Paeds · rheumatology-musculoskeletal-and-sports
Slipped capital femoral epiphysis
Also known as slipped upper femoral epiphysis · SCFE · SUFE · adolescent coxa vara · epiphysiolysis capitis femoris · Drehmann sign
A fellowship approach to the overweight adolescent with an antalgic gait and referred knee pain: the Loder stability classification that separates stable from unstable slipped capital femoral epiphysis and predicts the risk of avascular necrosis, the Southwick angle that grades slip severity on the frog-lateral radiograph, Klein's line that reveals the subtle slip on the AP view, the single-screw in-situ pinning that is the gold standard for stable slips, the urgent reduction strategy for the unstable slip, and the endocrine work-up that the atypical age-weight presentation demands.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A thirteen-year-old boy with a body mass index above the ninety-fifth percentile presents to the emergency department with three weeks of left knee pain and a limp that has worsened over two days to the point where he cannot put any weight on the leg. Or a twelve-year-old girl is brought to the general practitioner with a six-month history of an intermittent aching hip that she has attributed to growing pains, with a recent acute worsening that now stops her walking. Or an eight-year-old boy with known hypothyroidism and a short stature develops a limp and an externally rotated leg. In each, the question is the same — is this a slipped capital femoral epiphysis, is it stable or unstable, and how urgently does the physis need stabilising? [1] [3]
The six moves — Classify, Confirm, Crane, Crack, Cage, Companion
Overview & Definition
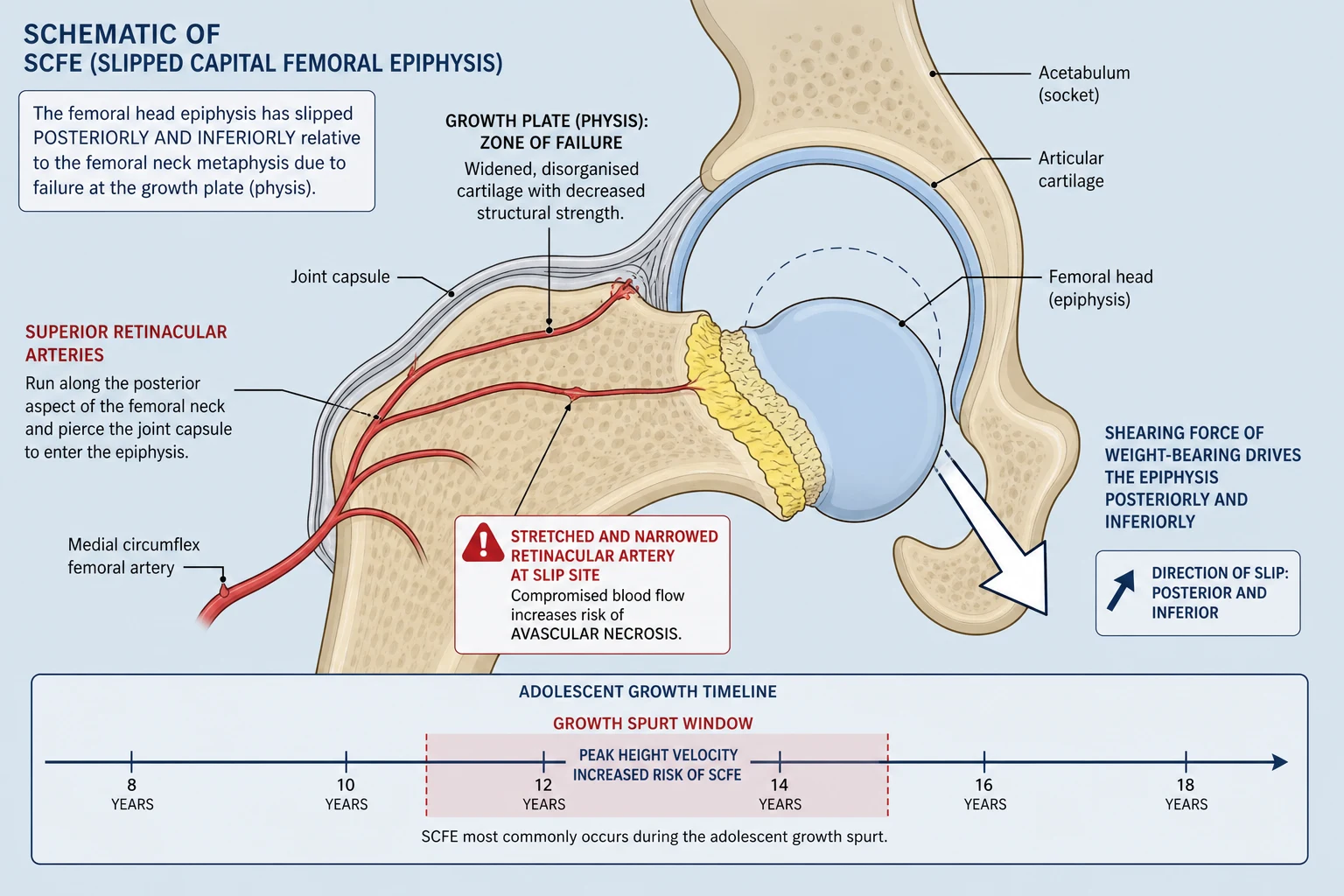
Slipped capital femoral epiphysis is the displacement of the capital femoral epiphysis — the growing head of the femur — relative to the metaphysis of the femoral neck, occurring through the physis during the period of adolescent skeletal immaturity. The epiphysis slips posteroinferiorly while the metaphysis rotates anteriorly and superiorly, producing the characteristic external rotation deformity and the loss of internal rotation that the examiner detects at the bedside. It is the commonest hip disorder of adolescence, and its importance lies in the twin threats of progressive slip with weight-bearing and of avascular necrosis of the femoral head, both of which can produce a permanent, crippling deformity if the diagnosis is delayed. [7] [4]
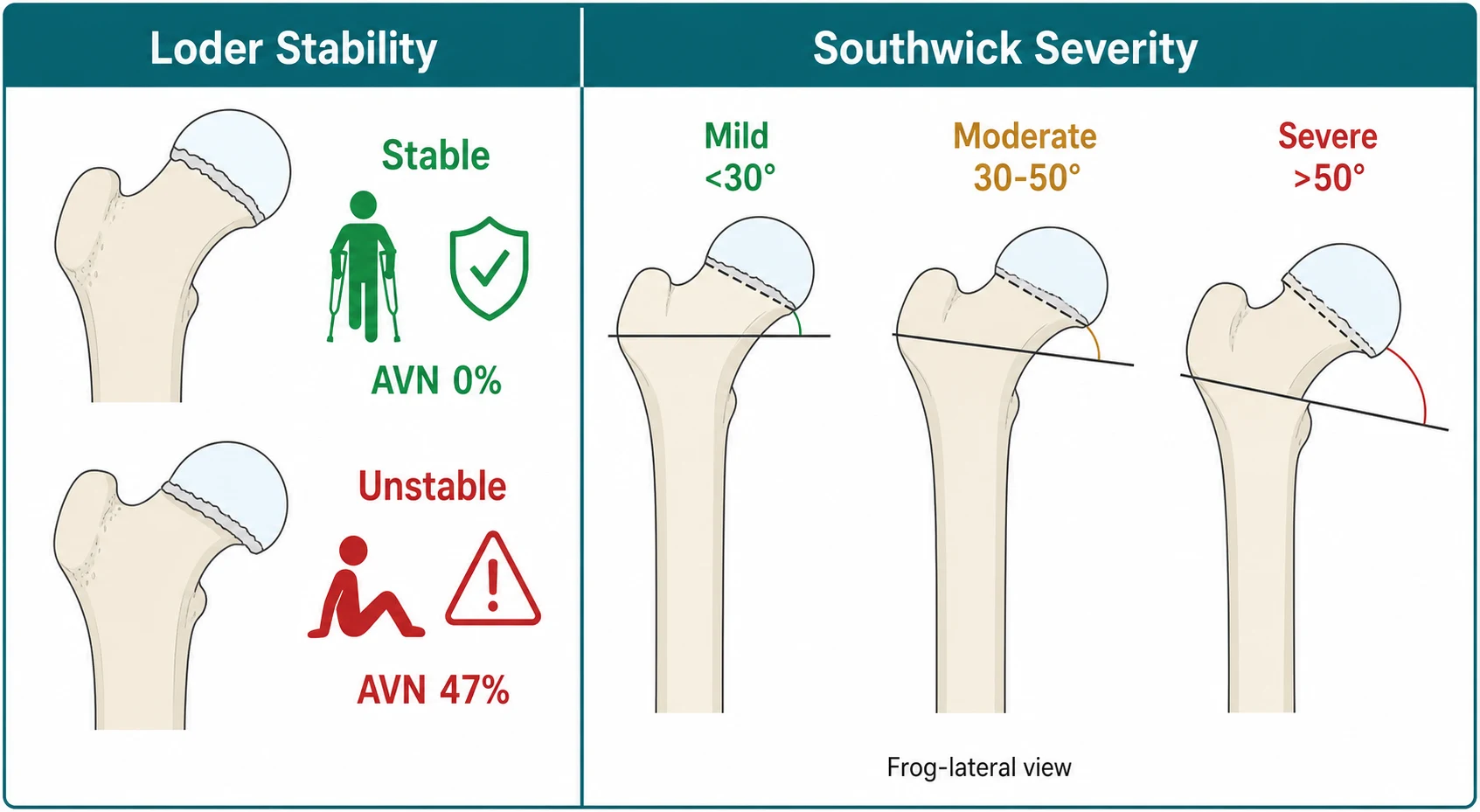
The fellowship framing rests on a single clinical decision that the Loder stability classification makes explicit. A slip is stable when the child can bear weight, even with crutches, and unstable when the child cannot bear weight at all, and this single distinction predicts the risk of avascular necrosis — approximately zero per cent in the stable slip and approaching fifty per cent in the unstable slip. This is why the stability classification drives the urgency: the stable slip is fixed electively, and the unstable slip is an orthopaedic emergency that goes to theatre for urgent reduction and fixation. [1] [6]
The clinical importance comes from what happens if the slip is missed or the unstable slip is left. Progressive displacement under weight-bearing worsens the deformity and increases the risk of avascular necrosis, chondrolysis, femoroacetabular impingement from the residual cam lesion, and early osteoarthritis. In the atypical child — the one who is younger than ten or older than sixteen, or whose weight is below the fiftieth percentile — the slip is the first clue to an underlying endocrinopathy, renal osteodystrophy, or chromosomal syndrome, and the work-up extends beyond the hip. [3] [7]
Classification
Classification of the slipped capital femoral epiphysis rests on two axes that together drive the management — the stability of the physis, which the Loder classification captures and which predicts avascular necrosis, and the severity of the slip, which the Southwick angle measures on the frog-lateral radiograph and which guides the surgical strategy. The Loder stability classification was derived in 1993 from a study of seventy-two children with acute slips, and it remains the single most important prognostic framework because it separates the emergency from the elective and predicts the complication that defines the outcome. [1]
The Loder stability classification defines a slip as stable when the child is able to ambulate with or without crutches, and unstable when the child is unable to bear weight even with crutches. The predicted risk of avascular necrosis follows the stability directly — Loder reported zero per cent avascular necrosis in the stable group and forty-seven per cent in the unstable group, a finding that has been reproduced across cohorts and meta-analyses and that frames the unstable slip as the orthopaedic emergency. The unstable child is kept strictly non-weight-bearing, given adequate analgesia, and taken to theatre for urgent reduction and fixation. [1] [10]
