Paeds · rheumatology-musculoskeletal-and-sports
Reactive arthritis and post-infectious inflammatory syndromes
Also known as Reactive arthritis · Reiter syndrome · Post-streptococcal reactive arthritis · Post-infectious arthritis · Enthesitis-related arthritis · Post-enteric arthropathy
Fellowship guide to reactive arthritis and the post-infectious inflammatory syndromes of childhood. Covers the classic post-enteric and post-genitourinary reactive arthritis with its one-to-four-week latency, its asymmetric lower-limb oligoarthritis with enthesitis and its HLA-B27 association, the post-streptococcal reactive arthritis with its additive pattern and shorter latency, the acute rheumatic fever differential with the 2015 Jones criteria and the carditis that is the hallmark, the naproxen and ibuprofen first-line treatment, the intra-articular triamcinolone hexacetonide, the sulfasalazine and anti-tumour-necrosis-factor escalation, and the molecular mimicry and the cytokine cascade that link the distant infection to the sterile joint.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A nine-year-old boy limps into the emergency department three weeks after a bout of bloody diarrhoea on a family camping trip. His right knee and his left ankle are swollen and warm, his right heel hurts where the Achilles tendon inserts, and his right great toe is a puffy sausage digit. He is afebrile and otherwise well, and the joint fluid is sterile. This is the textbook face of reactive arthritis, and the post-infectious latency is the anchor that frames every question the examiner will ask. [4][9]
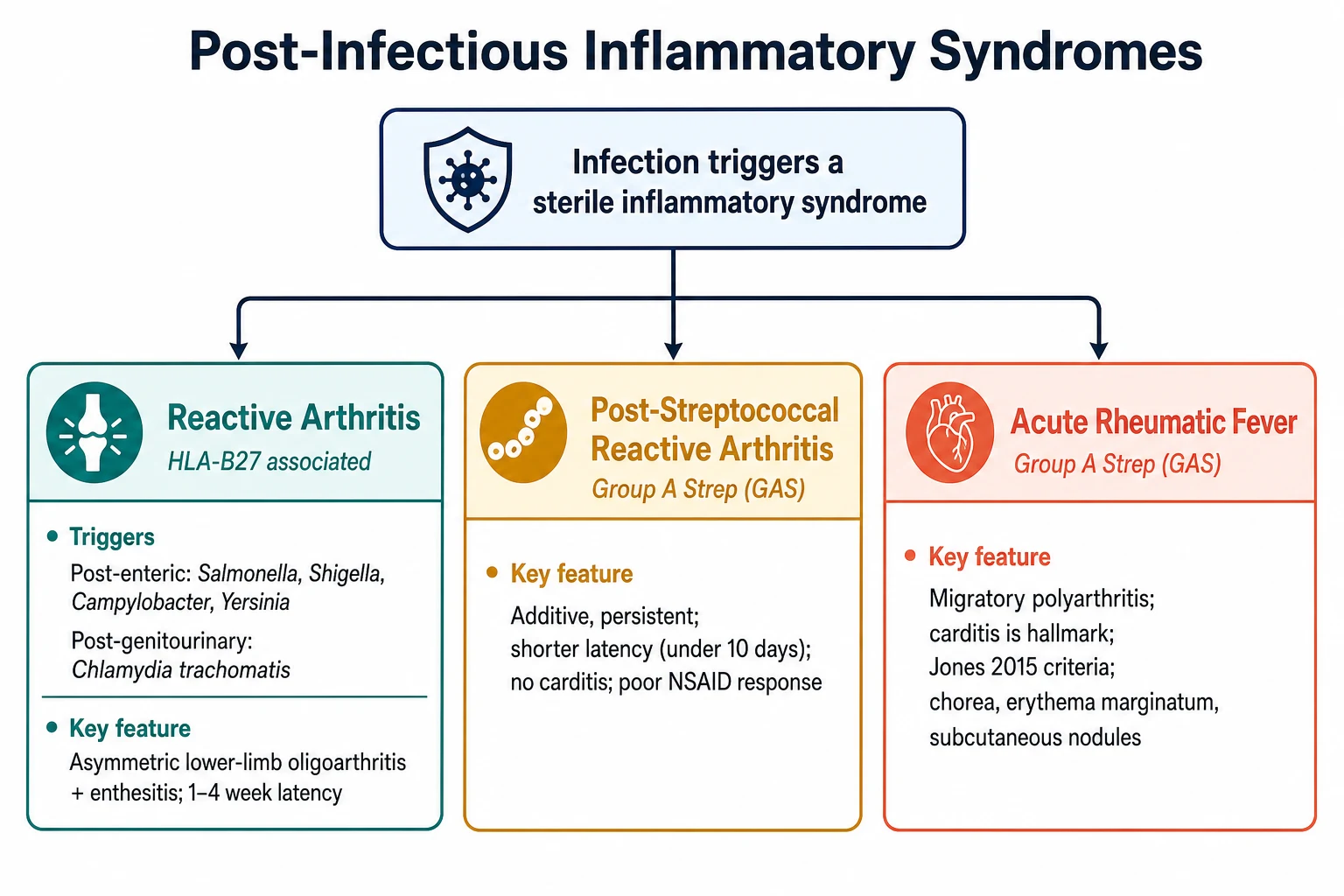
Reactive arthritis is a sterile inflammatory arthritis that arises one to four weeks after a distant infection of the genitourinary or the gastrointestinal tract, in a joint that contains no cultivable organism. The classic triggers are the enteric bacteria Salmonella, Shigella, Campylobacter and Yersinia, and the genitourinary Chlamydia trachomatis, and the disease sits on the spondyloarthritis spectrum alongside the enthesitis-related juvenile idiopathic arthritis. The full Reiter triad of the arthritis, the conjunctivitis and the urethritis is uncommon in children, and the term is now discouraged in favour of reactive arthritis because Hans Reiter's Nazi history and the rarity of the complete triad make it a poor label. [4][10]
The topic earns its fellowship weight from two demands. The first is the safety demand. The acute swollen joint in a febrile child is septic arthritis until proven otherwise, and the candidate who labels a reactive arthritis without the Kocher criteria, the blood cultures and the joint aspirate fails the patient and the viva. The second is the discrimination demand. The post-streptococcal reactive arthritis, the acute rheumatic fever, the enthesitis-related juvenile idiopathic arthritis and the periodic fever syndromes all masquerade as the post-infectious arthritis, and the candidate who can defend each distinction with the latency, the pattern, the carditis and the response to the non-steroidal anti-inflammatory drugs is the candidate who passes. [1][3]
Classification
Reactive arthritis is classified first by the triggering infection, and the trigger determines the workup, the contact tracing and the prognosis. The post-enteric form follows the Salmonella, the Shigella, the Campylobacter or the Yersinia gastroenteritis, and it is the commonest paediatric form in regions where the food-borne and the water-borne diarrhoea dominate. The post-genitourinary form follows the Chlamydia trachocinfection, and it rises in the adolescence with the sexual activity, carrying the obligation of the partner notification. [4][9]
The post-streptococcal reactive arthritis occupies a separate and contested niche, because the group A streptococcus triggers two distinct post-infectious syndromes through different immune mechanisms. The acute rheumatic fever is the better-known streptococcal syndrome with its migratory polyarthritis, its carditis and its Jones criteria, while the post-streptococcal reactive arthritis is the additive, persistent arthritis with the shorter latency and the absent carditis. The distinction is not academic, because the acute rheumatic fever demands the long-term penicillin prophylaxis and the cardiac surveillance, while the post-streptococcal reactive arthritis does not, or does so only under debate. [1][2]
