Paeds · rheumatology-musculoskeletal-and-sports
Performance-enhancing substances in young athletes
Also known as doping in young athletes · anabolic steroid use in adolescents · performance and image enhancing drugs · PIEDs · ergogenic aid use in children · WADA prohibited substances · sports supplement misuse · androgen abuse in the young athlete · unintentional doping from supplements
A fellowship approach to performance-enhancing substances in the young athlete: the WADA prohibited list and the principle of strict liability, the anabolic steroids that dominate illicit use and the cardiovascular, hepatic, endocrine, and psychiatric harm they inflict on a still-growing body, the supplements that work and the contaminated supplements that trigger inadvertent positive tests, and the non-judgemental, evidence-based counselling that prevents use.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A fifteen-year-old opens the consultation with a sore shoulder, but the real story is in his body: he has gained nine kilograms of lean mass in a term, his back and shoulders are covered in cystic acne, his testicles are small for his stage of puberty, and he admits, only when you ask alone and without his father in the room, that he has been injecting testosterone and an oral steroid he bought online for the last four months. You do not lecture him. You acknowledge the effort he has put in, you explain what the drugs are doing to his growth plate and his heart, you arrange baseline bloods, and you plan a slow, supported taper with a mental-health safety net, because abrupt cessation can precipitate a depressive crash. [6] [7]
The five questions to ask a young athlete about substances
PERFORM
Overview & Definition
Performance-enhancing substances are agents taken with the intention of improving sporting performance, body composition, or appearance, and they span a spectrum from permitted ergogenic aids such as creatine and caffeine through to prohibited androgenic hormones and blood manipulations. The fellowship candidate holds the spectrum in mind rather than reaching for the single word "steroids", because the adolescent in front of the clinician may be using anything from a whey protein shake to a vial of injectable testosterone bought without a prescription. The clinical task is to find out which, to gauge the harm, and to intervene proportionately. [1] [7]
Two frameworks organise the field for the clinician. The first is the World Anti-Doping Agency prohibited list, which governs competitive athletes and defines which substances and methods are banned in and out of competition. The second is the wider public-health category of appearance- and performance-enhancing drugs and substances, which captures the non-competitive adolescent who uses androgens, growth hormone, or image-enhancing drugs for the mirror rather than the medal. The young athlete often sits in both frameworks at once, and the clinician who forgets the second misses the gym-using teenager who will never be drug-tested. [10] [4]
The paediatric and adolescent dimension is what makes this a distinct topic from adult sports medicine. The adolescent is still growing, so the gonadal suppression and the premature epiphyseal fusion carry an irreversible cost the adult does not pay. The adolescent brain is still maturing, so the mood, impulse-control, and dependence risks carry greater weight. And the adolescent is forming identity and habits, so a non-judgemental, harm-reducing intervention at this window can redirect a trajectory that a punitive response would only drive underground. [6] [7]
Classification
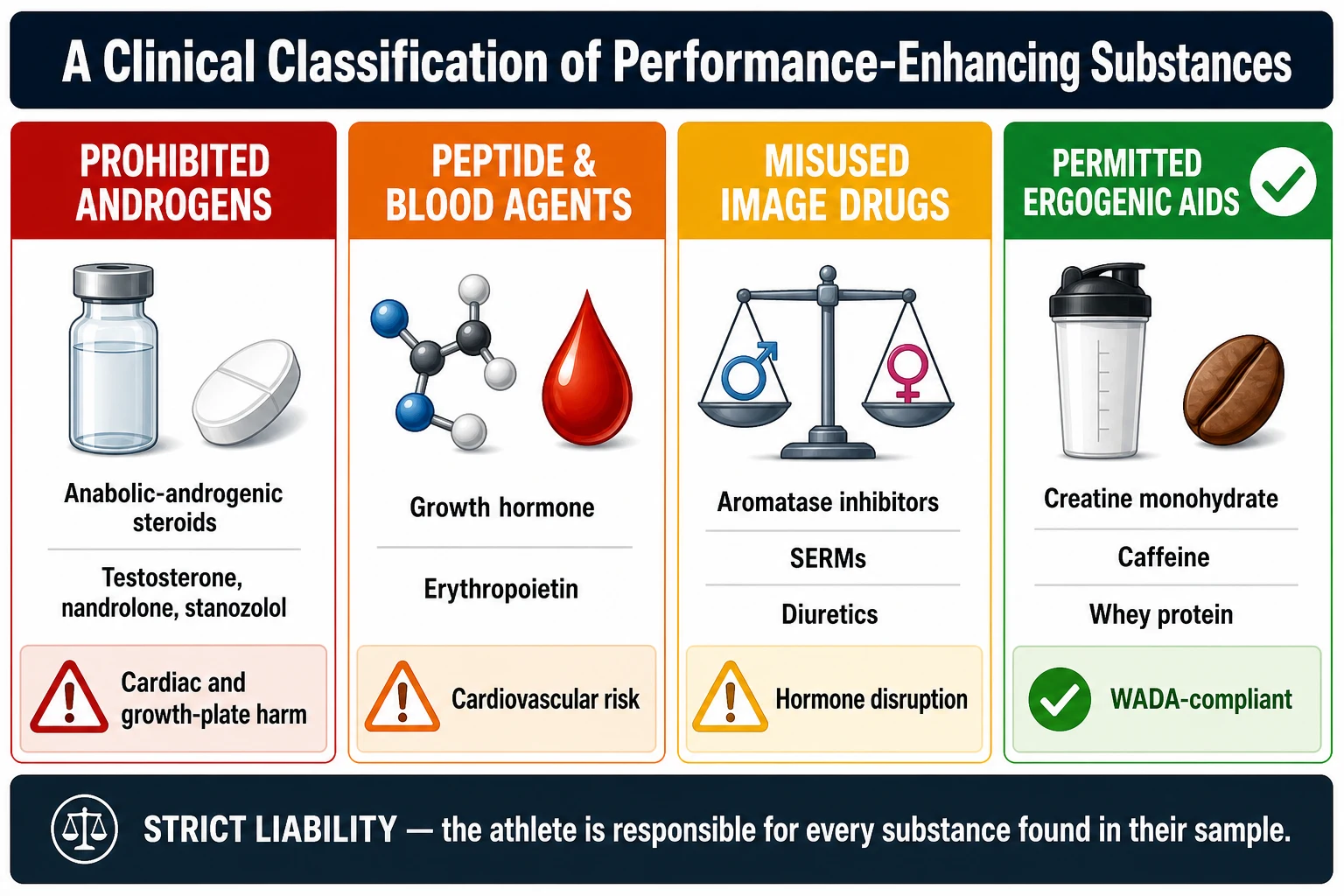
