise
The definitive management of transient synovitis is rest, simple analgesia, and review, and the condition resolves within one to two weeks in the great majority of children. The child is followed up if the limp persists beyond two weeks, because a persistent irritable hip that does not resolve may be an early Perthes, a juvenile idiopathic arthritis, or an unrecognised fracture. The key management decision is the one made at the outset: the Kocher score that confirms the low probability of sepsis and allows the safe, conservative pathway. [4] [7]
The definitive management of septic arthritis is surgical washout and drainage of the joint, combined with intravenous antibiotics. The hip is approached surgically, the pus is evacuated, the joint is irrigated, and the antibiotics are continued for a total course of two to four weeks. The outcome depends on the duration of infection before drainage and the virulence of the organism, and the fellowship answer stresses that the timing of the operation is the single most important determinant of outcome. [4] [6]
The definitive management of Perthes disease is controversial and depends on the age of the child and the extent of the femoral head involvement. The goal is to contain the femoral head within the acetabulum during the reossification phase, and this is achieved by observation and activity modification in the young child with mild involvement, and by containment surgery — a femoral or pelvic osteotomy — in the older child with extensive involvement. The lateral pillar classification of the femoral head fragments guides the decision, and the prognosis is better in children under six years and in those with less than half the head involved. [7] [9]
The definitive management of slipped capital femoral epiphysis is urgent surgical fixation with a single cannulated screw placed across the physis in situ, regardless of whether the slip is stable or unstable. The unstable slip is a surgical emergency, because the risk of avascular necrosis is high and the window for fixation is narrow. The contralateral hip is imaged and monitored, because bilateral involvement occurs in roughly a quarter of children, and prophylactic fixation of the unaffected hip is considered in high-risk groups. [8] [7]
The age-stratified diagnoses and their first management
Specific Subtypes & Scenarios
Transient synovitis is the archetype of the benign irritable hip, and it is the diagnosis that the Kocher rule is designed to confirm by exclusion. The child is three to eight years, presents one to two weeks after a viral upper respiratory infection, and walks with an antalgic gait while still bearing weight. The hip is held in flexion and external rotation, the range is slightly limited, and the child is afebrile or has a low-grade fever. The inflammatory markers are normal or mildly elevated, the ultrasound may show a small effusion, and the limp resolves within one to two weeks with rest and simple analgesia. The fellowship skill is to apply the Kocher rule, confirm the low probability of sepsis, and follow up if the limp persists. [4] [7]
Septic arthritis is the subtype that demands the most urgent action. The child is febrile, toxic, and refuses to bear weight, the hip is held rigidly in the position of maximum capsular volume, and any movement is agonising. The Kocher score is high, the C-reactive protein is elevated, the ultrasound confirms an effusion, and the aspirate shows a high white cell count and organisms on gram stain. The management is immediate surgical washout and intravenous antibiotics, and the outcome depends on the speed of the operation. The fellowship answer never underestimates this subtype and never delays the aspiration. [4] [6]
Perthes disease is the subtype that teaches patience. The child is four to eight years, presents with an insidious limp and pain referred to the thigh or knee, and the initial radiographs may be normal or show only a widened joint space. The diagnosis becomes clear as the femoral head fragments and flattens over the following months, and the management is containment of the head within the acetabulum during the reossification phase, which takes two to four years. The prognosis is better in the young and the mildly affected, and the fellowship answer frames the long timeline and the role of the orthopaedic team in guiding containment. [7] [9]
Slipped capital femoral epiphysis is the subtype that presents with knee pain. The overweight adolescent walks with an external rotation gait, the hip has a loss of internal rotation, and the frog-lateral radiograph reveals the posterior and inferior slip of the epiphysis. The stable slip is fixed urgently and the unstable slip is fixed emergently, and the contralateral hip is monitored. The fellowship skill is to image the hips of any overweight adolescent with unexplained knee or thigh pain, because the referred pain is the trap that delays the diagnosis. [8] [7]
Complications & Pitfalls
The complications of a delayed or missed diagnosis span the joint, the bone, and the child's future. A septic hip drained late develops avascular necrosis of the femoral head, growth disturbance of the proximal femur, and premature osteoarthritis, and the child may need multiple reconstructive operations across childhood and adolescence. The harm is permanent, and it is the reason the Kocher rule exists and the reason the aspirate is not delayed. [4] [6]
