Phys · cardiovascular
Cardiovascular Prevention and Rehabilitation
Also known as cardiovascular risk assessment · absolute cardiovascular risk · lipid management · statin therapy · LDL targets · primary prevention · secondary prevention · cardiac rehabilitation · familial hypercholesterolaemia · statin intolerance
Consultant-physician-depth guide to cardiovascular prevention — absolute risk assessment, lipid targets and the statin-to-PCSK9 ladder, statin intolerance and the nocebo problem, triglycerides, Lp(a) and familial hypercholesterolaemia, lifestyle prescription with numbers, the post-ACS secondary prevention bundle, and cardiac rehabilitation — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Cardiovascular Prevention and Rehabilitation

The answer first
Prevention is absolute-risk medicine: you treat a person's probability of an event, not a number on a lipid panel. Four rules carry you through almost every DWE question, every DCE long case, and every prevention clinic decision [1]:
- Treat the risk, not the number. A statin is prescribed against calculated absolute cardiovascular risk — or against established disease, familial hypercholesterolaemia, or another condition that makes the patient high-risk by definition. The LDL value alone never answers "should I treat?" [1] [5].
- LDL lowering is dose-dependent, additive and boringly reliable. Each 1.0 mmol/L fall in LDL cuts major vascular events by about a fifth, whatever drug achieves it — statin, ezetimibe, or PCSK9 antibody. Start high-intensity statin, then climb the ladder to target [5] [8] [9].
- Secondary prevention is a bundle, and rehabilitation is part of it. Post-ACS, the statin, the antiplatelet, the beta-blocker, the ACE inhibitor and the cardiac rehabilitation referral each carry event-reduction evidence. Forgetting the referral is forgetting a mortality intervention [15] [22] [23].
- Primary prevention in the elderly and low-risk is where harm hides. Aspirin for primary prevention in people over 70 causes more bleeding than benefit; statin decisions in low-risk people need absolute numbers, not relative ones [16].
Treat the risk, not the number
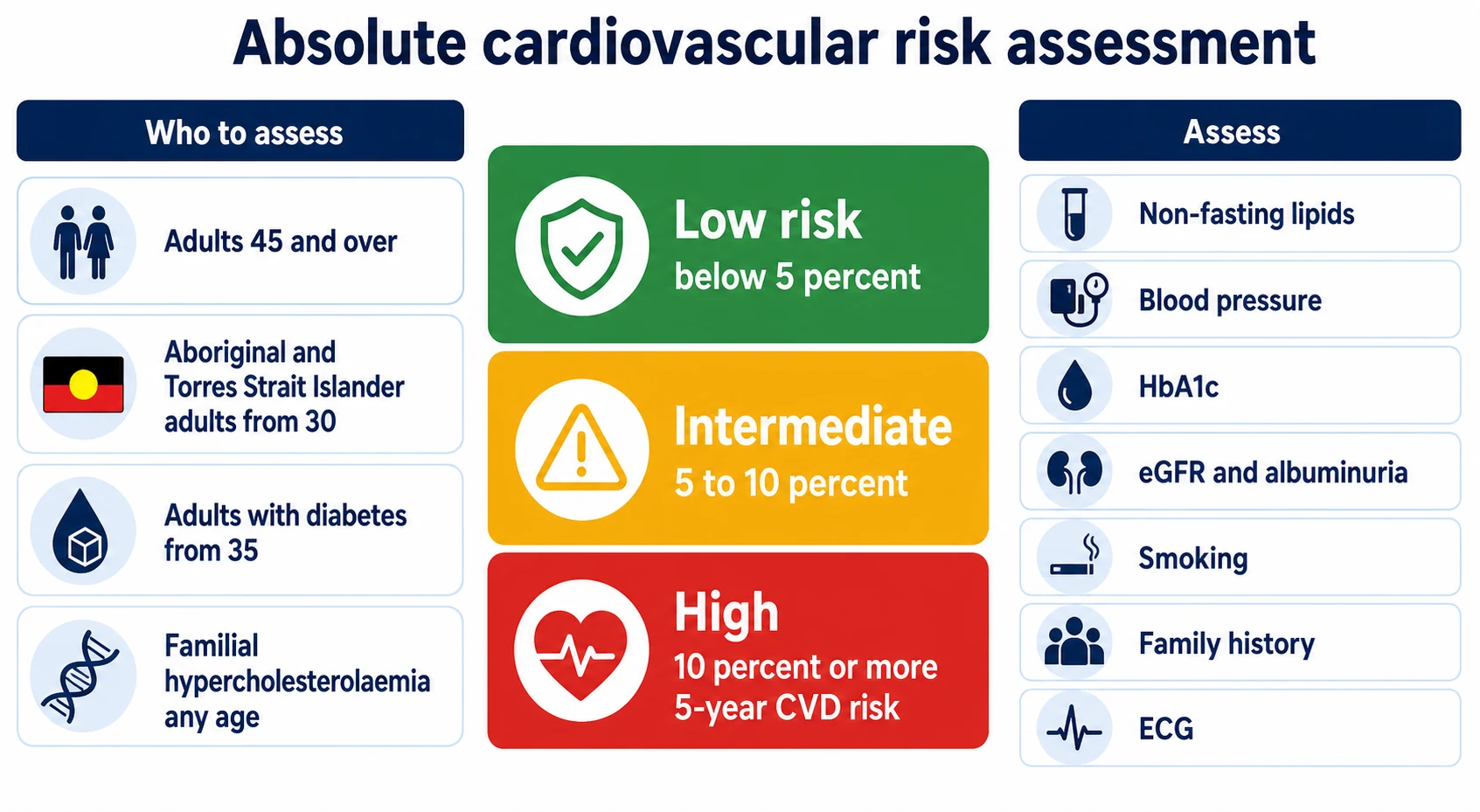
Absolute risk is the probability of a cardiovascular event over a defined period, computed from the whole risk-factor profile rather than any single factor. It is the only honest way to decide preventive treatment, because the benefit of a statin is proportional to baseline risk while the harms are roughly constant — the same drug that saves one in twenty high-risk patients over a decade does almost nothing measurable for a low-risk one [1] [5].
