Paeds · rheumatology-musculoskeletal-and-sports
Osteomyelitis and discitis
Also known as acute haematogenous osteomyelitis · AHO · paediatric bone infection · Kingella kingae osteomyelitis · spondylodiscitis · discitis · vertebral osteomyelitis in children · subperiosteal abscess
A fellowship approach to paediatric acute haematogenous osteomyelitis and discitis: the metaphyseal capillary bed where bacteria seed, the age-stratified microbiology dominated by Kingella kingae under four years and Staphylococcus aureus at all ages, magnetic resonance imaging as the diagnostic gold standard, and the evidence-based intravenous-to-oral antibiotic switch strategy that shortens hospital stays without compromising cure.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A two-year-old boy is brought in with three days of fever and a refusal to walk. He holds his left leg still and cries when you palpate the distal tibial metaphysis. His C-reactive protein is 85 milligrams per litre, his white cell count is 16,000, and his blood culture grows Kingella kingae on day three. The magnetic resonance image shows marrow oedema in the distal tibia with a small subperiosteal collection, and he improves within forty-eight hours of intravenous cefazolin. He switches to oral amoxicillin-clavulanate at day five, completes a four-week course, and recovers fully. A four-year-old girl refuses to sit and holds her back rigid, with an erythrocyte sedimentation rate of 60 — discitis until the magnetic resonance image reveals high signal in two adjacent vertebral bodies and the intervening disc. [1] [9]
The five moves — Suspect, Culture, Image, Treat, Switch
Overview & Definition
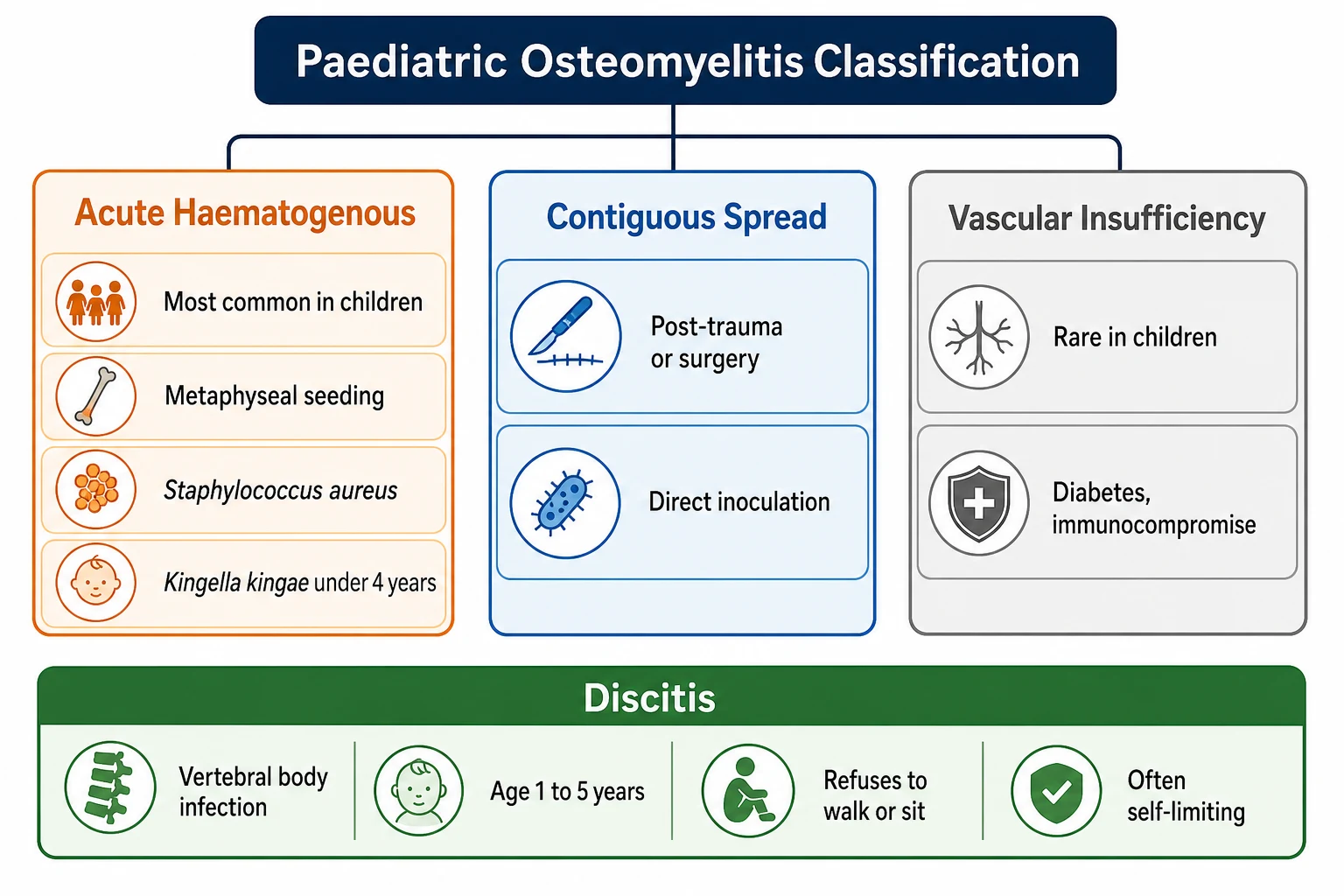
Acute haematogenous osteomyelitis is a bacterial infection of bone that reaches the skeleton through the bloodstream rather than by contiguous spread or direct inoculation. In children, it is the commonest form of bone infection, and it arises because the rich capillary network of the growing metaphysis creates a slow-flowing, low-oxygen environment in which bacteria can lodge and multiply. The haematogenous route distinguishes it from contiguous osteomyelitis, which follows trauma or surgery, and from the vascular-insufficiency pattern seen rarely in children. [2] [11]
The clinical syndrome is defined by the triad of fever, focal bone pain, and functional impairment. In the pre-verbal child, the pain manifests as pseudoparalysis — the child simply stops using the limb — and in the ambulant child, it manifests as a limp or a refusal to bear weight. The pain is typically well localised to the metaphysis of a long bone, most often the tibia or the femur, and it is constant, progressive, and unrelated to activity. The systemic features — fever, malaise, irritability — may precede the localising pain by a day or two, which is why the febrile child with an apparent limb problem is assessed with osteomyelitis in the differential from the outset. [2] [4]
Discitis, or spondylodiscitis, is the vertebral analogue of acute haematogenous osteomyelitis, and it affects the disc space and the adjacent vertebral bodies in children aged one to five years. The presentation is distinctive — a toddler who refuses to walk, sit, or crawl, holds the spine rigid, and may complain of abdominal or back pain — and the diagnosis is confirmed by magnetic resonance imaging. Discitis is often a milder, more self-limiting infection than long-bone osteomyelitis, but the potential for spinal cord compression and permanent neurological injury demands the same urgency of diagnosis and imaging. [9] [10]
Classification
Paediatric osteomyelitis is classified by route of infection, by duration, and by the presence or absence of complications. The route of infection is the primary classifier because it determines the microbiology, the clinical course, and the management. Acute haematogenous osteomyelitis accounts for the great majority of paediatric bone infections, and it arises when bacteria transiently present in the bloodstream lodge in the metaphyseal capillaries. Contiguous-focus osteomyelitis follows penetrating trauma, open fractures, or surgery, and the microbiology reflects the skin and environmental organisms introduced at the time of injury. Chronic osteomyelitis, defined by symptoms lasting more than six weeks, may follow inadequately treated acute infection and is characterised by necrotic bone, or sequestra, that harbour bacteria and sustain the infection. [2] [11]
The anatomical classification distinguishes uncomplicated from complicated disease, and this distinction drives both the surgical and the antibiotic strategy. Uncomplicated osteomyelitis involves the bone without a drainable collection, and it responds to antibiotics alone in the great majority of cases. Complicated osteomyelitis includes subperiosteal abscess, intraosseous abscess, septic arthritis of the adjacent joint, pathologic fracture, and chronic infection with sequestrum formation, and these subtypes require surgical intervention in addition to antibiotics. The 2021 Pediatric Infectious Diseases Society and Infectious Diseases Society of America guideline makes this distinction central to the management algorithm, because the presence of a drainable collection is the single most important reason for surgical referral. [1] [4]
Discitis is classified separately from long-bone osteomyelitis because it has a distinct epidemiology, microbiology, and clinical course. Pyogenic spondylodiscitis in children is most often caused by Staphylococcus aureus or Kingella kingae, it affects the lumbar spine preferentially, and it runs a more indolent course than long-bone disease. The classification also distinguishes discitis from vertebral osteomyelitis proper, in which the infection is confined to the vertebral body without disc involvement, and from epidural abscess, which is the neurological emergency that demands urgent surgical decompression. [9] [10]
