Phys · cardiovascular
Arrhythmias and Conduction Disease
Also known as arrhythmia · SVT · supraventricular tachycardia · AVNRT · AVRT · VT · ventricular tachycardia · Torsades de pointes · atrial flutter · heart block · AV block · Mobitz · bradycardia · sick sinus syndrome · bundle branch block · bifascicular block · pacemaker · ICD · adenosine · cardioversion
Consultant-physician-depth guide to tachy- and bradyarrhythmias — the stability rule, SVT and adenosine, AF rate/rhythm strategy and anticoagulation evidence, VT and Torsades, ICD primary prevention, heart block and pacing decisions, and conduction disease — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Arrhythmias and Conduction Disease

The answer first
Arrhythmia management at physician level reduces to three rules, and the exams test all three relentlessly [1]:
- Stability decides everything. Before you name the rhythm, look at the patient. Shock, pulmonary oedema, ischaemic chest pain or reduced conscious level in any sustained tachycardia means immediate synchronised cardioversion — drug algorithms are for the stable patient [1].
- Localise before you medicate. Three questions sort nearly every ECG: is the QRS narrow or wide, is the rhythm regular or irregular, and can you find atrial activity. Narrow-and-regular is supraventricular; wide-and-regular in a scarred heart is ventricular tachycardia until proven otherwise; irregular-and-narrow is almost always atrial fibrillation [3].
- In bradycardia, the question is where the block lives. AV nodal block responds to atropine and rarely kills; infra-Hisian block (Mobitz II, complete heart block with a wide escape) ignores atropine and can progress to asystole — it is a pacing problem [21].
Classification — organise by origin and rate
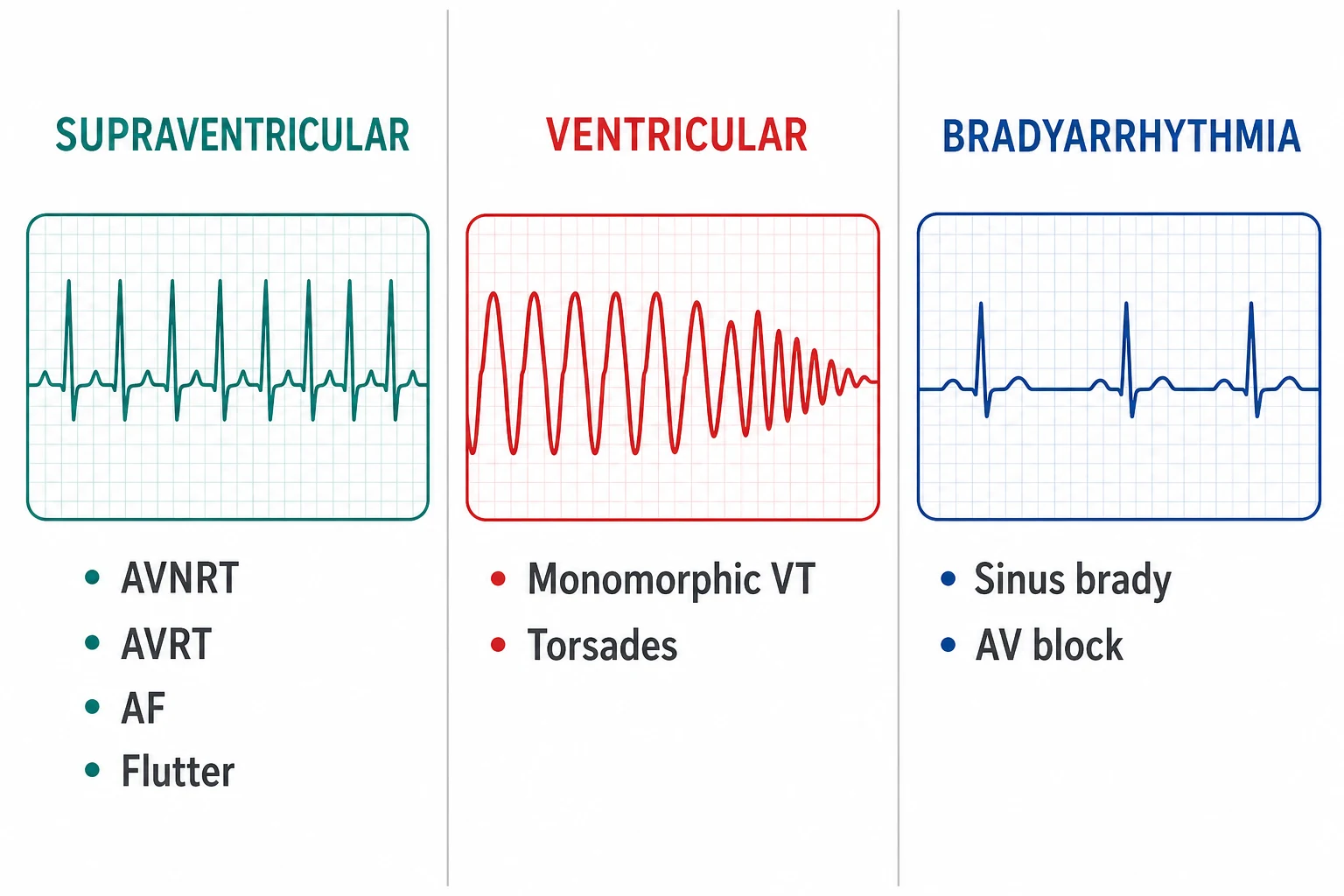
Arrhythmias classify cleanly by two axes: where the impulse comes from (supraventricular versus ventricular) and what it does to the rate (tachy versus brady). The classification is not pedantry — each family has a distinct acute treatment, a distinct long-term strategy and a distinct exam question style [3].
