Paeds · rheumatology-musculoskeletal-and-sports
Perthes disease
Also known as Legg-Calve-Perthes disease · Perthes' disease · coxa plana · idiopathic avascular necrosis of the capital femoral epiphysis · osteochondritis of the femoral head
A fellowship approach to Legg-Calve-Perthes disease: idiopathic avascular necrosis of the capital femoral epiphysis in the four-to-eight-year-old child, the four radiographic phases of necrosis through fragmentation to reossification and remodeling, the Herring lateral pillar classification that drives prognosis, and the containment principle that keeps the soft femoral head moulded within the acetabulum during reossification.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A six-year-old boy limps into your clinic. His mother says the limp has been present for three weeks, comes and goes, is worse after activity, and that the boy sometimes points to his knee rather than his hip. He is afebrile, well in himself, and on examination he has a mild antalgic gait and a hip that loses abduction and internal rotation. His radiograph shows a slightly smaller, denser right femoral head with a faint subchondral line. You recognise Perthes, you confirm the lateral pillar grade in the fragmentation phase, and you refer for a containment decision based on his age and his pillar height. A nine-year-old girl presents the same way but her head is already collapsing — older age at onset is the single strongest poor prognostic factor, and her window for containment is narrow. [4] [2]
The four phases — Necrosis, Fragmentation, Reossification, Remodeling
Overview & Definition
Legg-Calve-Perthes disease is the idiopathic avascular necrosis of the capital femoral epiphysis in a growing child. The femoral head loses its blood supply, the bone and marrow die, and the body then resorbs the dead bone and replaces it with new bone over a course of eighteen to thirty-six months. The disease is self-limiting in that it always heals, but the shape of the healed head determines whether the child enters adult life with a normal hip or with a flattened head destined for early osteoarthritis. The illness is named for the three authors who described it independently in 1910 — Legg, Calve, and Perthes. [4] [3]
The clinical hallmark is the persistent limp of a young child. The child is typically a boy between four and eight years old who has limped for weeks, who is often afebrile and well, and whose pain is mild, intermittent, and sometimes referred to the knee or the thigh. The hip examination shows a loss of motion, most reliably a loss of abduction and internal rotation, and a muscle spasm that splints the joint. The contrast with transient synovitis is the key first fork: transient synovitis resolves within a week or two, while Perthes persists and progresses, and any limp that lasts beyond two to three weeks in this age group is Perthes until the radiograph and the clinical course settle the question. [4] [3]
The disease stands apart from the other causes of the limping child because it is chronic and because the role of the general paediatrician is to recognise it early, exclude the urgent mimics, and refer for a containment decision based on age and lateral pillar grade. The mistake to avoid is to accept the limp as a minor injury or to discharge the child with a diagnosis of transient synovitis when the limp has persisted. The safeguard is the rule that a limp beyond two to three weeks in a four-to-eight-year-old earns a hip radiograph and, if the picture fits, a referral. [4]
Classification
Perthes disease is classified along two axes that every fellowship candidate must hold separately: the radiographic phase the disease is in, and the lateral pillar grade that predicts the outcome. The Waldenstrom radiographic phases describe the temporal evolution — the initial or necrosis phase, the fragmentation phase, the reossification phase, and the remodeling or healed phase. The lateral pillar grade is assigned during the fragmentation phase, because that is when the height of the lateral third of the femoral head can be read most reliably, and it is the single most important prognostic variable. [1] [4]
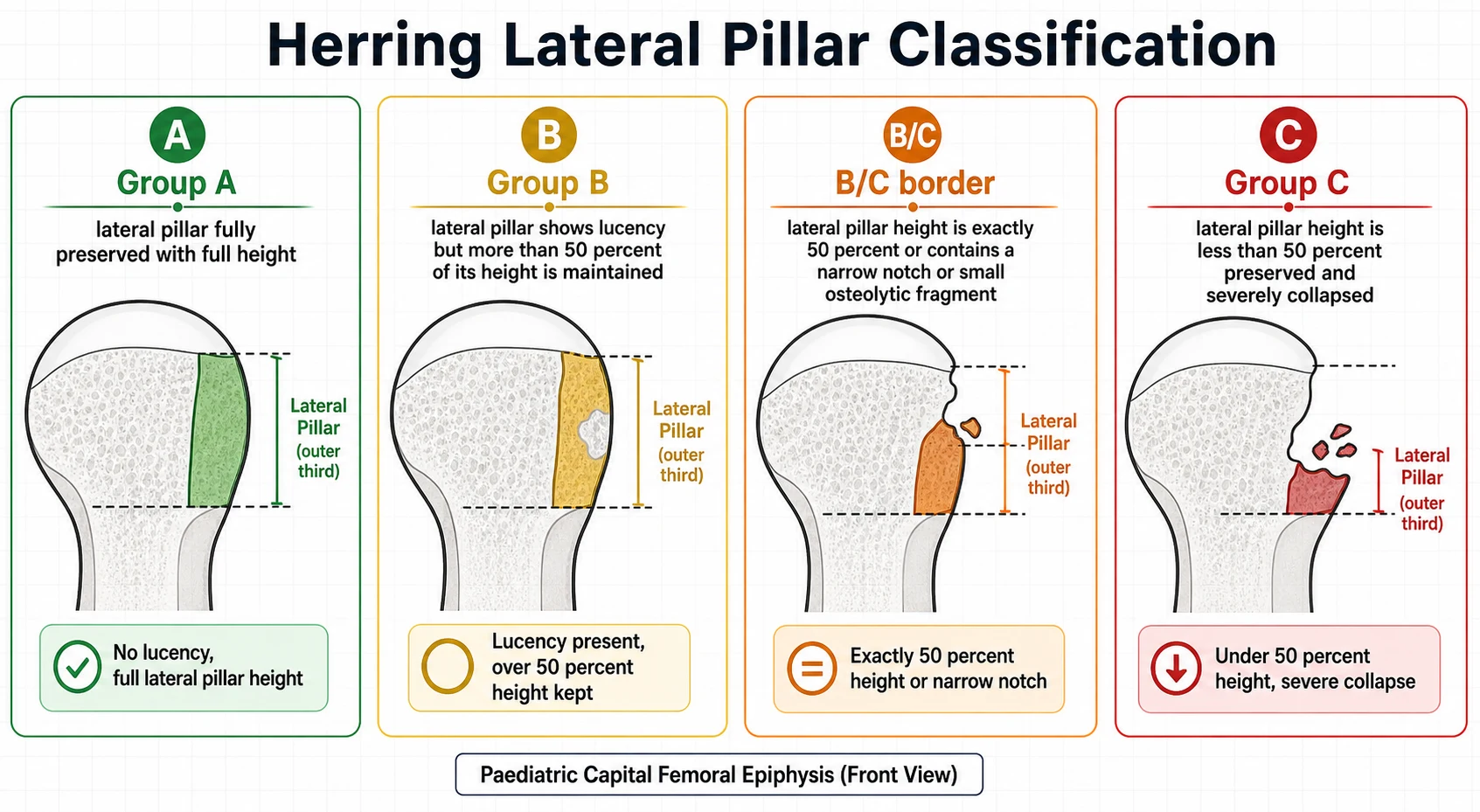
The Herring lateral pillar classification grades the height of the lateral pillar of the femoral head on the anteroposterior radiograph of the hip during the fragmentation phase. The femoral head is divided mentally into three pillars — medial, central, and lateral — and the lateral pillar is the outer third. Group A means the lateral pillar is fully preserved with no lucency and full height. Group B means the lateral pillar shows lucency but maintains more than fifty per cent of its original height. Group C means the lateral pillar has collapsed to less than fifty per cent of its height. The B/C border describes the head whose lateral pillar is at exactly fifty per cent, or that shows a narrow notch or a small osteolytic fragment at its outer edge, and it is the grade around which the surgical decision turns. [1]
The older classifications still appear in examination answers and a candidate should know them by name. The Catterall classification grades the extent of head involvement into four groups from I to IV, with higher groups meaning more of the head is involved, and it introduced the head-at-risk signs — lateral calcification, lateral subluxation, metaphyseal widening, and a horizontal growth plate — that warn of a poor outcome. The Salter-Thompson classification uses the extent of the subchondral resorption line, the crescent sign, to predict involvement, with type A meaning less than half the head and type B meaning more than half. These classifications are less reproducible than the lateral pillar system and they have been overtaken by it in modern practice, but they remain fair examination material. [4]
