Paeds · rheumatology-musculoskeletal-and-sports
Pre-participation sports evaluation
Also known as pre-participation physical evaluation · sports clearance · pre-participation examination · PPE · cardiovascular screening in athletes · athletic pre-screening · sports pre-participation history
A fellowship approach to the pre-participation sports evaluation of the child and adolescent: the AHA 14-element cardiovascular history and examination and its red-flag items, the common causes of sudden cardiac death in the young athlete, the history-versus-ECG screening debate, the AAP paediatric blood pressure thresholds, the female athlete triad and relative energy deficiency in sport, the focused musculoskeletal screen, the clearance decision into cleared, cleared with conditions and restricted pending evaluation, and the written emergency action plan with access to an automated external defibrillator that protects every athlete when the screen misses a latent condition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A fifteen-year-old basketball player presents for clearance and mentions that he blacked out briefly during a sprint last month, or a fourteen-year-old cross-country runner has a maternal uncle who died suddenly at forty-two, or a sixteen-year-old swimmer is found to have a murmur that gets louder when she stands up. In each, the question is the same — does this history or this finding put the athlete at risk, and what is the right clearance. [1] [5]
The three P's of the cardiovascular history — Pain, Pass-out, Pathological family
Overview & Definition
A fifteen-year-old walks into the clinic the week before the season starts, and the question is whether sport is safe. The pre-participation sports evaluation answers that question. It is a systematic medical and musculoskeletal assessment of a child or adolescent before sport, and its goal is to detect the conditions that threaten life or limb and to promote safe participation. It is not a general health check, and it is not a search for every minor ailment that a young person carries. [1] [3]
The evaluation rests on four parts. The medical and cardiovascular history asks the questions that screen for the dangerous conditions. The physical examination listens to the heart, feels the pulses and measures the blood pressure. The musculoskeletal screen checks the limbs and the spine. The clearance decision turns the findings into a safe plan. The history is the most powerful of the four, because most of the conditions that kill young athletes declare themselves in the personal or the family history before they declare themselves on the field. [1] [2]
The fellowship framing turns on a single idea. The screen detects the threat, the clearance promotes safe participation, and the emergency action plan protects the athlete when the screen misses. A candidate who holds all three in mind avoids the two opposite errors — the false reassurance that clears the dangerous athlete, and the over-cautious restriction that bars the healthy one. [3] [10]
Classification
The cardiovascular screen that drives the clearance is the AHA 14-element personal and family history and physical examination, and the fellowship candidate must reproduce it. The fourteen elements divide into three groups. Seven personal history items ask the athlete about symptoms, three family history items ask about the family, and four physical examination items look for the signs of cardiac disease. [1] [2]
The seven personal history items are the symptoms that point to a dangerous cardiac condition. They are exertional chest pain, pressure or tightness, unexplained syncope or near-syncope, excessive and unexplained dyspnea or fatigue with exercise, a previously recognised heart murmur, an elevated blood pressure, a prior restriction from sport, and prior cardiac testing ordered by a physician. The three family history items are a sudden and unexpected death before fifty in a relative, disability from heart disease in a close relative under fifty, and a known familial cardiomyopathy, channelopathy or Marfan syndrome. [1]
The four physical examination items are the signs that the history might miss. They are a heart murmur listened to supine and standing, the femoral pulses palpated to exclude coarctation, the physical stigmata of Marfan syndrome, and the brachial blood pressure measured sitting and preferably in both arms. The standing examination is the fellowship detail, because the murmur of hypertrophic cardiomyopathy intensifies on standing or with the Valsalva manoeuvre while the innocent flow murmur softens or disappears. [1] [2]