The severity is graded by the Southwick angle, measured on the frog-lateral radiograph as the angle between the axis of the femoral shaft and a line perpendicular to the base of the epiphysis. A mild slip has a Southwick angle below thirty degrees, a moderate slip between thirty and fifty degrees, and a severe slip above fifty degrees. The severity guides the surgical choice — single-screw in-situ pinning is the standard for stable mild and moderate slips, while severe slips and unstable slips may require reduction, realignment, or the modified Dunn surgical dislocation, depending on the surgeon and the centre. [2] [7]
Epidemiology & Risk Factors
Slipped capital femoral epiphysis is the commonest hip disorder of adolescence, with an incidence of roughly ten per hundred thousand children per year in normal-weight populations, rising steeply with the obesity epidemic to over fifty per hundred thousand in the most overweight groups. The peak age is between ten and sixteen years, coinciding with the rapid growth spurt of puberty when the physis is widest, most vulnerable, and most exposed to shearing forces. Boys are affected roughly one and a half times as often as girls, the left hip more than the right, and between twenty and forty per cent of children have bilateral involvement at presentation or go on to develop a contralateral slip during growth. [4] [9]
The risk factors that matter for the fellowship answer are those of mechanical overload and of physeal weakness. Obesity is the single strongest risk factor — a body mass index above the eighty-fifth percentile is present in the majority of affected children, and the mechanical load across a vertically oriented and histologically weak physis produces the shearing failure. The adolescent growth spurt itself is a risk factor, because the physis widens and remodels during peak height velocity and becomes structurally vulnerable for the two to three years before closure. African-American and Polynesian populations carry a higher incidence, and the seasonal peak in the late summer and autumn reflects the period of greatest physical activity. [4] [5]
The atypical risk factors are those that weaken the physis biochemically rather than mechanically, and they define the subgroup that demands an endocrine and renal work-up. Endocrinopathies — particularly hypothyroidism, growth hormone deficiency, hypogonadism, and panhypopituitarism — produce a histologically abnormal physis that slips at a lower mechanical load. Renal osteodystrophy from chronic kidney disease, and prior radiation therapy to the pelvis, produce the same vulnerability. The Loder age-weight test identifies these children: an age below ten or above sixteen years, or a weight below the fiftieth percentile, flags the atypical slip that is not idiopathic and that needs the investigation. [3] [8]
Pathophysiology
The pathophysiology begins with the mechanical and biochemical weakening of the capital femoral physis during the adolescent growth spurt. The physis is a cartilaginous plate that separates the epiphysis — the femoral head and its secondary ossification centre — from the metaphysis of the femoral neck, and it is the weakest point of the growing skeleton because its matrix is less able to resist shear than the bone above and below it. During the rapid growth of puberty, the physis widens, its columnar architecture becomes disorganised, and the perichondrial ring that braces its perimeter thins and loses mechanical competence, so the shearing force of weight-bearing across the obliquely oriented proximal femoral physis produces a gradual or sudden failure. [7]
The slip occurs through the hypertrophic zone of the physis, the layer that is weakest because the chondrocytes are enlarged and the matrix between them is sparse. The epiphysis remains in the acetabulum while the metaphysis rotates anteriorly and superiorly, carrying the femoral neck and the diaphysis with it, so the epiphysis appears to slip posteriorly and inferiorly relative to the neck. The result is that the weight-bearing axis shifts from the centre of the femoral head to the posterior and inferior margin of the epiphysis, the lever arm lengthens, and the mechanical disadvantage worsens with every degree of additional slip — a positive feedback that explains the tendency to progressive displacement under load. [7] [2]
The relevance to avascular necrosis lies in the blood supply to the epiphysis and the retinacular vessels that traverse the physis. The capital femoral epiphysis receives its blood supply predominantly from the medial circumflex femoral artery, whose deep branch gives rise to the superior retinacular vessels that run along the posterior aspect of the femoral neck, pierce the capsule, and enter the epiphysis at its superolateral margin. When the slip displaces the epiphysis, or when it is manipulated roughly, these retinacular vessels are stretched, kinked, or torn, and the blood supply to the femoral head is compromised. This is the anatomical basis for the high avascular necrosis rate in the unstable slip and for the cardinal surgical rule against forceful reduction. [1] [10]