Who to assess. The 2023 Australian guideline recommends assessing absolute risk in all adults from 45 years (from 30 years for Aboriginal and Torres Strait Islander adults, and from 35 years for people with diabetes), using the AusCVDRisk calculator — a PREDICT-derived, Australian-recalibrated equation that replaced the old Framingham-derived NVDPA charts [1]. QRISK3 does the same job in the UK and adds inputs the older tools lacked — chronic kidney disease, atrial fibrillation, corticosteroids, severe mental illness and erectile dysfunction — validated in more than ten million patients [2].
The bands. Australia now uses three five-year risk categories: low (below 5%), intermediate (5% to below 10%), and high (10% or more). High risk earns blood-pressure and lipid-modifying treatment alongside lifestyle; intermediate risk earns a full discussion with reclassification factors (coronary artery calcium, Lp(a), family history, ethnicity, social deprivation) before deciding [1]. NICE expresses the same logic through QRISK3: offer atorvastatin 20 mg when ten-year risk reaches 10% [2].
Communicating risk is half the consultation. Percentages mean little to patients; "of 100 people like you, about 12 will have a heart attack or stroke in the next ten years — this tablet brings that to about 9" lands better. Shared decision-making around that number is a formal recommendation of the Australian guideline, not a courtesy [1].
Lipids: the treatment ladder
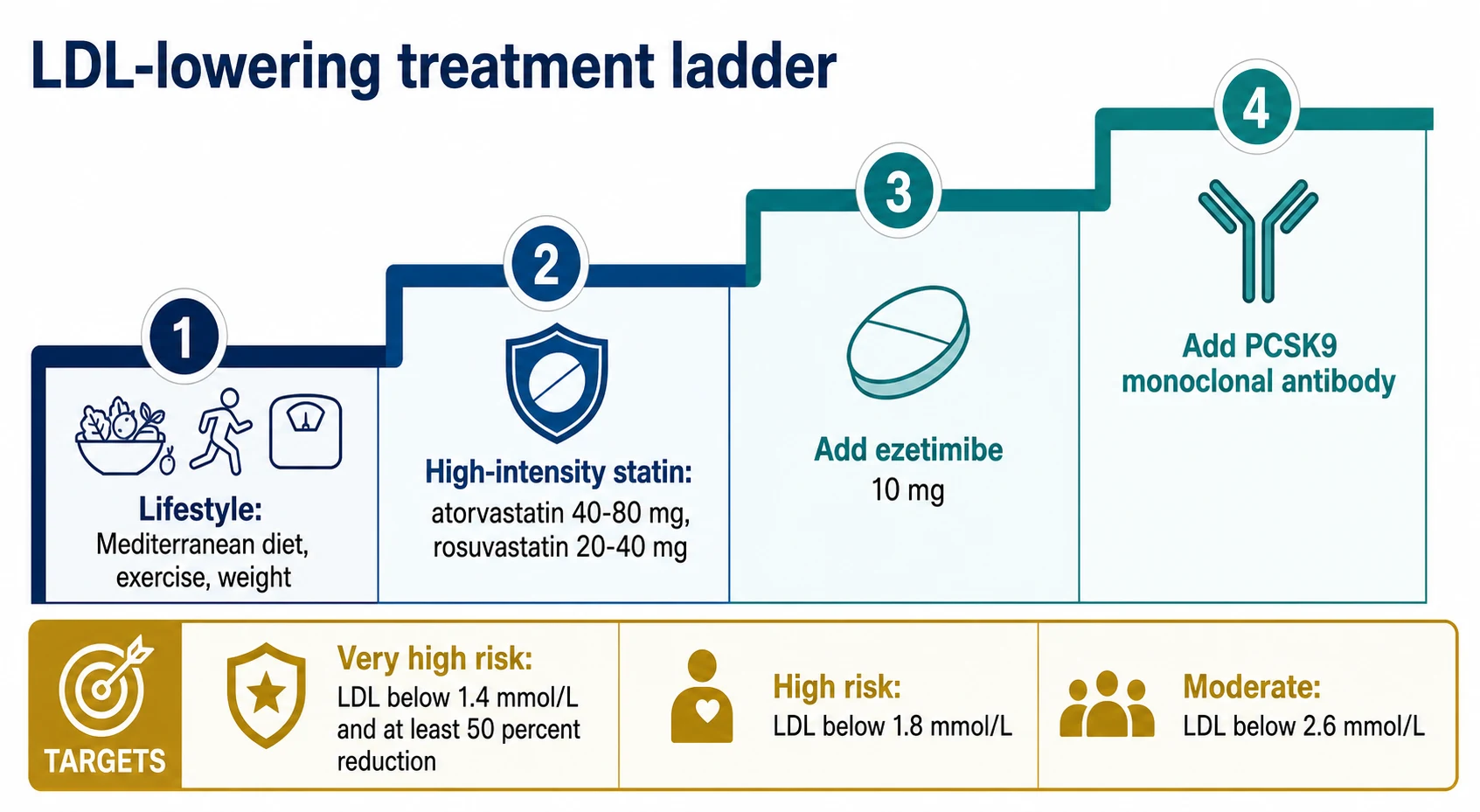
Lifestyle is the foundation for everyone; drugs are layered on by risk. The ladder has four rungs, and each rung has a named trial behind it [5] [8] [9].
Rung 1 — statins, at the right intensity. Statins block HMG-CoA reductase, upregulate hepatic LDL receptors, and remain the cheapest, most proven cardiovascular drug after aspirin in secondary prevention. High-intensity dosing (atorvastatin 40–80 mg or rosuvastatin 20–40 mg daily) lowers LDL by 50% or more and is the default after ACS and in very-high-risk patients; moderate intensity (atorvastatin 10–20 mg, rosuvastatin 5–10 mg, simvastatin 20–40 mg) lowers LDL by roughly a third and suits many primary-prevention patients [6] [7]. More intensive regimens win: in the CTT 2010 meta-analysis, pushing LDL a further 0.5 mmol/L down with intensive versus standard statin dosing cut major vascular events a further 15% [6].