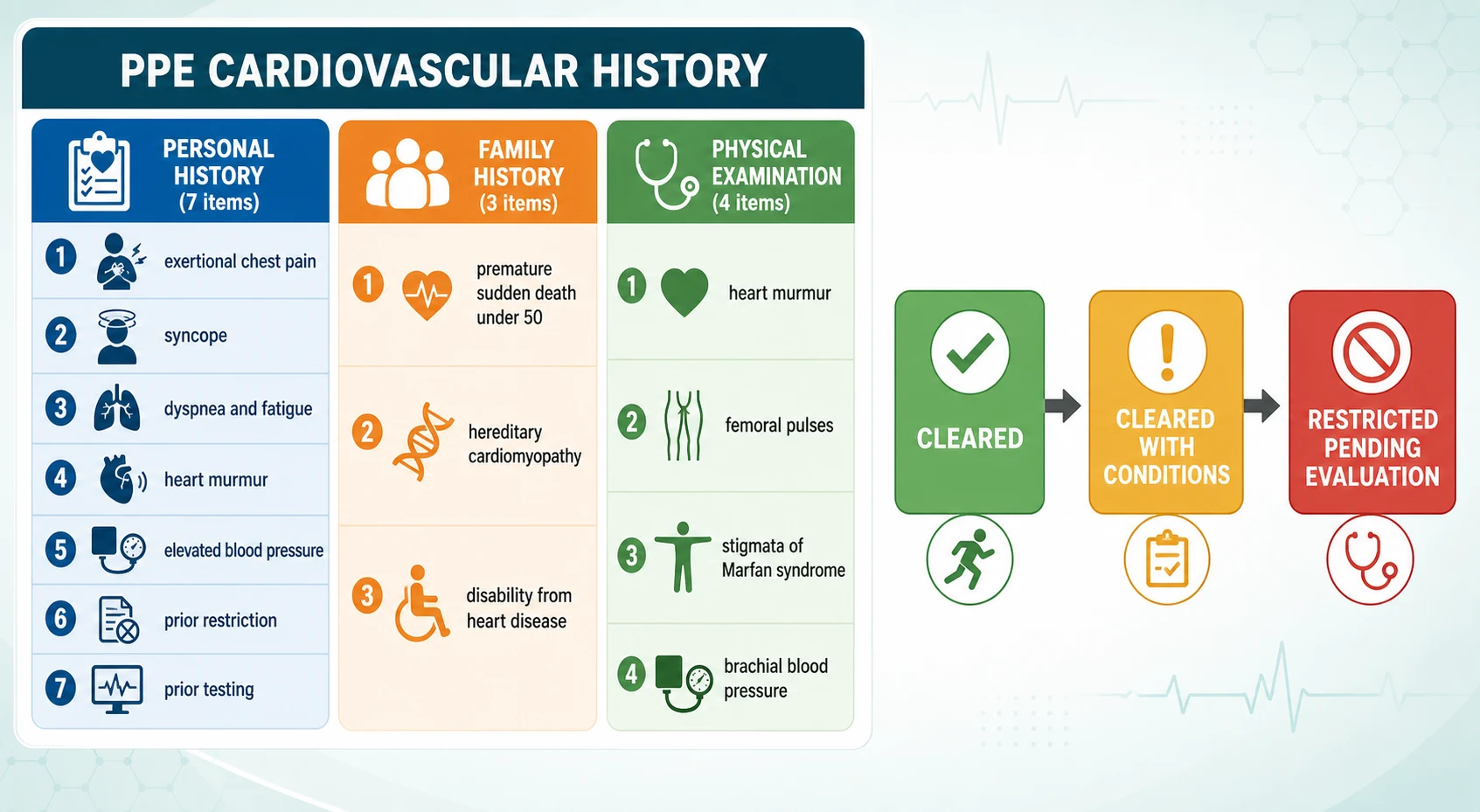
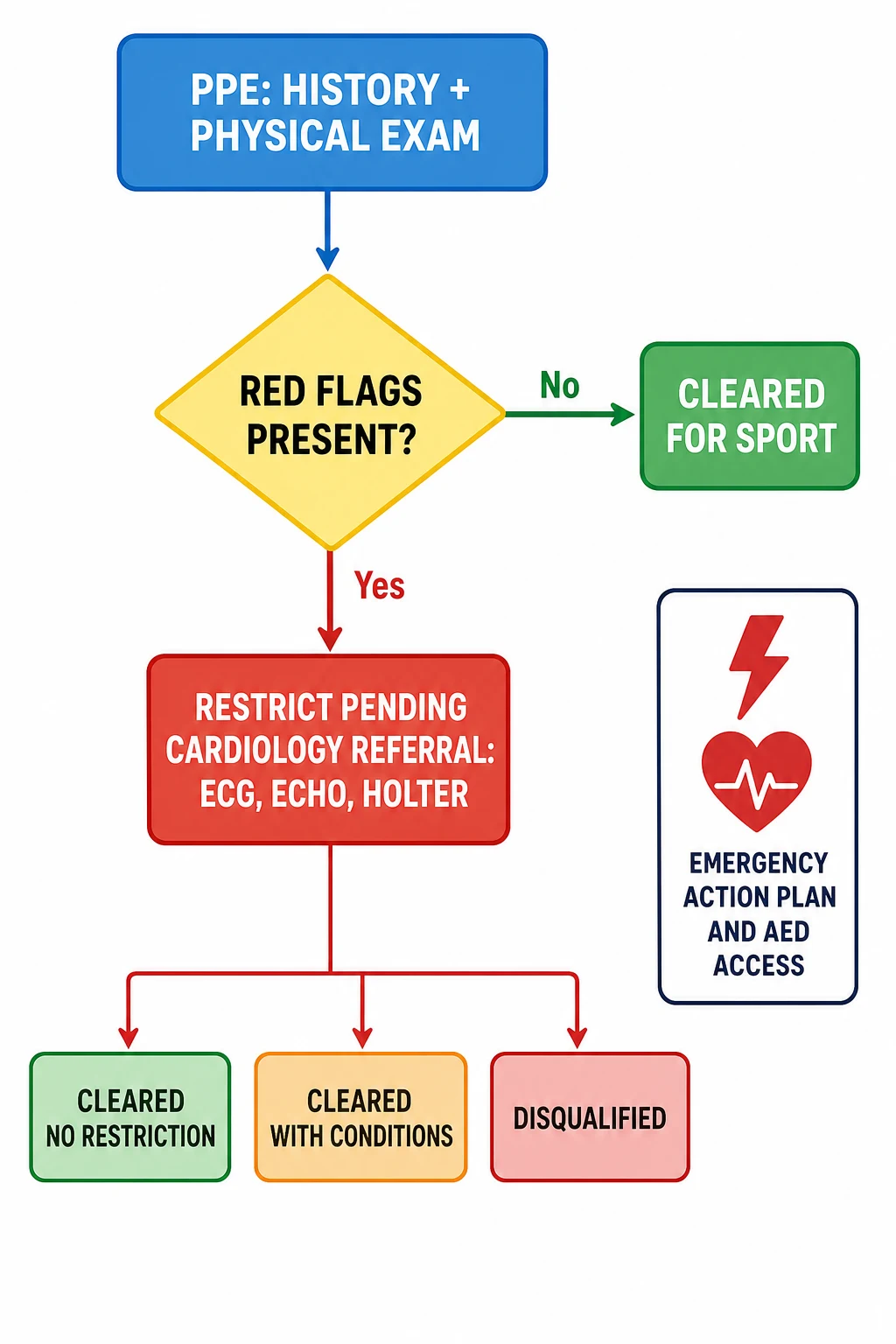
The screen ends in a decision the athlete takes home. When every cardiovascular element is negative and the examination is normal, the athlete is cleared without restriction. A stable, treated problem that needs an action plan but not a bar earns a clearance with conditions. A positive screen that resolves on the work-up earns a clearance after the further evaluation is complete. An unresolved positive screen, or a dangerous condition found, means the athlete is not cleared or is restricted pending the specialist evaluation. [3] [6]
Epidemiology & Risk Factors
Sudden cardiac death in the young athlete is rare but devastating, and it is the event the cardiovascular screen seeks to prevent. Estimates from the United States registry place the incidence between one and two deaths per one hundred thousand athlete-years, and the true figure is probably higher because many events go unreported. The deaths cluster in male athletes, in basketball and American football, and in the late school-age and adolescent years when the body is large enough and the exertion intense enough to unmask a latent cardiac condition. [5] [3]
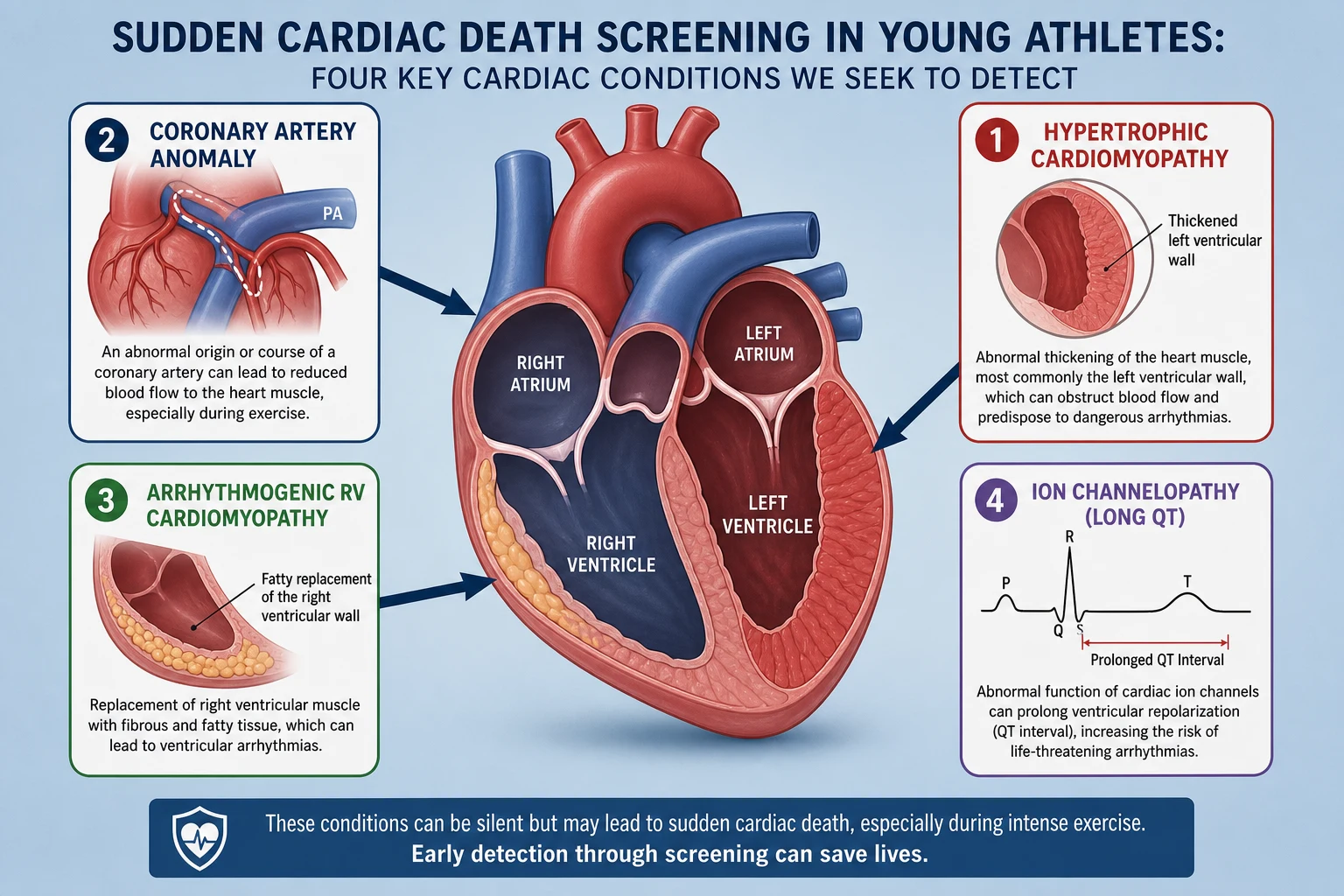
The conditions that cause these deaths are the structural and electrical diseases of the heart. Hypertrophic cardiomyopathy is the commonest in the United States registry, followed by congenital coronary artery anomalies, arrhythmogenic right ventricular cardiomyopathy, and the ion channelopathies such as long QT syndrome. Myocarditis and aortic rupture in Marfan syndrome also claim athletes. In the Italian registry, where electrocardiogram-inclusive screening has run for decades, arrhythmogenic right ventricular cardiomyopathy leads the list, which reflects both the local prevalence and the ability of the electrocardiogram to detect it. [5] [4]
The non-cardiac risks of sport are the overuse injuries and the triad that the evaluation also seeks to identify. Training-load errors, early sports specialisation, and the rapid growth of puberty raise the risk of overuse injury. The female athlete triad and relative energy deficiency in sport cluster in the aesthetic and endurance sports, where low energy availability drives the menstrual disturbance and the bone loss. The evaluation screens for these because they are common, they are treatable, and they carry their own long-term harm. [8] [9]
The socioeconomic gradient is the last risk marker. Survival from exertional sudden cardiac arrest is lower where access to defibrillation and emergency planning is poor, and the athlete in a disadvantaged or a remote setting carries a risk that the evaluation alone cannot remove. The emergency action plan and the defibrillator are therefore part of the disposition, not an afterthought. [10]
Pathophysiology
Hypertrophic cardiomyopathy is the condition the screen works hardest to find, and its mechanism explains why exertion triggers the event. The heart muscle thickens abnormally, most often in the left ventricular wall, and the disordered myofibrillar architecture sets up re-entrant ventricular arrhythmia. The thickened wall can also narrow the outflow tract, and the murmur that intensifies on standing is the bedside clue to that obstruction. A sudden ventricular arrhythmia during intense exertion is the mode of death. [5] [6]
A congenital coronary artery anomaly kills through exertional ischaemia. The left coronary artery arises from the wrong sinus and runs between the great vessels, and the acute angle and the interarterial course compress the vessel during exercise. The first symptom is often chest pain or syncope on exertion, and because the first presentation is so often fatal, the exertional symptom in the history is the only chance to detect it before the event. [5]
The ion channelopathies kill through an exercise-triggered arrhythmia of a structurally normal heart. Long QT syndrome prolongs cardiac repolarisation, and exercise or emotion sets off polymorphic ventricular tachycardia. The family history is the screen's way in, because the condition is inherited and a relative may have died suddenly or been diagnosed. The electrocardiogram detects the prolonged QT that the history and the examination cannot. [4] [6]
