Paeds · rheumatology-musculoskeletal-and-sports
Transient synovitis and the irritable hip
Also known as irritable hip · transient synovitis · toxic synovitis · observation hip · coxitis fugax
A fellowship approach to the child with an irritable hip: transient synovitis as the commonest benign cause of acute limp, the Kocher clinical prediction rule that separates it from septic arthritis at the bedside, the ultrasound effusion and the inflammatory markers that frame the decision, and the watchful waiting with rest and a non-steroidal anti-inflammatory drug that resolves the limp within one to two weeks once pus has been excluded.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A five-year-old boy is brought to the emergency department with a one-day limp and a sore right hip, two days after a runny nose; he is afebrile, he walks cautiously but he walks, his inflammatory markers are normal, and the ultrasound shows a small hip effusion. Or an eight-year-old girl limps after school with a stiff hip and a recent cough, and the question is whether to send her home or to tap the joint. In each, the move is the same — score the probability of sepsis, exclude the mimics, and only then call it transient synovitis. [6] [9]
The irritable hip in four moves — Score, Scan, Sample-if, Soothe
Overview & Definition
The irritable hip is the clinical syndrome of a painful, stiff hip in a child who limps or refuses to walk, and transient synovitis is its commonest and most benign cause — a self-limiting, non-infectious inflammation of the hip synovium that resolves without sequelae. The two terms travel together because the bedside problem is the stiff, painful hip, and the diagnostic work is to separate the harmless transient synovitis from the dangerous septic arthritis, the surgical Perthes, and the structural slipped capital femoral epiphysis. [6] [9]
The fellowship framing rests on a single diagnostic truth. Transient synovitis is a diagnosis of exclusion, made only once septic arthritis has been ruled out by the Kocher clinical prediction rule, the inflammatory markers, and — when the probability is high — the synovial fluid. The pathology is a transient, reactive inflammation of the synovium, often following a viral upper respiratory infection, that produces a small effusion, a stiff hip, and a limp, and that resolves spontaneously over one to two weeks without antibiotics, without surgery, and without permanent damage. [1] [7]
The clinical importance comes from what happens when the exclusion is skipped. A child with septic arthritis mislabelled as transient synovitis loses the window for drainage, and the intracapsular pus destroys the cartilage and the femoral head blood supply within hours. A child with early Perthes mislabelled as transient synovitis loses the chance for early imaging and containment planning. The safeguard is the discipline of scoring the probability of sepsis before reassuring anyone, and of reviewing the child whose limp does not resolve within the expected window. [4] [9]
Classification
Classification of the irritable hip rests on the single axis that matters at the bedside — the probability of bacterial infection, estimated by the Kocher clinical prediction rule. The Kocher criteria were derived in 1999 from a retrospective study of children presenting with an irritable hip, identifying four independent predictors that separate septic arthritis from transient synovitis, and they remain the taught framework for the decision of whether to aspirate the joint. [1]
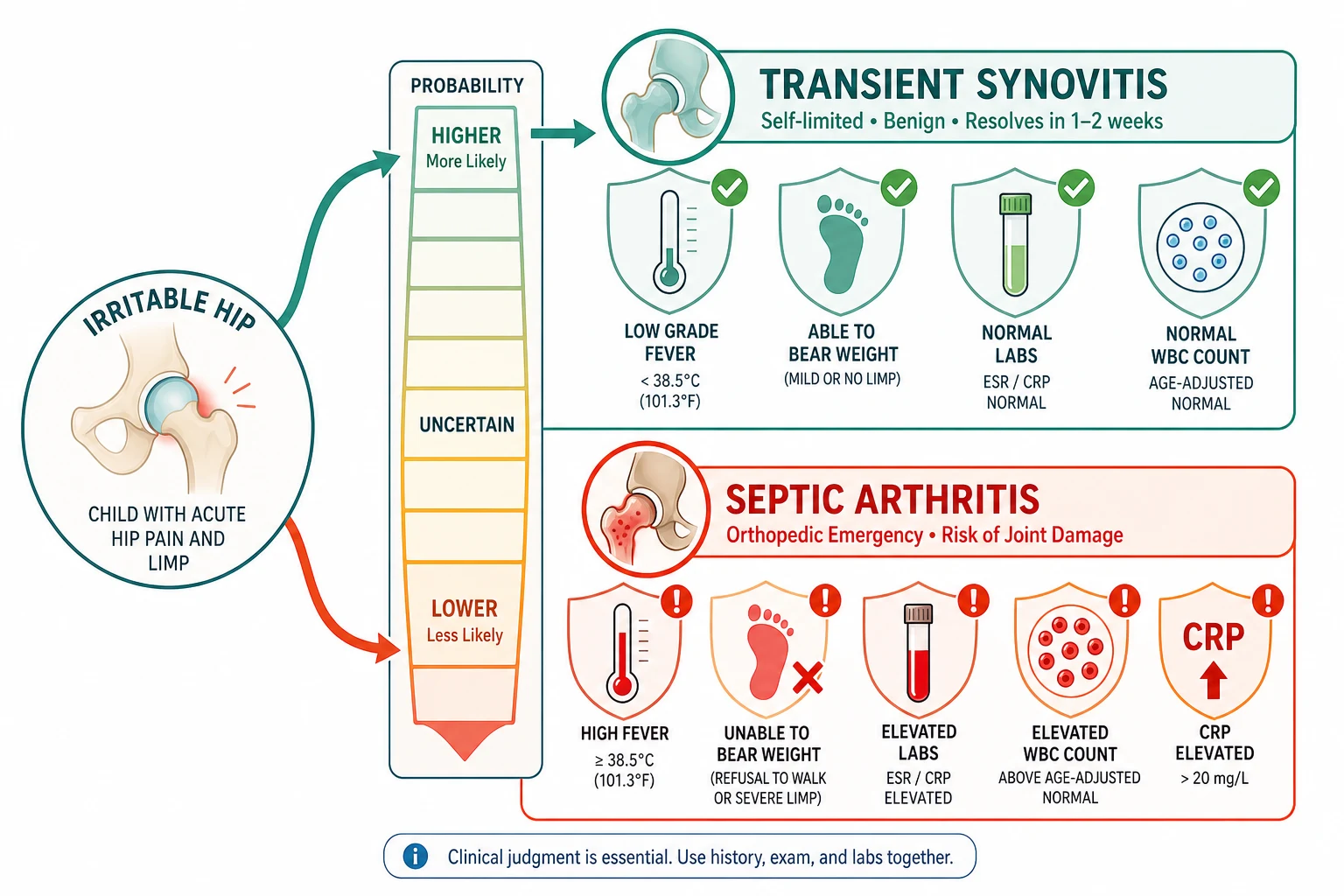
The four Kocher predictors are a history of fever above thirty-eight point five degrees Celsius, an inability to bear weight on the affected limb, an erythrocyte sedimentation rate above forty millimetres per hour, and a peripheral white blood cell count above twelve thousand per microlitre. The predicted probability of septic arthritis rises steeply with the number of predictors — below one per cent with none, roughly three per cent with one, forty per cent with two, ninety-three per cent with three, and over ninety-nine per cent with all four — so a child with zero or one predictor and a well appearance fits transient synovitis, while two or more predictors demand joint aspiration. [1] [2]
