Paeds · rheumatology-musculoskeletal-and-sports
Sports injury prevention and overuse injuries
Also known as overuse injury · microtrauma injury · traction apophysitis · Osgood-Schlatter disease · Sever disease · calcaneal apophysitis · Sinding-Larsen-Johansson syndrome · little league elbow · medial epicondyle apophysitis · physeal stress injury · bone stress injury · stress fracture · sport specialization injury · relative energy deficiency in sport · load management
A fellowship approach to the overuse, or microtrauma, injuries of the young athlete — anchored by the acute-versus-overuse distinction, the vulnerability of the open physis and traction apophysis to repetitive load, the traction apophysitides (Sever, Osgood-Schlatter, Sinding-Larsen-Johansson, medial epicondyle), the injury-risk triad of sport specialization, training volume and inadequate recovery, the load-management principle of relative rest with a graded return to play, the neuromuscular warm-up prevention programmes, and the red-flag screen for the bone stress injury or stress fracture that points to relative energy deficiency in sport.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A thirteen-year-old boy who plays basketball for three teams presents with six weeks of knee pain that comes on with jumping and eases with rest — Osgood-Schlatter disease, the traction apophysitis at the tibial tubercle, in a child whose twenty training hours a week exceed his age. An eleven-year-old runner has a month of bilateral heel pain reproduced by squeezing the calcaneus — Sever disease, the traction apophysitis at the calcaneal apophysis, in the prepubertal jumper. A fifteen-year-old distance runner has three months of shin pain that now wakes her at night, with weight loss and lost periods — a tibial stress fracture driven by relative energy deficiency in sport, the case that load management alone will not fix. The task in each is to read the load, to name the failing tissue, and to separate the apophysitis that resolves with growth from the stress fracture that demands imaging and referral. [7] [2]
The three questions of every overuse injury
Overview & Definition
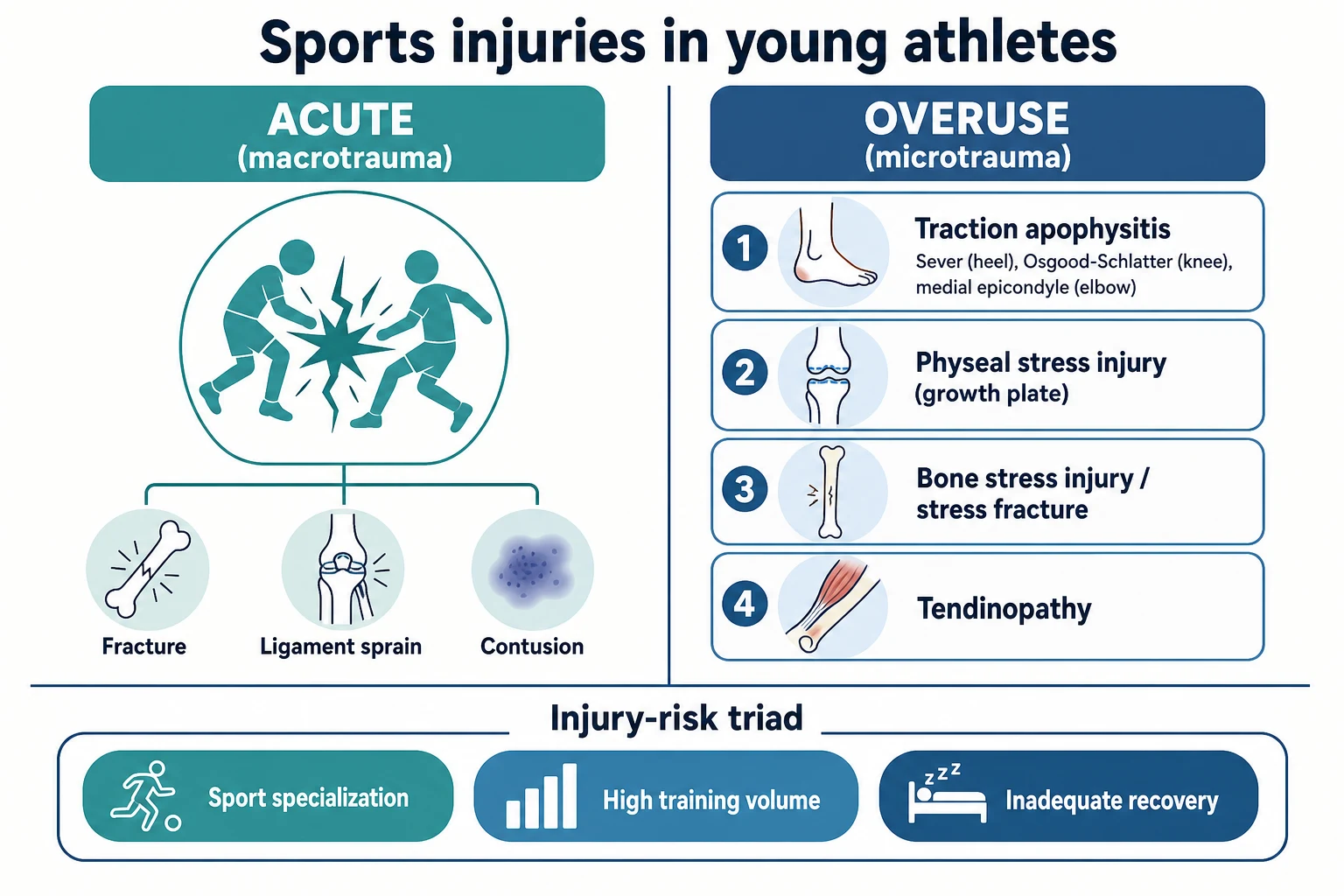
Overuse injuries are the injuries of repetition. They are the cumulative damage that builds when a tissue is loaded more often, or more intensely, than it can repair between sessions, and they stand in contrast to the acute injuries that come from a single high-energy event such as a collision, a twist, or a fall. In an adult, the tissue that gives way under repetition is usually the tendon, the bone, or the joint surface. In a child or an adolescent, the tissue that gives way first is the growing skeleton — the open physis and the traction apophysis — because cartilage is weaker than the tendon that pulls on it, and the growing bone has not yet reached its adult density. [2]
The clinical importance of this distinction is that the overuse injury is, in large part, preventable. An acute ligament tear is hard to prevent because it depends on a chance event, but an overuse injury depends on a load that the clinician, the family, and the coach can change. The fellowship task is therefore two-handed: recognise the overuse pattern and manage it with load modification, and, more broadly, prevent it through the specialization, volume, and recovery choices that the American Academy of Pediatrics and the American Medical Society for Sports Medicine have set out. [1] [2]
The terms matter because they point to the tissue. A traction apophysitis is inflammation at a growth-centre where a tendon pulls, and the common examples are Sever disease at the calcaneus, Osgood-Schlatter disease at the tibial tubercle, Sinding-Larsen-Johansson syndrome at the lower pole of the patella, and medial epicondyle apophysitis at the elbow. A physeal stress injury is repetitive microdamage across an open growth plate. A bone stress injury is the spectrum from bone stress reaction to a frank stress fracture, where repetitive impact outruns the bone's remodelling. A tendinopathy is overload of a tendon itself, and it is less common in children than in adults precisely because the apophysis and the physis yield first. [2] [8]
Classification
The first classification fork is the one the whole topic turns on: acute versus overuse. Acute injuries are the macrotrauma of a single high-energy event — a fracture, a ligament sprain, a contusion. Overuse injuries are the microtrauma of repetition, where many submaximal loads summate into damage that exceeds the tissue's repair capacity. The fork decides the history you take, because the acute injury is dated to an event and the overuse injury is dated to a rising training load. [2] [8]
Within the overuse group, the second classifier is the tissue that fails first in the growing skeleton, because the immature physis and the traction apophysis are the weak link and they fail before the adult tissue around them. The traction apophysitides sit at the tendon insertions: Sever disease at the calcaneal apophysis in the prepubertal runner or jumper, Osgood-Schlatter at the tibial tubercle and Sinding-Larsen-Johansson at the inferior pole of the patella in the early adolescent, and medial epicondyle apophysitis in the throwing or racquet arm. The physeal stress injuries sit at the open growth plates subjected to repetitive shear, classically the proximal humerus, the distal radius, and the elbow in the thrower, and the vertebral ring apophysis and the pars in the spine of the gymnast or the fast bowler. [2] [7]
