Paeds · rheumatology-musculoskeletal-and-sports
Nursemaid's elbow and common upper-limb injury
Also known as nursemaid's elbow · pulled elbow · radial head subluxation · annular ligament displacement · hyperpronation reduction · supination-flexion reduction · supracondylar humerus fracture · Gartland classification · torus fracture · buckle fracture · greenstick fracture · clavicle fracture · lateral pinning
A fellowship approach to nursemaid's elbow (radial head subluxation) and the common paediatric upper-limb injuries: the classic traction history and the well child holding the arm in flexion and pronation, the two reduction manoeuvres with hyperpronation as the preferred first technique over supination-flexion on the evidence of the Macias and Aksel randomised trials, the dispensable role of radiographs in the classic case, the counselling to prevent recurrence, and the broader family of common upper-limb injuries — the supracondylar humerus fracture read through the Gartland classification with the lateral-entry pinning and the volar pulseless hand, the torus and the greenstick forearm fractures with the remodelling principle and the FORCE soft-bandage evidence, and the clavicle fracture of birth and fall.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A two-year-old girl is carried into the emergency department forty minutes after her father, hurrying across a carpark, lifted her by the right wrist to swing her over a gutter. She cried briefly, then refused to use the arm. She is afebrile, alert, and smiling, holding the right arm at her side with the elbow flexed to twenty degrees and the forearm pronated. There is no swelling, no deformity, no warmth, and no point tenderness on palpation of the elbow, but she resists supination. The history is classic for a radial head subluxation. The reduction is attempted by hyperpronation: the examiner holds the elbow and fully pronates the extended forearm in one smooth motion. Two minutes later the child reaches for a toy with the right hand. The clinical skill is to recognise the pattern, reduce without a radiograph, and counsel the family. [1] [4]
Pronation-Preferred — the reduction you reach for first
Overview & Definition
Nursemaid's elbow, also called a pulled elbow or a radial head subluxation, is the displacement of the annular ligament onto or into the radiocapitellar joint that follows a sudden longitudinal traction force applied to the pronated and extended forearm of a young child. It is the commonest upper-limb injury of early childhood seen in primary care and in the emergency department, and it is the archetype of a benign, easily treatable condition whose recognition is entirely clinical. The child is well, the arm is guarded in flexion and pronation, and there is no swelling, no deformity, and no bony tenderness — features that, together with the classic pulling history, make the diagnosis without any imaging. [4] [5]
The clinical importance of nursemaid's elbow lies in the ease of the bedside cure and in the prevention of the recurrence. The reduction is a ten-second manoeuvre, performed in the consulting room or the emergency department, that restores the arm to full use within minutes; the radiograph is unnecessary in the classic case and is reserved for the atypical history or the failed reduction; and the counselling — the single most important element of the disposition — turns the family into the safeguard against recurrence, because the child who is pulled by the wrist or swung by the arms will subluxate again. Roughly a quarter to a third of children recur, and the recurrence is prevented by the simple avoidance of longitudinal traction, not by any immobilisation or restriction. [3] [4]
The page that follows treats nursemaid's elbow as the paediatric generalist encounters it: recognised on the history, reduced at the bedside, discharged with counselling, and prevented from recurring. It then widens to the broader family of the common upper-limb injuries that share the presentation of the guarding arm or the injured limb — the supracondylar humerus fracture, the torus and the greenstick forearm fractures, and the clavicle fracture — because the generalist's task at the bedside is to separate the easily reduced subluxation from the fractures that need splinting, orthopaedic referral, or the vascular check. [5] [7]
Classification
Nursemaid's elbow itself is a single clinical entity, but the upper-limb injury page classifies along two axes that together guide the management. The first axis is the mechanism: the traction injury that produces the radial head subluxation, and the fall-on-outstretched-hand mechanism that produces the fractures. The traction injury is the longitudinal pull on the pronated, extended forearm — the parent lifting the child by the wrist to prevent a fall, or swinging the child by the arms in play — and it is the signature mechanism of nursemaid's elbow. The fall-on-outstretched-hand mechanism is the axial load transmitted up the extended limb, and it is the signature mechanism of the supracondylar humerus fracture, the distal forearm fractures, and the clavicle fracture sustained in a fall. [4] [7]