Reactive arthritis
Post-strep reactive arthritis
Acute rheumatic fever
Epidemiology & Risk Factors
Reactive arthritis is the commonest form of the childhood spondyloarthritis, though the exact incidence is hard to pin because the trigger is often missed and the mild cases never reach the rheumatologist. The enteric form dominates in the young child, driven by the Salmonella and the Campylobacter that cause the gastroenteritis, while the genitourinary form rises in the adolescence with the Chlamydia exposure. Only a minority of the children exposed to a given trigger develop the arthritis, and the HLA-B27 allele is the chief host factor that tilts the susceptibility. [4][7]
The HLA-B27 allele is present in roughly half to three-quarters of the adults with the reactive arthritis, and it modifies the severity as well as the susceptibility, because the HLA-B27-positive patient is the one more likely to develop the chronic disease, the sacroiliitis and the uveitis. The allele is commoner in the indigenous populations of the Australia and the New Zealand and the North America, and it partly explains the heavier burden of the spondyloarthritis and the acute rheumatic fever in these communities. The candidate should carry the allele as a susceptibility marker, not as a diagnostic test, because the HLA-B27 is positive in a substantial fraction of the healthy population. [5][8]
Pathophysiology
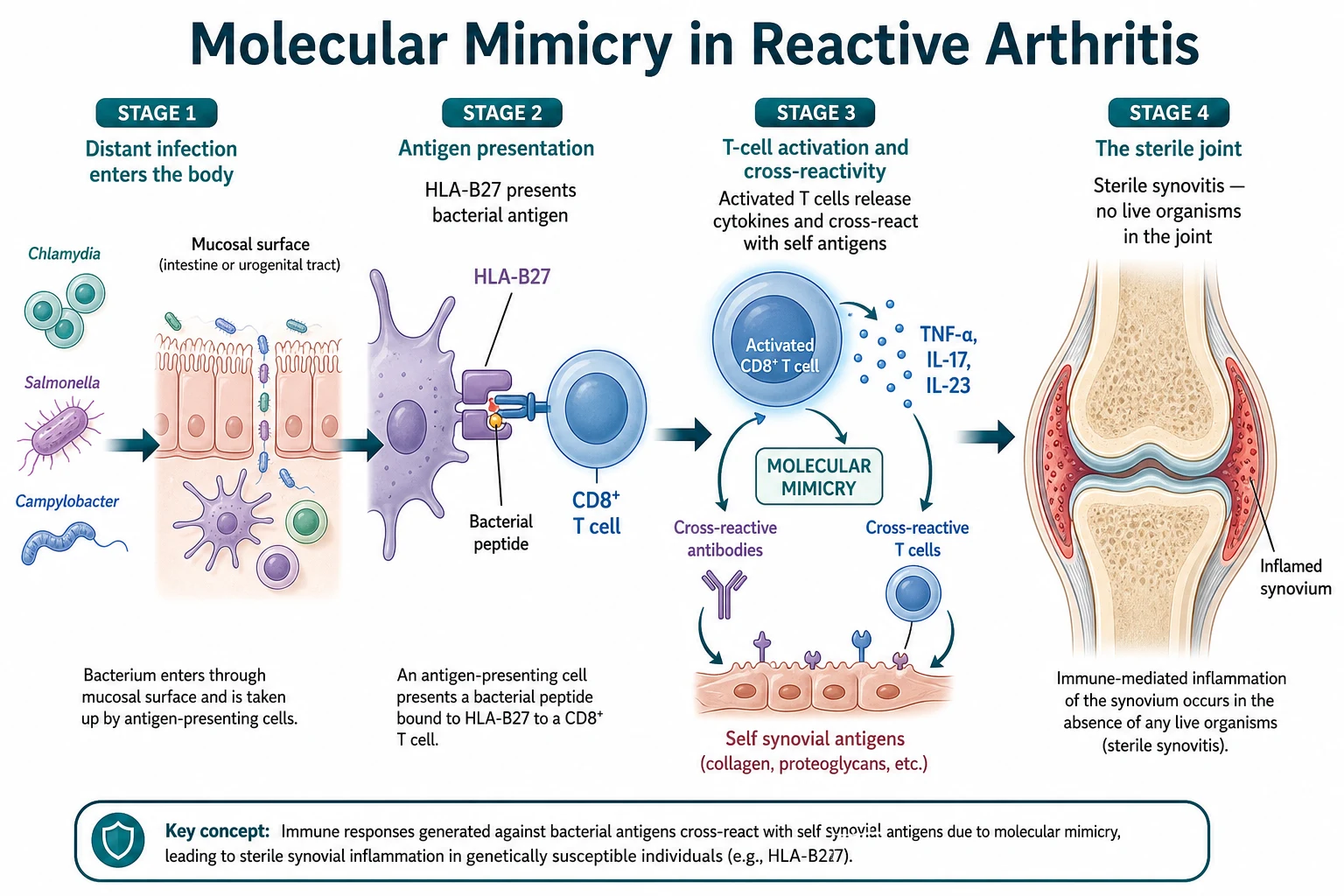
The central question of the reactive arthritis is why a sterile joint inflames weeks after a distant gut or genitourinary infection, and the answer is the molecular mimicry. The HLA-B27 molecule on the antigen-presenting cell picks up the bacterial peptide from the Chlamydia or the Salmonella, and it presents it to the CD8-positive T cell. The activated T cell then cross-reacts with the self-antigens in the synovium, because the bacterial peptide and the self-peptide share a similar shape, and the cross-reactive immune response drives the sterile synovitis. [5][4]
The cytokine cascade that follows is the interleukin-23 and the interleukin-17 axis, which is the signature of the entire spondyloarthritis family. The interleukin-23 drives the T-helper-seventeen cells to release the interleukin-17, and the interleukin-17 recruits the neutrophils and the further T cells into the synovium and the enthesis. The tumour necrosis factor alpha amplifies the inflammation, and it is the target of the biologic therapy that transformed the refractory disease. The joint remains sterile because the live organisms do not seed it, though the chlamydial ribonucleic acid and the bacterial antigens persist in the synovial macrophages and sustain the inflammation long after the gut or the genitourinary infection has cleared. [5][4]
The post-streptococcal reactive arthritis uses a different mechanism, because the group A streptococcus drives the arthritis through the immune-complex deposition and the antibody response rather than through the HLA-B27-restricted T cell. The streptococcal antigens lodge in the synovium, the antibodies form the immune complexes, and the complement activation generates the inflammation. The acute rheumatic fever, by contrast, is the antibody-mediated cross-reactivity between the streptococcal M protein and the human cardiac tissue, which is why the carditis is its hallmark and not a feature of the post-streptococcal reactive arthritis. [1][3]
Clinical Presentation
The child with the classic reactive arthritis presents one to four weeks after the gastrointestinal or the genitourinary infection, and the arthritis is the presenting complaint. The pattern is the asymmetric lower-limb oligoarthritis, with the knee, the ankle and the joints of the foot the commonest targets, and the involvement is additive rather than migratory. The enthesitis is the spondyloarthritis hallmark, and it is sought at the Achilles tendon insertion at the heel and the plantar fascia insertion at the sole, where the child localises a sharp pain that is worse in the morning. The dactylitis, the puffy sausage digit of a single toe or finger, is another spondyloarthritis sign that the examiner rewards the candidate who finds it. [4][10]