| Family | Members | Core mechanism | Acute treatment anchor |
|---|---|---|---|
| Supraventricular tachycardias | AVNRT, AVRT (including WPW), atrial tachycardia, atrial flutter, AF | Re-entry around or above the AV node; the AV node is usually part of the circuit or the gatekeeper | Vagal manoeuvres, adenosine, rate control, cardioversion if unstable [2] |
| Ventricular tachycardias | Monomorphic VT (scar-related re-entry), polymorphic VT and Torsades de pointes | Myocardial re-entry or triggered activity below the His bundle | Cardioversion if unstable; treat the substrate and the QT [1] |
| Bradyarrhythmias and conduction disease | Sinus node disease, AV block (first-degree, Mobitz I, Mobitz II, complete), bundle branch and fascicular blocks | Failure of impulse generation or propagation | Treat the cause, atropine for nodal problems, pacing for infra-Hisian disease [21] |
The acute tachycardia — the stability rule in action
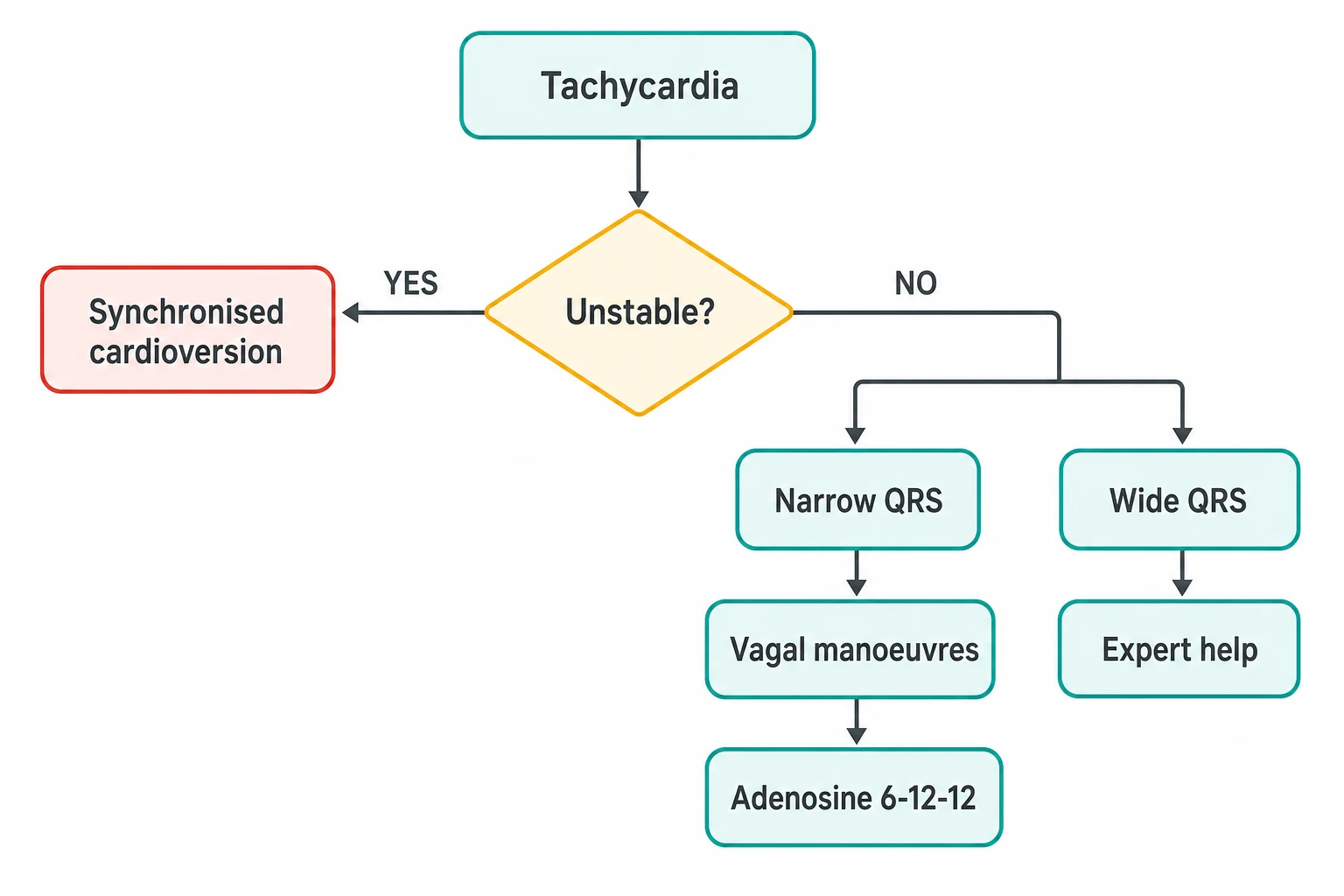
The first assessment of any tachycardia is not the ECG — it is the blood pressure, the chest, the lungs and the conscious level. Adverse features buy the rhythm a shock regardless of its name [1].