The second axis is the severity of the common fractures, classified by the system that governs the disposition. The supracondylar humerus fracture is classified by the Gartland system — type I, undisplaced; type II, displaced with an intact posterior cortex; type III, completely displaced with no cortical contact — and the Gartland grade predicts the need for reduction and pinning and the risk of neurovascular injury. The distal forearm fracture is classified by the pattern — the torus or buckle fracture, the greenstick fracture, and the complete or both-bone fracture — and the pattern predicts the remodelling potential and the immobilisation. The clavicle fracture is classified by the site — the midshaft, the medial third, and the lateral third — and the displacement, which together predict the non-operative versus the operative disposition. [7] [10]
The atypical radial head subluxation — the child with a non-classic history, the point tenderness, the swelling, or the failure to reduce — is the classification problem that demands the radiograph, because the missed lateral condyle fracture and the undisplaced supracondylar fracture hide among the pseudoparalysed arms. The Macias 2000 study showed that a non-classic history for the mechanism raises the relative risk of a fracture, and that the radiograph is the safeguard when the classic picture is absent. The classification of the guarding arm is therefore the recognition of the classic radial head subluxation first, and the radiograph second, in every case that does not fit. [2] [5]
The guarding arm — the four common upper-limb patterns
Nursemaid's elbow
Supracondylar fracture
Torus (buckle) fracture
Clavicle fracture
Epidemiology & Risk Factors
Radial head subluxation affects children between the ages of six months and about five or six years, with the peak incidence in the second and third years of life, when the annular ligament is thin and lax and the child is newly mobile and frequently lifted by the arms. It is rare under six months and uncommon after five years, because the annular ligament thickens and strengthens with age and the radial head enlarges, so that the ligament no longer slips over it. The left arm is affected slightly more often than the right, a fact attributed to the predominantly right-handed adults who lift the child with their dominant hand by the child's contralateral arm. [4] [5]
The recurrence is the single most important epidemiological fact for the family. Roughly a quarter to a third of children who have one radial head subluxation will have another, and the recurrence is driven by the same mechanism — the longitudinal traction on the extended, pronated forearm — until the annular ligament matures. The recurrence is not a marker of instability or of a connective tissue disorder in the typical case; it is the predictable consequence of the child's anatomy and the pulling behaviour, and it is prevented by the counselling alone. The family is told to lift the child under the axillae, to avoid swinging the child by the arms, and to hold the hand rather than the wrist when walking, and the recurrence rate falls accordingly. [3] [4]
The common upper-limb fractures follow their own epidemiology. The supracondylar humerus fracture is the commonest elbow fracture in children, peaking between five and seven years, and it is the fracture that carries the neurovascular risk. The distal forearm fracture — the torus, the greenstick, and the complete fracture — is the commonest fracture of childhood overall, sustained in the low-energy fall of the playground. The clavicle is the most commonly fractured bone at birth and in early childhood, from the birth canal or the fall onto the shoulder. Each pattern tells the examiner the mechanism, the expected deformity, and the disposition. [7] [9]
Pathophysiology
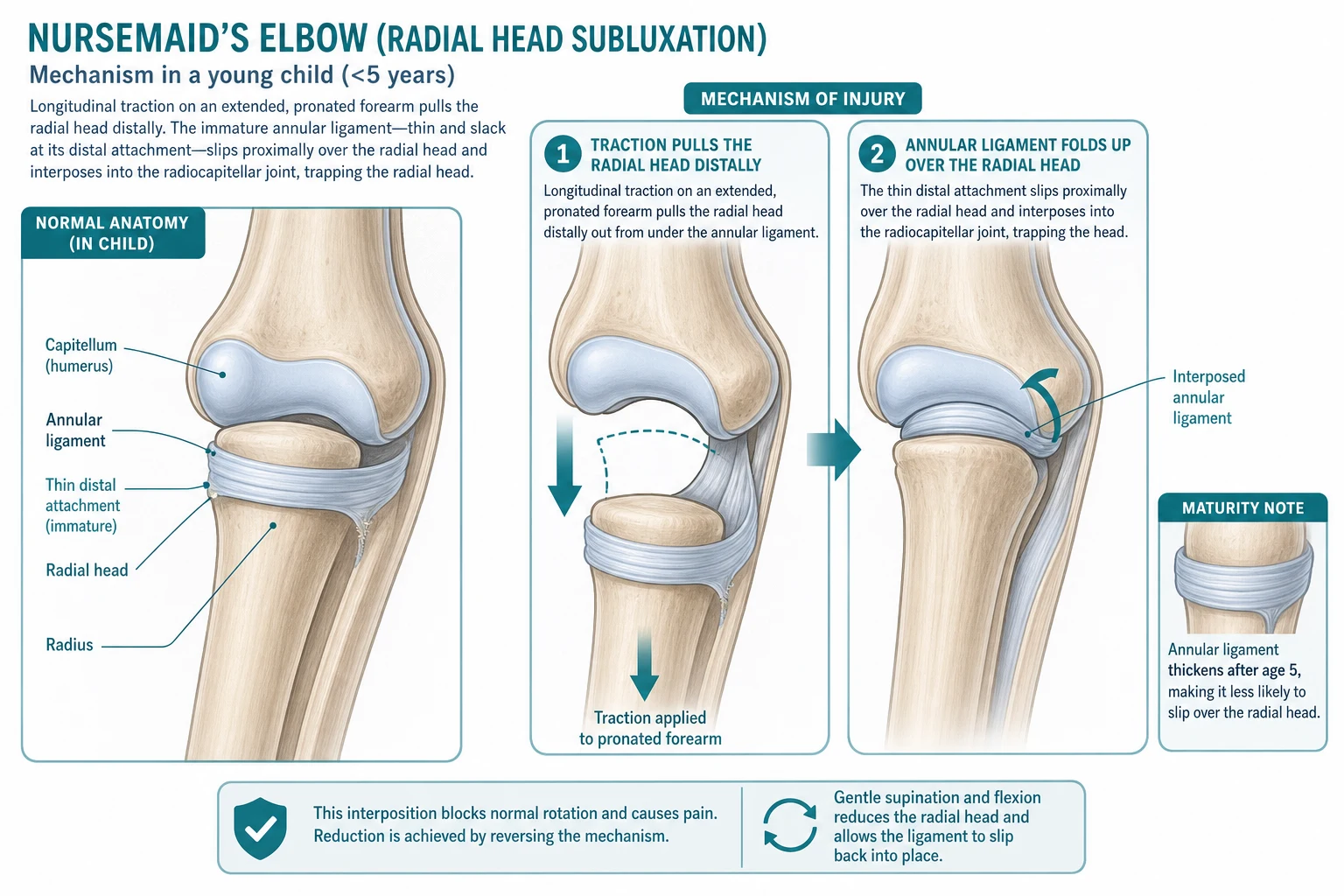
The pathophysiology of the radial head subluxation lies in the anatomy of the annular ligament in the young child. The annular ligament is a strong band that encircles the radial head and holds it in the radial notch of the ulna, forming the proximal radioulnar joint. In the child under five, the radial head is small and the distal attachment of the annular ligament to the radius is thin, lax, and only loosely attached to the periosteum. When a longitudinal traction force is applied to the pronated and extended forearm, the radial head is pulled distally within the lax ligament, and the thin distal part of the annular ligament tears or stretches and slips proximally over the radial head, interposing into the radiocapitellar joint and trapping the head. The result is the painful locking of the elbow in the flexed and pronated position and the refusal to use the arm. [4] [5]