The Stulberg classification is the outcome classification, applied at skeletal maturity, and it is the measure by which the success of treatment is judged. Stulberg I and II are spherical or ovoid heads that are congruent with the acetabulum and carry a low risk of osteoarthritis. Stulberg III is an ovoid head, Stulberg IV is a flat head that remains congruent with a flat acetabulum, and Stulberg V is a flat head that is incongruent, and the higher Stulberg grades carry the rising lifetime risk of osteoarthritis. The Huhnstock twenty-year follow-up confirmed that the Stulberg grade is a strong predictor of the long-term radiological outcome. [9]
Epidemiology & Risk Factors
Legg-Calve-Perthes disease affects roughly one in one thousand two hundred children, with regional variation that ranges from one in seven hundred in some Northern European populations to one in several thousand in others. Boys outnumber girls by about four to one, and the typical age at onset is between four and eight years, with the peak around six. The disease is bilateral in roughly ten to twenty per cent of children, and the bilateral case is distinguished from Meyer dysplasia, the benign self-limiting dysplasia of the under-fours, by the age and the clinical course. [4] [3]
The risk factors cluster around skeletal maturity and body habitus. Affected children are often small for their age with a delayed bone age, and the delayed maturation is thought to render the capital femoral epiphysis more vulnerable to a vascular insult. An association with attention-deficit hyperactivity disorder, with minor congenital anomalies, and with a low birth weight has been described, although no single cause has been established. The disease is genuinely idiopathic, and the candidate should resist the temptation to over-commit to a thrombophilia explanation, because the evidence for a consistent clotting abnormality is weak and inconsistent. [4] [11]
An excess of body weight has emerged as a reproducible risk factor. Neal and colleagues showed that the prevalence of obesity is significantly higher among children with Legg-Calve-Perthes disease than in the general paediatric population, and the proposed mechanism is that the greater mechanical load on an already-vulnerable epiphysis worsens the collapse during the fragmentation phase. Secondhand smoke exposure has been associated with the disease in some studies, again on a vascular basis, but the association is weaker than the obesity signal. These epidemiological threads matter less for the individual patient than the two hard prognostic facts: the age at onset and the lateral pillar grade. [10]
Pathophysiology
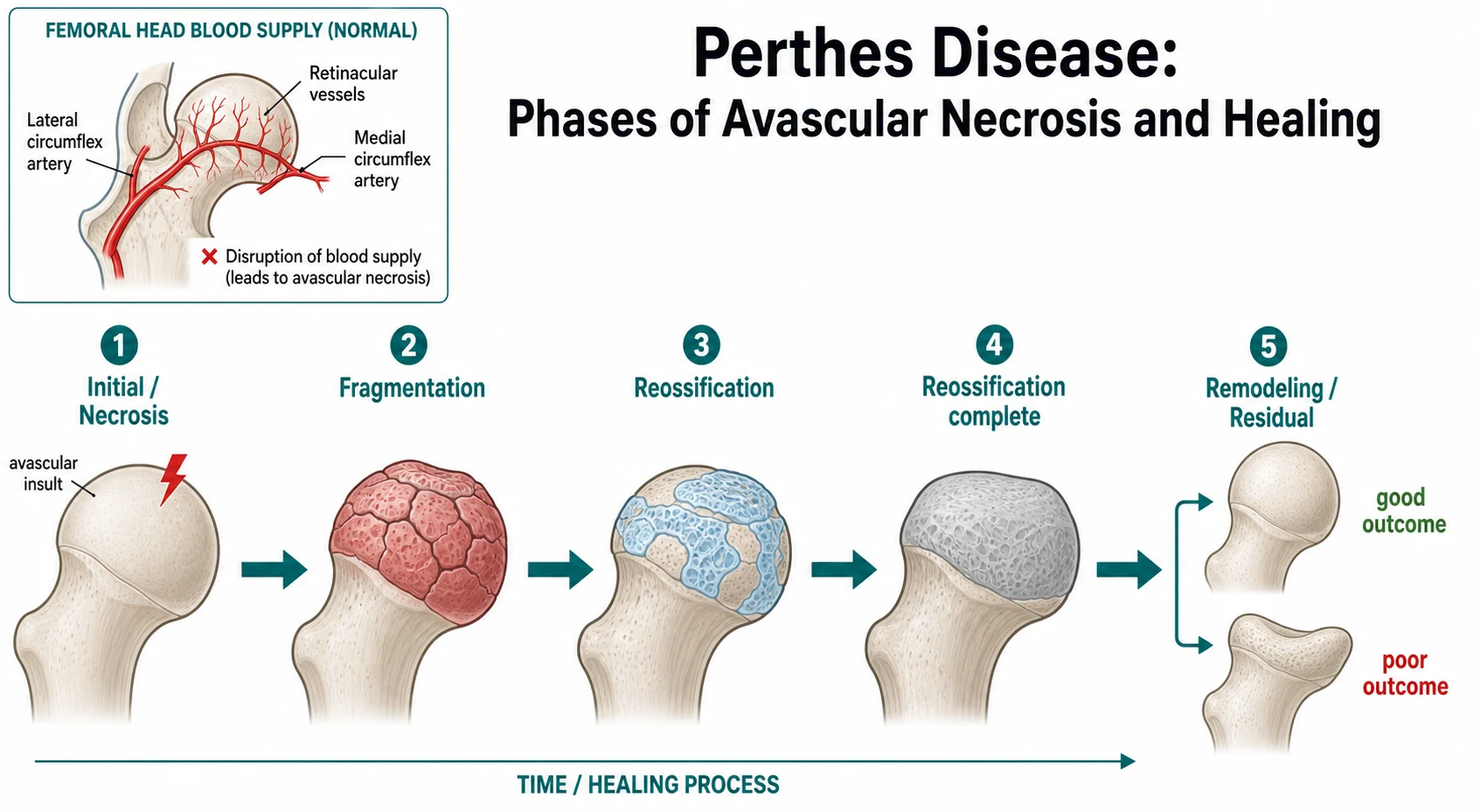
The pathophysiology of Perthes disease is the interruption of the blood supply to the capital femoral epiphysis, followed by the orderly death and rebirth of the femoral head. In the growing child the femoral head receives its blood from the medial and lateral circumflex femoral arteries, whose retinacular branches run along the femoral neck and enter the epiphysis at its periphery, because the growth plate blocks a direct supply from the metaphysis. This tenuous, peripherally entering supply is the structural reason the child's femoral head is vulnerable — a single or recurrent interruption leaves the head without a collateral route, and the bone and the marrow die. [8] [4]
The sequence that follows the ischaemic insult is the four-phase course that defines the disease. In the necrosis phase the dead bone retains its architecture on the radiograph and may even look denser, because the surrounding living bone continues to remodel while the dead bone cannot. In the fragmentation phase the body resorbs the dead bone, the head loses structural integrity, and it collapses and fragments under load — this is the phase of lateral pillar loss and the phase in which the head is soft and mouldable. In the reossification phase the new bone creeps into the head by vascular invasion, and in the remodeling phase the healed head is reshaped over years toward, or away from, a sphere. [3] [8]
The perfusion work of Kim and colleagues gave the ischaemic basis a measurable correlate. Using perfusion magnetic resonance imaging in the early stage of the disease, they demonstrated reduced blood flow to the femoral head that predicted the subsequent lateral pillar involvement, which links the unseen vascular insult to the radiographic pillar grade that drives the prognosis. The disease is therefore best understood as a vascular event whose severity — how much head dies and how much pillar collapses — sets the clinical course, and the candidate who frames Perthes as an ischaemic, self-healing, shape-determining disease has the right model. [8] [1]
The timing of the insult is itself a clue to the disease. Loder and colleagues modelled the age distribution of affected children and inferred that the triggering vascular event occurs some months before the limp appears, which explains why the first radiograph may already show sclerosis and why the limp often seems to begin after a minor injury that merely drew attention to a head already in trouble. This incubation logic also frames the bilateral disease and the delayed bone age as features of a systemic predisposition rather than of a single accident. [11]