Epidemiology & Risk Factors
Acute haematogenous osteomyelitis is one of the commonest serious bacterial infections of childhood, with an incidence of approximately one in five thousand children per year in high-income settings. The peak incidence is in children under five years, reflecting both the vulnerability of the rapidly growing metaphyseal circulation and the frequency of bacteraemia from mucosal colonisation in this age group. Boys are affected more often than girls, with a ratio of roughly two to one, and the long bones of the lower limb — the tibia and the femur — are the most frequently involved sites. [2] [4]
The microbiology is age-stratified, and this is the single most important epidemiological fact for the fellowship candidate. Staphylococcus aureus is the leading cause across all paediatric ages, accounting for 70 to 90 per cent of cases in most series. Kingella kingae is the second most common cause overall and the leading cause in children under four years, where it may account for up to half of culture-confirmed cases when sensitive molecular methods are used. Group A Streptococcus and Streptococcus pneumoniae contribute a smaller share, and in unimmunised or immunocompromised children, Haemophilus influenzae type b and other organisms enter the differential. [6] [7]
The risk factors for osteomyelitis include preceding viral upper respiratory infection, which disrupts mucosal barriers and predisposes to transient bacteraemia, and this is particularly relevant to Kingella kingae, which colonises the pharynx and is transmitted via the respiratory route. Immunocompromise, indwelling venous catheters, chronic skin conditions such as atopic dermatitis, and sickle cell disease are further risk factors that broaden the microbiological differential. In Indigenous and remote communities, the incidence of osteoarticular infection is substantially higher than in urban populations, reflecting both the burden of skin and soft-tissue infection and the challenges of timely access to care. [4] [8]
Pathophysiology
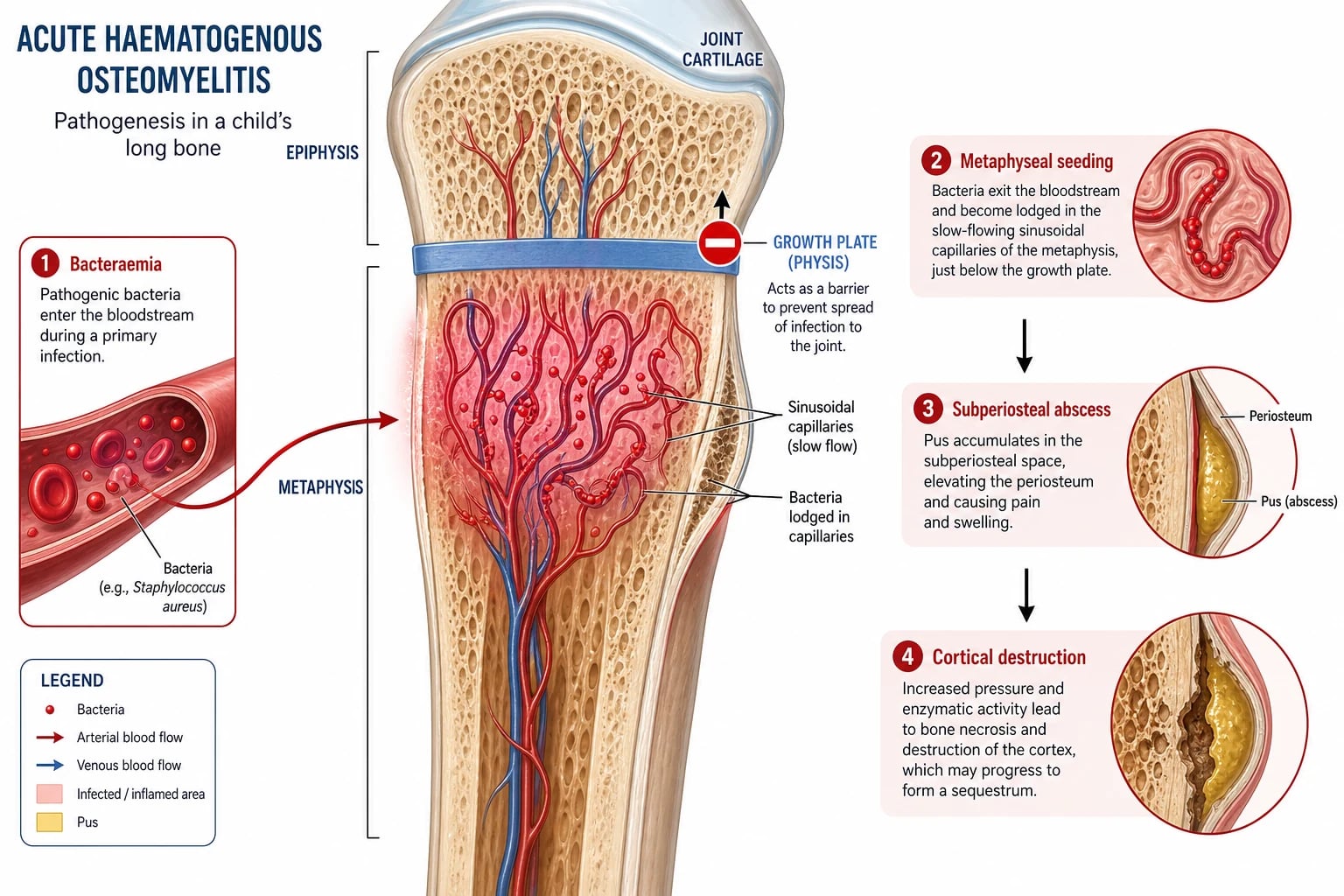
The pathophysiology of acute haematogenous osteomyelitis is rooted in the unique vascular anatomy of the growing child's bone. The metaphysis is supplied by terminal capillary loops that arise from the nutrient artery, turn sharply at the growth plate, and drain into the metaphyseal venous sinusoids. This hairpin turn creates a zone of slow, turbulent blood flow and low oxygen tension — an ideal environment for bacteria to lodge and multiply. The bacteria that arrive via the bloodstream are trapped in these sinusoids, where they evade clearance, replicate, and initiate the inflammatory cascade that defines osteomyelitis. [2] [11]
Once established, the infection spreads along predictable anatomical lines. The bacteria provoke an acute inflammatory response, neutrophils infiltrate the marrow space, and the resulting oedema and pus raise the intraosseous pressure, compressing the venous outflow and eventually the arterial supply. The pus tracks through the Haversian and Volkmann canals of the cortex, reaches the subperiosteal space, and lifts the periosteum to form a subperiosteal abscess. In infants under approximately eighteen months, the transphyseal blood vessels cross the growth plate and allow the infection to spread into the adjacent epiphysis and joint, producing a combined osteomyelitis and septic arthritis that is uncommon in older children, in whom the growth plate acts as a barrier. [5] [11]
The necrosis of bone is the critical event that converts acute osteomyelitis into a disease that may become chronic. As the intraosseous pressure rises and the blood supply is compromised, segments of cortical bone die and become separated from the living bone as sequestra. These avascular fragments are inaccessible to antibiotics and to immune cells, and they serve as a reservoir for persistent infection. Meanwhile, the elevated periosteum lays down new bone — the involucrum — around the infected area, and the radiographic combination of sequestrum and involucrum is the hallmark of chronic osteomyelitis. The pathophysiology of discitis differs in that the infection begins in the vascularised disc and the adjacent vertebral endplates, where the rich capillary network is vulnerable to haematogenous seeding in the young child. [5] [9]
Clinical Presentation
The presentation of acute haematogenous osteomyelitis is shaped by the age of the child, the site of infection, and the virulence of the organism. In the ambulant child, the classical presentation is acute onset of fever with focal bone pain at the metaphysis of a long bone, refusal to bear weight, and a protective posture of the affected limb. The tibia and the femur together account for the majority of cases, followed by the humerus, the fibula, and the calcaneus. The pain is constant, progressive, and worse with any movement, and the child holds the limb immobile. Local examination reveals warmth, swelling, and exquisite tenderness over the affected metaphysis, and the overlying skin may be erythematous in advanced cases. [2] [4]
