Phys · cardiovascular
Anticoagulation and Antiplatelet Therapy (Physician-Managed)
Also known as anticoagulation · antiplatelet therapy · warfarin · DOAC · apixaban · rivaroxaban · dabigatran · edoxaban · DAPT · dual antiplatelet therapy · anticoagulant reversal · bridging anticoagulation · HIT
Consultant-physician-depth guide to anticoagulant and antiplatelet prescribing — warfarin and the DOACs with doses and renal thresholds, VTE duration, mechanical valves, reversal agents, perioperative management, HIT, cancer-associated VTE, DAPT and triple therapy — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Anticoagulation and Antiplatelet Therapy (Physician-Managed)

The answer first
Antithrombotic prescribing is risk arbitration, not drug selection — every decision trades a thrombotic risk you can quantify against a bleeding risk you can modify, and the examiner wants to hear you do the arithmetic aloud. Four rules carry almost every DWE question and every consultant viva [9]:
- DOACs are the default for atrial fibrillation and for VTE. Across RE-LY, ROCKET AF, ARISTOTLE and ENGAGE AF, the direct oral anticoagulants were non-inferior or superior to warfarin for stroke prevention with roughly half the intracranial haemorrhage — warfarin survives only where DOACs have no evidence or proven harm [1] [2] [3] [4].
- Warfarin still owns three territories: mechanical heart valves (DOACs are contraindicated — RE-ALIGN), moderate-to-severe rheumatic mitral stenosis, and antiphospholipid syndrome; plus patients whose renal failure puts them below DOAC thresholds [5].
- Reversal and perioperative management are protocols, not improvisations. Know the antidotes (vitamin K plus PCC, idarucizumab, andexanet alfa, protamine), know that bridging is dead for most AF patients (BRIDGE), and know that device surgery is done ON warfarin (BRUISE CONTROL) [15] [16] [18] [19].
- Antiplatelets are secondary-prevention drugs. Aspirin has no default role in primary prevention (ASPREE, ASCEND, ARRIVE); DAPT duration after stenting is a bleeding-versus-thrombosis decision; and after PCI in an anticoagulated AF patient, the winning regimen is the shortest one — triple therapy measured in days, not months (AUGUSTUS, PIONEER AF-PCI) [26] [29].
The agents and their targets
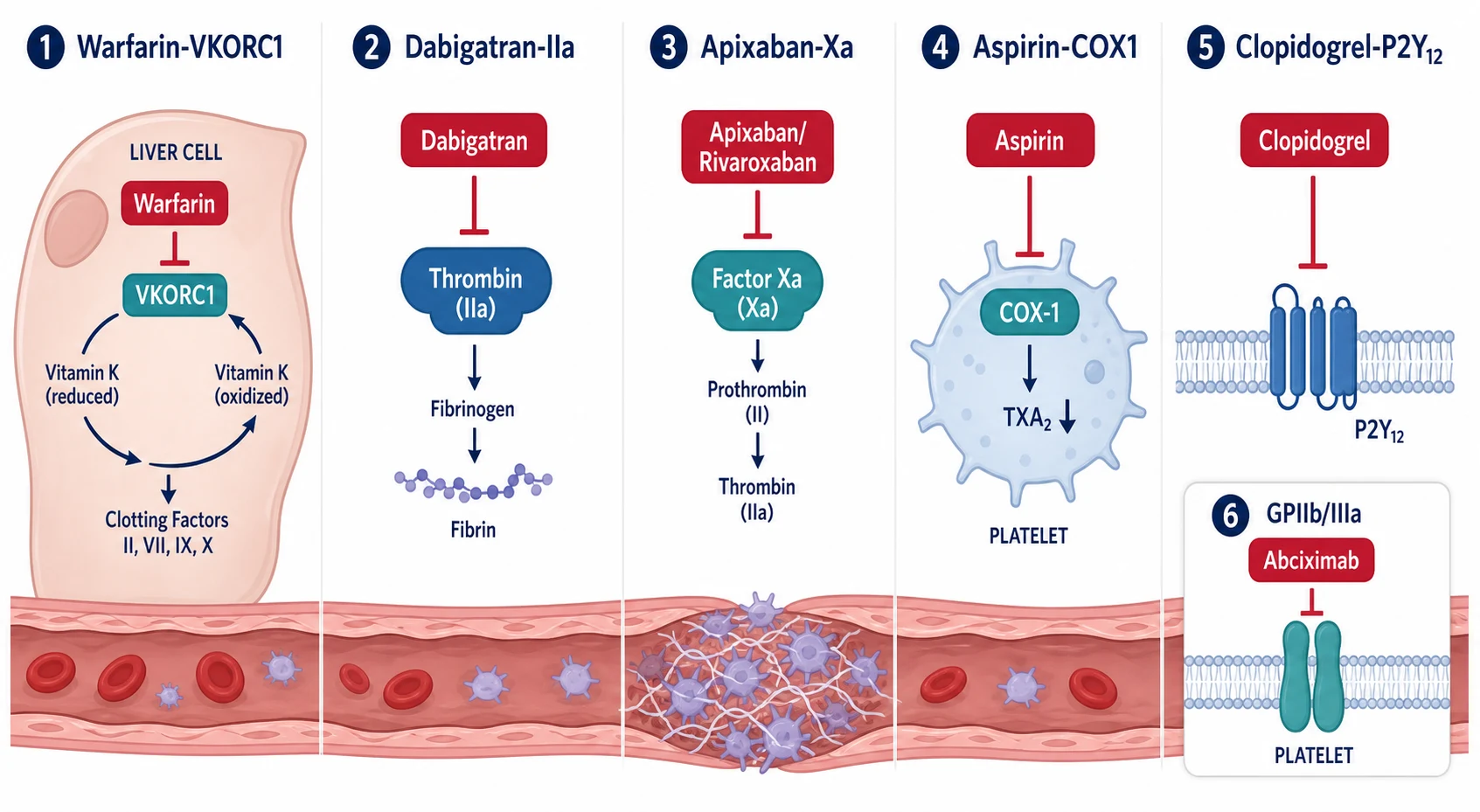
Every antithrombotic question reduces to two pathways: the coagulation cascade (target of warfarin, heparins and DOACs) and platelet activation (target of aspirin, P2Y12 inhibitors and GPIIb/IIIa antagonists). Arterial thrombosis — stroke, myocardial infarction, stent thrombosis — is platelet-driven, which is why antiplatelets dominate there; venous thrombosis and AF-related cardioembolism are fibrin-driven, which is why anticoagulants dominate there. The crossover mistake — aspirin for AF stroke prevention, or warfarin alone for a stent — fails both the biology and the exam [21] [34].