Targets give the ladder its direction. The ESC prevention framework sets LDL goals by risk tier: very high risk — below 1.4 mmol/L and at least a 50% reduction from baseline; high risk — below 1.8 mmol/L; moderate risk — below 2.6 mmol/L. Australian practice tracks the same logic, checking lipids 6–8 weeks after starting or changing therapy [1] [6].
Rung 2 — ezetimibe. IMPROVE-IT randomised 18,144 post-ACS patients to simvastatin 40 mg with or without ezetimibe 10 mg: median LDL fell to 1.4 versus 1.8 mmol/L, and the composite endpoint fell with it (absolute benefit about 2% over seven years). The trial matters beyond its modest effect size — it proved that a non-statin LDL-lowering drug reduces events in proportion to LDL lowering, validating LDL as the causal target [8] [5].
Rung 3 — PCSK9 monoclonal antibodies. Evolocumab 140 mg every two weeks (FOURIER, 27,564 patients with established ASCVD on statins) drove median LDL to 0.78 mmol/L and cut the key composite of cardiovascular death, MI or stroke by 20% [9]. Alirocumab after recent ACS (ODYSSEY OUTCOMES) cut the primary composite by 15% with a suggestion of mortality benefit in those treated longest and with baseline LDL at or above 2.6 mmol/L [10]. These drugs are for the patient still above target — or with recurrent events — despite maximally tolerated oral therapy; cost and access criteria keep them behind ezetimibe in the queue [9] [10].
Bempedoic acid is the rung for the statin-intolerant: an oral ATP-citrate lyase inhibitor (180 mg daily) that is inactive in skeletal muscle and so largely spares it. CLEAR Outcomes randomised 13,970 statin-intolerant patients and found a 13% relative reduction in the four-component MACE composite — the first outcomes evidence for a drug built specifically for this population [11].