In the infant and the pre-verbal toddler, the presentation is less specific and the diagnosis is harder. The child may present with fever, irritability, and pseudoparalysis — a failure to move the affected limb that may be mistaken for a neurological problem or for non-accidental injury. The infant may cry when handled or when the limb is moved during a nappy change, and the parent may report that the child has stopped using one arm or leg. A high index of suspicion is essential, and any febrile infant with a painful-looking limb or a refusal to move receives a full examination of all limbs and the spine, with palpation of each metaphysis for localised tenderness. [4] [11]
Discitis presents with a distinctive cluster of symptoms in the toddler. The child, typically aged one to five years, refuses to walk, sit, or crawl, holds the spine rigid, and may present with a limp, a refusal to stand, or abdominal pain that mimics an intra-abdominal process. The older child may localise the pain to the back. Fever may be low-grade or absent, and the inflammatory markers may be only mildly elevated, which can delay the diagnosis. The examination reveals a child who resists spinal movement, holds a rigid posture, and cries when the spine is palpated. Any toddler with unexplained refusal to walk or sit, or with back pain, receives a magnetic resonance image of the spine to exclude discitis and epidural abscess. [9] [10]
Kingella kingae osteomyelitis deserves a specific mention because its presentation is milder and more deceptive than that caused by Staphylococcus aureus. Children with Kingella kingae infection often have lower fevers, lower inflammatory markers, and a more subacute presentation, and they may have concomitant or recent upper respiratory symptoms, stomatitis, or diarrhoea. The milder inflammatory response can lead to delayed investigation and delayed treatment, and it is the reason the fellowship answer stresses a low threshold for blood culture and molecular diagnostics in children under four years with any clinical suspicion of bone infection. [6] [7]
Which reassuring-sounding presentations must never close the search? A child with a limp and a low-grade fever may still have osteomyelitis, and the inflammatory markers, not the temperature alone, guide the workup. A child with an apparently minor injury may have osteomyelitis masquerading as trauma, and the history of a fall does not exclude a bone infection. A child with normal initial radiographs has not been cleared, because the plain film is insensitive in the first one to two weeks. And a child with improving pain on oral analgesia may still harbour a subperiosteal abscess that needs surgical drainage. [1] [4]
Differential Diagnosis
The differential diagnosis of the febrile child with a painful limb spans trauma, infection, inflammation, and malignancy, and the fellowship candidate must hold these in parallel rather than sequentially. Trauma — accidental and non-accidental — produces focal pain and tenderness, and a toddler's fracture or a spiral tibial fracture may mimic osteomyelitis. The history of injury, the radiographic findings, and the absence of fever and systemic inflammation point toward trauma, but the distinction is not always clean, and osteomyelitis may coexist with or follow a minor injury. [4] [2]
Septic arthritis is the closest mimic and the most important one to distinguish, because both present with fever, pain, and a refusal to use the limb, and both may coexist when the infection crosses the growth plate in the infant. Septic arthritis typically produces more joint-centred findings — a held joint in the position of maximum capsular volume, extreme pain on any movement through the joint range — whereas osteomyelitis produces more metaphyseal-centred tenderness. The Kocher prediction rule helps to risk-stratify the irritable hip, but when the two conditions overlap, magnetic resonance imaging distinguishes them. Transient synovitis is the benign mimic that resolves with rest, and it is distinguished by the absence of high fever, the ability to bear weight, and near-normal inflammatory markers. [4] [11]
The malignant mimics must never be missed. Leukaemia may present with bone pain, fever, and limp, and the full blood count may reveal cytopenias, blasts, or an unexplained elevation in the lactate dehydrogenase. Bone tumours — osteosarcoma and Ewing sarcoma — peak in adolescence and produce progressive, unrelenting pain that is often worse at night, and the radiograph may show a destructive lesion with periosteal reaction. Langerhans cell histiocytosis may produce a lytic lesion that mimics osteomyelitis. In the limping child who does not fit the pattern of osteomyelitis or whose inflammatory markers are paradoxically low, these diagnoses are actively sought through the blood film, the lactate dehydrogenase, and the bone imaging. [4] [2]
Clinical & Bedside Assessment
The bedside assessment begins with the general appearance and the vital signs, because the febrile, toxic, or irritable child may be septicaemic as well as having a localised bone infection. The temperature, the heart rate, the capillary refill, and the overall tone of the child are noted, and the child in septic shock is resuscitated before the local examination proceeds. The history focuses on the onset, the progression, and the site of the pain; the presence or absence of fever; any preceding viral illness, trauma, or skin infection; and the immunisation status. A history of a recent upper respiratory infection, stomatitis, or diarrhoea in a child under four years raises the specific suspicion of Kingella kingae. [2] [6]
