Phys · cardiovascular
Atrial Fibrillation
Also known as AF · AFib · atrial fibrillation and flutter · paroxysmal AF · persistent AF · permanent AF · lone AF · valvular AF · non-valvular AF · rapid ventricular response · RVR
Consultant-physician-depth guide to atrial fibrillation — pathophysiology, classification, rate versus rhythm control, anticoagulation with CHA₂DS₂-VASc and DOACs, catheter ablation, and rapid ventricular response management — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Atrial Fibrillation
The answer first
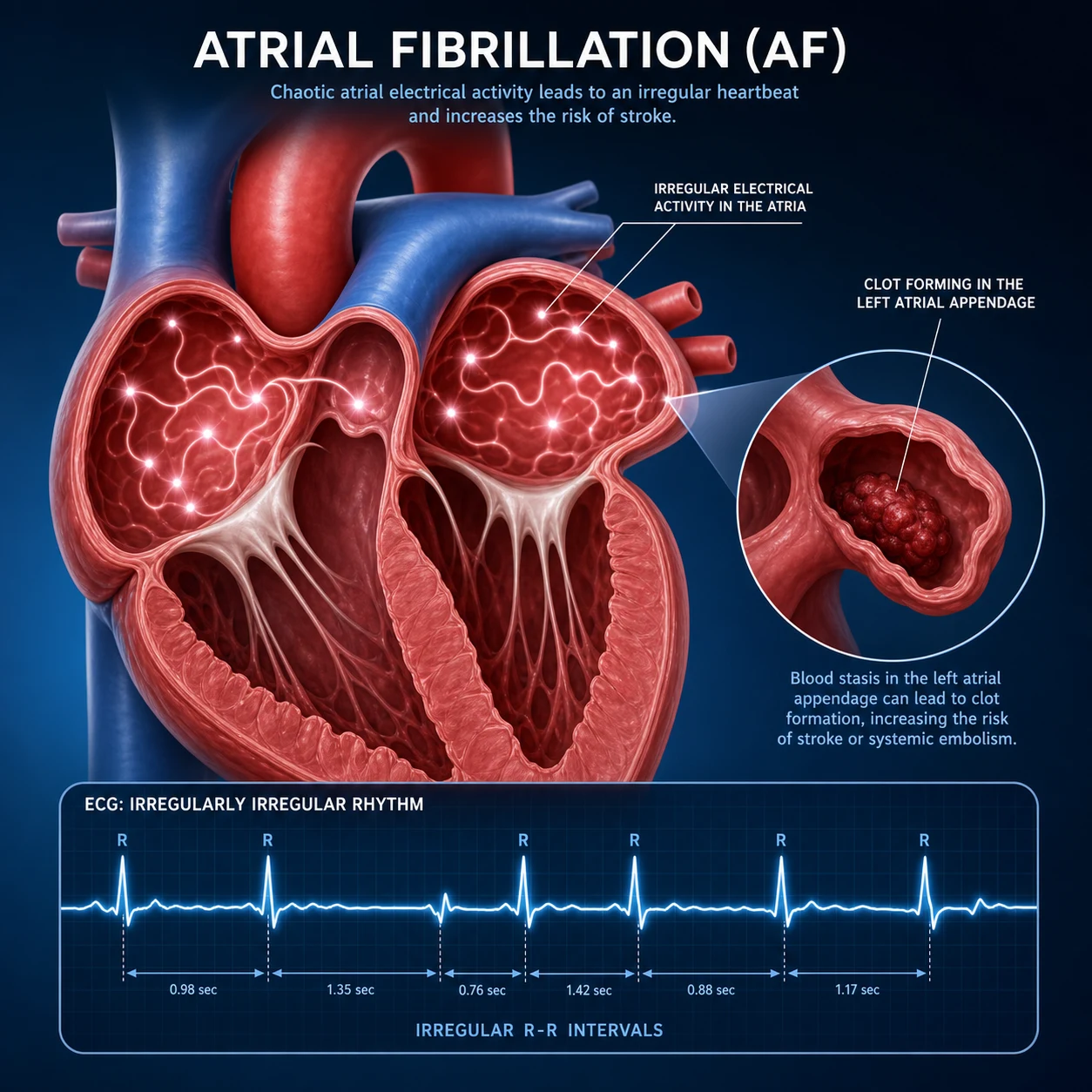
Atrial fibrillation is the most common sustained arrhythmia, characterised by chaotic, disorganised atrial electrical activity leading to an irregularly irregular ventricular response. Two decisions define management in every AF patient: [1]
- Rate or rhythm control — the strategy decision.
- Anticoagulation — the stroke prevention decision, driven by CHA₂DS₂-VASc. [1]
Rate control is the initial strategy for most stable patients. The AFFIRM trial (PMID 12466506) demonstrated no mortality advantage of rhythm over rate control in older patients, and rate control has fewer adverse drug effects. However, the EAST-AFNET 4 trial (PMID 32865375) has reinvigorated early rhythm control for recently diagnosed AF with cardiovascular comorbidities, showing a 21% reduction in a composite cardiovascular outcome. [1]
Anticoagulation is driven by stroke risk, not by the AF pattern or whether it is rate- or rhythm-controlled. CHA₂DS₂-VASc (Congestive heart failure, Hypertension, Age 75+, Diabetes, Stroke/TIA, Vascular disease, Age 65–74, Sex category) determines the decision. A DOAC (apixaban, rivaroxaban, dabigatran, edoxaban) is preferred over warfarin for non-valvular AF. ARISTOTLE (PMID 21870978) showed apixaban reduced stroke, major bleeding, and mortality versus warfarin. [1]
DWE trap: The single highest-yield discriminator is the patient who needs anticoagulation despite "only" paroxysmal AF. Stroke risk is identical for paroxysmal and persistent AF at a given CHA₂DS₂-VASc score. Never withhold anticoagulation because the AF "self-terminated." [1]
Definition and epidemiology
Atrial fibrillation is a supraventricular tachyarrhythmia defined electrocardiographically by:
- Absent P waves (no organised atrial depolarisation)
- Atrial activity: rapid, low-amplitude oscillations (fibrillatory or "f" waves) at 350–600 bpm
- Irregularly irregular ventricular response (unless complete heart block coexists) [1]
AF affects approximately 1–2% of the general population and its prevalence doubles with each decade after age 50, reaching nearly 10% in those over 80. The lifetime risk of developing AF after age 40 is approximately one in four. It is the single most common cardiac reason for hospital admission in older adults and accounts for roughly one-third of all arrhythmia-related admissions. [1]