The female athlete triad and relative energy deficiency in sport develop through a chain that begins with low energy availability. When the athlete burns more energy than she eats, the body suppresses the hypothalamic-pituitary-gonadal axis, the menses stop, and the low oestrogen and the low energy supply weaken the bone. The stress fracture and the recurrent bony injury follow. The IOC relative energy deficiency in sport model extends the triad to the metabolic, immune and cardiovascular consequences of chronic under-fuelling. [8]
Clinical Presentation
The cardiovascular red flags declare themselves in the history, and the fellowship candidate must ask for them directly. Exertional chest pain, pressure or tightness is the first. Unexplained syncope or near-syncope with exercise is the second, and it is the most ominous because exertional syncope is sudden cardiac death until proven otherwise. Excessive and unexplained dyspnea or fatigue with exercise is the third. A previously recognised murmur or an elevated blood pressure completes the personal history. [1] [2]
The family history declares itself in the sudden and unexpected death of a relative. A close relative who died suddenly before fifty, a relative disabled by heart disease before fifty, or a known familial cardiomyopathy, channelopathy or Marfan syndrome each raise the risk. The family history identifies the at-risk athlete before the event, because many of these conditions are inherited, and the single most powerful screening question is who in the family died young and why. [1] [6]
The female athlete triad presents in the amenorrhoeic endurance or aesthetic athlete. The menses are absent or irregular, a stress fracture or a recurrent bony injury has occurred, and the body mass index is low or the eating is disordered. The exercise-induced bronchoconstriction of the asthmatic athlete presents as cough, wheeze or chest tightness five to ten minutes into or after exercise, and the evaluation must separate it from a cardiac symptom because the treatment and the clearance differ. [8]
Which reassuring-sounding stories must never close the search? The syncope written off as dehydration, the chest pain called musculoskeletal, and the murmur attributed to a flow murmur without the effort to listen standing up are the three classic errors. Each turns a detectable cardiac condition into a sudden death, and each is avoided by asking the fourteen questions and listening to the heart supine and standing. [1] [5]
Differential Diagnosis
The differential begins with the murmur, because the innocent flow murmur of the athletic adolescent is common and the pathological murmur of hypertrophic cardiomyopathy is rare but lethal. The flow murmur is soft, short, systolic, and heard at the left sternal edge, and it softens or disappears on standing. The pathological murmur is louder, often harsh, and it intensifies on standing or with the Valsalva manoeuvre. The standing examination is the bedside test that separates them, and a murmur that behaves abnormally is referred for an echocardiogram. [1] [6]
The differential of exertional syncope separates the dangerous from the benign. Syncope from hypertrophic cardiomyopathy, a coronary artery anomaly or long QT syndrome occurs during exertion and is the danger. Syncope that occurs after the exertion stops, with a prodrome of warmth and nausea and a prompt recovery, is the benign vasovagal or post-exertional pattern. The timing and the prodrome separate them, and any doubt restricts the athlete pending the work-up. [2] [3]
The differential of exertional dyspnea separates the cardiac from the respiratory and the deconditioned causes. Exercise-induced bronchoconstriction produces cough, wheeze and chest tightness that peak after the exertion begins, and it responds to a bronchodilator. Cardiac dyspnea is disproportionate, progressive, and accompanied by the other cardiovascular elements. Upper-airway dysfunction and simple deconditioning complete the differential, and each demands a different clearance pathway. [3]
When the combination of symptoms and family history is strong, the differential turns to the work-up rather than the clearance in primary care. The athlete with two cardiovascular symptoms, a positive family history, or an abnormal murmur is referred to cardiology for an electrocardiogram, an echocardiogram and, where indicated, a Holter monitor or an exercise test, before a return-to-sport decision is made. [3] [6]
