Phys · cardiovascular
Coronary Artery Disease
Also known as ischaemic heart disease · coronary heart disease · acute coronary syndrome · ACS · myocardial infarction · STEMI · NSTEMI · unstable angina · stable angina · chronic coronary syndrome
Consultant-physician-depth guide to coronary artery disease — atherosclerotic pathophysiology, stable angina, the ACS spectrum (UA/NSTEMI/STEMI), troponin and ECG interpretation, acute reperfusion strategy, and secondary prevention — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Coronary Artery Disease
The answer first
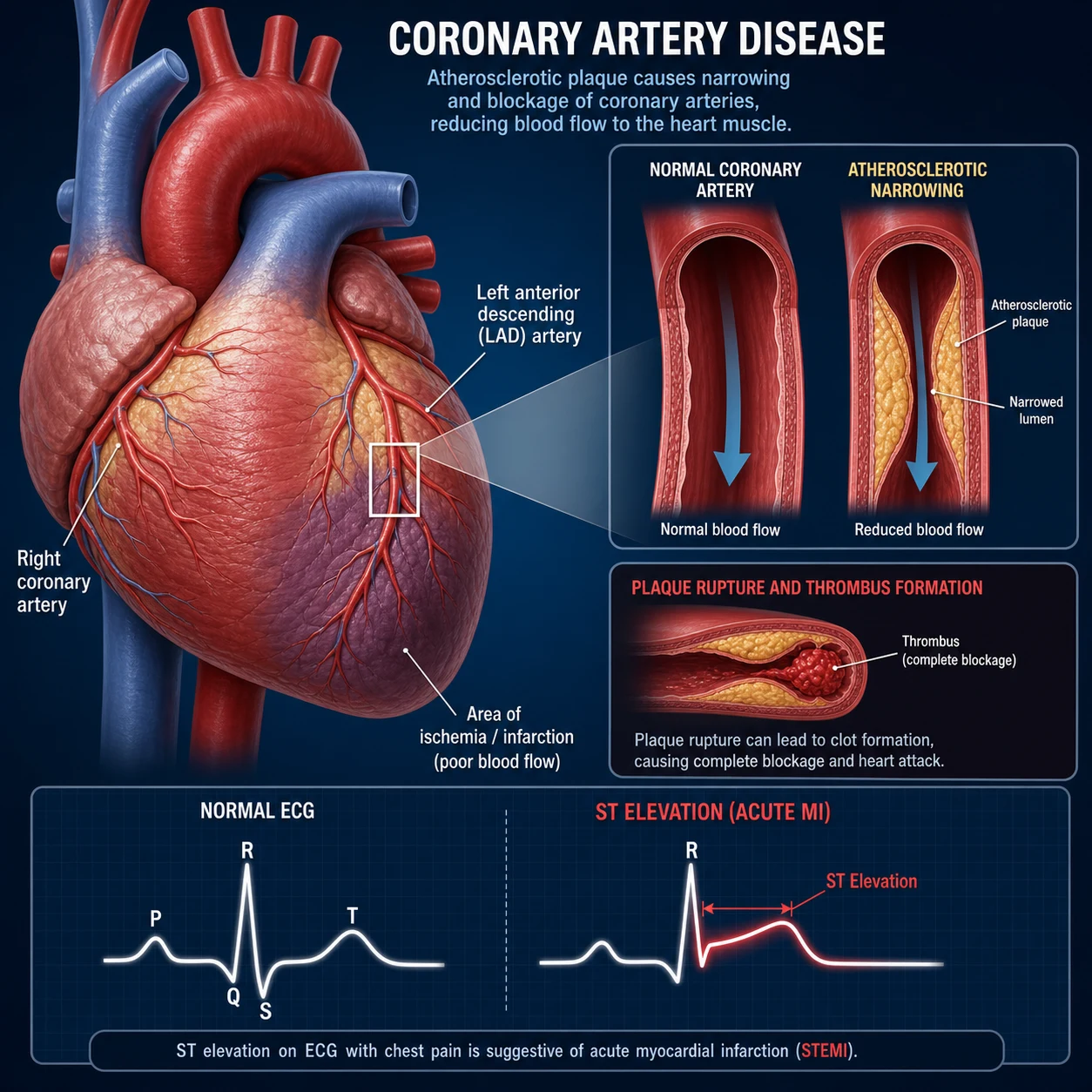
Coronary artery disease (CAD) is the clinical manifestation of coronary atherosclerosis — lipid-driven plaque accumulation in the arterial wall that narrows the lumen and, when complicated by rupture or erosion, triggers thrombosis. The clinical spectrum runs from silent ischaemia and stable angina at one end to the acute coronary syndromes (unstable angina, NSTEMI, STEMI) at the other. The unifying mechanism is a mismatch between myocardial oxygen supply and demand. [1]
Two management decisions dominate fellowship exams and bedside practice: [1]
-
Is this an acute coronary syndrome requiring immediate reperfusion? If the ECG shows ST elevation or equivalent, the patient is having a STEMI — activate the catheter lab for primary PCI (door-to-balloon ≤90 min), or give fibrinolytics if PCI is not achievable within 120 minutes of first medical contact. Every minute of delay kills myocardium ("time is muscle"). [1]
-