The extra-articular features frame the spondyloarthritis, though they are uncommon in the children. The conjunctivitis is the commonest ocular feature, and it is usually mild and bilateral, but the acute anterior uveitis is the sight-threatening inflammation that demands the urgent slit-lamp and the ophthalmology referral. The cutaneous stigmata include the keratoderma blennorrhagicum, the painless pustular rash on the palms and the soles, and the circinate balanitis, the painless erosions on the glans penis, and both are the sterile reactions to the triggering infection. The Reiter triad of the arthritis, the conjunctivitis and the urethritis is the classic but uncommon combination, and the candidate should name the components while noting that the full triad is rare in the paediatric practice. [10][4]
The post-streptococcal reactive arthritis presents differently, and the pattern is the key to the distinction. The latency is shorter, under ten days after the streptococcal pharyngitis, the arthritis is additive and persistent rather than migratory, the enthesitis is prominent, and the response to the non-steroidal anti-inflammatory drugs is poor or slow. The carditis is absent, and this is the feature that separates the post-streptococcal reactive arthritis from the acute rheumatic fever. The candidate who finds a murmur or a prolonged PR interval in a child with the post-streptococcal arthritis is dealing with the acute rheumatic fever, not the post-streptococcal reactive arthritis, and the echocardiogram and the penicillin prophylaxis follow. [1][6]
Differential Diagnosis
The differential of the acute swollen joint in a child is the safety-critical question, and the septic arthritis is the diagnosis that must never be missed. The febrile, unwell child with a single hot joint and a refusal to bear weight is septic arthritis until proven otherwise, and the Kocher criteria, the blood cultures and the joint aspirate separate the infection from the reactive arthritis. The reactive arthritis, by contrast, presents in an afebrile or a low-grade-febrile child who is systemically well, after the one-to-four-week latency, and the joint aspirate is sterile with a lower cell count. [4][9]
Septic arthritis
Reactive arthritis
Transient synovitis
The acute rheumatic fever is the streptococcal syndrome that the candidate must separate from the post-streptococcal reactive arthritis, and the 2015 revised Jones criteria are the framework. The acute rheumatic fever presents two to three weeks after the streptococcal pharyngitis with the migratory polyarthritis that moves from joint to joint and resolves dramatically with the non-steroidal anti-inflammatory drugs, the carditis that is the hallmark and that includes the subclinical echocardiographic valvitis, the Sydenham chorea, the erythema marginatum and the subcutaneous nodules. The post-streptococcal reactive arthritis, by contrast, is additive, persistent, with the shorter latency and the absent carditis, and it does not respond as dramatically to the non-steroidal anti-inflammatory drugs. [3][2]
CAN'T MISS
The enthesitis-related juvenile idiopathic arthritis is the chronic cousin on the spondyloarthritis spectrum, and it overlaps with the reactive arthritis on the enthesitis, the HLA-B27 and the asymmetric lower-limb pattern. The distinction is the chronicity, because the enthesitis-related juvenile idiopathic arthritis requires the arthritis or the enthesitis for at least six weeks with the onset under sixteen, while the reactive arthritis is an acute post-infectious event that typically resolves within the three to six months. The periodic fever syndromes, including the PFAPA and the familial Mediterranean fever, enter the differential when the recurrent fever and the pharyngitis accompany the arthritis, and the Gattorno criteria for the autoinflammatory recurrent fevers guide the classification. [7][12][11]
Clinical & Bedside Assessment
The focused history anchors the diagnosis on the timeline, and the first question is always the infection. The candidate asks about the gastrointestinal illness in the preceding four weeks, with the bloody diarrhoea, the abdominal pain and the camp or the travel exposure, and about the genitourinary symptoms in the adolescent, with the dysuria, the discharge and the sexual history taken in the confidence and the privacy. The family history of the spondyloarthritis, the ankylosing spondylitis, the inflammatory bowel disease and the acute anterior uveitis supports the HLA-B27-linked susceptibility. [4][8]