The first minutes of any sustained tachycardia
Assess stability
Systolic pressure under 90, pulmonary oedema, ischaemic chest pain, or reduced conscious level — any one makes it unstable
Unstable: synchronised cardioversion
Sedate if time allows, synchronise to the R wave, shock — up to three attempts, then antiarrhythmic support. An irregular shockable rhythm (unstable AF or polymorphic VT) may need higher energy and expert help early
Stable: read the width and regularity
Narrow and regular: vagal manoeuvres, then adenosine. Narrow and irregular: AF or flutter with variable block — rate control. Wide and regular: VT until proven otherwise
Get the 12-lead and the context
A 12-lead ECG, electrolytes including magnesium, troponin where relevant, thyroid function, and an echo for structural heart disease — these shape every downstream decision
Plan beyond the termination
Every terminated arrhythmia earns a recurrence plan: trigger correction, drug strategy, ablation referral, and anticoagulation where indicated
SVT — AVNRT, AVRT and atrial tachycardia
Paroxysmal SVT is a regular narrow-complex tachycardia, typically 150–250 beats per minute, that starts and stops abruptly. The three common substrates are AV nodal re-entrant tachycardia (a dual-pathway circuit within the AV node — the commonest), AV re-entrant tachycardia (a circuit using an accessory pathway, as in Wolff-Parkinson-White), and atrial tachycardia (a focal atrial source driving the heart) [2].
Acute termination follows a strict sequence [2]:
| Step | Action | Notes for the exam |
|---|---|---|
| 1 | Vagal manoeuvres — modified Valsalva (strain then supine leg raise) or carotid sinus massage | Terminates about a quarter of SVTs; modified Valsalva outperforms the standard strain |
| 2 | Adenosine 6 mg rapid IV push, flush immediately | If no effect: 12 mg, then a further 12 mg. Transient AV nodal block either terminates the circuit or unmasks atrial activity (flutter waves, atrial tachycardia) [2] |
| 3 | Still not terminated | Repeat ECG scrutiny, then IV verapamil/diltiazem or a beta-blocker; cardioversion at any point if instability develops [3] |
| 4 | Long term | Catheter ablation is first-line for recurrent AVNRT and AVRT — cure rates above 95 percent with low risk; drugs are for patients who decline or are poor candidates [3] |
Atrial tachycardia and typical atrial flutter behave like cousins of SVT: flutter is a macro-re-entrant circuit around the tricuspid annulus producing the sawtooth baseline, classically at an atrial rate near 300 with 2:1 conduction giving a ventricular rate near 150. A regular narrow tachycardia at exactly 150 should make you suspect flutter with 2:1 block — adenosine will not terminate it but will reveal the sawtooth by increasing the block [3].
Flutter's long-term management is one of the cleanest wins in electrophysiology: cavotricuspid isthmus ablation is highly effective and is preferred over long-term drug suppression. The exam point that catches candidates: flutter carries the same thromboembolic risk as AF and is anticoagulated by the same rules — cardioversion and ablation do not remove the indication to assess stroke risk [3].