Is this patient's risk high enough to warrant an invasive strategy? For NSTE-ACS, risk scores (GRACE, TIMI) and dynamic ECG/troponin changes separate those needing angiography within 2 hours (very high risk), within 24 hours (high risk), or conservatively. Under-treating risk kills; over-treating exposes patients to procedural harm. [1]
Classification
The clinical spectrum of CAD is divided into chronic coronary syndromes (stable angina, silent ischaemia, stable post-MI) and acute coronary syndromes (ACS), which are further stratified by ECG and troponin: [1]
| Syndrome | ECG | Troponin | Pathology | Urgency |
|---|---|---|---|---|
| Stable angina | Normal or stable changes | Normal | Fixed stenosis, demand ischaemia | Routine |
| Unstable angina (UA) | No ST elevation, ± T-wave inversion/ST depression | Normal | Subtotal occlusion, no necrosis | Urgent |
| NSTEMI | No ST elevation, ± ST depression/T-wave inversion | Elevated | Subtotal occlusion with necrosis | Urgent–emergency |
| STEMI | ST elevation or equivalent | Elevated (may be early-normal) | Total occlusion, transmural necrosis | Emergency |
DWE high-yield: UA and NSTEMI are clinically indistinguishable at presentation — both present with ischaemic chest pain and no ST elevation. The distinction is troponin: elevated = NSTEMI; normal = unstable angina. This matters because NSTEMI implies myocardial necrosis and a higher event rate, mandating a more aggressive invasive strategy. [1]
Pathophysiology
Atherosclerosis — the slow disease
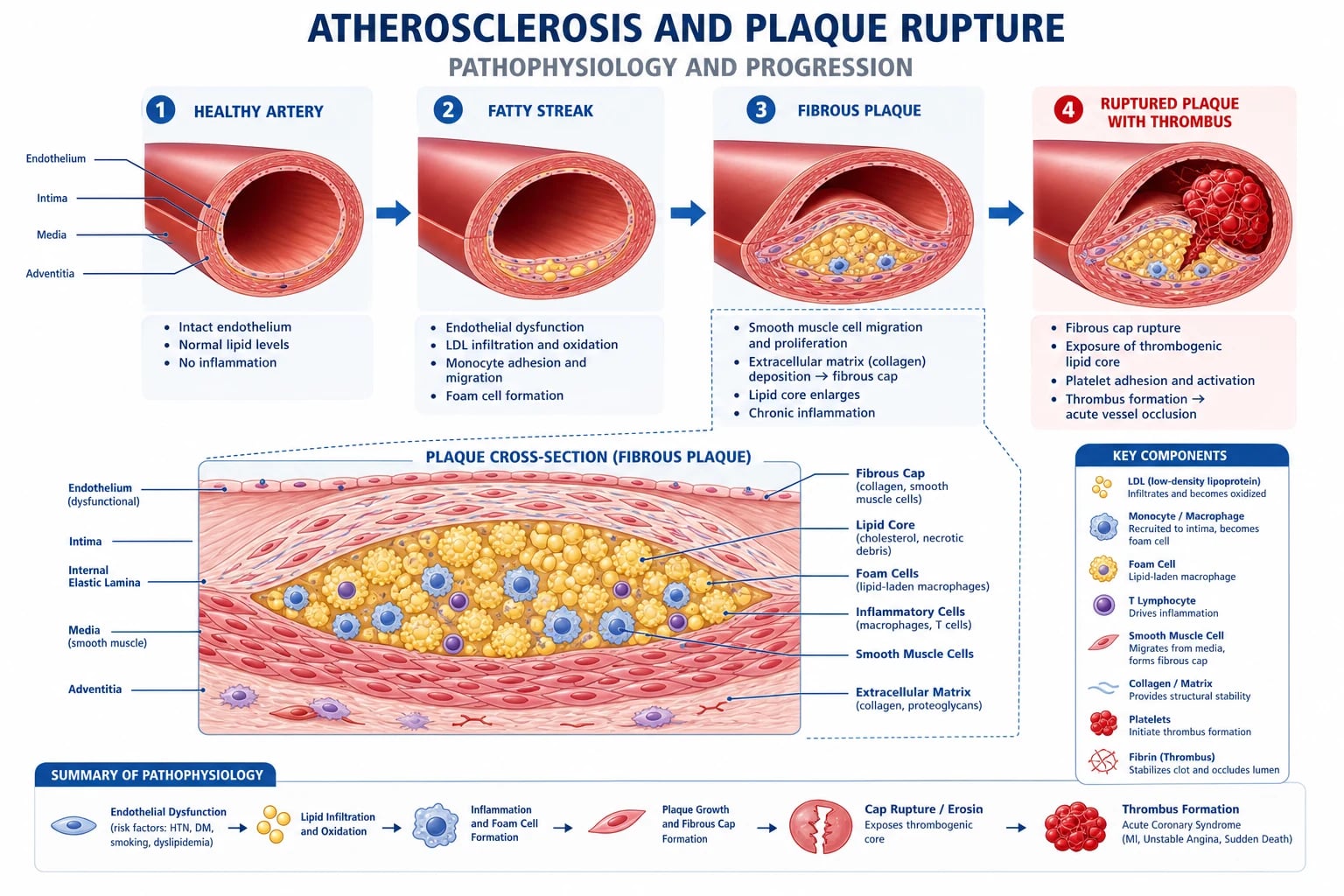
Atherosclerosis begins decades before symptoms. The process: [1]
- Endothelial dysfunction — driven by cardiovascular risk factors (smoking, hypertension, hyperlipidaemia, diabetes). The dysfunctional endothelium is more permeable, pro-thrombotic, and pro-inflammatory.
