Paeds · rheumatology-musculoskeletal-and-sports
Relative energy deficiency in sport and athlete nutrition
Also known as RED-S · relative energy deficiency in sport · female athlete triad · low energy availability · athlete under-fuelling · energy availability · functional hypothalamic amenorrhoea · athlete triad · bone stress injury in the athlete · delayed menarche in the athlete
A fellowship approach to relative energy deficiency in sport and athlete nutrition: low energy availability is the central driver that, when energy intake falls short of the energy spent in training, suppresses the hypothalamic-pituitary axis and dismantles reproductive function, bone accrual, and a dozen other systems in the growing athlete — anchored by the Female Athlete Triad screen of energy intake, menstrual function, and bone health, the energy-availability threshold of approximately thirty kilocalories per kilogram of fat-free mass per day, and the multidisciplinary, energy-restoration-first pathway that protects the adolescent from the stress fracture, the lost menstrual cycles, and the lifelong bone deficit.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A fourteen-year-old cross-country runner presents with three months of shin pain and no menstrual period since she increased her training — a bone stress injury on the background of low energy availability and secondary amenorrhoea, the classic Triad presentation. A sixteen-year-old dancer who restricts her intake to stay lean has a sacral stress fracture and a body mass index that has fallen across the centiles — relative energy deficiency in sport at its most destructive, with an eating disorder driving the deficit. A fifteen-year-old swimmer has never had a period, and her bone age lags her chronological age — delayed puberty and slowed growth from the chronic energy deficit of the growing athlete. The task in each is to find the energy deficit, quantify the risk, and restore the energy before the bone breaks and before the window for bone accrual closes. [4] [9]
RED-S Screen — Screen, Cycle, Bone, Fuel, Refer
Overview & Definition
Relative energy deficiency in sport is the syndrome that arises when the energy an athlete expends in training chronically exceeds the energy consumed in the diet, and the body, unable to sustain every system on the deficit, down-regulates the functions it can defer. The central and measurable quantity is energy availability, defined as the dietary energy intake minus the exercise energy expenditure, divided by the fat-free mass, and expressed as kilocalories per kilogram of fat-free mass per day. Energy availability is the single number that ties the diet to the sport to the physiology, and the fellowship candidate can say the definition aloud and explain why the fat-free mass is the denominator rather than the total body weight. [5] [1]
The threshold that the candidate must hold is the level of energy availability at which the reproductive axis is disrupted. The seminal experiment of Loucks and Thuma established that luteinising hormone pulsatility, the brain's signal to the ovary, is measurably disrupted when energy availability falls below approximately thirty kilocalories per kilogram of fat-free mass per day in regularly menstruating women, and that optimal function is sustained at approximately forty-five kilocalories per kilogram of fat-free mass per day and above. The thirty-kilocalorie threshold is the number the examiner probes, and the forty-five-kilocalorie optimal is its complement. [5] [2]
The clinical importance flows from the fact that the growing athlete is building her bone bank in parallel with her sport, and the energy deficit dismantles the bone accrual at the exact developmental window when it matters most. An adolescent accrues the great majority of her adult skeletal mass between the early teens and the early twenties, and the bone she fails to lay down during these years is never fully recovered. A stress fracture in a cross-country runner is the visible tip of the deficit, and the lifelong deficit in bone mineral density is the invisible mass of the iceberg beneath it. The fellowship task is to find the deficit, quantify the risk, and restore the energy while the bone window is still open. [9] [10]
Classification
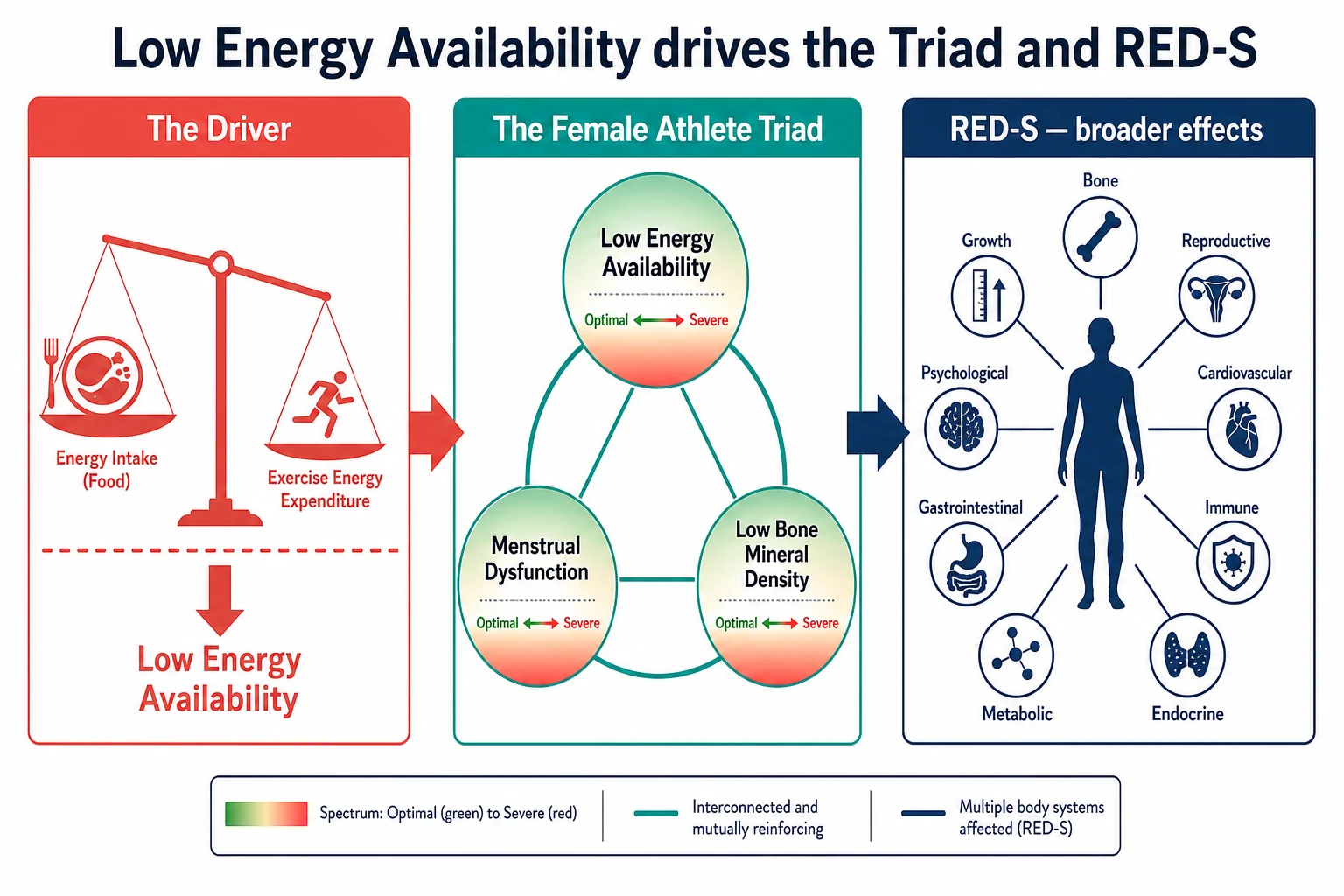
The classification of the energy-deficient athlete is held by two complementary frameworks that share the same underlying physiology, and the fellowship candidate presents both without forcing a choice between them. The Female Athlete Triad is the older and the narrower framework, organising the deficit around three spectra — energy availability with or without disordered eating, menstrual function from eumenorrhoea through oligomenorrhoea to amenorrhoea, and bone mineral density from optimal through low to osteoporosis. The three spectra move together, and the severity along each determines the cumulative risk. [4] [1]
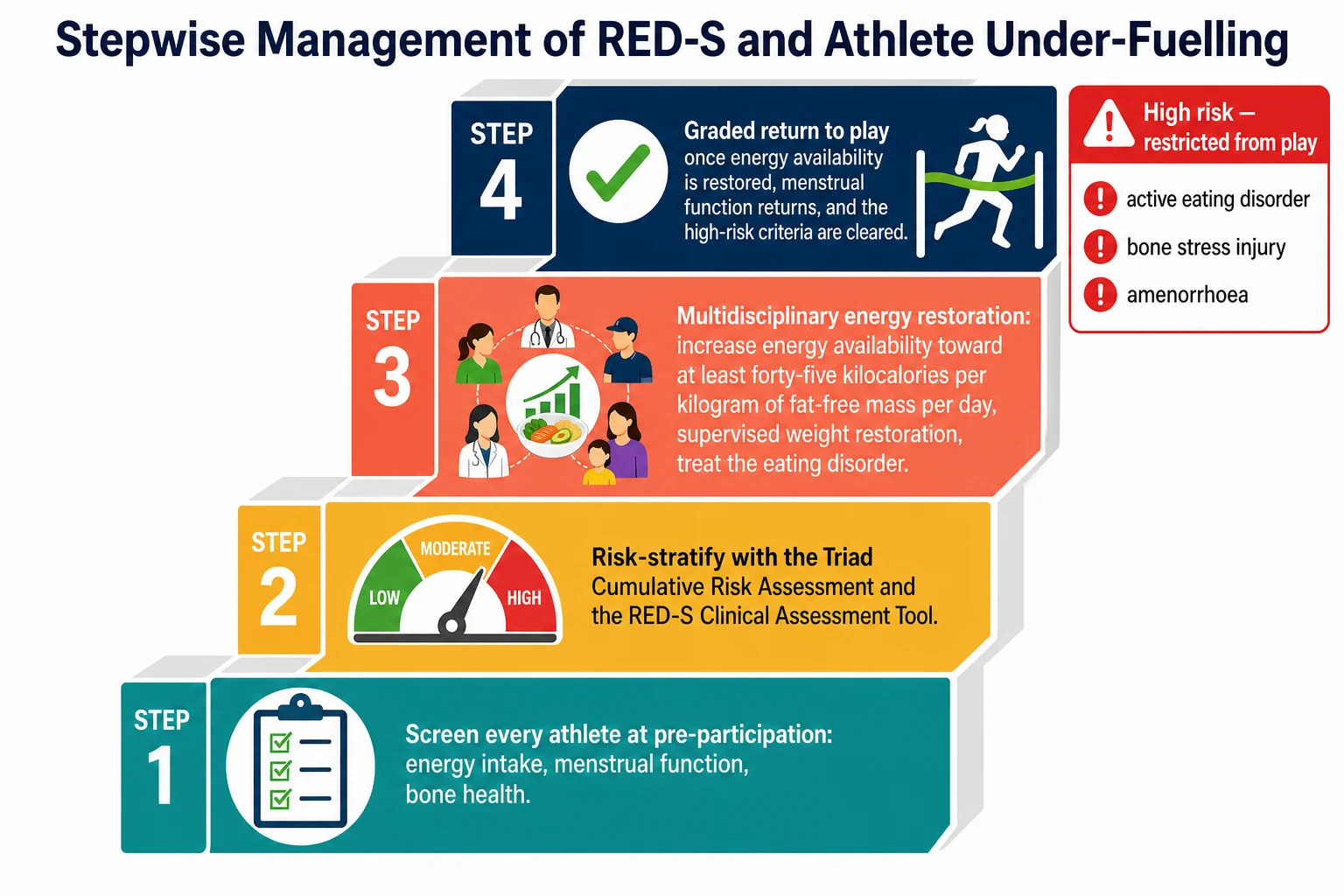
The 2014 Female Athlete Triad Coalition Consensus Statement operationalised the three spectra into a Cumulative Risk Assessment that scores the athlete along each axis — the energy availability, the body mass index, the menstrual delay, the bone mineral density Z-score, and the stress-fracture history — and stratifies her into low, moderate, or high risk. The risk stratum, in turn, decides the clearance to train and to compete, and the high-risk athlete is restricted from play until the energy is restored and the criteria for return are met. The Cumulative Risk Assessment is the tool the team-sport physician and the general paediatrician use at the pre-participation visit. [4] [11]
Relative energy deficiency in sport is the 2014 International Olympic Committee reframing that widens the lens beyond the three Triad spectra to the full web of systems the energy deficit dismantles. The 2018 and 2023 updates extended the framework and introduced the RED-S Clinical Assessment Tool, a severity-and-risk model that captures the reproductive, the bone, the haematological, the cardiovascular, the immune, the metabolic, the endocrine, the gastrointestinal, the psychological, and the growth-and-development effects, and that applies to the male athlete as much as the female. The comparison study confirmed that the two tools place the high-risk athlete in the same restricted-from-play category, so the candidate may use either with confidence. [3] [11]