Reading the ECG — five strips that carry the exam
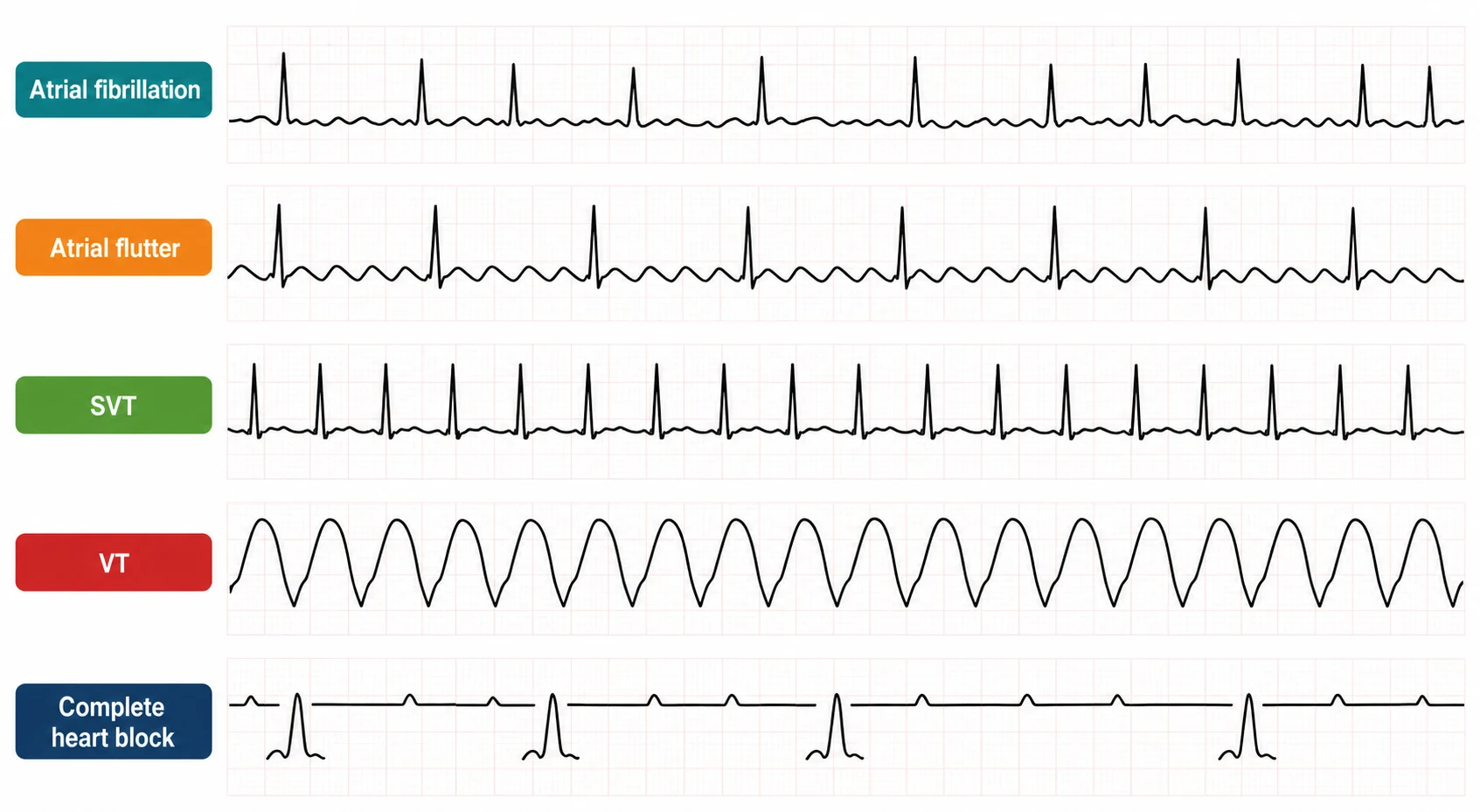
Most DWE rhythm questions are answerable from five patterns. Learn the discriminator, not just the picture [3].
| Strip | Pattern | The discriminator | The classic trap |
|---|---|---|---|
| Atrial fibrillation | Irregularly irregular narrow complexes, no P waves, fibrillatory baseline | Irregularity plus absent atrial activity | AF with complete heart block becomes regular (junctional escape) — classically digoxin toxicity |
| Atrial flutter | Sawtooth flutter waves, best seen in II, III, aVF or V1; ventricular response often near 150 (2:1) | Rate of exactly 150 with invisible P waves | Calling it SVT and missing that adenosine unmasks rather than terminates [3] |
| SVT (AVNRT/AVRT) | Regular narrow complex, 150–250, P waves buried or just after the QRS | Abrupt onset/offset history; pseudo-R' in V1 for AVNRT | Missing pre-excitation on the sinus-rhythm ECG between attacks |
| VT | Regular wide complex, rate usually 120–250 | AV dissociation, capture/fusion beats, extreme axis, concordance | Giving verapamil to a wide-complex tachycardia — haemodynamic collapse follows [1] |
| Complete heart block | P waves march through at their own rate, independent of QRS | PR interval is entirely chaotic; atrial rate exceeds ventricular rate | Mistaking 2:1 block for sinus bradycardia |
Atrial fibrillation — the two decisions
AF management is two largely independent decisions: what to do about the rhythm (rate versus rhythm control) and what to do about the stroke risk (anticoagulation). Confusing the two is the commonest candidate error — restoring sinus rhythm does not remove the indication to anticoagulate [4].