- Lipid accumulation — low-density lipoprotein (LDL) particles enter the intima, become oxidised, and are taken up by macrophages to form foam cells — the hallmark of the fatty streak.
- Plaque formation — smooth muscle cells migrate into the intima and proliferate, secreting collagen to form a fibrous cap over a lipid-rich necrotic core.
- Luminal narrowing — as the plaque grows, it encroaches on the lumen. Because coronary flow occurs predominantly in diastole, flow-limiting stenosis (>70%) produces ischaemia only on exertion — this is stable angina. [1]
Why this matters clinically: Stable plaques with thick fibrous caps cause exertional angina but rarely rupture. The plaques that cause ACS are often mild-to-moderate angiographic stenoses with thin caps and large lipid cores — "vulnerable plaques." This is why a patient can have a normal stress test one month and an MI the next. [1]
Plaque rupture and thrombosis — the acute event
An ACS occurs when a plaque's fibrous cap ruptures (or, less commonly, erodes), exposing the thrombogenic lipid core to circulating blood: [1]
- Cap rupture — inflammatory mediators (matrix metalloproteinases from macrophages) weaken the cap; haemodynamic stress tears it.
- Platelet adhesion and activation — exposed collagen and tissue factor trigger platelet adhesion (via glycoprotein Ib) and activation (via the P2Y12 receptor). Platelets aggregate (glycoprotein IIb/IIIa).
- Coagulation cascade — tissue factor activates the extrinsic pathway, generating thrombin, which converts fibrinogen to fibrin and further activates platelets.
- Thrombus formation — the balance between thrombosis and endogenous lysis determines outcome:
- Total occlusion → transmural ischaemia → STEMI (ST elevation).
- Subtotal occlusion with embolisation → patchy necrosis → NSTEMI (no ST elevation, troponin rise).
- Subtotal occlusion without necrosis → unstable angina (no troponin rise). [1]
This thrombosis cascade is the target of every acute ACS intervention: antiplatelets block platelet activation/aggregation; anticoagulants block thrombin generation; reperfusion (PCI or fibrinolytics) removes the thrombus and restores flow. [1]
DWE trap: "Why does type 2 MI not respond to PCI?" Type 2 MI is caused by supply–demand mismatch (tachyarrhythmia, hypotension, sepsis, severe anaemia) without plaque rupture. The troponin rises because of subendocardial ischaemia in a structurally stressed myocardium. Treating the underlying cause (rate control, transfusion, inotropes) — not catheterisation — is the management. Always classify troponin elevation: type 1 (plaque rupture) vs type 2 (demand) vs other causes (myocarditis, PE, sepsis, renal failure). [1]
Clinical presentation
Typical ischaemic chest pain
The classic description is retrosternal pressure, tightness, or heaviness, lasting minutes (not seconds, not days), that may radiate to the jaw, shoulders, or arms, and is brought on by exertion or stress and relieved by rest or GTN. Three features define "typical" angina: [1]
- Constricting discomfort in the retrosternal region.
- Provoked by exertion or emotional stress.
- Relieved by rest or GTN within minutes. [1]
Two of three = atypical; one or none = non-anginal. [1]
Atypical presentations — the high-yield trap
The single most dangerous error is assuming chest pain is "atypical" and therefore not cardiac. Women, older adults, and people with diabetes frequently present without classic chest pain: [1]
- Epigastric pain or indigestion-like discomfort (inferior MI masquerading as "gastritis")