The limb examination is systematic and unhurried. Each limb is inspected for swelling, erythema, and deformity, palpated for warmth and tenderness, and moved gently through the range of the adjacent joints. The site of maximum tenderness is localised — typically the metaphysis of a long bone — and the presence of a joint effusion, which suggests concomitant septic arthritis, is sought. In the infant, the examination relies on observation of spontaneous movement, palpation of each limb for tenderness, and gentle passive movement to detect guarding. The spine is examined in any child with back pain, refusal to walk, or a rigid posture, and the finding of spinal tenderness or a refusal to flex the spine prompts urgent magnetic resonance imaging. [4] [11]
The inflammatory markers are the bedside laboratory backbone of the assessment. The C-reactive protein is the most useful individual marker because it rises rapidly, it correlates with disease severity, and it falls predictably with effective treatment, making it the single most important parameter for monitoring the response to therapy. The erythrocyte sedimentation rate rises more slowly and falls more slowly, and it is a useful adjunct that is less practical for day-to-day monitoring. The white blood cell count is elevated in roughly one-third of cases and is the least sensitive of the three markers. Blood cultures are obtained before antibiotics, and they are positive in 30 to 50 per cent of cases — a yield that is higher with Kingella kingae when sensitive culture methods are used. [1] [3]
Which findings must never be dismissed? A child with a high C-reactive protein, a febrile illness, and focal bone tenderness has osteomyelitis until a magnetic resonance image proves otherwise. A child who fails to improve within forty-eight to seventy-two hours of appropriate intravenous antibiotics has a complication — a drainable abscess, a resistant organism, or an alternative diagnosis — and the imaging and the microbiology are revisited. And a toddler who refuses to walk and holds the spine rigid has discitis or epidural abscess until the magnetic resonance image of the spine is reviewed. [1] [9]
Investigations
The investigation of suspected paediatric osteomyelitis is built around blood tests, cultures, and imaging, and the magnetic resonance image is the centrepiece. Blood tests include the full blood count, the C-reactive protein, and the erythrocyte sedimentation rate, and blood cultures are drawn before antibiotics are started. A positive blood culture — obtained in 30 to 50 per cent of cases — provides the microbiological diagnosis and spares the child a bone biopsy. In children under four years, a blood culture or a polymerase chain reaction assay that specifically targets Kingella kingae increases the diagnostic yield, because this fastidious organism is easily missed on routine culture. [1] [6]
Plain radiographs are the first imaging study, but their role is to exclude fracture, tumour, and other mimics rather than to confirm osteomyelitis. The radiographic signs of osteomyelitis — soft-tissue swelling, periosteal reaction, and cortical lucency — do not appear until seven to fourteen days into the illness, and a normal early radiograph does not exclude the diagnosis. When the clinical suspicion is high, the radiograph is immediately followed by magnetic resonance imaging, which is the gold standard. The magnetic resonance image reveals marrow oedema as low signal on T1-weighted and high signal on T2-weighted sequences, it defines the extent of the infection, and it identifies the subperiosteal or intraosseous abscess that demands surgical drainage. [5] [4]
The magnetic resonance imaging protocol for suspected osteomyelitis includes T1-weighted, T2-weighted, and post-gadolinium T1-weighted sequences, and it covers the entire affected bone and the adjacent joint to detect concomitant septic arthritis. The gadolinium enhancement is critical because it distinguishes the vascularised, inflamed tissue from the non-enhancing, necrotic pus within an abscess cavity. The sensitivity of magnetic resonance imaging for osteomyelitis exceeds 90 per cent, and it is the investigation that definitively confirms or excludes the diagnosis in the child with a normal radiograph but a high clinical suspicion. Ultrasound has a limited role — it may detect a subperiosteal collection or a joint effusion, and it can guide aspiration — but a negative ultrasound does not exclude osteomyelitis, because the infection may be confined to the marrow. [5] [1]
Management — Resuscitation
Resuscitation is the first priority in the child who presents with sepsis or septic shock alongside the bone infection. The airway, breathing, and circulation are assessed and stabilised, intravenous access is obtained, and fluid resuscitation is given to the child in shock. Blood cultures are drawn before the first dose of antibiotics, but the antibiotics are not delayed for cultures — a single set of cultures followed by immediate empirical intravenous therapy is the correct sequence in the unwell child. The empirical antibiotic is chosen to cover the age-stratified organisms, and it is given at full dose intravenously as soon as possible after the cultures. [1] [8]
The empirical antibiotic regimen is guided by the age of the child and the local resistance patterns, and the 2021 Pediatric Infectious Diseases Society and Infectious Diseases Society of America guideline provides the framework. For children of all ages, an anti-staphylococcal agent is the backbone of empirical therapy — a first-generation cephalosporin such as cefazolin, or clindamycin where local methicillin-resistant Staphylococcus aureus rates are high, or vancomycin where methicillin resistance or severe sepsis warrants it. For children under four years, coverage for Kingella kingae is added, and because Kingella kingae is a gram-negative organism that is susceptible to beta-lactams, a third-generation cephalosporin such as ceftriaxone is often added to or substituted for the regimen in this age group. The regimen is refined when the culture and sensitivity results return. [1] [11]