Rate versus rhythm — the evidence arc. The AFFIRM and RACE trials established that a rate-control strategy was not inferior to rhythm control for mortality in predominantly older, minimally symptomatic AF patients, with fewer hospitalisations and less proarrhythmia — which made "rate control first" the default for two decades [4] [5]. EAST-AFNET 4 then reframed the question: in patients with recently diagnosed AF (within about a year) and cardiovascular risk factors, early rhythm control — antiarrhythmic drugs or ablation started promptly — reduced a composite of cardiovascular death, stroke, and hospitalisation for heart failure or acute coronary syndrome compared with usual care [6]. The synthesis examiners expect: rate control remains a legitimate default for asymptomatic or minimally symptomatic patients, but early rhythm control is now preferred for recently diagnosed AF with cardiovascular comorbidity, for symptomatic patients, for younger patients, and where tachycardia is impairing ventricular function [6].
How aggressive should rate control be? RACE II showed lenient rate control (resting ventricular rate under 110 per minute) was non-inferior to strict control (under 80) for the composite clinical outcome — do not stack drugs to chase a number in an asymptomatic patient [7]. For drug selection: beta-blockers are first line for most; non-dihydropyridine calcium channel blockers (verapamil, diltiazem) suit patients without reduced ejection fraction; digoxin earns its place in sedentary or frail older patients — the RATE-AF trial found digoxin achieved similar symptomatic improvement to bisoprolol in elderly AF patients with fewer adverse effects [15].
Anticoagulation is decided by the stroke score, not the rhythm pattern. CHA₂DS₂-VASc (heart failure, hypertension, age 75 or older — two points, diabetes, prior stroke/TIA — two points, vascular disease, age 65–74, female sex) estimates annual stroke risk and drives the decision; a score of 2 or more in men, or 3 or more in women, generally mandates anticoagulation [8]. Critically, paroxysmal AF carries the same stroke risk as persistent AF at a given score — "it self-terminated" is never a reason to withhold anticoagulation [8]. HAS-BLED quantifies bleeding risk, but its correct use is as a checklist of modifiable bleeding risks (uncontrolled hypertension, interacting drugs, alcohol, labile INR) — a high HAS-BLED is a prompt to fix what can be fixed and follow up, not a reason to deny anticoagulation [9].
DOAC or warfarin? For non-valvular AF the direct oral anticoagulants are preferred: RE-LY (dabigatran), ARISTOTLE (apixaban) and ROCKET-AF (rivaroxaban) each showed non-inferior or superior stroke prevention versus warfarin with less intracranial haemorrhage; ARISTOTLE additionally showed a mortality benefit [10] [11] [12]. Warfarin retains its role in mechanical valves and moderate-to-severe rheumatic mitral stenosis ("valvular AF"), and DOAC doses must be adjusted for renal function, age and weight per the trial-derived criteria [11].
Catheter ablation. Pulmonary vein isolation is now a mainstream rhythm-control tool. CABANA randomised symptomatic AF patients to ablation versus drug therapy: the primary composite endpoint was not significantly reduced on intention-to-treat analysis, but ablation improved quality of life and reduced AF recurrence — framing it as an effective symptom and burden intervention rather than proven mortality therapy [13]. CASTLE-AF is the important carve-out: in AF with heart failure with reduced ejection fraction, ablation reduced death and heart-failure hospitalisation — which is why ablation is offered early in the AF-plus-HFrEF phenotype, where tachycardia and irregularity are themselves harming the ventricle [14].
The numbers the DWE expects verbatim
Ventricular tachycardia, Torsades and sudden death prevention
Monomorphic VT — a uniform wide-complex tachycardia — usually arises from re-entry around an old infarct or cardiomyopathic scar. A stable patient may be trialled on an antiarrhythmic (procainamide is a defensible exam answer; amiodarone the familiar one), but any deterioration means cardioversion. The durable questions are about the substrate: ischaemic workup, echocardiography or MRI for ventricular function, and whether the ejection fraction crosses the defibrillator threshold [1].
Polymorphic VT with a long QT is Torsades de pointes, and it has its own rules. The mechanism is triggered activity from early afterdepolarisations in a ventricle with delayed repolarisation — most often drug-induced (QT-prolonging antiarrhythmics, macrolides, fluoroquinolones, antipsychotics, methadone, ondansetron), potentiated by hypokalaemia, hypomagnesaemia, bradycardia and female sex [18].
