Phys · cardiovascular
Cardiac Investigations
Also known as echocardiography · transthoracic echo · transoesophageal echo · stress testing · exercise ECG · exercise tolerance test · myocardial perfusion imaging · CT coronary angiography · coronary angiography · cardiac MRI · cardiac CT · calcium score · electrophysiology study · high-sensitivity troponin · NT-proBNP
Consultant-physician-depth guide to cardiac investigations — echocardiography, stress testing, CT coronary angiography, coronary angiography, cardiac MRI, electrophysiology, implantable devices, and biomarkers — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Cardiac Investigations

The answer first
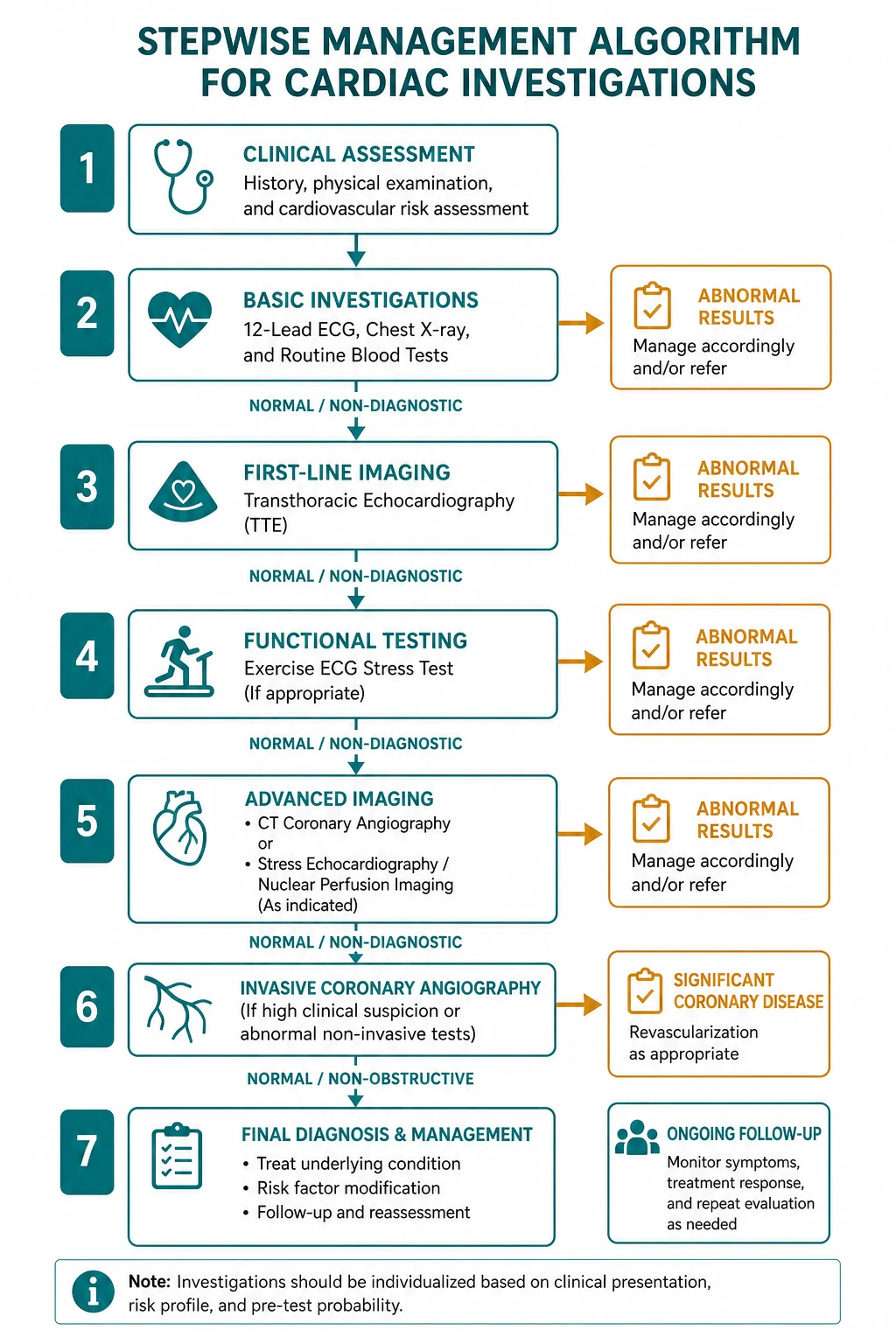
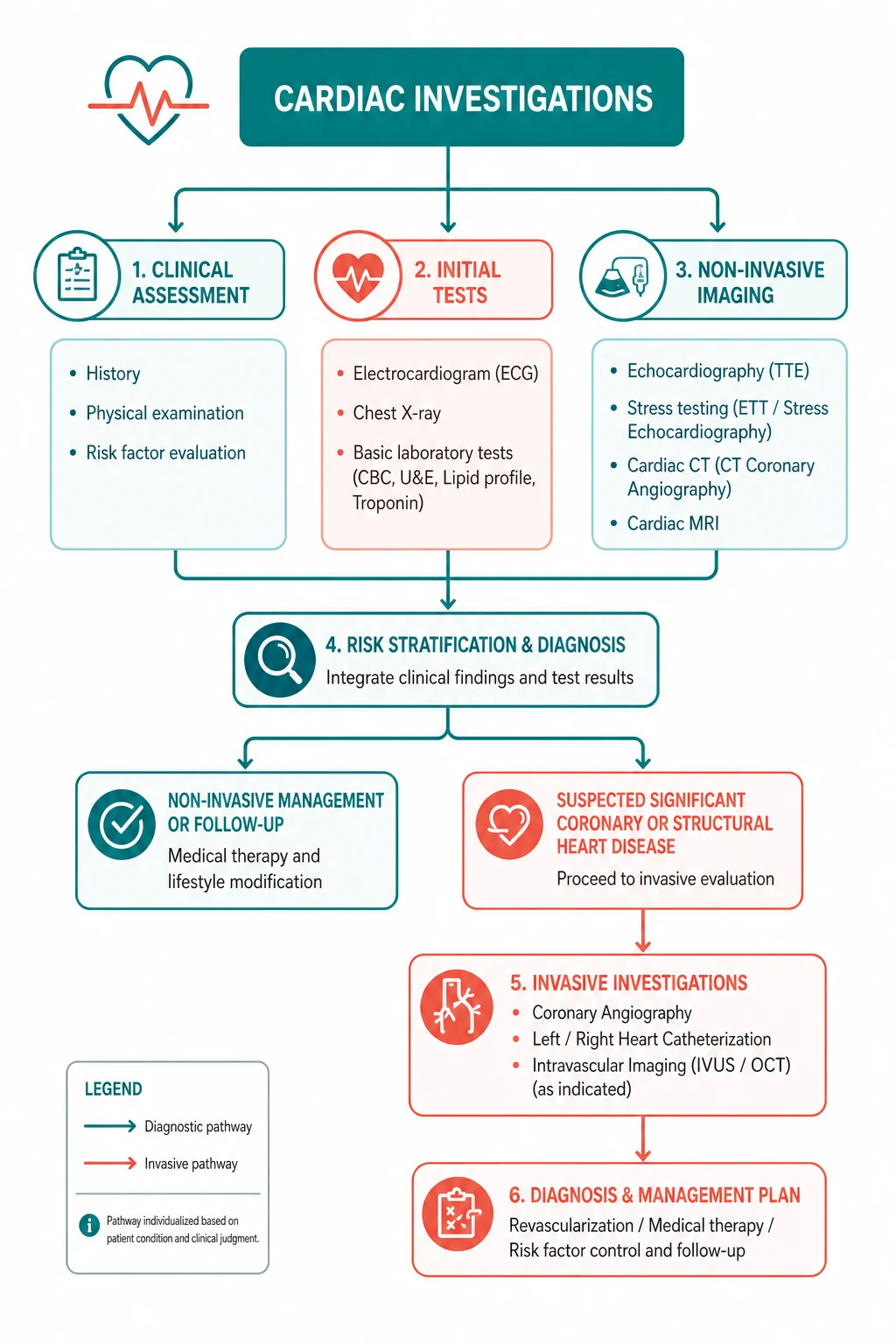
Cardiac investigations exist to answer a clinical question, not to fill a template. Every test you order should have a question attached to it: Does this patient have obstructive coronary disease? What is the ejection fraction? Is there a structural abnormality causing this murmur? Is this chest pain an acute coronary syndrome? The test you choose depends entirely on the question, the pre-test probability, and the downstream consequence of the result. [1]
The three decisions examiners test again and again: [1]
- The right stress test for the right patient. Exercise ECG is cheap and simple but has modest diagnostic accuracy (approximately 70 percent) and is uninterpretable in several common scenarios (LBBB, pre-excitation, digoxin, resting ST changes, LVH). In these patients, choose stress imaging (stress echo or myocardial perfusion imaging) or CT coronary angiography instead.
- CT coronary angiography rules disease out, it does not rule disease in. The high negative predictive value (above 95 percent for obstructive CAD) makes CTCA the test of choice for ruling out CAD in low-to-intermediate risk patients. A positive CTCA still needs functional assessment or invasive confirmation.
- Late gadolinium enhancement patterns on cardiac MRI distinguish ischaemic from non-ischaemic disease. Subendocardial or transmural LGE in a coronary territory is ischaemic (infarction). Midwall, epicardial, or diffuse LGE is non-ischaemic (myocarditis, sarcoidosis, HCM, amyloidosis). [1]
DWE high-yield: When a stem describes a patient with stable chest pain and asks for the best first-line investigation, the 2019 ESC CCS guidelines favour CT coronary angiography for most low-to-intermediate probability patients. Exercise ECG is now a lower-tier test. Stress imaging (echo or perfusion) is preferred when the patient cannot exercise or the ECG is uninterpretable. [1]
Echocardiography
Echocardiography is the workhorse of cardiac imaging — portable, radiation-free, real-time, and capable of assessing virtually every cardiac structure and function in a single study. It is the first-line imaging test for almost every cardiac presentation except suspected ischaemia. [1]
Transthoracic echocardiography (TTE)
TTE is the standard echocardiographic study. Every physician must be able to read and structure a TTE report. The five domains to assess systematically: [1]
| Domain | What to assess |
|---|---|
| Chamber size and wall thickness | LV end-diastolic diameter (normal under 5.5 cm in men, 5.0 cm in women), LV wall thickness (normal under 1.1 cm), LA size (LA volume index under 34 mL/m2), RV size and function |
| Diastolic function | Mitral inflow pattern (E and A waves), tissue Doppler (e-prime at the septal and lateral annulus), E/e-prime ratio (under 8 normal, over 14 elevated filling pressure), LA volume, TR velocity |
| Valves | Stenosis (mean gradient, valve area, velocity), regurgitation (severity by vena contracta, regurgitant volume, PISA), prosthetic valve function (gradients, presence of regurgitation or thrombus) |
| Pericardium | Effusion size and location, signs of tamponade (RA collapse, RV diastolic collapse, IVC plethora), pericardial thickening, septal bounce in constriction |