The musculoskeletal examination follows the look-feel-move-measure approach across all the joints, and the specific search is for the enthesitis, the dactylitis and the sacroiliac tenderness. The enthesitis is palpated at the Achilles tendon insertion at the posterior heel and the plantar fascia insertion at the calcaneum, where the squeeze reproduces the pain. The dactylitis is the diffuse swelling of a single digit, the sausage digit, and it is a spondyloarthritis sign that the examiner rewards. The sacroiliac joints are tested by the sacroiliac compression and the FABER test, though the sacroiliitis is uncommon in the acute paediatric reactive arthritis and is more a feature of the chronic enthesitis-related arthritis. [8][7]
The eye examination looks for the conjunctivitis, the redness and the discharge, and the slit-lamp is indicated for the painful, photophobic eye that suggests the acute anterior uveitis. The skin examination looks for the keratoderma blennorrhagicum on the palms and the soles, the circinate balanitis on the glans, and the erythema nodosum on the shins, the last of which points to the Yersinia and the streptococcal trigger. The cardiac examination auscultates for the murmur of the mitral regurgitation or the aortic regurgitation that would redirect the diagnosis to the acute rheumatic fever, and the careful candidate listens for the Carey Coombs murmur and the basal diastolic murmur. [10][3]
Investigations
The joint aspirate is the first investigation when the septic arthritis is in the differential, and it is both therapeutic and diagnostic. The septic joint yields the pus with the white cell count above fifty thousand per microlitre and the positive gram stain and culture, while the reactive arthritis yields the sterile fluid with the lower cell count and the negative culture. The blood cultures and the inflammatory markers complete the sepsis screen, and the empiric intravenous antibiotics precede the culture results when the septic arthritis is suspected. [9][4]
The trigger identification relies on the stool culture, the urine and the throat. The stool culture isolates the Salmonella, the Shigella, the Campylobacter and the Yersinia, and the urine nucleic-acid-amplification test detects the Chlamydia trachomatis in the adolescent. The throat swab and the rapid antigen test detect the group A streptococcus, and the antistreptolysin-O titre and the anti-DNase B confirm the recent streptococcal infection when the throat swab is negative. The human immunodeficiency virus serology is warranted in the sexually active adolescent or the high-risk child, because the human immunodeficiency virus-associated arthritis and the reactive arthritis can coexist. [4][9]
The HLA-B27 testing supports the spondyloarthritis diagnosis but is not diagnostic on its own, because the allele is present in a substantial fraction of the healthy population. The inflammatory markers, the C-reactive protein and the erythrocyte sedimentation rate, are typically elevated in the active disease and are useful for the monitoring rather than the diagnosis. The antinuclear antibody and the rheumatoid factor are usually negative in the reactive arthritis, and they are sent to exclude the juvenile idiopathic arthritis and the lupus. The echocardiogram is the critical investigation in the suspected acute rheumatic fever or the post-streptococcal reactive arthritis, because it excludes the subclinical carditis that the auscultation misses, and the 2015 Jones criteria formally include the echocardiographic valvitis as a major criterion. [3][1]
Management — Resuscitation
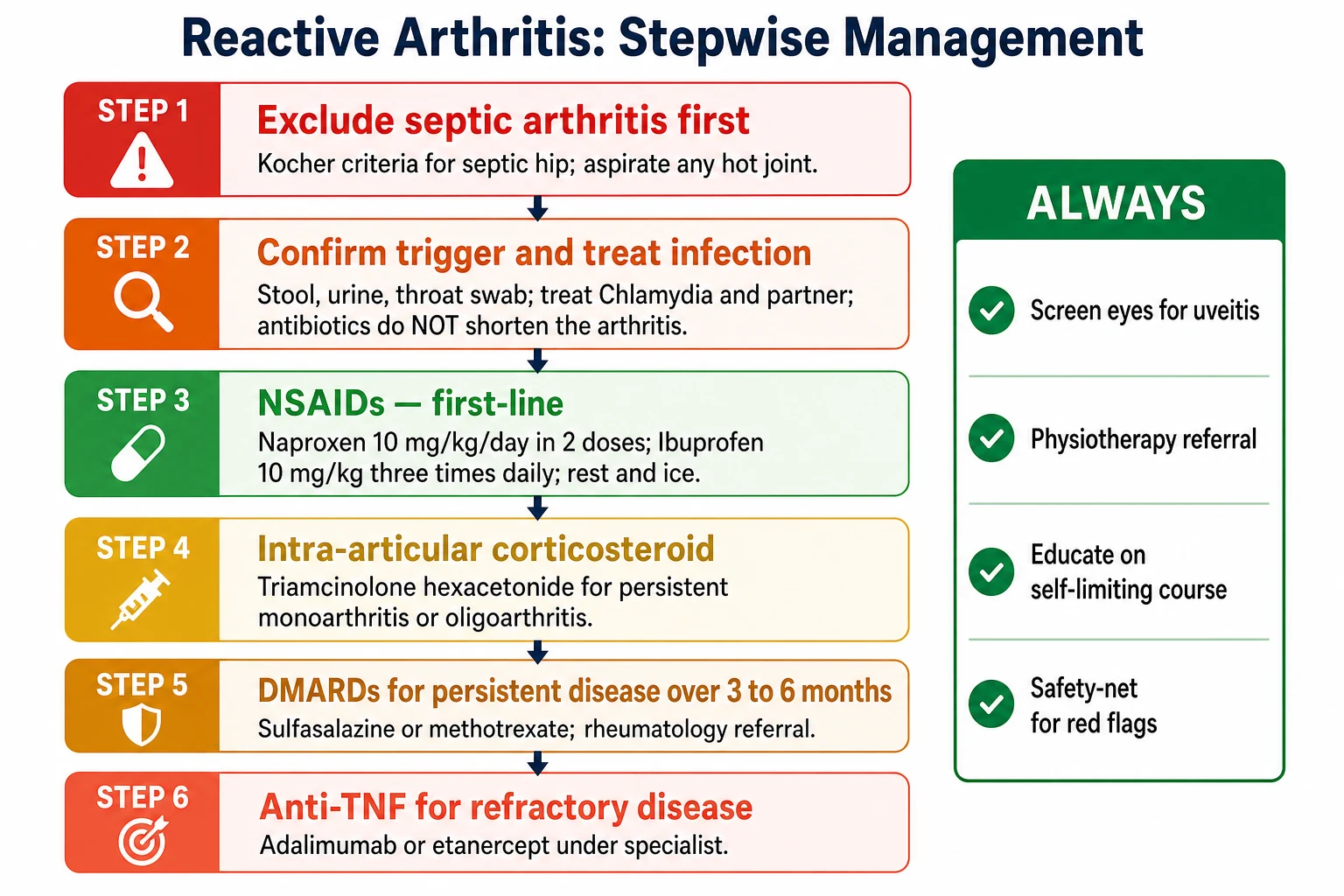
The immediate priority is the exclusion of the septic arthritis, because a missed septic joint scars the cartilage within hours. The febrile, unwell child with a single hot joint and a refusal to bear weight receives the joint aspiration, the blood cultures and the empiric intravenous antibiotics, and the reactive arthritis label is applied only when the aspirate is sterile and the sepsis is excluded. The analgesia with the paracetamol at fifteen milligrams per kilogram and the loading non-steroidal anti-inflammatory drug make the child comfortable while the workup proceeds. [9][4]