Epidemiology & Risk Factors
Low energy availability is common in the young athlete, and the prevalence rises with the training load, the leanness demand of the sport, and the developmental stage. Surveys of adolescent female athletes in leanness and endurance sports find that a substantial proportion fall below the energy-availability threshold, and the inadvertent undereating study confirmed that many of these young women are not restricting their intake intentionally but simply failing to match the energy they spend. The endurance, the aesthetic, and the weight-class sports — distance running, cross-country, swimming, gymnastics, dance, rowing, and the combat sports — carry the highest prevalence, and the team sports with a leanness component are close behind. [7] [8]
The risk factors for the energy deficit cluster around the sport, the body, and the mind. The leanness and endurance sport is the sporting risk factor, because the sport rewards a low body weight and demands a high training volume. The adolescent growth spurt is the developmental risk factor, because the energy cost of growth compounds the energy cost of the training, and the athlete who holds her intake steady while she grows falls into deficit. The drive for thinness and the perfectionist temperament are the psychological risk factors, and the manifest eating disorder is the highest-risk state. The early sport specialisation and the sudden increase in training load are the mechanical risk factors for the bone stress injury. [4] [9]
The bone stress injury is the complication that brings the deficit to clinical attention, and the epidemiology of the stress injury mirrors the epidemiology of the deficit. The middle-school runner study found that a meaningful proportion of young runners sustain a bone stress injury, and the risk rises with the low energy availability, the menstrual delay, the prior stress fracture, and the late menarche. The tibia is the commonest site, and the high-risk sites — the femoral neck, the sacrum, the pelvis, and the anterior tibial cortex — are the ones that demand the urgent imaging and the protected rehabilitation. The male athlete is not spared, and the deficit in the male presents with the stress injury, the low testosterone, and the impaired bone. [9] [10]
Pathophysiology
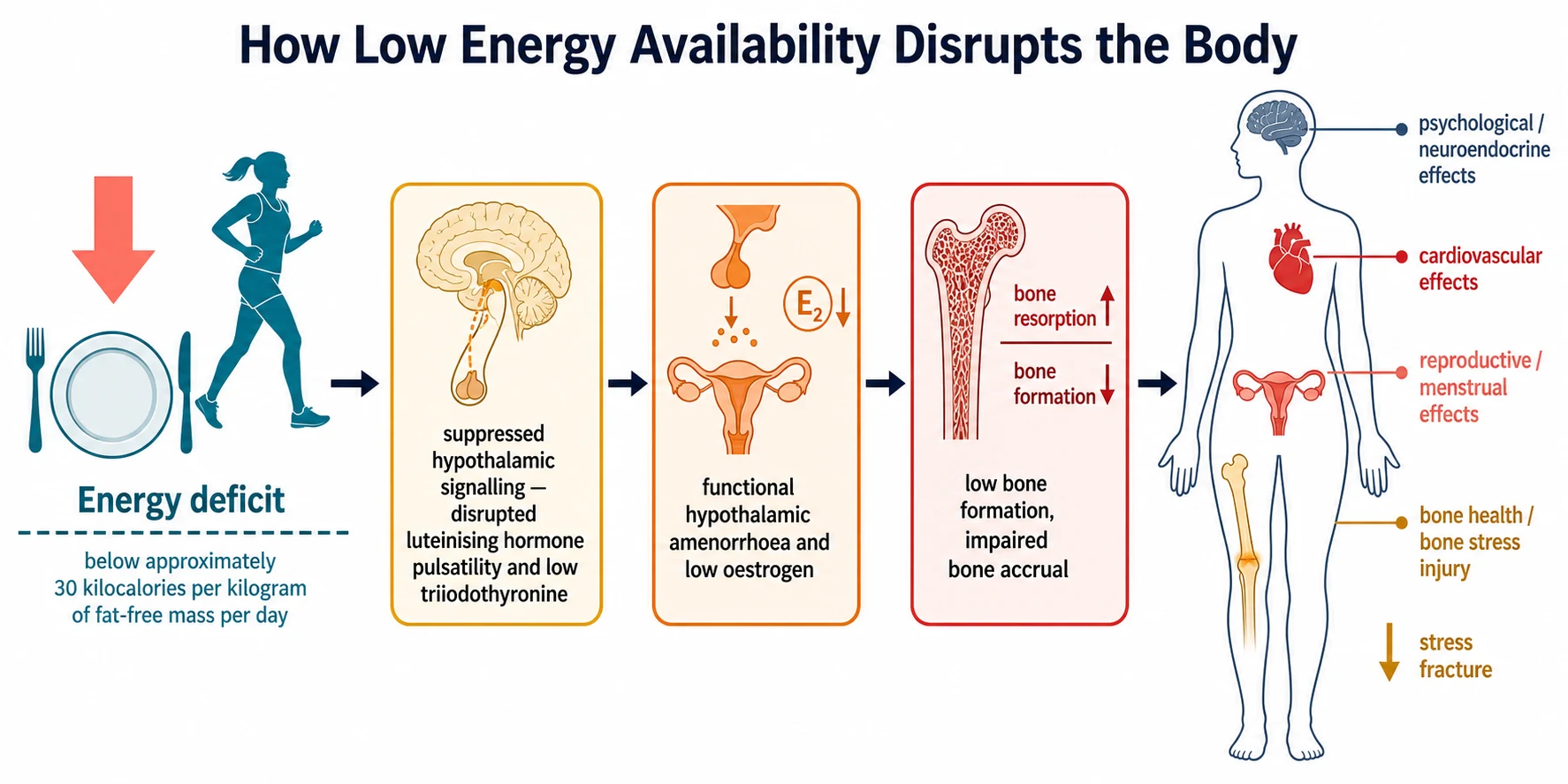
The pathophysiology of relative energy deficiency in sport is the physiology of the body's survival response to an energy deficit, and it is best understood as a cascade that begins in the brain and ends in the bone. The deficit is detected by the hypothalamus, which interprets the low energy availability as a threat to survival and down-regulates the systems it can defer to preserve the energy for the essential functions of the heart, the brain, and the locomotion. The reproductive axis is the first and the most energy-costly system to be deferred, and the bone and the growth follow. [5] [6]
The reproductive cascade begins with the disruption of the pulsatile secretion of gonadotropin-releasing hormone from the hypothalamus, which is the master signal to the pituitary. The Loucks and Thuma experiment established that the luteinising hormone pulsatility, the pituitary's relay to the ovary, is disrupted at the threshold of approximately thirty kilocalories per kilogram of fat-free mass per day, and the disruption cascades to a fall in the ovarian oestrogen and the loss of the menstrual cycle. The triiodothyronine falls, reflecting the metabolic down-regulation, and the resting energy expenditure drops as the body defends its stores. The clinical correlate is the oligomenorrhoea and the amenorrhoea, and the invisible correlate is the hypoestrogenaemia that dismantles the bone. [5] [6]
The bone cascade is the most clinically and developmentally important consequence. The oestrogen normally restrains the bone resorption and supports the bone formation, and the hypoestrogenaemia of the energy deficit tips the balance toward the resorption. In the growing athlete, the energy deficit additionally suppresses the bone formation through the low insulin-like growth factor and the low triiodothyronine, so the adolescent fails to accrue the bone mass at the developmental window when the accrual is most rapid and most consequential. The bone that is not laid down during the late teens is never fully recovered, and the stress fracture is the symptomatic expression of the weakened, under-built skeleton. [9] [10]
The wider RED-S pathophysiology extends the cascade to the other systems, and the 2023 update frames the multi-system model. The cardiovascular system shows the bradycardia and the orthostatic hypotension of the physiological down-regulation, and the endothelial dysfunction adds a cardiovascular risk. The immune system is impaired, and the athlete suffers the recurrent infections and the slow recovery. The metabolic and the endocrine systems show the low triiodothyronine, the hypercortisolaemia, and the impaired glucose handling. The gastrointestinal system shows the delayed gastric emptying and the constipation that worsen the energy intake. The psychological effects include the depression and the anxiety, and the drive for thinness that drives the deficit. The growth and the maturation are slowed in the younger athlete, with the bone age lagging the chronological age. [3] [2]
Clinical Presentation
The presentation of the energy-deficient athlete is shaped by which system the deficit has dismantled first, and the fellowship candidate holds the full differential in mind from the moment the young athlete walks, or limps, into the room. The bone stress injury is the commonest presentation, and the athlete describes a progressive, activity-related pain in a weight-bearing bone — the shin of the runner, the foot of the dancer, the hip of the rower — that began as an ache and worsened to a pain that forces her to stop. The high-risk sites, the femoral neck and the sacrum, present with the groin or the buttock pain and the limp, and they demand the urgent imaging. [9] [10]