- Jaw, neck, or arm pain without chest pain
- Breathlessness alone (ischaemia presenting as pulmonary oedema)
- Syncope (arrhythmia or complete heart block with inferior MI)
- Fatigue or collapse in the elderly ("silent MI") [1]
DCE long-case rule: Any acute breathlessness, syncope, epigastric pain, or new arrhythmia in a patient with vascular risk factors warrants an ECG and troponin. Do not anchoring on a gastrointestinal diagnosis until you have excluded ACS. [1]
Differential diagnosis
The five life-threatening causes of chest pain must be excluded on first assessment: [1]
| Condition | Discriminating features |
|---|---|
| ACS | Typical pain, troponin rise, ECG changes, risk factors |
| Aortic dissection | Tearing pain radiating to back, pulse/BP differential, widened mediastinum on CXR |
| Pulmonary embolism | Pleuritic pain, dyspnoea, tachycardia, DVT risk factors, right heart strain on ECG/echo |
| Tension pneumothorax | Sudden dyspnoea, tracheal deviation, absent breath sounds, hypoxia |
| Oesophageal rupture (Boerhaave) | Vomiting then chest pain, subcutaneous emphysema, pleural effusion |
Aortic dissection is the critical mimic: a patient with both ACS and dissection can have a normal right-arm BP and ECG changes (the dissection can extend into the right coronary ostium causing an inferior STEMI pattern). If the pain is tearing and radiates to the back, check for pulse deficits and BP differentials before giving anticoagulation or fibrinolytics — giving a lytic to a dissection is a fatal error. [1]
Investigations
Acute chest pain — immediate panel
| Test | Why |
|---|---|
| 12-lead ECG within 10 min | Diagnose STEMI; identify ischaemic changes (ST depression, T-wave inversion), arrhythmia, old changes |
| High-sensitivity troponin (hs-cTn) | Detect myocardial necrosis; use 0/1-h or 0/3-h algorithm to rule in/out |
| CXR | Exclude pneumothorax, widened mediastinum (dissection), pulmonary oedema |
| Bloods | FBC, U&E, creatinine, glucose, lipids, LFTs, coagulation, β-HCG (if applicable) |
ECG interpretation — the decision-maker
ST elevation defines STEMI and triggers reperfusion. Diagnostic ST elevation requires:
- ≥1 mm in two contiguous limb leads (I, II, III, aVF, aVL), OR
- ≥2 mm in two contiguous precordial leads (V1–V6) in men (≥1.5 mm in women). [1]
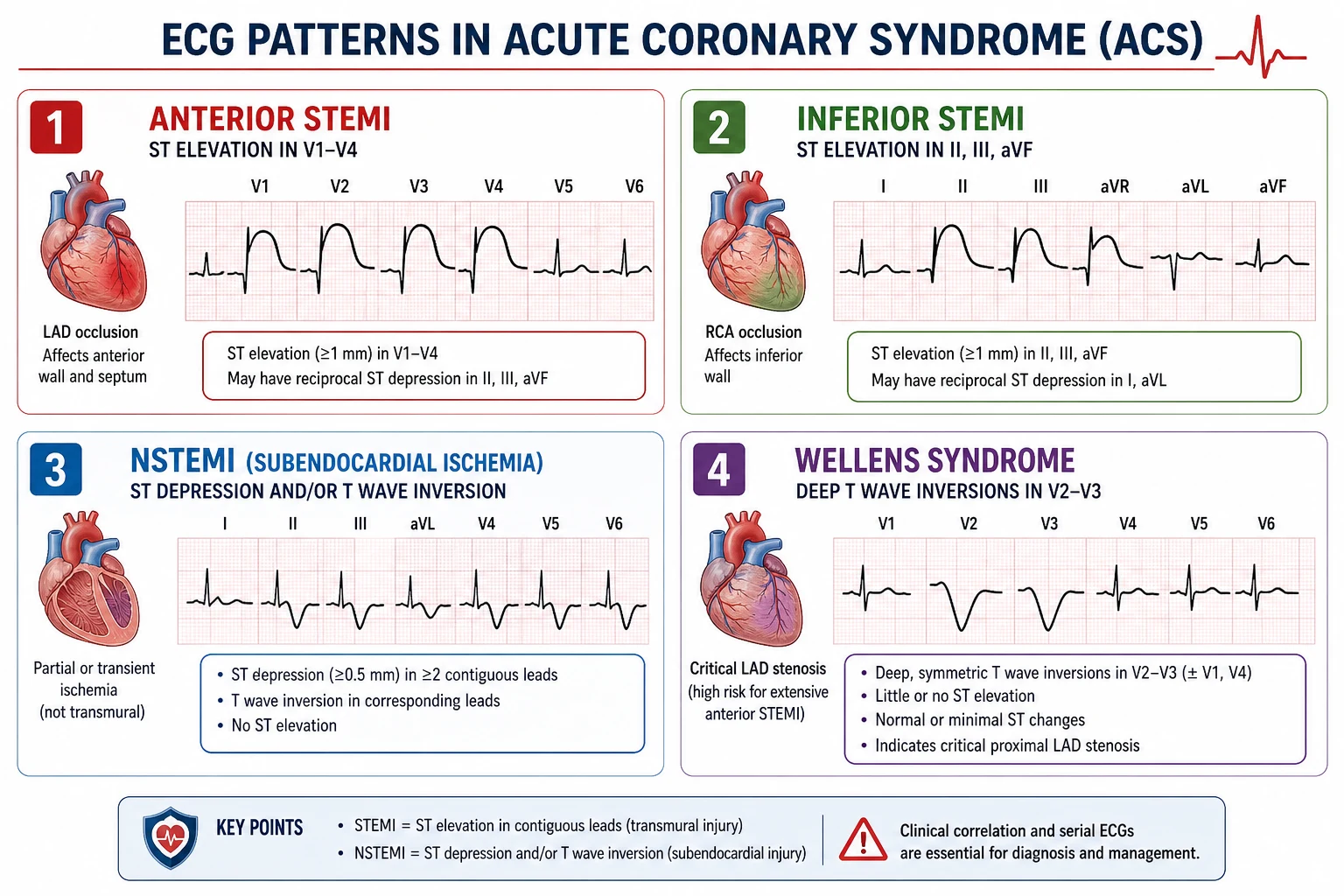
Localise the occluded artery from the leads with ST elevation: [1]
| ST elevation leads | Territory | Culprit artery |
|---|---|---|
| V1–V4 | Anterior | LAD |
| II, III, aVF | Inferior | RCA (~80%) or LCx |
| I, aVL, V5–V6 | Lateral | LCx or diagonal of LAD |
| V7–V9 (V1–V3 ST depression as mirror) | Posterior | RCA or LCx |
| V1–V2 (right-sided V4R) | Right ventricular | Proximal RCA |
Reciprocal ST depression in opposing leads (e.g., ST depression in I/aVL with inferior STEMI) strongly supports STEMI and distinguishes it from mimics. [1]
DWE high-yield mimics of ST elevation: Early repolarisation (diffuse, concave, no reciprocal), left bundle branch block (use Sgarbossa criteria), left ventricular aneurysm (persistent ST elevation with Q waves, no troponin rise), Brugada syndrome (coved ST in V1–V3), pericarditis (diffuse PR depression, concave ST elevation). Do not fibrinolyse these. [1]
ST depression or T-wave inversion without ST elevation points to NSTE-ACS, but beware:
- Deep symmetric T-wave inversion across the anterior leads (Wellens syndrome) — critical LAD stenosis; refer urgently for angiography.