The surgical assessment runs in parallel with the antibiotic resuscitation, because a subperiosteal or intraosseous abscess demands surgical drainage and cannot be cured by antibiotics alone. The magnetic resonance image is reviewed by the orthopaedic team as soon as it is available, and the decision to operate is based on the presence, size, and accessibility of the drainable collection. The general paediatrician's role is to ensure the cultures are drawn, the antibiotics are started, the imaging is obtained, and the surgical and infectious-diseases teams are involved early and together. [8] [4]
Management — Definitive & Stepwise
The definitive management of uncomplicated acute haematogenous osteomyelitis is intravenous antibiotics followed by an early switch to oral therapy, and this intravenous-to-oral strategy is the evidence-based standard that has transformed the treatment of this disease. The child is treated with intravenous antibiotics until the clinical and laboratory criteria for the oral switch are met — typically three to five days — and then the therapy is completed orally. The 2021 guideline and the UK consensus guidelines both endorse this approach, and the randomised feasibility data from de Graaf and colleagues demonstrated that a short intravenous course followed by oral therapy is safe and acceptable to families. [1] [8] [12]
The criteria for the intravenous-to-oral switch are the centrepiece of the modern management algorithm, and the fellowship candidate must state them precisely. The switch is made when the child is afebrile, when the clinical signs are improving — less pain, less swelling, willing to bear weight or use the limb — and when the C-reactive protein is falling, typically by at least 50 per cent from its peak. The oral antibiotic must be well absorbed, achieve adequate serum levels, and be acceptable to the child. For Staphylococcus aureus, first-generation oral cephalosporins such as cephalexin, or clindamycin, are commonly used; for Kingella kingae, oral amoxicillin or amoxicillin-clavulanate is effective, because the organism is reliably susceptible to beta-lactams. [1] [3]
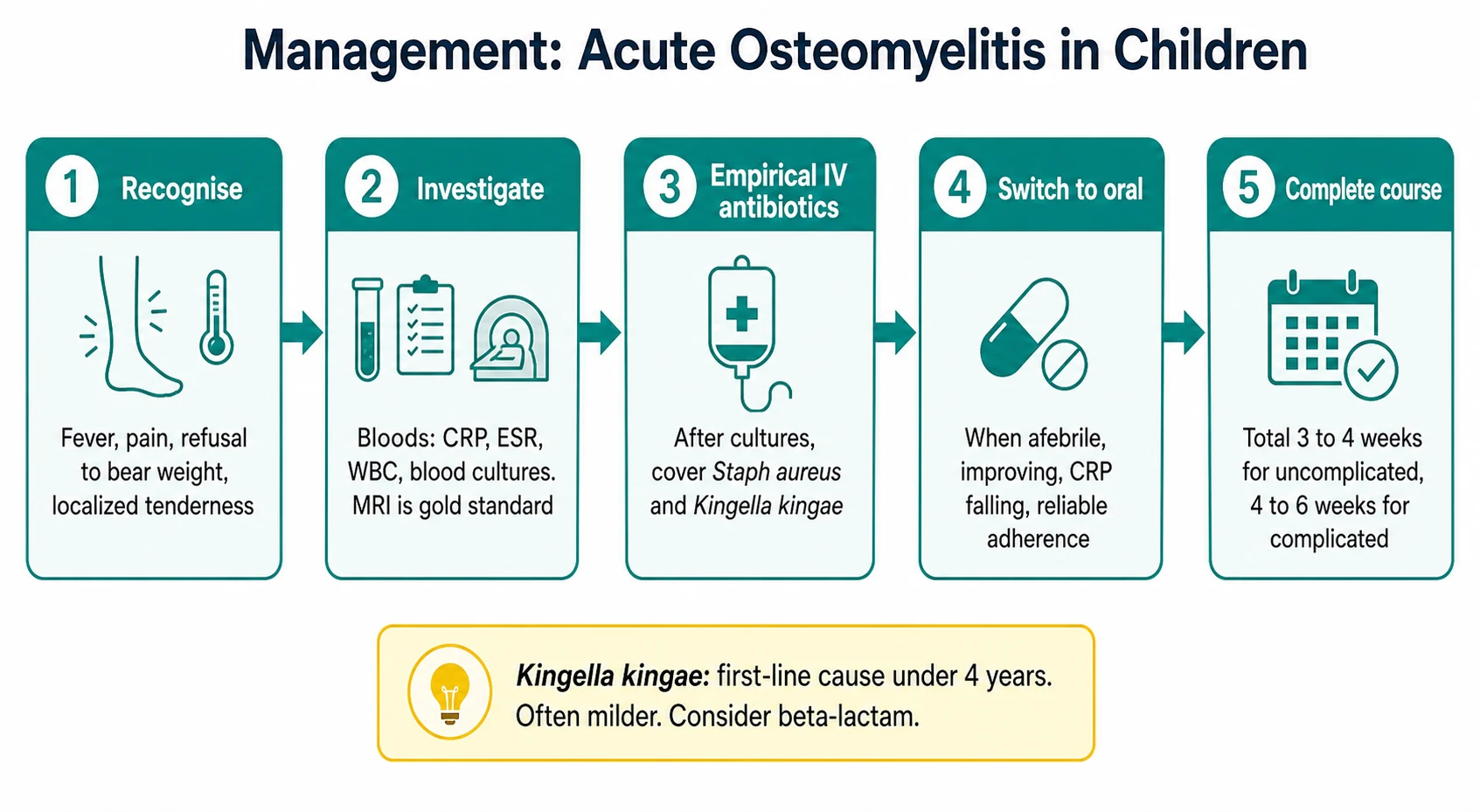
The total duration of antibiotic therapy is three to four weeks for uncomplicated acute haematogenous osteomyelitis and four to six weeks for complicated disease, including cases with abscess, septic arthritis, or slow clinical response. The duration is guided by the clinical course and the C-reactive protein trend, and the trend is more important than any fixed calendar. A child whose C-reactive protein has normalised and who is clinically well may complete the course earlier, while a child with persistent elevation or slow improvement is treated longer. The traditional approach of four to six weeks of intravenous therapy for every child has been replaced by this individualised, response-guided strategy, and the evidence demonstrates equivalent outcomes with shorter intravenous courses and lower rates of line-related complications. [3] [12]
The management of discitis follows the same principles but with some differences. Discitis is often a milder infection that may resolve with a shorter course of antibiotics — typically two to four weeks — and the empirical regimen covers Staphylococcus aureus and Kingella kingae as for long-bone osteomyelitis. Immobilisation and analgesia are important supportive measures in the acute phase, and the child is monitored for signs of neurological compromise that would indicate epidural abscess or spinal cord compression and demand urgent surgical decompression. The majority of children with discitis recover fully with medical management, and surgical intervention is reserved for the minority with abscess, cord compression, or failure of medical therapy. [9] [10]
The intravenous-to-oral switch criteria
Specific Subtypes & Scenarios
Neonatal osteomyelitis is a distinct subtype with a unique pathophysiology and microbiology. In the neonate, the transphyseal blood vessels cross the growth plate, and the infection can spread from the metaphysis into the epiphysis and the adjacent joint, producing a combined osteomyelitis and septic arthritis that is rare in older children. The microbiology of neonatal osteomyelitis includes group B Streptococcus, Escherichia coli, and Staphylococcus aureus, and the empirical regimen must cover all three. The neonate may present with pseudoparalysis, irritability, and refusal to feed rather than with the classical fever and localised pain, and a high index of suspicion is essential. [11] [4]
Kingella kingae osteomyelitis is the subtype that defines the under-four age group and that is increasingly recognised with improved diagnostic methods. Kingella kingae is a fastidious gram-negative coccobacillus that colonises the pharynx of young children and causes transient bacteraemia that seeds the metaphyseal capillaries. The infection it produces is characteristically milder than staphylococcal osteomyelitis, with lower fevers, lower inflammatory markers, and a more subacute presentation, and it is frequently accompanied by upper respiratory, oral, or gastrointestinal symptoms. The organism is susceptible to beta-lactam antibiotics, and the diagnosis is confirmed by blood culture using enriched media or by nucleic-acid amplification assays. The fellowship answer always includes Kingella kingae in the microbiological differential of any child under four years with suspected osteomyelitis. [6] [7]