Clinical Presentation
The presentation of Perthes disease is shaped by the age of the child, the mildness of the pain, and the tendency of the pain to refer away from the hip. The classical patient is a boy between four and eight years old with a limp that has been present for two to four weeks, often worse after activity and relieved by rest. The pain is mild, intermittent, and frequently absent, and the child is well in himself and afebrile, which is the contrast with the infected joint that demands urgent action. Many parents date the limp to a minor fall, and the fall is usually coincidental rather than causal. [4] [3]
The pain of a hip joint is often felt in the knee or the thigh rather than the groin, because the hip and the knee share the obturator and femoral nerve supply, and the fellowship rule holds: any child with knee pain receives a hip examination. The parent may report only that the child limps and points to the knee, and the unwary clinician who examines only the knee misses the stiff hip that is the source. The limp is typically antalgic, shortening the stance phase on the affected side, and in later disease a Trendelenburg limp appears as the abductors fail on the unstable head. [4]
The hip examination reveals the loss of motion that is the physical signature of the disease. The child loses abduction and internal rotation first, because the inflamed and then the deformed head is most compressed in these positions, and the loss is best demonstrated by comparing the two hips in flexion. A fixed flexion or an adduction contracture may develop, and the child holds the hip in a position of comfort — slight flexion and external rotation — that maximises the capsular volume. Muscle spasm and guarding are common in the early and fragmentation phases, and they settle as the disease enters reossification. [3] [4]
Which reassuring-sounding presentations must never close the search? A limp attributed to a minor injury may be Perthes, and the history of a fall does not exclude it. A child who limps but is afebrile and well may still have Perthes, because the disease is not a febrile illness. A normal early radiograph does not exclude Perthes, because the sclerosis and fragmentation take weeks to declare. And a child whose pain improves with simple analgesia may still have a head that is collapsing, because the collapse is mechanical rather than inflammatory. The persistent limp, the stiff hip, and the radiograph together settle the diagnosis. [4] [3]
Differential Diagnosis
The differential diagnosis of the limping four-to-eight-year-old child spans the transient, the infectious, the developmental, and the malignant, and the fellowship candidate holds them in parallel. Transient synovitis is the commonest mimic and the safest one, a self-limiting post-viral irritable hip that resolves within one to two weeks with rest and simple analgesia. The distinction is the duration: transient synovitis resolves, Perthes persists, and the limp that lasts beyond two to three weeks earns the radiograph that separates them. [4] [3]
Septic arthritis is the urgent mimic that must never be missed, because a delay of hours compromises the joint. The septic child is febrile, unwell, and holds the joint rigid in the position of maximum capsular volume, and the inflammatory markers are high, with a C-reactive protein often above twenty milligrams per litre or higher in the florid case. The Kocher prediction rule risk-stratifies the irritable hip, and a child who meets high-risk criteria receives joint imaging and aspiration before Perthes is considered, because a hot, septic joint and a cold, avascular head are opposite emergencies. [4]
Slipped capital femoral epiphysis is the mimic of the older child and the adolescent, and the age overlap at the upper end of the Perthes range is the trap. The slipped epiphysis presents in the overweight eleven-to-fifteen-year-old with a limp and an externally rotated leg, and the radiograph shows the posterior and inferior slip of the capital epiphysis on the neck, best seen on the frog-lateral view. The two diseases share a limp and a stiff hip, but the age, the body habitus, and the radiograph separate them, and missing a slip because it was labelled Perthes delays the urgent stabilisation that the slip demands. [4]
The inflammatory and the malignant mimics complete the list. Juvenile idiopathic arthritis may present with a chronic hip effusion and stiffness, and the morning stiffness, the other-joint involvement, and the elevated inflammatory markers point the way. Meyer dysplasia affects children under four, is often bilateral, runs a mild self-limiting course, and is distinguished from bilateral Perthes by the age and the benign outcome. Leukaemia and bone tumours may present with bone pain and a limp, and the abnormal blood film, the night pain, and the destructive radiographic lesion prompt the further workup that these diagnoses demand. [4] [3]
Clinical & Bedside Assessment