The bone stress injuries form their own spectrum from a bone stress reaction, where the bone is painful and oedematous but not broken, through to a frank stress fracture with a fracture line, and they cluster at the tibia, the metatarsals, the femoral neck, and the sacrum. Tendinopathy, the overuse of the tendon substance itself, is recognised but is the less common pattern in the child, because the apophysis or the physis usually yields first. A useful third classifier is the presence or absence of the red flags, because a bone stress injury with night pain, a limp, or focal bony tenderness moves out of the simple load-management pathway and into imaging and referral. [9] [2]
Epidemiology & Risk Factors
Overuse injuries have risen in children and adolescents as youth sport has reorganised around the year-round, single-sport, multi-team model, and the epidemiology now tracks that model rather than the seasonal play of earlier decades. The pattern is familiar: a child specialises early, joins a school team, a club team, and a representative squad in the same sport, trains more hours each week than is healthy for the age, takes no rest days, and presents with a gradual activity-related pain. The Stracciolini age-comparison study confirmed that the injury profile differs between children and adolescents, with the apophysitides clustering in the younger child and the stress injuries and tendinopathies rising in the adolescent. [8] [3]
The validated injury-risk triad is sport specialization, high training volume, and inadequate recovery, and each arm is measurable at the bedside. Sport specialization is the year-round commitment to a single sport at the exclusion of others, and it is graded by the three-question definition of training more than eight months a year in one sport, naming a single main sport, and giving up other sports. High training volume is flagged when the weekly training hours exceed the child's age in years, and when the organised training hours exceed twice the free-play hours. Inadequate recovery is the absence of rest days and the absence of two to three months away from the specialised sport each year. [3] [4]
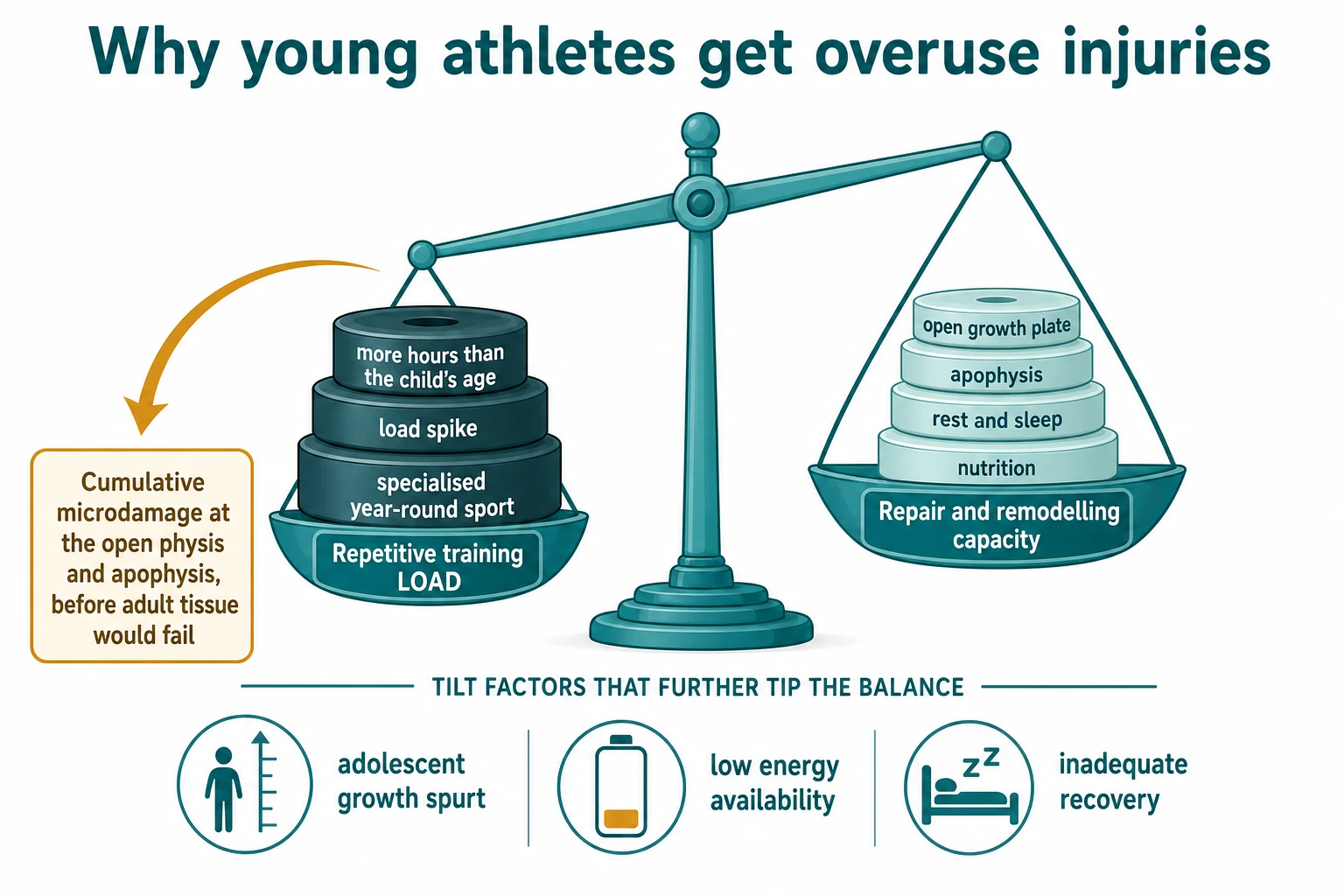
The growth-related factor is the adolescent growth spurt, during which bone lengthens faster than the muscle-tendon unit lengthens, the traction at the apophyses rises, and the bone mineral accrual lags the height gain, so the skeleton is transiently more vulnerable. The Jayanthi case-control study linked sports-specialized intensive training to a higher injury risk, and the Post study tied both specialization and training volume independently to the injury history in youth athletes. [3] [4]
The metabolic factor is low energy availability, whether from intentional weight control, disordered eating, or simply an intake that cannot match the expenditure, and it drives the bone stress injury through relative energy deficiency in sport. The 2023 IOC consensus extended the older female athlete triad model to show that the syndrome affects bone, reproductive, cardiovascular, gastrointestinal, and mental-health function, and applies to male athletes as well as female. The Tenforde study linked low bone mineral density to bone stress injuries at sites rich in trabecular bone, which is exactly the bone most sensitive to the energy-availability signal. [5] [9]
Pathophysiology
The unifying mechanism is an imbalance between the load applied to a tissue and the tissue's capacity to repair and remodel between loads. Every load produces a small amount of microdamage, and the tissue normally remodels that damage and adapts to become stronger, which is the basis of training. The injury appears when the load outpaces the repair, the microdamage accumulates faster than it is cleared, and the tissue fails. In the child, the cartilaginous physis and apophysis have a lower tolerance than the surrounding tendon and bone, so they fail first. [2] [10]
At a traction apophysis, the tendon pulls repeatedly on a growth-centre that is mostly cartilage, and the cartilage-fatigue and the small avulsions at the junction produce the inflammation, the swelling, and the bony prominence of an apophysitis. This is the mechanism of Sever disease at the calcaneus, of Osgood-Schlatter at the tibial tubercle, and of Sinding-Larsen-Johansson at the inferior pole of the patella. The Circi review of Osgood-Schlatter treatment found that the lesion settles as the apophysis fuses, which confirms that the open, cartilaginous apophysis is the vulnerable tissue. [7] [2]