The public health burden is enormous because AF is a major cause of ischaemic stroke — increasing stroke risk 4- to 5-fold — and is associated with heart failure, cognitive decline, and increased all-cause mortality. AF-related strokes are more severe and more disabling than non-AF strokes, because atrial thrombi are typically large and embolise to major cerebral vessels. [1]
Pathophysiology
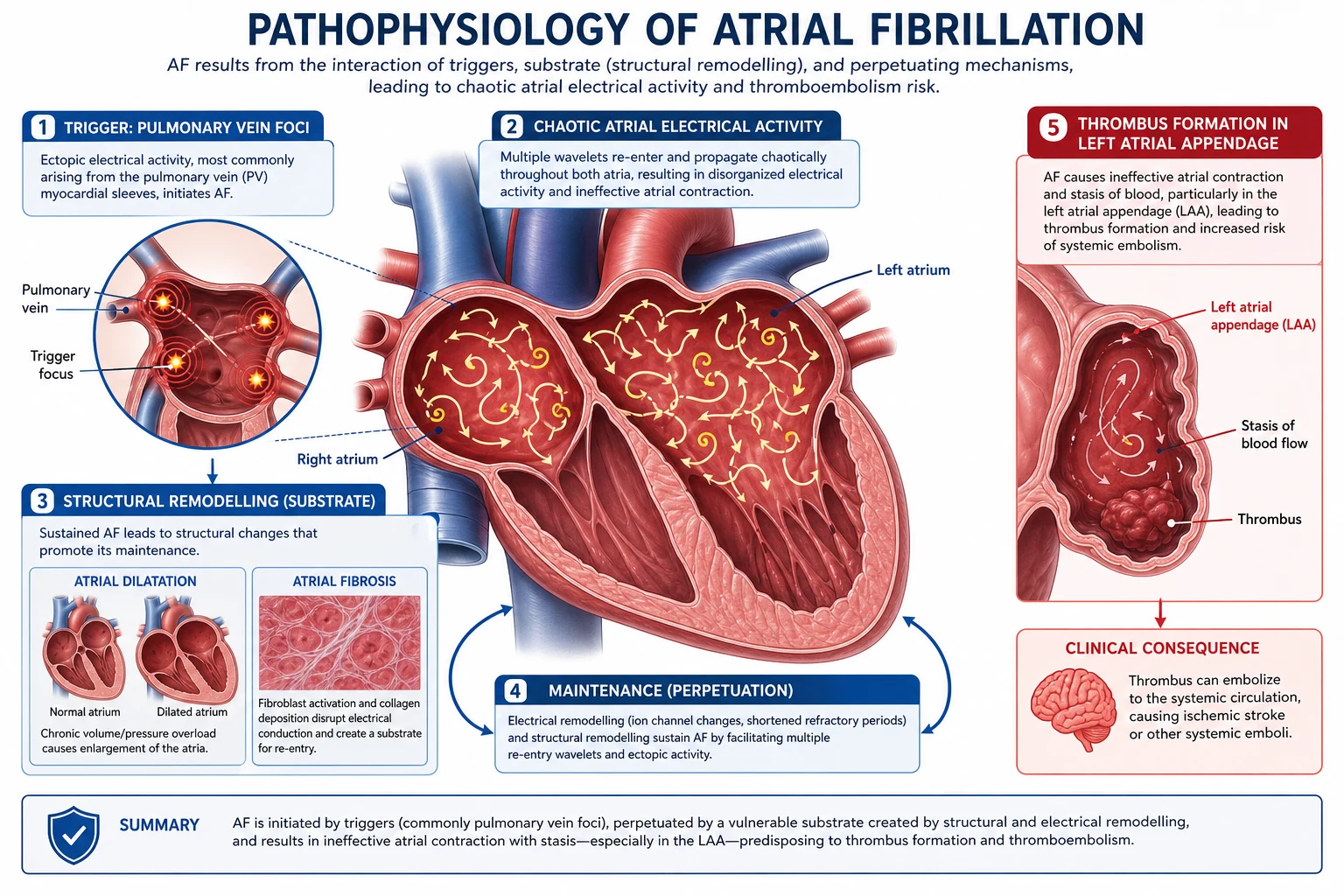
Understanding the mechanism matters because every layer — trigger, substrate, and modulator — has a corresponding therapy. Ablation targets the trigger. Antiarrhythmics modify the substrate. Rate control acts on the AV node. Anticoagulation addresses the downstream thromboembolic consequence. [1]
Trigger foci: the pulmonary vein origin
The seminal mechanistic discovery was that rapidly firing ectopic foci within the pulmonary vein ostia initiate most paroxysmal AF. These foci are clusters of atrial-like cardiomyocytes extending 1–3 cm into the pulmonary veins. They have enhanced automaticity and triggered activity. This observation is the rationale for pulmonary vein isolation (PVI) — the cornerstone of catheter ablation. [1]
Non-pulmonary vein triggers exist (superior vena cava, coronary sinus, ligament of Marshall, left atrial appendage) and become more important in persistent and long-standing persistent AF. [1]
Atrial substrate and reentry
Once AF is initiated, it sustains itself through multiple wandering reentrant wavelets moving through atrial tissue. Maintenance requires:
- A critical mass of atrial tissue (larger atria sustain AF more easily)
- Heterogeneous conduction (slow and fast pathways)
- Short refractory periods [1]
The multiple wavelet hypothesis (Moe, refined by Allessie) explains why AF begets AF: the chaotic electrical activity itself remodels the atria, shortening refractoriness and widening conduction, making the substrate ever more hospitable to the arrhythmia. [1]
Structural and electrical remodelling
AF begets AF. Sustained atrial tachyarrhythmia produces two forms of remodelling: [1]
| Remodelling type | Mechanism | Consequence |
|---|---|---|
| Electrical | Downregulation of L-type calcium channels; shortened atrial action potential and refractory period | More reentry circuits; AF harder to terminate; easier to re-induce |
| Structural | Atrial fibrosis, dilatation, gap junction remodelling (connexin downregulation) | Conduction slowing and heterogeneity; persistent substrate even after sinus rhythm restored |
This explains why early rhythm control may be beneficial: interrupting AF before irreversible structural remodelling occurs (the rationale behind EAST-AFNET 4, PMID 32865375). [1]
Autonomic modulation
The autonomic nervous system is a powerful modulator:
- Vagal tone promotes AF by shortening atrial refractoriness heterogeneously — vagally mediated AF often occurs at night, after meals, or in athletes.
- Sympathetic tone increases triggered activity in pulmonary vein foci — adrenergic AF occurs during exertion, stress, illness, or alcohol.