Clinical & Bedside Assessment
The focused physical examination of the pre-participation evaluation takes a few minutes and follows a fixed sequence. Measure the blood pressure in both arms with the athlete sitting. Feel the pulse and note the general appearance. Listen to the heart supine and standing, and perform the dynamic assessment for a murmur that changes with position. Feel the femoral pulses to screen for coarctation, and run the focused musculoskeletal screen. [1] [7]
The stigmata of Marfan syndrome are sought because aortic rupture is a cause of sudden death in the young athlete. Look for an arm span that exceeds the height, a reduced upper-to-lower body segment ratio, scoliosis, pectus excavatum or carinatum, a history of lens dislocation, and a positive wrist and thumb sign. A constellation of these signs triggers a cardiology referral and an echocardiogram of the aorta, because the connective tissue disease carries its own sport-restriction rules. [1] [6]
The femoral pulses and the four-limb blood pressure screen for coarctation of the aorta. A delayed or absent femoral pulse, or a blood pressure that is higher in the arms than in the legs, is coarctation until proven otherwise, and the finding is never attributed to cuff error. A blood pressure that is elevated on the first reading is repeated, and a persistently elevated reading is staged by the AAP clinical practice guideline. [1] [7]
Which examination findings must never be dismissed? A loud, harsh or diastolic murmur, an absent or delayed femoral pulse, a four-limb pressure difference, and the stigmata of a connective tissue disorder are the four findings that move the athlete straight from the examination couch to the cardiology referral. Each is a red flag on its own, and none is cleared without a work-up. [1] [3]
Investigations
The AHA 14-element history and physical examination is the minimum standard for cardiovascular screening, and the fellowship candidate must know what it can and cannot do. The 2007 AHA update established the elements, and the 2014 AHA-ACC statement reconfirmed them. The strength of the history and examination is that they are cheap, universal and reproducible. The weakness, which the AHA acknowledges, is that the sensitivity is low, because many of the conditions that kill young athletes produce no symptom and no sign until the event. [1] [2]
The electrocardiogram-inclusive model adds a twelve-lead electrocardiogram to the history and examination, and the Italian experience is the evidence behind it. After Italy introduced nationwide electrocardiogram-inclusive screening in 1982, the rate of sudden cardiac death in young competitive athletes fell, and arrhythmogenic right ventricular cardiomyopathy became the leading detected cause. The European Society of Cardiology endorses electrocardiogram screening where the infrastructure and the interpreter expertise exist. [4] [6]
The AMSSM 2017 position statement frames the controversy in the language a fellowship candidate is expected to use. It states that the standard history and examination misses most of the conditions that cause sudden cardiac death, that the electrocardiogram improves the sensitivity, and that the electrocardiogram carries a false-positive rate and a cost. It supports a shared, evidence-informed decision on whether to add the electrocardiogram, rather than a blanket mandate or a blanket refusal. [3]
Further investigation follows a positive screen. A pathological murmur, an exertional syncope, or an abnormal electrocardiogram triggers an echocardiogram, a Holter monitor, or an exercise test, and the cardiology opinion refines the clearance. The paediatric blood pressure measurement is itself an investigation that stages the athlete, and the AAP clinical practice guideline defines the thresholds. For an adolescent aged thirteen and over, an elevated blood pressure runs from 120 with a diastolic under 80 up to 130 over 80, stage 1 hypertension runs from 130 over 80 up to 140 over 90, and stage 2 hypertension is 140 over 90 or higher. [7] [3]
Management — Resuscitation