The classification that governs competitive sport is the World Anti-Doping Agency prohibited list, which groups substances and methods into ten categories and applies the principle of strict liability, meaning that the athlete is responsible for any prohibited substance found in their sample regardless of how it got there or whether they intended to dope. The categories most relevant to the young athlete are the anabolic agents, the peptide hormones and growth factors, the hormone and metabolic modulators, the diuretics and masking agents, and the stimulants. Some categories are prohibited at all times, while the stimulants, narcotics, cannabinoids, and glucocorticoids are prohibited only in competition, and the candidate must hold that in-competition versus out-of-competition distinction because it explains why a cold remedy can fail a test on game day. [1] [7]
A second, clinically driven classification sorts substances by the harm they carry and the legitimacy of their evidence, and this is the classification the clinician uses at the bedside. At one end sit the prohibited androgenic hormones, the anabolic-androgenic steroids, testosterone and its synthetic derivatives, along with growth hormone, erythropoietin, and blood transfusion, which carry the greatest harm and zero legitimate place in the young athlete. In the middle sit the regulated or misused image-enhancing drugs such as the androgens used for cosmetic muscle gain and the non-steroidal aromatase inhibitors used to blunt oestrogen. At the permitted end sit the evidence-based ergogenic aids, creatine monohydrate for repeated high-intensity work and caffeine for endurance and focus, which a young athlete can use within the rules and with comparatively low risk when dosed sensibly and sourced cleanly. [1] [11]
A third axis the clinician must name is the route and the source, because they govern both the harm and the legal exposure. The injectable androgens bought without a prescription carry blood-borne virus risk from shared or unsterile equipment, and the oral androgens carry the greater hepatic load that drives cholestasis and, rarely, tumours. The over-the-counter supplement is the stealth source of harm, because a substantial minority of products sold as protein, pre-workout, or fat-burner contain undeclared prohibited substances, and under strict liability the athlete who takes them bears the consequence of a positive test regardless of the label. The clinician who classifies by route and source counsels safer practice and flags the inadvertent-doping risk that no competitor expects. [9] [8]
| Feature | Creatine and caffeine | Anabolic-androgenic steroids |
|---|---|---|
| WADA status | Not prohibited | Prohibited at all times |
| Evidence for benefit | Moderate and consistent for specific tasks | Potent, but obtained illicitly and at high cost |
| Main physical harms | Few when dosed sensibly | Cardiac, hepatic, growth-plate, gonadal |
| Main mental-health harm | None established | Mood disturbance, aggression, dependence, withdrawal |
| Doping-test risk | Low if sourced cleanly | Sanction, and contamination adds risk |
| Clinical stance | Honest risk-benefit discussion | Counsel cessation with a supported plan |
Epidemiology & Risk Factors
The use of performance-enhancing substances among adolescents is commoner than most clinicians assume, and the figures are sobering when they are asked for. The Project EAT study of more than four thousand adolescents found that roughly five per cent of high-school students reported steroid use, with higher rates among boys and among those engaged in strength-focused sport and weight training. The global meta-analysis of Sagoe and colleagues estimated the lifetime prevalence of anabolic-androgenic steroid use across populations at around three to four per cent, with much higher rates in specific groups such as recreational gym users, and the rates among the young have been sustained by the rise of social-media body-image culture. [3] [4]