The Caird prospective study refined the framework by adding the C-reactive protein, which emerged as the single strongest independent predictor, with a cut-off of twenty milligrams per litre. The Caird study also offered the important calibration caveat — the original Kocher probabilities were derived retrospectively and may overestimate the true risk, so in Caird's prospective cohort the presence of all four predictors carried a probability closer to fifty-nine per cent rather than ninety-nine. The clinical message is that the Kocher criteria sharpen suspicion but never rule out sepsis with certainty, and a reassuring score never overrides a septic-looking child. [3]
Epidemiology & Risk Factors
Transient synovitis is the commonest cause of acute hip pain and limp in children, and it accounts for the majority of irritable hip presentations seen in primary care and emergency departments. The peak age is three to eight years, with the highest incidence around four to six years, and boys are affected roughly twice as often as girls. The knee and the ankle may also be the site of transient synovitis, but the hip dominates the clinical picture because of its deep location and its surgical stakes. [6] [4]
The single strongest epidemiological association is a recent viral illness. Roughly a third to a half of children report an upper respiratory infection or another viral illness in the one to two weeks before the limp, which supports the reactive, post-infectious mechanism and gives the diagnosis its characteristic story. Minor trauma is a second, weaker association, but the relationship to vaccination, allergy, and atopy is unproven and should not anchor the assessment. [6] [7]
The risk factor that matters most for the fellowship answer is the age group itself, because it overlaps with the peak ages of the dangerous mimics. The three-to-eight-year window of transient synovitis also contains the peak of Perthes disease in the young school-age child, and it sits just below the ten-to-fifteen-year window of slipped capital femoral epiphysis. The age therefore widens the differential rather than narrowing it, and the well-looking child with the classic story still warrants the exclusion of sepsis and the review of the persistent limp. [9] [6]
Pathophysiology
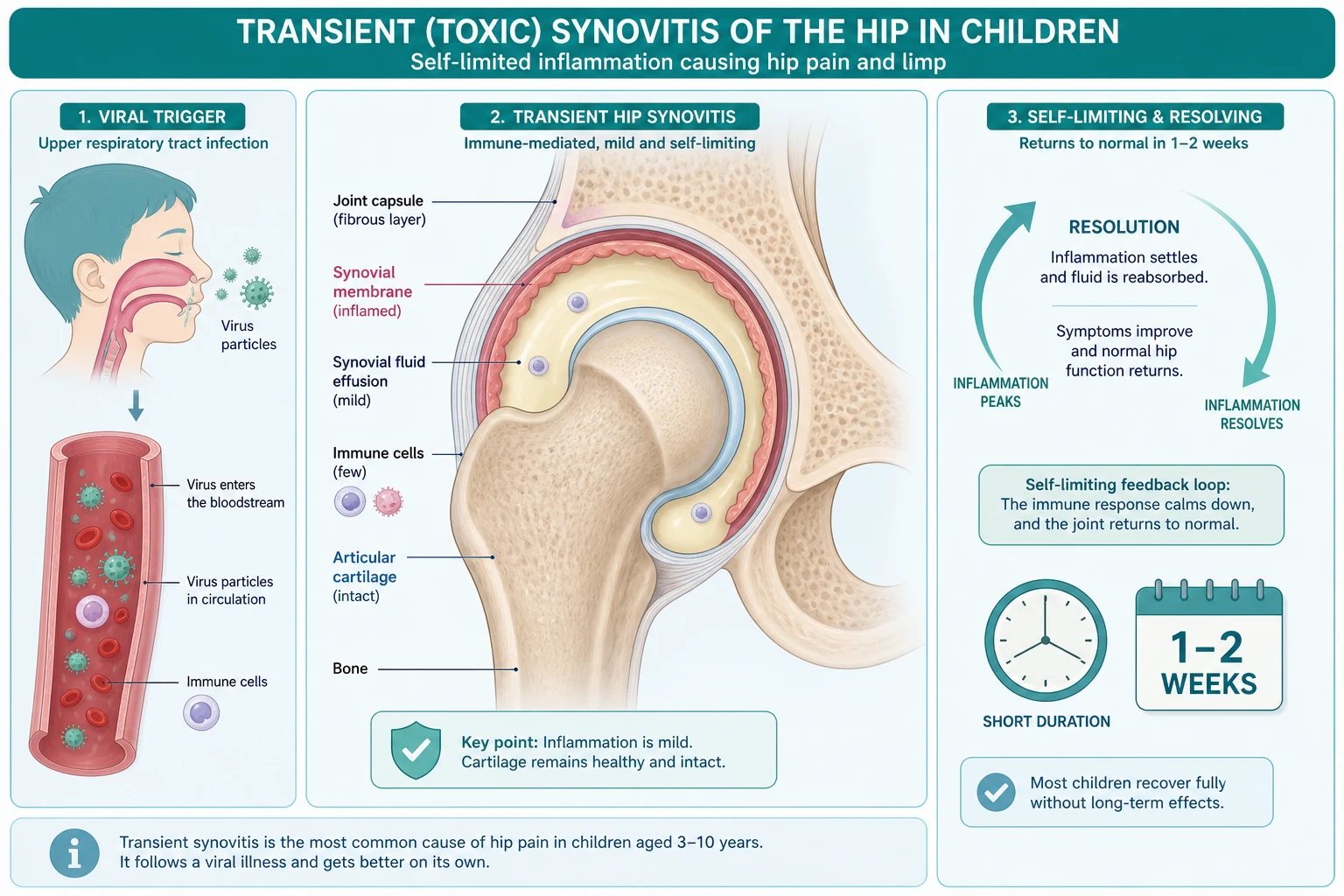
The pathophysiology of transient synovitis is a transient, reactive inflammation of the synovial membrane, and the leading mechanism is a post-infectious immune response. A viral upper respiratory infection precedes the limp in many children, and the temporal relationship, the self-limiting course, and the absence of a recoverable organism all support an immune-mediated synovitis rather than a direct infection of the joint. [6] [7]
The inflammation produces a small effusion and a stiff, painful hip. The synovial membrane becomes mildly oedematous and hyperaemic, the joint space fills with a modest volume of clear or straw-coloured fluid, and the raised intra-articular pressure stretches the capsule and limits movement, producing the characteristic flexion, abduction, and external rotation posture that relieves the capsular tension. Unlike septic arthritis, the neutrophilic response is modest, the cartilage is spared, and the fluid remains sterile on culture, which is why the process resolves without the destruction that defines pus under pressure. [6] [10]
The contrast with septic arthritis defines the urgency. In septic arthritis, bacteria seed the synovium, neutrophils pour into the joint, and proteases erode the cartilage within hours, with the intracapsular pressure strangulating the femoral head blood supply. In transient synovitis, the inflammation is self-limiting, the effusion is small and sterile, and the cartilage and the blood supply are preserved, so the outcome is full recovery without sequelae. This biological difference is the reason transient synovitis is managed by rest and time, while septic arthritis is a surgical emergency. [1] [9]
Clinical Presentation