The histological abnormality in the atypical slip extends the mechanism beyond the mechanical. In the endocrine, renal, and post-radiation physis, the cartilage matrix is biochemically disordered — widened, irregular, and structurally incompetent — so the slip occurs at a normal or low mechanical load and may present in a younger, lighter, or systemically unwell child. This is why the atypical age-weight presentation demands the endocrine and renal work-up: the slip is the local manifestation of a systemic disease that weakens every physis in the growing skeleton. [3] [8]
Clinical Presentation
The presentation is the overweight adolescent who limps. The onset is usually insidious, with weeks to months of a dull aching pain in the groin, the thigh, or — most commonly and most dangerously — the knee, and an antalgic gait that the child and the family attribute to a sports injury or growing pains. The pain is mechanical, worsening with activity and weight-bearing and easing with rest, and the child may describe a click or a giving-way sensation in the hip. The acute or acute-on-chronic presentation is the unstable slip — a sudden worsening over hours to days that stops the child walking — and it is the presentation that carries the avascular necrosis risk and demands the emergency pathway. [4] [7]
The examination reveals the external rotation deformity and the loss of internal rotation, which are the signature signs of the slipped epiphysis. The affected leg is held in external rotation, it appears slightly short, and the gait is antalgic with a shortened stance phase on the affected side. Passive flexion of the hip produces obligatory external rotation — the Drehmann sign — because the slipped epiphysis impinges on the anterior acetabular rim as the hip flexes, and the leg rotates outward to accommodate. Internal rotation is lost and is painful at the limit, and abduction and flexion are restricted in proportion to the severity of the slip. [7]
Which reassuring-sounding stories must never close the search for the slip? An adolescent who reports only knee pain is not a musculoskeletal strain — the hip refers to the knee through the obturator nerve, and the child with knee pain and a limp must have the hip examined and imaged or the slip is missed. A child who attributes the limp to a recent sports injury is not necessarily wrong, but the injury is the precipitant of a slip that was already developing, and the physis must be assessed radiographically. And a child with a chronic aching hip labelled as growing pains is the classic delayed presentation — growing pains do not cause a limp, do not localise to a single joint, and do not produce an external rotation deformity, so any of these features warrants the frog-lateral radiograph. [4] [5]
Differential Diagnosis
The differential diagnosis of the limping adolescent is broad, and the fellowship skill is to separate the slipped capital femoral epiphysis from its mimics using the age, the body habitus, the stability, and the frog-lateral radiograph. A transient synovitis or an irritable hip is the commonest mimic in the younger child, but it is rare in the overweight adolescent, it resolves within a week or two, and the radiographs are normal. A septic arthritis of the hip is the must-not-miss in the febrile child with a held hip, and the Kocher criteria, the inflammatory markers, and the ultrasound-guided aspiration separate it from the afebrile slip. [7]
A Perthes disease — idiopathic avascular necrosis of the capital femoral epiphysis in the young school-age child — enters the differential when the limp is chronic and the hip is stiff, but it peaks between four and eight years, well below the slipped capital femoral epiphysis age range, and the radiographs show the characteristic fragmentation and collapse of the epiphysis rather than the slip. An avulsion fracture of the apophyses around the hip — the anterior inferior iliac spine from the rectus femoris, or the ischial tuberosity from the hamstrings — presents with acute pain after a sprinting injury in the athletic adolescent, and the radiographs show the displaced apophysis rather than the epiphyseal slip. [7] [4]
For the child presenting primarily with knee pain, the differential includes an Osgood-Schlatter lesion or a Sinding-Larsen-Johansson lesion at the knee extensor mechanism, a tibial spine avulsion, a stress fracture of the tibia or the femur, and a meniscal or ligamentous injury. The discipline is that any adolescent with knee pain and a limp or an external rotation deformity has the hip imaged before the knee is investigated, because the slipped capital femoral epiphysis hiding behind the referred knee pain is the diagnosis that the missed imaging allows to worsen. A stress fracture of the femoral neck and an early osteoid osteoma of the proximal femur complete the bone differential, and each is resolved by the frog-lateral and the AP radiographs. [7] [5]