The menstrual presentation is the most reliable clinical marker of the energy deficit, and it is the signal the candidate must ask about explicitly and document carefully. The secondary amenorrhoea, the absence of menses for three or more months, is the classic presentation in the athlete who has increased her training. The oligomenorrhoea, the cycles longer than thirty-five days, is the earlier signal. The primary amenorrhoea, the absence of the menarche by fifteen years in an athlete with the secondary sexual development, is the presentation in the younger athlete who entered the deficit before her cycle began. The fellowship skill is to treat the absent or the irregular cycle as the energy deficiency until proven otherwise, and never to dismiss it as normal for a sportswoman. [6] [4]
The nutritional and the psychological presentation is the third axis, and it ranges from the inadvertent undereating of the athlete who simply fails to match her training to the manifest eating disorder of the athlete who restricts her intake to control her weight. The inadvertent undereater describes a full training schedule with a diet that has not grown to match it, and she is often surprised to learn she is in deficit. The athlete with the drive for thinness describes a preoccupation with her body, a restriction of the food groups, and a fear of weight gain, and the manifest eating disorder carries the bradycardia, the orthostatic hypotension, the lanugo, and the hypothermia that mark the advanced deficit. The fatigue, the recurrent infections, and the slow recovery are the multi-system presentations that the candidate elicits with a directed history. [7] [8]
Which reassuring-sounding stories must never close the search for the energy deficit? An athlete who has never had a period may be told that the late menarche is familial, and the energy deficit that is delaying her puberty is missed. An athlete with a stress fracture may be told that the injury is purely mechanical, and the underlying low bone density is not assessed. And an athlete who is performing well may be told that her weight loss is the sign of improved fitness, and the eating disorder that is driving the deficit is not recognised. The full Triad and RED-S screen is run on every young athlete with a stress injury, a menstrual change, or a falling weight, every time. [3] [9]
Differential Diagnosis
The differential diagnosis of the energy-deficient athlete is built around the presenting system, and the fellowship candidate works through the causes of the amenorrhoea, the stress fracture, and the weight loss in parallel. The secondary amenorrhoea in the athlete is functional hypothalamic amenorrhoea from the energy deficit until the full endocrine evaluation excludes the other causes, and the polycystic ovary syndrome, the hyperprolactinaemia, the thyroid dysfunction, and the premature ovarian insufficiency are the principal mimics. The key discriminator is the low or the normal gonadotropins and the low oestrogen of the functional hypothalamic amenorrhoea, against the elevated luteinising hormone and the normal oestrogen of the polycystic ovary syndrome. [6] [4]
The bone stress injury in the athlete is the mechanical failure of an under-built or an over-loaded bone, and the differential includes the stress fracture of the high training load, the stress fracture of the low bone density, the stress reaction without a fracture line, and the rare but serious causes of the bone pain — the osteoid osteoma, the osteomyelitis, and the malignancy. The high-risk sites, the femoral neck and the sacrum, are imaged early, because the delay risks the displacement and the avascular necrosis. The repetitive-loading injury of the tibia is separated from the chronic exertional compartment syndrome and the medial tibial stress syndrome by the history, the examination, and the imaging. [10] [9]
The weight loss and the falling body mass index in the athlete carry the differential of the eating disorder, the inadvertent undereating, the over-training, the thyroid dysfunction, the coeliac disease, the inflammatory bowel disease, and the malignancy. The drive for thinness, the restriction of the food groups, and the preoccupation with the body weight point to the eating disorder, and the coeliac and the inflammatory markers screen for the organic causes. The fellowship answer runs the screen for the organic cause while it assesses the energy balance, because the two are not mutually exclusive and the organic cause may compound the deficit. [7] [8]
The male athlete with the energy deficit presents with the stress fracture, the low testosterone, and the impaired libido, and the differential includes the primary and the secondary hypogonadism. The relative energy deficiency in sport framework is the one that captures the male, and the candidate applies the same energy-availability logic and the same multidisciplinary pathway. The delayed puberty and the slowed growth in the child athlete raise the differential of the constitutional delay, the growth hormone deficiency, and the chronic disease, and the energy deficit is the cause that is reversible with the energy restoration. [3] [2]
Clinical & Bedside Assessment
The bedside assessment of the young athlete begins with the history, and the history is structured around the three Triad spectra and the wider RED-S web. Ask about the sport, the training volume, the weekly hours, and the recent change in the load, because the sudden increase is the mechanical trigger for the stress injury. Ask about the diet, the meal pattern, the food groups, and the energy intake, and ask directly about the restriction, the bingeing, the purging, and the use of the laxatives and the diuretics, because the disordered eating is the highest-risk state. Ask about the menstrual history, the age at the menarche, the cycle length, and the last period, because the absent cycle is the vital sign of the deficit. Ask about the fatigue, the infections, the mood, and the sleep, because the multi-system effects are elicited only by the directed question. [4] [7]