At an open physis, the repetitive shear and compression produce a physeal stress injury, with widening and irregularity of the growth plate on imaging and, in the worst case, premature partial closure. At the bone, repetitive impact produces a bone stress reaction that progresses along a spectrum to a stress fracture, where the trabecular microcracks coalesce into a fracture line. The risk is highest where the bone is loaded in tension or in shear, at the tibia in the runner, the metatarsals in the dancer or the military-style marcher, the femoral neck in the distance runner, and the pars in the spine of the gymnast or the fast bowler. [9] [2]
The metabolic amplifier is low energy availability. When the energy left for the body after exercise is too low, the hormonal signals that drive bone formation fall, the menstrual cycle is suppressed in the female athlete, and the bone mineral density drops. The bone then remodels more slowly than it is loaded, the trabecular bone at the rich sites is the first to crack, and a stress fracture follows. The relative energy deficiency in sport model frames this as a mismatch of energy availability rather than a problem of any one hormone, which is why the syndrome affects bone, reproductive, cardiovascular, and other systems at once. [5] [9]
Clinical Presentation
The presentation of an overuse injury is built around the load, and the chief complaint is a pain that has a clear relationship to the sport and to rest. The pain comes on after a predictable amount of the activity, it builds as the session continues, and it eases when the child stops, and over weeks it begins earlier in the session and takes longer to settle. The onset is gradual and the family often traces it to a rise in training, a new surface, new footwear, or a growth spurt. The child is otherwise well, with no fever, no weight loss, and, in the simple case, no limp. [2] [8]
The presentation of the traction apophysitides is the tender growth-centre, and the site and the age band point to the diagnosis. Sever disease presents in the prepubertal, often eight-to-twelve-year-old runner or jumper with bilateral heel pain that comes on with running and jumping and is reproduced by squeezing the medial and lateral calcaneus together. Osgood-Schlatter disease presents in the early adolescent, often twelve-to-fifteen-year-old, with a tender bony prominence at the tibial tubercle that hurts with jumping, kneeling, and resisted knee extension. Sinding-Larsen-Johansson syndrome presents at the inferior pole of the patella in the same age band, and medial epicondyle apophysitis presents in the throwing or racquet arm of the young athlete with gradual medial elbow pain that worsens with pitching or serving. [7] [11]
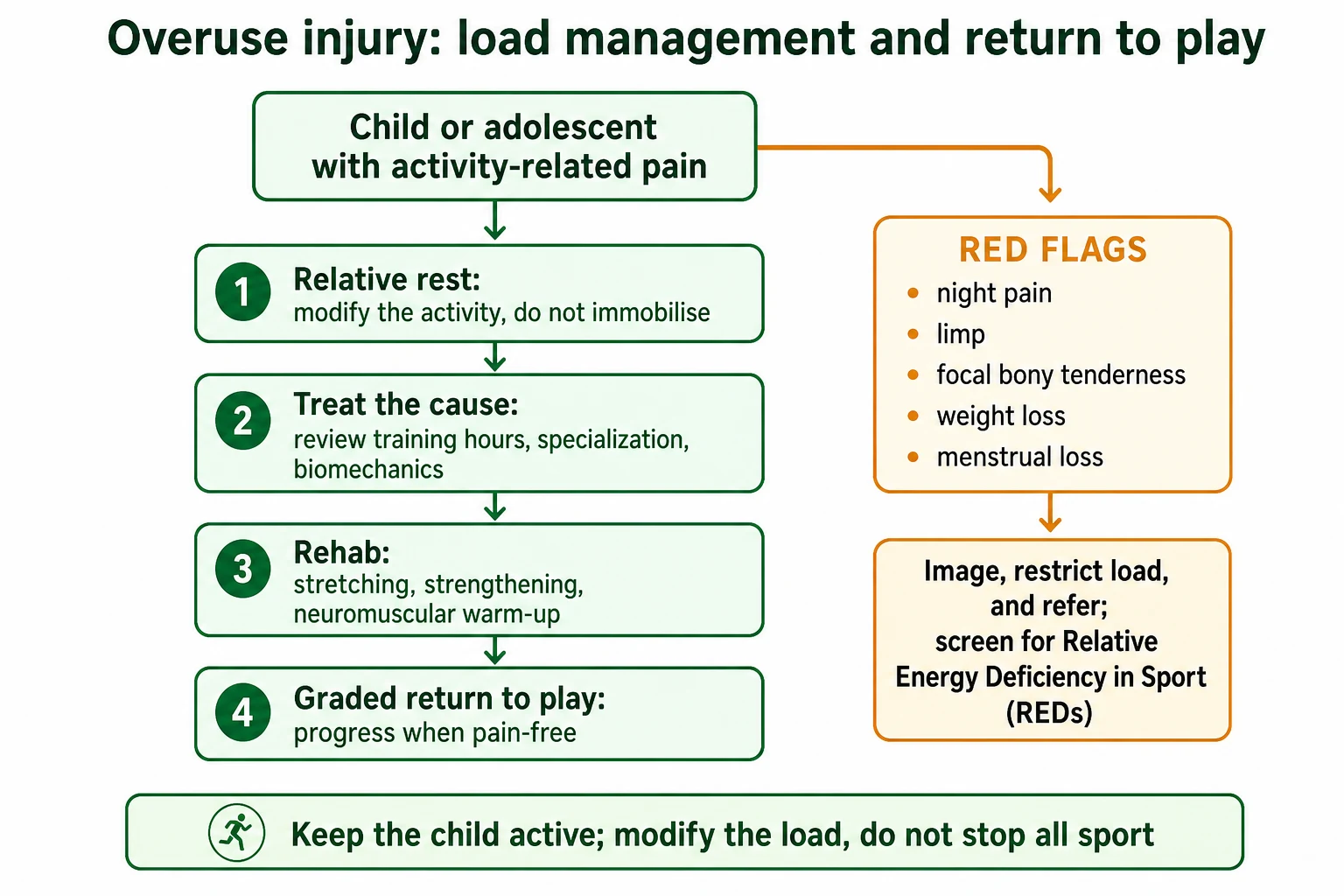
The presentation of a bone stress injury or a stress fracture differs in the details that must be elicited, and these details are the red flags. The pain no longer eases fully with rest, it begins to hurt at night, and it may hurt on walking. There is focal bony tenderness on a single point of bone, most often the tibia, the metatarsal, or the femur, and the child may develop a limp. The history that points to relative energy deficiency in sport is the history of weight loss, food restriction or fear of weight gain, a high training load, and, in the female athlete, loss of menses. A candidate who hears these features stops managing the pain as a simple apophysitis and moves to imaging and referral. [5] [9]
Differential Diagnosis
The differential of an activity-related knee pain in a young athlete runs from the common traction apophysitis to the serious bone and joint problems, and the history and the red-flag screen decide it. Osgood-Schlatter disease is the tender tibial tubercle in the early adolescent, and it is separated from a patellofemoral pain syndrome, which is a poorly localised retropatellar pain without the focal tenderness, from a meniscal injury, which has an effusion and mechanical symptoms, and from referred hip pathology such as a slipped capital femoral epiphysis, which is the trap of the knee pain that comes from the hip. [7] [8]
The differential of heel pain in the child runs from Sever disease to the problems that need imaging. Sever disease is bilateral, activity-related, and reproduced by the calcaneal squeeze, and it is separated from a calcaneal stress fracture, which is unilateral, focal, and progressive with night pain, from a tarsal coalition, which presents in early adolescence with recurrent ankle sprains or a rigid flatfoot, and from osteomyelitis or a bone tumour, which carry systemic features, severe night pain, or a single hot lesion on the radiograph. [11] [8]
The differential of a throwing-arm elbow pain runs from the apophysitis to the acute and the chronic injuries of the medial elbow. Medial epicondyle apophysitis is the gradual pain of the young thrower, and it is separated from an acute medial epicondyle avulsion, which follows a single violent pitch and is far more symptomatic with a sudden pop and an inability to continue, and from a ulnar collateral ligament injury, which is the adult-pattern injury that is uncommon before skeletal maturity because the apophysis yields first. [2]