Chronic osteomyelitis and chronic recurrent multifocal osteomyelitis are the subtypes that complicate the acute disease or present independently. Chronic osteomyelitis follows inadequately treated acute infection, and it is characterised by sequestrum formation, sinus tracts, and persistent or recurrent symptoms. The management is surgical — debridement of the necrotic bone — combined with prolonged, targeted antibiotic therapy. Chronic recurrent multifocal osteomyelitis is a non-infectious, autoinflammatory bone disease that presents with recurrent episodes of bone pain and radiographic changes in multiple sites, and it is distinguished from infectious osteomyelitis by the absence of a causative organism and by its relapsing-remitting course. [4] [2]
Discitis is the subtype that affects the spine. The child is typically one to five years old, presents with refusal to walk or sit, and holds the spine rigid. The magnetic resonance image reveals high signal in two adjacent vertebral bodies and the intervening disc, and blood cultures may identify the organism. The management is empirical antibiotics covering Staphylococcus aureus and Kingella kingae, immobilisation, and analgesia, and the majority of children recover without surgical intervention. The critical complication is epidural abscess with cord compression, which presents with neurological signs and demands urgent surgical decompression. [9] [10]
Complications & Pitfalls
The complications of acute haematogenous osteomyelitis span the bone, the joint, and the child's growth. The growth plate may be damaged by the infection or by the raised intraosseous pressure, producing a growth disturbance that ranges from a mild limb-length discrepancy to a major angular deformity. The younger the child, the greater the growth potential that is at risk, and a physeal injury in an infant has a greater long-term consequence than the same injury in an adolescent. Avascular necrosis of the bone, pathologic fracture through the weakened cortex, and premature osteoarthritis of the adjacent joint are the further complications that follow severe or delayed disease. [4] [5]
The transition from acute to chronic osteomyelitis is the complication that most often follows inadequate or delayed treatment. The formation of sequestra — avascular fragments of necrotic bone that harbour bacteria and are inaccessible to antibiotics and immune cells — sustains the infection and demands surgical removal. The involucrum, the new bone laid down around the infection, further isolates the sequestrum, and the radiographic combination of the two is the hallmark of chronic disease. The prevention of chronic osteomyelitis is the prevention of delayed treatment, and the fellowship answer stresses the urgency of early diagnosis and adequate antibiotic therapy. [5] [11]
The pitfall of the normal radiograph is the error that most often delays the diagnosis. A child with a painful limb and a normal early radiograph is assumed to have a soft-tissue injury, and the magnetic resonance image is not requested until the symptoms persist or the inflammatory markers rise. The safeguard is the rule that a normal radiograph does not exclude osteomyelitis, and that the child with clinical suspicion receives a magnetic resonance image regardless of the plain film. The pitfall of the missed Kingella kingae infection is the related error — the child with mild symptoms and normal inflammatory markers is discharged, and the infection is identified only when it progresses. The safeguard is the low threshold for blood culture and molecular diagnostics in children under four years. [6] [1]
The pitfall of the overlong intravenous course is the modern error. A child who meets the criteria for the oral switch but who remains on intravenous therapy because of tradition or inertia suffers the complications of prolonged intravenous access — line infection, thrombosis, displacement — without any therapeutic benefit. The safeguard is the structured application of the switch criteria and the regular review of the child by the treating team. The randomised evidence supports the safety and efficacy of the early oral switch, and the fellowship candidate who advocates for it demonstrates the evidence-based practice that the examination rewards. [3] [12]
Prognosis & Disposition
The prognosis of acute haematogenous osteomyelitis is excellent when the diagnosis is made promptly and the treatment is adequate. The great majority of children with uncomplicated disease recover fully, with no long-term sequelae, when the antibiotic therapy is started within the first few days of the illness and when the course is completed. The prognosis worsens with delay: a child whose treatment is delayed beyond the first week has a higher rate of complications, including growth disturbance, chronic infection, and avascular necrosis. The severity of the infection, the virulence of the organism, and the presence of complications are the further determinants of the outcome. [4] [2]
The prognosis of discitis is similarly favourable, with the great majority of children recovering fully with medical management. The outcome depends on the timeliness of the diagnosis and the absence of epidural abscess or cord compression. A child who presents with neurological signs and who undergoes urgent surgical decompression has a variable prognosis that depends on the duration and severity of the cord compression, and the fellowship answer stresses the urgency of imaging in the child who refuses to walk or sit. [9] [10]