DCE short-case strategy: When presenting an echo report, use the same structure every time: "The left ventricle is normal in size with mild-moderately impaired systolic function, ejection fraction 40 percent by Simpson method, with apical and anterior hypokinesia consistent with prior infarction. The right ventricle is normal in size and function. There is no significant valvular disease and no pericardial effusion." Structure demonstrates competence. [1]
Ejection fraction classification (ESC HF Guidelines 2021, PMID 34447992)
| Category | LVEF | Key point |
|---|---|---|
| HFrEF (reduced) | 40 percent or under | Benefits from GDMT — ARNI/ACEi, beta-blocker, MRA, SGLT2 inhibitor |
| HFmrEF (mildly reduced) | 41 to 49 percent | SGLT2 inhibitors recommended; benefits of other GDMT emerging |
| HFpEF (preserved) | 50 percent or above | Diuretics for congestion; treat comorbidities; SGLT2 inhibitors recommended |
Diastolic dysfunction grading
Diastolic dysfunction is assessed on tissue Doppler because the transmitral inflow pattern alone is load-dependent: [1]
| Grade | Findings | Clinical correlate |
|---|---|---|
| Grade 1 (impaired relaxation) | E/A ratio under 0.8, E velocity under 50 cm/s, normal filling pressure (E/e-prime under 8) | Usually asymptomatic; mild |
| Grade 2 (pseudonormal) | E/A ratio 0.8 to 2, E/e-prime 9 to 14, LA enlarged | Mild-moderate symptoms |
| Grade 3 (restrictive) | E/A ratio over 2, E/e-prime over 14, short deceleration time | Severe; high filling pressures |
Examiner insight: The E/e-prime ratio is the most robust echo estimate of LV filling pressure. An E/e-prime ratio over 14 suggests elevated filling pressure. Combined with an enlarged LA and elevated TR velocity, these three findings diagnose elevated LV filling pressure with high specificity. [1]
Transoesophageal echocardiography (TOE / TEE)
TOE provides superior image quality because the oesophageal probe sits directly behind the heart, bypassing the lungs and chest wall. It is indicated when TTE is nondiagnostic or when specific structures require high-resolution imaging. [1]
| Indication | Why TOE is superior |
|---|---|
| Left atrial appendage thrombus | TTE cannot visualise the LAA reliably; TOE is mandatory before cardioversion in AF of duration over 48 hours (or unknown) |
| Prosthetic valve assessment | Mechanical and bioprosthetic valves create acoustic shadowing on TTE; TOE overcomes this to detect thrombus, vegetation, or dehiscence |
| Aortic dissection | TOE is highly sensitive and specific for the intimal flap, entry tear, and true/false lumen — used in the operating theatre or unstable patient |
| Endocarditis vegetations | TOE detects smaller vegetations (under 3 mm) and peri-valvular complications (abscess) that TTE misses; sensitivity 90 to 100 percent vs 40 to 60 percent for TTE |
| Intraoperative imaging | Real-time guidance for valve repair, ASD closure, myxoma resection |
DCE trap: Do not request a TOE for LAA thrombus if the patient has been in sinus rhythm for over 48 hours without anticoagulation — the question does not arise. The decision to perform TOE before cardioversion applies to AF of duration over 48 hours or unknown duration without adequate anticoagulation for 3 weeks prior. [1]
Stress echocardiography
Stress echo combines exercise or pharmacological stress with echocardiographic imaging to detect ischaemia-induced regional wall motion abnormalities. The principle: ischaemic myocardium becomes hypokinetic or akinetic during stress. [1]
- Stress mode: treadmill or bicycle exercise (if the patient can exercise), or dobutamine (if the patient cannot exercise — dobutamine increases heart rate and contractility).
- Ischaemia is detected as new or worsening regional wall motion abnormalities in a coronary territory during stress compared to rest.
- Diagnostic accuracy: sensitivity approximately 80 to 85 percent, specificity approximately 80 to 88 percent — better than exercise ECG.