The time-critical event is anticipated through the written emergency action plan, and every venue that hosts sport must hold one and rehearse it. The plan names the team that responds, the chain of communication, the location of the equipment, and the route to the hospital. It is practised at least once a year, because the team that has never rehearsed does not perform under the pressure of a collapse. The plan is the second layer of protection that catches the athlete the screen missed. [3] [10]
Access to an automated external defibrillator within one to three minutes of collapse is the single most important determinant of survival from exertional sudden cardiac arrest. The defibrillator is the device that converts the ventricular fibrillation of the young athlete's arrest, and survival falls by about ten per cent for every minute that defibrillation is delayed. A venue without a defibrillator within reach turns a survivable arrest into a death, which is why the device is a part of the disposition and not an option. [3] [10]
The response to the athlete who collapses on the field follows the chain of survival. The responder assesses responsiveness, calls for help and the defibrillator, starts chest compressions, and applies the defibrillator as soon as it arrives, and the defibrillator instructs the responder through the shock. The same chain applies to a collapse in the clinic, and the pre-participation evaluation that clears the athlete without confirming the plan has done only half the job. [10]
The athlete with a suspected cardiac symptom at the evaluation is managed by restriction, not by clearance. The athlete is held from sport pending an urgent cardiology referral, an electrocardiogram and an echocardiogram, and the return-to-sport decision waits for the work-up. The temptation to clear and review later is the error that costs the life, because the next exertional event may be the fatal one. [1] [3]
Management — Definitive & Stepwise
The standard evaluation is performed stepwise. The history is taken, the physical examination is performed, the musculoskeletal screen is run, and the clearance decision is made. When every cardiovascular element is negative and the examination is normal, the athlete is cleared without restriction, and the counselling covers injury prevention, training load, hydration, sleep and the avoidance of early specialisation. [1] [9]
The clearance pathway — from screen to decision
Take the AHA 14-element history — seven personal, three family — and ask the three P's of pain, pass-out and pathological family.
Examine the heart supine and standing, palpate the femoral pulses, measure the blood pressure in both arms, and seek the stigmata of Marfan syndrome.
Run the focused musculoskeletal screen for asymmetry, weakness and limited range of motion.
Decide the clearance — cleared, cleared with conditions, or restricted pending evaluation — based on the screen.
Confirm the written emergency action plan and the automated external defibrillator access at the venue before the season starts.
The athlete with a positive screen is managed by referral and restriction. A positive cardiovascular element moves the athlete into the restricted-pending-evaluation category, and the cardiology work-up decides the return. The athlete with the female athlete triad or relative energy deficiency in sport is managed by restoring energy availability, addressing the menstrual disturbance and the bone health, and clearing the athlete only when the risk has fallen, according to the IOC framework. [8] [3]
The athlete with a chronic condition needs a sport-specific conditional clearance and an action plan. The asthmatic athlete carries an exercise action plan, the diabetic athlete carries a glucose plan, and the athlete with a single kidney or another organ condition is matched to the sport by the collision risk. The hypertensive athlete is staged by the AAP guideline, the blood pressure is confirmed and managed, and the clearance reflects the staging. [7] [8]
Specific Subtypes & Scenarios
The routine, low-risk clearance is the commonest scenario and the one the evaluation handles in minutes. The fourteen elements are negative, the examination is normal, the musculoskeletal screen is normal, and the athlete is cleared without restriction. The counselling that follows covers injury prevention and the emergency action plan, and the athlete leaves with a clearance and a return date for the next annual evaluation. [1] [9]