The bedside assessment begins with the general appearance and the gait, because the well, afebrile child with a chronic limp points toward Perthes while the febrile, toxic child points toward sepsis. The child is observed walking, and the limp is characterised — antalgic, with a short stance phase, or Trendelenburg, with a dipping of the shoulder toward the affected side. The leg length is measured, because a true shortening from a collapsed head or an apparent shortening from an adduction contracture may develop in later disease. The temperature, the ease of the child, and the presence of any systemic features are noted, because their absence supports the Perthes diagnosis and their presence redirects toward infection. [4]
The hip examination is systematic and always bilateral, with the normal hip as the comparator. The child lies supine, and each hip is taken through flexion, abduction, adduction, and internal and external rotation, comparing the two sides for the asymmetry that reveals the stiff hip. The loss of abduction and internal rotation is the earliest and the most reliable finding, demonstrated by flexing both hips to ninety degrees and abducting them together toward the table. A fixed external rotation contracture, a palpable effusion, and the warmth of an inflamed joint are sought, and the knee and the spine are examined to exclude a referred source. [3] [4]
The bedside laboratory assessment is largely a tool to exclude the mimics rather than to confirm Perthes, because the bloods are typically normal in the disease. A full blood count, a C-reactive protein, and an erythrocyte sedimentation rate are sent to exclude septic arthritis and inflammatory arthritis, and they are reassuringly normal in the uncomplicated case. The Kocher prediction rule is applied to the irritable hip when septic arthritis is a possibility, and a child who scores highly on fever, inability to bear weight, a high white cell count, and a high C-reactive protein is managed as septic until proven otherwise. Perthes is a diagnosis made on the history, the examination, and the radiograph, not on the bloods. [4]
Which findings must never be dismissed? A fever with a stiff hip is not Perthes until sepsis is excluded. A child who cannot bear weight at all and who holds the joint rigid is not the typical Perthes picture. A limp with night pain that wakes the child from sleep is a red flag for malignancy, not for an avascular head. And a rapidly progressive limp with a destructive radiographic lesion demands the further imaging and the biopsy that the malignancy workup requires. The bedside assessment is the filter that sends the right child to the right pathway. [4]
Investigations
The investigation of suspected Perthes disease rests on the plain radiograph, supported by magnetic resonance imaging in selected cases, and the radiograph is both the diagnostic and the staging tool. The standard views are an anteroposterior pelvis and a frog-lateral view of both hips, and the two views together reveal the lateral pillar grade, the phase of the disease, and the head-at-risk signs. The earliest radiographic change is a widened medial joint space and lateralisation of the head, followed by the subchondral fracture line — the crescent or Salter sign — that is the radiographic hallmark of the necrotic phase. [4] [3]
The fragmentation phase that follows shows increasing sclerosis, then patchy lucency, and finally the fragmentation and the loss of height of the femoral head that allow the lateral pillar grade to be assigned. The reossification phase shows the new bone creeping in from the periphery, the head becoming progressively denser and more solid, and the remodeling phase shows the gradual reshaping of the healed head. A normal early radiograph does not exclude Perthes, because the sclerosis and the fragmentation take weeks to declare, and a child with a persistent limp and a normal film is re-imaged or sent for magnetic resonance imaging. [3] [8]
Magnetic resonance imaging has a growing role in the early and the uncertain case. Perfusion magnetic resonance imaging, as studied by Kim and colleagues, demonstrates the reduced blood flow to the femoral head in the earliest stage of the disease and predicts the lateral pillar involvement before the plain radiograph changes, and it is the modality that confirms Perthes when the radiograph is normal but the limp is persistent. Magnetic resonance imaging also assesses the articular cartilage, the extent of the involvement, and the presence of hinge abduction, and it guides the containment decision in the borderline case. [8]
Bone scintigraphy has largely been supplanted by magnetic resonance imaging for the early diagnosis, but it remains a tool in settings where magnetic resonance imaging is unavailable, and it shows the photopenic defect of the avascular head. Ultrasound may detect a hip effusion and exclude transient synovitis or septic arthritis, but it does not assess the femoral head itself. The laboratory tests are directed at the mimics: a full blood count and inflammatory markers exclude infection and inflammation, and they are normal in the uncomplicated Perthes case. The diagnosis is radiographic, and the staging is by phase and by lateral pillar grade. [4] [8]
Management — Resuscitation
Perthes disease is not a resuscitation emergency in the way that septic arthritis is, and the opening priority is the safe exclusion of the diagnoses that demand urgent action. The febrile, toxic, or Kochar-high-risk child with an irritable hip is managed as septic arthritis until proven otherwise, with joint imaging, aspiration, and empirical antibiotics as the pathway dictates, and Perthes is considered only once infection is excluded. The child with a slip is kept non-weight-bearing and referred for urgent fixation, because the unstable slip can progress to a devastating acute-on-chronic displacement. [4]