The suspected acute rheumatic fever with the carditis is the time-critical issue that demands the bed rest, the echocardiogram and the paediatric cardiology referral. The child with the migratory arthritis, the fever, the murmur and the recent streptococcal pharyngitis is managed as the acute rheumatic fever until proven otherwise, and the aspirin and the penicillin are commenced once the diagnosis is secured. The missed carditis may scar the mitral valve and cause the chronic valvular regurgitation, and this is the complication that drives the echocardiogram in every child with the post-streptococcal arthritis. [3][2]
The admission is indicated for the child with the severe pain, the high fever, the inability to bear weight or the diagnostic uncertainty, and the paediatric rheumatology or the orthopaedic referral is made for the joint aspiration, the intra-articular injection and the ongoing management. The safety-net is explicit: the family is told to return immediately for the fever, the spreading redness, the increasing pain or the visual change, and the written advice is given because the post-infectious course is unpredictable in the early phase. [9]
Management — Definitive & Stepwise
The first-line treatment of the reactive arthritis is the non-steroidal anti-inflammatory drugs, and the naproxen and the ibuprofen are the standard paediatric agents. The naproxen is given at ten milligrams per kilogram per day in two divided doses, and the ibuprofen is given at thirty milligrams per kilogram per day in three divided doses, and the child takes the medication regularly rather than as needed, because the regular dosing controls the inflammation and the morning stiffness. The full anti-inflammatory dose is continued for the duration of the active arthritis and is tapered as the symptoms resolve. [9][4]
The intra-articular corticosteroid injection is the second step for the persistent monoarthritis or the oligoarthritis that does not respond to the non-steroidal anti-inflammatory drugs. The triamcinolone hexacetonide is the preferred agent because its insolubility gives it the longest intra-articular duration and the lowest systemic absorption, and it is injected under the aseptic technique, often under the sedation or the general anaesthetic in the young child. The joint is rested for the twenty-four hours after the injection, and the response is typically rapid and durable. [9]
Naproxen (first-line NSAID)
Dose
10 mg/kg/day
The disease-modifying drugs are the third step for the persistent disease that lasts beyond the three to six months, and the sulfasalazine and the methotrexate are the standard agents. The sulfasalazine is started at thirty to fifty milligrams per kilogram per day in divided doses and is titrated to the response, and it is the preferred agent for the spondyloarthritis and the enthesitis-related pattern. The methotrexate is given at ten to fifteen milligrams per square metre once weekly, subcutaneously for the better bioavailability, with the folic acid, and it is reserved for the disease that does not respond to the sulfasalazine. [7][9]
The anti-tumour-necrosis-factor biologic is the fourth step for the refractory disease, and the adalimumab and the etanercept are the standard paediatric agents. The adalimumab is given at twenty-four milligrams per square metre every two weeks to a maximum of forty milligrams, and the etanercept is given at zero point eight milligrams per kilogram once weekly to a maximum of fifty milligrams, both under the specialist supervision. The child on the biologic with a fever has a serious infection until proven otherwise, because the tumour-necrosis-factor blockade masks the signs of the sepsis, and the empiric antibiotics come before the cultures return. [7][9]
The triggering infection is treated in parallel, with the antibiotic chosen for the organism. The Chlamydia trachomatis is treated with the azithromycin as a single oral dose of one gram in the adolescent, or the doxycycline at one hundred milligrams twice daily for seven days in the child over eight years who is not pregnant, and the partner notification and the treatment are the non-negotiable public-health obligations. The enteric infections are usually self-limiting by the time the arthritis appears, and the antibiotics do not shorten the arthritis once the trigger has been cleared, though they may be indicated for the severe or the persistent Salmonella or the Campylobacter. The candidate should carry the point that the antibiotic treats the infection, not the arthritis, because the arthritis is the sterile immune reaction. [4][9]
Specific Subtypes & Scenarios