Clinical & Bedside Assessment
The recognition move is to treat every overweight adolescent with a limp, knee pain, or an external rotation deformity as a slipped capital femoral epiphysis until proven otherwise, and to perform a focused hip and gait examination before any radiograph. The history must establish the onset and the pace of the pain, the site — groin, thigh, or knee — the ability to bear weight, the recent growth and weight trajectory, any endocrine or renal history, and the pubertal stage. The stability of the slip is a clinical determination made at the bedside, and it is the question that drives the urgency: can this child bear weight, even with crutches? [1] [7]
The bedside examination must look, feel, move, and measure the hip and the gait. Look at the gait — the antalgic limp with the shortened stance phase, and the externally rotated leg that swings outward. Look at the posture — the leg held in external rotation and slight flexion, the position of greatest capsular laxity and least pain. Feel for warmth and effusion, which are absent in the slip and present in the septic joint, and palpate the knee, the thigh, and the groin for local tenderness. Move the hip, assessing internal rotation first — the movement that is lost earliest and most reliably — and watching for the obligatory external rotation of the Drehmann sign as the hip flexes. Compare both sides, because the subtle loss of internal rotation on the affected hip is detected only against the normal side. [7] [4]
Which examination findings must never be dismissed? A child who cannot bear weight even with crutches has an unstable slip until proven otherwise, and the avascular necrosis risk demands the emergency pathway. A child with a Drehmann sign — the leg that obligatorily externally rotates as the hip flexes — has a slipped epiphysis until proven otherwise, because the sign is produced by the anterior impingement of the slipped epiphysis on the acetabular rim. And a child who is younger than ten or older than sixteen, or whose weight is below the fiftieth percentile, has an atypical slip that demands the endocrine and renal work-up alongside the radiograph. [1] [3]
Investigations
The radiograph is the single most important investigation, and it must include both the AP pelvis and the frog-lateral view of both hips, because the slip is a posterior displacement that is invisible or subtle on the AP and obvious on the frog-lateral. The frog-lateral view shows the epiphysis displaced posteroinferiorly relative to the metaphysis, the widened and irregular physis, and the Southwick angle that grades the severity. The early or mild slip may show only a physeal widening or irregularity — the preslip — and it is the view that distinguishes the true slip from the normal hip, so the frog-lateral is never omitted. [2] [7]
The Klein's line is the sign that catches the subtle slip on the AP pelvis. A line drawn along the superior cortex of the femoral neck, extended proximally, normally intersects a segment of the capital femoral epiphysis. In the slipped capital femoral epiphysis, the line passes above the epiphysis and misses it — the Trethowan sign — because the epiphysis has slipped posteriorly out of the plane of the line. The metaphyseal blanch sign, or Steel's sign, is the area of increased density at the metaphysis where the posteriorly displaced epiphysis overlaps it, and it is a useful confirmatory sign on the AP view. [7]
The blood tests do not confirm the slip but they frame the atypical presentation and the surgical fitness. A full blood count and inflammatory markers exclude the septic joint, and a renal and bone profile, a thyroid function test, and a growth hormone and sex hormone panel are requested when the age-weight test flags the atypical child. The endocrine work-up is not urgent in the typical overweight adolescent with a normal age, but it is essential in the atypical presentation, and the bilateral slip in a young or thin child is the classic clue to a systemic endocrinopathy. Magnetic resonance imaging is reserved for the child with a normal radiograph and a high clinical suspicion, where it reveals the physeal oedema and the preslip, and for the assessment of avascular necrosis after the unstable slip. [3] [8]
Management — Resuscitation
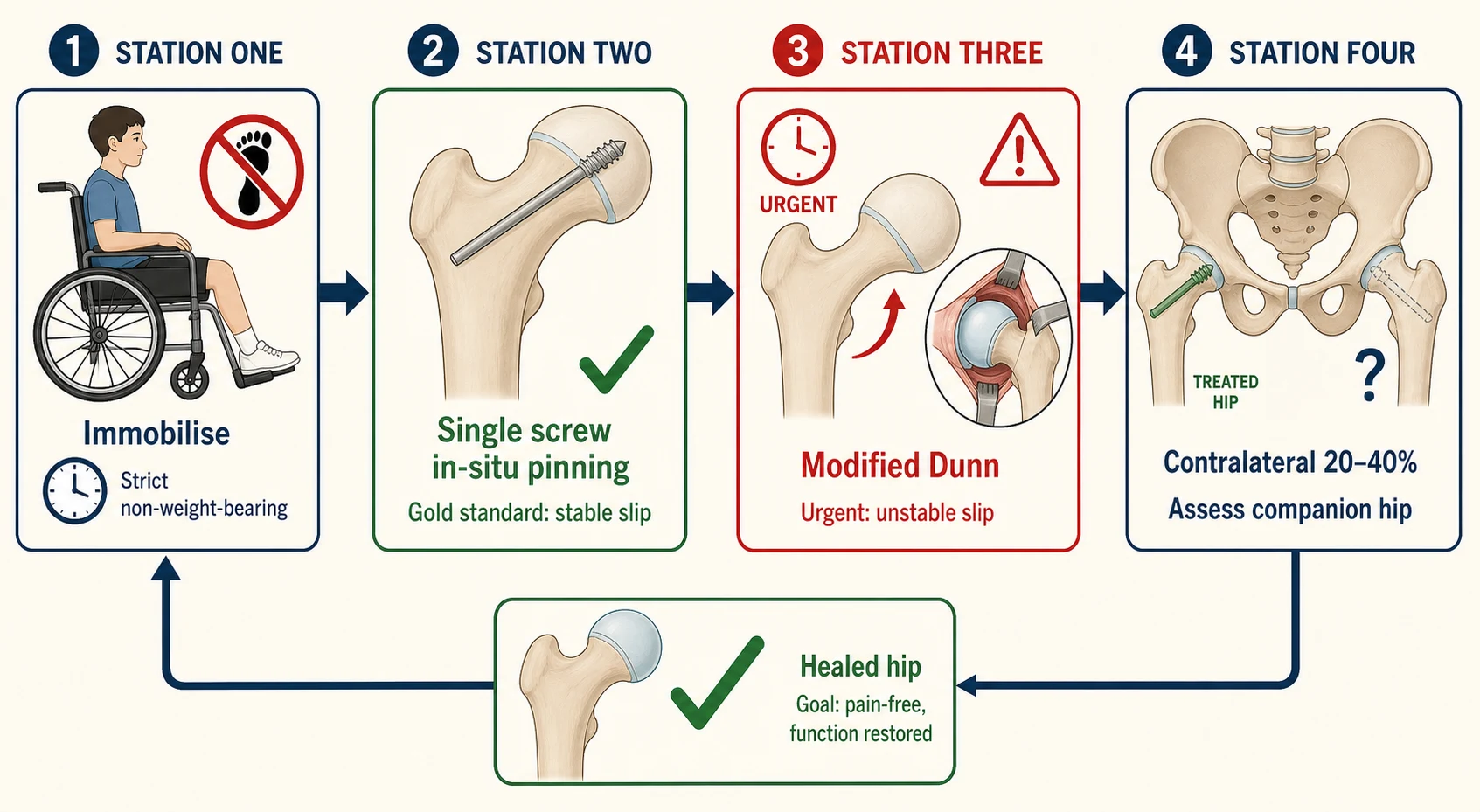
Resuscitation in the slipped capital femoral epiphysis is the discipline of making the child safe for surgery, and its core is strict non-weight-bearing and adequate analgesia. The child is transported by wheelchair or stretcher, never allowed to walk, and the affected leg is supported in a comfortable position of slight flexion and external rotation. Intravenous analgesia — morphine or a regional block — is given for the acute or unstable slip, because the pain of the acute displacement is severe and because the child who is in pain cannot cooperate with the examination and the imaging. [1] [7]