Warfarin — the drug with a century of baggage
Warfarin inhibits VKORC1, blocking regeneration of reduced vitamin K and so depleting functional factors II, VII, IX and X (plus proteins C and S). Three properties explain its entire clinical behaviour [17]:
- Narrow therapeutic window, monitored by INR. Target 2.0–3.0 for AF, VTE and most mechanical aortic valves; some mechanical mitral valves target 2.5–3.5. Quality is measured as time in therapeutic range — below about 65–70% TTR, the case for a DOAC (if the indication permits) strengthens.
- Interactions everywhere. Amiodarone, macrolides, azole antifungals, sulfonamides and metronidazole all raise the INR; rifampicin, carbamazepine and St John's Wort lower it. The exam answer is not to memorise forty drugs but to say: any new prescription or antibiotic course in a warfarin patient triggers an INR check within 3–5 days [17].
- Diet is about consistency, not prohibition. Vitamin K–rich foods (leafy greens) antagonise warfarin; the advice is a stable intake, not avoidance, plus honest limits on alcohol [17].
Warfarin's slow offset (days, not hours) is why acute VTE treatment starts with a parenteral overlap — and why, in HIT, warfarin alone early can precipitate limb gangrene: proteins C and S fall before factor II does, briefly worsening thrombosis [32].
The DOACs — one target each, no monitoring, renal rules
The four DOACs share three features that changed practice: fixed dosing without routine monitoring, rapid onset and offset, and renal clearance that must be respected. The pivotal AF trials are the spine of the evidence [1] [2] [3] [4]:
| Agent | Target | AF dose (VTE dose) | Dose reduction | Renal rule (CrCl, Cockcroft–Gault) | Trial |
|---|---|---|---|---|---|
| Apixaban | Factor Xa | 5 mg twice daily (10 mg bd ×7 days, then 5 mg bd) | 2.5 mg bd if ≥2 of: age 80+, weight ≤60 kg, creatinine ≥133 µmol/L | Usable down to CrCl 15–25; best evidence in advanced CKD among DOACs [3] | ARISTOTLE; AMPLIFY for VTE [7] |
| Rivaroxaban | Factor Xa | 20 mg once daily with food (15 mg bd ×21 days, then 20 mg od) | 15 mg od if CrCl 15–49 | Avoid below CrCl 15; take with food for absorption [2] | ROCKET AF; EINSTEIN for VTE [6] |
| Dabigatran | Thrombin (IIa) | 150 mg twice daily | 110 mg bd in elderly or high bleeding risk | ~80% renally cleared — avoid when CrCl below 30; the wrong choice in renal impairment [1] | RE-LY |
| Edoxaban | Factor Xa | 60 mg once daily | 30 mg od if CrCl 15–50, weight ≤60 kg, or strong P-gp inhibitors | Do NOT use if CrCl above 95 (reduced efficacy signal in ENGAGE AF) [4] | ENGAGE AF; Hokusai-VTE (needs 5 days of parenteral lead-in) [8] |
Indications — who gets anticoagulated
Atrial fibrillation. Stroke prevention in AF is risk-stratified prescribing: CHA₂DS₂-VASc estimates annual stroke risk, HAS-BLED flags modifiable bleeding factors, and a DOAC is the default agent unless a warfarin-only indication exists [34] [35]. The full discussion — thresholds, rhythm versus rate, valvular versus non-valvular — lives in the atrial fibrillation topic; what this topic owns is the drug logic above and everything below.
Venous thromboembolism. The EINSTEIN, AMPLIFY and Hokusai-VTE trials established DOACs as first-line VTE treatment, non-inferior to the traditional heparin-to-warfarin bridge with less major bleeding [6] [7] [8]. Apixaban and rivaroxaban are started directly at treatment intensity (apixaban 10 mg twice daily for 7 days then 5 mg twice daily; rivaroxaban 15 mg twice daily for 21 days then 20 mg daily); edoxaban and dabigatran require at least 5 days of parenteral anticoagulation first [7] [8]. Diagnostic strategy, Wells scoring and thrombolysis decisions are the pulmonary embolism and thrombophilia/VTE topics' business — the duration question below is yours.
Mechanical valves — warfarin, full stop. RE-ALIGN randomised mechanical valve patients to dabigatran versus warfarin and was stopped early: dabigatran produced more thromboembolism AND more bleeding — a rare double loss that killed the hypothesis for the whole class [5]. Mechanical valves need warfarin with valve-specific INR targets (2.0–3.0 for most modern bileaflet aortic valves, 2.5–3.5 for mitral and higher-risk valves) plus low-dose aspirin in some practices. The same warfarin-only logic extends to moderate-to-severe rheumatic mitral stenosis with AF and to antiphospholipid syndrome (especially triple-positive or arterial events), where DOACs underperform [5].