The first analgesic and functional management of the confirmed Perthes case is symptom relief and the protection of the soft head. Simple analgesia, such as oral paracetamol or a non-steroidal anti-inflammatory drug, controls the pain of the irritable phase, and activity modification reduces the load on the collapsing head. The child is encouraged to avoid high-impact activities, and a brief period of rest or protected weight-bearing is used in the painful fragmentation phase. These measures do not alter the natural history of the disease, but they keep the child comfortable and mobile while the lateral pillar grade declares itself and the containment decision is made. [4]
The early containment decision runs in parallel with the symptomatic management, because the window for containment is the fragmentation and the reossification phases, and it cannot be recovered once the head has healed in a poor shape. The general paediatrician's role is to recognise the disease, exclude the urgent mimics, grade the lateral pillar in the fragmentation phase, and refer early to the paediatric orthopaedic service for the containment decision based on the age and the pillar height. The decision is not made at the first visit in every case, because the pillar grade must declare itself, but the referral is made early. [1] [4]
Management — Definitive & Stepwise
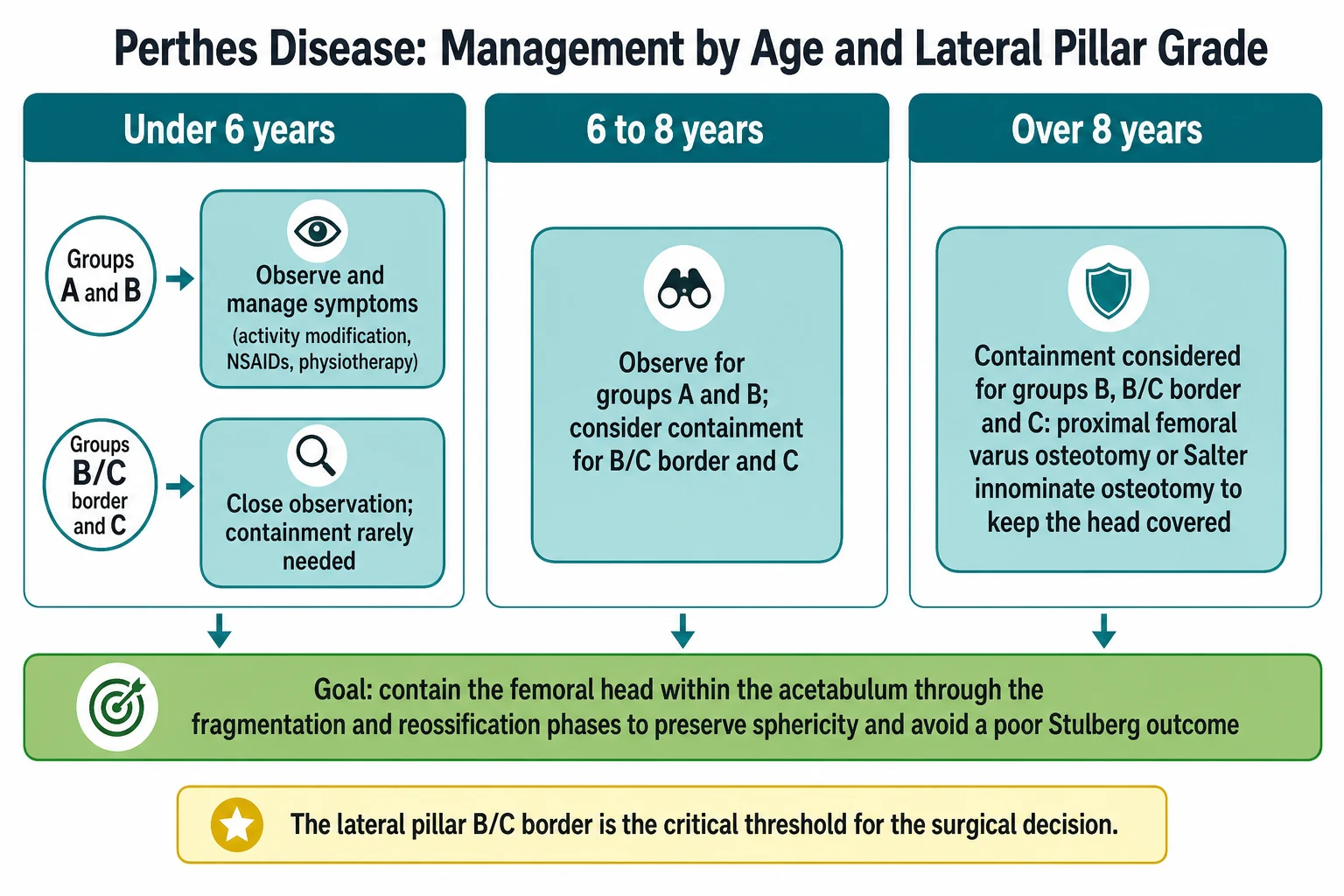
The definitive management of Perthes disease turns on the containment principle and on two variables: the age of the child and the lateral pillar grade. Containment means keeping the soft, mouldable femoral head within the acetabulum during the fragmentation and the reossification phases, so that the acetabulum acts as a mould and the head heals spherical rather than flat. Containment is achieved either on the femoral side, by a proximal femoral varus osteotomy that medialises the greater trochanter and deepens the head beneath the acetabulum, or on the acetabular side, by a Salter innominate osteotomy that redirects the acetabular roof over the head. [1] [4]
The Herring multicentre prospective study is the evidence that anchors the containment decision. It found that children eight years and older at onset, by bone age, with lateral pillar B and C involvement, had better Stulberg outcomes when treated with surgical containment than when treated without, while children under six at onset did well regardless of treatment. The B/C border in the six-to-eight-year age band is the grade around which the decision is most finely balanced, and it is the grade that the examiner probes. The study established that not every child needs surgery, that age and pillar grade together drive the decision, and that over-treatment of the young, mild case is as much an error as under-treatment of the older, severe case. [1]
The surgical options each have their place. The proximal femoral varus osteotomy works on the femoral side, and Kim and colleagues defined the degree of varus needed to preserve the head, while Terjesen and colleagues showed that the varus osteotomy improves the sphericity of the head in older children with severe disease. The Salter innominate osteotomy works on the acetabular side, redirecting the roof over the head, and it is preferred when the head is already well contained but the coverage is marginal. The choice between them is a surgical judgement that depends on the congruency of the joint, the direction of the subluxation, and the surgeon's experience, and the general paediatrician's task is to refer in time for that judgement to be made. [6] [7]
The containment decision by age and lateral pillar grade
The non-containment options remain relevant in selected cases. A period in an abduction brace or a Petrie cast — a bilateral cylinder cast holding the hips in abduction and internal rotation — is used to maintain head coverage in some centres, and it may precede or substitute for surgery in the child who is too young or whose head is not yet declared. The long-term follow-up of Larson and colleagues, reporting the twenty-year outcomes of nonoperative treatment, confirmed that many children do well without surgery, especially the young and the lateral pillar A and B, while the older child and the lateral pillar C fare worse and remain the candidates for intervention. Sankar and colleagues added the caution that an early varus osteotomy does not shorten the fragmentation phase, which tempers any expectation that surgery accelerates healing. [5] [12]
Specific Subtypes & Scenarios
Bilateral Perthes disease is the subtype that affects roughly ten to twenty per cent of children, and it must be distinguished from Meyer dysplasia. Bilateral Perthes presents sequentially, with the two hips often in different phases, and it runs the same phase and pillar course as the unilateral disease. Meyer dysplasia, by contrast, affects children under four, is bilateral from the outset, runs a mild and self-limiting course with minimal symptoms, and resolves without residual deformity, and the age and the benign outcome are the distinguishing features. The bilateral Perthes case is managed hip by hip, with the containment decision made for each side according to its own phase and pillar grade. [4] [3]