The contemporary signal is that the problem is not confined to elite competitors and is increasingly reported to physicians. Ganson and colleagues' physician-report study documented that appearance- and performance-enhancing drug use among adolescents is encountered in paediatric and adolescent practice, and the use clusters with other health-risk behaviours, with disordered eating, and with mental-health concerns. The supplement layer is wide: Nieper found that the great majority of junior national track and field athletes used nutritional supplements, and Jovanov and colleagues showed that supplement use among young athletes is near-universal and driven by knowledge gaps and the belief that supplements are inherently safe. [10] [2]
The numbers the fellowship candidate should hold
The risk factors cluster into three groups that guide who to screen. The performance and appearance pressure group includes the strength-sport athlete, the bodybuilder, the adolescent chasing a social-media physique, and the athlete facing selection or scholarship pressure. The vulnerability group includes the adolescent with low self-esteem, body-image dissatisfaction, disordered eating, or a mental-health condition, and the male who links his worth to muscularity. The access group includes the older sibling or coach who normalises use, the online marketplace that sells androgens without a prescription, and the gym culture that supplies both the substances and the instruction to use them. The clinician screens the adolescent who sits in any of these groups, because early identification redirects a trajectory that delay hardens. [6] [7]
Pathophysiology
The pathophysiology of the dominant class, the anabolic-androgenic steroids, is the action of supraphysiological androgen on the androgen receptor and the downstream disruption of the hypothalamic-pituitary-gonadal axis. The athlete who injects or ingests testosterone or a synthetic derivative floods the receptor with androgen, and the anabolic effects, increased protein synthesis and muscle hypertrophy, deliver the performance gain. The same flood suppresses the gonadotropins luteinising and follicle-stimulating hormone through negative feedback, the testes stop producing endogenous testosterone, and testicular atrophy and infertility follow. The axis can recover after cessation, but recovery is slow, incomplete in some, and punctuated by a symptomatic hypogonadal window. [1] [4]
The harm to the still-growing adolescent arises from aromatisation and from the cardiovascular and metabolic effects. A fraction of the excess androgen is aromatised to oestrogen, which in the adolescent accelerates the fusion of the epiphyseal growth plates and can reduce final adult height, an irreversible harm that is the specific paediatric cost of use. The oestrogen excess also produces gynaecomastia in the male user. The cardiovascular effects include a pro-atherogenic shift in the lipid profile with a fall in high-density lipoprotein, a rise in blood pressure, left ventricular hypertrophy, and an association with thrombosis and sudden cardiac events. The hepatic effects, seen especially with the oral seventeen-alpha-alkylated steroids, range from cholestasis and elevated transaminases to peliosis hepatis and, rarely, hepatic tumours. [1] [6]
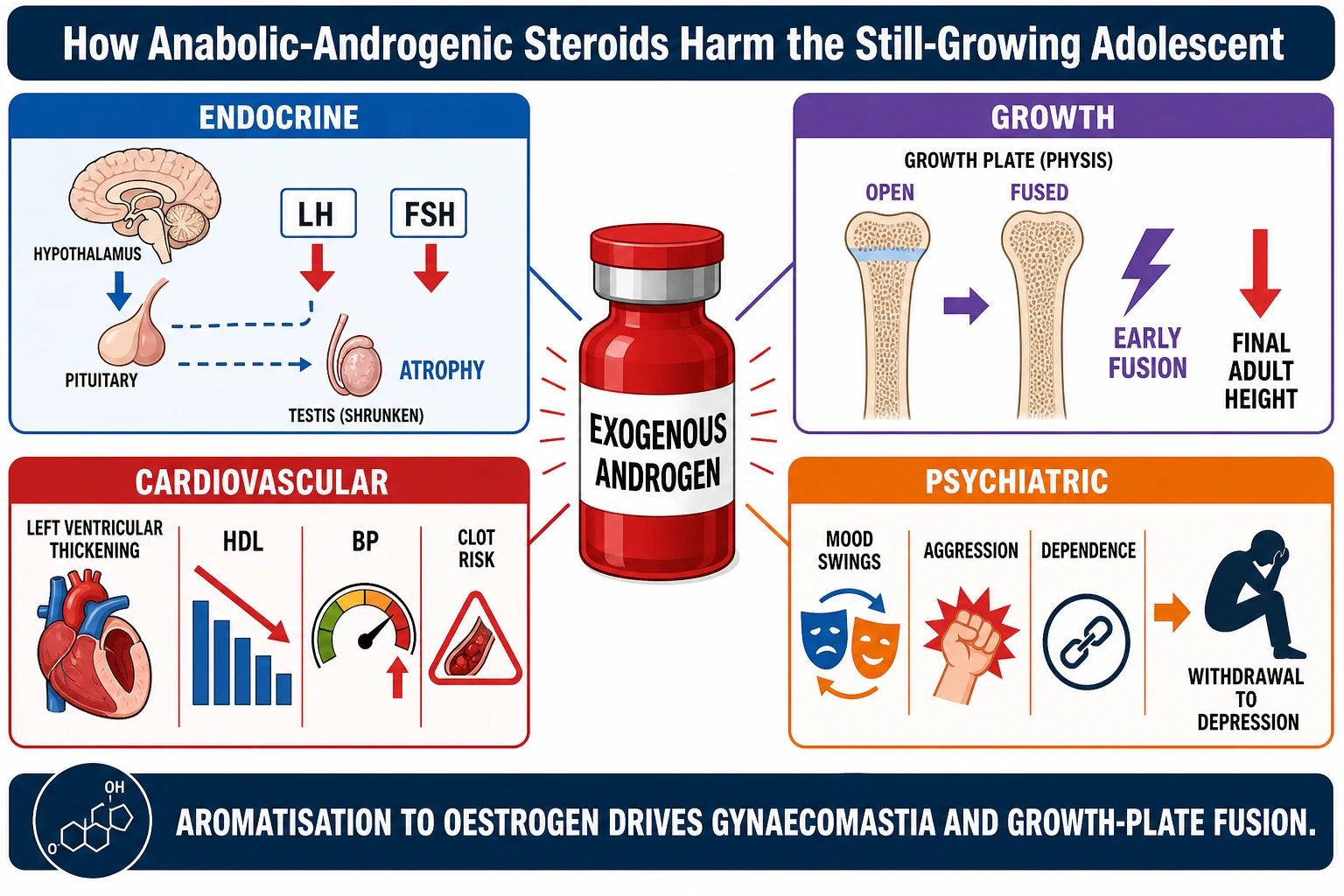
The psychiatric pathophysiology is the dimension the clinician most often underestimates, and it is the dimension that drives the morbidity and the mortality. The androgen excess is associated with mood elevation, irritability, impulsivity, and in some a hypomanic or frank aggressive state, and the chronic use carries an established risk of dependence. The cessation exposes the suppressed axis, the endogenous testosterone is low, and the withdrawal syndrome is a genuine hypogonadal depression that can include suicidal ideation, which is why stopping must never be abrupt or unsupported. The candidate who frames androgen use as a brain disease as much as a muscle one is equipped to keep the young athlete safe. [4] [6]
The cascade from supraphysiological androgen to harm
Exogenous androgen floods the androgen receptor, driving muscle protein synthesis and the sought-after performance gain.