VTE duration — the 3-month fork
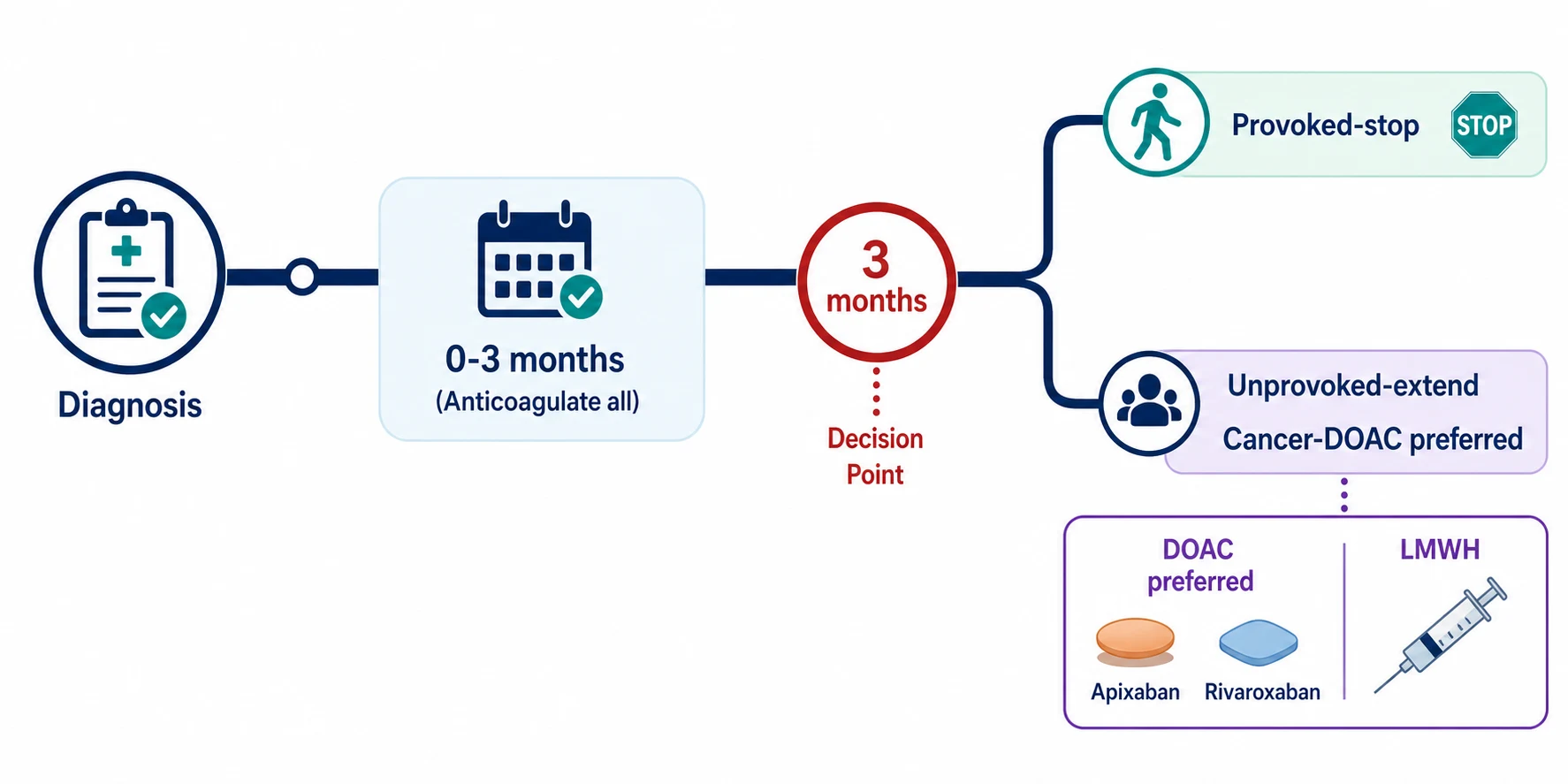
Duration is where VTE management earns its physician stripes. The CHEST framework (2016, updated 2021) divides treatment into the initial 3 months — during which everyone is anticoagulated — and then a decision at the 3-month fork driven by why the clot happened [9] [10]:
| VTE category | Recurrence risk off treatment | Recommended duration | Reasoning |
|---|---|---|---|
| Provoked by a major transient factor (surgery, immobilisation, oestrogen therapy) | Low — about 1% per year | 3 months, then stop [9] | The provoking factor has resolved; extended therapy buys little and costs bleeding |
| Provoked by a persistent factor (active cancer, antiphospholipid syndrome) | High while factor persists | Extended, reviewed periodically [10] | The driver is still present |
| Unprovoked (first event) | About 10% in year one, 30% by 5 years | Extended if bleeding risk is low-moderate, with annual review [9] | Recurrence risk outweighs bleeding for most; men and those with PE (rather than distal DVT) recur more |
| Distal DVT (calf), ultrasound-surveilled | Low if not extending | Surveillance or 3 months if treated [10] | Isolated calf DVT without severe symptoms can be watched rather than anticoagulated |
For extended therapy, full-dose is not the only option. AMPLIFY-EXT showed apixaban 2.5 mg twice daily prevents recurrence as well as 5 mg with less bleeding, and EINSTEIN CHOICE showed rivaroxaban 10 mg daily (and 20 mg) beat aspirin for extended prophylaxis without excess major bleeding — aspirin has no role in VTE secondary prevention [11] [12].