- Viability assessment: low-dose dobutamine stress echo can detect viable but hibernating myocardium (improvement in function with low-dose dobutamine) — important for predicting recovery after revascularisation. [1]
Limitation: Stress echo requires adequate image quality and is operator-dependent. Image quality may be limited by obesity, lung disease, or poor acoustic windows. In these patients, myocardial perfusion imaging or CTCA may be preferable. [1]
Stress testing
Stress testing assesses the heart's response to increased demand — either by exercising the patient or by pharmacologically increasing myocardial oxygen demand or causing coronary vasodilation. The goal is to provoke ischaemia that is detectable on ECG, imaging, or both. [1]
Exercise ECG (exercise tolerance test)
The exercise ECG (commonly Bruce protocol) is the simplest and cheapest stress test. The patient walks on a treadmill at increasing speed and incline while the ECG, blood pressure, and symptoms are monitored continuously. [1]
Bruce protocol: 7 stages, each 3 minutes. Stage 1: 1.7 mph at 10 percent grade. Peak heart rate target is 85 percent of age-predicted maximum (220 minus age). [1]
Positive test: horizontal or downsloping ST depression of 1 mm or more, 60 to 80 ms after the J point, in two contiguous leads. ST elevation during exercise (in leads without Q waves) is highly specific for ischaemia. [1]
Diagnostic accuracy:
- Sensitivity approximately 68 percent, specificity approximately 77 percent
- Accuracy approximately 70 percent overall — moderate, not high
- Higher accuracy in higher pre-test probability populations (Bayesian theorem)
- Less accurate in women (more false positives, possibly related to oestrogen effects on ST segments and microvascular disease) [1]
When exercise ECG is NOT interpretable (the DWE contraindication list): [1]
| Scenario | Why exercise ECG fails | What to use instead |
|---|---|---|
| Left bundle branch block | LBBB causes ST changes that are concordant with the QRS and cannot be interpreted during exercise | Stress imaging (perfusion) or CTCA |
| Pre-excitation (WPW) | Delta wave and pre-excitation repolarisation changes mask ischaemic ST changes | Stress imaging or CTCA |
| Digoxin | Causes ST depression (digitalis effect) that mimics ischaemia | Stress imaging or CTCA |
| Resting ST depression over 1 mm | Baseline abnormality precludes interpretation of further change | Stress imaging or CTCA |
| LVH with strain pattern | ST-T changes from LVH confound ischaemic interpretation | Stress imaging or CTCA |
| Paced rhythm | Ventricular pacing produces LBBB-type pattern | Stress imaging or CTCA |
DWE high-yield: If a stem describes a patient with LBBB and suspected angina, the correct answer is stress imaging (preferably myocardial perfusion imaging, which is more accurate than stress echo in LBBB) or CT coronary angiography. Exercise ECG is NEVER the answer in LBBB. [1]
Absolute contraindications to exercise testing:
- Acute MI within 2 days
- Unstable angina
- Uncontrolled arrhythmias with haemodynamic compromise
- Severe symptomatic aortic stenosis
- Uncontrolled symptomatic heart failure
- Acute pulmonary embolism or infarction
- Acute myocarditis or pericarditis
- Acute aortic dissection [1]
Myocardial perfusion imaging (MPI)
MPI uses radioactive tracers (thallium-201 or technetium-99m sestamibi/tetrofosmin) to image myocardial blood flow at rest and during stress. The principle: normal coronaries dilate during stress, increasing flow; stenotic coronaries cannot dilate proportionally, producing a relative perfusion defect. [1]
SPECT (single-photon emission computed tomography):
- The most common MPI technique.
- Stress mode: exercise or vasodilator pharmacological stress (adenosine, regadenoson, dipyridamole).
- A perfusion defect that is present on stress images but normal on rest images (reversible defect) indicates ischaemia.