The cardiac red-flag clearance is the scenario that decides a life. The athlete with exertional syncope or a positive family history is restricted from sport pending an electrocardiogram, an echocardiogram and a cardiology opinion. The specialist return-to-sport decision follows the diagnosis, and the athlete is cleared, cleared with conditions, or disqualified according to the sport-cardiology guidelines. The single most important act is the restriction before the work-up, because clearance and review later is the fatal error. [3] [6]
The female athlete triad clearance is the scenario of the amenorrhoeic endurance or aesthetic athlete. The energy availability is assessed, the menstrual disturbance is documented, and the bone density is measured where indicated. The clearance is conditional on the recovery, and the athlete returns to full training only when the energy availability is restored and the menses have returned, because a premature return perpetuates the bone loss and the stress fracture. [8]
The hypertensive clearance is the scenario of the elevated blood pressure. A single elevated reading is repeated, and a persistently elevated reading is staged by the AAP clinical practice guideline. The athlete with an elevated or a stage 1 reading is managed and may be cleared with conditions and a follow-up, and the athlete with a stage 2 reading or an associated symptom is restricted pending the work-up. The blood pressure is never ignored and never dismissed as white-coat effect on a single reading alone. [7]
The remote or school-based clearance is the scenario of the station-based evaluation. A team of clinicians runs the stations, the history is taken by a nurse or a trained volunteer, and the flagged athlete is referred by a clear pathway to a centre with cardiology capability. Telehealth supports the remote site, and the emergency action plan and the defibrillator are confirmed before the season, because the athlete in a remote setting carries the risk that distance adds to the cardiac clock. [10] [3]
Complications & Pitfalls
The complications of a poor evaluation fall into the missed and the over-diagnosed. The missed cardiac condition causes a sudden death that the evaluation failed to detect, and the missed triad causes a stress fracture or a long-term bone loss. The over-diagnosed benign flow murmur or vasovagal syncope consumes resources, causes anxiety, and bars a healthy athlete without improving safety. A structured screen avoids both errors. [3] [6]
The false reassurance of a normal history and examination is the central pitfall. The standard evaluation has a low sensitivity for the latent conditions that cause sudden cardiac death, because hypertrophic cardiomyopathy, a coronary artery anomaly and a channelopathy may produce no symptom and no sign until the event. The emergency action plan and the defibrillator exist precisely because the screen misses, and the clearance is never a guarantee of zero risk. [1] [5]
The over-investigation of the innocent murmur or the vasovagal syncope is the opposite pitfall. A soft flow murmur that disappears on standing and a syncope with a clear vasovagal prodrome after exertion do not demand an echocardiogram in every case, and a structured application of the standing examination and the symptom pattern avoids the cascade. The shared decision with the athlete and the family balances the reassurance against the small residual risk. [3]
The missing emergency action plan and defibrillator is the pitfall that turns a survivable arrest into a death, even when the evaluation was correctly performed. The plan must be written, rehearsed, and equipped, and the defibrillator must be reachable within minutes. The failure to follow up a conditional clearance is the final pitfall, because the athlete cleared pending a cardiology review who returns to sport before the review happens is the athlete who dies between the two visits. [10] [3]
Prognosis & Disposition
The prognosis of the cleared athlete remains a low but non-zero risk, and this is the single most important thing to tell the athlete and the family. The evaluation reduces the risk, the clearance promotes safe participation, and the emergency action plan and the defibrillator catch the athlete the screen misses, but no evaluation eliminates the risk entirely. The honest counselling sets the residual risk against the benefits of sport and the protection in place. [3] [10]