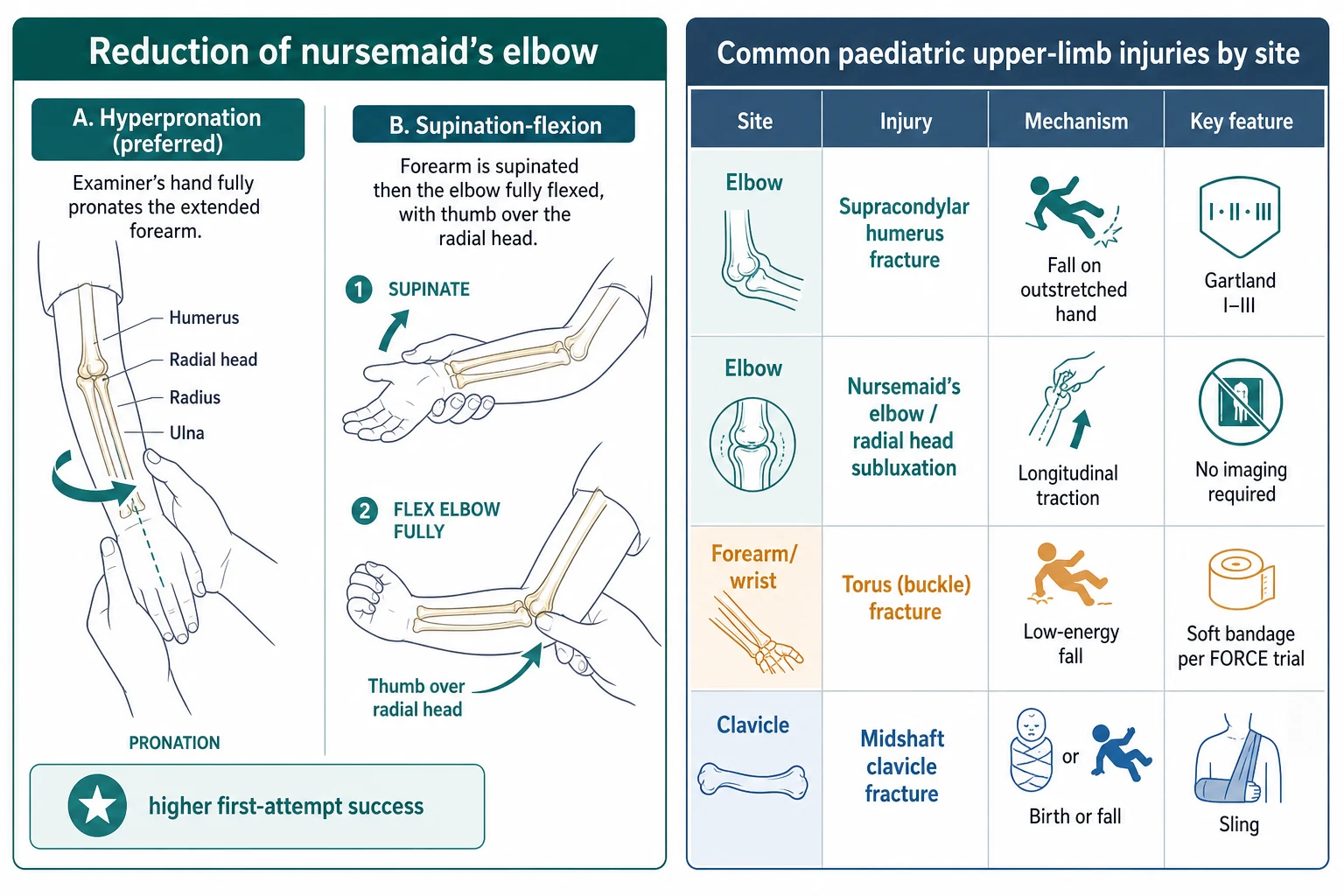
The reduction manoeuvres work by reversing the mechanism. The hyperpronation technique fully pronates the extended forearm, which tightens the annular ligament and squeezes the interposed ligament back over the radial head and out of the joint. The supination-flexion technique supinates the forearm and flexes the elbow, which opens the joint space and allows the ligament to slip back, often with a palpable or audible click. The hyperpronation technique is the more effective because it applies a tighter circumferential force to the ligament, and the randomised evidence confirms the higher first-attempt success rate. The maturation of the ligament after the age of five — the thickening and the firm attachment to the radius — is the reason the condition becomes rare, and the reason the recurrence eventually ceases. [1] [6]
The pathophysiology of the common upper-limb fractures frames the management. The supracondylar humerus fracture is the extension injury of the distal humerus, the distal fragment pushed posteriorly and proximally by the fall on the outstretched hand, and the displacement threatens the brachial artery and the median and the anterior interosseous nerves on the anterior surface. The torus fracture is the compression failure of the dorsal cortex of the distal radius, the bone buckled but not broken through, and the intact periosteum confers the inherent stability and the rapid union. The greenstick fracture is the incomplete fracture, the tension side broken and the compression side bent, and the periosteal hinge guides the remodelling. The clavicle fracture is the bending failure of the S-shaped bone, the midshaft the commonest site because it is the thinnest and the least supported. [7] [10]
Clinical Presentation
The child with the radial head subluxation presents with the arm held still. The classic history is the sudden longitudinal pull on the arm — the parent lifting the child by the wrist to step over a curb, to prevent a fall, or to swing the child in play — followed by a brief cry and the immediate refusal to use the arm. The child is well, afebrile, and comfortable, and the only sign is the guarding. The arm is held at the side, the elbow flexed to twenty to thirty degrees, and the forearm pronated. The child will not reach for a toy, will not take an object, and resists any attempt to move the arm, particularly the supination of the forearm. There is no swelling, no deformity, no warmth, and no bruising, and palpation reveals no point tenderness, though the child may be vaguely uncomfortable around the lateral elbow. [4] [5]
The atypical presentation is the radiograph trigger. A history of a fall rather than a pull, a history that does not fit the traction mechanism, the presence of swelling, deformity, bruising, or point tenderness on palpation, or the refusal to use the arm that persists after two adequate reduction attempts with both techniques — these are the features that demand the radiograph, because the missed lateral condyle fracture, the undisplaced supracondylar fracture, and the occult fracture hide among them. The Macias 2000 study showed that the non-classic history raises the relative risk of an underlying fracture, and the safeguard is the radiograph in every case that does not fit the classic picture. [2] [5]
The supracondylar fracture presents after a fall on an outstretched hand with the elbow swollen, painful, and held in flexion, and with the S-deformity or the prominent olecranon of the displaced type III. The anterior interosseous nerve is the commonest nerve injured in the extension type — tested by the OK sign and the thumb-index pinch — and the brachial artery may be compromised, so the radial pulse, the capillary refill, and the warmth of the hand are documented. The torus fracture presents with the minimal swelling and tenderness of the distal radius after a low-energy fall, and the child may even use the arm with reluctance. The clavicle fracture presents with the pain on movement of the arm and the palpable lump at the midshaft, and the newborn may present with the pseudoparalysis of the birth fracture, not moving the arm on the affected side. [7] [10]
Differential Diagnosis
The differential of the guarding arm is the first decision the general paediatrician makes. The radial head subluxation is the classic pattern, and the diagnosis is made on the traction history and the absence of swelling and tenderness. The supracondylar humerus fracture is the diagnosis when the history is a fall and the elbow is swollen or deformed, and the radiograph confirms the Gartland grade. The lateral condyle fracture is the diagnosis when the swelling is lateral and the child fell onto an extended, varus-stressed elbow, and it is the fracture most easily missed because the displacement may be subtle on the initial film. The occult fracture — the undisplaced distal radius or the torus fracture — is the diagnosis when the tenderness is localised to a bone and the radiograph is warranted. [5] [7]