The stability is determined at the bedside and it sets the urgency. The stable slip is admitted and fixed on the next available operating list, with the child kept non-weight-bearing and adequately analgesed in the interim. The unstable slip is the orthopaedic emergency — the child is kept strictly non-weight-bearing, given intravenous analgesia, and taken to theatre for urgent reduction and fixation, because the avascular necrosis risk rises with every hour of delay and the window for the gentle reduction that protects the retinacular vessels narrows rapidly. [1] [10]
The pre-operative preparation is brief and focused. The child is fasted, the bloods are drawn for the group and save and the atypical work-up if indicated, and the consent is obtained for the in-situ fixation or the reduction and fixation. The surgical team is informed, the theatre is arranged, and the anaesthetic review is completed. The child with the unstable slip is prioritised on the emergency list, and the transfer to a centre with paediatric orthopaedic capability is arranged if the local service cannot provide the urgent fixation. [7] [5]
Management — Definitive & Stepwise
The definitive management is the surgical stabilisation of the physis, and the gold standard for the stable slip is single-screw in-situ pinning. A single cannulated screw is placed percutaneously across the physis from the anterolateral femoral neck into the centre of the epiphysis, perpendicular to the physis, engaging the epiphysis without breaching the joint, and the screw stabilises the slip in its current position without attempting a reduction. The rationale is that the stable slip does not need reduction — the deformity is accepted and the physis is fused to prevent further displacement — and that the manipulation required to reduce a chronic slip risks the retinacular vessels and the avascular necrosis that the surgery is meant to prevent. [7] [2]
The unstable slip is managed more urgently and more controversially. The child is taken to theatre for urgent gentle reduction and single-screw fixation, with the reduction achieved by gentle traction and internal rotation under anaesthesia — never by forceful manipulation — and the screw placed to stabilise the reduced or accepted position. The modified Dunn procedure, a surgical hip dislocation with a subcapital osteotomy and capital realignment, offers the restoration of the normal anatomy and the direct visualisation and protection of the retinacular vessels, and it is used in centres with the expertise for the severe and the unstable slip, though it carries its own learning curve and complication profile. The choice between the gentle reduction and pinning and the modified Dunn depends on the severity, the stability, the timing, and the surgeon, and the fellowship answer names both and frames the controversy. [7] [10]
The prophylactic pinning of the contralateral hip is the debated question that the examiner probes. Between twenty and forty per cent of children develop a contralateral slip, and the risk is higher in the younger child with an open triradiate cartilage, in the thin or endocrine child, and in the child who presents at the younger end of the age range. Some centres pin the contralateral hip prophylactically at the index operation in the high-risk child, while others monitor with serial radiographs every three to six months until physeal closure, and the decision is individualised on the risk profile. The child and the family are counselled on the risk and the monitoring, and the contralateral hip is assessed at every follow-up visit. [6] [9]
Specific Subtypes & Scenarios
The unstable slip is the subtype that defines the orthopaedic emergency. The child presents with an acute or acute-on-chronic worsening and cannot bear weight even with crutches, and the physis is unstable and at risk of further displacement and of avascular necrosis. The Loder 1993 study established the forty-seven per cent avascular necrosis rate in this group, and the modern systematic reviews confirm that the unstable slip carries the bulk of the disease burden. The management is urgent — strict non-weight-bearing, intravenous analgesia, and theatre for the gentle reduction and fixation or the modified Dunn, because the window for protecting the retinacular vessels is narrow. [1] [10]
The atypical slip is the subtype that demands the endocrine and renal work-up. The Loder age-weight test identifies the child who is younger than ten or older than sixteen, or whose weight is below the fiftieth percentile, as atypical rather than idiopathic, and these children have a higher prevalence of endocrine, renal, and chromosomal disease. Hypothyroidism is the commonest endocrine association, followed by growth hormone deficiency, hypogonadism, and panhypopituitarism. The bilateral slip in a young or thin child is the classic clue to a systemic endocrinopathy, and the case of the child with bilateral slips and a nodular neck leading to the diagnosis of multiple endocrine neoplasia illustrates the importance of the work-up. [3] [8]