Sudden cardiac death prevention is where the ICD evidence lives. Two trials define primary prevention thresholds: MADIT II (post-infarction, LVEF at or below 30 percent) and SCD-HeFT (ischaemic and non-ischaemic cardiomyopathy, LVEF at or below 35 percent, NYHA II–III) — both showed ICDs reduce all-cause mortality compared with medical therapy, and SCD-HeFT importantly showed amiodarone did not improve survival [16] [17].
Sudden-death prevention numbers
The fine print examiners probe: the ICD decision is made after guideline-directed medical therapy has been given time to work (guidelines typically require about three months of optimised therapy and reassessment of the ejection fraction), after revascularisation where indicated, and in a patient with a prognosis that makes arrhythmic protection meaningful [17].
Bradycardia and heart block
Bradycardia management starts with the same stability question as tachycardia: hypotension, ischaemia, heart failure or altered conscious level in a slow rhythm demands immediate action — atropine while preparing transcutaneous pacing [1]. The physician-level nuance is anatomical: atropine works by blocking vagal tone at the AV node, so it helps sinus bradycardia and AV nodal block, and frequently fails in infra-Hisian block — Mobitz II, complete heart block with a wide escape rhythm, and the denervated transplanted heart [21].
| Block | ECG signature | Level | What it means | Action |
|---|---|---|---|---|
| First-degree | PR above 200 ms, every P conducted | Usually AV nodal | A marker, not a disease | Observe; review drugs |
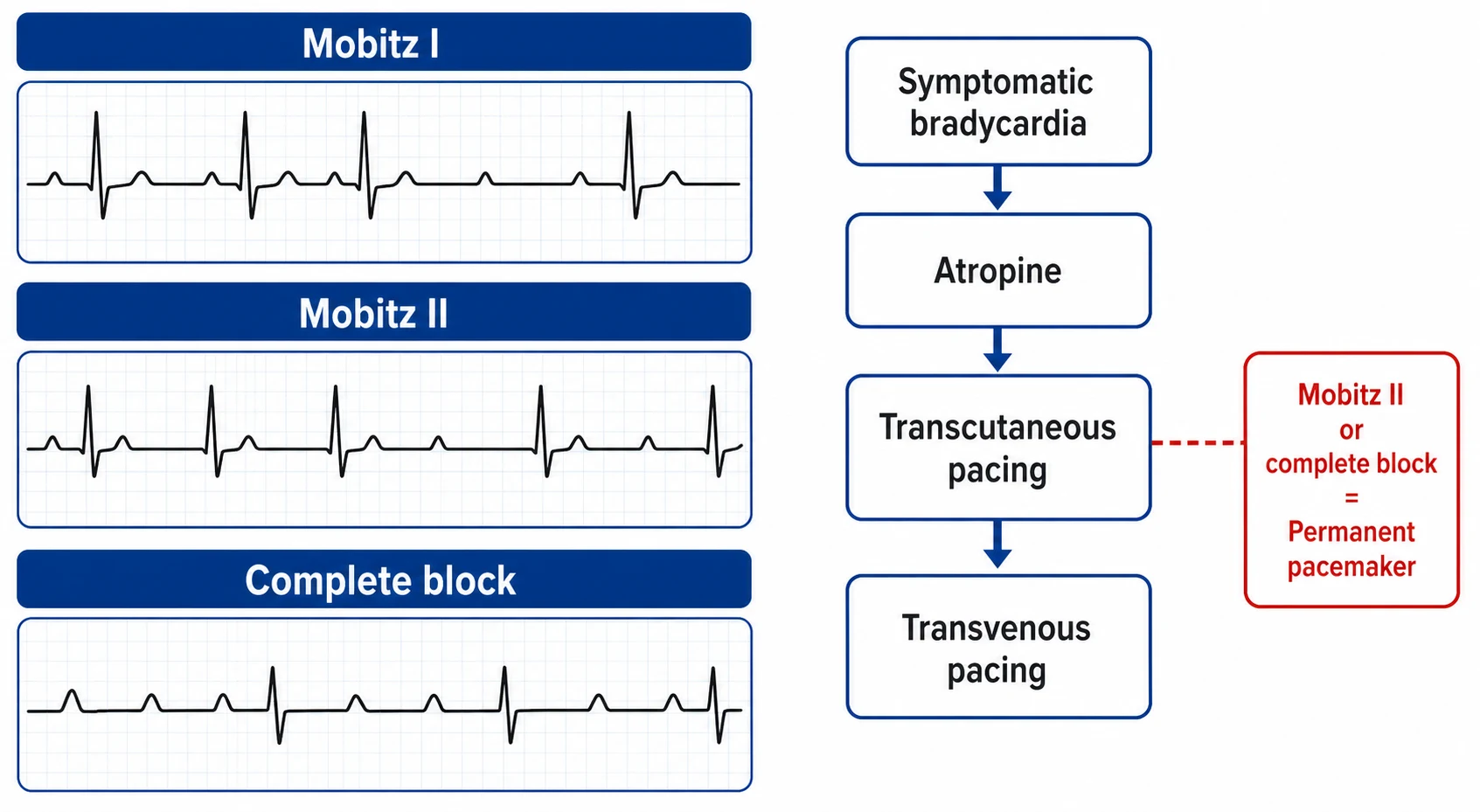
| Mobitz I (Wenckebach) | Progressive PR prolongation then a dropped beat | AV nodal | Usually benign; vagal tone, inferior ischaemia, drugs | Treat symptoms and causes; pacing rarely needed [21] |
| Mobitz II | Constant PR with sudden non-conducted P waves | Infra-Hisian | Diseased His-Purkinje system; can progress to complete block without warning | Permanent pacemaker even without symptoms [21] |
| 2:1 block | Every second P conducted | Cannot be classified as Mobitz I or II on one strip | Wide QRS escape points infra-Hisian | Usually paced [22] |
| Complete (third-degree) | AV dissociation — atria and ventricles beat independently | Nodal or infra-Hisian | Escape rhythm determines stability | Permanent pacemaker; temporary pacing if unstable [21] |
Symptomatic bradycardia — the acute sequence
Confirm adverse features
Hypotension, ischaemic chest pain, heart failure, syncope or reduced conscious level
Atropine 500 micrograms IV
Repeat to a maximum of 3 mg; expect failure in Mobitz II, complete block with wide escape, and transplanted hearts
Transcutaneous pacing
Pads on, demand mode, increase current until electrical and mechanical capture; sedate and analgese — it hurts
Bridge to transvenous pacing
Temporary wire for persistent instability or unreliable capture while the permanent decision is made
Fix reversible causes
Stop beta-blockers, verapamil, digoxin and amiodarone; correct potassium and treat ischaemia, hypothyroidism and hypothermia
Decide on permanent pacing