Negative feedback suppresses luteinising and follicle-stimulating hormone, endogenous testosterone falls, and the testes atrophy.
Aromatisation of excess androgen to oestrogen fuses the adolescent growth plate early and can reduce final adult height, and it produces gynaecomastia.
The lipid profile shifts toward atheroma, blood pressure rises, and the left ventricle hypertrophies, raising the cardiovascular risk.
The oral seventeen-alpha-alkylated steroids impose a hepatic load of cholestasis and, rarely, peliosis or tumour.
On cessation the suppressed axis produces a hypogonadal withdrawal that can include depressive symptoms and suicidal ideation.
Clinical Presentation
The young athlete who uses performance-enhancing substances presents in one of three ways, and only one of them is the candid disclosure. The candid adolescent volunteers the use, often when asked routinely in a confidential adolescent interview, and this is the presentation the clinician creates by asking. Far commoner is the incidental presentation through physical signs, the rapid lean-mass gain, the severe acne, the striae, the gynaecomastia, the testicular atrophy, or the premature balding in an adolescent boy, and the alert clinician who notices these asks the question privately. The third presentation is through harm, the new hypertension, the mood disturbance or aggression reported by the family, the chest pain or palpitations, or, tragically, the psychiatric crisis of withdrawal or the sudden cardiac event. [6] [7]
The history is the diagnostic instrument, and it succeeds only when it is confidential, non-judgemental, and developmentally appropriate. The clinician sees the adolescent alone, guarantees confidentiality within the bounds of safety, and asks directly about performance and image goals, training, supplements, and any androgen or hormone use, because most users will not disclose unless asked. A HEADSS-shaped adolescent assessment frames the questions and captures the co-occurring risks, the disordered eating, the recreational drug and alcohol use, the mental-health symptoms, and the performance and appearance pressures that sustain the use. The route, the dose, the regimen, and the injection practice are mapped, because they govern the harm and the blood-borne virus risk. [7] [6]
Which reassuring-sounding presentations must never close the search? The well-muscled athlete who attributes his gains to protein and hard work may still be using androgens, and the absence of disclosure is not the absence of use. The athlete who uses only over-the-counter supplements is not risk-free, because the supplement may be contaminated and the cardiovascular and psychiatric profile of high-dose stimulant fat-burners is real. The athlete with no physical signs may be early in use or may be using peptides and image drugs that leave few external marks. And the family that reports only that their son has become angry and withdrawn has handed the clinician the psychiatric presentation of androgen cycling, and the direct question must follow. [6] [4]
Differential Diagnosis
The differential diagnosis turns on which presentation brought the athlete to the clinician. The rapid-mass-gain presentation must be distinguished from a legitimate and well-coached strength programme fuelled by adequate nutrition, from the physiological pubertal muscle gain of a late-maturing boy, and from the weight gain of anabolic recovery from illness. The clues to illicit androgen use are the speed and pattern of the gain, the androgenic signs of acne and striae and testicular atrophy, and the gap between the stated training and the achieved physique. The candid history settles most of these, and the examination confirms the rest. [1] [6]
The acne, gynaecomastia, and mood presentation must be distinguished from the common adolescent conditions that share these features. Physiological adolescent gynaecomastia is common, transient, and bilateral, but it is usually modest in volume, whereas the androgen-driven gynaecomastia of aromatisation sits alongside other androgenic signs. Severe nodulocystic acne can be ordinary adolescent acne, but its abrupt onset and distribution across the shoulders and back in a rapidly muscled adolescent point to androgen use. The mood disturbance and aggression must be distinguished from a primary mood disorder, a conduct disorder, or a substance-use disorder, and the clinician holds the possibility that androgen use coexists with and aggravates each of these. [7] [4]
The short-stature and pubertal presentation must be distinguished from constitutional delay, growth-hormone deficiency, and the other endocrine causes of short stature, because the adolescent who has fused his growth plates early with androgens presents with a height that has fallen off his curve and a bone age that is advanced. The hypertensive or cardiac presentation must be distinguished from essential hypertension, a primary cardiac cause, and the stimulant effect of high-dose pre-workout or caffeine supplements. The fellowship answer holds these mimics in parallel and uses the confidential history and the targeted examination to separate the androgen user from the look-alike. [1] [11]
Clinical & Bedside Assessment
The bedside assessment begins with the general appearance and the vital signs, because the still-growing body tells the story of androgen use. The blood pressure is measured, because hypertension is common and often missed in the young, and the resting heart rate and the cardiovascular examination seek the left ventricular hypertrophy and the flow murmur that chronic androgen use can produce. The growth chart is plotted, because height falling off the centiles with weight and muscle climbing is the signature of premature epiphyseal fusion, and the pubertal stage is assessed, because discordance between muscle development and testicular volume is a red flag. [1] [6]