The valgus slip is the rare subtype that slips anterosuperiorly rather than posteroinferiorly, producing an internal rotation rather than an external rotation deformity, and it is easily missed because the Klein's line and the Southwick angle are calibrated for the posteroinferior pattern. The Loder 2023 demographic study documented the valgus slip as a distinct entity with a different clinical presentation and a different radiographic signature, and it is sought specifically when the external rotation sign is absent and the clinical picture is otherwise consistent. [6]
The bilateral and the sequential slip is the subtype that demands the contralateral vigilance. Between twenty and forty per cent of children have bilateral involvement, and the second slip may develop silently months to years after the first, so the contralateral hip is examined and imaged at presentation and at every follow-up visit until physeal closure. The younger the child at the index slip, the greater the risk of the contralateral slip, because the years of remaining growth offer the window for the second physis to fail. [9] [6]
Complications & Pitfalls
The complications of the slipped capital femoral epiphysis are permanent and crippling when the slip is missed or the unstable slip is left. Avascular necrosis of the femoral head is the feared complication, occurring in approximately zero per cent of stable slips and approaching fifty per cent of unstable slips, and it produces a collapsed, deformed femoral head with pain, stiffness, and a progressive osteoarthritis that often requires a total hip replacement in early adulthood. Chondrolysis — the acute destruction of the articular cartilage — produces a stiff, painful hip with a markedly reduced range, and it may occur after the surgery as well as from the slip itself. [1] [10]
The femoroacetabular impingement is the delayed complication that follows the residual deformity of the moderate or severe slip that was pinned in situ without realignment. The slipped epiphysis produces a cam lesion — a bony prominence on the anterior femoral neck — that impinges on the acetabular labrum during flexion and internal rotation, producing pain, labral tears, and a progressive cartilage damage that accelerates the osteoarthritis. This is the rationale for the modified Dunn procedure in the severe slip: the realignment of the epiphysis restores the normal head-neck offset and reduces the impingement, at the cost of a more complex operation. [7]
The pitfall of the referred knee pain is the commonest and the deadliest diagnostic error. An overweight adolescent presents with knee pain, the knee is examined and investigated, the hip is not imaged, and the slip worsens under weight-bearing until it becomes unstable and avascular necrosis supervenes. The safeguard is the rule that any adolescent with knee pain and a limp or an external rotation deformity has the hip imaged first. The pitfall of the forceful reduction is the iatrogenic disaster — the chronic slip that is manipulated acutely tears the retinacular vessels and produces the avascular necrosis that the surgery was meant to prevent, and the safeguard is the rule that the chronic slip is pinned in situ without reduction. [7] [1]
The pitfall of the missed atypical slip is the child whose endocrine disease is not diagnosed. A young, thin child with a bilateral slip is treated as idiopathic, the endocrinopathy is not sought, the second and the third physis fail, and the systemic disease progresses unrecognised. The safeguard is the Loder age-weight test — every child below ten or above sixteen, or below the fiftieth percentile in weight, has the endocrine and renal work-up. The pitfall of the unmonitored contralateral hip is the silent second slip — the child whose opposite hip is not imaged at the follow-up develops an unstable slip that could have been prevented by the prophylactic pinning or the early detection. [3] [6]
Prognosis & Disposition
The prognosis of the stable slipped capital femoral epiphysis treated with single-screw in-situ pinning is good, with most children returning to full activity within three to six months and the physis fusing uneventfully. The avascular necrosis risk is approximately zero per cent in the stable slip, and the long-term outcome is determined by the residual deformity and the risk of femoroacetabular impingement, which is lower in the mild slip and higher in the moderate and severe. The prognosis of the unstable slip is guarded, with the avascular necrosis risk approaching fifty per cent and the long-term outcome dependent on the degree of the head collapse and the development of the osteoarthritis. [1] [7]
The long-term outlook is shaped by the severity and the stability at presentation. The mild stable slip carries the best prognosis, with a low risk of impingement and a near-normal hip through early adulthood. The moderate and severe slips carry a higher risk of impingement and of the late osteoarthritis, even when the avascular necrosis is avoided, and the realignment procedures aim to reduce this burden. The unstable slip, with or without avascular necrosis, carries the worst prognosis, and the child is followed for years to detect the head collapse and to plan the reconstructive surgery if it develops. [7] [10]