The arithmetic of the ladder
The evidence spine — how we know LDL is causal
Prevention examiners expect you to quote trials, not vibes. Four studies form the spine [3] [4] [5] [6]:
| Trial | Population | Intervention | Headline result | What it proved |
|---|---|---|---|---|
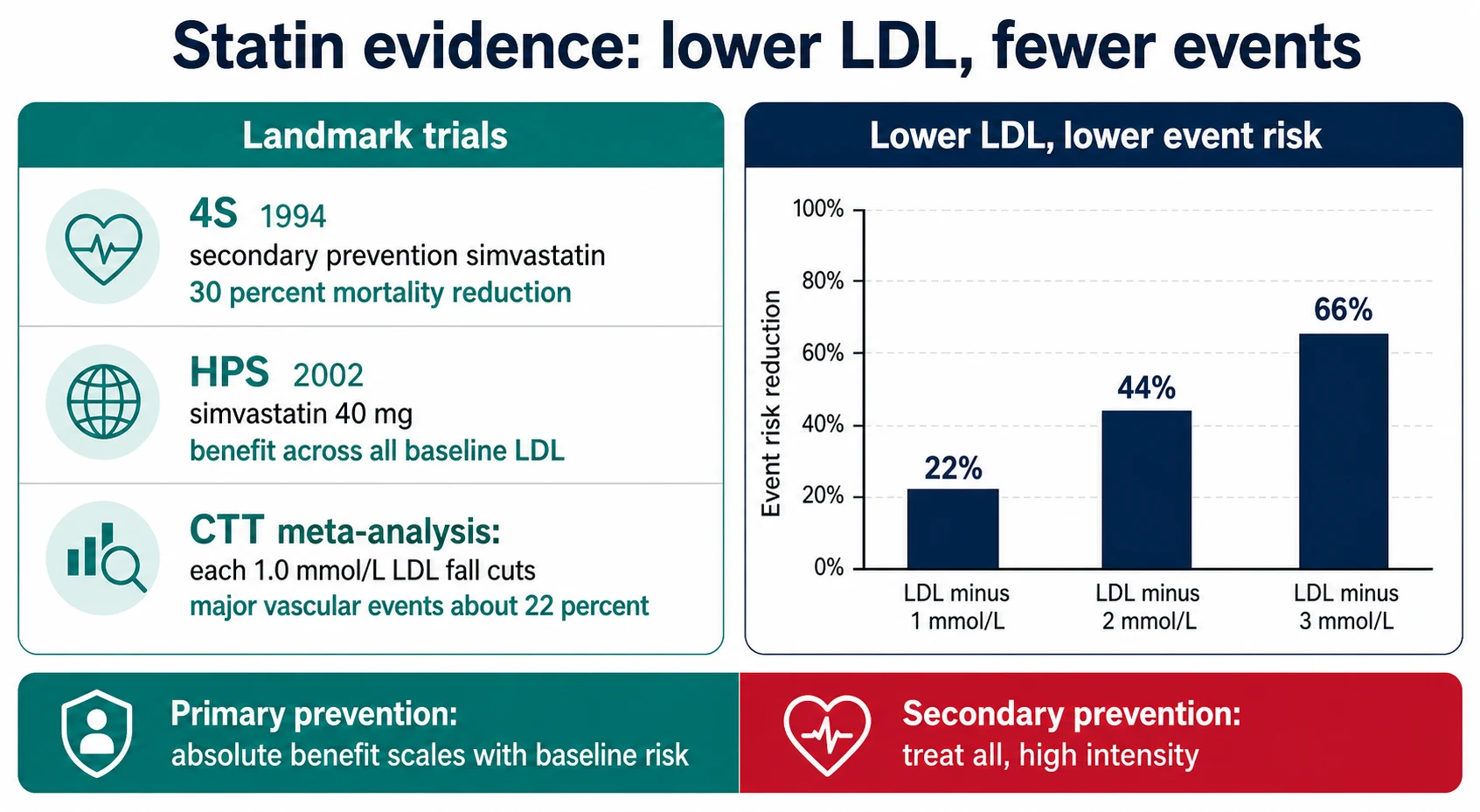
| 4S (1994) | 4,444 patients with coronary disease | Simvastatin 20–40 mg vs placebo | All-cause mortality down 30% over 5.4 years | Statins save lives in secondary prevention — the founding trial [3] |
| HPS (2002) | 20,536 high-risk adults including diabetics | Simvastatin 40 mg vs placebo | Major vascular events down ~25%, benefit even with baseline LDL below 3.0 mmol/L | Treat risk, not the starting LDL [4] |
| CTT 2005 | 90,056 participants, 14 statin trials | Meta-analysis | Each 1.0 mmol/L LDL fall: major vascular events down ~22%, all-cause mortality down 12% | The dose-response law; benefit proportional to LDL lowering [5] |
| CTT 2010 | 170,000 participants, 26 trials | More vs less intensive statin | Further 0.5 mmol/L LDL fall: further 15% event reduction | More intensive is better in high-risk patients [6] |
| JUPITER (2008) | 17,802 apparently healthy people, LDL below 3.4 mmol/L but hsCRP elevated | Rosuvastatin 20 mg vs placebo | Primary composite down 44% | Primary prevention works when baseline risk (not LDL) is elevated — though absolute benefit stays modest [7] |
The primary-versus-secondary distinction is about absolute benefit. Secondary prevention treats a population whose event rate is several per cent per year, so the number needed to treat is small and every high-risk patient benefits. In primary prevention the same relative reduction applies to a much smaller absolute risk, which is why the risk calculation — not the cholesterol — is the gatekeeper for treatment [1] [5].