The differential extends to the non-traumatic causes of the guarding arm in the young child. The septic arthritis and the osteomyelitis of the elbow or the shoulder present with the fever, the swelling, the warmth, and the refusal to move the arm, and the inflammatory markers and the imaging separate them from the injury. The transient synovitis of the shoulder, rare but recognised, presents with the limping-equivalent of the upper limb. The brachial plexus injury of the newborn, the obstetric palsy, presents with the asymmetric Moro and the arm held internally rotated, not with the acute guarding. The non-accidental injury is the differential when the history does not fit the injury or the child is pre-mobile, and the safeguarding workup runs alongside the treatment. [5]
The skill at the bedside is to separate the traction-injured, well child — reduced at the chairside without imaging — from the fall-injured, swollen child who needs the radiograph, the splint, and the orthopaedic referral. The radial head subluxation is excluded by the appearance of any of these mimics, and the mimics are excluded by the radiograph and the clinical assessment. The generalist who holds this differential in mind avoids both the unnecessary radiograph in the classic subluxation and the missed fracture in the atypical case. [2] [7]
Clinical & Bedside Assessment
The examination of the guarding arm begins with the observation of the child at rest. The posture is the first clue: the flexed and pronated forearm held at the side, with the child refusing to use the arm but otherwise well, is the posture of the radial head subluxation. The swollen, deformed, or bruised elbow is the posture of the fracture, and the febrile, irritable child with the swollen joint is the posture of the infection. The general appearance — the well, afebrile, comfortable child — is the feature that supports the radial head subluxation and argues against the infection. [4] [5]
The palpation follows. The elbow is palpated for the swelling, the warmth, and the point tenderness, and the radial head is palpated just distal to the lateral epicondyle. In the radial head subluxation, there is no point tenderness, no swelling, and no warmth, though the child may be mildly uncomfortable. The presence of the point tenderness, the swelling, or the deformity is the feature that argues for the fracture or the infection and that warrants the radiograph or the further workup. The forearm and the clavicle are palpated for the tenderness and the deformity of the occult fracture, because the guarding arm may hide an injury proximal or distal to the elbow. [5]
The range of motion is then tested gently. The child with the radial head subluxation resists the supination and the extension of the forearm, the movements that stress the interposed ligament, and the pronation and the flexion are relatively comfortable. The child with the fracture resists all movement. The neurovascular assessment is the safeguard in every upper-limb injury: the radial pulse, the capillary refill, the warmth, and the colour of the hand are documented, the median, the radial, and the ulnar nerves are tested by the OK sign, the thumb extension, and the finger spreading, and the anterior interosseous nerve is tested by the thumb-index pinch. The neurovascular compromise is the emergency, and the documentation before and after any reduction is the medico-legal and the clinical standard. [7] [10]
Investigations
The diagnosis of the radial head subluxation is clinical, and no imaging is required in the classic case. The history of the longitudinal traction on the pronated, extended forearm, the well child, the flexed and pronated posture, and the absence of the swelling, the deformity, and the point tenderness are sufficient to make the diagnosis and to attempt the reduction. The radiograph is unnecessary, it delays the cure, and it exposes the child to the radiation without changing the management in the classic case. [2] [4]
The radiograph is indicated in the atypical case and in the failed reduction. The non-classic history — the fall rather than the pull, the absence of a clear traction mechanism — raises the relative risk of an underlying fracture, as the Macias 2000 study showed, and the radiograph is the safeguard. The point tenderness, the swelling, the deformity, or the bruising argues for the fracture and the radiograph. The failure to reduce after two adequate attempts with both the hyperpronation and the supination-flexion techniques argues for an alternative diagnosis and the radiograph. In each of these scenarios, the radiograph excludes the missed lateral condyle fracture, the undisplaced supracondylar fracture, and the occult fracture of the forearm. [2] [5]