The presentation is the well-looking child with an acute limp and a stiff hip. The onset is over hours to a day or two, the pain is in the groin, the thigh, or sometimes the knee because hip pain refers distally, and the child holds the hip flexed, abducted, and externally rotated to relieve the capsular tension. The child is afebrile or has a low-grade fever, and the defining feature is that the child remains systemically well and is usually still willing to bear weight cautiously, even if with a limp. [6] [9]
The recent viral illness is the story that points toward transient synovitis. A parent describes a runny nose, a cough, or a sore throat in the one to two weeks before the limp, and the child who was recovering from the virus then develops the hip pain, which supports the reactive mechanism. The absence of a high fever, the absence of a toxic appearance, and the preserved ability to walk — however reluctantly — are the features that separate the benign picture from the septic one, and they are what the Kocher criteria formalise. [1] [4]
Which reassuring stories must never close the search for sepsis? A child with a recent viral illness and a limp is not automatically transient synovitis — the Kocher criteria and the inflammatory markers, not the preceding virus, separate the two. A well-looking toddler who walks may still harbour early septic arthritis, because Kingella kingae produces a deceptively mild picture in the under-four. And a child whose limp persists beyond two weeks is not a slow transient synovitis but a candidate for repeat imaging, because the mimics declare themselves by not resolving. [8] [4]
Differential Diagnosis
The differential diagnosis of the limping child is broad, and the fellowship skill is to separate the benign transient synovitis from its dangerous mimics using the Kocher criteria, the inflammatory markers, the age, and the imaging. Septic arthritis is the must-not-miss mimic and the one most easily confused, and it is separated by the fever, the refusal to bear weight, the raised markers, and the frankly purulent synovial fluid. The Kocher criteria and the synovial fluid cell count are the tools, and when the distinction remains unclear, the joint is aspirated. [1] [9]
Perthes disease enters the differential in the young school-age child, because its peak age overlaps with transient synovitis. Perthes is an avascular necrosis of the femoral head that produces a persistent or intermittent limp and a stiff hip, and it is separated from transient synovitis by its persistence beyond the expected one-to-two-week window and by the radiographic changes that appear over weeks. A limp attributed to transient synovitis that does not resolve demands repeat radiographs and specialist review, because early Perthes looks normal on the first film. [6] [9]
Slipped capital femoral epiphysis enters the differential in the older child and adolescent, presenting with a limp and a stiff or externally rotated hip, and it is identified by its older age group and its radiographic slip. Reactive arthritis follows a gastrointestinal or genitourinary infection and tends to be oligoarticular. Juvenile idiopathic arthritis declares itself by persistence beyond six weeks or by recurrence, and a toddler's fracture, a stress fracture, and rarely a bone tumour complete the list. The single rule is that transient synovitis is excluded by exclusion, not by the appearance of any mimic. [6] [7]
Clinical & Bedside Assessment
The recognition move is to treat every child with an acute stiff hip and a limp as septic arthritis until the bedside assessment and the markers suggest otherwise, and to perform a full musculoskeletal and systemic examination. The history must establish the onset and pace of the limp, the fever pattern, the ability to bear weight, any preceding viral illness, recent trauma, and the immunisation status. The well appearance and the cautious weight bearing point toward transient synovitis, but they never close the search for sepsis. [1] [9]