The differential that the red-flag screen exists to surface is relative energy deficiency in sport. An adolescent athlete with a stress fracture, a second stress fracture after a first, a low bone mineral density for age, or a stress fracture at a low-risk site in a male athlete must prompt the energy-availability, menstrual, and nutritional history, because the bone injury is the visible tip of a metabolic problem that will recur until the energy availability is restored. [5] [9]
Clinical & Bedside Assessment
The assessment begins with the training history, because the load is both the cause and the treatment in this topic. Ask what sport or sports the child plays, how many teams, how many hours each week, how many months a year, how many rest days, and how the current hours compare with last month and last year. Quantify the free-play hours against the organised hours, and ask about a recent spike in training, a new surface or footwear, a growth spurt, and a recent change in weight or in eating. The growth and the puberty are recorded, including the height, the weight, the body mass index, and, in the female athlete, the age at menarche and the menstrual pattern. [1] [4]
The examination is built around the failing tissue and the red-flag screen. Inspect the limb for swelling, a bony prominence, or an asymmetry, and palpate the growth-centre for focal tenderness — the calcaneus for Sever disease, the tibial tubercle for Osgood-Schlatter, the inferior pole of the patella for Sinding-Larsen-Johansson, and the medial epicondyle for the throwing arm. Reproduce the pain with the offending activity where possible: resisted knee extension for the tibial tubercle, a heel raise or a jump for the calcaneus, and a throwing or a wrist-flexion action for the elbow. Perform the calcaneal squeeze test by pressing the medial and lateral calcaneus together, and a positive test in the prepubertal runner supports Sever disease. [11] [7]
The red-flag screen is run on every overuse injury, because it is the screen that separates the simple apophysitis from the stress fracture and the metabolic bone injury. Ask about night pain, pain on walking, and a limp, and palpate for a single point of focal bony tenderness. Weigh the child and plot the weight, ask about weight loss and about food restriction or exercise for weight control, and, in the female athlete, ask about the menses and any loss of periods. A positive red-flag screen redirects the encounter from load management to imaging, to referral, and to the relative energy deficiency in sport workup. [5] [9]
Investigations
The investigation of the simple traction apophysitis is the history and the examination, because the diagnosis is clinical and the imaging is avoided. A child with a typical apophysitis at the expected age band, a consistent story, and a negative red-flag screen needs no radiograph and no blood test, and the imaging in this setting exposes the child to radiation and the family to anxiety without changing the management. The investigation is reserved for the child in whom a stress fracture, a physeal stress injury, or an alternative diagnosis is suspected. [7] [2]
A radiograph is the first-line imaging when a red flag is present, and it serves two purposes: to exclude the mimics, such as an osteomyelitis, a tumour, or an acute avulsion, and to seek the stress injury. In Osgood-Schlatter disease the radiograph may show fragmentation of the tibial tubercle apophysis, which is supportive but not required, and in a physeal stress injury it may show physeal widening or irregularity. The limitation of the radiograph in the bone stress injury is that early stress fractures are often invisible on plain film, so a normal radiograph does not exclude the diagnosis. [8] [7]
Magnetic resonance imaging is the modality that resolves the early bone stress injury, and it is the next step when the radiograph is normal but the clinical suspicion remains. The MRI shows the bone marrow oedema of a stress reaction, the fracture line of a stress fracture, and the grade of the injury, and it guides the period of load restriction and the return to play. The MRI is also the modality for the physeal stress injury that is occult on the radiograph, and for the spondylolysis of the pars in the young athlete with low-back pain that extends into the leg. [9] [8]
The biochemistry and the dual-energy x-ray absorptiometry are reserved for the child or adolescent in whom relative energy deficiency in sport, low bone mineral density, or a recurrent stress fracture is suspected. The energy-availability, the hormonal, and the nutritional picture is built with the relevant bloods and the menstrual history, and the bone mineral density is measured with dual-energy x-ray absorptiometry read against paediatric reference values, because an adult comparison will miss the low-for-age bone density that drives the injury. The Tenforde study showed that low bone mineral density in male athletes is associated with bone stress injuries at trabecular-rich sites, which is the bone most sensitive to the energy-availability signal. [9] [5]
Management — Resuscitation