Statin intolerance — and the nocebo elephant
Statin-associated muscle symptoms (SAMS) are the commonest reason prevention fails in practice. The pivotal modern evidence is SAMSON: a crossover n-of-1 trial in 60 patients who had abandoned statins through side effects, randomising months on atorvastatin 20 mg, placebo, and no treatment. Symptom intensity on statin and placebo was statistically indistinguishable — the nocebo effect accounted for about 90% of the symptom burden — and half the patients were able to restart statins within six months of seeing their own data [13].
This does not mean symptoms are imaginary; it means the attribution is usually wrong, and the physician's job is a structured workup rather than a reflex cessation [13] [5].
A defensible SAMS protocol
Characterise
Symmetrical proximal ache or cramp, typically within weeks of starting or uptitrating; systemic upset absent; note the temporal link to the drug
Exclude mimics
TSH, vitamin D, renal function, alcohol, exercise injury, and interacting drugs — macrolides, azole antifungals, ciclosporin, fibrates (especially gemfibrozil)
Check CK
Asymptomatic rise below 5 times the upper limit of normal: continue and monitor. Symptoms with marked CK rise, or dark urine: stop, hydrate, check creatinine and potassium — treat as rhabdomyolysis risk
Dechallenge and rechallenge
Stop 2-4 weeks until asymptomatic, then restart the same or a different statin at low dose; recurrence on rechallenge with resolution on stopping is the strongest attribution evidence
Re-establish LDL lowering
Alternate-day rosuvastatin or atorvastatin (long half-lives permit this), ezetimibe 10 mg backbone, and bempedoic acid 180 mg daily — which has outcomes evidence in exactly this population (CLEAR Outcomes)
Beyond LDL: triglycerides, Lp(a) and familial hypercholesterolaemia
Triglycerides. Moderate hypertriglyceridaemia marks residual risk in statin-treated patients. REDUCE-IT randomised 8,179 statin-treated patients (established CVD, or diabetes plus risk factors) with fasting triglycerides 1.5–5.6 mmol/L to icosapent ethyl 2 g twice daily — purified EPA, not fish-oil shop omega-3 — versus mineral-oil placebo: the primary composite fell 25% and cardiovascular death fell 20%. This is the only triglyceride-directed therapy with hard outcomes evidence; mixed fish oils and fibrates do not share it [12].
Lipoprotein(a) is a genetically determined LDL-like particle whose level is barely moved by lifestyle or statins. The EAS consensus flags concentrations above about 50 mg/dL (roughly the 80th percentile) as a risk-enhancing finding. Measure it once in adults with premature CVD, familial hypercholesterolaemia, a strong family history, or borderline risk decisions — a high result upgrades risk, tightens every other factor, and strengthens the case for aggressive LDL lowering while targeted therapies complete their trials [20].
Familial hypercholesterolaemia is the prevention diagnosis you must not miss: autosomal dominant, roughly 1 in 250–500 people, LDL very high from birth, and coronary disease a decade or more early if untreated. The EAS consensus makes three points every physician should carry: it is common and underdiagnosed; cascade screening of first-degree relatives is the most cost-effective case-finding in preventive cardiology; and treatment starts early with high-intensity statins, escalating to ezetimibe and PCSK9 antibodies to reach targets [19].
| Dutch Lipid Clinic Network criterion | Points to remember |
|---|---|
| Family history — first-degree relative with premature CVD, or known LDL very high | 1–2 points |
| Personal premature coronary artery disease (cerebral or peripheral disease scores 1) | 2 points |
| Tendon xanthomata | 6 points — the most specific sign |
| Corneal arcus before 45 years | 4 points |
| LDL 8.5 mmol/L or more | 8 points; 6.5–8.4 gives 5; 5.0–6.4 gives 3 |
| DNA-confirmed functional LDL-receptor, apoB or PCSK9 variant | 8 points [19] |
Score 6 or more makes probable-to-definite FH; 3–5 is possible and triggers family screening regardless [19].
Lifestyle — with numbers, not slogans
Lifestyle advice fails when it is vague. The evidence-backed prescription has quantities attached [14] [24] [25].