- Posterior MI — ST depression V1–V3 with tall R waves; confirm with posterior leads V7–V9. [1]
Troponin interpretation
High-sensitivity cardiac troponin (hs-cTn) is the cornerstone of ACS diagnosis. Interpret by change (delta) between serial measurements, not a single value: [1]
- 0/1-hour algorithm (ESC preferred): Baseline and 1-hour troponin with values stratified into rule-out, observe, or rule-in zones based on absolute delta.
- 0/3-hour algorithm: Baseline and 3-hour troponin; a rise/fall of ≥50% from baseline with a value above the 99th percentile confirms acute MI. [1]
A single mildly elevated troponin is not diagnostic of type 1 MI. Troponin elevation occurs in many non-ACS conditions: sepsis, PE, myocarditis, renal failure, tachyarrhythmias, heart failure, stroke. The discriminator is the clinical context and a rising trend — a troponin that is high and flat (no delta) in a clinically stable patient suggests chronic myocardial injury, not acute plaque rupture. [1]
Exam trap: A patient with sepsis and a troponin of 80 (reference <20) but no chest pain and no ECG changes does not have a type 1 MI. The troponin reflects demand ischaemia / septic cardiomyopathy. Treat the sepsis. Serial troponins that rise dynamically with ischaemic chest pain and ECG changes are the type 1 MI pattern. [1]
Acute management — STEMI
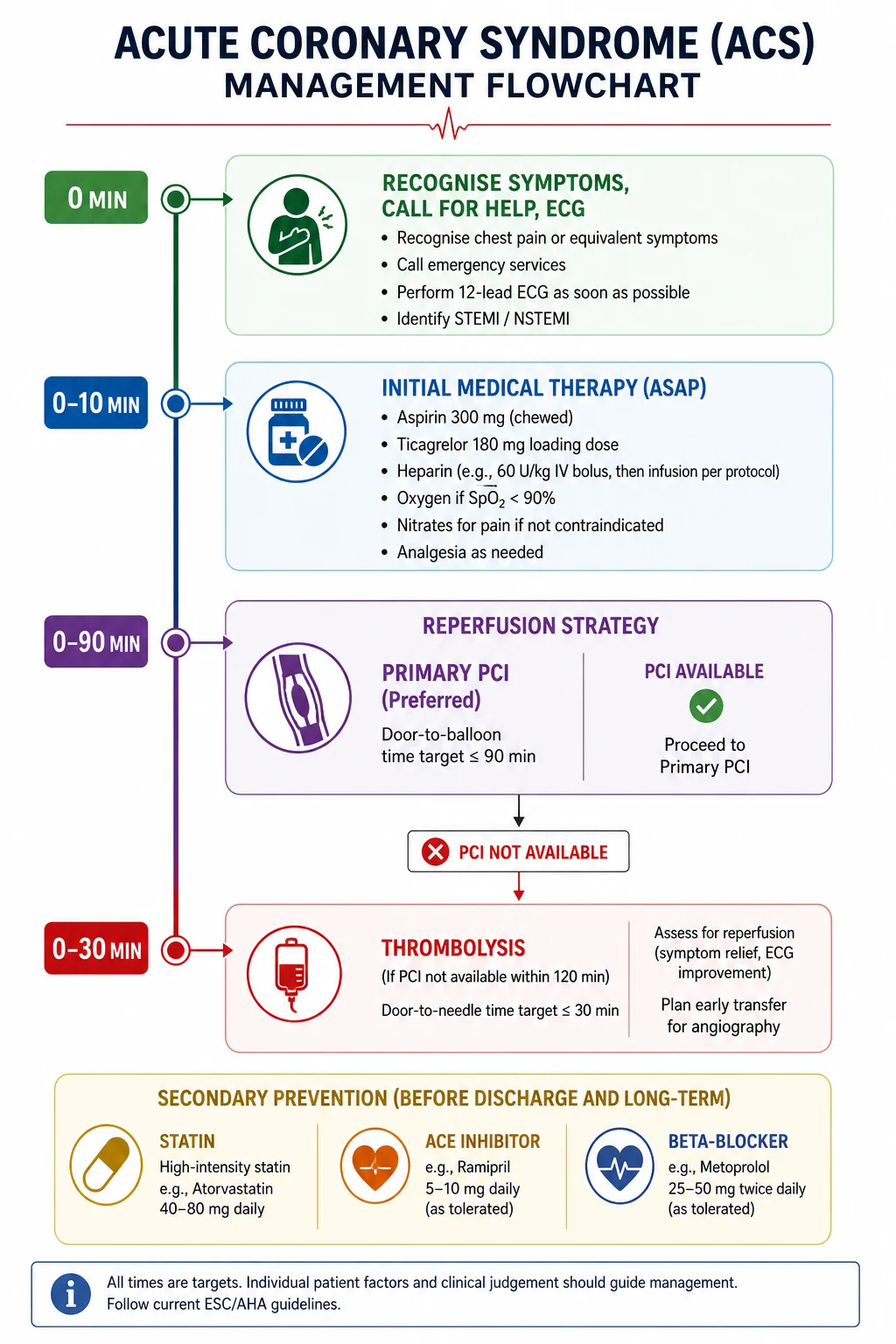
Immediate (the first 30 minutes)
- Aspirin 300 mg orally (chewed, non-enteric coated) — irreversible COX-1 inhibition of platelets. [1]2. P2Y12 inhibitor loading — ticagrelor 180 mg (preferred per PLATO), prasugrel 60 mg (if proceeding to PCI and no prior stroke/TIA), or clopidogrel 600 mg (if the others are contraindicated or fibrinolysis is planned).