Resuscitation is not the task in the typical overuse injury, because these are walking, well children with no threat to life or limb, and the encounter is an outpatient or a community encounter. The rare exception is the overuse injury that has progressed to a high-risk stress fracture, such as a femoral-neck stress fracture at risk of completion, or a displaced avulsion on a pre-existing apophysitis, in whom the priority is the protected weight-bearing or the orthopaedic referral that prevents a catastrophic completion. [2] [9]
The rarer exception is the adolescent with severe relative energy deficiency in sport and medical instability — a dangerously low weight, an abnormal heart rate or an electrolyte disturbance, or an eating disorder with physiological compromise — in whom the acute medical and mental-health stabilisation precedes the load-management plan. This is uncommon, but the fellowship candidate holds it as the one situation in this topic where the acute stabilisation and the multidisciplinary admission precede the activity modification, and the threshold to involve the eating-disorder and the mental-health teams is low. [5]
The harm in this topic is the harm of omission — the missed stress fracture that completes, the unrecognised relative energy deficiency in sport that recurs, and the simple apophysitis that is immobilised and deconditioned — and it is prevented by the assessment and the red-flag screen rather than by a resuscitation step. The candidate who runs the red-flag screen on every overuse injury, and who restricts load and refers when the screen is positive, prevents the progression that the bedside resuscitation would otherwise have to rescue. [9] [2]
Management — Definitive & Stepwise
The definitive management of the overuse injury is load management, and the central principle is relative rest. Relative rest is the modification of the aggravating activity to a level the child can tolerate, while keeping the child active and the limb moving, and it stands in deliberate contrast to the two errors of continuing the full load and of stopping all activity. The evidence is clear that immobilising a simple apophysitis weakens the limb, deconditions the athlete, and prolongs the injury, and that the graded return to play, paced by the pain, restores function faster than rest alone. [7] [2]
The load is addressed at its source, because the pain recurs unless the training volume is changed. The weekly hours are brought below the child's age in years, the organised hours are brought below twice the free-play hours, and the rest days and the two-to-three months away from the specialised sport are written into the plan. The American Academy of Pediatrics guidance delays sport specialization to late adolescence and protects at least one to two rest days a week, and the American Medical Society for Sports Medicine position statement frames overuse prevention as a family, coach, and clinician task. A biomechanical review of the footwear, the surface, the technique, and the throwing or the running mechanics addresses the local contributors to the load. [1] [2]
The rehabilitation is a programme of stretching and strengthening of the muscle-tendon units that cross the failing apophysis, with a quadriceps and hamstring programme for the tibial tubercle and a calf programme for the calcaneus, and a graded return to play that progresses through walking, jogging, sport-specific drills, and full play as the pain-free interval lengthens. The Circi review of Osgood-Schlatter treatment confirmed that the conservative, activity-modification approach is the standard of care, with surgery reserved for the rare persistent case after skeletal maturity. [7]
The bone stress injury is managed with a stricter load restriction, graded to the site and the MRI grade, with protected weight-bearing or, for a high-risk site such as the femoral neck, non-weight-bearing and orthopaedic input, and a return to play only when the pain-free interval is sustained and the imaging has settled. The relative energy deficiency in sport is managed with a multidisciplinary plan that restores energy availability through nutrition and load reduction, addresses the menstrual disturbance, and protects bone mineral density, with the physician, the dietitian, the physiotherapist, and a mental-health clinician, and the athlete does not return to full training until the energy availability, the menstrual function, and the bone are on a safe trajectory. [5] [9]
The four steps of load management
Specific Subtypes & Scenarios
Sever disease, or calcaneal apophysitis, is the traction apophysitis of the prepubertal runner or jumper, and the eight-to-twelve-year-old presents with bilateral heel pain that comes on with running and jumping and is reproduced by the calcaneal squeeze. The child is otherwise well, walks normally between bursts of pain, and has no night pain. The management is relative rest, a heel cup or a small heel raise to cushion the pull of the calf, calf stretching, and a graded return, and the condition resolves as the calcaneal apophysis fuses at skeletal maturity. [11] [8]