The growth and the anthropometry are measured and plotted, because the falling weight and the falling body mass index across the centiles are the objective signs of the deficit. Measure the height, the weight, and the body mass index, and plot them on the age-appropriate chart, because the slowing of the growth velocity is the sign of the energy deficit interfering with the growth in the younger athlete. The body composition, when available, quantifies the fat-free mass that anchors the energy-availability calculation, and the skinfold measures provide the field estimate when the laboratory method is not available. The documentation of the trend over time is more informative than any one-off value, because the trajectory of the weight and the body mass index reveals the deficit that the isolated reading conceals. [8] [6]
The physical examination screens for the multi-system signs of the deficit and excludes the organic mimics. Check the heart rate for the bradycardia and the orthostatic vital signs for the postural drop, because the physiological down-regulation and the volume depletion are the cardiovascular signatures of the advanced deficit. Examine for the lanugo, the cold extremities, and the hypothermia of the eating disorder. Examine the painful bone for the focal tenderness and the limp that demand the imaging. Perform the pubertal Tanner staging, because the delayed puberty and the slow progression are the growth-and-development signs. Examine the skin for the hyperpigmentation of the Addison disease and the striae of the cortisol excess, because the organic endocrine cause is excluded at the bedside. [6] [3]
The validated screening tools refine the assessment and quantify the risk. The Low Energy Availability in Females Questionnaire, the LEAF-Q, is the validated tool that screens the female endurance athlete for the energy availability risk through the menstrual, the injury, and the gastrointestinal items. The Female Athlete Triad Cumulative Risk Assessment and the RED-S Clinical Assessment Tool score the athlete along the risk axes and stratify her into the low, the moderate, or the high risk, and the comparison study confirmed the agreement of the two tools on the high-risk, restricted-from-play category. The candidate names the tool and applies it, because the risk stratum decides the clearance to train and to compete. [7] [11]
Investigations
The investigation of the energy-deficient athlete is guided by the presenting system and the risk stratification, and the tests are chosen to confirm the deficit, to exclude the mimics, and to quantify the bone. The laboratory tests confirm the functional hypothalamic amenorrhoea and exclude the organic causes, and the bone imaging quantifies the density and reveals the stress injury. The investigation is not a blanket panel but a directed workup that the risk assessment frames. [6] [4]
The endocrine laboratory tests in the amenorrhoeic athlete confirm the functional hypothalamic pattern and exclude the mimics. The follicle-stimulating hormone and the luteinising hormone are low or in the low-normal range, and the oestradiol is low, confirming the hypogonadotrophic hypogonadism of the energy deficit. The prolactin excludes the hyperprolactinaemia, the thyroid-stimulating hormone and the free thyroxine exclude the thyroid dysfunction, and the morning cortisol excludes the adrenal insufficiency. The triiodothyronine is often low, reflecting the metabolic down-regulation, and the insulin-like growth factor may be reduced. A pregnancy test is performed in every sexually active amenorrhoeic adolescent before the endocrine workup. [6] [2]
The nutritional laboratory tests quantify the deficiencies that compound the bone and the haematological effects. The full blood count and the ferritin screen for the iron-deficiency anaemia that is common in the athlete and that worsens the fatigue and the performance. The 25-hydroxyvitamin D level screens for the vitamin D deficiency, with the sufficiency defined as a level of fifty nanomoles per litre or above, and the calcium and the phosphate complete the bone screen. The coeliac serology and the inflammatory markers screen for the organic cause of the weight loss, and the renal and the liver function frame the general health. [2] [3]
The bone assessment is the cornerstone of the investigation, and the dual-energy X-ray absorptiometry is the modality that quantifies the bone mineral density. The paediatric and the adolescent athlete is reported with the Z-score, the age-matched comparison, and never the T-score that is used in the older adult. A Z-score of negative two or below defines the low bone mineral density for the chronological age, and a Z-score between negative one and negative two with the risk factors of the energy deficit and the menstrual dysfunction is the concerning intermediate zone. The bone density is measured at the lumbar spine, which is the trabecular site most affected by the energy deficit, and the hip. The repeat measurement tracks the response to the energy restoration over the year. [9] [4]
The imaging of the stress injury is chosen by the site and the suspicion. The magnetic resonance imaging is the modality that reveals the bone marrow oedema of the early stress reaction and the fracture line of the established stress fracture, and it is the investigation of choice for the high-risk site such as the femoral neck and the sacrum, where the delay risks the displacement. The computed tomography defines the cortical lesion of the anterior tibia. The high-risk site is imaged urgently, and the low-risk site is managed with the activity cessation and the reassessment, reserving the imaging for the pain that fails to settle. [10] [9]
Management — Resuscitation
Resuscitation is rarely the immediate need in the energy-deficient athlete, because most present with the sub-acute or the chronic deficit, but the exceptions are the athlete with the advanced eating disorder and the displaced high-risk stress fracture, and these demand the urgent pathway. The athlete with the bradycardia, the orthostatic hypotension, the hypothermia, and the falling weight of the advanced eating disorder is the medical emergency that demands the hospital admission, the cardiac monitoring, and the careful, supervised refeeding, because the rapid refeeding carries the refeeding syndrome with the hypophosphataemia and the arrhythmia. [6] [4]