- Anticoagulation — unfractionated heparin, enoxaparin, or bivalirudin (for primary PCI).
- Analgesia — morphine 2.5–5 mg IV (only for distress; avoid over-sedation which delays antiplatelet absorption). GTN sublingual if systolic BP is adequate.
- Oxygen — only if hypoxic (SpO₂ <90%). Routine supplemental oxygen in non-hypoxic MI patients may worsen outcomes.
- High-intensity statin — atorvastatin 80 mg or rosuvastatin 40 mg immediately. [1]
Reperfusion — PCI vs fibrinolysis
Primary PCI is the preferred reperfusion strategy when it can be performed within 120 minutes of first medical contact (target door-to-balloon ≤90 min). It achieves higher TIMI 3 flow, lower rates of intracranial haemorrhage, and lower mortality than fibrinolysis. [1]
Fibrinolysis is indicated when primary PCI cannot be delivered within 120 minutes and the patient presents within 12 hours of symptom onset with no contraindications. The agent (tenecteplase, weight-based single bolus) should be given within 30 minutes of arrival ("door-to-needle ≤30 min"). Patients who receive fibrinolysis should be transferred to a PCI centre for routine angiography within 24 hours (pharmacoinvasive strategy), or immediately if reperfusion fails (ongoing pain, <50% ST resolution at 60–90 min, haemodynamic instability). [1]
Contraindications to fibrinolysis include prior intracranial haemorrhage, known cerebral vascular lesion, ischaemic stroke within 6 months, intracranial neoplasm, active bleeding, suspected aortic dissection, and major surgery within 3 weeks. [1]
DWE trap: Do not give fibrinolytics to a patient with ST depression (this is NSTE-ACS, not STEMI — lytics increase risk without benefit). The only exception is posterior MI presenting as ST depression V1–V3 (true posterior STEMI), which benefits from reperfusion. [1]
Acute management — NSTE-ACS (UA and NSTEMI)
Risk stratification — who goes to the cath lab?
NSTE-ACS management hinges on risk stratification, because the benefit of an invasive strategy is concentrated in high-risk patients while low-risk patients are managed conservatively (and may not have CAD at all). [1]
GRACE score (Global Registry of Acute Coronary Events): incorporates age, heart rate, systolic BP, creatinine, Killip class, cardiac arrest at admission, ST deviation, and troponin. Predicts in-hospital and 6-month mortality. GRACE >140 = high risk → early invasive strategy. [1]
TIMI score: 7 variables (age ≥65, ≥3 CAD risk factors, known CAD (≥50% stenosis), aspirin in last 7 days, severe angina (≥2 episodes in 24h), ST deviation ≥0.5 mm, elevated cardiac biomarkers). TIMI ≥3 = higher-risk benefit from invasive strategy. [1]
TIMI risk score components — memorise for viva:
- Age ≥65 years
- At least 3 risk factors for CAD (family history, hypertension, hypercholesterolaemia, diabetes, current smoker)
- Known CAD (≥50% stenosis on prior angiography)
- Aspirin use in past 7 days
- Severe angina (≥2 episodes within 24 hours)
- ST-segment deviation ≥0.5 mm
- Elevated cardiac biomarkers [1]
Each present scores 1; range 0–7. Higher scores predict worse outcomes and greater benefit from early invasive management. [1]
Invasive strategy timing
| Risk category | Criteria | Timing of angiography |
|---|---|---|
| Very high risk | Haemodynamic compromise, refractory angina, cardiac arrest, mechanical complications, acute heart failure, recurrent dynamic ST/T changes | ≤2 hours |
| High risk | GRACE >140, troponin rise/fall, dynamic ST/T changes | Within 24 hours |
| Low risk | Non-diagnostic troponin, no ECG changes | Non-invasive imaging first; invasive only if positive |
Antiplatelet and anticoagulant therapy
Dual antiplatelet therapy (DAPT)
All ACS patients receive aspirin (loading 300 mg, then 75–100 mg daily, lifelong) plus a P2Y12 inhibitor: [1]
| Agent | Loading | Maintenance | Key trial / evidence |
|---|---|---|---|
| Ticagrelor | 180 mg | 90 mg BID | PLATO: 16% RRR vs clopidogrel in CV death/MI/stroke; preferred in most ACS [4] |
| Prasugrel | 60 mg | 10 mg OD (5 mg if <60 kg or ≥75 yr) | TRITON-TIMI 38: superior to clopidogrel but more bleeding; contraindicated in prior stroke/TIA [6] |
| Clopidogrel | 600 mg (PCI) / 300 mg (lysis) | 75 mg OD | CURE: foundation of DAPT in NSTE-ACS; default if the others are contraindicated [3] |
DWE high-yield selection rule: For ACS managed with an invasive strategy, ticagrelor is the preferred P2Y12 inhibitor (PLATO mortality benefit). Prasugrel is an alternative for patients proceeding to PCI who have no prior stroke/TIA. Clopidogrel is used when fibrinolysis is planned (prasugrel and ticagrelor are contraindicated with lysis) or when the others are not tolerated. Ticagrelor is held 24 h, clopidogrel 5 days, and prasugrel 7 days before elective surgery. [1]