- Mediterranean diet. PREDIMED randomised about 7,400 high-risk Spaniards without CVD to a Mediterranean diet supplemented with extra-virgin olive oil or nuts versus low-fat control; major cardiovascular events fell by about 30%. The republished analysis (after randomisation corrections) preserved the result. Prescribe the pattern — olive oil, nuts, legumes, fish, vegetables, minimal processed food — not a supplement [14].
- Exercise. At least 150 minutes of moderate aerobic activity weekly (or 75 vigorous) plus resistance work is the guideline floor. The dose-response is real: each 1-MET increment in cardiorespiratory fitness tracks with about 13% lower all-cause mortality and 15% fewer cardiovascular events in meta-analysis [25].
- Smoking cessation is the single biggest intervention. In the Lung Health Study's 14.5-year follow-up, a sustained cessation intervention cut all-cause mortality — the rare lifestyle trial with a survival endpoint. Every prevention consult to a smoker starts here, combining behavioural support with pharmacotherapy (varenicline, NRT, bupropion) rather than advice alone [24].
- Alcohol. There is no cardiovascular indication for alcohol; keep within national low-risk limits and do not "prescribe" red wine for the heart — the PREDIMED benefit belongs to the dietary pattern, not the bottle [14].
Blood pressure and diabetes — the risk multipliers
Hypertension and diabetes rarely appear in the prevention exam as themselves; they appear as the factors that push a borderline risk calculation over the treatment line [1] [21].
SPRINT randomised 9,361 non-diabetic adults at high cardiovascular risk to systolic targets below 120 versus below 140 mmHg: the intensive target cut the primary composite by 25% and all-cause death by 27%, at the cost of more hypotension, syncope, electrolyte disturbance and acute kidney injury. The lesson for prevention is that blood pressure targets, like lipid targets, tighten as risk rises — and that intensive treatment trades absolute benefit against monitoring burden [21].
For diabetes, the statin evidence is unambiguous: CTT included large diabetic cohorts and found the same proportional LDL benefit as in non-diabetics, which is why most adults with diabetes over 40 earn a statin on risk grounds even when lipids look unremarkable [5]. What diabetes no longer earns by default is aspirin — see the controversy section below [17].
The post-ACS secondary prevention bundle
Secondary prevention is where the bundle lives. Each component has its own trial lineage, and the DCE examiner wants to hear you prescribe all five deliberately [22] [23] [26]:
| Component | Evidence anchor | The point to make |
|---|---|---|
| Antiplatelet — aspirin (plus a P2Y12 inhibitor for the guideline-defined DAPT period) | ISIS-2: aspirin 160 mg within 24 hours of suspected MI cut five-week vascular mortality by 23% — one of the cheapest mortality interventions in medicine | Aspirin's home is secondary prevention; its primary-prevention role has collapsed [22] |
| High-intensity statin — atorvastatin 40–80 mg or rosuvastatin 20–40 mg | 4S and the CTT intensive meta-analysis | Start in hospital, do not titrate timidly, target LDL below 1.4 mmol/L and at least a 50% fall [3] [6] |
| Beta-blocker | Freemantle meta-analysis: long-term beta-blockade after MI cut the odds of death by about 23% | Strongest case with reduced ejection fraction or ongoing ischaemia; review need in preserved-EF patients without other indication [26] |
| ACE inhibitor | SAVE: captopril after MI with LV dysfunction (EF 40% or less) cut mortality 19% | Near-mandatory with reduced EF, anterior MI, diabetes or hypertension [23] |
| Cardiac rehabilitation referral | Cochrane 2016 | Exercise-based rehabilitation cuts cardiovascular mortality about 26% — a drug-equivalent effect delivered by a program [15] |
Add the surrounding work: influenza vaccination, depression screening (post-MI depression is common and worsens outcomes), driving and return-to-work advice, and explicit smoking-cessation pharmacotherapy for smokers [15] [24].