- A fixed defect (present on both stress and rest) indicates infarction or scar.
- Diagnostic accuracy: sensitivity approximately 85 to 90 percent, specificity approximately 70 to 80 percent. [1]
PET (positron emission tomography):
- Uses rubidium-82 or nitrogen-13 ammonia.
- Higher spatial resolution and more accurate quantification of absolute myocardial blood flow (mL/g/min).
- Can measure coronary flow reserve (CFR) — the ratio of stress to rest flow. A reduced CFR (under 2.0) indicates microvascular disease or multivessel CAD even when perfusion images appear normal (balanced ischaemia).
- Lower radiation dose than SPECT.
- Less widely available and more expensive. [1]
Examiner insight: In LBBB, myocardial perfusion imaging is preferred over exercise ECG. However, LBBB can cause septal perfusion defects (even without LAD stenosis) due to septal dyssynchrony. Vasodilator stress (rather than exercise) reduces this artefact. PET with coronary flow reserve measurement is the most accurate test in LBBB. [1]
Cardiac MRI stress perfusion
Cardiac MRI can perform stress perfusion imaging using vasodilator stress (adenosine or regadenoson). It offers:
- Superior spatial resolution to SPECT.
- No ionising radiation.
- Combined assessment of perfusion, function, viability (late gadolinium enhancement), and even coronary anatomy in a single study.
- Diagnostic accuracy comparable to or better than SPECT, with sensitivity approximately 85 to 90 percent and specificity approximately 80 to 90 percent. [1]
Modern paradigm: Cardiac MRI stress perfusion is increasingly the preferred functional test in many centres, especially in younger patients (no radiation) and when a comprehensive assessment (function, viability, perfusion) is needed in one study. [1]
Pharmacological stress agents
| Agent | Mechanism | Pros | Cons and contraindications |
|---|---|---|---|
| Adenosine | Direct A2A receptor agonist — coronary vasodilation | Short half-effect (30 sec); rapid offset | AV block, bronchospasm; contraindicated in asthma and second/third degree AV block without pacemaker |
| Regadenoson | Selective A2A receptor agonist | Fewer side effects (less bronchospasm); single bolus injection; preferred in mild-moderate asthma | Can still cause dyspnoea and AV block; expensive |
| Dipyridamole | Indirect vasodilator — blocks adenosine reuptake | Inexpensive | Longer half-effect; more side effects; can be reversed with aminophylline |
| Dobutamine | Beta-1 agonist — increases heart rate and contractility (ischaemia by demand) | Can be used when vasodilators are contraindicated (asthma, AV block) | More arrhythmias; contraindicated in severe hypertension, severe AS, HOCM |
DWE trap: Adenosine is contraindicated in asthma and high-degree AV block. Regadenoson is the safer alternative in mild asthma. In severe asthma or AV block, dobutamine stress (with imaging) is the alternative. Remember this when a stem offers a patient with asthma needing stress testing. [1]
CT coronary angiography (CTCA)
CT coronary angiography is a non-invasive anatomical test that visualises the coronary arteries using contrast-enhanced computed tomography. It has revolutionised the investigation of stable chest pain over the past decade. [1]
Diagnostic performance
CTCA has two defining performance characteristics: [1]
| Metric | Value | Clinical implication |
|---|---|---|
| Negative predictive value | Above 95 percent for obstructive CAD (over 50 percent stenosis) | Excellent at ruling out CAD — a negative CTCA effectively excludes obstructive disease |
| Positive predictive value | 50 to 80 percent (lower in calcified arteries) | Moderate — a positive CTCA overestimates stenosis severity due to calcium blooming and may need confirmation |
Key principle: CTCA is a rule-out test. It is most useful in low-to-intermediate pre-test probability patients where a negative result avoids further testing and a positive result prompts functional assessment or invasive angiography. [1]
Calcium score (coronary artery calcium, CAC)
The calcium score (Agatston score) is a non-contrast CT measurement of coronary artery calcification: [1]
| Score | CAD likelihood and risk |
|---|---|
| 0 | No detectable calcium — very low risk of obstructive CAD; excellent prognosis |
| 1 to 99 | Mild calcification — moderate risk |
| 100 to 399 | Moderate calcification — high risk |
| Over 400 | Extensive calcification — very high risk; consider invasive assessment |
Prognostic value: A calcium score of 0 has powerful prognostic value — the 10-year event rate is very low (under 1 percent in most studies). In selected asymptomatic or low-risk patients, a CAC of 0 can safely defer statin therapy. However, a CAC of 0 does not exclude non-calcified plaque, so it should not be used alone in symptomatic patients. [1]
When to use CTCA
The 2019 ESC CCS guidelines (PMID 31504439) recommend CTCA as the first-line test in patients with:
- Low to intermediate pre-test probability of CAD (approximately 15 to 50 percent)
- Stable chest pain (suspected chronic coronary syndrome)
- Inconclusive or uninterpretable functional tests
- Suspected coronary anomalies
- Evaluation prior to non-cardiac surgery in selected patients [1]
When CTCA is NOT preferred:
- High pre-test probability (over 50 to 65 percent) — functional imaging or direct invasive angiography is more efficient
- Severe coronary calcification (calcium score over 400) — calcium blooming degrades image quality and diagnostic accuracy
- Inability to cooperate with breath-hold instructions or lie flat
- Severe renal impairment (contrast contraindication)
- Significant tachyarrhythmia or inability to achieve low heart rate (beta-blocker resistant) [1]
Key trials
SCOT-HEART (PMID 25788230 initial, PMID 30145934 5-year): In 4,146 patients with stable chest pain, the addition of CTCA to standard care increased diagnostic certainty, changed management (more preventive therapy and revascularisation), and reduced fatal and non-fatal MI by 41 percent over 5 years (2.3 percent vs 3.9 percent, HR 0.59). This trial drove the adoption of CTCA as first-line for stable chest pain. [1]