The focused examination seeks the physical stigmata of androgen use and the harm it causes. The skin is inspected for severe nodulocystic acne, for striae, for accelerated male-pattern baldness, and for injection sites or abscesses. The chest is examined for gynaecomastia. The genital examination, performed sensitively and with consent and a chaperone, assesses testicular volume and atrophy, and the secondary sexual characteristics are staged. The cardiovascular and abdominal examination seeks the left ventricular hypertrophy and the hepatomegaly that signal systemic harm. The mental state examination assesses mood, irritability, insight, and risk, because the psychiatric burden is the dimension most often missed at the bedside. [7] [6]
Which findings must never be dismissed? A new hypertension in a muscular adolescent is not automatically benign essential hypertension until androgen and stimulant use is excluded. Testicular atrophy in an adolescent is not a normal variant. Severe acne of abrupt onset across the shoulders and back in a rapidly muscled boy is a flag, not a cosmetic problem. And the family report of a sudden personality change, of anger and withdrawal and secrecy, is the psychiatric presentation that demands the direct question. The bedside assessment is the filter that turns these findings into the confidential history that makes the diagnosis. [6] [1]
Investigations
The investigation of the young athlete who uses or is suspected of using performance-enhancing substances is directed at quantifying the harm, confirming the suppression, and excluding the mimics, because the diagnosis itself rests on the history. The baseline panel for the confirmed or suspected androgen user includes a full blood count, a lipid profile, a liver panel including transaminases, a renal panel, and a fasting glucose, because the cardiovascular and hepatic and metabolic harms are quantified and followed. The blood pressure is measured and rechecked, and an electrocardiogram and, in selected cases, an echocardiogram are obtained when cardiovascular signs or a long duration of use raise the concern for left ventricular hypertrophy. [1] [7]
The endocrine investigation confirms the gonadal suppression and excludes the mimics of short stature. A morning total testosterone, luteinising hormone, and follicle-stimulating hormone demonstrate the suppressed axis of active use, and the repeat testing after cessation tracks the recovery that is often slow. A bone age radiograph of the left hand is obtained when premature fusion or advanced skeletal maturation is suspected, because it quantifies the growth cost and informs the prognostic conversation. The sex-hormone-binding globulin and oestradiol may be measured when the picture is mixed, and the prolactin and thyroid studies are reserved for the differential of gynaecomastia. [6] [4]
The screening for the reversible and the co-occurring harm completes the panel. The mental-health screen, using a validated adolescent depression tool, is mandatory, because the depressive and suicidal risk is the harm that kills. The blood-borne virus screen for hepatitis and human immunodeficiency virus is obtained when injection practice is reported or suspected, because the shared or unsterile equipment of illicit androgen injection carries the same risk as any injecting drug use. The doping test itself is not the clinician's tool, because the clinician is not the tester, and the therapeutic alliance depends on the guarantee that the clinical consultation is not a drug test. [6] [9]
Management — Resuscitation
The resuscitation priority is the acute harm, and in this topic the acute harm is most often psychiatric or cardiovascular. The adolescent who presents in an agitated or aggressive state, or in the depressive or suicidal crash of an unsupported withdrawal, is assessed for risk as a matter of urgency, with a structured risk assessment, a safety plan, the removal of access to means, and the involvement of mental-health services and the family within the bounds of confidentiality. The suicidal adolescent is not sent home to wait, and the androgen withdrawal is framed as a treatable hypogonadal depression rather than a moral failing. [6] [4]
The acute cardiovascular presentation is managed on its merits. The young athlete with chest pain, palpitations, syncope, or severe hypertension receives the standard evaluation for the cardiac cause, with an electrocardiogram, troponin where indicated, and an echocardiogram, because the androgen-associated left ventricular hypertrophy, the dyslipidaemia, and the thrombotic risk raise the possibility of a genuine cardiac event in a young person. The hypertensive urgency is managed with standard agents and with cessation counselling, and the stimulant-toxicity picture from high-dose fat-burners or pre-workout is managed with supportive care and benzodiazepine sedation where required. [1] [11]
The first intervention with the stable, candid adolescent is to establish the therapeutic alliance that the rest of the management depends on. The clinician does not lecture, does not threaten sanction, and does not breach confidentiality within the bounds of safety, because the punitive response drives the use underground and ends the chance of change. The clinician acknowledges the effort and the pressure, explains the harm in terms the adolescent can use, frames cessation as a supported and gradual process, and sets up the follow-up that turns a single conversation into a trajectory of change. [7] [6]
Management — Definitive & Stepwise
The definitive management is counselling-first, harm-reduction-first, and evidence-based, and it proceeds in steps that the fellowship candidate can articulate. The first step is the assessment of the substance, the dose, the route, the duration, and the harm, and the establishment of the goals the athlete is trying to reach, because meeting those goals safely is the alternative the clinician offers. The second step is the honest risk-benefit discussion that names the cardiovascular, growth, gonadal, hepatic, and psychiatric harms in terms the young person can weigh, and that corrects the gym mythology that surrounds androgens. [6] [5]