The post-enteric reactive arthritis follows the Salmonella, the Shigella, the Campylobacter and the Yersinia gastroenteritis, and it is the commonest paediatric form. The arthritis erupts one to four weeks after the diarrhoea, and the stool culture may already be negative by the time the child presents, so the serology and the recent history are the clues. The Salmonella-triggered arthritis carries a slightly higher rate of the chronicity, and the Yersinia-triggered arthritis is associated with the erythema nodosum and, in the HLA-B27-positive child, the evolution to the spondyloarthritis. [4]
The post-genitourinary reactive arthritis follows the Chlamydia trachomatis infection, and it rises in the adolescence with the sexual activity. The arthritis is accompanied by the conjunctivitis and the urethritis in the full Reiter triad, though the triad is uncommon, and the keratoderma blennorrhagicum and the circinate balanitis are the cutaneous stigmata. The partner notification and the treatment are the public-health obligations, and the confidentiality of the adolescent is respected within the bounds of the mandatory reporting and the child-safety framework. [10]
The post-streptococcal reactive arthritis is the contested streptococcal syndrome, and its management hinges on the distinction from the acute rheumatic fever. The latency is under ten days, the arthritis is additive and persistent, the enthesitis is prominent, and the carditis is absent. The echocardiogram is performed to exclude the subclinical carditis, and the secondary penicillin prophylaxis is debated: the American Heart Association and the Australian guidance recommend the prophylaxis for a limited period, while some centres observe without the prophylaxis, because the post-streptococcal reactive arthritis does not carry the same carditis recurrence risk as the acute rheumatic fever. [1][6]
Complications & Pitfalls
The ocular complications are the chief concern, and the acute anterior uveitis is the sight-threatening inflammation that scars the eye through the synechiae, the cataract and the band keratopathy if it is missed. The slit-lamp surveillance is organised for the HLA-B27-positive child and the child with the enthesitis, because the uveitis is silent in its early stage, and the family is told to return immediately for the red eye, the pain or the photophobia. [7][8]
The chronicity and the evolution to the spondyloarthritis are the long-term concerns, and the predictors are the HLA-B27 positivity, the family history of the spondyloarthritis, the hip or the sacroiliac involvement, and the persistent enthesitis. The chronic reactive arthritis is defined as the persistence beyond the six months, and it is managed with the disease-modifying drugs and the biologics, and the child is referred to the paediatric rheumatology for the long-term care. The candidate should carry the point that the majority of the children resolve within the three to six months, and the chronicity is the minority outcome. [4][7]
The overdiagnosis of the reactive arthritis and the underdiagnosis of the septic arthritis is the classic pitfall, and it is the error that scars the child. The child with the acute swollen joint and the fever is septic arthritis until proven otherwise, and the joint aspirate and the cultures come before the reactive arthritis label. The missed carditis of the acute rheumatic fever is the other classic pitfall, because the post-streptococcal arthritis that is labelled without the echocardiogram may hide the subclinical valvitis that scars the mitral valve, and the child loses the opportunity for the penicillin prophylaxis and the cardiac surveillance. [3][1]
Prognosis & Disposition
The majority of the children with the reactive arthritis resolve within the three to six months, and the self-limiting course is the expected outcome that the family is told at the diagnosis. The chronic and the recurrent disease is the minority outcome, and it is predicted by the HLA-B27 positivity, the family history, the hip or the sacroiliac involvement and the persistent enthesitis. The follow-up is arranged with the paediatric rheumatology for the persistent disease, and the child is discharged when the disease is inactive and the function is restored. [4][9]