The prognosis of the athlete with a treated condition depends on the specialist return-to-sport decision and the ongoing surveillance. A controlled channelopathy, a repaired structural lesion, or a recovered triad may permit a conditional clearance, and the sport-cardiology guidelines frame the sport and the surveillance for each diagnosis. The disposition is shared between the primary-care clinician who owns the evaluation and the cardiologist or specialist who owns the positive-screen work-up. [6] [3]
The disposition extends to the school and the club, who own the emergency action plan and the defibrillator. The primary-care clinician confirms the plan at the evaluation, and the school or the club holds and rehearses it through the season. The annual review with an interval history update captures the condition that develops between evaluations, because the fifteen-year-old who was clear last year may have developed the first symptom this year. [10] [1]
Special Populations
The female athlete in an aesthetic or endurance sport carries the highest triad and relative energy deficiency in sport risk, and the evaluation screens for the energy availability, the menstrual disturbance and the bone health. The screening questions cover the menstrual pattern, the training volume, the dietary intake and the stress-fracture history, and a positive screen triggers the conditional clearance and the recovery plan. The early detection prevents the stress fracture and the long-term bone loss. [8]
The athlete with a chronic condition needs a sport-specific conditional clearance and an action plan that the evaluation structures. The athlete with congenital heart disease, asthma, diabetes, a single kidney, or epilepsy is matched to the sport by the diagnosis and the collision risk, and the action plan covers the exacerbation. The evaluation is the moment to coordinate the specialist, the school and the family around a single safe plan. [6] [8]
The athlete in a rural or remote setting needs a station-based or a telehealth-assisted evaluation and a clear pathway to restrict and refer the flagged athlete. The distance adds to the cardiac clock, and the defibrillator and the emergency action plan are even more important where the hospital is far away. Telehealth supports the remote site, and the flagged athlete is referred to a centre with cardiology capability. [10]
The Indigenous and the socioeconomically disadvantaged athlete faces barriers to the evaluation and to the defibrillation. The survival from exertional sudden cardiac arrest is lower where the access is poor, and the evaluation that does not address the access gap protects the athlete incompletely. The emergency action plan, the defibrillator and the referral pathway are the protections that close the gap, alongside the screen itself. [10] [9]
Evidence, Guidelines & Regional Differences
The AHA 2007 update and the 2014 AHA-ACC statement established the fourteen elements and the standard they represent. The AHA concludes that the history-and-examination screen is the minimum standard, that its sensitivity is too low to detect every condition, and that a mandatory electrocardiogram is not yet justified across the United States because of the cost, the false-positive rate and the infrastructure. The AHA position is the one a fellowship candidate must reproduce. [1] [2]
The Italian experience and the European Society of Cardiology take the opposite view on the electrocardiogram. The Corrado study showed that sudden cardiac death in young competitive athletes fell after nationwide electrocardiogram-inclusive screening began in 1982, and the European Society of Cardiology endorses the electrocardiogram where the interpreter expertise and the infrastructure exist. The two positions are not contradictory but reflect different health systems, and the AMSSM 2017 position statement frames the choice as a shared, evidence-informed decision. [4] [6]
The Maron registry of 1866 sudden deaths in young United States athletes frames the cause and the limitation of the standard model. Hypertrophic cardiomyopathy and the coronary artery anomalies lead the list, and the registry confirms that many of the deaths were not predicted by the history-and-examination screen alone. The registry is the evidence that the screen misses, and the defibrillator is the response. [5]