The athlete with the suspected displaced femoral-neck stress fracture is kept non-weight-bearing and imaged urgently, because the displacement risks the avascular necrosis and the early arthritis, and the orthopaedic team is involved from the outset. The high-risk sacral and pelvic stress injuries are managed with the protected weight-bearing and the pain control, and the urgent imaging confirms the diagnosis. The principle is that the high-risk bone is treated as the threatened fracture until the imaging proves the stable lesion, and the weight-bearing is restricted accordingly. [10] [9]
The refeeding of the severely under-fuelled athlete is the resuscitation that demands the greatest care, because the restoration of the energy after the prolonged deficit shifts the electrolytes and the fluid in the refeeding syndrome. The phosphate, the magnesium, and the potassium are monitored, the thiamine is given before the first feed, and the energy is increased gradually under the dietitian's supervision. The principle is that the energy is restored, but it is restored safely, because the harm of the rapid refeeding is as real as the harm of the deficit. The general paediatrician's role is to recognise the severe deficit, to arrange the admission, and to involve the eating-disorder and the dietitian team. [6] [3]
Management — Definitive & Stepwise
The definitive management of the energy-deficient athlete is the energy restoration, and the energy restoration is the only treatment that reverses the functional hypothalamic amenorrhoea and rebuilds the bone. The Endocrine Society guideline on the functional hypothalamic amenorrhoea is explicit that the first-line treatment is the increase in the energy availability and the weight gain, and that the hormonal therapy, including the combined oral contraceptive pill, is not the first-line treatment for the bone in the energy-deficient athlete, because it does not restore the bone and it masks the menstrual signal. The energy availability is increased toward the optimal level of approximately forty-five kilocalories per kilogram of fat-free mass per day, through the increase in the dietary intake and the reduction in the training load. [6] [5]
The energy restoration is achieved by the three levers of the intake, the expenditure, and the weight. The dietary intake is increased through the addition of the energy-dense, the nutrient-dense foods, with the protein spread across the day to support the muscle and the bone, and the carbohydrate timed around the training to fuel the session and the recovery. The training load is reduced, with the rest days scheduled and the intensity moderated, and the non-essential energy expenditure is curtailed. The weight is restored toward the healthy range, with the target weight that supports the menstrual function individualised to the athlete, and the weight gain of the order of the half to the one kilogram per month is a reasonable pace in the outpatient. The dietitian owns the prescription, and the physician owns the medical oversight. [8] [3]
The nutritional supplementation addresses the specific deficiencies that compound the deficit. The calcium intake is optimised toward the adequate intake of thirteen hundred milligrams per day for the nine-to-eighteen-year-old, preferably through the dairy and the fortified foods, and the supplement is added when the dietary intake is insufficient. The vitamin D is supplemented to maintain the 25-hydroxyvitamin D level at fifty nanomoles per litre or above, and the iron is supplemented when the ferritin is low, because the iron deficiency compounds the fatigue and the performance. The supplement is the adjunct to the energy restoration, never the substitute for it, and the fellowship answer frames the energy first. [2] [3]
The psychological management is the load-bearing part of the pathway in the athlete with the disordered eating or the manifest eating disorder, and the multidisciplinary team is the structure that delivers it. The psychologist or the eating-disorder clinician addresses the drive for thinness, the body image, and the perfectionism, and the family is involved in the treatment of the adolescent. The coach is engaged as the ally, because the modified training and the support of the recovery depend on the coach's understanding. The paediatrician, the dietitian, the psychologist, the physiotherapist, and the coach form the team, and the family is the centre. The manifest eating disorder may demand the specialist eating-disorder service, and the inpatient admission is reserved for the severe, the medically unstable case. [4] [7]
The Triad and RED-S management moves and their anchor
Specific Subtypes & Scenarios
The secondary amenorrhoea in the endurance athlete is the subtype that defines the classic Triad. The young runner or the rower who has increased her training presents with the absence of menses for three or more months, and the workup confirms the low gonadotropins and the low oestrogen of the functional hypothalamic amenorrhoea. The management is the energy restoration, with the reduction in the training load and the increase in the dietary intake, and the menstrual function returns as the energy availability is restored toward the optimal level. The Endocrine Society guideline frames the energy restoration as the first-line treatment, and the oral contraceptive pill is reserved for the contraception and the bone protection in the specific, counselled case where the energy restoration has failed. [6] [5]
The bone stress injury in the young runner is the subtype that brings the deficit to the orthopaedic and the sports-medicine attention. The progressive shin pain of the runner, or the groin pain of the high-risk femoral-neck lesion, is the bone stress injury on the background of the low energy availability and the menstrual dysfunction. The imaging confirms the stress reaction or the fracture line, and the management is the protected weight-bearing, the energy restoration, and the graded return. The high-risk site is managed with the urgency that the displacement risk demands, and the bone density is measured to quantify the underlying deficit. The fellowship skill is to treat every bone stress injury in a young athlete as the tip of the energy-deficiency iceberg. [9] [10]