PROMISE (PMID 25773919): In 10,003 symptomatic patients, initial CTA was compared with functional testing (exercise ECG, nuclear stress, or stress echo). No significant difference in the composite primary outcome (3.3 percent vs 3.0 percent, HR 1.04). CTA led to more catheterisations showing obstructive CAD and more preventive therapy. The trial established that CTA is a safe, equivalent alternative to functional testing as an initial strategy. [1]
DCE long-case integration: In a long case presenting with stable angina, the appropriate initial investigation is CTCA (per ESC 2019). If CTCA shows obstructive disease, proceed to functional assessment or invasive angiography depending on symptoms and risk. If CTCA shows non-obstructive disease, treat medically. If CTCA is equivocal, proceed to stress imaging. [1]
Coronary angiography
Invasive coronary angiography remains the gold standard for the anatomical diagnosis of coronary artery disease. It provides definitive visualisation of coronary stenoses and allows immediate intervention (PCI) when needed. [1]
What it does
Coronary angiography involves catheterisation of the coronary ostia (usually via radial or femoral artery access) and injection of iodinated contrast under fluoroscopy. It provides:
- Luminal visualisation of coronary stenoses (percentage diameter reduction)
- Collateral vessel assessment
- The opportunity for intracoronary imaging (IVUS — intravascular ultrasound, or OCT — optical coherence tomography) and physiological assessment (FFR — fractional flow reserve)
- The option for immediate PCI (stenting) if a significant lesion is found [1]
Indications
| Indication | Setting |
|---|---|
| Acute coronary syndrome (STEMI, NSTEMI, unstable angina) | Emergency or urgent — do not need a positive stress test first |
| Positive non-invasive test (stress imaging, CTCA showing obstructive disease) | Elective — to confirm and revascularise |
| High-risk stable angina not controlled by medical therapy | Elective — ISCHEMIA trial supports initial conservative therapy for many, but refractory symptoms warrant angiography |
| Pre-valvular surgery in patients with cardiac risk factors | To exclude concomitant CAD before valve surgery |
| Suspected coronary anomaly | CTCA may suffice; angiography if intervention needed |
| Cardiogenic shock or post-arrest | Emergency — to exclude acute ischaemic cause |
| Heart failure with suspected ischaemic aetiology | To define coronary anatomy and viability |
DWE high-yield: Invasive coronary angiography is indicated without prior non-invasive testing in: ACS (all types), cardiogenic shock, and high-risk presentations. For stable chest pain, the pathway is CTCA or stress imaging first, then angiography if positive. The ISCHEMIA trial (PMID 32227755) supports an initial conservative strategy for many stable patients with moderate-severe ischaemia — invasive management does not reduce death or MI compared with optimal medical therapy, though it improves symptom control. [1]
Risks
- Contrast-induced nephropathy (risk highest with eGFR under 60, diabetes, dehydration)
- Access site complications (bleeding, pseudoaneurysm, AV fistula — less with radial access)
- Stroke (under 0.5 percent)
- MI (under 0.5 percent)
- Mortality (under 0.1 percent)
- Radiation exposure (2 to 10 mSv) [1]
FFR (fractional flow reserve)
FFR is a physiological (not anatomical) measurement of coronary stenosis severity. A pressure wire is passed across the stenosis, and the ratio of distal coronary pressure to aortic pressure is measured during hyperaemia (adenosine): [1]
- FFR under 0.80 — functionally significant stenosis — PCI improves outcomes (FAME trial)
- FFR 0.80 or above — not functionally significant — defer PCI; medical therapy [1]
Examiner insight: Angiography tells you what the stenosis looks like; FFR tells you what it does. Intermediate stenoses (40 to 70 percent) on angiography should be assessed with FFR before committing to PCI — this is the principle of physiological guidance and is now standard of care. [1]
Cardiac MRI
Cardiac MRI (CMR) is the gold standard for myocardial tissue characterisation. Its unique capability is late gadolinium enhancement (LGE) — the ability to distinguish scarred or infiltrated myocardium from normal myocardium based on how gadolinium distributes after contrast injection. [1]
Late gadolinium enhancement (LGE) — the key to tissue characterisation
Gadolinium accumulates in tissues with expanded extracellular space (scar, fibrosis, infiltration, oedema). The pattern of LGE is the single most discriminating finding for differentiating cardiomyopathies: [1]
| LGE pattern | Distribution | Diagnosis |
|---|---|---|
| Subendocardial or transmural in a coronary territory | Obeying the endocardium-to-epicardium gradient | Ischaemic — myocardial infarction (LAD, RCA, LCx territory) |
| Midwall (non-ischaemic) | Intramural, not touching the endocardium | Non-ischaemic — dilated cardiomyopathy, myocarditis (septal), sarcoidosis, Chagas |
| Epicardial or patchy | Outer myocardium, may involve the lateral wall | Myocarditis (lateral epicardial), sarcoidosis, Chagas disease |
| Patchy, focal at RV insertion points (septum) | RV-LV insertion point | Hypertrophic cardiomyopathy (HCM) |
| Diffuse, subendocardial circumferential | Global, difficult to null (no normal reference) | Cardiac amyloidosis |
| RV insertion point or midwall | Non-ischaemic patterns | Consider sarcoidosis, HCM |
DWE high-yield discriminator: The pattern that distinguishes ischaemic from non-ischaemic cardiomyopathy on cardiac MRI is the subendocardial involvement. Ischaemic infarction always starts at the subendocardium (the region most vulnerable to ischaemia, furthest from the epicardial coronaries) and extends outward toward the epicardium in a coronary territory. Non-ischaemic LGE (myocarditis, sarcoidosis, HCM, amyloid) does NOT involve the subendocardium in this pattern — it is midwall, epicardial, or diffuse. [1]
Viability assessment
CMR with LGE is the most accurate technique for assessing myocardial viability. The principle: the transmural extent of LGE predicts the likelihood of functional recovery after revascularisation. [1]
| LGE transmurality | Likelihood of functional recovery after revascularisation |
|---|---|
| Under 25 percent of wall thickness | High likelihood of recovery — viable myocardium |