- Ganglionated plexi clustered around the pulmonary vein ostia are autonomic hubs; ablation of these ganglia may contribute to PVI efficacy. [1]
Thromboembolic mechanism
Blood stasis in the left atrial appendage (LAA) is the dominant source of AF-related thrombus. The LAA is a trabeculated outpouching where flow velocity drops during AF (loss of organised atrial contraction). On transoesophageal echo, spontaneous echo contrast ("smoke") and LAA thrombus are markers of thrombogenic risk. This is why LAA occlusion devices are an alternative to lifelong anticoagulation in selected patients. [1]
Classification
AF is classified by its temporal pattern and the likelihood of spontaneous or therapeutic termination. The classification guides the management conversation but does not determine anticoagulation — stroke risk is driven by CHA₂DS₂-VASc in all patterns. [1]
| Type | Definition | Clinical implication |
|---|---|---|
| Paroxysmal | Self-terminating within 7 days (usually within 48 hours) | Often mediated by pulmonary vein triggers; highest ablation success rate |
| Persistent | Sustained beyond 7 days, or requiring cardioversion | More remodelling; ablation success lower; rhythm control more challenging |
| Long-standing persistent | Continuous for more than 12 months when a rhythm-control strategy is adopted | Significant structural remodelling; extensive ablation often needed |
| Permanent | Accepted as the long-term rhythm (rate control is the strategy; no further rhythm attempts) | A clinical decision, not an inherent property — the patient and clinician accept AF as the rhythm |
| Lone AF | AF in a patient younger than 60 with no clinical or echocardiographic evidence of cardiopulmonary disease | Lower stroke risk historically; still warrants CHA₂DS₂-VASc-based assessment |
| First-diagnosed AF | First documented episode, regardless of duration | Defines the moment of entry into the management pathway |
Valvular versus non-valvular AF is a critical distinction:
- Valvular AF traditionally refers to AF in the presence of moderate-to-severe rheumatic mitral stenosis or a mechanical prosthetic heart valve. These patients require warfarin, not a DOAC. The stroke risk is very high and DOAC trials excluded (or showed harm in) this population.
- Non-valvular AF encompasses all other AF, including that associated with other valve disease (bioprosthetic valves, mitral regurgitation). DOACs are first-line here. [1]
DWE trap: A patient with a bioprosthetic mitral valve replacement and AF still qualifies for a DOAC (per ARISTOTLE subgroup data and ESC 2024). Only rheumatic mitral stenosis and mechanical valves mandate warfarin. Do not reflexively reach for warfarin just because there is "valve disease." [1]
Clinical presentation
AF presents across a wide spectrum, from incidental finding to life-threatening emergency. [1]
Symptomatic presentations
| Presentation | Mechanism | Clinical features |
|---|---|---|
| Palpitations | Irregular, rapid ventricular response | Sudden onset; patient feels "fluttering" or "racing"; may be paroxysmal |
| Dyspnoea / heart failure | Loss of atrial contribution to filling (atrial kick); tachycardia-induced cardiomyopathy | Especially in HFrEF, hypertrophic cardiomyopathy, restrictive cardiomyopathy — where atrial contraction is 30–40% of filling |
| Syncope / presyncope | Rapid rate with poor filling; or pause on termination of paroxysmal AF (sick sinus syndrome) | "Tachy-brady" syndrome: fast AF alternating with sinus pauses |
| Stroke / TIA | LAA thrombus embolisation | AF may be first diagnosed on stroke workup; silent AF commonly detected on post-stroke monitoring |
| Fatigue / exercise intolerance | Inadequate cardiac output at high rate; irregularity itself reduces cardiac efficiency | Often attributed to aging; found incidentally |
| Asymptomatic | Discovered on routine examination or ECG | Up to one-third of AF patients are truly asymptomatic |
Red flag: pre-excited AF
In a patient with an accessory pathway (Wolff-Parkinson-White syndrome), AF can conduct very rapidly down the bypass tract — ventricular rates can exceed 250 bpm and degenerate into ventricular fibrillation. The ECG shows wide, bizarre, irregular QRS complexes at very fast rates. AV nodal blocking agents (beta-blockers, diltiazem, verapamil, digoxin, adenosine) are contraindicated — they block the AV node and preferentially funnel conduction down the accessory pathway, accelerating the ventricular rate. The correct treatment is procainamide or synchronised electrical cardioversion if unstable. [1]
Physical examination
The cardinal sign is the irregularly irregular pulse. Other useful findings: [1]
- Pulse deficit: The apical rate exceeds the radial rate because some beats are too weak to transmit to the periphery (short diastolic filling time produces weak stroke volumes).
- JVP: Absent "a" waves (no organised atrial contraction); a chaotic, undulating baseline.
- Heart sounds: Variable intensity of S1 (the AV valve position varies with the short/long cycles).
- Signs of the underlying cause: Murmurs of mitral valve disease; signs of hyperthyroidism (tremor, thyroid bruit, eye signs); stigmata of ischaemic heart disease or heart failure. [1]
DCE short-case tip: In the cardiovascular examination short case, the first thing you report is "the pulse is irregularly irregular." Then immediately state what you are looking for: "This raises the possibility of atrial fibrillation; I will listen carefully for mitral murmurs and assess for signs of thyroid disease and heart failure." Examiners reward a structured differential before you reach the apex. [1]
ECG diagnosis
The ECG is the definitive diagnostic test. All four features should be present: [1]
- Absent P waves — no discrete atrial depolarisation.
- Atrial fibrillatory waves — fine or coarse baseline undulations at 350–600/min. Fine AF can mimic a flat baseline.
- Irregularly irregular R-R intervals.
- Narrow QRS (unless there is aberrancy, pre-excitation, or pre-existing bundle branch block). [1]
Key differential: atrial flutter. Flutter has organised sawtooth flutter waves (best in inferior leads and V1), typically at 300/min, with a regular ventricular response (often 2:1 giving 150 bpm, or variable conduction giving irregularity). The distinction matters: ablation strategy differs, and some rate-control drugs behave differently. [1]
Wearable and ambulatory detection
- 24–48 hour Holter monitoring for frequent symptoms.
- Event recorders / patch monitors (7–14 days) for less frequent episodes.
- Implantable loop recorders (ILR) for cryptogenic stroke workup (CRYPTO-AF, loop recorder post-stroke studies detect silent AF in 10–30% of patients over months of monitoring).