The disordered eating and the eating disorder in the aesthetic athlete is the subtype that carries the highest risk and the greatest complexity. The dancer or the gymnast with the drive for thinness restricts her intake to control her weight, and the deficit deepens to the manifest eating disorder with the bradycardia and the falling weight. The management is the specialist eating-disorder pathway, with the psychologist, the dietitian, and the paediatrician, and the inpatient admission is reserved for the medically unstable case. The athlete is restricted from play until the eating disorder is treated and the energy is restored, and the multidisciplinary team owns the clearance. The fellowship answer frames the eating disorder as the medical condition, not the lifestyle choice, and treats it with the urgency it demands. [7] [4]
The male athlete with the energy deficit is the subtype that the RED-S framework captures and the Triad framework misses. The male endurance athlete or the weight-class athlete presents with the stress fracture, the low testosterone, and the impaired libido, and the energy availability is the driver. The workup confirms the low gonadotropins and the low testosterone, and the management is the energy restoration, with the same multidisciplinary pathway. The male athlete is screened at the pre-participation visit, and the deficit is treated with the same urgency as the female, because the bone and the hormonal consequences are real. The 2023 update frames the male in the RED-S severity-and-risk model. [3] [2]
The delayed puberty and the slowed growth in the child athlete is the subtype that the general paediatrician must recognise, because the energy deficit interferes with the growth and the maturation at the developmental window when the growth is most rapid. The child athlete who trains intensively may present with the delayed puberty and the bone age that lags the chronological age, and the energy deficit is the reversible cause. The management is the reduction in the training and the restoration of the energy, with the monitoring of the growth and the puberty, and the endocrinology team is involved when the delay is significant. The fellowship skill is to hold the energy balance and the growth together in the child athlete. [3] [6]
Complications & Pitfalls
The complications of the unrecognised or the untreated energy deficit span the skeleton, the reproductive system, and the cardiovascular system, and the harms are both the acute and the lifelong. The displaced femoral-neck stress fracture is the acute orthopaedic complication, and it carries the risk of the avascular necrosis and the early arthritis that the urgent imaging and the protected weight-bearing prevent. The recurrent and the multiple stress fractures are the chronic orthopaedic complication, and they reflect the persistent low bone density that the uncorrected deficit maintains. [9] [10]
The lifelong complication is the deficit in the bone mineral density that the adolescent fails to accrue during the energy-deficient years, and the bone that is not laid down during the late teens is never fully recovered. The energy-deficient adolescent enters the adult life with the lower peak bone mass, and the lower peak bone mass raises the lifetime risk of the osteoporosis and the fragility fracture. The fellowship answer frames the bone accrual as the finite developmental window, and the energy restoration as the intervention that protects the bone for the lifetime, not only for the sport. The reduced fertility and the prolonged time to the conception are the reproductive complications of the prolonged amenorrhoea. [10] [6]
The pitfall of the reassuring label is the error that delays the recognition of the deficit. The athlete who has never had a period is told that the late menarche is familial, and the energy deficit is missed. The athlete with the stress fracture is told that the injury is mechanical, and the low bone density is not assessed. The athlete who is performing well is told that her weight loss is the sign of the fitness, and the eating disorder is not recognised. The safeguard is the rule that the full Triad and RED-S screen is run on every young athlete with a stress injury, a menstrual change, or a falling weight, and the absent cycle is the energy deficiency until proven otherwise. [3] [9]
The pitfall of the oral contraceptive pill is the specific error that the fellowship candidate must name. The pill is prescribed to the amenorrhoeic athlete to induce the withdrawal bleed and to protect the bone, but the induced bleed is not the menstrual recovery, and the pill does not restore the bone density in the energy-deficient athlete. The pill masks the menstrual signal, and the athlete, the coach, and the family are falsely reassured that the deficit is resolved. The safeguard is the Endocrine Society guideline, which frames the energy restoration as the first-line treatment and reserves the pill for the specific, counselled case. The candidate who names the pill as not the first-line treatment demonstrates the depth the fellowship demands. [6] [5]
The pitfall of the missed eating disorder is the error that the psychological assessment catches. The athlete with the drive for thinness is overlooked because she is high-performing and disciplined, and the eating disorder is missed until the weight falls and the bradycardia appears. The safeguard is the direct question about the restriction, the body image, and the drive for thinness at every visit, and the multidisciplinary referral when the screen is positive. The fellowship answer holds the physical and the psychological frames together, because the eating disorder is the medical condition that drives the highest-risk deficit. [7] [4]
Prognosis & Disposition