The non-cardiac components of the evaluation draw on the AAP blood pressure guideline, the IOC relative energy deficiency in sport consensus, and the neuromuscular-training injury-prevention trials. The AAP guideline defines the paediatric blood pressure stages, the IOC consensus frames the energy availability and the triad, and the iSPRINT trial showed that a school-based neuromuscular-training programme reduced the sports-injury rate in junior high students. The regional differences are modest but real, and the contemporary practice in Australasia and the United Kingdom aligns the screen with the AHA elements while the electrocardiogram remains a shared decision. [7] [8]
Exam Pearls
The fellowship answer turns on a handful of elements and numbers. The AHA screen has fourteen elements, split into seven personal history, three family history and four physical examination items. The three personal-history symptoms are exertional chest pain, exertional syncope and excessive dyspnea or fatigue. The leading causes of sudden cardiac death are hypertrophic cardiomyopathy in the United States and arrhythmogenic right ventricular cardiomyopathy in Italy. The single most important determinant of survival from exertional sudden cardiac arrest is access to a defibrillator within minutes. [1] [5]
The examiner probes three traps. The first is the exertional syncope cleared as dehydration — it is sudden cardiac death until proven otherwise, and it is restricted pending the work-up. The second is the murmur auscultated only supine — the standing examination separates the flow murmur from the dynamic murmur of hypertrophic cardiomyopathy. The third is the clearance without the emergency action plan — the defibrillator and the rehearsed plan protect the athlete the screen misses. A candidate who names these three traps demonstrates the screen, clearance and protection thinking the fellowship rewards. [3] [10]
The examiner rewards the candidate who frames the pre-participation evaluation around three ideas. The screen detects the threat, the clearance promotes safe participation, and the emergency action plan protects when the screen misses. The candidate who states both the AHA and the European positions on the electrocardiogram demonstrates the evidence-informed thinking the fellowship rewards, and the candidate who applies the standing examination to every murmur demonstrates the bedside skill the screen demands. [1] [4]
[2] [4]The AHA 14-element screen — 7-3-4
References
- [1]Maron BJ, Thompson PD, Ackerman MJ, Balady G, Berger S, Cohen D, et al. Recommendations and considerations related to preparticipation screening for cardiovascular abnormalities in competitive athletes: 2007 update. Circulation, 2007.PMID 17353433
- [2]Maron BJ, Friedman RA, Kligfield P, Levine BD, Viskin S, Chaitman BR, et al. Assessment of the 12-lead ECG as a screening test for detection of cardiovascular disease in healthy general populations of young people (12-25 years of age). Circulation, 2014.PMID 25223981
- [3]Drezner JA, O'Connor FG, Harmon KG, Fields KB, Asplund CA, Asif IM, et al. AMSSM Position Statement on Cardiovascular Preparticipation Screening in Athletes: Current evidence, knowledge gaps, recommendations and future directions. Br J Sports Med, 2017.PMID 27660369
- [4]Corrado D, Basso C, Pavei A, Michieli P, Schiavon M, Thiene G. Trends in sudden cardiovascular death in young competitive athletes after implementation of a preparticipation screening program. JAMA, 2006.PMID 17018804
- [5]Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation, 2009.PMID 19221222
- [6]Pelliccia A, Sharma S. The 2020 ESC Guidelines on Sport Cardiology. Eur Heart J, 2021.PMID 33428717
- [7]Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, et al. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics, 2017.PMID 28827377
- [8]Mountjoy M, Ackerman KE, Bailey DM, Burke LM, Constantini N, Hackney AC, et al. 2023 International Olympic Committee's (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs). Br J Sports Med, 2023.PMID 37752011
- [9]Emery CA, van den Berg C, Richmond SA, Palacios-Derflingher L, McKay CD, Doyle-Baker PK, et al. Implementing a junior high school-based programme to reduce sports injuries through neuromuscular training (iSPRINT): a cluster randomised controlled trial. Br J Sports Med, 2020.PMID 31822477
- [10]Schattenkerk J, Kucera K, Peterson DF, Huggins RA, Drezner JA. Socioeconomic factors and outcomes from exercise-related sudden cardiac arrest in high school student-athletes in the USA. Br J Sports Med, 2022.PMID 34716143