Cardiac rehabilitation
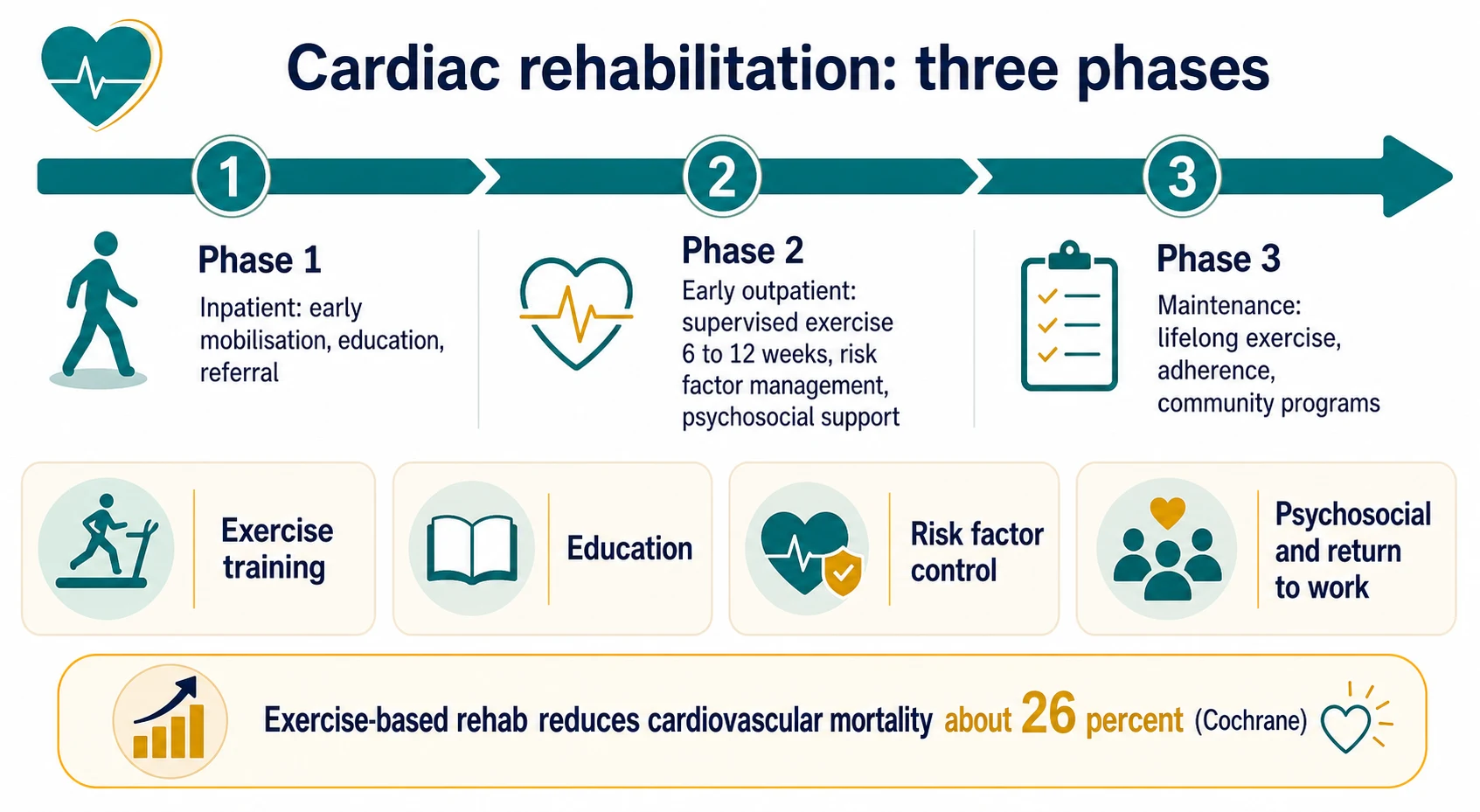
Cardiac rehabilitation is a structured, multidisciplinary secondary-prevention program — and the Cochrane evidence says it works: across 63 trials and nearly 15,000 patients, exercise-based rehabilitation reduced cardiovascular mortality by about 26% (relative risk 0.74) and hospital readmissions, with improved quality of life, even in the modern statin-and-PCI era [15].
The three phases
Phase 1 — inpatient
Early mobilisation after ACS or cardiac surgery, risk education, medication reconciliation, and the outpatient referral — which should be automatic at discharge, not opt-in
Phase 2 — early outpatient
Supervised exercise over about 6-12 weeks with education, risk-factor management, psychosocial support and return-to-work planning; typically starts within 2-6 weeks of discharge
Phase 3 — maintenance
Lifelong exercise habit, adherence support, community or home-based programs; the benefits decay if the habit decays
Who gets referred: every post-ACS patient, post-revascularisation (PCI or CABG), stable angina, and heart failure with reduced ejection fraction. The scandal is utilisation — referral and attendance rates sit far below eligibility everywhere, with women, rural patients, the elderly and the socioeconomically deprived least likely to attend. Naming those barriers, and offering home-based or telehealth models, is the consultant-level answer to "is rehab worth it?" [15].
Primary prevention controversies — where guidelines moved
Aspirin has left primary prevention. Three 2018 trials closed the era: ASPREE (19,114 healthy people aged 70 and over) found aspirin 100 mg gave no cardiovascular benefit and more major haemorrhage, with a signal of higher all-cause mortality [16]; ASCEND (15,480 people with diabetes and no CVD) found vascular benefits roughly cancelled by major bleeding [17]; and ARRIVE (12,546 moderate-risk adults) found no event reduction with doubled gastrointestinal bleeding [18]. The current rule: aspirin is for secondary prevention; in primary prevention it is an individualised exception for selected high-risk, low-bleeding-risk younger adults — never routine, and essentially never after 70 [16] [18].