Occult malignancy in unprovoked VTE. An unprovoked clot in a patient over 50 carries a real — but modest — risk of occult cancer, and the physician's response is targeted, not a reflex total-body CT. The defensible workup: thorough history (weight loss, change in bowel habit, haemoptysis, night sweats), full examination including breast, prostate and rectal, FBC, chemistry, calcium, urinalysis, chest imaging, and completion of age-appropriate screening programmes. Extensive screening beyond that finds little and harms through incidentalomas [9].
Antiplatelet therapy — aspirin and the P2Y12 family
Aspirin irreversibly acetylates platelet COX-1, abolishing thromboxane A₂ production for the platelet's 7–10 day lifespan. Its modern role is precise: secondary prevention of established atherosclerotic disease (prior MI, ischaemic stroke, symptomatic PAD) and partner duty in DAPT — and almost nothing else [21].
Primary prevention is dead. Three 2018 trials closed the case. ARRIVE (moderate-risk adults) found no reduction in vascular events with aspirin. ASCEND (diabetes) found a small vascular benefit exactly offset by major bleeding. ASPREE (healthy people over 70) found no benefit in disability-free survival or cardiovascular events, more major haemorrhage, and a troubling all-cause mortality signal — so routine aspirin in healthy elderly patients is now an exam error, not an exam answer [26] [25] [27].
The P2Y12 inhibitors block the platelet ADP receptor that amplifies activation [22]:
| Agent | Pharmacology | Key evidence | What the exam tests |
|---|---|---|---|
| Clopidogrel | Prodrug, CYP2C19 activation; irreversible | CURE: aspirin + clopidogrel after NSTE-ACS reduced the composite of death/MI/stroke [21] | CYP2C19 loss-of-function variants make some patients non-responders; the default partner in DAPT |
| Prasugrel | Prodrug, more potent and consistent than clopidogrel; irreversible | TRITON-TIMI 38: fewer ischaemic events than clopidogrel in PCI'd ACS, more major bleeding [22] | Contraindicated with prior stroke/TIA (net harm); caution in elderly and low body weight |
| Ticagrelor | Direct-acting, reversible, no metabolic activation | PLATO: superior to clopidogrel including mortality, with more non-CABG bleeding [23] | Causes transient dyspnoea (adenosine-mediated) and bradyarrhythmias — expected, not always a reason to stop |
DAPT duration after PCI. The default after ACS with stenting is 12 months of aspirin plus a P2Y12 inhibitor — the era defined by CURE and confirmed through the drug-eluting stent trials [21]. The DAPT trial then showed that extending to 30 months reduces stent thrombosis and MI at the cost of more bleeding and a mortality signal — so duration is individualised: shorter (3–6 months) when bleeding risk dominates, longer when ischaemic risk dominates and bleeding has been clean [24].
Reversal — the antidotes, cold