- Smartwatch / consumer ECG detection is increasingly common; a physician must confirm any device-detected arrhythmia with a diagnostic-quality 12-lead ECG before committing to anticoagulation. [1]
Investigations
Essential (all patients)
| Investigation | Purpose |
|---|---|
| 12-lead ECG | Confirm diagnosis; assess for LVH, ischaemia, pre-excitation, bundle branch block, QRS duration (relevant for ablation) |
| Echocardiogram (TTE) | Identify structural heart disease (valve disease, LV dysfunction, LA size, hypertrophic cardiomyopathy); essential before cardioversion and before starting antiarrhythmics |
| Thyroid function (TSH) | Exclude hyperthyroidism — a reversible cause. Check in all new AF. |
| FBE, U&E, LFTs, coagulation | Baseline before anticoagulation; detect anaemia, renal dysfunction (affects DOAC dose), electrolyte disturbance |
| Blood pressure | Hypertension is the commonest associated condition and a CHA₂DS₂-VASc criterion |
Context-dependent
| Investigation | When |
|---|---|
| Troponin | If chest pain or ischaemia suspected; chronically mildly elevated in HF — do not over-treat a single value |
| BNP / NT-proBNP | If heart failure suspected; elevated in AF even without HF |
| Transoesophageal echo (TOE) | Before cardioversion if duration greater than 48 hours or unknown and no prior 3 weeks of therapeutic anticoagulation; to exclude LAA thrombus |
| Sleep study | Sleep apnoea is a risk factor and exacerbant; treat if present |
| Drug / alcohol screen | If suspected precipitant (cocaine, amphetamines, alcohol — "holiday heart") |
| Exercise test | If ischaemia suspected before starting a class IC antiarrhythmic (flecainide); or to reproduce exercise-induced AF |
Rate versus rhythm control
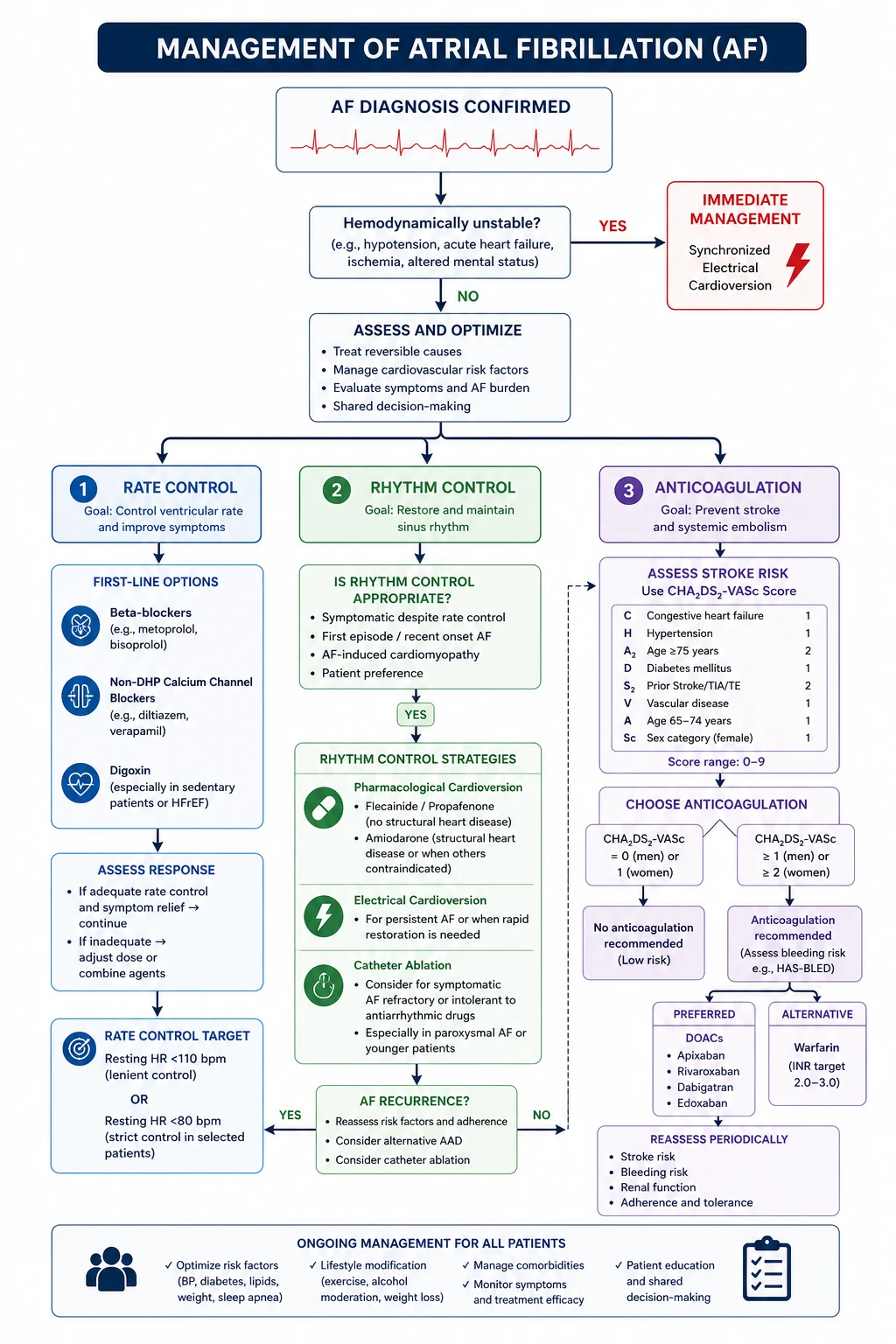
This is the central strategic decision in AF management. It is not an either/or — every patient needs rate control assessed, and selected patients benefit from rhythm control on top. [1]
The AFFIRM legacy
The AFFIRM trial (PMID 12466506) randomised 4,060 patients (mean age 69.7) with AF at high stroke/death risk to a rhythm-control strategy (antiarrhythmic drugs, cardioversion as needed) versus rate control. There was no significant difference in mortality (5-year mortality 23.8% rhythm vs 21.3% rate; HR 1.15, 95% CI 0.99–1.34, P=0.08). The rhythm arm had more hospitalisations and adverse drug effects. Critically, most strokes occurred when warfarin was stopped or subtherapeutic — emphasising that rhythm control does not remove the need for anticoagulation. [1]
Modern paradigm: EAST-AFNET 4
EAST-AFNET 4 (PMID 32865375) randomised 2,789 patients with recently diagnosed AF (within 1 year) plus cardiovascular comorbidities to early structured rhythm control versus usual care. The primary composite (cardiovascular death, stroke, hospitalisation for HF or ACS) was reduced by 21% (HR 0.79, 95% CI 0.66–0.94, P=0.005). This has shifted practice toward earlier rhythm control in recently diagnosed AF with comorbidities, using ablation and antiarrhythmics, alongside (not instead of) rate control and anticoagulation. [1]
When to favour rate control (initial strategy)
Rate control is the appropriate initial strategy for most stable patients, especially:
- Older patients
- Minimal or no symptoms
- First episode with reversible precipitant (treat the precipitant)
- Significant comorbidities where antiarrhythmic toxicity outweighs benefit
- Patient preference [1]
Rate-control targets:
- Lenient rate control (resting HR up to 110 bpm): the RACE II trial showed lenient control was non-inferior to strict (under 80 resting, under 110 with moderate exercise) for cardiovascular outcomes in stable, asymptomatic patients.