Osgood-Schlatter disease is the traction apophysitis of the tibial tubercle, and the early adolescent presents with a tender bony prominence below the knee that hurts with jumping, kneeling, and resisted knee extension. The management is relative rest with modification of jumping and sprinting, a quadriceps and hamstring programme, and a graded return, and the Circi review confirmed that conservative management is the standard of care. Sinding-Larsen-Johansson syndrome is the related traction apophysitis at the inferior pole of the patella, with the same age band and the same principles, and it is separated by the site of the focal tenderness. [7]
Medial epicondyle apophysitis is the traction apophysitis of the throwing or racquet arm, and it is the childhood counterpart of the adult ulnar collateral ligament injury, because the open apophysis yields before the ligament. The young thrower presents with gradual medial elbow pain that worsens with pitching or serving, and the management is relative rest, pitching-volume limits, a review of the throwing mechanics, and a graded return. It is separated from an acute medial epicondyle avulsion, which follows a single violent throw with a pop and an inability to continue, and which needs orthopaedic assessment. [2]
The bone stress injury and the stress fracture are the subtypes that the red-flag screen exists to surface. The distance runner with tibial pain that hurts at night, the dancer with a metatarsal stress fracture, and the runner with a femoral-neck stress fracture are managed with a load restriction graded to the site and the MRI grade, with orthopaedic input for the high-risk sites. The adolescent with a stress fracture and weight loss, food restriction, or loss of menses is managed for relative energy deficiency in sport with the multidisciplinary team, because the bone injury is the visible tip of the metabolic problem. [9] [5]
Complications & Pitfalls
The complications of this topic are the harms on both sides of the load decision. The harm of over-treatment is the unnecessary imaging, the prolonged immobilisation, and the cessation of sport applied to a simple traction apophysitis, and it costs the family money and anxiety, exposes the child to radiation, and deconditions the athlete. The contemporary management of the apophysitides is relative rest, and the stewardship of the consultation is to remove the immobiliser and the cessation of sport from the management of the typical child. [7] [2]
The harm of under-treatment is the missed stress fracture and the unrecognised relative energy deficiency in sport. A tibial pain that is dismissed as shin splints while the load continues can progress to a complete fracture, and an adolescent with recurrent stress fractures whose energy availability is never addressed will recur until the metabolism is restored. The Tenforde study linked low bone mineral density to bone stress injuries at trabecular-rich sites, which is the bone most sensitive to the energy-availability signal, and the safeguard is the red-flag screen run on every overuse injury. [9] [5]
The pitfall of treating the site while ignoring the load is the commonest error. A child whose tibial tubercle is iced and stretched but whose twenty weekly training hours are never reduced returns with the same pain, because the cause has not changed. The safeguard is the load history taken at every visit, and the willingness to write the reduction in hours into a plan the family and the coaches can act on. [3] [1]
The pitfall of the reassuring label is the error that the red-flag screen prevents. A stress fracture that is reassured as an apophysitis continues to load and may complete, and a relative energy deficiency in sport that is missed in the athlete with a single stress fracture recurs as a second or a third. The safeguard is the discipline of asking, in every overuse injury, about night pain, a limp, focal bony tenderness, weight loss, and menstrual loss, and of moving to imaging and referral the moment the answer is yes. [5] [2]
Prognosis & Disposition
The prognosis of the traction apophysitides is excellent, and the resolution is the rule, because the open, cartilaginous apophysis that fails under load fuses at skeletal maturity and the traction at the site resolves. Sever disease settles as the calcaneal apophysis fuses, Osgood-Schlatter settles as the tibial tubercle apophysis fuses, and the tender bony prominence may persist into adulthood as a painless lump that needs no treatment. The Circi review confirmed that the conservative, activity-modification approach carries the lesion through to its natural resolution, with surgery reserved for the rare persistent case after maturity. [7] [8]
The prognosis of the bone stress injury depends on the early recognition and the site. A low-risk tibial stress reaction managed early with a period of load restriction heals and returns to sport, while a high-risk femoral-neck stress fracture that is loaded after the onset of pain can complete and displace, with a lasting burden. The relative energy deficiency in sport, managed early with the multidisciplinary restoration of energy availability, protects both the bone and the reproductive and cardiovascular health, while the unrecognised syndrome recurs and erodes the bone mineral density across the adolescent years. [9] [5]