The ultrasound and the magnetic resonance imaging are not part of the radial head subluxation workup. The radiograph of the supracondylar fracture is the anteroposterior and the lateral of the elbow, read for the Gartland grade, the anterior fat pad sign, the posterior fat pad sign, and the capitellum-to-humerus alignment. The radiograph of the torus fracture shows the cortical buckling of the dorsal distal radius, and the radiograph of the clavicle shows the midshaft fracture and the displacement. The imaging is the adjunct to the clinical assessment, and the recognition of the radial head subluxation on the history alone is the skill the fellowship rewards. [7] [9]
Management — Resuscitation
The management of the radial head subluxation does not, in the typical case, demand a resuscitation. The child is well, the airway and the breathing are normal, and the circulation is intact. The management is the prompt recognition of the pattern and the bedside reduction, performed in the consulting room or the emergency department without delay. The early reduction is the resuscitative principle, because it relieves the child's discomfort and restores the arm to use within minutes, and the delay serves no purpose when the diagnosis is clear. [1] [4]
The resuscitation is reserved for the upper-limb injuries that threaten the limb or the life. The supracondylar fracture with the pulseless, cold, or pale hand is the vascular emergency: the elbow is reduced and stabilised, the hand is re-perfused, and the child is taken to theatre for the closed reduction and the percutaneous pinning, with the vascular surgeon on standby. The open fracture is the emergency: the wound is covered, the tetanus is updated, the intravenous antibiotics are given, and the child is taken to theatre for the washout and the fixation. The child with the suspected non-accidental injury enters the safeguarding pathway alongside the treatment of the fracture. [7] [10]
The analgesia is the humane element of the resuscitation. The radial head subluxation is briefly uncomfortable during the reduction, and the parent's reassurance and the distraction are often sufficient, though the brief pain of the manoeuvre is the price of the cure. The fracture is splinted and the analgesia is given — the oral paracetamol at fifteen milligrams per kilogram and the oral ibuprofen at five to ten milligrams per kilogram for the mild to the moderate pain, the intravenous morphine or the ketamine for the severe — before the imaging and the orthopaedic referral. The neurovascular status is documented before and after any splinting or reduction. [7]
Management — Definitive & Stepwise
The reduction of the radial head subluxation is the definitive treatment, and the hyperpronation is the preferred first technique. The examiner faces the child, holds the elbow with one hand, and with the other hand grasps the child's wrist and fully pronates the forearm in one smooth, firm, continuous motion, often carrying the wrist into hyperpronation. The manoeuvre is held for a moment, then released. The supination-flexion is the alternative: the forearm is fully supinated and the elbow is fully flexed, with the examiner's thumb pressing over the radial head. The Macias 1998 randomised trial showed that hyperpronation was successful on the first attempt in thirty-nine of forty-one children (ninety-five per cent) compared with thirty-four of forty-four (seventy-seven per cent) for supination, and the Aksel 2025 randomised trial of one hundred and nineteen children confirmed the lower first-attempt failure rate for hyperpronation. [1] [6]
The reduction of the radial head subluxation — the steps
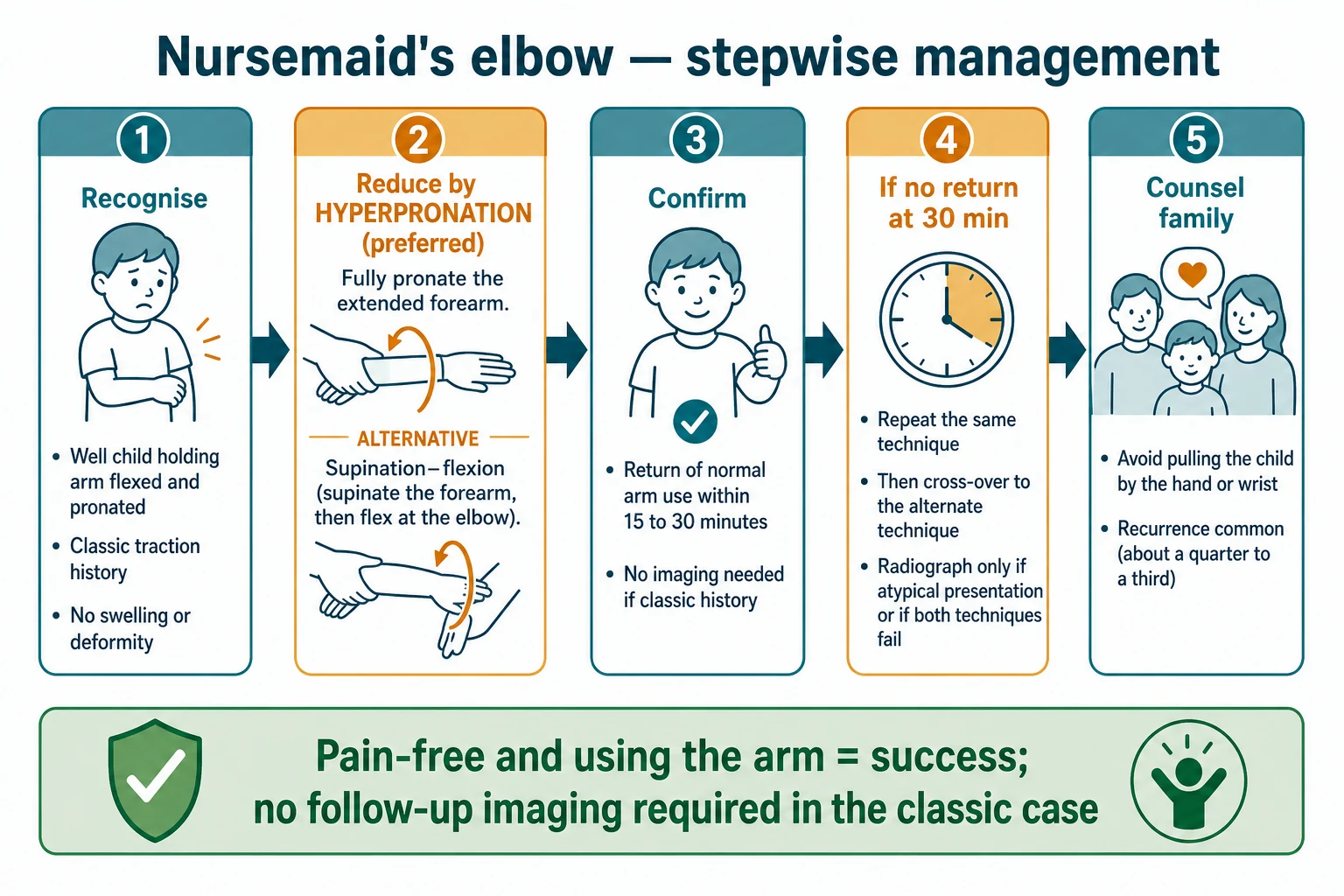
Recognise the pattern: the well child under five, the classic traction history, the arm held flexed and pronated, no swelling, no deformity, no point tenderness. The diagnosis is clinical, and the reduction is attempted before any radiograph.
Reduce by hyperpronation, the preferred first technique: hold the elbow with one hand, grasp the wrist with the other, and fully pronate the extended forearm in one smooth, firm, continuous motion, carrying the wrist into hyperpronation. Hold briefly, then release.
Confirm the success: the child begins to use the arm normally, reaching for a toy, within fifteen to thirty minutes. The return of function is the proof, whether or not a click was felt. No radiograph is needed if the history is classic.
If the arm is not used by thirty minutes, repeat the hyperpronation once, then cross over to the supination-flexion technique: supinate the forearm fully and flex the elbow fully with a thumb over the radial head.
If both techniques fail or the history is atypical, obtain the elbow radiograph to exclude the missed fracture, and reconsider the diagnosis before further attempts.