The bedside examination must look, feel, move, and measure the hip and every joint. Look for the posture of greatest comfort — the flexed, abducted, externally rotated hip — and for any swelling or erythema, which is uncommon in transient synovitis and worrying when present. Feel for warmth, comparing with the contralateral hip, and for the boggy swelling of an effusion, which is rarely palpable at the hip because the joint is deep. Attempt gentle passive movement, expecting a mild to moderate restriction and discomfort at the extremes in transient synovitis, in contrast to the severe pain and rigid refusal of septic arthritis, and document the willingness to bear weight. [6] [4]
Which examination findings must never be dismissed? A child who holds the hip absolutely still and screams at any movement has a septic hip until proven otherwise, because the profound pseudoparalysis is the sign of pus under pressure. A febrile child with a swollen or warm hip and a refusal to bear weight is not transient synovitis regardless of the preceding virus, and the markers and the ultrasound are obtained without delay. And a child with knee pain must have the hip examined and imaged, because hip pain refers to the knee and a septic hip hides behind a normal-looking knee. [1] [4]
Investigations
Ultrasound is the first-line investigation for the irritable hip, because it confirms the presence of a hip effusion, excludes some of the mimics, and guides an aspiration when one is needed. The effusion appears as a widened joint space with fluid in the anterior recess, and an asymmetry of more than two millimetres between the two hips or an absolute measurement above five to seven millimetres is taken as significant. Ultrasound is rapid, radiation-free, and available at the bedside, and a normal ultrasound in a child with a convincing clinical picture does not exclude early septic arthritis, because a small effusion may be missed. [11] [7]
The blood tests frame the probability of sepsis and the baseline for follow-up. A full blood count, an erythrocyte sedimentation rate, and a C-reactive protein provide the Kocher and Caird predictors — the ESR above forty and the white cell count above twelve thousand are the original Kocher cut-offs, and a CRP above twenty milligrams per litre is the Caird addition and the strongest single predictor. Normal or mildly raised markers in a well-looking child who bears weight support transient synovitis, while raised markers in a febrile child who refuses to bear weight demand aspiration. Blood cultures are drawn when sepsis is suspected, before any antibiotic. [1] [3]
Joint aspiration is the single investigation that excludes pus, and it is performed under ultrasound guidance when the Kocher probability is two or more predictors or when the clinical picture is septic. The synovial fluid is sent for a cell count, a Gram stain, and culture, with direct inoculation into blood-culture bottles to recover fastidious organisms such as Kingella kingae. In transient synovitis the fluid is clear or straw-coloured with a low cell count, usually below fifteen thousand and rarely approaching the frankly purulent counts of sepsis, a negative Gram stain, and a sterile culture. Plain radiographs are usually normal in transient synovitis, and they are obtained to exclude the mimics — a fracture, early Perthes, a slipped epiphysis, or a destructive bone lesion. Magnetic resonance imaging is reserved for the atypical or non-resolving case, because Yang showed that it distinguishes transient synovitis from septic arthritis by the marrow signal and the enhancement pattern. [1] [10]
Management — Resuscitation
Resuscitation is rarely needed in transient synovitis, because the child is systemically well, but the same pathway that excludes sepsis also screens for the child who needs resuscitation. The airway, breathing, and circulation are assessed, and a febrile, toxic, or shocked child is managed as septic arthritis with intravenous access, fluid resuscitation, cultures before antibiotic, and urgent drainage, not as transient synovitis. The recognition that a sick child belongs on the sepsis pathway is the most important resuscitation move. [4] [9]