The older child at onset is the subtype that demands the most careful management. Children over eight, and particularly those over nine, run a more severe course, because the reduced remodeling potential of the older skeleton leaves the deformed head less able to reshape itself during the healing phase, and the lateral pillar C grade is commoner and more destructive in this group. The Wiig prospective study identified older age, female sex, and lateral pillar C as the independent poor prognostic factors, and the older child is the prime candidate for early containment. The fellow who treats the nine-year-old Perthes as a benign disease of the young misses the narrow window. [2]
The lateral pillar C head is the subtype that defines the severe end of the disease. The collapse of the lateral pillar to less than fifty per cent of its height predicts a poor Stulberg outcome and a high lifetime risk of osteoarthritis, and the head may hinge out of the acetabulum — the hinge abduction that marks the closing of the containment window. The management of the group C head is the containment decision at its sharpest, and the salvage options — a shelf arthroplasty, a Chiari osteotomy, or in the severely deformed head a femoral head osteotomy in later life — enter the discussion when containment has failed or the window has closed. [1] [9]
The child with a late, deformed head is the subtype that presents the long-term consequences. The Stulberg III, IV, and V heads carry the rising risk of premature osteoarthritis, often presenting in the fourth or fifth decade, and the management shifts from containment to the management of the young adult with a painful deformed hip. The arthroplasty options — a hip resurfacing or a total hip replacement in the severely symptomatic — are the late salvage, and the disease is one in which the quality of the paediatric management shapes the adult life. [9]
Complications & Pitfalls
The complications of Perthes disease span the shape of the head, the length of the leg, and the lifetime of the hip. The flattening and the lateral subluxation of the femoral head produce the Stulberg III, IV, and V outcomes that carry the rising risk of premature osteoarthritis, and the degree of the deformity is the single most important determinant of the long-term prognosis. A limb-length discrepancy from a coxa breva — a shortened femoral neck produced by the growth-plate disturbance — is common, and a significant discrepancy is managed with an epiphysiodesis of the longer leg in due course. [9] [4]
Hinge abduction is the mechanical complication that signals the closing of the containment window. When the femoral head has collapsed and broadened beyond the acetabular margin, the abducted hip hinges the deformed head against the acetabular rim, and the head is levered laterally out of the joint rather than rotating within it. The clinical sign is the loss of passive abduction with lateral pain, and the radiographic sign is the lateral extrusion of the head on the abducted view. Hinge abduction is a contraindication to a simple containment osteotomy, because it worsens the levering, and it redirects the management toward salvage. [4] [9]
The pitfall of the missed early diagnosis is the error that most often costs the child the containment window. The limp is attributed to a minor injury, the radiograph is not obtained because the child is well and afebrile, and the diagnosis is made only when the head has already fragmented and the pillar has collapsed. The safeguard is the rule that a limp beyond two to three weeks in a four-to-eight-year-old earns a hip radiograph. The pitfall of the over-treated young child is the opposite error — the child under six with a lateral pillar A or B head is subjected to surgery it does not need, because the natural history in this group is good. The safeguard is the age-and-pillar-guided decision. [1] [4]
The pitfall of the mislabelled septic arthritis is the dangerous error in the other direction. The irritable hip that is labelled Perthes when it is in fact a septic joint loses the hours that the infected joint cannot afford, and the safeguard is the disciplined application of the Kocher criteria and the exclusion of sepsis before Perthes is settled upon. The pitfall of the missed slip in the older child is the related error — the eleven-year-old with a limp is labelled Perthes when the radiograph, unreviewed on the frog-lateral view, shows a slipped capital femoral epiphysis, and the safeguard is the frog-lateral view in every limping child at the upper end of the age range. [4]
Prognosis & Disposition
The prognosis of Perthes disease is dominated by two factors: the age at onset and the lateral pillar grade. The young child, under six at onset, has an excellent prognosis, because the generous remodeling potential of the young skeleton reshapes the head toward a sphere during the healing phase, and the lateral pillar A and B heads in this age group heal well regardless of treatment. The older child, over eight at onset, has a poorer prognosis, because the reduced remodeling potential leaves the deformed head less able to correct itself, and the lateral pillar C grade compounds the outlook. The Stulberg grade at skeletal maturity is the measure of the outcome, and the Huhnstock twenty-year follow-up confirmed it as the strong predictor of the long-term radiological result. [1] [9]