Mobitz II, high-grade and complete AV block, and symptomatic sinus node disease are the classic indications
Sinus node disease (sick sinus syndrome) is the other bradycardia exam home: inappropriate sinus rates, sinus pauses, and the tachycardia-bradycardia syndrome where paroxysmal AF alternates with long post-conversion pauses. Pacing is indicated for symptomatic sinus node disease with a documented rhythm-symptom correlation — the number alone is never enough [22].
Conduction disease — the bundle branches and the bifascicular trap
Isolated right bundle branch block is common and usually benign; new LBBB in the right clinical setting can mark ischaemia or cardiomyopathy and always deserves structural assessment. The examinably dangerous pattern is bifascicular block — RBBB with left anterior or posterior fascicular block (or alternating bundle branch blocks) — because only one fascicle remains between the patient and complete heart block [21].
The decision that defines the DCE short case and DWE vignette is what to do with syncope plus bifascicular block. Intermittent complete heart block is the presumptive cause when syncope is sudden, without prodrome, with brief loss of consciousness and rapid recovery — and guidelines support permanent pacing in unexplained syncope with bifascicular block after other causes are excluded, because progression rates are substantial and the consequences are traumatic [21] [23].
Investigations — matching the monitor to the symptom frequency
The investigation that captures the rhythm is chosen by how often the symptom happens — this logic is itself an exam answer [23].
| Symptom frequency | Tool | Why |
|---|---|---|
| Daily | 24–48 hour Holter | High yield when symptoms are frequent |
| Weekly to monthly | Patch or event monitor (7–14 days) | Better compliance and yield for infrequent events |
| Rare, unexplained, high-stakes syncope | Implantable loop recorder (up to 3 years) | The ESC syncope guideline positions ILR early for unexplained syncope in high-risk patients once structural and neurological causes are assessed [23] |
| Sustained arrhythmia or curative intent | Electrophysiological study | Diagnostic and therapeutic in one sitting for SVT, flutter and many VTs [3] |
Every new arrhythmia also earns the context screen: 12-lead ECG in sinus rhythm (pre-excitation, QT interval, conduction intervals), potassium and magnesium, thyroid function, troponin where ischaemia is plausible, and echocardiography for structural heart disease — because the same rhythm is managed entirely differently in a normal and a scarred ventricle [23].
Peri-procedural anticoagulation and devices
Two trials anchor the perioperative questions the DWE asks. BRIDGE: in anticoagulated AF patients needing surgery, foregoing warfarin bridging with low-molecular-weight heparin was non-inferior for arterial thromboembolism and produced less major bleeding — routine bridging is dead [24]. BRUISE CONTROL: pacemaker and defibrillator surgery is performed without interrupting warfarin (and later evidence extended the principle to DOACs) — continued anticoagulation caused fewer pocket haematomas than heparin bridging [25].