The pitfall of the referred knee pain is the error that delays the diagnosis of slipped capital femoral epiphysis. An adolescent who presents with knee pain is examined at the knee and discharged, and the hip slip progresses until it becomes unstable or until the radiograph is finally taken. The safeguard is the rule that every child with knee pain receives a hip examination and, when the knee is normal, a hip radiograph. The pitfall of the normal initial radiograph in Perthes is the related error, and the safeguard is the follow-up and the magnetic resonance imaging when the limp persists. [7] [9]
The pitfall of the overcalled Kocher score is the error that leads to an unnecessary aspiration. A child with transient synovitis and a low-grade fever may score one or two on the Kocher rule, and an overcautious clinician aspirates a sterile joint, causing pain, anxiety, and a small risk of introducing infection. The safeguard is the accurate application of the rule, the addition of the C-reactive protein from the Caird study, and the use of ultrasound to confirm a significant effusion before the needle is placed. [5] [6]
The pitfall of the unrecognised non-accidental injury is the error with the gravest consequences beyond the joint. A toddler with a fracture and an inconsistent history, a delayed presentation, or other injuries on examination may be a victim of abuse, and the missed diagnosis returns the child to a dangerous environment. The safeguard is the careful history, the full examination including the skin and the retina, the skeletal survey when indicated, and the involvement of the child protection team. [9] [8]
Prognosis & Disposition
The prognosis of the limping child is generally excellent when the serious causes are identified and treated promptly. Transient synovitis resolves completely within one to two weeks in the great majority, with a small recurrence rate and no long-term sequelae. Septic arthritis, when drained within the first day or two, has a good outcome in most children, and the prognosis worsens with each day of delay and with the virulence of the organism. Perthes disease has a variable prognosis that depends on the age at onset and the extent of the femoral head involvement, with children under six years and those with less than half the head involved doing well. [7] [9]
Slipped capital femoral epiphysis has a prognosis that depends on the stability of the slip and the occurrence of avascular necrosis. A stable slip fixed in situ has a good outcome, while an unstable slip carries a high risk of avascular necrosis and chondrolysis, and the long-term outlook includes premature osteoarthritis in a significant proportion. The contralateral hip is monitored for the lifetime risk of a second slip, and prophylactic fixation is considered in high-risk children. [8] [7]
The disposition is shared between the general paediatrician, the orthopaedic surgeon, and the paediatric rheumatologist. The general paediatrician owns the initial assessment, the pGALS screen, the Kocher score, and the decision to refer. The orthopaedic surgeon owns the septic joint, the slipped epiphysis, and the containment of Perthes. The paediatric rheumatologist owns the juvenile idiopathic arthritis and the chronic, multisystem rheumatic disease. The fellowship answer names the right specialist for the right diagnosis and never holds a child with a red flag in the outpatient clinic when the emergency pathway is indicated. [3] [11]
Special Populations
Children with developmental disability and neurodiversity present particular challenges in the musculoskeletal examination. A child with cerebral palsy may have a pre-existing gait abnormality that masks a new limp, and a child with limited communication may not localise pain, so the examination relies on observing the change from the baseline, the refusal to bear weight, and the physiological signs of distress. The pGALS screen is adapted to the child's abilities, and the threshold for imaging and bloods is lower when the history is uncertain. [3] [8]
Indigenous, remote, and socioeconomically disadvantaged children face the additional burdens of access and equity. The incidence of osteoarticular infection, including osteomyelitis and septic arthritis from Staphylococcus aureus and other organisms, is higher in many remote Indigenous communities, and the distance to imaging and specialist review delays the diagnosis and the drainage. A newly arrived migrant or refugee child may have an undocumented history of musculoskeletal disease, and the workup may need to begin from first principles. The fellowship answer acknowledges these inequities and builds the rapid-referral pathways that close the gap. [9] [7]
The child in out-of-home care and the child at risk of maltreatment are the special populations that demand the highest vigilance. A limp or a fracture in a pre-verbal child, an inconsistent history, a delay in presentation, or a pattern of injury that does not fit the mechanism raises the question of non-accidental injury, and the safeguard is the careful history, the full examination, the skeletal survey when indicated, and the involvement of the child protection team. The musculoskeletal examination is one window into the child's safety, and the fellowship candidate does not close it after the bone is dealt with. [9] [8]
Evidence, Guidelines & Regional Differences
The evidence base for the paediatric musculoskeletal examination rests on the pGALS studies from Foster and colleagues. The original 2006 paper validated pGALS in school-age children and demonstrated that it is a simple, acceptable screen that detects musculoskeletal abnormalities in a meaningful proportion of children. The 2013 update provided a practical guide to the pGALS examination, and the 2006 review with Cabral framed the paediatric musculoskeletal history and examination within the broader clinical context. The "cries from the joints" study documented the poor documentation of the musculoskeletal system in routine paediatric clerking, which is the problem pGALS was built to solve. [1] [10]