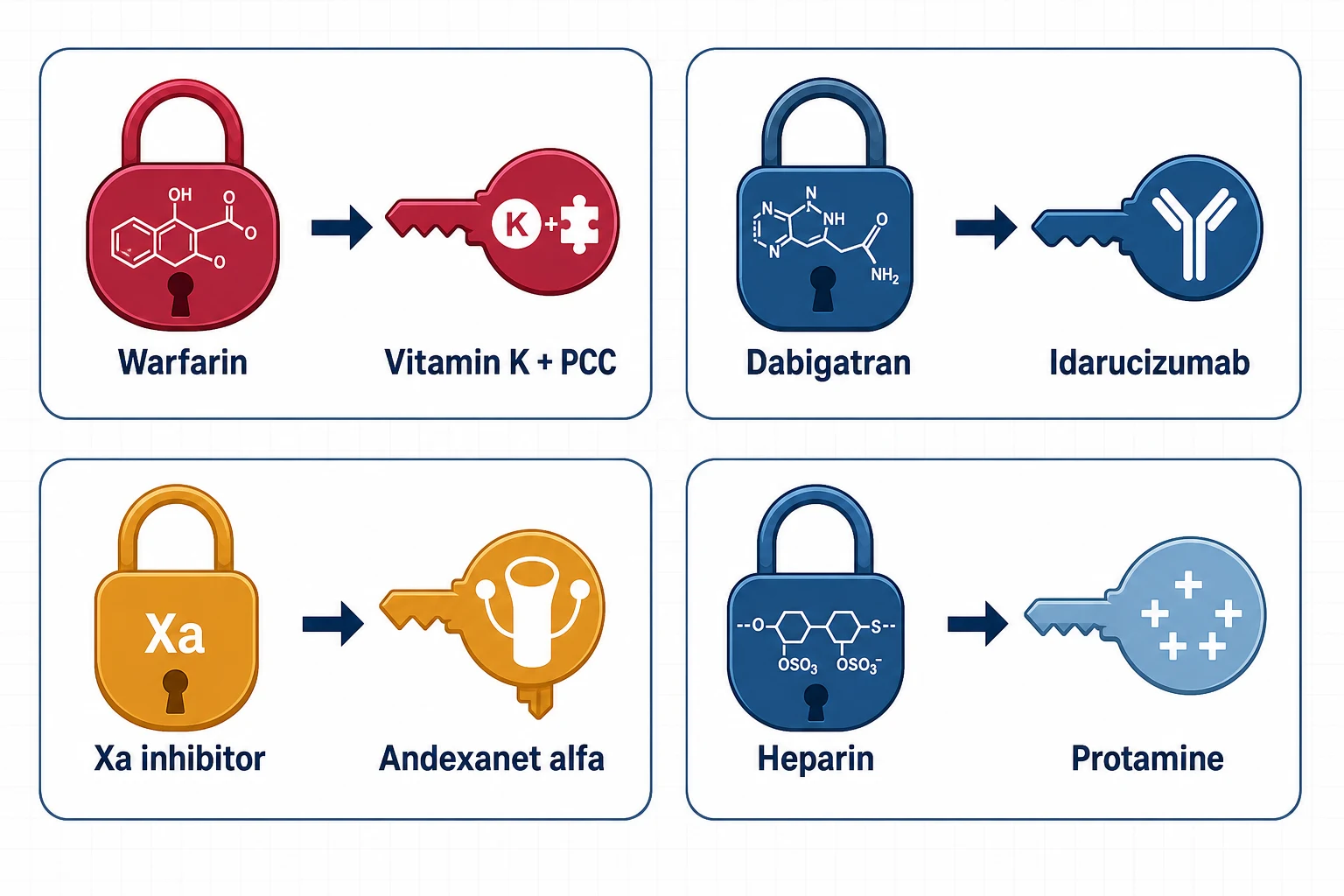
Reversal is for life-threatening bleeding, critical-site bleeding (intracranial, pericardial, retroperitoneal), or urgent surgery that cannot wait — not for a high INR, a nosebleed, or reassurance. The first moves are agent-agnostic: stop the drug, establish when the last dose was taken, check renal function (it determines how long the drug will linger), apply local haemostatic measures, and resuscitate. Then match the antidote [15] [16]:
| Agent | Reversal | Evidence anchor | Notes that earn marks |
|---|---|---|---|
| Warfarin | Vitamin K 5–10 mg IV (slow) PLUS 4-factor PCC (dosed to INR); FFP only if PCC unavailable | 4F-PCC corrected INR faster than plasma with similar haemostasis in major bleeding [17] | Vitamin K alone works in 6–24 hours — too slow alone for major bleeding; PCC works in minutes but wears off, which is why you give both |
| Dabigatran | Idarucizumab 5 g IV (two 2.5 g boluses) | RE-VERSE AD: immediate, complete, sustained reversal; haemostasis restored in most within hours [15] | Dabigatran is dialysable if idarucizumab unavailable and renal failure prolongs exposure |
| Apixaban / rivaroxaban / edoxaban (Xa) | Andexanet alfa (IV bolus then 2-hour infusion, dose by agent and time since last dose); 4-factor PCC as pragmatic alternative | ANNEXA-4: 82% achieved excellent or good haemostasis at 12 hours; thrombotic events in about 10% [16] | Andexanet's prothrombotic signal is real — reserve for the genuinely life-threatening |
| Unfractionated heparin | Protamine sulfate, titrated to dose and time since heparin | Long-standing pharmacology; neutralises UFH fully, LMWH only partially (about 60%) | Protamine itself is an anticoagulant in overdose and can cause hypotension/anaphylaxis — give slowly |
Resuming after a major bleed is the mark of a physician answer. AF stroke risk and VTE recurrence risk persist after haemostasis. The framework: treat the bleeding source definitively (endoscopic therapy, surgery, embolisation), wait until haemostasis is secure — typically days to two weeks for GI bleeding, longer after intracranial haemorrhage with neurology input — then restart, and document the shared decision with the patient [10].
Perioperative management — protocols, not improvisation
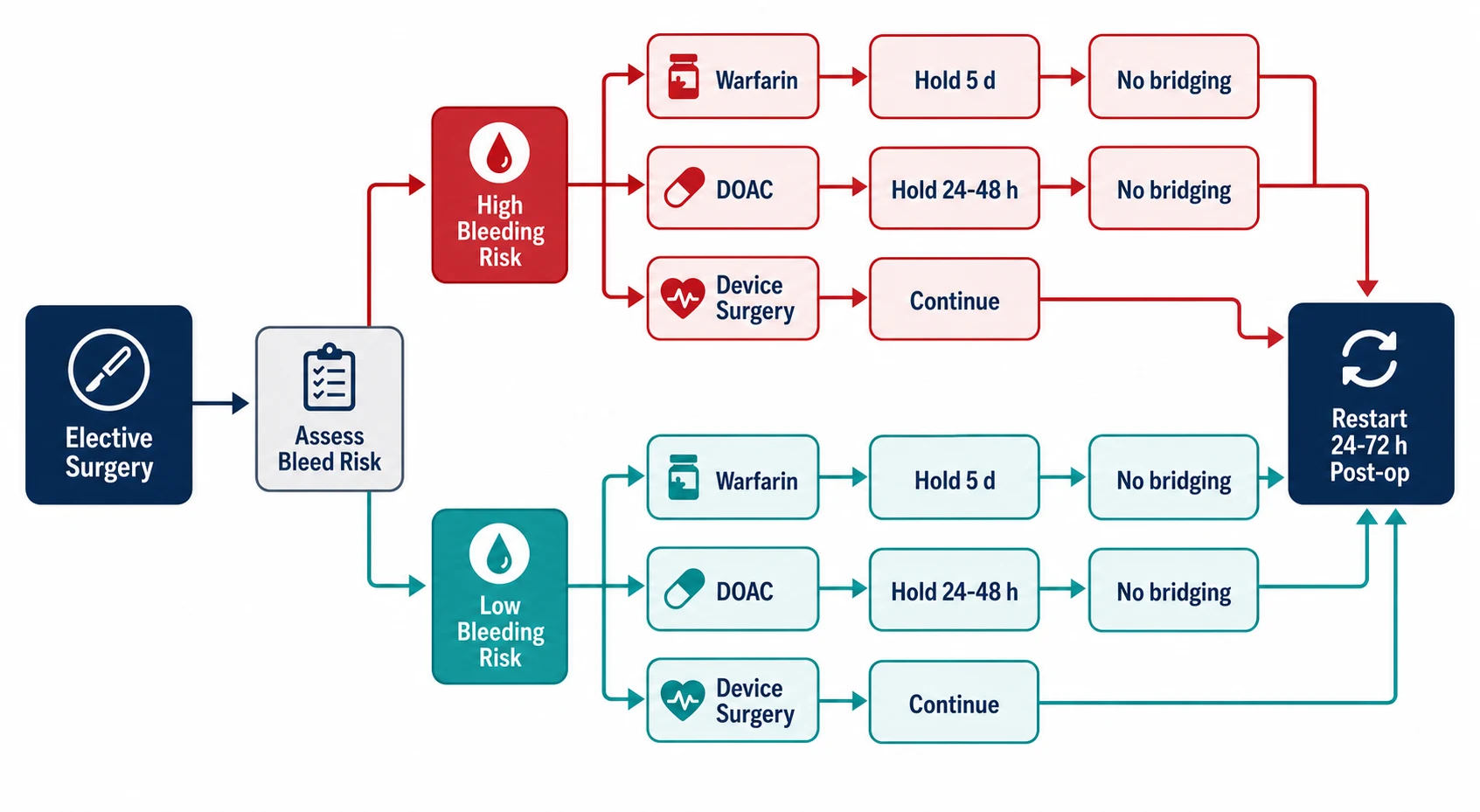
The elective-surgery questions collapse into four facts, each backed by a named trial [18] [19] [20]:
The perioperative numbers that answer most DWE items
Bridging is dead for most AF patients. BRIDGE randomised warfarin-treated AF patients undergoing procedures to LMWH bridging versus placebo interruption: no difference in thromboembolism, significantly more major bleeding with bridging [18]. The residual candidates for bridging are the exceptions the examiner wants named: mechanical mitral valves, stroke/TIA or VTE within the last 3 months, and very high-risk mechanical valve anatomy — decisions made with haematology, not habit [18].