The disposition is shared between the general paediatrician, the sports-medicine clinician, the physiotherapist, the dietitian, and the mental-health team. The general paediatrician owns the initial assessment, the load history, the red-flag screen, and the simple load-management plan, and the sports-medicine clinician and the physiotherapist own the graded return to play and the biomechanical review. The dietitian and the mental-health clinician join the team for the relative energy deficiency in sport, and the orthopaedic surgeon owns the high-risk stress fracture and the rare persistent apophysitis after maturity. The fellowship answer names the right specialist for the right diagnosis, and the load plan is communicated to the school, the coach, and the family so the prevention message travels beyond the clinic. [2] [5]
Special Populations
The early-specializing, year-round single-sport athlete carries the highest injury risk, and the prevention message is tailored to this child. The family and the coach are counselled on delaying specialization to late adolescence, on the protective rest days and the two-to-three months away from the specialised sport each year, and on the value of diverse movement and free play through growth. The Jayanthi and Post work quantified the risk, and the family that understands the triad is the family that can change the load before the injury appears. [3] [1]
The female adolescent athlete carries a higher risk of the bone stress injury through low energy availability, and the menstrual and the nutritional history are taken routinely, not only when a stress fracture appears. The 2023 IOC consensus extended the syndrome beyond the female athlete, but the female athlete remains the higher-risk group for the combination of low energy availability, menstrual disturbance, and low bone mineral density, and the early menarche, the regular cycle, and the adequate intake are the protective markers the clinician seeks. The candidate who asks about the menses at every sports visit catches the syndrome before the second stress fracture. [5] [9]
Children with a disability, a neurodiversity, or a chronic condition participate in sport and carry their own load profiles, and the load plan is adapted to the condition rather than copied from the typical athlete. The child with cerebral palsy, a limb difference, or an autism-spectrum pattern may have an altered gait, an altered muscle balance, or a reduced ability to report pain, and the threshold for the load review and the physiotherapy input is lower. The safeguarding of the child is kept central, because the pressure to train and to specialise can sit alongside a vulnerability that the clinician protects. [2]
Children in remote, Indigenous, and socioeconomically disadvantaged settings face additional barriers to the pre-participation care, the footwear, the surfaces, and the sports-medicine access that the prevention message assumes, and the public-health and the school-based programmes carry the prevention where the clinic cannot reach. The newly arrived migrant or refugee child may have an undocumented history and a family carrying strong expectations of sporting success, and the counselling is delivered with the interpreter and the cultural respect the encounter demands, with the load-management message kept plain and the child kept central. [1]
Evidence, Guidelines & Regional Differences
The evidence base for the specialization and the intensive-training guidance rests on the Brenner American Academy of Pediatrics clinical report, which advises delaying sport specialization to late adolescence, scheduling at least one to two rest days each week, and taking two to three months away from the specialised sport each year. The report is the framework the fellowship answer reaches for when a family asks whether a child should specialise, and it is paired with the DiFiori American Medical Society for Sports Medicine position statement on overuse injury and burnout, which frames prevention as a shared family, coach, and clinician task. [1] [2]
The evidence for the injury-risk triad rests on the Jayanthi case-control study and the Post youth-athlete study. The Jayanthi study linked sports-specialized intensive training to a higher injury risk and offered the practical thresholds of training more hours per week than the child's age and more than twice the free-play hours, and the Post study tied both specialization and training volume independently to the injury history. The Stracciolini age-comparison study framed the differing injury profile of children and adolescents, with the apophysitides in the younger child and the stress injuries and tendinopathies in the adolescent. [3] [4]
The evidence for the prevention programmes rests on the Soligard cluster randomised trial of a comprehensive warm-up programme in young female footballers aged thirteen to seventeen years, which showed a lower injury rate in the intervention arm and underpins the neuromuscular warm-up such as the FIFA 11+ that is now applied across sports. The evidence for the relative energy deficiency in sport rests on the 2023 IOC consensus, which extended the older female athlete triad model and showed the syndrome's reach across bone, reproductive, cardiovascular, gastrointestinal, and mental-health function, and on the Tenforde study, which linked low bone mineral density to bone stress injuries at trabecular-rich sites. [6] [5]