Counsel the family: lift the child under the axillae, avoid swinging the child by the arms, and hold the hand rather than the wrist, because roughly a quarter to a third of children recur until the annular ligament matures.
The proof of the successful reduction is the return of the normal arm use, not the click. The Quan and Marcuse study showed that when a click is felt or heard, fifty-three of fifty-four children (ninety-eight per cent) regain the use of the arm within thirty minutes, but when no click is felt, four of thirteen (thirty-one per cent) do — so the click is reassuring but not necessary, and the return of the function is the arbiter. The child who does not use the arm within thirty minutes is re-manipulated, and the child who still does not use it after both techniques has the radiograph. The family is counselled at the discharge, and the follow-up is unnecessary in the classic, successfully reduced case. [4] [2]
The management of the common upper-limb fractures is the domain of the orthopaedic team, and the generalist's role is the recognition, the splinting, and the referral. The Gartland I supracondylar fracture is managed in a long-arm splint or a cast for three to four weeks. The Gartland II and III are taken to theatre for the closed reduction and the percutaneous pinning, with the lateral-entry pins preferred to the crossed pins because the Skaggs study showed a lower rate of the iatrogenic ulnar nerve injury. The torus fracture of the distal radius is managed by a soft bandage or a removable splint for three to four weeks, because the FORCE equivalence trial showed the bandage to be no worse than the rigid cast and better tolerated, with the rapid return to function. The clavicle fracture is managed non-operatively by a sling or a figure-of-eight bandage in the great majority, including most angulated and displaced fractures in the young child, with the operative fixation reserved for the completely displaced, shortened shaft fracture in the adolescent, as the FACTS study informed. [7] [8] [9] [11]
Specific Subtypes & Scenarios
The classic radial head subluxation of the one-to-four-year-old is the commonest scenario, and it responds to the hyperpronation in the great majority, with the return of the function within minutes and the discharge with the counselling. The long-term outcome is excellent: the annular ligament matures, the recurrence ceases, and there is no residual deformity, no stiffness, and no long-term sequelae. The family is reassured that the condition is benign and the recurrence is preventable, and the counselling is the single most important element of the disposition. [4] [3]
The recurrent radial head subluxation is the scenario that tests the counselling. Roughly a quarter to a third of children recur, and the recurrence is most common in the year after the first episode, while the annular ligament is still lax. The family is counselled on the avoidance of the traction, the lifting under the axillae, and the holding of the hand rather than the wrist, and the recurrence rate falls. The recurrent subluxation does not warrant any immobilisation, any restriction of activity, or any orthopaedic referral in the typical case, and the family is taught the reduction technique so that the recurrent episode may be managed at home. The recurrence eventually ceases as the ligament matures. [3] [4]
In Australia and Aotearoa New Zealand, the radial head subluxation is managed in the general practice, the emergency department, and the primary care setting, with the reduction performed by the trained clinician and the counselling delivered at the discharge. The outreach clinics and the telehealth support the rural and the remote families, and the recurrent episode may be managed with the telehealth guidance once the family is taught the technique. The common upper-limb fractures are referred to the paediatric orthopaedic services in the major centres, with the regional and the remote children retrieved safely to the centre with the theatre capability. [5] [7]
The supracondylar fracture of the five-to-seven-year-old is the scenario that demands the vascular vigilance. The Gartland III is completely displaced, and the brachial artery may be kinked, entrapped, or torn, with the pulseless, cold, or pale hand as the emergency. The elbow is reduced and stabilised in the emergency department, the hand is re-perfused, and the child is taken to theatre for the closed reduction and the percutaneous pinning, with the vascular surgeon involved if the pulse does not return. The anterior interosseous nerve is the commonest nerve injured, and the nerve function is documented before and after the reduction, with the majority of the nerve palsies recovering spontaneously over weeks to months. [7] [10]
The torus fracture of the distal radius is the scenario that demands the restraint. The FORCE equivalence trial settled the immobilisation debate by showing that a soft bandage was no worse than a rigid below-elbow cast for the torus fracture, with the better function, the less pain, and the more rapid return to the activity. The contemporary ANZ and the UK practice now favours the soft bandage or the removable splint, and the over-immobilisation in a rigid cast for weeks is the overtreatment that the trial was designed to prevent. [9]
The clavicle fracture of the newborn and the young child is the scenario that demands the reassurance. The vast majority of the clavicle fractures, including the angulated and the displaced midshaft fractures, heal with the callus and the remodelling, and the cosmetic and the functional outcome is excellent with the non-operative management by a sling or a figure-of-eight bandage. The operative fixation is reserved for the completely displaced, shortened, or tenting shaft fracture in the adolescent, and the FACTS prospective multicentre study informed the shared decision in this group. [11]
Complications & Pitfalls
The complications of the radial head subluxation itself are few. The recurrence is the commonest, seen in roughly a quarter to a third of the children, and it is managed by the counselling and the home reduction. The failed reduction is the pitfall that demands the radiograph and the reconsideration of the diagnosis, because the missed fracture hides among the unreduced arms. The iatrogenic harm — from the repeated, forceful attempts or the unnecessary radiographs — is avoided by the gentle technique, the limit of two attempts per technique, and the restraint on the imaging in the classic case. [2] [4]
The complications of the supracondylar fracture are the vascular and the nerve injuries and the compartment syndrome. The brachial artery injury, the median and the anterior interosseous nerve palsies, and the Volkmann ischaemic contracture of the forearm are the feared complications of the displaced fracture, and they are prevented by the prompt reduction, the pinning, and the vascular and the nerve documentation before and after. The cubitus varus deformity, the gunstock deformity, is the late complication of the malunion, and it is prevented by the accurate reduction and the pinning. [7] [10]