Coronary artery calcium scoring is the tiebreaker for the undecided middle: a CAC of zero downgrades an intermediate-risk estimate enough to defer a statin in many patients, while a high score upgrades. It appears in the Australian guideline as a reclassification tool for intermediate risk — use it when the result will genuinely change the decision [1].
How low should LDL go? FOURIER achieved median LDL 0.78 mmol/L with no new safety signal over its follow-up, and the CTT analyses show a log-linear benefit with no floor — the exam-safe statement is "lower is better, at least down to the levels achieved in the outcomes trials" [6] [9].
The DCE angles
Long case. The classic defence is the post-ACS patient with multimorbidity — CKD, diabetes, hypertension — complicated by statin-associated muscle symptoms. The examiner watches three things: whether you defend the whole bundle rather than the drug of the moment; whether your statin plan is a protocol (exclude mimics, dechallenge, rechallenge, alternate-day dosing, ezetimibe or bempedoic acid backbone) rather than capitulation; and whether rehabilitation, smoking, depression and adherence feature as seriously as the pharmacology [11] [13] [15].
Short case. The risk-factor examination: blood pressure done properly, BMI and waist circumference, eyes for xanthelasma and corneal arcus, tendons for xanthomata (Achilles and extensor tendons of the hands), hands for nicotine staining, and pulses for established disease. Tendon xanthomata are the highest-value physical sign in preventive cardiology — near-pathognomonic of FH and worth 6 Dutch Lipid Clinic points on their own [19].
Exam traps, collected
References
- [1]Nelson MR, Doust JA, Ryan J, et al. 2023 Australian guideline for assessing and managing cardiovascular disease risk Med J Aust, 2024.PMID 38623719
- [2]Hippisley-Cox J, Coupland C, Brindle P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: prospective cohort study BMJ, 2017.PMID 28536104
- [3]Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S) Lancet, 1994.PMID 7968073
- [4]Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial Lancet, 2002.PMID 12114036
- [5]Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins Lancet, 2005.PMID 16214597
- [6]Cholesterol Treatment Trialists' (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials Lancet, 2010.PMID 21067804
- [7]Ridker PM, Danielson E, Fonseca FAH, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein N Engl J Med, 2008.PMID 18997196
- [8]Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes N Engl J Med, 2015.PMID 26039521
- [9]Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease N Engl J Med, 2017.PMID 28304224
- [10]Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome N Engl J Med, 2018.PMID 30403574
- [11]Nissen SE, Lincoff AM, Brennan D, et al. Bempedoic Acid and Cardiovascular Outcomes in Statin-Intolerant Patients N Engl J Med, 2023.PMID 36876740
- [12]Bhatt DL, Steg PG, Miller M, et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia N Engl J Med, 2019.PMID 30415628
- [13]Wood FA, Howard JP, Finegold JA, et al. N-of-1 Trial of a Statin, Placebo, or No Treatment to Assess Side Effects N Engl J Med, 2020.PMID 33196154
- [14]Estruch R, Ros E, Salas-Salvadó J, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts N Engl J Med, 2018.PMID 29897866
- [15]Anderson L, Oldridge N, Thompson DR, et al. Exercise-based cardiac rehabilitation for coronary heart disease Cochrane Database Syst Rev, 2016.PMID 26730878
- [16]McNeil JJ, Wolfe R, Woods RL, et al. Effect of Aspirin on Cardiovascular Events and Bleeding in the Healthy Elderly N Engl J Med, 2018.PMID 30221597
- [17]ASCEND Study Collaborative Group. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus N Engl J Med, 2018.PMID 30146931
- [18]Gaziano JM, Brotons C, Coppolecchia R, et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial Lancet, 2018.PMID 30158069
- [19]Nordestgaard BG, Chapman MJ, Humphries SE, et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society Eur Heart J, 2013.PMID 23956253
- [20]Nordestgaard BG, Chapman MJ, Ray K, et al. Lipoprotein(a) as a cardiovascular risk factor: current status Eur Heart J, 2010.PMID 20965889
- [21]SPRINT Research Group, Wright JT Jr, Williamson JD, et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control N Engl J Med, 2015.PMID 26551272
- [22]ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group Lancet, 1988.PMID 2899772
- [23]Pfeffer MA, Braunwald E, Moyé LA, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators N Engl J Med, 1992.PMID 1386652
- [24]Anthonisen NR, Skeans MA, Wise RA, et al. The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trial Ann Intern Med, 2005.PMID 15710956
- [25]Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis JAMA, 2009.PMID 19454641
- [26]Freemantle N, Cleland J, Young P, et al. beta Blockade after myocardial infarction: systematic review and meta regression analysis BMJ, 1999.PMID 10381708