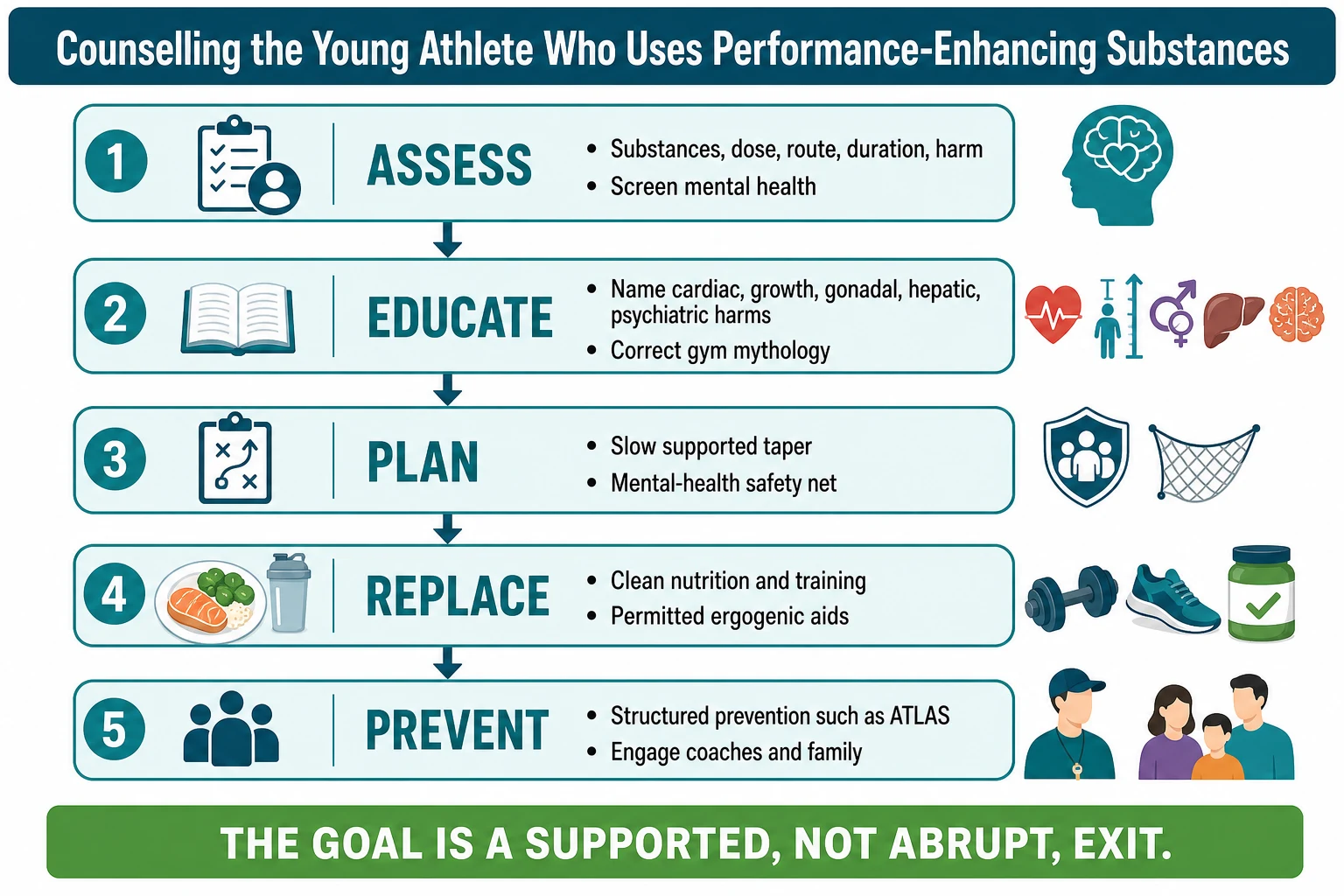
The third step is the cessation plan, and its cardinal rule is that withdrawal must be slow and supported, never abrupt. The young athlete who stops androgens suddenly enters a hypogonadal window with depressive symptoms and suicidal-ideation risk, so the clinician plans a taper, screens and re-screens for depression and suicide risk, builds a safety plan, and arranges close follow-up, with mental-health referral for the symptomatic. The harm-reduction layer is offered to the athlete who is not yet ready to stop: sterile injecting equipment and education to reduce blood-borne virus risk, blood-pressure and lipid monitoring, and the honest statement that any reduction in dose is a gain. The clinician who insists on all-or-nothing abstinence loses the adolescent who would have accepted a graduated plan. [4] [6]
The fourth and fifth steps are the safe replacement and the prevention. The safe replacement offers the young athlete a clean, evidence-based plan of nutrition, periodised training, and, where appropriate, permitted ergogenic aids such as creatine and caffeine sourced from reputable third-party-tested suppliers, so that the goal that drove the use is met without the harm. The prevention step engages the evidence: the ATLAS programme of Goldberg and colleagues showed that a multidimensional, team-centred prevention intervention reduced the intent to use and the actual use of anabolic steroids among adolescent athletes, and the fellowship candidate cites it as the model that works. The coach, the family, and the sporting environment are engaged, because the pressure that drives use lives in the environment, and the clinician who changes only the adolescent changes too little. [5] [8]
All-or-nothing abstinence
- Drives use underground and ends the alliance
- Precipitates abrupt unsupported withdrawal
- Ignores the goal that drives the use
- Misses the chance of graduated change
Supported, graduated plan
- Keeps the adolescent in care and in follow-up
- Plans a slow taper with a mental-health safety net
- Offers a safe replacement that meets the goal
- Engages prevention and the sporting environment
Specific Subtypes & Scenarios
The competitive adolescent athlete is the subtype governed by the anti-doping framework, and the clinician's task is to keep this athlete both healthy and eligible. The competitive athlete who uses a prohibited substance risks a sanction under strict liability, and the inadvertent positive from a contaminated supplement is the scenario the clinician must prevent through supplement counselling. The young athlete is advised to use only third-party-tested supplements, to avoid proprietary blends and products making extreme claims, and to understand that they alone are responsible for what is found in their sample. The therapeutic-use exemption process is explained when a legitimate medication is prohibited, because the clinician who prescribes an inhaler or a stimulant for a competitive athlete must know whether it requires an exemption. [9] [2]
The recreational gym user is the subtype who will never be drug-tested and who is invisible to the anti-doping system, and it is the subtype the paediatric clinician most often meets. This adolescent uses androgens for the mirror rather than the medal, is driven by social-media body-image culture, and presents through the physical signs or the psychiatric harm rather than through a doping control. The clinical pathway is the same counselling-first approach, with particular attention to the image and mental-health drivers, to the injection practice and blood-borne virus risk, and to the gradual supported cessation. The clinician who remembers that the gym user is the commoner subtype does not wait for a doping test to find the use. [10] [4]
The supplement user and the inadvertent-doping scenario are the subtypes that sit at the permitted end of the spectrum but carry real risk. The supplement-using young athlete, studied by Nieper and by Jovanov and colleagues, is near-universal, and the clinician's task is to sort the safe from the risky, to recommend third-party-tested products, and to warn that contamination with undeclared prohibited substances is documented in a substantial minority of products. The inadvertent positive is the consequence under strict liability, and the candidate frames the supplement discussion as a doping-risk and a health-risk conversation, not merely a nutrition one. The young athlete who understands that the label is no guarantee is equipped to protect both eligibility and health. [2] [9]
Complications & Pitfalls
The complications of performance-enhancing substance use in the young athlete are the cardiovascular, the endocrine and growth, the hepatic, the psychiatric, and the infectious, and the irreversible among them define the paediatric stakes. The cardiovascular complications include the pro-atherogenic dyslipidaemia, the hypertension, the left ventricular hypertrophy, and the association with thrombosis and sudden cardiac death. The growth complication is the premature epiphyseal fusion that can reduce final adult height, and the gonadal complication is the atrophy and the infertility that may persist after cessation. The hepatic complications range from cholestasis to peliosis and tumour with the oral steroids, and the psychiatric complications span the mood, aggression, dependence, and the suicidal withdrawal. The infectious complications are the blood-borne viruses of unsterile injection. [1] [4]
The pitfall of the punitive response is the error that most often ends the chance of change. The clinician who lectures, threatens sanction, or breaches confidentiality within the bounds of safety drives the use underground and loses the adolescent to follow-up, and the family that discovers the use and reacts with anger precipitates the abrupt withdrawal that carries the suicidal risk. The safeguard is the non-judgemental, harm-reducing stance that keeps the adolescent in care. The pitfall of the missed psychiatric burden is the related error, in which the physical signs are addressed and the mood and suicide risk are not, and the safeguard is the routine mental-health screen of every identified user. [6] [7]