The prognosis of the energy-deficient athlete is excellent when the deficit is recognised early and the energy is restored promptly, because the functional hypothalamic amenorrhoea reverses and the bone accrual resumes with the restoration of the energy balance. The menstrual function typically returns within the months of the energy restoration, and the bone density improves over the year with the continued restoration. The athlete who is rested and re-fed early returns to her sport with the restored cycle and the protected bone, and the long-term bone and the reproductive outcomes are favourable. The fellowship answer frames the prognosis as the function of the early recognition and the prompt restoration. [6] [5]
The prognosis worsens with the delay in the recognition and the persistence of the deficit. The athlete whose deficit is maintained through the adolescent years accrues the lower peak bone mass, and the bone deficit is never fully recovered. The recurrent and the multiple stress fractures reflect the persistent low density, and the prolonged amenorrhoea extends the time to the conception and the reduced fertility. The eating disorder carries the prognosis of the psychiatric condition, and the outcome depends on the engagement with the treatment and the multidisciplinary team. The candidate frames the prognosis as the function of the early intervention, because the bone window is finite. [10] [9]
The disposition is shared between the general paediatrician, the sports-and-exercise physician, the dietitian, the psychologist, the physiotherapist, and the coach, and the family is the centre of the team. The general paediatrician owns the initial assessment, the risk stratification, the energy-restoration oversight, and the safety-net. The sports-and-exercise physician owns the bone and the return-to-play decision, and the orthopaedic surgeon owns the displaced high-risk fracture. The dietitian owns the energy prescription, and the psychologist owns the eating-disorder treatment. The physiotherapist owns the rehabilitation of the stress injury and the graded return, and the coach owns the modified training. The fellowship answer names the team and the roles, and never holds a high-risk athlete in the unrestricted training when the restriction is indicated. [4] [11]
Special Populations
The adolescent athlete is the population at the centre of this topic, and the developmental vulnerability of the growing skeleton and the growing reproductive axis is the reason the deficit is most consequential in this age group. The energy deficit interferes with the growth, the puberty, and the bone accrual at the developmental window when each is most rapid, and the harm is both the acute and the lifelong. The fellowship candidate frames the adolescent athlete as the priority for the screen and the early intervention, because the bone window is finite and the early restoration protects the bone for the lifetime. [3] [9]
The male athlete is the population that the RED-S framework captures and the older Triad framework overlooked. The male endurance and the weight-class athlete presents with the stress fracture and the low testosterone, and the energy availability is the driver. The male is screened at the pre-participation visit, with the questions adapted to the male presentation, and the deficit is treated with the same multidisciplinary pathway and the same urgency as the female. The fellowship answer names the male athlete and applies the RED-S framework, because the bone and the hormonal consequences are real and the deficit is reversible. [3] [2]
The athlete with the gender and the sexual diversity is the population that carries the additional consideration of the body composition and the hormonal context. The transgender and the gender-diverse athlete may face the pressures of the body image and the weight that compound the energy deficit, and the assessment adapts to the individual's hormonal and the developmental context. The eating disorder and the drive for thinness are not confined to the cisgender female, and the screen and the multidisciplinary pathway are applied without the assumption. The fellowship candidate holds the inclusive frame and the individualised assessment. [3] [7]
The Indigenous, the remote, and the socioeconomically disadvantaged athlete is the population that faces the additional burdens of the access and the equity. The distance to the dietitian, the psychologist, and the dual-energy X-ray absorptiometry delays the recognition and the treatment of the deficit, and the cost of the food and the supplements compounds the under-fuelling. The newly arrived migrant or the refugee athlete may carry the nutritional and the cultural context that the assessment must understand, and the screen is adapted to the language and the cultural frame. The fellowship answer acknowledges the inequities and builds the pathways that close the gap, because the energy restoration depends on the access as much as on the knowledge. [8] [9]
Evidence, Guidelines & Regional Differences
The evidence base for the relative energy deficiency in sport rests on the foundational experiment of Loucks and Thuma, which established the energy-availability threshold at which the reproductive axis is disrupted. The 2003 paper demonstrated that the luteinising hormone pulsatility is disrupted when the energy availability falls below approximately thirty kilocalories per kilogram of fat-free mass per day in regularly menstruating women, and it set the threshold that every subsequent guideline has reaffirmed. The optimal level of approximately forty-five kilocalories per kilogram of fat-free mass per day is the complementary number that the candidate holds. [5] [2]
The guideline framework is anchored by the three International Olympic Committee consensus statements on the relative energy deficiency in sport. The 2014 statement introduced the RED-S concept as the reframing that widened the lens beyond the Female Athlete Triad to the full web of the affected systems, the 2018 update refined the Clinical Assessment Tool and the severity model, and the 2023 update extended the framework with the contemporary evidence and the male-athlete emphasis. The three statements are the spine of the RED-S framework, and the candidate cites them in sequence. [1] [3]