DAPT duration: Minimum 12 months after ACS (regardless of stent type, with current-generation DES). After 12 months, bleeding risk is weighed against ischaemic risk to decide on continued single antiplatelet therapy (aspirin, or P2Y12 monotherapy in selected patients). For CABG, aspirin is continued peri-operatively; P2Y12 inhibitors are stopped 5 days (clopidogrel) or 7 days (prasugrel/ticagrelor) pre-operatively. [1]
Anticoagulation
Anticoagulation is given alongside DAPT during the acute phase to prevent further thrombus propagation. Options include unfractionated heparin (UFH, preferred in primary PCI and renal failure), low-molecular-weight heparin (enoxaparin), fondaparinux (lowest bleeding risk, suitable for conservative strategy), and bivalirudin (direct thrombin inhibitor, used in primary PCI). Anticoagulation is stopped after successful PCI unless there is another indication (AF, mechanical valve, LV thrombus). [1]
Dual pathway inhibition
Low-dose rivaroxaban (2.5 mg BID) added to aspirin reduces CV death, MI, and stroke post-ACS, at the cost of increased major bleeding (ATLAS ACS 2–TIMI 51) [8]. It is an option for patients with high ischaemic and low bleeding risk, continued beyond the standard DAPT period.
Secondary prevention
Secondary prevention after MI reduces mortality by up to 50% and is examined relentlessly. The mnemonic is ABCDE: Antiplatelet/ACE; Beta-blocker/Blood pressure; Cholesterol/Cigarettes; Diet/Diabetes; Exercise/Education. [1]
Pharmacotherapy — the non-negotiables
| Therapy | Agent and dose | Rationale |
|---|---|---|
| Antiplatelet | Aspirin 75–100 mg lifelong + P2Y12 inhibitor for 12 months (see above) | Prevents stent thrombosis and recurrent ACS |
| High-intensity statin | Atorvastatin 80 mg or rosuvastatin 20–40 mg; add ezetimibe if LDL not at target | LDL target <1.4 mmol/L (55 mg/dL); IMPROVE-IT showed ezetimibe adds benefit [7] |
| PCSK9 inhibitor | Evolocumab 140 mg SC fortnightly or alirocumab — if LDL remains above target on max statin ± ezetimibe | FOURIER: 15% RRR in major CV events; 20% RRR in CV death/MI/stroke [5] |
| ACE inhibitor | Ramipril 2.5–10 mg, perindopril, or lisinopril — for all post-MI, especially with LV dysfunction, diabetes, hypertension, CKD | Reduces remodelling, recurrent MI, mortality |
| Beta-blocker | Metoprolol, bisoprolol, or carvedilol — for all post-MI with LVEF ≤40%, or ongoing angina | Reduces arrhythmic death and recurrent ischaemia |
| MRA | Eplerenone or spironolactone — post-MI with LVEF ≤40% and heart failure or diabetes | Reduces mortality (EPHESUS) |
| SGLT2 inhibitor | Empagliflozin or dapagliflozin — for post-MI patients with HFrEF or diabetes | Reduces HF hospitalisation and CV death |
DWE trap on statins: The dose matters. Post-ACS, start a high-intensity statin (atorvastatin 80 mg), not a moderate-intensity one. The LDL target is <1.4 mmol/L, and "lower is better" — IMPROVE-IT and FOURIER proved that incremental LDL lowering with ezetimibe and PCSK9 inhibitors, respectively, produces further event reduction on top of statins. [1]
Lifestyle
- Smoking cessation — the single most effective secondary prevention measure. Offer nicotine replacement, varenicline, or bupropion; refer to a cessation programme.
- Cardiac rehabilitation — supervised exercise and education; reduces mortality and rehospitalisation by ~20–30%.
- Diet — Mediterranean diet (PREDIMED evidence).
- Glycaemic control — target HbA1c individually; SGLT2 inhibitors preferred for diabetics with CVD.
- Blood pressure — target <130/80 mmHg. [1]
Chronic coronary syndrome (stable CAD)
Diagnostic strategy for stable chest pain
In the patient with stable, exertional chest pain, the goal is to estimate the pre-test probability of CAD and choose the right test. Modern guidelines (NICE, ESC) now favour CT coronary angiography (CTCA) as the first-line test for low-to-intermediate probability: [1]
| Test | When | Strength |
|---|---|---|
| CT coronary angiography | Low-to-intermediate pre-test probability; rules out CAD with high NPV | Anatomical; high negative predictive value |
| Functional imaging (stress perfusion MRI, stress echo, SPECT/PET) | Intermediate-to-high probability, equivocal CTCA | Detects ischaemia, guides revascularisation |
| Exercise ECG | Less favoured now (lower sensitivity/specificity) | Cheap but limited accuracy |
Medical management of stable angina
Optimal medical therapy (OMT) is the foundation of stable CAD management. The COURAGE trial established that adding PCI to OMT does not reduce death or MI in stable CAD, though it improves symptom control [2].