Analgesia is part of the assessment, because a child in pain cannot be examined or imaged properly. A non-steroidal anti-inflammatory drug such as ibuprofen at five milligrams per kilogram three times a day, to a maximum of thirty milligrams per kilogram per day, relieves the synovitis pain and allows a gentle examination, and simple analgesia such as paracetamol at fifteen milligrams per kilogram every four to six hours is added as needed. The child who is still in severe pain despite simple measures, or whose pain is disproportionate to a small effusion, is reassessed for sepsis or a mimic. [6]
The cultures and the aspiration, when indicated, are obtained before any antibiotic in the child who sits on the sepsis side of the Kocher score. In the well-looking child with zero or one predictor, the resuscitation phase is brief and the pathway moves quickly to the definitive symptomatic care and the safety-net review. The discipline of scoring the probability first holds in every case, because it is the score, not the appearance alone, that decides whether the child is observed or aspirated. [1] [3]
Management — Definitive & Stepwise
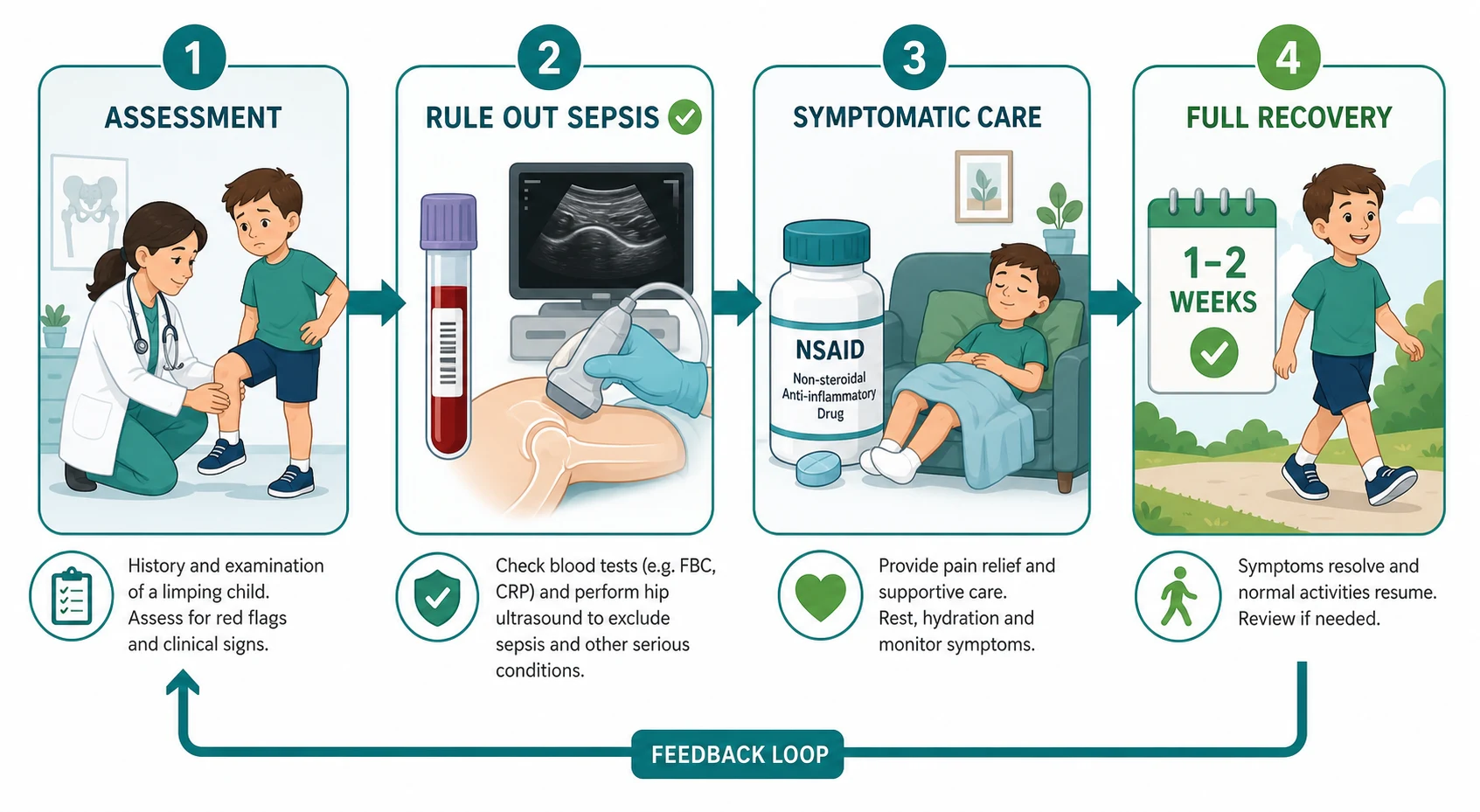
The definitive management of transient synovitis, once sepsis has been excluded, is rest and symptomatic relief, and the condition resolves spontaneously within one to two weeks. The child is advised to rest and to avoid weight bearing until the pain subsides, then to return to normal activity as the symptoms allow. A non-steroidal anti-inflammatory drug such as ibuprofen at five milligrams per kilogram three times a day, to a maximum of thirty milligrams per kilogram per day, reduces the synovial inflammation and the pain, and simple analgesia is added as needed. No antibiotics are given, because the process is non-infectious and sterile. [6] [7]
The safety-net is the non-negotiable part of the discharge. The family is told that transient synovitis resolves within one to two weeks, and that a return of fever, a refusal to bear weight, or a worsening of the pain demands urgent review, because these are the features of a declaring septic arthritis or a missed mimic. A routine review at one to two weeks is arranged, either in primary care or in the clinic, and the limp that has not resolved by then prompts repeat imaging and specialist referral. The safety-net turns the benign diagnosis into a safe diagnosis. [4] [9]
The stepwise decision is framed by the Kocher score. A child with zero or one predictor, a well appearance, normal or mildly raised markers, and an ultrasound effusion is managed as transient synovitis with rest and review. A child with two or more predictors, a fever, or a refusal to bear weight is aspirated to exclude pus, and managed as septic arthritis until the fluid proves otherwise. The child whose clinical picture is septic regardless of the score is aspirated and treated without waiting for the count, because a frankly purulent aspirate is treated as sepsis. [1] [3]
Specific Subtypes & Scenarios
The classic transient synovitis is the well-looking child of three to eight years with an acute limp following a viral illness, and it is the scenario that the Kocher criteria are designed to triage. The child has a low-grade or absent fever, bears weight cautiously, has normal or mildly raised markers, and shows a small effusion on ultrasound, and the pathway is rest and review with resolution in one to two weeks. This is the bread-and-butter presentation, and the skill is the confidence to observe once sepsis is excluded. [6] [4]
The Kingella kingae mimic is the scenario that most often fools the clinician in the under-four. Kingella kingae septic arthritis presents with a deceptively mild, low-fever, modestly inflammatory picture that overlaps with transient synovitis, and it grows poorly on routine culture, so standard cultures are often negative. Yagupsky showed that the young child with a culture-negative hip effusion is not safely labelled transient synovitis, and the diagnosis is made by inoculating the synovial fluid into blood-culture bottles or by a polymerase chain reaction assay. The lesson is that a culture-negative effusion in the under-four is investigated for Kingella, not reassured. [8]