The disposition is shared between the general paediatrician, the orthopaedic surgeon, and the infectious-diseases physician. The general paediatrician owns the initial assessment, the empirical antibiotic resuscitation, the monitoring of the clinical and C-reactive-protein response, and the coordination of the oral switch and the outpatient follow-up. The orthopaedic surgeon owns the drainable abscess, the surgical debridement, and the management of the growth disturbance and the chronic infection. The infectious-diseases physician owns the antibiotic selection in complex cases, the management of resistant organisms, and the guidance of the total duration. The fellowship answer names the right specialist at the right time and never manages a complicated case in isolation. [1] [8]
Special Populations
Indigenous and remote-dwelling children face a higher burden of osteoarticular infection and the additional challenge of geographic distance from imaging and specialist services. The incidence of acute haematogenous osteomyelitis, and of skin and soft-tissue infection that predisposes to it, is substantially higher in many remote Indigenous communities, and the Staphylococcus aureus strains in these settings may carry a higher rate of community-acquired methicillin resistance. The distance to a magnetic resonance scanner and to a paediatric orthopaedic service delays the diagnosis and the surgical intervention, and the clinical pathway must incorporate the principles of retrieval, telehealth consultation, and the early empirical antibiotic therapy that can be started in the remote setting while the child is being transferred. [8] [4]
Newly arrived migrant and refugee children may present with advanced or chronic osteomyelitis that has been untreated during displacement, and the workup must consider organisms that are uncommon in the host country, including tuberculosis. Skeletal tuberculosis — most often Pott disease of the spine — presents with a chronic, destructive vertebral infection that mimics pyogenic discitis but runs a more indolent course, and the diagnosis is confirmed by biopsy and culture. The immunisation history, the tuberculosis exposure, and the nutritional status of the child are reviewed, and the empirical antibiotic regimen for pyogenic osteomyelitis is started while the tuberculosis workup proceeds. [9] [4]
The immunocompromised child — whether from chemotherapy, transplantation, or primary immunodeficiency — has a broader microbiological differential and a more aggressive disease course. The empirical antibiotic regimen is broadened to cover gram-negative organisms and fungi, and the threshold for surgical biopsy to obtain a tissue diagnosis is lower, because the culture may reveal an unexpected organism that demands a targeted therapy. The fellowship answer for the immunocompromised child always involves the infectious-diseases team early and always treats the regimen as provisional until the organism is identified. [1] [11]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric acute haematogenous osteomyelitis rests on the 2021 Pediatric Infectious Diseases Society and Infectious Diseases Society of America clinical practice guideline, which is the definitive contemporary reference. The guideline was developed by a multidisciplinary panel and it provides evidence-based recommendations on the diagnosis, the empirical antibiotic selection, the intravenous-to-oral switch, the total duration of therapy, and the surgical indications. The UK consensus guidelines from 2023, authored by Mitchell and colleagues, provide a complementary set of recommendations that reflect the European context, and together the two documents define the standard of care. [1] [8]
The evidence for the intravenous-to-oral switch strategy is drawn from the de Graaf feasibility study, published in 2017, which demonstrated that a short intravenous course followed by oral therapy was acceptable to families and clinically safe, and from the broader body of observational evidence that has accumulated over two decades. The Weichert review from 2008 framed the question of treatment duration and highlighted the absence of high-quality evidence for the long intravenous courses that tradition once dictated, and the subsequent research, culminating in the 2021 guideline, has established the shorter, response-guided strategy as the standard. The antibiotic selection evidence is drawn from the Arnold and Bradley review and the Gornitzky critical analysis, which summarise the age-stratified microbiology and the empirical regimens. [3] [12] [11]
The Kingella kingae evidence rests on the Yagupsky review and the Wong systematic review, which together document the epidemiology, the clinical features, the diagnostic methods, and the management of Kingella kingae musculoskeletal infection. The evidence for discitis and spondylodiscitis is drawn from the Al Yazidi review and the Ferri systematic review, which summarise the clinical characteristics, the management, and the outcomes of paediatric vertebral infection. The imaging evidence, including the role and the protocol of magnetic resonance imaging, is drawn from the Restrepo comprehensive review and the Gornitzky critical analysis. [6] [7] [9] [10] [5]
The regional differences are modest but real. The rates of community-acquired methicillin-resistant Staphylococcus aureus vary by geography, and the empirical regimen is adjusted to the local resistance patterns — clindamycin or vancomycin where the rate is high, a first-generation cephalosporin where it is low. The availability of magnetic resonance imaging varies by setting, and the rural or remote clinician may rely on ultrasound and clinical judgment while arranging transfer. The access to paediatric orthopaedic and infectious-diseases services is uneven, and the general paediatrician in a remote setting must be prepared to initiate the full empirical regimen and to coordinate the retrieval. [8] [1]