- Strict rate control (resting HR under 80 bpm): reserved for symptomatic patients, those with tachycardia-induced cardiomyopathy, or HFrEF where tachycardia worsens filling. [1]
DWE trap: Lenient rate control (resting HR up to 110) is acceptable for asymptomatic patients, but a patient who is breathless or in HFrEF still needs strict rate control. The target is individualised, not applied universally. [1]
When to pursue rhythm control
Rhythm control is preferred or should be added when:
- Symptomatic despite adequate rate control
- Younger patients (cumulative burden of lifelong AF)
- Heart failure with reduced EF — maintaining sinus rhythm may improve cardiac function and prevent tachycardia-induced cardiomyopathy (CABANA HF subgroup showed 43% mortality reduction)
- Recently diagnosed AF with comorbidities (EAST-AFNET 4 rationale)
- AF with a clear, reversible trigger that has resolved (post-operative, post-alcohol, thyroid treated) — cardiovert to break the cycle before remodelling sets in
- First episode — many clinicians attempt early cardioversion [1]
Pharmacological rate control
| Drug | Typical dose | Key cautions |
|---|---|---|
| Beta-blocker (metoprolol, bisoprolol, atenolol) | Metoprolol tartrate 25–100 mg BID; bisoprolol 2.5–10 mg OD | First-line. Avoid in severe asthma; caution in decompensated HFrEF (but evidence-based beta-blockers are part of GDMT in stable HFrEF) |
| Digoxin | 0.0625–0.25 mg OD (adjust for renal function) | Adjunct; useful in HFrEF and sedentary patients. Poor exertional rate control. Toxicity: nausea, visual disturbance (yellow-green halos), arrhythmias. Serum level 0.5–0.9 ng/mL |
| Amiodarone | 200 mg OD (maintenance) | Effective but reserved for resistant cases due to multi-organ toxicity (pulmonary, thyroid, hepatic, photosensitivity). Useful in HFrEF where other agents fail |
Combination therapy is commonly needed: a beta-blocker plus digoxin, or a beta-blocker plus diltiazem, for patients not achieving target on monotherapy. Combine cautiously — additive bradycardia and AV block risk. [1]
Rhythm control: cardioversion and antiarrhythmics
Electrical cardioversion
- Indicated for haemodynamic instability (hypotension, pulmonary oedema, ischaemia) — urgent synchronised DC shock.
- Elective cardioversion for symptomatic persistent AF. Requires either: (a) AF duration less than 48 hours (low thromboembolic risk), or (b) 3 weeks of therapeutic anticoagulation before cardioversion, or (c) TOE-guided approach (exclude LAA thrombus, then cardiovert with anticoagulation from the day of the procedure).
- After cardioversion, continue anticoagulation for at least 4 weeks regardless of baseline CHA₂DS₂-VASc (stunned atria regain contractile function slowly; thrombus can form during this recovery period).
- Success rate: approximately 80–90% for recent-onset AF, lower for long-standing AF with large atria. [1]
Pharmacological cardioversion
- Flecainide (class IC): "pill in the pocket" approach for paroxysmal AF in patients without structural heart disease. 200–300 mg PO. Onset within 2–6 hours. Avoid in ischaemia, HFrEF, bundle branch block.
- Amiodarone: slower conversion but effective; safe in structural heart disease and HFrEF.
- Vernakalant (available in some regions): rapid IV conversion agent for recent-onset AF; contraindicated in recent MI, severe aortic stenosis, HFrEF. [1]
Antiarrhythmic drug maintenance
The choice of maintenance antiarrhythmic depends on the underlying cardiac substrate — this is a key DWE discriminator: [1]
| Substrate | Preferred agent | Rationale |
|---|---|---|
| No/minimal structural heart disease | Flecainide, propafenone (class IC) | Effective; low pro-arrhythmic risk in normal hearts |
| Ischaemic heart disease | Sotalol, amiodarone | Avoid class IC (pro-arrhythmia with ischaemia — CAST trial lesson) |
| Heart failure (HFrEF) | Amiodarone, dofetilide | Safe in HFrEF; class IC contraindicated; sotalol use with caution |
| All substrates (broadest safety) | Amiodarone | Most effective; but toxicity limits long-term use |
DWE trap: Flecainide is contraindicated in ischaemic heart disease and HFrEF because it is pro-arrhythmic in diseased myocardium. The most common error is prescribing flecainide to a patient with a history of MI or a low EF. If you must choose one safe antiarrhythmic across all substrates, it is amiodarone — but you pay for it with organ toxicity. [1]
Anticoagulation
Anticoagulation is the single most impactful intervention in AF. It prevents the most devastating complication — cardioembolic stroke. The decision is driven entirely by stroke risk (CHA₂DS₂-VASc), not by the AF pattern, the rate-control strategy, or whether the patient is in sinus rhythm at the time of assessment. [1]
CHA₂DS₂-VASc score
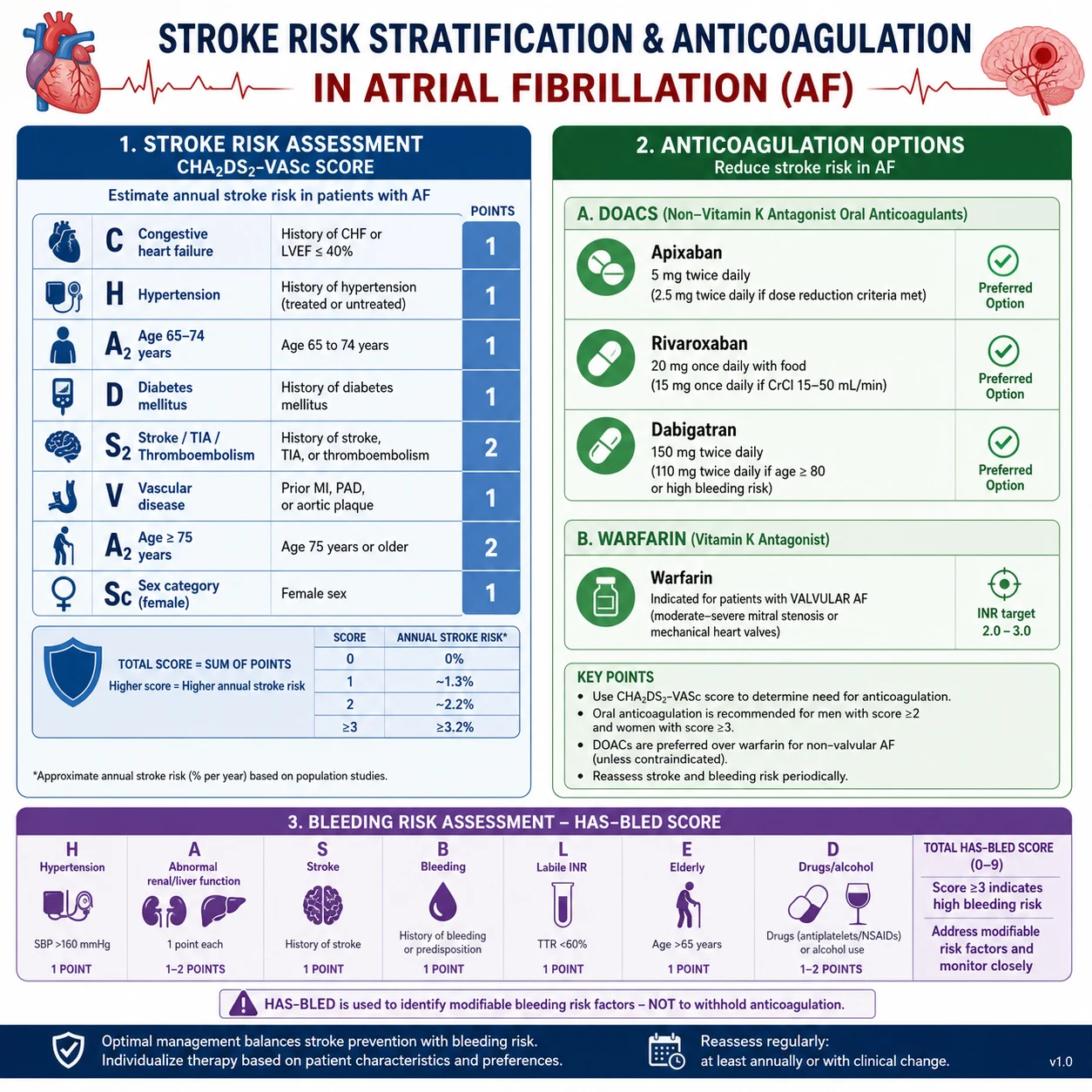
| Letter | Component | Points |
|---|---|---|
| C | Congestive heart failure (or LV dysfunction) | 1 |
| H | Hypertension (treated or untreated) | 1 |
| A₂ | Age 75 years or older | 2 |
| D | Diabetes mellitus | 1 |
| S₂ | Stroke, TIA, or systemic thromboembolism (prior) | 2 |
| V | Vascular disease (prior MI, PAD, aortic plaque) | 1 |
| A | Age 65–74 years | 1 |
| Sc | Sex category (female = 1 point) | 1 |
Maximum score: 9 (for females); 8 (for males). [1]
Decision thresholds (ESC 2024, consistent with ACC/AHA 2023):
- Score 0 in men, 1 in women: anticoagulation generally not recommended. (The lone "female sex" point does not independently increase stroke risk without other factors.)
