Paeds · rural-remote-and-contextual-paediatrics
Implementing culturally safe Indigenous care in rural and remote services
Also known as Implementing culturally safe Indigenous care in rural and remote services · Implementing culturally safe Indigenous care in rural and remote services rural · Implementing culturally safe Indigenous care in rural and remote services remote · Implementing culturally safe Indigenous care in rural and remote services paediatric · Implementing culturally safe Indigenous care in rural and remote services fellowship
Fellowship guide to implementing culturally safe indigenous care in rural and remote services. Covers context-specific assessment, resource-aware pathways, escalation and retrieval, equity and cultural safety, documentation, and board-relevant practice for RACP, RCPCH/MRCPCH, ABP/ACGME and RCPSC examinations.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
An Aboriginal family travels 400 km for a paediatric clinic and leaves without understanding the plan after a rushed encounter with no Aboriginal health worker present. The fellowship task is to convert geography and resource limits into a safe, equitable plan rather than an excuse for delayed care. [1] [2] [3]
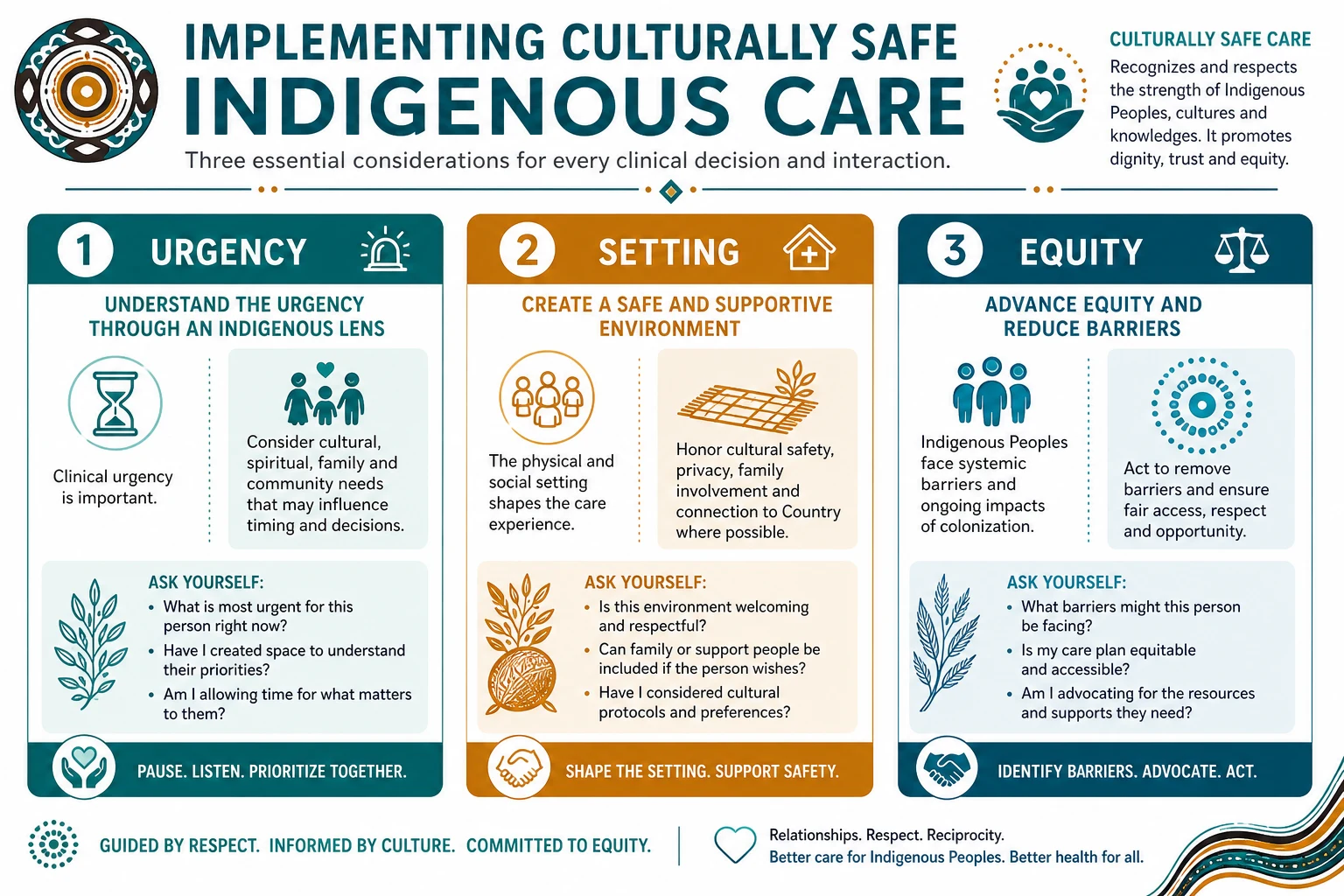
Culturally safe Indigenous child health care in rural and remote services is designed with community, privileges family voice, removes institutional racism, and measures safety by the experience of Aboriginal and Torres Strait Islander families. [1] [2] [3]