The controversies are few but genuine. The optimal total duration of antibiotic therapy — three versus four versus six weeks — is debated for the borderline case, and the guideline provides a framework rather than a fixed answer. The role of serial C-reactive protein measurements to guide the duration and the switch is endorsed but not rigidly quantified, and the clinical judgment of the treating team remains central. And the threshold for surgical intervention in the child with a small subperiosteal collection that might resolve with antibiotics alone is a judgement call that the orthopaedic and the infectious-diseases teams make together. [1] [4]
Exam Pearls
The fellowship answer turns on five facts. Acute haematogenous osteomyelitis seeds the metaphyseal capillaries through the bloodstream, and the long-bone metaphysis is the canonical site. Staphylococcus aureus is the leading organism at all ages, but Kingella kingae is the leading cause in children under four years and it presents with a milder inflammatory response. Magnetic resonance imaging is the diagnostic gold standard, and a normal early radiograph does not exclude the diagnosis. The management is empirical intravenous antibiotics followed by an early oral switch guided by the clinical and C-reactive-protein response. And the total course is three to four weeks for uncomplicated disease, with the oral switch made when the child is afebrile, improving, and the C-reactive protein is falling. [1] [6]
The examiner probes three traps. The first is the normal radiograph that is accepted as reassurance — the magnetic resonance image is the gold standard, and the child with clinical suspicion is imaged regardless of the plain film. The second is the mild, afebrile presentation in a child under four years that is discharged without investigation — Kingella kingae osteomyelitis is missed, and the low threshold for blood culture and molecular diagnostics is the safeguard. The third is the child who fails to improve within forty-eight to seventy-two hours and whose imaging is not repeated — the subperiosteal abscess is missed, and the child is treated with antibiotics alone for an infection that demands surgical drainage. [1] [5]
The examiner rewards the candidate who frames osteomyelitis as an urgent, curable infection that demands early diagnosis and structured management. The febrile child with a painful limb is assessed for osteomyelitis, the cultures and the inflammatory markers are obtained, the magnetic resonance image is requested, the empirical antibiotics are started, the response is monitored, the oral switch is made, and the course is completed. The specialist teams are involved early, the family is given a clear explanation and plan, and the child is followed up to confirm the recovery and to detect any growth disturbance. A candidate who shows this breadth and this safety demonstrates the systems thinking that the fellowship demands. [4] [8]
References
- [1]Woods CR, Bradley JS, Chatterjee A, Copley L, Robinson J, McNeil JC, et al. Clinical Practice Guideline by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America: 2021 Guideline on Diagnosis and Management of Acute Hematogenous Osteomyelitis in Pediatrics. Journal of the Pediatric Infectious Diseases Society, 2021.PMID 34350458
- [2]Yeo A, Ramachandran M. Acute haematogenous osteomyelitis in children. BMJ (Clinical research ed.), 2014.PMID 24446020
- [3]Weichert S, Sharland M, Clarke NM, Avent M, Doherty C, Zaoutis T, et al. Acute haematogenous osteomyelitis in children: is there any evidence for how long we should treat? Current Opinion in Infectious Diseases, 2008.PMID 18448970
- [4]Gornitzky AL, Kim AE, O'Donnell JM, Baldwin KD, Hosseinzadeh P, Baldwin K, et al. Diagnosis and Management of Osteomyelitis in Children: A Critical Analysis Review. JBJS Reviews, 2020.PMID 33006465
- [5]Restrepo R, Park HJ, Karakas SP, Gao J, D'Agostino C, Greenberg D, et al. Bacterial osteomyelitis in pediatric patients: a comprehensive review. Skeletal Radiology, 2024.PMID 38504031
- [6]Yagupsky P. Diagnosing Kingella kingae infections in infants and young children. Expert Review of Anti-infective Therapy, 2017.PMID 28918656
- [7]Wong M, Williams N, Cooper C. Systematic Review of Kingella kingae Musculoskeletal Infection in Children: Epidemiology, Impact and Management Strategies. Pediatric Health, Medicine and Therapeutics, 2020.PMID 32158303
- [8]Mitchell PD, Abraham A, Carpenter C, Collingwood J, Donaldson L, Drew R, et al. Consensus guidelines on the management of musculoskeletal infection affecting children in the UK. The Bone and Joint Journal, 2023.PMID 37399098
- [9]Al Yazidi LS, Hameed H, Kesson A, Marais S, Pithie A, Webb R, et al. Spondylodiscitis in children. Journal of Paediatrics and Child Health, 2022.PMID 36000507
- [10]Ferri I, Ristori G, Lisi C, Danti G, Folli F, Galli L, et al. Characteristics, Management and Outcomes of Spondylodiscitis in Children: A Systematic Review. Antibiotics (Basel), 2020.PMID 33396379
- [11]Arnold JC, Bradley JS. Osteoarticular Infections in Children. Infectious Disease Clinics of North America, 2015.PMID 26311358
- [12]de Graaf H, Sukhtankar P, Arch B, Le Doare K, Radia T, Sharland M, et al. Duration of intravenous antibiotic therapy for children with acute osteomyelitis or septic arthritis: a feasibility study. Health Technology Assessment, 2017.PMID 28862129