The recurrent irritable hip is the scenario that raises the suspicion of an alternative diagnosis. A second or third episode of a stiff, effused hip in the same child is not simply recurrent transient synovitis, because recurrence raises the possibility of juvenile idiopathic arthritis, of early Perthes disease presenting with intermittent symptoms, or of an underlying structural lesion. The recurrent hip warrants specialist review, repeat imaging, and a lower threshold for further investigation, because the benign diagnosis is one that resolves and does not return. [6] [9]
The non-resolving limp is the scenario that re-opens the differential. A limp attributed to transient synovitis that persists beyond two weeks is not a slow resolution but a different diagnosis, and the child is reassessed with repeat radiographs for early Perthes, consideration of magnetic resonance imaging for an occult stress fracture or osteomyelitis, and specialist referral. The persistence of the limp is the single most reliable discriminator between transient synovitis and its mimics, because the benign condition resolves on its own schedule. [7] [9]
Complications & Pitfalls
The complications of transient synovitis itself are few and benign, because the process resolves without sequelae in the overwhelming majority of children. A small proportion have a prolonged effusion or a residual stiffness that takes a few weeks longer to settle, and an even smaller proportion have a recurrence, but permanent joint damage, avascular necrosis, and growth disturbance are not features of the disease itself. The benign natural history is the reason the management is rest and review, not intervention. [6] [7]
The pitfall of the premature diagnosis is the commonest and the deadliest error, and it is the one the Kocher criteria exist to prevent. A febrile child who refuses to bear weight is labelled transient synovitis on the strength of a preceding viral illness, the markers are not measured, the joint is not aspirated, and the child returns with a destroyed septic hip. The safeguard is the discipline of scoring the probability of sepsis before reassuring anyone, of measuring the inflammatory markers, and of aspirating when the score is two or more predictors or the picture is septic. [1] [4]
The pitfall of the missed mimic is the error that costs the child the early diagnosis of Perthes or of a structural lesion. A child with early Perthes disease presents with a limp and a stiff hip that looks like transient synovitis on the first assessment, and the radiographs are normal in the early stage, so the diagnosis is missed until the limp persists and the radiographic changes declare themselves weeks later. The safeguard is the safety-net review at one to two weeks, because transient synovitis resolves and the mimics declare themselves by not resolving. [9] [6]
The pitfall of the reassured culture-negative effusion is the error that misses Kingella kingae in the under-four. A young child with a culture-negative effusion and a mild picture is labelled transient synovitis and discharged, when the fluid was simply not cultured in the blood-culture bottle or by polymerase chain reaction that would have revealed the organism. The safeguard is the awareness that Kingella produces a deceptively mild, low-inflammatory picture, and the discipline of requesting the extended culture and the assay in the young child with an effusion of uncertain cause. [8]
Prognosis & Disposition
The prognosis of transient synovitis is excellent, with full recovery and no sequelae in the overwhelming majority of children. The limp and the effusion resolve within one to two weeks, the hip returns to a full and painless range of movement, and the child returns to normal activity without restriction. The reassuring natural history is the reason the condition is managed conservatively, and it is the feature that the safety-net review confirms — the child who is better at one to two weeks had transient synovitis, and the child who is not is reinvestigated. [6] [7]