- Score 1 in men, 2 in women: consider anticoagulation; shared decision-making.
- Score 2 or more in men, 3 or more in women: recommend anticoagulation unless contraindicated. [1]
DWE high-yield rule: The female sex point only counts if there is at least one other risk factor. A 55-year-old woman with no other risk factors (score 1, from sex alone) does not need anticoagulation. A 75-year-old woman with hypertension (score 4: age 2, HTN 1, sex 1) definitely does. [1]
HAS-BLED (bleeding risk)
HAS-BLED (Hypertension uncontrolled, Abnormal renal/liver function, Stroke history, Bleeding history/predisposition, Labile INR, Elderly age 65+, Drugs/alcohol concomitantly) estimates major bleeding risk. A score of 3 or more indicates high bleeding risk — it is not a reason to withhold anticoagulation, but a prompt to identify and correct modifiable bleeding risk factors (uncontrolled blood pressure, concomitant antiplatelets, NSAIDs, alcohol excess). Net clinical benefit almost always favours anticoagulation in patients with CHA₂DS₂-VASc at or above threshold. [1]
DOACs versus warfarin
| Feature | DOACs (apixaban, rivaroxaban, dabigatran, edoxaban) | Warfarin |
|---|---|---|
| Mechanism | Direct inhibition (thrombin for dabigatran; factor Xa for the others) | Vitamin K antagonism (factors II, VII, IX, X; proteins C, S) |
| Monitoring | None required (renal function periodically) | Regular INR (target 2.0–3.0 for non-valvular AF) |
| Onset/offset | Rapid (hours) | Slow (days); requires bridging in some contexts |
| Efficacy | Non-inferior or superior to warfarin | Long-standing evidence base |
| Bleeding profile | Lower intracranial haemorrhage; similar or lower major bleeding; higher GI bleeding for some agents | Higher intracranial bleeding |
| Reversal | Idarucizumab (dabigatran); andexanet alfa (apixaban, rivaroxaban); PCC for all | Vitamin K + PCC/FFP |
| Indication for warfarin | Not preferred — mechanical valves, rheumatic mitral stenosis | Mechanical valves, moderate-severe rheumatic MS, antiphospholipid syndrome |
Key trial: ARISTOTLE (PMID 21870978). Apixaban 5 mg BID versus warfarin in 18,201 patients with non-valvular AF. Apixaban was superior — 21% reduction in stroke/systemic embolism, 31% reduction in major bleeding, and 11% reduction in all-cause mortality. Apixaban is often the preferred DOAC based on this combination of superior efficacy and safety. [1]
Key trial: RE-LY (PMID 19717844). Dabigatran 150 mg BID was superior to warfarin for stroke prevention with similar major bleeding; 110 mg BID was non-inferior with less bleeding. Dabigatran is the only direct thrombin inhibitor DOAC. [1]
DOAC dosing adjustments
Apixaban dose reduction criteria (must meet at least two of three):
- Age 80 years or older
- Body weight 60 kg or less
- Serum creatinine 133 micromol/L or greater (1.5 mg/dL) [1]
If two of these are present, reduce to apixaban 2.5 mg BID. This is a common DWE stem: the elderly, small, renally impaired patient who needs dose reduction. [1]
Rivaroxaban: 20 mg OD reduces to 15 mg OD if CrCl 15–50 mL/min. Dabigatran: 150 mg BID reduces to 110 mg BID if age over 80 or CrCl 30–50 (regional variation). [1]
Left atrial appendage occlusion
For patients with a contraindication to anticoagulation (prior life-threatening bleed), percutaneous LAA occlusion (Watchman device) is an alternative. It excludes the LAA from the circulation, eliminating the primary source of thrombus. Post-procedure, temporary antithrombotic therapy is required until endothelialisation. [1]
Catheter ablation
Catheter ablation (pulmonary vein isolation) electrically isolates the pulmonary vein triggers from the left atrium, preventing them from initiating AF. [1]
Indications
- Symptomatic paroxysmal AF failing or intolerant to at least one class I or III antiarrhythmic (class I indication in most guidelines)
- Symptomatic persistent AF failing antiarrhythmic therapy
- AF with heart failure and reduced EF — the CASTLE-AF and CABANA heart-failure subgroup data support ablation as superior to antiarrhythmic drugs for survival and hospitalisation in selected HF patients
- First-line ablation is increasingly considered for highly symptomatic paroxysmal AF in younger patients without extensive structural remodelling [1]
CABANA trial (PMID 30874766)
The CABANA trial randomised 2,204 patients to catheter ablation versus drug therapy (rate or rhythm control). The primary composite (death, disabling stroke, serious bleeding, cardiac arrest) was not significantly different (8.0% ablation vs 9.2% drug; HR 0.86, P=0.30), partly due to a 27% crossover from drug to ablation. However, ablation significantly reduced AF recurrence (HR 0.52) and showed benefit in the heart failure subgroup (36% reduction in primary composite, 43% reduction in mortality). [1]
Procedure
- Radiofrequency ablation or cryoballoon ablation to achieve pulmonary vein isolation (circumferential lesions around the PV ostia).
- Persistent AF may require additional substrate modification (linear lesions, complex fractionated atrial electrogram ablation, posterior wall isolation), though PVI alone is the foundation.