The Female Athlete Triad framework is anchored by the 2014 Coalition Consensus Statement, which operationalised the three spectra into the Cumulative Risk Assessment and the return-to-play criteria. The comparison study of the Triad Cumulative Risk Assessment and the RED-S Clinical Assessment Tool confirmed that the two tools place the high-risk athlete in the same restricted-from-play category, so the candidate may use either with the confidence that the high-risk decision is consistent. The functional hypothalamic amenorrhoea is anchored by the 2017 Endocrine Society guideline, which frames the energy restoration as the first-line treatment. [4] [11]
The evidence on the energy availability in the adolescent athlete is anchored by the inadvertent undereating study and the Low Energy Availability in Females Questionnaire work, which confirmed that a substantial proportion of the young female athletes fall below the threshold and that many do so without the intentional restriction. The bone stress injury in the young athlete is anchored by the middle-school runner study and the bone stress injury reviews, which established the prevalence, the risk factors, and the high-risk sites. The regional differences are modest but real, and the access to the dietitian, the psychologist, and the dual-energy X-ray absorptiometry varies by the geography and the system, with the rural and the remote athlete facing the longer pathway. The fellowship answer names the guideline without pretending that a single algorithm resolves every judgement call. [8] [9]
Exam Pearls
The fellowship answer turns on five facts. The energy availability is the dietary intake minus the exercise energy expenditure divided by the fat-free mass, and it is disrupted below approximately thirty kilocalories per kilogram of fat-free mass per day and optimal at approximately forty-five. The Female Athlete Triad is the three spectra of the energy, the menstruation, and the bone, and relative energy deficiency in sport is the wider web of the affected systems that applies to the male as much as the female. The treatment is the energy restoration, and the combined oral contraceptive pill is not the first-line treatment for the bone in the energy-deficient athlete. The menstrual cycle is the vital sign of the energy balance, and the absent cycle is the energy deficiency until proven otherwise. And the high-risk athlete is restricted from play until the energy, the cycle, and the bone are restored. [5] [3]
The examiner probes three traps. The first is the athlete with the absent cycle who is dismissed as normal for a sportswoman — the functional hypothalamic amenorrhoea is missed, and the bone is dismantled, and the energy restoration is delayed. The second is the athlete with the stress fracture who is treated as the purely mechanical injury — the underlying low bone density is not assessed, and the energy deficit is missed. The third is the amenorrhoeic athlete who is prescribed the oral contraceptive pill for the bone — the pill masks the menstrual signal and does not restore the bone, and the energy restoration that is the actual treatment is delayed. The candidate who names these three traps demonstrates the depth the fellowship demands. [6] [4]
The examiner rewards the candidate who frames the athlete assessment as a clinical reasoning exercise, not a list. The energy availability is quantified, the three Triad spectra are assessed, the wider RED-S web is held, the risk is stratified, the energy is restored, the team is engaged, and the return to play is cleared by the criteria. A candidate who shows this breadth and this safety demonstrates the systems thinking that the fellowship demands, and the recognition that the energy deficit in the growing athlete is the preventable harm that the early screen and the prompt restoration avert. [1] [11]
References
- [1]Mountjoy M, Sundgot-Borgen J, Burke L, Carter S, Constantini N, Lebrun C, et al. The IOC consensus statement: beyond the Female Athlete Triad—Relative Energy Deficiency in Sport (RED-S). Br J Sports Med, 2014.PMID 24620037
- [2]Mountjoy M, Sundgot-Borgen JK, Burke LM, Ackerman KE, Blauwet C, Constantini N, et al. International Olympic Committee (IOC) Consensus Statement on Relative Energy Deficiency in Sport (RED-S): 2018 Update. Int J Sport Nutr Exerc Metab, 2018.PMID 29771168
- [3]Mountjoy M, Ackerman KE, Bailey DM, Burke LM, Constantini N, Hackney AC, et al. 2023 International Olympic Committee's (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs). Br J Sports Med, 2023.PMID 37752011
- [4]De Souza MJ, Nattiv A, Joy E, Misra M, Williams NI, Mallinson RJ, et al. 2014 Female Athlete Triad Coalition Consensus Statement on Treatment and Return to Play of the Female Athlete Triad. Curr Sports Med Rep, 2014.PMID 25014387
- [5]Loucks AB, Thuma JR. Luteinizing hormone pulsatility is disrupted at a threshold of energy availability in regularly menstruating women. J Clin Endocrinol Metab, 2003.PMID 12519869
- [6]Gordon CM, Ackerman KE, Berga SL, Kaplan JR, Mastorakos G, Misra M, et al. Functional Hypothalamic Amenorrhea: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab, 2017.PMID 28368518
- [7]Fahrenholtz IL, Melin AK, Wasserfurth P, Stenqvist TB, Garthe I, Areta JL, et al. Risk of Low Energy Availability, Disordered Eating, Exercise Addiction, and Food Intolerances in Female Endurance Athletes. Front Sports Act Living, 2022.PMID 35592590
- [8]Barrack MT, Domino S, Gray VB, Winkelmann ZK, Hunnicutt JN, VanLoan MD. Support for inadvertent undereating in female adolescent athletes with clinical indicators of low energy availability. J Sci Med Sport, 2023.PMID 37248163
- [9]Tenforde AS, DeLuca S, Wu AC, Jepsen C, Chatterjee A, STARS Study Collaborators, et al. Prevalence and factors associated with bone stress injury in middle school runners. PM R, 2022.PMID 34251763
- [10]Tenforde AS, Kraus E, Fredericson M. Bone Stress Injuries in Runners. Phys Med Rehabil Clin N Am, 2016.PMID 26616181
- [11]Holtzman B, Tenforde AS, Parziale AL, Mitevska I, Sainani KL, Fredericson M. Characterization of Risk Quantification Differences Using Female Athlete Triad Cumulative Risk Assessment and Relative Energy Deficiency in Sport Clinical Assessment Tool. Int J Sport Nutr Exerc Metab, 2019.PMID 31034246