| 25 to 50 percent | Intermediate likelihood |
| Over 50 percent | Low likelihood of recovery — predominantly scar; revascularisation unlikely to improve function |
Clinical application: In a patient with ischaemic cardiomyopathy being considered for revascularisation, CMR viability assessment helps predict which segments will recover. Segments with less than 25 percent transmural LGE are viable and should be revascularised. Segments with over 50 percent LGE are unlikely to recover and may not benefit from revascularisation. [1]
Cardiomyopathy phenotyping
CMR is the definitive test for differentiating cardiomyopathy phenotypes when echo is equivocal: [1]
| Cardiomyopathy | CMR hallmarks |
|---|---|
| Hypertrophic cardiomyopathy (HCM) | Asymmetric LVH (basal septum), small LV cavity, LGE at RV insertion points (prognostic — over 15 percent LV mass predicts SCD risk) |
| Cardiac amyloidosis | Diffuse subendocardial or transmural LGE, difficulty nulling the myocardium, increased native T1 and ECV, LVH with low voltages on ECG, raised NT-proBNP |
| Cardiac sarcoidosis | Patchy midwall or epicardial LGE (basal septum, lateral wall), aneurysms, conduction disease, associated pulmonary/systemic sarcoidosis |
| Myocarditis | Lateral epicardial or midwall septal LGE, raised T1/T2 (oedema), pericardial effusion |
| ARRVC (arrhythmogenic RV cardiomyopathy) | RV dilatation and dysfunction, RV free wall fat and LGE, epsilon waves on ECG |
| Iron overload cardiomyopathy | Reduced T2 star (iron deposition), reduced T1, thickened LV wall with systolic dysfunction — thalassaemia, haemochromatosis |
Myocarditis — Lake Louise criteria (2018 update, PMID 30545455)
The Lake Louise criteria were originally proposed in 2009 (requiring 2 of 3 qualitative markers: T2 oedema, early gadolinium enhancement, or LGE). The 2018 update modernised the criteria to incorporate quantitative parametric mapping: [1]
2018 Lake Louise Criteria — requires BOTH:
- At least one T1-based marker (non-ischaemic myocardial injury):
- Abnormal native T1 mapping, OR
- Increased extracellular volume (ECV), OR
- Positive LGE (midwall septal or lateral epicardial)
- At least one T2-based marker (myocardial oedema):
- Abnormal T2 mapping, OR
- Regional high signal intensity on T2-weighted imaging [1]
Supportive features: reduced LV systolic function, regional wall motion abnormalities, pericardial effusion, pericardial LGE. [1]
Examiner insight: The 2018 Lake Louise update removed early gadolinium enhancement (EGE) because of poor diagnostic performance and replaced the qualitative approach with quantitative T1 and T2 mapping. The sensitivity increased from approximately 60 percent (2009 criteria) to approximately 88 percent (2018 criteria). When a stem describes CMR findings in suspected myocarditis, state whether the T1 and T2 criteria are met. [1]
Cardiac amyloidosis
Cardiac amyloidosis is increasingly recognised as a cause of heart failure with preserved ejection fraction, and CMR plays a central role in its diagnosis: [1]
- Echo clues: concentric LVH with low voltages on ECG (the discordance between thick walls and low QRS voltage is suggestive), bi-atrial enlargement, thickened interatrial septum and valves, restrictive filling pattern, pericardial effusion.
- CMR findings: diffuse subendocardial LGE (difficult to null — no normal reference myocardium), elevated native T1 and extracellular volume fraction (reflecting amyloid infiltration of the extracellular space).
- Confirmation: technetium-99m pyrophosphate (99mTc-PYP) or DPD scintigraphy for transthyretin (ATTR) amyloidosis — grade 2 or 3 cardiac uptake is diagnostic in the absence of a monoclonal protein. Serum free light chains and serum/urine immunofixation to exclude AL amyloidosis (which requires biopsy confirmation and different treatment). [1]
DWE high-yield: In a stem describing a man over 65 with heart failure, concentric LVH on echo, low voltages on ECG, and raised NT-proBNP, consider cardiac amyloidosis (ATTR). The next step is CMR and technetium pyrophosphate scanning. This is increasingly tested because disease-modifying therapy (tafamidis for ATTR) is available. [1]
Cardiac CT (non-coronary applications)
Beyond coronary angiography, cardiac CT has several important applications: [1]
| Application | Role |
|---|---|
| Coronary anatomy | CTCA — covered above |
| Congenital coronary anomalies | Anomalous origin (ALCAPA, anomalous coronary from opposite sinus), coronary fistula, myocardial bridging |
| Aortic dissection | CT angiography of the aorta — type A (ascending, surgical) vs type B (descending, medical). Preferred over TOE in the stable patient |
| Pericardial calcification | Constrictive pericarditis — CT elegantly demonstrates pericardial calcification (especially in the atrioventricular groove) |
| Cardiac masses | Thrombus, tumour (myxoma), tumour extension (renal cell carcinoma via IVC into RA) |
| Pre-procedural planning | TAVI (transcatheter aortic valve implantation) sizing, left atrial anatomy before AF ablation |
Electrophysiology studies and ablation
Electrophysiology (EP) studies involve catheter-based recording of intracardiac electrograms to define the mechanism and substrate of arrhythmias. They are both diagnostic and therapeutic (ablation). [1]
Diagnostic EP studies
| Arrhythmia | What EP study reveals |
|---|---|
| SVT (AVNRT, AVRT, atrial tachycardia) | Mechanism — reentrant circuit, accessory pathway (manifest or concealed), focal origin. Enables ablation |
| VT | Substrate (scar-related reentry), origin of focal VT, feasibility of ablation |
| Unexplained syncope with bifascicular block | HV interval (conduction time through the His-Purkinje system) — prolonged HV over 70 ms predicts high-grade AV block, supporting pacemaker |
| Wide complex tachycardia of uncertain origin | Differentiates VT from SVT with aberrancy |
Ablation
| Arrhythmia | Role of ablation |
|---|---|
| AV node reentrant tachycardia (AVNRT) | Slow pathway ablation — cure rate over 95 percent; first-line for recurrent SVT |
| AV reentrant tachycardia (AVRT, WPW) | Accessory pathway ablation — cure rate over 95 percent |
| Atrial fibrillation | Pulmonary vein isolation — reduces AF burden, particularly in paroxysmal AF; rate control for rhythm control in selected patients |