Rural, remote and contextual paediatrics is not second-class metropolitan care. It is a distinct craft: excellent basics, honest capability assessment, early escalation, cultural safety, and system design that stops blaming families for distance. [1] [2] [3] [4]
Classification
Classification is useful when it changes the stay-versus-go decision or the equity intervention. [1] [2] [3]
By urgency. Preventive/ambulatory; urgent same-day; emergency stabilisation; critical retrieval. [1] [2] [3]
By resource setting. Regional hospital with paediatric cover; small rural hospital; remote clinic; retrieval platform. [1] [2] [3]
By equity lens. Distance and transport; cultural safety; socioeconomic barrier; workforce gap. [1] [2] [3]
Restate the classification whenever physiology, weather, staffing or transport capacity changes. [1] [2] [3]
Epidemiology & Risk Factors
Rural and remote children experience higher rates of injury, some infectious diseases, developmental service gaps and delayed specialist access compared with metropolitan peers. Workforce shortages and transport barriers amplify every risk. [1] [2] [3]
Risk concentrates where poverty, racism, disability, newborn vulnerability and distance intersect. [1] [2] [3] [4]
Service design that ignores these gradients reproduces inequity even when individual clinicians work hard. [1] [2] [3]
Pathophysiology
The pathophysiology of harm is often systems physiology: delayed recognition, delayed antibiotics or airway support, hypothermia, hypoglycaemia, and information loss at handover. [1] [2] [3]