The disposition is shared between the general paediatrician, who owns the recognition and the atypical work-up, the orthopaedic surgeon, who owns the stabilisation and the reduction, and the endocrinologist, who owns the investigation and the management of the atypical disease. The child is admitted for the surgical stabilisation, and the follow-up is shared — the orthopaedic review for the radiographic monitoring and the impingement assessment, the paediatric and endocrine review for the growth and the atypical work-up, and the physiotherapy for the rehabilitation. The family is counselled on the diagnosis, the weight management, the contralateral risk, and the importance of the follow-up until physeal closure. [5] [9]
Special Populations
The atypical child is the population in whom the slip is not idiopathic and the systemic disease must be sought. The Loder age-weight test identifies the child below ten or above sixteen years, or below the fiftieth percentile in weight, as atypical, and the work-up extends to the thyroid function, the growth hormone, the sex hormones, the renal function, and the chromosomal analysis. Hypothyroidism, growth hormone deficiency, hypogonadism, and panhypopituitarism are the endocrine associations, and the bilateral slip in a young or thin child is the classic presentation that prompts the diagnosis. The management of the slip is the same — the physis is stabilised — but the systemic disease is treated alongside, and the endocrinologist is involved early. [3] [8]
The child with renal osteodystrophy from chronic kidney disease is the population in whom the physis is biochemically weakened and the slip may occur at multiple sites and at a young age. The secondary hyperparathyroidism, the disordered mineral metabolism, and the widened, irregular physis produce a high slip risk, and the management combines the surgical stabilisation with the medical optimisation of the bone disease. The child with prior pelvic radiation therapy carries the same vulnerability, and the slip is monitored throughout the remaining growth. [3] [7]
Children in the indigenous and socioeconomically disadvantaged populations of Australia and New Zealand carry a higher burden of obesity and of the delayed presentation, through the same pathways of limited primary care access, delayed imaging, and the late referral that drive other conditions of inequity. The Navarre review of the New Zealand literature documented the presentation patterns and the outcomes across the regions, and the fellowship answer frames the disease as one in which the access to the timely imaging and the orthopaedic fixation shapes the outcome as much as the biology. The weight management, the health literacy, and the culturally safe follow-up are part of the comprehensive care. [5] [9]
The adolescent with a body mass index above the ninety-fifth percentile is the population at the centre of the disease, and the weight management is part of the definitive care. The obesity drives the mechanical overload that produces the slip, it raises the risk of the contralateral slip, and it complicates the surgical and the anaesthetic management. The weight management programme — the dietary intervention, the physical activity, the behavioural support, and the family engagement — is initiated during the admission and continued through the follow-up, because the reduction of the mechanical load is the single most effective secondary prevention. [4] [5]
Evidence, Guidelines & Regional Differences
The Loder 1993 stability classification, derived from a study of seventy-two children with acute slipped capital femoral epiphysis at the Indiana University School of Medicine, is the taught framework for the prediction of avascular necrosis, and its finding of zero per cent in the stable group and forty-seven per cent in the unstable group has been reproduced across the cohorts and the systematic reviews of the subsequent three decades. The 2001 Loder age-weight test extended the classification to the atypical child, defining the age and weight thresholds that prompt the endocrine and renal work-up, and these two papers frame the bedside decision of the stability and the work-up. [1] [3]
The Southwick 1967 osteotomy paper introduced the angle that grades the slip severity on the frog-lateral view, and it remains the taught measurement for the mild, moderate, and severe classification that guides the surgical strategy. The modern comprehensive review by Dussa synthesised the pathomechanism, the clinical presentation, the diagnosis, the natural history, and the treatment of the slipped capital femoral epiphysis, framing the in-situ pinning as the standard and the modified Dunn as the realignment option for the severe and the unstable slip. The 2025 systematic review by Xu and colleagues quantified the risk factors for the avascular necrosis following the unstable slip, confirming the stability, the timing, and the reduction technique as the dominant predictors. [2] [7] [10]