| Atrial flutter | Cavotricuspid isthmus ablation — cure rate over 90 percent for typical flutter |
| VT | Substrate ablation in structural heart disease (post-MI, ARVC); reduces ICD shocks |
| AV node ablation | For rate control in AF when pharmacological rate control fails — "ablate and pace" (ablate the AV node, implant a pacemaker, patient is then pacemaker-dependent) |
DCE insight: "Ablate and pace" (AV node ablation with pacemaker implantation) is a palliative strategy for AF with uncontrolled ventricular rate despite maximal drug therapy. It does not cure the AF — it electrically disconnects the atria from the ventricles — but it provides excellent rate control. The patient becomes pacemaker-dependent. It is reserved for patients who have failed or cannot tolerate rate-controlling drugs and are not candidates for pulmonary vein isolation. [1]
Implantable devices
| Device | Indication | What it does |
|---|---|---|
| Pacemaker | Symptomatic bradycardia (sinus node dysfunction, high-degree AV block), alternating bifascicular block, carotid sinus hypersensitivity | Senses intrinsic rhythm and paces when the rate falls below a programmed lower limit |
| ICD (implantable cardioverter-defibrillator) | Secondary prevention (survived VT/VF arrest), primary prevention (HFrEF with LVEF under 35 percent despite over 3 months GDMT, HCM with high SCD risk, ARVC, long QT, Brugada) | Detects and terminates VT/VF with anti-tachycardia pacing or shock |
| CRT (cardiac resynchronisation therapy) | HFrEF (LVEF under 35 percent) with LBBB and QRS over 150 ms, despite optimal medical therapy | Biventricular pacing resynchronises dyssynchronous contraction; improves symptoms and survival |
| Implantable loop recorder (ILR) | Unexplained syncope or palpitations with infrequent events not captured on Holter; risk stratification in selected patients | Continuously monitors the ECG for up to 3 years; automatically records arrhythmias; patient-activated recording |
DWE high-yield on CRT: CRT is indicated in HFrEF (LVEF under 35 percent), NYHA class II to IV, on optimal medical therapy for at least 3 months, with LBBB and QRS over 150 ms. The benefit is greatest with LBBB morphology and wider QRS. Non-LBBB patterns (RBBB) or narrower QCS derive less benefit. CRT-P (pacemaker) and CRT-D (with defibrillator) are available — the choice depends on the indication for ICD back-up. [1]
DCE long-case integration: In a heart failure long case, always state the LVEF, the QRS duration and morphology, and whether CRT is indicated. This demonstrates integrated assessment. "Given the LVEF of 30 percent with LBBB and QRS of 160 ms despite 4 months of optimal quadruple therapy, this patient meets criteria for CRT-D implantation." [1]
Biomarkers
High-sensitivity troponin
Troponin (I or T) is the gold standard biomarker for myocardial injury. High-sensitivity assays (hs-cTn) detect troponin at much lower concentrations than older assays, enabling earlier rule-out of MI. [1]
Key principles: [1]
| Principle | Detail |
|---|---|
| What troponin measures | Myocardial necrosis or injury (not ischaemia itself) — any cause of myocyte death releases troponin |
| High-sensitivity advantages | Detectable in most healthy individuals; enables faster rule-out (1 to 2 hour protocols); higher sensitivity (over 95 percent) but lower early specificity |
| Rising pattern | A rise and/or fall of troponin with at least one value above the 99th percentile upper reference limit defines acute myocardial injury |
| Type 1 vs Type 2 MI | Type 1 — atherothrombotic plaque rupture (need PCI). Type 2 — supply-demand mismatch (tachyarrhythmia, hypotension, sepsis, severe anaemia) — treat the cause |
| Universal definition of MI | Acute myocardial injury (rise/fall of troponin) PLUS clinical evidence of ischaemia (symptoms, ECG changes, imaging) |
DWE trap: Troponin is elevated in many conditions besides MI — PE, sepsis, renal failure, tachyarrhythmias, myocarditis, heart failure, stroke. An elevated troponin alone does NOT diagnose MI — you need a rise/fall pattern AND evidence of ischaemia. The most common DWE error is treating an isolated troponin elevation in a patient with sepsis and AF as a type 1 MI and sending them for catheterisation. [1]
Causes of elevated troponin without MI:
- Sepsis and critical illness
- Renal failure (reduced clearance)
- Tachyarrhythmias (AF with rapid ventricular response, SVT)
- Acute pulmonary embolism (RV strain)
- Acute decompensated heart failure
- Myocarditis and pericarditis
- Stroke and subarachnoid haemorrhage
- Cardiac contusion
- Extreme exercise (ultramarathon) [1]
NT-proBNP and BNP
BNP (B-type natriuretic peptide) and NT-proBNP are released by ventricular myocytes in response to wall stretch. They are the key biomarkers for heart failure. [1]
Role in heart failure diagnosis (ESC HF Guidelines 2021, PMID 34447992): [1]
| Setting | NT-proBNP threshold |
|---|---|
| Acute heart failure (ED) — rule-out | Under 300 ng/L — heart failure unlikely |
| Acute HF — rule-in | Over 1000 ng/L in patients over 75 years; over 1800 ng/L is strongly supportive |
| Chronic HF (outpatient) — rule-out | Under 125 ng/L — heart failure unlikely |
Key principle: NT-proBNP is a rule-out test for heart failure. A normal NT-proBNP makes heart failure very unlikely, especially in the acute setting. However, NT-proBNP is elevated in many non-HF conditions (AF, renal failure, PE, sepsis) and can be paradoxically lower in obesity (dilutional effect). It is a triage tool — not a standalone diagnosis. Echocardiography confirms the diagnosis. [1]
D-dimer
D-dimer is a fibrin degradation product used primarily in the diagnosis of venous thromboembolism (VTE — DVT and PE). [1]
- Role in PE diagnosis: In a patient with low or moderate pre-test probability (PERC or Wells score), a negative D-dimer (under 500 micrograms/L, or age-adjusted: age times 10 in patients over 50) effectively rules out PE — no imaging needed.
- Limitation: D-dimer is elevated in many conditions (pregnancy, malignancy, infection, inflammation, post-surgery, age). It has high sensitivity but low specificity. A positive D-dimer requires imaging (CTPA or V/Q scan) to confirm PE.