- Periprocedural anticoagulation is required; TOE is performed pre-procedure to exclude LAA thrombus. [1]
Outcomes and complications
- Success rate: 60–80% for paroxysmal AF (single procedure); higher with redo procedures. 40–60% for persistent AF.
- Complications: cardiac tamponade (1–2%), stroke/TIA (under 1%), pulmonary vein stenosis (rare with modern techniques), phrenic nerve injury (cryoballoon), atrio-oesophageal fistula (very rare, catastrophic), vascular access complications.
- Late recurrence is common; ablation is not a cure but a management strategy. [1]
Acute management: AF with rapid ventricular response
AF with RVR (ventricular rate typically above 120 bpm) is a common acute presentation. Management depends on haemodynamic stability. [1]
Haemodynamically unstable (hypotension, ischaemia, pulmonary oedema, altered consciousness)
Immediate synchronised electrical cardioversion. Do not wait for rate control to work. This is the correct answer in every unstable AF scenario. Start anticoagulation (unless contraindicated) after cardioversion. [1]
Haemodynamically stable
-
Rate control first:
- IV metoprolol (5 mg boluses, titrated) or IV diltiazem (0.25 mg/kg bolus then infusion) are first-line for rapid rate control.
- IV digoxin or IV amiodarone if beta-blocker/diltiazem ineffective or contraindicated (e.g., severe HFrEF where CCB is harmful).
- Target ventricular rate: under 110 bpm initially (lenient), then titrate to under 80 bpm if symptomatic or in HFrEF. [1]
-
Assess for and treat precipitants: sepsis, thyrotoxicosis, dehydration, ACS, PE, alcohol, electrolyte disturbance (hypokalaemia, hypomagnesaemia). [1]
-
Rhythm control (cardioversion) can be considered for recent-onset AF (within 48 hours) if rate control fails or symptoms persist — pharmacological (flecainide, amiodarone) or electrical. If AF duration is over 48 hours or unknown, anticoagulate for 3 weeks first or use TOE-guided approach. [1]
Special situation: AF with pre-excitation (WPW)
As noted above, never give AV nodal blockers in pre-excited AF. The ECG shows wide, irregularly irregular QRS at very fast rates. Use IV procainamide or synchronised cardioversion if unstable. The mechanism: blocking the AV node funnels all conduction down the accessory pathway, which can conduct at 300+ bpm and degenerate to VF. [1]
AF in heart failure
AF and heart failure frequently coexist and each worsens the other. AF is both a consequence of HF (atrial dilatation from elevated filling pressures) and a cause (tachycardia-induced cardiomyopathy). [1]
Why AF worsens HF
- Loss of atrial kick: Atrial contraction contributes 20–30% of LV filling in normal hearts, but 30–40% in HFrEF where diastolic filling is impaired. Loss of this in AF dramatically reduces preload and cardiac output.
- Tachycardia: Rapid ventricular response reduces diastolic filling time and coronary perfusion time; chronic tachycardia causes tachycardia-induced cardiomyopathy — a reversible form of LV dysfunction that improves with rate or rhythm control.
- Irregularity: Beat-to-beat variability itself reduces cardiac output and is haemodynamically disadvantageous. [1]
Management priorities in AF + HFrEF
- Rate control: Beta-blocker (evidence-based: bisoprolol, carvedilol, metoprolol succinate) is ideal — dual benefit for AF rate and HF mortality. Digoxin is safe and useful in HFrEF (no negative inotropy). Avoid non-DHP CCB (diltiazem, verapamil) — they are negative inotropes and worsen HFrEF.
- Rhythm control: Amiodarone is the safest antiarrhythmic in HFrEF. Dofetilide is an alternative (requires in-hospital initiation with QT monitoring). Flecainide is contraindicated (pro-arrhythmic in structural heart disease).
- Ablation: The CABANA HF subgroup and CASTLE-AF data support catheter ablation for AF in HFrEF, showing improved survival and reduced hospitalisation versus medical therapy. This is an increasingly important referral pathway.
- Anticoagulation: Heart failure is a CHA₂DS₂-VASc criterion. Most HFrEF patients with AF warrant anticoagulation.
- Optimise GDMT: The four pillars of HF therapy (ARNI, beta-blocker, MRA, SGLT2i) reduce AF burden and improve outcomes. [1]
DCE long-case trap: In the complex patient with AF and HFrEF, do not reach for diltiazem for rate control. The examiner is testing whether you know non-DHP CCB is contraindicated in HFrEF. Use a beta-blocker and/or digoxin instead. [1]
Stroke prevention and AF-related stroke
Magnitude of risk
AF increases stroke risk 4- to 5-fold. AF-related strokes are:
- More severe (larger infarct volumes, more often involving major vessel territories)
- More disabling (higher modified Rankin scores, higher mortality)
- More likely to haemorrhically transform (large embolic infarct with fragile tissue) [1]
Anticoagulation is the cornerstone
Antiplatelet therapy (aspirin, clopidogrel) is not adequate for stroke prevention in AF — it reduces risk by approximately 20%, versus 60–70% for anticoagulation. Antiplatelets have been removed from AF guidelines as monotherapy for stroke prevention. The exception is the AVOID regime (aspirin plus clopidogrel) which is inferior to anticoagulation and carries higher bleeding risk — essentially a historical footnote. [1]
Timing of anticoagulation after stroke
After an ischaemic stroke in a patient with AF, the timing of (re)initiating anticoagulation balances thromboembolic protection against haemorrhagic transformation: [1]
| Infarct size | Suggested delay before anticoagulation |
|---|---|
| TIA | 1 day |
| Small (under 1.5 cm) | 3 days |
| Moderate (1.5–3 cm or any size with no haemorrhage on imaging) | 6 days |
| Large (over 3 cm or extensive territory) | 12–14 days |
These are the 1-3-6-12 day rule (or similar regional variants). The principle is individualised: larger infarcts need longer delay because haemorrhagic transformation risk is highest in the first 1–2 weeks. [1]
Long-term management and follow-up
Structured follow-up
- Annual review of rate-control adequacy (symptoms, heart rate / ECG), anticoagulation need (re-assess CHA₂DS₂-VASc as comorbidities accrue), and bleeding risk (HAS-BLED).
- Renal function monitoring (at least annually) for all patients on DOACs — dose adjustments are triggered by declining CrCl.