The load-management concept draws on the Gabbett training-injury prevention paradox, which framed the protective effect of a high chronic load that is built gradually and the injurious effect of an acute spike in load, and which underpins the acute-to-chronic workload ratio used in the adult and the elite-athlete literature. The paediatric application is treated with caution, because the ratio was derived in adult and elite athletes and the growing skeleton, the apophysis, and the energy availability add variables the adult model does not carry. The regional differences are modest: the specialization and the prevention guidance is broadly consistent across the regions, while the access to sports medicine, the school-based prevention, and the public-health vitamin D and nutrition support vary with the setting. [10] [1]
Exam Pearls
The fellowship answer turns on five facts. An overuse injury is the microtrauma of repetition, distinct from the acute macrotrauma of a single event. The immature physis and the traction apophysis fail before the adult tendon, ligament, or bone, which is why the apophysitides are the pattern of the child. The injury-risk triad of specialization, training volume, and inadequate recovery is measured at the bedside with the hours-per-week and the free-play ratio. The management is relative rest and a graded return to play, with the load addressed at its source and the child kept active. And the red flags — night pain, a limp, focal bony tenderness, weight loss, and menstrual loss — move the child off the load-management pathway and into imaging, restriction, and the relative energy deficiency in sport workup. [2] [5]
The examiner probes three traps. The first is the over-treated apophysitis — a child placed in a brace or an immobiliser, or taken out of all sport, that the evidence does not support, and the safeguard is the principle of relative rest. The second is the under-treated stress fracture — a tibial pain dismissed as shin splints while the load continues, and the safeguard is the red-flag screen and the MRI when the radiograph is normal. The third is the missed relative energy deficiency in sport — an adolescent with a stress fracture whose energy availability is never addressed, and the safeguard is the menstrual and the nutritional history taken at every sports visit, with the multidisciplinary team engaged early. [9] [7]
The examiner rewards the candidate who frames the overuse injury as a load-management exercise rather than a diagnosis-and-rest exercise. The load history is built, the failing tissue is named, the red-flag screen is run, the simple apophysitis is managed with relative rest and a graded return, and the stress fracture and the relative energy deficiency in sport are imaged, restricted, and referred. A candidate who shows this safety and this stewardship — the confident load management and the vigilant screen — demonstrates the systems thinking that the fellowship demands, and the prevention message that carries beyond the clinic into the family, the school, and the coach. [1] [2]
References
- [1]Brenner JS, Council on Sports Medicine and Fitness. Sports Specialization and Intensive Training in Young Athletes. Pediatrics, 2016.PMID 27573090
- [2]DiFiori JP, Benjamin HJ, Brenner J, et al. Overuse injuries and burnout in youth sports: a position statement from the American Medical Society for Sports Medicine. Clin J Sport Med, 2014.PMID 24366013
- [3]Jayanthi NA, LaBella CR, Fischer D, et al. Sports-specialized intensive training and the risk of injury in young athletes: a clinical case-control study. Am J Sports Med, 2015.PMID 25646361
- [4]Post EG, Trigsted SM, Riekena JW, et al. The Association of Sport Specialization and Training Volume With Injury History in Youth Athletes. Am J Sports Med, 2017.PMID 28288281
- [5]Mountjoy M, Ackerman KE, Bailey DM, et al. 2023 International Olympic Committee's (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs). Br J Sports Med, 2023.PMID 37752011
- [6]Soligard T, Myklebust G, Steffen K, et al. Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. BMJ, 2008.PMID 19066253
- [7]Circi E, Atalay Y, Beyzadeoglu T. Treatment of Osgood-Schlatter disease: review of the literature. Musculoskelet Surg, 2017.PMID 28593576
- [8]Stracciolini A, Casciano R, Levey Friedman H, et al. Pediatric sports injuries: an age comparison of children versus adolescents. Am J Sports Med, 2013.PMID 23739684
- [9]Tenforde AS, Parziale AL, Popp KL, et al. Low Bone Mineral Density in Male Athletes Is Associated With Bone Stress Injuries at Anatomic Sites With Greater Trabecular Composition. Am J Sports Med, 2018.PMID 28985103
- [10]Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med, 2016.PMID 26758673
- [11]Morancie NA, Irvin L, Rayala BZ. Heel Pain: Diagnosis and Management. Am Fam Physician, 2025.PMID 41533410