The mechanism of harm in implementing culturally safe indigenous care in rural and remote services is often delayed recognition plus delayed escalation rather than lack of a single drug. [1] [2] [3]
Distance multiplies every decision: what is safe to watch locally, what must move, and how packaging preserves physiology in transit. [1] [2] [3]
Trust, cultural safety and clear communication determine whether families engage early enough for prevention and safe follow-up. [1] [2] [3]
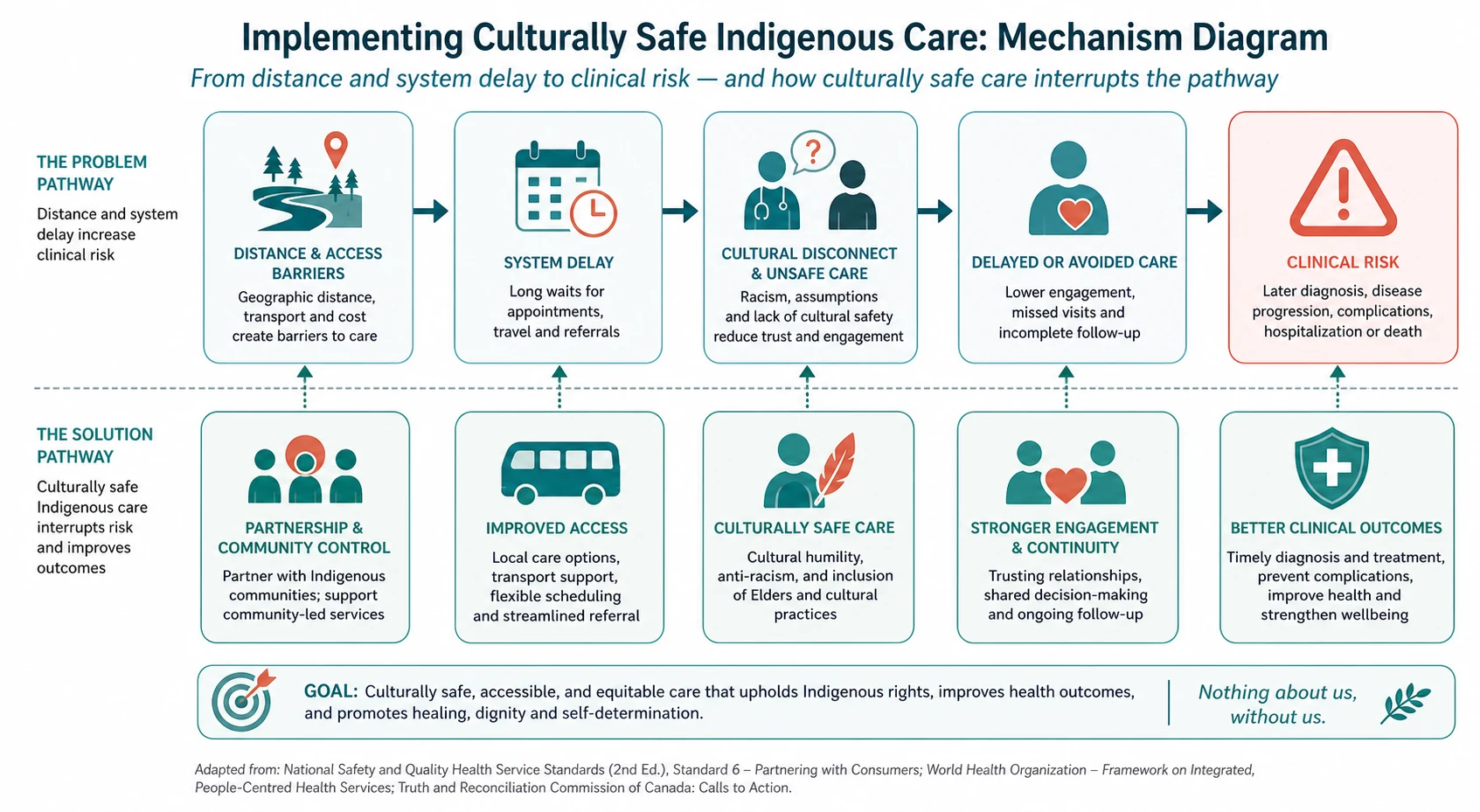
Understanding this pathway keeps the focus on time-critical basics and escalation rather than rare tertiary procedures that cannot be delivered on site. [1] [2] [3]
Clinical Presentation
Presentations range from the unexpected delivery and septic infant to chronic developmental need, mental-health crisis, child-protection concern and disaster displacement. [1] [2] [3]
Families may present late because of cost, weather, work on the land, distrust or prior racist encounters. Staff may present with skill-mix gaps and moral distress. [1] [2] [3] [4]
Red flags include physiological deterioration, inability to observe safely, cultural unsafety, and repeated failed access. [1] [2] [3]
Differential Diagnosis
Not every transfer request is necessary and not every local observation plan is safe. Differentiate true time-critical pathology from logistics-driven anxiety, and differentiate family non-attendance from system-created barriers. [1] [2] [3]
[1] [2] [3]Clinical & Bedside Assessment