Recurrence occurs in a minority of children, and a single recurrence does not by itself indicate a different diagnosis, but it lowers the threshold for specialist review and repeat imaging. The historical concern that transient synovitis predisposes to Perthes disease has not been substantiated, and the consensus is that the apparent association reflects early Perthes misdiagnosed as transient synovitis, rather than a causal link. The family is counselled on the benign outlook, the expected timeline, and the features that demand review. [6] [9]
The disposition is shared between the primary care clinician or the emergency team, who own the recognition, the exclusion of sepsis, and the safety-net, and the paediatric or orthopaedic team, who own the review of the non-resolving or recurrent limp and the investigation of the mimics. The child is discharged with clear advice, reviewed at one to two weeks, and referred only if the limp persists or recurs. The family is the most important disposition partner, because the safety-net depends on their return if the features of sepsis or of a declaring mimic appear. [4] [9]
Special Populations
The young child under four is the population in whom the mimic is most easily missed, because Kingella kingae produces a deceptively mild picture that overlaps with transient synovitis. The under-four with a culture-negative effusion is investigated for Kingella by blood-culture-bottle inoculation and polymerase chain reaction, and a low-grade fever with modestly raised markers is treated with a high index of suspicion rather than reassurance. The age group lowers the threshold for aspiration and extended culture, because the missed organism is the missed diagnosis. [8]
Children in rural and remote settings are the population in whom the access to ultrasound, to rapid markers, and to specialist review shapes the safety of the management. A child managed conservatively in a remote setting depends on a reliable safety-net and on the capacity to return for review or escalation, and the threshold for transfer to a centre with imaging and orthopaedic support is lower when the follow-up cannot be guaranteed. The fellowship answer acknowledges that the safety of watchful waiting depends on the access to care, not on the biology of the disease. [4]
Indigenous and socioeconomically disadvantaged children are over-represented in the burden of late-presenting musculoskeletal infection, through the same pathways of crowding, limited primary care access, and delayed presentation that drive other infectious diseases. The recognition and the exclusion of sepsis that protect the hip depend on access to care, and the conservative management of transient synovitis is safe only when the safety-net is reliable. The fellowship answer frames the disease as one in which the social determinants shape the outcome as much as the organism or the inflammation. [9] [4]
Evidence, Guidelines & Regional Differences
The Kocher clinical prediction rule, derived in 1999 from a retrospective cohort at Boston Children's Hospital, is the taught framework for the probability of septic arthritis of the hip in children, and it is the tool that decides whether the irritable hip is observed or aspirated. The 2004 validation by Kocher, Mandiga, and colleagues confirmed the discriminant performance in a separate cohort, and the 2006 prospective study by Caird, Flynn, and colleagues added the C-reactive protein and provided the calibration caveat that the original probabilities may overestimate the true risk. These three papers frame the bedside decision. [1] [2] [3]
The modern evidence guides the investigations and the safety-netting. The 2014 comprehensive review by Nouri and colleagues synthesised the epidemiology, the mechanism, the investigations, and the management of transient synovitis, and the 2015 Swiss review by Dubois-Ferrière and colleagues asked which investigations are truly useful and concluded that ultrasound and the inflammatory markers are the core, with magnetic resonance imaging reserved for the atypical case. The 2022 review by Lipshaw and Walsh examined the current practice and the risk of misdiagnosis, emphasising the safety-net and the review of the persistent limp, and the 2024 study by Benoit and colleagues developed and validated a new diagnostic algorithm to refine the exclusion of sepsis. [6] [7] [4] [5]