The post-streptococcal reactive arthritis has a variable prognosis, with the arthritis persisting for the weeks to the months in the majority and resolving without the sequelae. The secondary penicillin prophylaxis, when it is given, is continued for the duration determined by the local guidance, and the recurrence is monitored. The functional outcome and the quality of life are generally good, and the physiotherapy and the occupational therapy support the restoration of the range of the movement and the return to the school and the sport. [1][6]
Special Populations
The younger child under six presents with the limp and the refusal to bear weight, and the differential from the transient synovitis and the septic arthritis is the immediate concern. The transient synovitis of the hip follows the viral upper respiratory infection, resolves within the days to weeks, and affects a single hip in a well child, while the reactive arthritis is the asymmetric lower-limb oligoarthritis with the enthesitis and the one-to-four-week latency. The septic arthritis is the diagnosis that is never missed, and the Kocher criteria and the joint aspirate guide the distinction. [4]
The adolescent with the sexually acquired Chlamydia presents with the post-genitourinary reactive arthritis, and the confidentiality and the partner notification are the management priorities. The sexual history is taken in the private and the non-judgemental setting, the sexually transmitted infection screen is offered, and the partner notification and the treatment are arranged within the public-health framework. The mandatory reporting of the underage sexual activity and the child-safety concerns are assessed within the local legal framework, and the confidentiality is respected within these bounds. [10][4]
In the Australia and the Aotearoa New Zealand, the indigenous populations carry a heavier burden of the group A streptococcal disease and the acute rheumatic fever, driven by the household crowding, the socioeconomic disadvantage and the reduced access to the primary care. The candidate in the ANZ exam is expected to frame the acute rheumatic fever and the post-streptococcal reactive arthritis within the social determinants and the Closing the Gap framework, and to carry the heightened threshold for the echocardiogram and the penicillin prophylaxis in these communities. [3]
The immunocompromised child presents with a broader differential, because the disseminated gonococcaemia, the fungal arthritis and the mycobacterial infection enter the picture alongside the reactive arthritis. The human immunodeficiency virus-associated arthritis and the reactive arthritis can coexist, and the broader infection screen and the lower threshold for the joint aspiration are warranted. The child with the inflammatory bowel disease and the established spondyloarthritis presents with the peripheral arthritis and the enthesitis that overlap with the reactive arthritis, and the gastroenterology and the rheumatology coordination is the management framework. [9]
Evidence, Guidelines & Regional Differences
The ASAS-EULAR recommendations for the management of the axial spondyloarthritis provide the framework for the persistent and the chronic reactive arthritis, and they endorse the non-steroidal anti-inflammatory drugs as the first-line, the tumour-necrosis-factor inhibitors for the refractory disease, and the physiotherapy and the exercise throughout. The recommendations are derived largely from the adult data, and their application to the children is extrapolated, because the paediatric randomised trials for the reactive arthritis are scarce. [9]
The antibiotic treatment for the reactive arthritis is the controversy, and the evidence is mixed. The prolonged courses of the azithromycin and the doxycycline have been tested in the adult trials for the Chlamydia-triggered disease, with the some benefit in the early disease and the no benefit in the established disease, and the antibiotics are not routinely recommended for the arthritis itself. The antibiotic is given to treat the active infection and to prevent the transmission, and the candidate should carry the distinction between the infection-treating role and the arthritis-modifying role of the antibiotic. [9][4]
The secondary penicillin prophylaxis after the post-streptococcal reactive arthritis is the regional difference, and the guidance varies. The American Heart Association and the Australian guidance recommend the prophylaxis for a limited period, often twelve months with the review and the echocardiogram, while some centres in the Europe observe without the prophylaxis, because the post-streptococcal reactive arthritis does not carry the same carditis recurrence risk as the acute rheumatic fever. The candidate should name the local guidance and the rationale for the chosen approach. [1][6]