- Age-adjusted cutoff: In patients over 50, use age times 10 as the cutoff (e.g., a 70-year-old has a cutoff of 700 micrograms/L). This improves specificity without sacrificing sensitivity in older patients. [1]
DWE high-yield: In a stem describing a patient with pleuritic chest pain and dyspnoea, the investigation pathway is: assess pre-test probability (Wells score), if low use PERC rule (if all negative, no testing needed), if not PERC negative or moderate probability, check D-dimer; if D-dimer is negative, PE is excluded; if positive, perform CTPA. [1]
When to use which test — integrated clinical decision-making
The key skill examiners test is not knowing what each test does, but knowing which test to choose for a specific patient. The decision depends on the clinical question, the pre-test probability, the patient's characteristics (ability to exercise, ECG interpretability, renal function, body habitus), and the downstream consequence of the result. [1]
Stable chest pain — the decision algorithm

| Clinical scenario | Best first-line test | Rationale |
|---|---|---|
| Low-intermediate risk, interpretable ECG, can exercise | CTCA (ESC 2019 preferred) or stress imaging | CTCA has highest diagnostic accuracy and rules out disease |
| Low-intermediate risk, LBBB or pre-excitation or digoxin | Stress imaging (MPI preferred) or CTCA | Exercise ECG is uninterpretable |
| Low-intermediate risk, cannot exercise | Pharmacological stress imaging or CTCA | Exercise not feasible; CTA needs beta-blocker for rate control |
| High risk (typical angina, high pre-test probability over 50 percent) | Invasive coronary angiography or stress imaging | High likelihood of obstructive disease; angiography allows definitive treatment |
| Young patient, atypical chest pain, low risk | CTCA or calcium score | Rule out CAD with minimal radiation |
| High calcium score (over 400) on prior scan | Invasive angiography or stress imaging | CTCA image quality degraded by calcium; functional assessment preferred |
Acute chest pain
| Clinical scenario | Best investigation | Rationale |
|---|---|---|
| Ongoing chest pain with ST elevation | Primary PCI — do not wait | STEMI — emergency reperfusion |
| Suspected ACS without ST elevation | High-sensitivity troponin at 0 and 1 to 2 hours (or 0 and 3 hours) | Rule in/out NSTEMI; invasive strategy if high-risk |
| Low-risk chest pain, troponin negative | CTCA in the ED | Ruled out CAD — safe discharge |
| Suspected PE | D-dimer, then CTPA if positive | Rule out PE |
Suspected heart failure
| Clinical scenario | Best investigation | Rationale |
|---|---|---|
| Acute dyspnoea, suspected HF | NT-proBNP, then echocardiography | NT-proBNP rules out HF; echo confirms and defines phenotype |
| New heart failure, suspected ischaemic | Echo, then coronary angiography | Define LVEF, exclude valvular cause; define coronary anatomy |
| Heart failure with nondiagnostic echo | Cardiac MRI | Tissue characterisation — ischaemic vs non-ischaemic, infiltrative, inflammatory |
Exam synthesis — high-yield discriminators

| Question | Discriminator |
|---|---|
| Is this LGE pattern ischaemic or non-ischaemic? | Subendocardial in a coronary territory = ischaemic. Midwall, epicardial, or diffuse = non-ischaemic |
| Which stress test for a patient with LBBB? | Stress imaging (MPI or stress MRI), NOT exercise ECG. CTCA is an alternative if pre-test probability is low-intermediate |
| CTCA shows 30 percent stenosis — what next? | Medical management. CTCA has high NPV; under 50 percent stenosis is non-obstructive |
| CTCA shows 70 percent stenosis in the LAD — what next? | Functional assessment (FFR) or invasive angiography. CTCA overestimates stenosis in calcified arteries |
| Which patients need TOE before cardioversion? | AF over 48 hours or unknown duration, not adequately anticoagulated for 3 weeks. TOE to exclude LAA thrombus |
| Troponin elevated in sepsis — is this an MI? | Not necessarily. Myocardial injury requires a rise/fall AND evidence of ischaemia. Sepsis causes type 2 injury. Treat the sepsis |
| Patient with HFrEF, LVEF 30 percent, LBBB, QRS 160 ms — what device? | CRT-D (cardiac resynchronisation therapy with defibrillator). Meets all criteria |
Regional guideline anchoring
- 2019 ESC Guidelines for chronic coronary syndromes (Knuuti et al, PMID 31504439) — the primary guideline for stable chest pain investigation. Favours CTCA as first-line for low-intermediate pre-test probability. Note: updated by the 2024 ESC CCS guidelines, which further refine the clinical likelihood model.
- 2021 ESC Guidelines for heart failure (McDonagh et al, PMID 34447992) — defines HF phenotypes by LVEF, recommends NT-proBNP for diagnosis and echo for phenotyping.
- NICE Chest Pain Guideline (NG95/2016, updated) — recommends CTCA as the first-line investigation for stable chest pain in the UK, driven by SCOT-HEART evidence. [1]
Summary of verified references
- Knuuti J, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 2020;41(3):407-77. PMID 31504439.
- Douglas PS, et al. Outcomes of anatomical versus functional testing for coronary disease (PROMISE). N Engl J Med 2015;372:1291-300. PMID 25773919.
- SCOT-HEART Investigators. Coronary CT angiography and 5-year risk of MI. N Engl J Med 2018;379:1317-26. PMID 30145934.
- SCOT-HEART Investigators. CT coronary angiography in patients with suspected angina. Lancet 2015;385:2333-41. PMID 25788230.
- Ferreira VM, et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: Lake Louise update. J Am Coll Cardiol 2018;72(24):3158-76. PMID 30545455.
- McDonagh TA, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021;42(36):3599-726. PMID 34447992.
- Maron DJ, et al. Initial invasive or conservative strategy for stable coronary disease (ISCHEMIA). N Engl J Med 2020;382:1395-407. PMID 32227755. [1]
All PMIDs were verified live via web search before entry. Primary guideline sources: ESC CCS 2019; ESC Heart Failure 2021; Lake Louise Criteria 2018; SCOT-HEART and PROMISE trials. [1]
References
- [1]Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes Eur Heart J, 2020.PMID 31504439
- [2]Douglas PS, Hoffmann U, Patel MR, et al. Outcomes of anatomical versus functional testing for coronary artery disease N Engl J Med, 2015.PMID 25773919
- [3]SCOT-HEART Investigators Coronary CT Angiography and 5-Year Risk of Myocardial Infarction N Engl J Med, 2018.PMID 30145934
- [4]SCOT-HEART Investigators CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial Lancet, 2015.PMID 25788230
- [5]Ferreira VM, Schulz-Menger J, Holmvang G, et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations J Am Coll Cardiol, 2018.PMID 30545455
- [6]McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure Eur Heart J, 2021.PMID 34447992
- [7]Maron DJ, Hochman JS, Reynolds HR, et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease N Engl J Med, 2020.PMID 32227755