The regional differences are modest in the framework but real in the epidemiology and the access. The Loder stability classification and the in-situ pinning apply globally, but the incidence of the slipped capital femoral epiphysis tracks the obesity epidemic, and it is higher in the populations and the regions with the greatest overweight burden. The Navarre review of the New Zealand literature documented the presentation patterns and the outcomes across the regions, and the Herngren population-based Swedish study quantified the incidence and the bilateral risk in a universal-access system. The access to the timely imaging and the orthopaedic fixation shapes the outcome, and the resource-limited experience offers the pragmatic pathway of the non-weight-bearing, the early frog-lateral, and the referral to the centre with the fixation capability. [5] [9]
Exam Pearls
The fellowship answer turns on five numbers. The Loder stability classification separates the stable slip, with an avascular necrosis risk of approximately zero per cent, from the unstable slip, with a risk approaching fifty per cent. The Southwick angle grades the severity into mild below thirty degrees, moderate between thirty and fifty, and severe above fifty, on the frog-lateral view. The peak age is between ten and sixteen years, and the bilateral risk is between twenty and forty per cent. The gold standard for the stable slip is single-screw in-situ pinning, and the atypical child — below ten or above sixteen, or below the fiftieth percentile in weight — has the endocrine work-up. [1] [2]
The examiner probes three traps. The first is the referred knee pain — the overweight adolescent with knee pain and a limp has the hip imaged first, because the obturator nerve refers the hip pain to the knee and the missed slip worsens with weight-bearing. The second is the forceful reduction — the chronic slip is pinned in situ without manipulation, because the rough reduction tears the retinacular vessels and produces the avascular necrosis that the surgery was meant to prevent. The third is the atypical age-weight presentation — the young, thin, or bilateral slip has the endocrine and renal work-up, because the slip may be the first clue to the hypothyroidism, the growth hormone deficiency, or the pituitary lesion. [4] [3]
The examiner rewards the candidate who frames the disease around the stability and the weight-bearing. The stable slip is fixed electively with the in-situ pinning, the unstable slip is the emergency with the urgent reduction and fixation, and the child is non-weight-bearing from the moment of diagnosis until the physis is stabilised. The contralateral hip is assessed at every visit, the atypical child has the endocrine work-up, and the weight management is part of the definitive care. A candidate who shows this awareness demonstrates the systems thinking and the safety culture that the fellowship demands. [7] [9]
The Loder stability classification — the single prognostic split
References
- [1]Loder RT, Richards BS, Shapiro PS, Reznick LR. Acute slipped capital femoral epiphysis: the importance of physeal stability. J Bone Joint Surg Am, 1993.PMID 8354671
- [2]Southwick WO. Osteotomy through the lesser trochanter for slipped capital femoral epiphysis. J Bone Joint Surg Am, 1967.PMID 6029256
- [3]Loder RT, Greenfield ML. Clinical characteristics of children with atypical and idiopathic slipped capital femoral epiphysis: description of the age-weight test and implications for further diagnostic investigation. J Pediatr Orthop, 2001.PMID 11433161
- [4]Loder RT, Skopelja EN. The epidemiology and demographics of slipped capital femoral epiphysis. ISRN Orthop, 2011.PMID 24977061
- [5]Navarre P. Slipped Capital Femoral Epiphysis: A Review of the New Zealand Literature. J Bone Joint Surg Am, 2020.PMID 32453109
- [6]Loder RT, Gunderson Z, Sun S. Idiopathic Slipped Capital Femoral Epiphysis: Demographic Differences and Similarities between Stable, Unstable, and Valgus Types. Children (Basel), 2023.PMID 37761517
- [7]Dussa CU. Slipped capital femoral epiphysis: pathomechanism, clinical presentation, diagnosis, natural history and treatment. A review of the literature. Orthopadie (Heidelb), 2026.PMID 41951777
- [8]Gladstein AZ, van Dijck S, Wasserman JD, Howard A. Painful Hips and a Nodular Neck: Bilateral Slipped Capital Femoral Epiphysis Leading to the Diagnosis of Multiple Endocrine Neoplasia: A Case Report. JBJS Case Connect, 2015.PMID 29252812
- [9]Herngren B, Stenmarker M, Vavruch L, Hagglund G. Slipped capital femoral epiphysis: a population-based study. BMC Musculoskelet Disord, 2017.PMID 28720145
- [10]Xu Z, Zhu L, Kong L, Qian Y. Risk factors associated with avascular necrosis following unstable slipped capital femoral epiphysis in pediatric patients: A systematic review and meta-analysis. PLoS One, 2025.PMID 40737348