The PFAPA syndrome, the periodic fever with the aphthous stomatitis, the pharyngitis and the adenitis, is the autoinflammatory differential that enters when the recurrent fever accompanies the arthritis. The tonsillectomy has shown the benefit in the randomised trials and the cohort studies, and the cimetidine and the colchicine are the medical alternatives, particularly in the familial Mediterranean fever overlap. The Gattorno criteria for the autoinflammatory recurrent fevers guide the classification, and the genetic testing for the MEFV and the MVK mutations is offered when the hereditary periodic fever is suspected. [11][12]
Exam Pearls
The one-to-four-week latency after the gastrointestinal or the genitourinary infection is the cardinal anchor of the reactive arthritis diagnosis, and it separates it from the septic arthritis, which has no latency, and from the post-streptococcal reactive arthritis, which has the latency under ten days. The candidate who quotes the latency for each syndrome defends the differential and earns the mark. [4][1]
The full Reiter triad of the arthritis, the conjunctivitis and the urethritis is uncommon in the children, and the term is now discouraged in favour of the reactive arthritis, both because of the rarity of the complete triad and because of the Hans Reiter Nazi history. The candidate who uses the term reactive arthritis and names the triad components while noting its rarity demonstrates the modern and the ethically aware practice. [10]
The asymmetric lower-limb oligoarthritis with the enthesitis at the Achilles tendon and the plantar fascia is the clinical signature, and the HLA-B27 is present in the majority but is not diagnostic. The candidate who examines for the enthesitis and the dactylitis, and who interprets the HLA-B27 as a susceptibility marker rather than a diagnostic test, demonstrates the fellowship-level reasoning. [8][5]
The post-streptococcal reactive arthritis is additive and persistent with the latency under ten days, while the acute rheumatic fever is migratory and responds dramatically to the non-steroidal anti-inflammatory drugs with the latency of two to three weeks, and the carditis is the hallmark that separates them. The naproxen at ten milligrams per kilogram per day in two divided doses and the ibuprofen at thirty milligrams per kilogram per day in three divided doses are the first-line non-steroidal anti-inflammatory drugs, and the intra-articular triamcinolone hexacetonide is the preferred corticosteroid for the persistent monoarthritis. [1][9]
References
- [1]Ahmed S, Padhan P, Misra R Update on Post-Streptococcal Reactive Arthritis: Narrative Review of a Forgotten Disease Curr Rheumatol Rep, 2021.PMID 33569668
- [2]Balan S, Krishna MP, Sasidharan A Acute rheumatic fever and Post-streptococcal reactive arthritis Best Pract Res Clin Rheumatol, 2025.PMID 40345912
- [3]Gewitz MH, Baltimore RS, Tani LY, et al Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association Circulation, 2015.PMID 25908771
- [4]Zeidler H, Hudson AP Reactive Arthritis Update: Spotlight on New and Rare Infectious Agents Implicated as Pathogens Curr Rheumatol Rep, 2021.PMID 34196842
- [5]Sharip A, Kunz J Understanding the Pathogenesis of Spondyloarthritis Biomolecules, 2020.PMID 33092023
- [6]Bawazir Y, Towheed T, Anastassiades T Post-Streptococcal Reactive Arthritis Curr Rheumatol Rev, 2020.PMID 31393253
- [7]Naveen R, Guleria S, Aggarwal A Recent updates in enthesitis-related arthritis Rheumatol Int, 2023.PMID 36629936
- [8]Weiss PF Update on enthesitis-related arthritis Curr Opin Rheumatol, 2016.PMID 27466726
- [9]Wendling D, Prati C, Chouk M Reactive Arthritis: Treatment Challenges and Future Perspectives Curr Rheumatol Rep, 2020.PMID 32458153
- [10]Stavropoulos PG, Soura E, Kanelleas A Reactive arthritis J Eur Acad Dermatol Venereol, 2015.PMID 25199646
- [11]Wang A, Manthiram K, Dedeoglu F Periodic fever, aphthous stomatitis, pharyngitis, and adenitis (PFAPA) syndrome: A review World J Otorhinolaryngol Head Neck Surg, 2021.PMID 34430824
- [12]Gattorno M, Hofer M, Federici S, et al Classification criteria for autoinflammatory recurrent fevers Ann Rheum Dis, 2019.PMID 31018962