The practical peri-procedural frame: DOACs are withheld for 24–72 hours depending on procedural bleeding risk and renal function, warfarin for about five days where interruption is truly needed, and bridging is reserved for exceptional thrombotic risk (mechanical valves, recent stroke) rather than AF in general [24].
The long and short case angles
Long case — AF anticoagulation in multimorbidity. The classic DCE long case is the elderly patient with persistent AF, chronic kidney disease, and a fall history. The examiner wants to watch you weigh stroke prevention against bleeding without reaching for a formula: quantify the stroke risk with CHA₂DS₂-VASc, treat HAS-BLED as a modifiable-risk list (blood pressure, interacting drugs, alcohol, fall-proofing rather than withholding), choose the agent against renal function — apixaban's renal profile makes it a common defensible choice in CKD — and state your monitoring plan [8] [9] [11]. Falls alone rarely tip the balance: modelled analyses consistently show the stroke risk of a scored patient outweighs subdural risk from all but the most extreme falls, and the guideline-consistent answer is anticoagulate while mitigating [9].
Short case — the irregular pulse. "Examine this patient's pulse" is a five-minute station with a full differential inside it. Report rate, rhythm, character; name the irregularly irregular rhythm with an apex-radial deficit as AF; then move to aetiology and consequence — blood pressure, signs of thyrotoxicosis, mitral valve disease, heart failure, and evidence of anticoagulation (bruising) or device scars. Close with your management frame: confirm on ECG, assess stroke risk, control rate, and look for the reversible driver [8].
Short case — the slow pulse and the device. A slow regular pulse asks for cannon A waves (complete heart block), drug causes, hypothyroid signs and exercise response. A pacemaker scar and device deserve description and interpretation: single versus dual leads by chest films you have seen, what the indication likely was, and the complications you would screen for — infection, erosion, lead failure, and in ICD patients, inappropriate shocks [21].
Exam traps, collected
References
- [1]Panchal AR, Bartos JA, Cabañas JG, et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Circulation, 2020.PMID 33081529
- [2]Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society J Am Coll Cardiol, 2016.PMID 26409259
- [3]Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC) Eur Heart J, 2020.PMID 31504425
- [4]Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation N Engl J Med, 2002.PMID 12466506
- [5]Van Gelder IC, Hagens VE, Bosker HA, et al. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation N Engl J Med, 2002.PMID 12466507
- [6]Kirchhof P, Camm AJ, Goette A, et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation N Engl J Med, 2020.PMID 32865375
- [7]Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation N Engl J Med, 2010.PMID 20231232
- [8]Lip GY, Nieuwlaat R, Pisters R, et al. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation Chest, 2010.PMID 19762550
- [9]Pisters R, Lane DA, Nieuwlaat R, et al. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey Chest, 2010.PMID 20299623
- [10]Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation N Engl J Med, 2009.PMID 19717844
- [11]Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation N Engl J Med, 2011.PMID 21870978
- [12]Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation N Engl J Med, 2011.PMID 21830957
- [13]Packer DL, Mark DB, Robb RA, et al. Effect of Catheter Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial JAMA, 2019.PMID 30874766
- [14]Marrouche NF, Brachmann J, Andresen D, et al. Catheter Ablation for Atrial Fibrillation with Heart Failure N Engl J Med, 2018.PMID 29385358
- [15]Kotecha D, Bunting KV, Gill SK, et al. Effect of Digoxin vs Bisoprolol for Heart Rate Control in Atrial Fibrillation on Patient-Reported Quality of Life: The RATE-AF Randomized Clinical Trial JAMA, 2020.PMID 33351042
- [16]Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure N Engl J Med, 2005.PMID 15659722
- [17]Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction N Engl J Med, 2002.PMID 11907286
- [18]Drew BJ, Ackerman MJ, Funk M, et al. Prevention of torsade de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation Circulation, 2010.PMID 20142454
- [19]Tzivoni D, Banai S, Schuger C, et al. Treatment of torsade de pointes with magnesium sulfate Circulation, 1988.PMID 3338130
- [20]Echt DS, Liebson PR, Mitchell LB, et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial N Engl J Med, 1991.PMID 1900101
- [21]Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society Circulation, 2019.PMID 30586771
- [22]Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy Eur Heart J, 2021.PMID 34455430
- [23]Brignole M, Moya A, de Lange FJ, et al. 2018 ESC Guidelines for the diagnosis and management of syncope Eur Heart J, 2018.PMID 29562304
- [24]Douketis JD, Spyropoulos AC, Kaatz S, et al. Perioperative Bridging Anticoagulation in Patients with Atrial Fibrillation N Engl J Med, 2015.PMID 26095867
- [25]Birnie DH, Healey JS, Wells GA, et al. Pacemaker or defibrillator surgery without interruption of anticoagulation N Engl J Med, 2013.PMID 23659733