Device surgery is the mirror image. BRUISE CONTROL showed that pacemaker/ICD surgery on continued warfarin caused markedly less pocket haematoma than interrupting warfarin and bridging with heparin — the bridging, not the warfarin, was the bleeding problem [19]. Most DOAC device cases are done with brief interruption or continuation depending on operator and bleeding risk.
DOAC interruption is clock arithmetic. PAUSE validated the simple schedule: skip doses to create about 1 day (low-bleed-risk) or 2 days (high-bleed-risk) between last dose and procedure — longer for dabigatran in renal impairment — with no bridging and low measured residual drug levels; neuraxial anaesthesia and very high-bleed-risk surgery extend interruption to about 48–72 hours [20].
The perioperative anticoagulation consult
Identify the agent and indication
Drug, dose, last dose time; why they are on it (AF stroke risk, VTE recency, mechanical valve) — the indication sets the thrombotic stakes
Grade the procedure's bleeding risk
Low (minor skin, dental, cataract, endoscopy) versus high (major surgery, neuraxial, resection) — this sets hold duration
Set the hold
Warfarin 5 days with day-of INR; DOAC 24–48 h by bleed risk and CrCl; NO bridging for AF; mechanical valve is the bridging exception — involve haematology
Plan the restart
Prophylactic-dose heparin or nothing until haemostasis is secure, then full anticoagulation at 24 h (low bleed risk) to 48–72 h (high); write it in the chart, not in your head
Communicate in writing
Exact last-dose date and restart date for the patient, the surgeon and the anaesthetist — most perioperative anticoagulation harm is a communication failure
Urgent surgery on a DOAC flips to the reversal logic above: delay 12–24 hours if the surgery allows (renal function dictates drug persistence), consider antidote for truly emergent high-bleed-risk surgery (idarucizumab for dabigatran; andexanet or PCC for Xa agents) [15] [16].
Heparin-induced thrombocytopenia — the thrombosis that looks like a side effect
HIT is an immune catastrophe: IgG against platelet factor 4–heparin complexes activates platelets, producing thrombosis with a falling platelet count — classically a 50% platelet fall beginning 5–10 days into heparin exposure (within 24 hours if prior exposure in the last ~100 days). Half the patients present WITH a thrombotic event; the platelet count often never reaches the classic "thrombocytopenia" ranges [31].
Score with the 4Ts before touching the lab: Thrombocytopenia magnitude, Timing, Thrombosis, and oTher causes. A low score (0–3) effectively excludes HIT; intermediate/high scores mandate action before confirmatory testing — immunoassay (sensitive, over-called) then functional assay (serotonin release, specific) [31] [32].