The complications of the torus and the forearm fractures are few, because the inherent stability and the remodelling potential confer the rapid union. The over-immobilisation in a rigid cast for weeks, with the stiffness and the disuse osteopenia, is the iatrogenic complication that the FORCE soft-bandage evidence was designed to prevent. The malunion of the completely displaced both-bone forearm fracture, with the loss of the rotation, is the complication that the orthopaedic reduction and the fixation prevent, and the remodelling potential of the young child is the principle that guides the acceptance of the angulation. [9] [7]
The pitfall of the missed non-accidental injury is the fracture in the non-mobile infant or the fracture that does not fit the offered mechanism. The safeguard is the safeguarding workup — the skeletal survey, the child-protection referral, and the involvement of the social-paediatrics team — running alongside the treatment of the fracture. The clavicle fracture of the newborn is distinguished from the obstetric brachial plexus palsy by the palpable callus and the radiograph, because both present with the pseudoparalysis of the arm. [5]
Prognosis & Disposition
The prognosis of the radial head subluxation is excellent. The reduction restores the arm to full use within minutes, the recurrence ceases as the annular ligament matures, and there is no residual deformity, no stiffness, and no long-term sequelae. The family is reassured, and the child returns to the full activity immediately. The follow-up is unnecessary in the classic, successfully reduced case, and the family is the safeguard against the recurrence. [4] [3]
The prognosis of the supracondylar fracture is good when the reduction and the pinning are prompt and the neurovascular status is documented and protected. The nerve palsies recover spontaneously in the great majority over weeks to months, and the vascular injuries, when recognised and managed, preserve the limb. The cubitus varus deformity is the cosmetic complication of the malunion, and the functional outcome is determined by the accuracy of the reduction. The prognosis of the torus fracture is excellent, with the rapid union and the full function, and the soft bandage confers the faster return to the activity. The prognosis of the clavicle fracture is excellent, with the callus formation and the remodelling, and the cosmetic outcome is good even in the angulated fracture. [7] [9] [11]
The disposition is shared. The general paediatrician and the emergency clinician own the recognition of the radial head subluxation, the bedside reduction, the counselling, and the discharge. The paediatric orthopaedic surgeon owns the displaced supracondylar fracture, the both-bone forearm fracture, and the operative clavicle fracture. The physiotherapist owns the rehabilitation of the stiffness and the nerve palsy. The general paediatrician is the coordinator of the multidisciplinary care, and the safeguarding team is involved in the non-accidental injury. The long-term follow-up, to the union of the fracture and the recovery of the nerve, is the safeguard. [5] [7]
Special Populations
The child with the recurrent radial head subluxation is managed with the family-centred counselling and the home reduction. The family is taught the hyperpronation technique, and the recurrent episode is managed at home with the telehealth guidance, sparing the child the repeated visits and the radiation. The family is reassured that the recurrence is not a marker of a connective tissue disorder in the typical case, and the recurrence ceases as the ligament matures. The counselling is the single most important element of the disposition in this group. [3] [4]
The child in the rural or the remote setting is managed with the telehealth and the outreach support. The radial head subluxation is reduced locally, with the telehealth guidance for the inexperienced clinician, and the common fractures are splinted and retrieved safely to the centre with the paediatric orthopaedic and the theatre capability. The vascular emergency of the pulseless supracondylar hand is retrieved urgently, because the time-critical injury is measured against the vascular clock, and the telehealth orthopaedic advice guides the reduction and the transfer decision in the interim. [7] [5]
The child with the suspected non-accidental injury enters the safeguarding pathway alongside the treatment of the fracture. The fracture in the non-mobile infant, the fracture that does not fit the offered mechanism, and the presence of the other injuries of different ages together demand the full safeguarding workup — the skeletal survey, the child-protection referral, and the involvement of the social-paediatrics team. The fracture is treated, but the cause is investigated, and the general paediatrician is the coordinator of the safeguarding care. [5]
The child with the disability or the neurodiversity is managed with the adapted communication and the behaviour support. The reduction of the radial head subluxation may require the distraction, the play therapy, or the sedation in the anxious or the uncooperative child, and the family is involved in the positioning and the reassurance. The common fractures are splinted and managed with the attention to the comfort and the ease of the care, and the follow-up is tailored to the child's needs. [5]
Evidence, Guidelines & Regional Differences
The Macias 1998 randomised trial in Pediatrics, "A comparison of supination/flexion to hyperpronation in the reduction of radial head subluxations," is the foundational evidence for the preferred technique. The trial enrolled ninety children under six, and the hyperpronation was successful on the first attempt in thirty-nine of forty-one (ninety-five per cent) compared with thirty-four of forty-four (seventy-seven per cent) for the supination; overall, hyperpronation succeeded in forty of forty-one (ninety-seven and a half per cent) versus thirty-eight of forty-four (eighty-six per cent). The trial concluded that the hyperpronation required fewer attempts, was successful more often, and was successful when the supination failed, and it established the hyperpronation as the preferred first technique. [1]
The Aksel 2025 randomised trial in the American Journal of Emergency Medicine confirmed and extended the finding. The trial enrolled one hundred and nineteen children aged six years and under, and the first-attempt failure rate was nine point eight per cent for the hyperpronation versus twenty-four point two per cent for the supination-flexion, a risk ratio of zero point four one favouring the hyperpronation. The trial found no difference in the second-attempt success, the ultimate failure, the procedural pain, the side effects, or the recurrence within seventy-two hours, and it recommended the hyperpronation as the preferred initial treatment. The two trials, twenty-seven years apart, converge on the same conclusion: the hyperpronation is the first technique. [6]
Macias 1998 — hyperpronation versus supination/flexion for radial head subluxation
Prospective randomised study of 90 children younger than 6 years with a clinical diagnosis of radial head subluxation, comparing the two reduction techniques, with a cross-over after a failed technique.
Key finding
Hyperpronation was successful on the first attempt in 39 of 41 children (95 per cent) versus 34 of 44 (77 per cent) for supination, and overall in 40 of 41 (97.5 per cent) versus 38 of 44 (86 per cent). Of the 6 patients who crossed over from supination to hyperpronation, 5 were reduced on the first attempt.