The pitfall of the unrecognised supplement contamination is the error that costs the competitive athlete their eligibility. The clinician who counsels supplements as inherently safe, or who fails to ask the competitive athlete about their supplement regimen, misses the chance to prevent the inadvertent positive. The safeguard is the supplement-risk conversation and the recommendation of third-party-tested products. The pitfall of the abrupt cessation is the iatrogenic error, in which a well-meaning clinician or parent insists on immediate stopping and precipitates the hypogonadal crash, and the safeguard is the slow, supported taper with a mental-health safety net. The fellowship answer names these pitfalls and their safeguards, because the harm is as often in the response as in the use. [9] [4]
Prognosis & Disposition
The prognosis is shaped by what was used, for how long, and how it is stopped. The reversible harms recover with cessation and time: the gonadal axis often recovers, the lipid profile improves, the blood pressure falls, the acne resolves, and the mood stabilises as the suppressed brain and body re-equilibrate. The partially reversible harms recover slowly and incompletely in some, with the gonadal recovery taking months and the fertility concern persisting in the long-term heavy user. The irreversible harms are the paediatric stakes: the growth-plate fusion that has already shortened the final adult height cannot be undone, and the cardiovascular structural changes may leave a residual risk. [1] [4]
The psychiatric prognosis is the dimension that most determines the outcome, because the mood and suicide risk of the withdrawal and the dependence that sustains relapse are the morbidity the clinician can most influence. The adolescent who stops with a supported plan, a safety net, and follow-up does better than the one who stops abruptly and alone, and the prevention of relapse depends on the engagement of the pressures and the vulnerabilities that drove the use. The recurrence risk is real, because the environment that drove the use persists, and the disposition must therefore include a plan for the sporting and social environment, not only for the individual. [6] [5]
The disposition is shared among the paediatrician or adolescent-medicine physician, the mental-health service, the dietitian and the strength-and-conditioning professional, and the sporting environment. The physician owns the assessment, the counselling, the cessation plan, and the follow-up, and coordinates the team. The mental-health service owns the depression and suicide-risk management and the dependence treatment. The dietitian and the strength professional build the safe replacement that meets the goal without the harm. The coach and the sporting body own the prevention and the environment. The fellowship answer frames the disposition as a supported, multi-professional exit from use, because the young athlete who leaves use alone relapses. [7] [8]
Special Populations
In Australia and New Zealand the anti-doping framework is administered by Sport Integrity Australia and Drug Free Sport New Zealand on behalf of the World Anti-Doping Agency, and the competitive young athlete is governed by the same prohibited list and the same strict-liability principle that applies internationally. The clinician in Australasia counsels the competitive athlete on the local supplement-risk resources, on the therapeutic-use exemption process for legitimate medications, and on the support services available through the sporting bodies, and frames the conversation within the regional framework the athlete actually faces. [9] [2]
The adolescent from a socioeconomically disadvantaged background or from a community with limited access to sport-science and nutrition support may be more vulnerable to the gym mythology that surrounds performance-enhancing substances, because the credible information and the safe supplementation are less accessible. The online marketplace sells androgens without a prescription across communities, and the absence of a trusted source of advice leaves the young athlete to the locker-room and the internet. The clinical pathway for this group prioritises access to credible information, to the safe replacement strategy, and to the mental-health support that the use may be masking, and it frames the harm within the social determinants that shape it. [10] [7]
The adolescent who belongs to a gender or sexual minority, and the adolescent engaged with youth-justice services, carry additional layers of body-image, identity, and risk behaviour that intersect with performance- and image-enhancing drug use, and the clinician screens these groups with the same confidential, non-judgemental approach and with particular attention to the mental-health and blood-borne-virus dimensions. The Indigenous young athlete, in the Australasian context, may face additional pressures of representation and expectation within community sport, and the culturally safe consultation that builds trust is the prerequisite for the disclosure that the management depends on. The fellowship answer names these groups and adapts the approach to each, because the single standardised response misses the young person in front of the clinician. [10] [6]
Evidence, Guidelines & Regional Differences
The evidence base rests on a small number of landmark studies that the fellowship candidate must cite by name. The Calfee and Fadale review in Pediatrics established the clinical framing of ergogenic drugs and supplements in young athletes and remains the readable entry point for the paediatric clinician. The Irving Project EAT study quantified the prevalence of steroid use among adolescents, and the Sagoe global meta-analysis placed the lifetime prevalence of anabolic-androgenic steroid use in its population context. The Holland-Hall review in the Pediatric Clinics framed the office-based detection of the adolescent user, and the Mulcahey review set out the risk identification and the prevention strategies. [1] [3]