- Medation review — check for drug interactions (especially with amiodarone, which affects warfarin, statins, and digoxin levels). [1]
Managing modifiable risk factors
| Risk factor | Intervention |
|---|---|
| Hypertension | Tight control (target under 130/80 per HF/CKD guidelines); reduces AF recurrence and stroke |
| Obesity | Weight reduction (LEGACY trial: 10% weight loss reduces AF burden and symptom severity) |
| Sleep apnoea | CPAP therapy reduces AF recurrence after cardioversion or ablation |
| Alcohol | Reduce to under 10–14 standard drinks/week (alcohol is an acute and chronic AF trigger) |
| Thyroid disease | Treat hyperthyroidism; AF often resolves with euthyroidism |
| Diabetes | Glycaemic control; SGLT2i may reduce AF incidence |
Stroke prevention as the overriding priority
In the patient with permanent AF and multiple comorbidities, the single intervention with the greatest impact on hard outcomes is adherence to appropriate anticoagulation. Counselling on this, addressing cost barriers (DOAC PBS/TGA access in ANZ), and ensuring continuity across care transitions are the highest-value clinician actions. [1]
Guideline controversies and regional differences
| Topic | ESC 2024 | ACC/AHA 2023 | NICE NG196 |
|---|---|---|---|
| Anticoagulation threshold | CHA₂DS₂-VASc 2+ (men), 3+ (women) recommended; 1/2 consider | CHA₂DS₂-VASc 2+ recommended; 1 shared decision | CHA₂DS₂-VASc 1+ (men) consider; anticoagulation for most |
| DOAC vs warfarin | DOAC preferred for non-valvular AF | DOAC preferred over warfarin | DOAC first-line; warfarin for mechanical valve / MS |
| Early rhythm control | Supported by EAST-AFNET 4 | Supported; ablation first-line for symptomatic refractory | Rhythm control for symptomatic failure of rate control |
| Ablation in HF | Recommended for symptomatic AF + HFrEF | Recommended; benefit over AAD | Recommended for refractory symptoms |
Shared decision-making is emphasised across all guidelines. The patient must understand: (1) why anticoagulation matters even if they feel well; (2) the bleeding risk and what to do if it occurs; (3) the option of rate versus rhythm strategies and the trade-offs; (4) that ablation is a management tool, not necessarily a cure. [1]
Exam integration
DWE MCQ — common stems and traps
The DWE tests AF in several recurring patterns. Master these: [1]
- The anticoagulation decision: A patient with AF and a list of comorbidities. Calculate CHA₂DS₂-VASc. Determine if anticoagulation is recommended. The trap is missing a risk factor (e.g., "vascular disease" includes PAD and aortic plaque, not just MI).
- DOAC dose adjustment: An elderly, small, renally impaired patient on apixaban. Does the dose need reducing? Check the two-of-three rule.
- Rate vs rhythm strategy: A 72-year-old asymptomatic patient with persistent AF. AFFIRM supports rate control. The trap is choosing rhythm control because "sinus rhythm is better."
- Antiarrhythmic choice by substrate: A patient with HFrEF and AF — which antiarrhythmic? Amiodarone (or dofetilide). The trap is flecainide.
- Pre-excited AF: Wide irregular QRS at very fast rate. What drug is contraindicated? AV nodal blockers. What do you give? Procainamide or cardiovert.
- AF with RVR in HFrEF: Which rate-control agent? Beta-blocker or digoxin. The trap is diltiazem (negative inotrope).
- Warfarin-mandating AF: Rheumatic mitral stenosis or mechanical valve. DOAC contraindicated.
- Cardioversion and anticoagulation timing: AF over 48 hours. Three weeks of anticoagulation before, four weeks after, regardless of CHA₂DS₂-VASc. [1]
DCE long case
The AF long case is typically a multi-morbidity patient: an older patient with persistent AF, hypertension, type 2 diabetes, CKD, and possibly heart failure or ischaemic heart disease. The examiner tests: [1]
- Structured problem list with prioritised AF management.
- CHA₂DS₂-VASc and HAS-BLED calculated accurately and interpreted.
- Rate vs rhythm reasoning tailored to this patient (symptoms, comorbidities, age, preference).
- DOAC dose appropriateness — check renal function, age, weight.
- Comorbidity management — hypertension control, glycaemic control, sleep apnoea, weight.
- Follow-up plan — annual review, renal monitoring, medication interactions. [1]
DCE short case
The cardiovascular short case with an irregularly irregular pulse tests: [1]
- Examination routine: radial pulse (irregularly irregular) → blood pressure → JVP (absent a waves) → precordial examination (variable S1 intensity, murmurs of mitral disease) → signs of heart failure → signs of thyroid disease.
- Presentation: "Irregularly irregular pulse consistent with atrial fibrillation. I will now look for the underlying cause and complications."
- Discussion: differential of an irregular pulse (AF, atrial flutter with variable block, multifocal atrial tachycardia, frequent ectopics); causes of AF (the "ABC" — Age, Blood pressure, Cardiac disease, endocrine, alcohol); management outline (rate/rhythm, anticoagulation). [1]
Summary cards
| Decision point | The answer |
|---|---|
| Stable AF, what strategy? | Rate control first (AFFIRM); add rhythm control if symptomatic |
| Recently diagnosed AF with comorbidities? | Consider early rhythm control (EAST-AFNET 4) |
| When to anticoagulate? | CHA₂DS₂-VASc: 2+ men / 3+ women recommend; 1 men / 2 women consider; female sex point alone does not warrant |
| DOAC or warfarin? | DOAC for non-valvular AF (ARISTOTLE, RE-LY); warfarin for mechanical valve or rheumatic MS |
| DOAC dose reduction (apixaban)? | Two of: age 80+, weight 60 kg or under, creatinine 133+ micromol/L → 2.5 mg BID |
| Antiarrhythmic in HFrEF? | Amiodarone or dofetilide; never flecainide |
| Unstable AF with RVR? | Synchronised electrical cardioversion |
| Pre-excited AF? | Procainamide or cardioversion; never AV nodal blockers |
| Ablation role? | Symptomatic AF refractory to AAD; strong in AF + HFrEF (CABANA HF subgroup) |
| Anticoagulation after stroke? | Delay by infarct size (1-3-6-12 day rule) |
References
- Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med 2002;347(23):1825–1833. PMID 12466506.
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361(12):1139–1151. PMID 19717844.
- Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365(11):981–992. PMID 21870978.
- Kirchhof P, Camm AJ, Goette A, et al. Early rhythm-control therapy in patients with atrial fibrillation (EAST-AFNET 4). N Engl J Med 2020;383(14):1305–1316. PMID 32865375.
- Packer DL, Piccini JP, Monahan KG, et al. Mortality in patients undergoing catheter ablation for atrial fibrillation (CABANA). JAMA 2019;321(13):1261–1274. PMID 30874766. [1]
Guidelines: 2023 ACC/AHA/ACCP/HRS AF Guideline; ESC AF Guidelines (2024); NICE NG196; National Heart Foundation of Australia / CSANZ AF Guidelines. [1]
References
- [1]Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation N Engl J Med, 2002.PMID 12466506
- [2]Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation N Engl J Med, 2009.PMID 19717844
- [3]Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation N Engl J Med, 2011.PMID 21870978
- [4]Kirchhof P, Camm AJ, Goette A, et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation N Engl J Med, 2020.PMID 32865375
- [5]Packer DL, Piccini JP, Monahan KG, et al. Effect of Catheter Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial JAMA, 2019.PMID 30874766