The Krul 2017 Cochrane review, "Manipulative interventions for reducing pulled elbow in young children," appraised the evidence for the two techniques and the recurrence, and it confirmed the higher success of the hyperpronation with the moderate-quality evidence, while noting the need for the larger trials that the Aksel 2025 subsequently provided. The Macias 2000 study, "History and radiographic findings associated with clinically suspected radial head subluxations," is the evidence for the selective use of the radiograph: the non-classic history raises the relative risk of the fracture, and the radiograph is reserved for the atypical and the unreduced case. The Quan and Marcuse 1985 study is the evidence for the click and the return of function, and for the epidemiology and the recurrence. [3] [2] [4]
The evidence for the common upper-limb fractures is anchored in the supracondylar and the forearm literature. The Howard 2012 and the Mulpuri 2015 reviews frame the supracondylar management and the prognosis, with the Gartland grade and the lateral-entry pinning as the standard. The Skaggs 2001 study, "Operative treatment of supracondylar fractures of the humerus in children. The consequences of pin placement," showed that the lateral-entry pins carry the lower rate of the iatrogenic ulnar nerve injury than the crossed pins, and established the lateral entry as the preferred configuration. The Perry 2022 FORCE equivalence trial settled the torus fracture immobilisation debate by showing the soft bandage to be no worse than the rigid cast, and the Heyworth 2022 FACTS prospective multicentre study informed the operative-versus-nonoperative decision for the displaced midshaft clavicle fracture in the adolescent. [7] [10] [8] [9] [11]
The regional differences are modest. The AAOS, the Royal Children's Hospital Melbourne, and the contemporary ANZ and the UK practice frame the radial head subluxation and the common-fracture management, with the hyperpronation as the first technique and the soft bandage for the torus fracture. The practice in some regions still defaults to the supination-flexion and the rigid cast, but the randomised evidence and the guideline updates converge on the hyperpronation and the bandage. The safeguarding pathway is the universal standard for the fracture in the non-mobile infant. [1] [9]
Exam Pearls
The fellowship answer turns on five facts. The first is the traction history and the well child holding the arm flexed and pronated — the classic pattern that needs no radiograph. The second is the hyperpronation as the preferred first reduction technique, on the evidence of the Macias 1998 and the Aksel 2025 randomised trials, with the supination-flexion as the alternative. The third is the return of the normal arm use within fifteen to thirty minutes as the proof of the success, and the radiograph reserved for the atypical and the unreduced case. The fourth is the counselling to prevent the recurrence, because roughly a quarter to a third recur. The fifth is the Gartland grade for the supracondylar fracture, with the lateral-entry pinning and the vascular vigilance for the pulseless hand. [1] [7]
The three examiner traps are the following. The first is the radiograph taken before the reduction in the classic case — the unnecessary radiation that delays the cure, when the diagnosis is clinical and the reduction precedes the imaging. The second is the atypical guarding arm reduced without the radiograph — the missed lateral condyle or supracondylar fracture that the Macias 2000 study warned of, demanding the radiograph when the history does not fit. The third is the torus fracture over-immobilised in a rigid cast for weeks, when the FORCE trial showed the soft bandage to be no worse and better tolerated. The candidate who names these three traps and their safeguards demonstrates the pattern-level thinking the fellowship rewards. [2] [9]
The examiner rewards the candidate who frames the upper-limb injury around the pattern recognition, the bedside reduction, and the safeguarding duty. The traction-injured, well child is reduced at the chairside without imaging; the fall-injured, swollen child is splinted, imaged, and referred; and the fracture in the non-mobile infant is investigated, not just treated. This three-part framing — reduce, splint-and-refer, safeguard — is the fellowship answer in miniature. [4] [5]
Which reduction technique do you use first for nursemaid's elbow, and why?
The hyperpronation, on the evidence of the two randomised trials. The Macias 1998 trial showed the first-attempt success of ninety-five per cent for the hyperpronation versus seventy-seven per cent for the supination-flexion, and the Aksel 2025 trial showed the first-attempt failure rate of nine point eight per cent versus twenty-four point two per cent, a risk ratio of zero point four one favouring the hyperpronation. Both trials recommend the hyperpronation as the preferred initial technique. The forearm is fully pronated in one smooth, firm motion, and the return of the normal arm use within fifteen to thirty minutes is the proof. [1] [6]
References
- [1]Macias CG, Bothner J, Wiebe R. A comparison of supination/flexion to hyperpronation in the reduction of radial head subluxations. Pediatrics, 1998.PMID 9651462
- [2]Macias CG, Wiebe R, Bothner J. History and radiographic findings associated with clinically suspected radial head subluxations. Pediatric Emergency Care, 2000.PMID 10698138
- [3]Krul M, van der Wouden JC, Kruithof EJ, van Suijlekom-Smit LW. Manipulative interventions for reducing pulled elbow in young children. Cochrane Database of Systematic Reviews, 2017.PMID 28753234
- [4]Quan L, Marcuse EK. The epidemiology and treatment of radial head subluxation. American Journal of Diseases of Children, 1985.PMID 4061421
- [5]Schutzman SA, Teach S. Upper-extremity impairment in young children. Annals of Emergency Medicine, 1995.PMID 7574131
- [6]Aksel G, Küka B, İslam MM, Demirkapı F, Öztürk İ, İşlek OM, Ademoğlu E, Eroğlu SE, Satıcı MO, Özdemir S. Comparison of supination/flexion maneuver to hyperpronation maneuver in the reduction of radial head subluxations: A randomized clinical trial. American Journal of Emergency Medicine, 2025.PMID 39579408
- [7]Howard A, Mulpuri K, Abel MF, Braun S, Broom A, Copley LA, et al. Management of supracondylar humerus fractures in children: current concepts. Journal of the American Academy of Orthopaedic Surgeons, 2012.PMID 22302444
- [8]Skaggs DL, Hale JM, Bassett J, Kaminsky C, Kay RM, Tolo VT. Operative treatment of supracondylar fractures of the humerus in children. The consequences of pin placement. Journal of Bone and Joint Surgery. American Volume, 2001.PMID 11379744
- [9]Perry DC, Achten J, Knight R, Tong J, Jackson K, Bruce G, et al. Offer of a bandage versus rigid immobilisation in 4- to 15-year-olds with distal radius torus fractures: the FORCE equivalence RCT. Health Technology Assessment, 2022.PMID 35904496
- [10]Mulpuri K, Wilkins K. Supracondylar humeral fractures in children: current concepts for management and prognosis. International Orthopaedics, 2015.PMID 26311512
- [11]Heyworth BE, Pennock AT, Li Y, Stitzski M, Bae DS, Endres NK, et al. Two-Year Functional Outcomes of Operative vs Nonoperative Treatment of Completely Displaced Midshaft Clavicle Fractures in Adolescents: Results From the Prospective Multicenter FACTS Study Group. American Journal of Sports Medicine, 2022.PMID 35984091