Assess the child and the context together: ABCDE, weight, glucose, temperature, pain, plus staffing, diagnostics, transport time and family logistics. [1] [2] [3]
Use structured communication tools and ask who else needs to be in the room, including Aboriginal health workers or interpreters. [1] [2] [3] [4]
[1] [2] [3]Investigations
Order tests that change the immediate plan and can be actioned locally or during transfer. Do not delay oxygen, fluids, glucose or antibiotics for non-essential imaging. [1] [2] [3]
Point-of-care glucose, oxygen saturation and, where available, blood gas or lactate often outrank delayed laboratory panels. [1] [2] [3] [4]
Management — Resuscitation
Resuscitation follows standard paediatric algorithms with local equipment reality. Start airway support, oxygen, fluids and glucose while help is called. [1] [2] [3]
If cardiac arrest or peri-arrest occurs, run PALS/APLS-aligned care and prepare for prolonged resuscitation logistics including parental presence. [1] [2] [3]
Management — Definitive & Stepwise
-
Assess with a context-aware ABCDE and local capability scan; measure weight and use paediatric references. [1] [2] [3]
-
Call for senior, telehealth or retrieval help early with a structured SBAR handover. [1] [2] [3]
-
Stabilise airway, breathing, circulation, glucose, temperature and pain while the pathway is decided. [1] [2] [3]
-
Document thresholds, destination, family plan and follow-up; close the loop with the receiving or community team. [1] [2] [3]
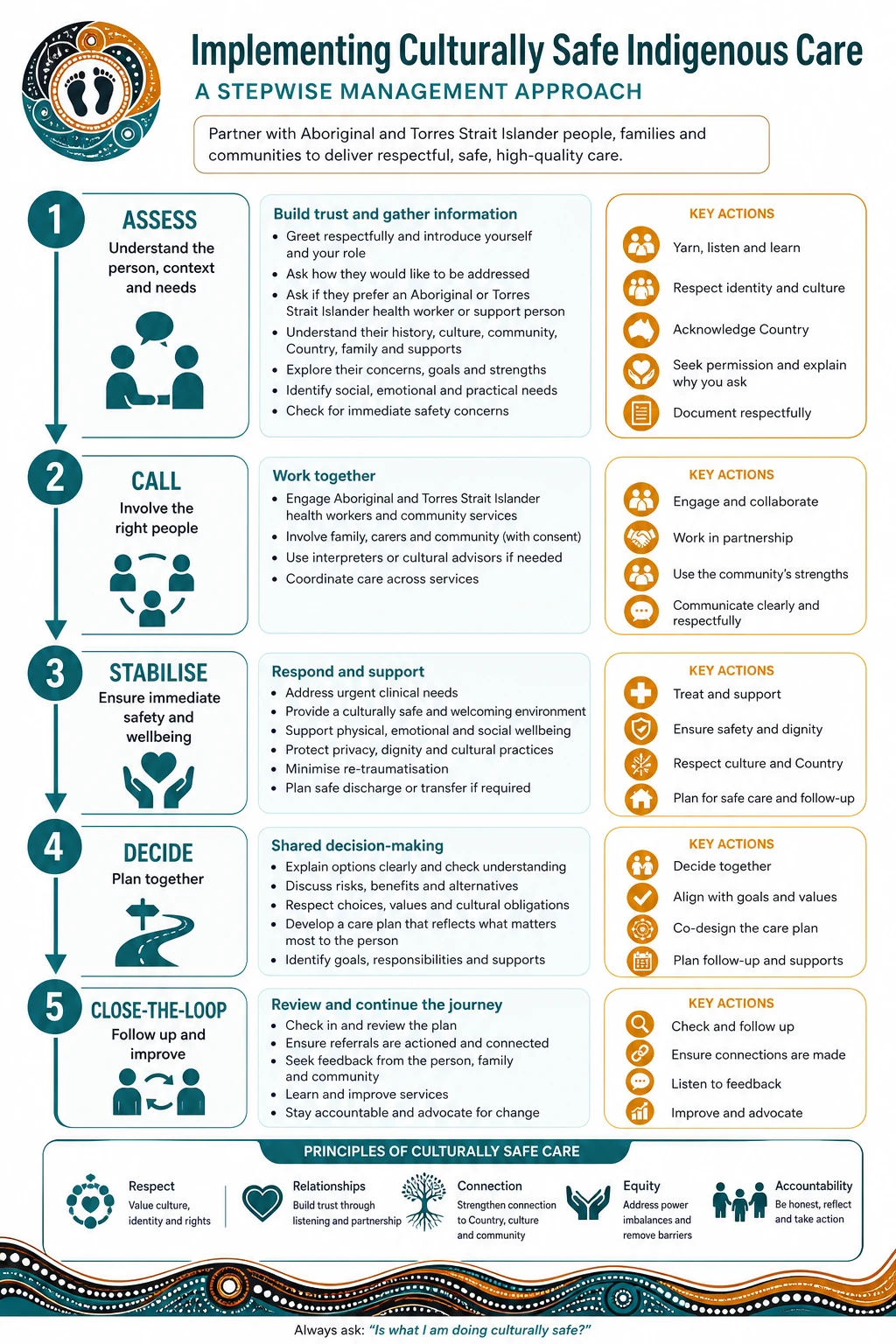
Assess
Context-aware ABCDE, weight, glucose and local capability scan.