Suspected HIT — act before the confirmatory result
Stop ALL heparin
Including LMWH (cross-reacts), line flushes, heparin-coated catheters — every molecule
Start a non-heparin anticoagulant at treatment dose
Argatroban (liver-cleared — the ICU/renal failure choice), fondaparinux, or a DOAC; do not wait for the serotonin-release assay
Never warfarin alone, never platelets
Warfarin alone drops protein C first → limb gangrene; prophylactic platelets add thrombotic substrate. Warfarin only after platelets recover above 150, overlapped ≥5 days with the non-heparin agent
Image for silent thrombosis
Bilateral leg ultrasounds even without symptoms — subclinical DVT is common and changes management
Document and flag
HIT in the allergy record; heparin re-exposure is constrained (cardiac surgery needs specialist planning)
Cancer-associated VTE — the DOAC era
Cancer shifts every part of the VTE calculus: higher recurrence, higher bleeding, drug interactions, thrombocytopenia from chemotherapy, and a treatment duration that runs while the cancer is active. For two decades the answer was LMWH (dalteparin) over warfarin; the modern trials have moved the default to DOACs [13] [14].
| Trial | Comparison | Result | Caveat |
|---|---|---|---|
| Caravaggio (2020) | Apixaban vs dalteparin in cancer-associated VTE | Non-inferior for recurrence, no increase in major bleeding | The cleanest result — apixaban is the usual first choice [13] |
| Hokusai VTE Cancer (2018) | Edoxaban (after LMWH lead-in) vs dalteparin | Non-inferior composite of recurrence + major bleeding | More major bleeding with edoxaban, driven by GI cancers — avoid in unresected GI luminal tumours [14] |
The prescribing synthesis: a DOAC (usually apixaban) for most cancer-associated VTE; LMWH retained for GI/GU luminal tumours with mucosal bleeding, significant drug–drug interactions with chemotherapy, severe thrombocytopenia (below about 50 × 10⁹/L — use half-dose or hold strategies), or malabsorption concerns; warfarin only when neither is feasible. Duration is at least 6 months and continues while cancer is active or treatment ongoing, reassessed periodically [10] [13].
Special populations — where physicians earn the fee
The elderly patient who falls. The falls objection is the most common reason anticoagulation is wrongly withheld, and the arithmetic refutes it. Man-Son-Hing's classic analysis found an AF patient would need to fall hundreds of times per year before the subdural haemorrhage risk from falls offset the stroke prevention benefit of warfarin — and DOACs, with their halved intracranial bleeding, only widen the margin [33]. The consultant response is not "stop the anticoagulant" but "treat the falls": review sedation and orthostatic drugs, correct vision, manage postural hypotension, strength-and-balance referral, and choose the agent with the best intracranial safety profile (apixaban) [3] [33]. The falls and syncope topic owns the falls workup; this topic owns the refusal to let falls veto stroke prevention.
Chronic kidney disease. Renal function is the DOAC gatekeeper, measured as creatinine clearance by Cockcroft–Gault (the trial metric), not eGFR. The practical ladder: apixaban retains evidence furthest down the GFR range (usable to CrCl 15–25); rivaroxaban and edoxaban need dose reduction in the 15–50 band; dabigatran — 80% renally cleared — is avoided once CrCl drops below 30; below the DOAC floor (CrCl under 15, dialysis), warfarin remains the default while acknowledging its own vascular-calcification concerns and the thin evidence in dialysis patients [2] [3] [4]. Whatever the agent, renal function is rechecked at least annually, more often in the elderly and the fluctuating.
The multimorbidity patient. Frailty, polypharmacy, intermittent NSAID use, antiplatelet co-prescription, and recurrent hospitalisation each multiply bleeding risk. The physician moves: strip interacting drugs, avoid "triple" combinations without a current indication, add PPI gastroprotection when combined antithrombotic therapy is genuinely required, choose the DOAC with the mildest bleeding profile, dose-reduce by the label criteria (not by instinct), and schedule the review — bleeding risk is re-scored, not assumed static [3] [35].
Pregnancy, briefly. Warfarin is embryopathic (first-trimester exposure) and DOACs are contraindicated — anticoagulation in pregnancy is LMWH, and the detailed management belongs to obstetric medicine. The physician's duty is the pre-pregnancy conversation for every woman of childbearing potential on long-term anticoagulation [9].
Triple therapy after PCI in AF — shortest wins
The patient with AF who gets a stent concentrates three risks — stroke, stent thrombosis, and bleeding — into one prescription. Triple therapy (anticoagulant + aspirin + P2Y12 inhibitor) suppresses the first two and maximises the third. Three trials rebuilt the strategy around double therapy with the earliest possible aspirin exit [28] [29] [30]:
| Trial | Design | Finding | What it changed |
|---|---|---|---|
| PIONEER AF-PCI (2016) | Rivaroxaban 15 mg + P2Y12 vs triple therapy with warfarin | Double therapy bled substantially less with similar efficacy | First proof that less antithrombotic intensity is safer [28] |
| RE-DUAL (2017) | Dabigatran + P2Y12 vs warfarin triple | Dual therapy cut bleeding, non-inferior for thromboembolism | Confirmed the class effect [30] |
| AUGUSTUS (2019) | 2×2: apixaban vs warfarin, aspirin vs placebo, after ACS/PCI in AF | Apixaban bled less than warfarin; aspirin roughly doubled bleeding without reducing ischaemic events | The cleanest indictment of routine prolonged aspirin [29] |
The working protocol: triple therapy only for the periprocedural window (up to about a week, rarely 30 days in very high ischaemic risk), then an anticoagulant plus a single P2Y12 inhibitor (clopidogrel — not prasugrel or ticagrelor, which were minimally studied here) to 12 months, then the anticoagulant alone [29] [30]. The exam trap is reflexly prescribing a year of triple therapy "because he has a stent AND AF".
The DCE long case — anticoagulation in multimorbidity
The archetypal long case is the 82-year-old with AF, CKD (CrCl 38), recurrent falls, a GI bleed last year, and apixaban stopped by a well-meaning locum. The examiner's interest is never the drug list — it is the reasoning chain: quantify the stroke risk (CHA₂DS₂-VASc), quantify and modify the bleeding risk (HAS-BLED points you to fixable items — uncontrolled BP, interacting drugs, labile behaviour), choose the agent on renal and bleeding pharmacology, then defend the choice against each objection the family raises [34] [35].