The evidence for the Kocher prediction rule rests on the 1999 derivation study and the 2004 validation study, both from the Boston group. The 1999 study identified four predictors of septic arthritis — fever, refusal to bear weight, an ESR above 40, and a white cell count above 12,000 — and assigned a probability of sepsis to each combination. The 2004 study validated the rule in a second cohort and showed that the probability held, though the absolute risks were somewhat lower than in the original. The Caird study from 2006 added the C-reactive protein as a further predictor and found it to be the strongest individual discriminator between septic arthritis and transient synovitis. [4] [6]
The regional differences are modest but real. The Kocher rule was derived in a North American population, and its performance varies by the local prevalence of septic arthritis and the organisms involved. In regions where Kingella kingae is a common cause of osteoarticular infection in young children, the presentation may be milder and the Kocher score lower, and the clinician maintains a low threshold for aspiration. The Paediatric Musculoskeletal Matters online portfolio provides open-access, region-appropriate guidance on pGALS and pREMS, and its evaluation confirmed its reach and utility across diverse settings. [11] [5]
The controversies are few but real. The role of magnetic resonance imaging in the early Perthes that has a normal radiograph, the decision to prophylactically fix the contralateral hip in slipped capital femoral epiphysis, and the threshold for the skeletal survey in the limping toddler are the judgement calls that the fellowship answer names without pretending that a single algorithm resolves them. The general paediatrician applies the evidence, recognises the uncertainty, and involves the specialist when the decision is at the margin. [7] [8]
Exam Pearls
The fellowship answer turns on five facts. pGALS is a simple screen of gait, arms, legs, and spine built on three questions, and an abnormal finding prompts pREMS. The limp is classified by pain and by age — transient synovitis in the three-to-eight-year-old, Perthes in the four-to-eight-year-old, slipped capital femoral epiphysis in the overweight adolescent, and developmental dysplasia or septic arthritis in the toddler. The Kocher rule turns four findings into a probability of sepsis, and the Caird addition of C-reactive protein tightens the call. Knee pain may be referred from the hip. And the septic hip is a surgical emergency. [1] [4]
The examiner probes three traps. The first is the irritable hip with a fever that is called transient synovitis — the Kocher score, not the label, decides the management, and a high score means aspiration. The second is the adolescent with knee pain who is discharged without a hip radiograph — the slipped capital femoral epiphysis is missed until it becomes unstable, and the frog-lateral film is the safeguard. The third is the limping toddler whose fracture is accepted at face value — the non-accidental injury is missed when the history is not interrogated and the skeletal survey is not considered. [4] [9]
The examiner rewards the candidate who frames the limping child as a clinical reasoning exercise, not a list. The gait is observed, the pGALS screen is run, the Kocher score is applied, the imaging is chosen, and the right specialist is called. The child is followed up, the persistent limp is investigated, and the family is given a clear explanation and plan. A candidate who shows this breadth and this safety demonstrates the systems thinking that the fellowship demands. [7] [11]
References
- [1]Foster HE, Kay LJ, Friswell M, Coady D, Myers A. Musculoskeletal screening examination (pGALS) for school-age children based on the adult GALS screen. Arthritis and Rheumatism, 2006.PMID 17013854
- [2]Foster HE, Jandial S. pGALS - paediatric Gait Arms Legs and Spine: a simple examination of the musculoskeletal system. Pediatric Rheumatology Online Journal, 2013.PMID 24219838
- [3]Foster HE, Cabral DA. Is musculoskeletal history and examination so different in paediatrics? Best Practice and Research. Clinical Rheumatology, 2006.PMID 16546055
- [4]Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction algorithm. Journal of Bone and Joint Surgery. American Volume, 1999.PMID 10608376
- [5]Kocher MS, Mandiga R, Zurakowski D, Barnewolt C, Kasser JR. Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. Journal of Bone and Joint Surgery. American Volume, 2004.PMID 15292409
- [6]Caird MS, Flynn JM, Leung YL, Millman JE, D'Italia JG, Dormans JP. Factors distinguishing septic arthritis from transient synovitis of the hip in children. A prospective study. Journal of Bone and Joint Surgery. American Volume, 2006.PMID 16757758
- [7]Payares-Lizano M. The limping child. Pediatric Clinics of North America, 2020.PMID 31779828
- [8]Adamson J, Waterfield T. Fifteen-minute consultation: the limping child. Archives of Disease in Childhood. Education and Practice Edition, 2020.PMID 31255998
- [9]Fischer SU, Beattie TF. The limping child: epidemiology, assessment and outcome. Journal of Bone and Joint Surgery. British Volume, 1999.PMID 10615981
- [10]Myers A, McDonagh JE, Gupta K, Hull R, Barker D, Kay LJ, Foster HE, et al. More cries from the joints: assessment of the musculoskeletal system is poorly documented in routine paediatric clerking. Rheumatology (Oxford), 2004.PMID 15187245
- [11]Smith N, Foster HE, Jandial S. A mixed methods evaluation of the Paediatric Musculoskeletal Matters (PMM) online portfolio. Pediatric Rheumatology Online Journal, 2021.PMID 34108019