The Wiig prospective study of three hundred and sixty-eight children defined the prognostic factors with the greatest rigour. Age over six at onset, a lateral pillar C grade, and female sex were the independent poor prognostic factors, and a child with all three carries the highest risk of a poor Stulberg outcome and of premature osteoarthritis. The natural history study of Terjesen and colleagues added the long-term perspective, showing that the disease is more severe in the older child and that the residual deformity persists into adult life. The prognosis is not a single number but a synthesis of the age, the pillar grade, the sex, and the achieved sphericity. [2] [3]
The disposition is shared between the general paediatrician and the paediatric orthopaedic surgeon. The general paediatrician owns the recognition, the exclusion of the urgent mimics, the grading of the lateral pillar in the fragmentation phase, and the timely referral. The paediatric orthopaedic surgeon owns the containment decision, the choice between observation, bracing, and surgery, the execution of the osteotomy, and the long-term follow-up through to skeletal maturity. The physiotherapist supports the range of motion and the gait, and the family is counselled on the long course of the disease, the activity modification, and the expected outcome. [4] [1]
The long-term outlook is shaped by the residual head shape and the patient's expectations. The Stulberg I and II heads carry a low risk of osteoarthritis and a normal functional life, while the Stulberg III, IV, and V heads carry a rising risk of symptomatic arthritis that often presents in the fourth or fifth decade. The fellowship answer frames Perthes as a disease whose paediatric management shapes the adult hip, and the candidate who conveys this long view demonstrates the systems thinking that the examination rewards. [9] [5]
Special Populations
The child in a rural or remote community faces the challenge of distance from the paediatric orthopaedic service and from magnetic resonance imaging, and the clinical pathway must incorporate the principles of retrieval and telehealth. The general paediatrician in the remote setting makes the diagnosis on the history, the examination, and the plain radiograph, grades the lateral pillar to the extent possible, excludes the urgent mimics, and initiates the referral and the symptomatic management while the retrieval and the specialist consultation are arranged. The early containment window is the same in the remote child as in the urban child, and the distance must not delay the referral. [4]
The child from a socioeconomically disadvantaged background may present later in the disease course, because the access to primary care and the threshold for seeking attention for a limp that seems minor both delay the presentation. The delayed presentation is the specific risk for this group, because the containment window may have narrowed or closed by the time the diagnosis is made, and the lateral pillar grade may already be a C. The clinical pathway for the disadvantaged child prioritises the early recognition of the limp, the prompt radiograph, and the facilitated referral, and the social determinants of the delayed presentation are part of the fellowship answer. [4]
The child with bilateral disease and the older child at the upper end of the age range are the special populations that the general paediatrician must flag early. The bilateral case demands a hip-by-hip management plan and a watch for the Meyer dysplasia distinction in the very young, and the older child demands an early containment referral because the natural history is worse. The fellowship answer names these groups and the urgency of their referral, and it resists the temptation to treat every Perthes case as a single benign disease of the young. [4] [2]
Evidence, Guidelines & Regional Differences
The evidence base for Perthes disease rests on a small number of large prospective studies that have shaped the modern management. The Herring multicentre prospective study, published in two parts, established the lateral pillar classification and demonstrated that surgical containment improves the Stulberg outcome in children eight years and older at onset with lateral pillar B and C involvement, while children under six do well regardless. This study is the definitive contemporary reference for the containment decision, and it is the paper the fellowship candidate must cite. [1]
The Norwegian prospective series has generated a parallel body of evidence. The Wiig prospective study of three hundred and sixty-eight children defined the prognostic factors — age over six, lateral pillar C, and female sex — and the natural history study of Terjesen and colleagues described the long-term course. The Huhnstock twenty-year follow-up confirmed the modified Stulberg classification as a strong predictor of the long-term radiological outcome, and the varus osteotomy studies of Terjesen and of Kim defined the role and the degree of the femoral-side containment. The American multicentre follow-up of Larson and colleagues reported the twenty-year outcomes of nonoperative treatment and tempered the move toward universal surgery. [2] [5] [6] [7]
The perfusion imaging evidence is the modern addition. The Kim perfusion magnetic resonance imaging study demonstrated the reduced blood flow to the femoral head in the earliest stage and its prediction of the lateral pillar involvement, grounding the disease in a measurable ischaemic basis. The Sankar multicentre cohort added the caution that an early varus osteotomy does not shorten the fragmentation phase, which is an honest correction of an earlier assumption. The Loder incubation modelling framed the timing of the insult, and the Neal obesity study added the body-habitus risk factor. [8] [12] [11] [10]