Call
Senior, telehealth or retrieval help with structured SBAR.
Stabilise
Airway, breathing, circulation, temperature, pain and packaging.
Decide
Local care versus transfer with explicit thresholds.
Close the loop
Document, hand over, and confirm receiving or community follow-up.
Never let documentation wait until after transfer without a contemporaneous plan; write thresholds and destination clearly. [1] [2] [3] [4]
Specific Subtypes & Scenarios
Regional hospital night cover
One senior decision-maker, limited diagnostics, high value on early retrieval thresholds. [1] [2] [3]
Remote clinic without inpatient beds
Stabilise, package, and move; do not invent phantom ward capacity. [1] [2] [3]
Indigenous community context
Work with Aboriginal health workers and family decision structures from the first contact. [1] [2] [3]
Multi-child family logistics
Plan transport, sibling care and return travel as part of the clinical plan. [1] [2] [3]
Complications & Pitfalls
Pitfalls include late calls, adult dosing errors, hypothermia in transfers, missing glucose, excluding family and cultural supports, and unsafe dual relationships in small towns. [1] [2] [3]
High-yield examiner traps
Do not delay the call for help while attempting heroic care beyond local capability. Do not ignore glucose, weight and oxygen. Do not treat cultural safety as optional. Do not hand over without closed-loop confirmation.
Prognosis & Disposition
Prognosis improves when time-critical therapies start before wheels-up and when follow-up is explicit. Disposition may be local ward care, outbound retrieval, telehealth-supported observation, or community follow-up with hard safety-net instructions. [1] [2] [3] [4]
Special Populations
Neonates, Indigenous children, children with disability and technology dependence, refugee families and adolescents in small communities each need tailored pathways. Confidentiality is harder and more important in small towns. [1] [2] [3]
Evidence, Guidelines & Regional Differences
[1] [2] [3] [4]Retrieval literature, telehealth evaluations and rural workforce studies converge on early escalation, networked care and equity-focused design. [1] [2] [3] [4] [5]
Exam Pearls
- Call early; pride is not a airway adjunct. [1] [2]
- Weight, glucose and oxygen first. [1] [2]
- SBAR every handover across distance. [1] [2]
- Cultural safety is a clinical intervention. [1] [2]
- Design the system; stop blaming the family for geography. [1] [2]
RURAL safety frame
References
- [1]John JR et al. Codesign and knowledge translation of the Strength-based, Tiered, Accessible Resources and Supports (STARS) for Kids study to identify and support child development, parental mentalwell-being and family psychosocial needs: a mixed-methods research protocol. BMJ Paediatr Open, 2026.PMID 42097825
- [2]Yap JF et al. Investigation of an outbreak of typhoid fever in a rural district of East Malaysia, 2019. Western Pac Surveill Response J, 2025.PMID 41573761
- [3]Lau G et al. The Determinants to Effective Diagnosis and Management of Otitis Media in Aboriginal Children in Primary Care From the Perspective of Health Care Practitioners. Aust J Rural Health, 2026.PMID 41517926
- [4]Paull S et al. Being Heard, Being Valued, Being Understood-Aboriginal Community Perspectives on Adapting a Healthy Lifestyle Program for Boorloo/Perth, Western Australia: A Qualitative Study. Health Expect, 2026.PMID 42460790
- [5]Bhat M et al. Prevalence of Cannabis Use Among Indigenous Populations - A Systematic Review. Subst Use Misuse, 2026.PMID 42190074
- [6]Franks PW et al. The Lancet Commission on precision health: equitable, data-driven health outcomes for all. Lancet, 2026.PMID 42184810
- [7]Singh M et al. Four years of experience of telemedicine for paediatric care in three Punjab hospitals, North India: achievements and lessons. Postgrad Med J, 2010.PMID 20870650
- [8]Smith AC et al. Clinical services and professional support: a review of mobile telepaediatric services in Queensland. Stud Health Technol Inform, 2010.PMID 21191168