The prevention and the supplement evidence frame the intervention. The Goldberg ATLAS trial in JAMA remains the landmark evidence that a multidimensional, team-centred prevention intervention reduces the intent to use and the actual use of anabolic steroids among adolescent athletes, and it is the model the clinician cites when prevention is discussed. The Nieper and Jovanov supplement studies documented the near-universal supplement use among young athletes and the knowledge gaps that drive it, and the Kozhuharov review established dietary supplements as a documented source of unintentional doping, which underpins the supplement-contamination counselling. The Edenfield review framed the pearls and pitfalls of the sports-supplement consultation. [5] [9]
The guideline framework is the World Anti-Doping Agency prohibited list and the principle of strict liability, which govern the competitive athlete internationally, and the regional anti-doping organisations, Sport Integrity Australia and Drug Free Sport New Zealand in the Australasian context, which administer it locally. The controversies are the adequacy of supplement regulation that permits contamination, the balance between anti-doping sanction and harm-reduction in the underage user, and the tension between the therapeutic alliance and the reporting obligations that some jurisdictions impose. The fellowship candidate frames the topic within the WADA framework while holding the paediatric harm-reduction principle that governs the non-competitive gym user, and cites the verified evidence rather than the gym mythology. [6] [10]
Exam Pearls
The fellowship answer turns on five facts. Performance-enhancing substances span a spectrum from permitted ergogenic aids such as creatine and caffeine to prohibited androgens and image-enhancing hormones, and the World Anti-Doping Agency prohibited list and the principle of strict liability govern the competitive athlete. Anabolic-androgenic steroids dominate illicit use, and the still-growing adolescent pays a unique cost because aromatisation to oestrogen fuses the growth plates early and can shorten final adult height. The cardiovascular, hepatic, endocrine, and psychiatric harms are real, the dependence is established, and the withdrawal can beget suicidal ideation. The diagnosis rests on a confidential, non-judgemental history rather than on blood tests. And the management is counselling-first, harm-reduction-first, with a slow and supported cessation and the ATLAS prevention model. [1] [6]
The examiner probes three traps. The first is the punitive response that drives the use underground and ends the alliance, and the safeguard is the non-judgemental, harm-reducing stance that keeps the adolescent in care. The second is the abrupt cessation that precipitates the hypogonadal crash and the suicidal risk, and the safeguard is the slow, supported taper with a mental-health safety net. The third is the unrecognised supplement contamination that costs the competitive athlete their eligibility under strict liability, and the safeguard is the supplement-risk conversation and the third-party-tested product. The candidate who names these traps and their safeguards demonstrates the systems thinking the examination rewards. [4] [9]
The examiner rewards the candidate who frames performance-enhancing substance use as a paediatric and adolescent-medicine problem as much as a sports-medicine one, because the morbidity lives in the still-growing body and the still-maturing brain. The young athlete is screened confidentially, the harm is quantified, the cessation is supported and gradual, the safe replacement meets the goal, and the prevention engages the environment. A candidate who shows this breadth, who cites the ATLAS evidence and the WADA framework, and who holds the harm-reduction principle alongside the strict-liability rule demonstrates the integrated answer the fellowship demands. [5] [7]
References
- [1]Calfee R, Fadale P. Popular ergogenic drugs and supplements in young athletes. Pediatrics, 2006.PMID 16510635
- [2]Nieper A. Nutritional supplement practices in UK junior national track and field athletes. British Journal of Sports Medicine, 2005.PMID 16118303
- [3]Irving LM, Wall M, Neumark-Sztainer D, Story M. Steroid use among adolescents: findings from Project EAT. Journal of Adolescent Health, 2002.PMID 11927236
- [4]Sagoe D, Molde H, Andreassen CS, Torsheim T, Pallesen S. The global epidemiology of anabolic-androgenic steroid use: a meta-analysis and meta-regression analysis. Annals of Epidemiology, 2014.PMID 24582699
- [5]Goldberg L, Elliot D, Clarke GN, MacKinnon DP, Moe E, et al. Effects of a multidimensional anabolic steroid prevention intervention. The Adolescents Training and Learning to Avoid Steroids (ATLAS) Program. JAMA, 1996.PMID 8918852
- [6]Mulcahey MK, Schiller JR, Hulstyn MJ. Anabolic steroid use in adolescents: identification of those at risk and strategies for prevention. The Physician and Sportsmedicine, 2010.PMID 20959703
- [7]Holland-Hall C. Performance-enhancing substances: is your adolescent patient using? Pediatric Clinics of North America, 2007.PMID 17723868
- [8]Jovanov P, Dordevic V, Obradovic B, Barak O, et al. Prevalence, knowledge and attitudes towards using sports supplements among young athletes. Journal of the International Society of Sports Nutrition, 2019.PMID 31272457
- [9]Kozhuharov VR, Ivanov K, Ivanova S. Dietary Supplements as Source of Unintentional Doping. BioMed Research International, 2022.PMID 35496041
- [10]Ganson KT, Alebraheem Z, Coelho J, Fournier C, et al. Appearance- and Performance-Enhancing Drugs and Substances Use Among Adolescents: Physician Reports. Academic Pediatrics, 2026.PMID 41724323
- [11]Edenfield KM. Sports Supplements: Pearls and Pitfalls. Primary Care, 2020.PMID 32014135