The regional differences are modest. The availability of paediatric orthopaedic services and of magnetic resonance imaging varies by setting, and the rural or remote clinician relies on the plain radiograph and the clinical judgment while arranging the referral and the retrieval. The thresholds for containment are broadly consistent across the major guidelines, which draw on the same Herring and Wiig evidence, and the controversies are the surgical decision in the B/C border and the six-to-eight-year age band, the role of bracing, and the management of the late deformed head. The Herring review at the centenary of the disease summarised the evidence-based treatment and remains the readable entry point. [4] [1]
Exam Pearls
The fellowship answer turns on five facts. Perthes disease is the idiopathic avascular necrosis of the femoral head in a four-to-eight-year-old boy with a persistent limp. The disease runs the four phases of necrosis, fragmentation, reossification, and remodeling over eighteen to thirty-six months, and the shape of the healed head sets the lifetime prognosis. The Herring lateral pillar classification — A, B, B/C border, and C — is the prognostic and the decision-making tool, graded in the fragmentation phase. The containment principle keeps the soft head moulded within the acetabulum, achieved by a femoral varus or a Salter innominate osteotomy. And the decision is driven by age and lateral pillar grade: the young do well without surgery, the older child with lateral pillar B and C benefits from containment. [1] [4]
The examiner probes three traps. The first is the persistent limp accepted as lingering transient synovitis — the limp beyond two to three weeks is Perthes, a slip, or worse, and it earns a radiograph. The second is the mislabelled septic arthritis — the febrile, toxic, or Kocher-high-risk child is septic until proven otherwise, and Perthes is a diagnosis of the well, afebrile child. The third is the older child treated as the benign young case — the child over eight, the girl, and the lateral pillar C head carry the worst prognosis, and they demand early containment referral. [4] [2]
The examiner rewards the candidate who frames Perthes as a long, self-healing, shape-determining disease whose paediatric management shapes the adult hip. The limp is recognised, the urgent mimics are excluded, the lateral pillar is graded in the fragmentation phase, the containment decision is made by age and pillar grade, and the child is followed through to skeletal maturity with the Stulberg outcome as the measure. A candidate who shows this breadth and this long view demonstrates the systems thinking that the fellowship demands. [1] [9]
References
- [1]Herring JA, Kim HT, Browne R, et al. Legg-Calve-Perthes disease. Part II: Prospective multicenter study of the effect of treatment on outcome. Journal of Bone and Joint Surgery (American Volume), 2004.PMID 15466720
- [2]Wiig O, Terjesen T, Svenningsen S. Prognostic factors and outcome of treatment in Perthes' disease: a prospective study of 368 patients with five-year follow-up. Journal of Bone and Joint Surgery (British Volume), 2008.PMID 18827249
- [3]Terjesen T, Wiig O, Svenningsen S. The natural history of Perthes' disease. Acta Orthopaedica, 2010.PMID 21067434
- [4]Herring JA. Legg-Calve-Perthes disease at 100: a review of evidence-based treatment. Journal of Pediatric Orthopaedics, 2011.PMID 21857427
- [5]Larson AN, Sucato DJ, Herring JA, et al. A prospective multicenter study of Legg-Calve-Perthes disease: functional and radiographic outcomes of nonoperative treatment at a mean follow-up of twenty years. Journal of Bone and Joint Surgery (American Volume), 2012.PMID 22488614
- [6]Kim HK, da Cunha AM, Browne R, et al. How much varus is optimal with proximal femoral osteotomy to preserve the femoral head in Legg-Calve-Perthes disease? Journal of Bone and Joint Surgery (American Volume), 2011.PMID 21325585
- [7]Terjesen T, Wiig O, Svenningsen S. Varus femoral osteotomy improves sphericity of the femoral head in older children with severe form of Legg-Calve-Perthes disease. Clinical Orthopaedics and Related Research, 2012.PMID 22101403
- [8]Kim HK, Wiesman KD, Kulkarni V, et al. Perfusion MRI in Early Stage of Legg-Calve-Perthes Disease to Predict Lateral Pillar Involvement: A Preliminary Study. Journal of Bone and Joint Surgery (American Volume), 2014.PMID 25031369
- [9]Huhnstock S, Wiig O, Merckoll E, et al. The modified Stulberg classification is a strong predictor of the radiological outcome 20 years after the diagnosis of Perthes' disease. The Bone and Joint Journal, 2021.PMID 34847712
- [10]Neal DC, Alford TH, Moualeu A, et al. Prevalence of Obesity in Patients With Legg-Calve-Perthes Disease. Journal of the American Academy of Orthopaedic Surgeons, 2016.PMID 27471901
- [11]Loder RT, Browne RH, Millis A, et al. The time of the insult/triggering event in Legg-Calve-Perthes' disease determined by incubation period modeling and the age distribution of children with Perthes'. Iowa Orthopaedic Journal, 2012.PMID 23576924
- [12]Sankar WN, Lavalva SM, McGuire MF, et al. Does Early Proximal Femoral Varus Osteotomy Shorten the Duration of Fragmentation in Perthes Disease? Lessons From a Prospective Multicenter Cohort. Journal of Pediatric Orthopaedics, 2020.PMID 31524767