The viva answer that distinguishes a physician: "The falls do not change the answer — the stroke risk dominates the arithmetic — but they change the work. I address the falls themselves, I pick the anticoagulant with the lowest intracranial bleeding rate, I check renal function on schedule, and I revisit the decision after every bleed rather than letting one event silently retire the drug" [33]. The second distinguishing move is anticipating the scenarios: what happens to this regimen at surgery, at a future bleed, if the creatinine worsens, if he develops cancer.
Short-case angles. The AF examination (irregularly irregular pulse, rate control, signs of valve disease, thyroid status, heart failure) ends in an anticoagulation discussion — so examine with the decision in mind: a mechanical valve click or a mitral stenosis murmur changes the drug answer completely. The pre-procedure short case tests the perioperative protocol above. The bleeding short case tests reversal and resumption logic [5] [18].
Exam traps, collected
References
- [1]Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation N Engl J Med, 2009.PMID 19717844
- [2]Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation N Engl J Med, 2011.PMID 21830957
- [3]Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation N Engl J Med, 2011.PMID 21870978
- [4]Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation N Engl J Med, 2013.PMID 24251359
- [5]Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves N Engl J Med, 2013.PMID 23991661
- [6]EINSTEIN Investigators, Bauersachs R, Berkowitz SD, et al. Oral rivaroxaban for symptomatic venous thromboembolism N Engl J Med, 2010.PMID 21128814
- [7]Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism N Engl J Med, 2013.PMID 23808982
- [8]Hokusai-VTE Investigators, Büller HR, Décousus H, et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism N Engl J Med, 2013.PMID 23991658
- [9]Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report Chest, 2016.PMID 26867832
- [10]Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report Chest, 2021.PMID 34352278
- [11]Agnelli G, Buller HR, Cohen A, et al. Apixaban for extended treatment of venous thromboembolism N Engl J Med, 2013.PMID 23216615
- [12]Weitz JI, Lensing AWA, Prins MH, et al. Rivaroxaban or Aspirin for Extended Treatment of Venous Thromboembolism N Engl J Med, 2017.PMID 28316279
- [13]Agnelli G, Becattini C, Meyer G, et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer N Engl J Med, 2020.PMID 32223112
- [14]Raskob GE, van Es N, Verhamme P, et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism N Engl J Med, 2018.PMID 29231094
- [15]Pollack CV, Reilly PA, Eikelboom J, et al. Idarucizumab for Dabigatran Reversal N Engl J Med, 2015.PMID 26095746
- [16]Connolly SJ, Crowther M, Eikelboom JW, et al. Full Study Report of Andexanet Alfa for Bleeding Associated with Factor Xa Inhibitors N Engl J Med, 2019.PMID 30730782
- [17]Sarode R, Milling TJ, Refaai MA, et al. Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: a randomized, plasma-controlled, phase IIIb study Circulation, 2013.PMID 23935011
- [18]Douketis JD, Spyropoulos AC, Kaatz S, et al. Perioperative Bridging Anticoagulation in Patients with Atrial Fibrillation N Engl J Med, 2015.PMID 26095867
- [19]Birnie DH, Healey JS, Wells GA, et al. Pacemaker or defibrillator surgery without interruption of anticoagulation N Engl J Med, 2013.PMID 23659733
- [20]Douketis JD, Spyropoulos AC, Duncan J, et al. Perioperative Management of Patients With Atrial Fibrillation Receiving a Direct Oral Anticoagulant JAMA Intern Med, 2019.PMID 31380891
- [21]Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation N Engl J Med, 2001.PMID 11519503
- [22]Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes N Engl J Med, 2007.PMID 17982182
- [23]Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes N Engl J Med, 2009.PMID 19717846
- [24]Mauri L, Kereiakes DJ, Yeh RW, et al. Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents N Engl J Med, 2014.PMID 25399658
- [25]ASCEND Study Collaborative Group, Bowman L, Mafham M, et al. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus N Engl J Med, 2018.PMID 30146931
- [26]McNeil JJ, Wolfe R, Woods RL, et al. Effect of Aspirin on Cardiovascular Events and Bleeding in the Healthy Elderly N Engl J Med, 2018.PMID 30221597
- [27]Gaziano JM, Brotons C, Coppolecchia R, et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial Lancet, 2018.PMID 30158069
- [28]Gibson CM, Mehran R, Bode C, et al. Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI N Engl J Med, 2016.PMID 27959713
- [29]Lopes RD, Heizer G, Aronson R, et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation N Engl J Med, 2019.PMID 30883055
- [30]Cannon CP, Bhatt DL, Oldgren J, et al. Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation N Engl J Med, 2017.PMID 28844193
- [31]Lo GK, Juhl D, Warkentin TE, et al. Evaluation of pretest clinical score (4 T's) for the diagnosis of heparin-induced thrombocytopenia in two clinical settings J Thromb Haemost, 2006.PMID 16634744
- [32]Cuker A, Arepally GM, Chong BH, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia Blood Adv, 2018.PMID 30482768
- [33]Man-Son-Hing M, Nichol G, Lau A, et al. Choosing antithrombotic therapy for elderly patients with atrial fibrillation who are at risk for falls Arch Intern Med, 1999.PMID 10218746
- [34]Lip GY, Nieuwlaat R, Pisters R, et al. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation Chest, 2010.PMID 19762550
- [35]Pisters R, Lane DA, Nieuwlaat R, et al. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey Chest, 2010.PMID 20299623