The regional differences are modest in the framework but real in the access. The Kocher criteria and the conservative management apply globally, but the access to ultrasound, to rapid inflammatory markers, and to reliable follow-up shapes the safety of watchful waiting, and the threshold for transfer or aspiration is lower where the safety-net cannot be guaranteed. The Yang magnetic resonance imaging study and the Martinoli hip ultrasound review frame the imaging choices, and the NICE guidance for the United Kingdom frames the assessment of the limping child. The fellowship answer holds the framework constant and adapts the safety-net to the setting. [10] [11]
Exam Pearls
The fellowship answer turns on five numbers. The four Kocher predictors are a fever above thirty-eight point five, an inability to bear weight, an erythrocyte sedimentation rate above forty, and a white cell count above twelve thousand, with the Caird addition of a C-reactive protein above twenty milligrams per litre. Two or more predictors demand joint aspiration to exclude sepsis. The ultrasound shows a hip effusion, the synovial fluid is clear with a low cell count when transient synovitis is aspirated, and the condition resolves within one to two weeks with rest and a non-steroidal anti-inflammatory drug. [1] [3]
The examiner probes three traps. The first is the febrile limping child sent home as transient synovitis — the Kocher criteria and the inflammatory markers separate the two, and the preceding virus never closes the diagnosis. The second is the culture-negative effusion of the under-four — Kingella kingae is sought in the blood-culture bottle and by the polymerase chain reaction, and the mild picture is not reassuring. The third is the persistent limp — transient synovitis resolves in one to two weeks, and a limp that persists is Perthes, juvenile idiopathic arthritis, or another mimic, not a slow resolution. [8] [9]
The examiner rewards the candidate who frames the irritable hip around the exclusion of sepsis and the safety-net review. The diagnosis of transient synovitis is made only once sepsis has been excluded by the score and the markers, the management is rest and a non-steroidal anti-inflammatory drug, and the safety-net of a one-to-two-week review catches the mimics that declare themselves by not resolving. A candidate who shows this awareness demonstrates the clinical reasoning and the systems thinking that the fellowship demands. [4] [6]
The four Kocher predictors — FEWW
References
- [1]Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction algorithm. J Bone Joint Surg Am, 1999.PMID 10608376
- [2]Kocher MS, Mandiga R, Zurakowski D, Barnewolt C, Kasser JR. Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am, 2004.PMID 15292409
- [3]Caird MS, Flynn JM, Leung YL, Millman JE, D'Italia JG, Dormans JP. Factors distinguishing septic arthritis from transient synovitis of the hip in children. A prospective study. J Bone Joint Surg Am, 2006.PMID 16757758
- [4]Lipshaw MJ, Walsh PS. Transient synovitis of the hip: Current practice and risk of misdiagnosis. Am J Emerg Med, 2022.PMID 35994972
- [5]Benoit J, El Khalifi S, Saoudi C, et al. Transient synovitis of the hip: Development and validation of a new diagnostic algorithm. Acta Paediatr, 2024.PMID 38366676
- [6]Nouri A, Walmsley D, Pruszczynski B, Synder M. Transient synovitis of the hip: a comprehensive review. J Pediatr Orthop B, 2014.PMID 23812087
- [7]Dubois-Ferrière V, Belaieff W, Lascombes P, et al. Transient synovitis of the hip: which investigations are truly useful?. Swiss Med Wkly, 2015.PMID 26295841
- [8]Yagupsky P, Dubnov-Raz G, Gené A, et al. Differentiating Kingella kingae septic arthritis of the hip from transient synovitis in young children. J Pediatr, 2014.PMID 25217199
- [9]Ryan DD. Differentiating Transient Synovitis of the Hip from More Urgent Conditions. Pediatr Ann, 2016.PMID 27294495
- [10]Yang WJ, Im SA, Lim GY, et al. MR imaging of transient synovitis: differentiation from septic arthritis. Pediatr Radiol, 2006.PMID 17019590
- [11]Martinoli C, Garello I, Marchetti A, et al. Hip ultrasound. Eur J Radiol, 2012.PMID 21571471