- Anti-anginal therapy:
- First-line: beta-blocker (bisoprolol, metoprolol) OR calcium channel blocker (amlodipine, diltiazem) — both lower heart rate and myocardial oxygen demand.
- Second-line: add the other class (beta-blocker + CCB); long-acting nitrate (isosorbide mononitrate) — use nitrate-free interval to prevent tolerance.
- Third-line: ivabradine (if HR ≥70 in sinus rhythm despite beta-blocker), ranolazine (anti-ischaemic without haodynamic effect), nicorandil.
- Avoid short-acting nifedipine (reflex tachycardia) and combine beta-blocker with verapamil/diltiazem (bradycardia, heart block).
- Secondary prevention (as above): aspirin, statin, ACE inhibitor. [1]
Coronary angiography indications
- NSTE-ACS or STEMI — per the pathways above.
- Stable angina refractory to OMT (CCS class III–IV despite two anti-anginals).
- High-risk findings on non-invasive testing (large perfusion defect, LV dysfunction with inducible ischaemia).
- Diagnostic uncertainty after non-invasive imaging.
- Occupational requirement (e.g., pilots with chest pain). [1]
CABG vs PCI
The choice between coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) depends on anatomy, diabetes, and surgical risk. [1]
The SYNTAX trial compared CABG with PCI (using first-generation drug-eluting stents) in patients with three-vessel or left main disease [1]. At 1 year, there was no difference in death or MI, but MACCE (major adverse cardiac or cerebrovascular events) was higher with PCI, driven by repeat revascularisation. Long-term follow-up (5 and 10 years) confirmed that for patients with intermediate or high SYNTAX scores (complex anatomy), CABG was superior for MACCE, death, and MI. For low SYNTAX scores (≤22), PCI was an acceptable alternative.
Key selection rules: [1]
| Scenario | Preferred strategy |
|---|---|
| Left main disease with low/intermediate complexity | CABG or PCI (heart team decision) |
| Left main with high complexity (high SYNTAX score) | CABG |
| Three-vessel disease (especially high SYNTAX score) | CABG |
| Diabetes with multivessel disease | CABG (FREEDOM trial: lower mortality with CABG) |
| One- or two-vessel disease with low complexity | PCI |
| Prohibitive surgical risk (frailty, severe COPD, poor LV) | PCI |
DCE long-case principle: Always invoke the heart team for multivessel disease decisions. State the SYNTAX score, surgical risk (EuroSCORE/STS), and patient preference. CABG offers more durable complete revascularisation at the cost of peri-operative stroke and infection; PCI is less invasive but has higher repeat revascularisation. For diabetics with multivessel disease, CABG is preferred unless anatomy is simple. [1]
Complications of MI
Mechanical complications typically occur days 1–5 post-MI: [1]
| Complication | Timing | Presentation | Management |
|---|---|---|---|
| Cardiogenic shock | Any time | Hypotension, hypoperfusion, pulmonary oedema | Inotropes, IABP/Impella, urgent revascularisation |
| Acute VSD | Days 1–5 (peak day 3–5) | New loud pansystolic murmur at LSE, haemodynamic collapse | Urgent surgical repair; mechanical circulatory support |
| Papillary muscle rupture | Days 1–5 (inferior MI; posteromedial papillary muscle) | Acute severe MR, pulmonary oedema | Urgent MV repair/replacement |
| Free wall rupture | Days 1–5 | Sudden collapse, cardiac tamponade, electromechanical dissociation | Emergent surgery (often fatal) |
| LV aneurysm | Weeks to months | Persistent ST elevation, heart failure, thrombus, VT | Anticoagulation, surgical consideration |
| Pericarditis (early) | Days 1–4 | Pleuritic chest pain, pericardial rub, diffuse ST elevation | Aspirin/NSAIDs; avoid anticoagulation (haemorrhagic risk) |
| Dressler syndrome | Weeks to months | Fever, pleuritic pain, friction rub | NSAIDs, colchicine; aspirin first-line |
Arrhythmias are the leading cause of death in the first 24 hours:
- Ventricular fibrillation / sustained VT — defibrillate (200 J biphasic); give amiodarone if recurrent.
- Complete heart block (inferior MI — RCA supplies AV node) — usually transient; atropine, temporary wire if unstable.
- Complete heart block (anterior MI — septal infarction) — usually permanent; permanent pacemaker. [1]
Prognosis
- STEMI in-hospital mortality: ~5–6% with primary PCI; higher with cardiogenic shock (~40–50%).
- NSTEMI 6-month mortality: ~5–10%.
- Post-MI 5-year survival: ~75–85% on optimal secondary prevention.
- Predictors of poor outcome: LV dysfunction (LVEF <40%), advanced age, diabetes, renal failure, Killip class ≥III, GRACE score >140, incomplete revascularisation. [1]
DCE long-case approach
Opening statement (SASPOP)
"Mr Davies is a 66-year-old retired taxi driver who presents with an acute NSTEMI, having had three episodes of crushing central chest pain at rest over 24 hours, the last 4 hours ago. He has a background of type 2 diabetes (15 years), hypertension, hyperlipidaemia, and a 40-pack-year smoking history. [1]
His main problems are:
- Non-ST-elevation myocardial infarction — high risk (GRACE 165, troponin positive, dynamic ST depression in V4–V6)
- Type 2 diabetes (HbA1c 72 mmol/mol) — under-optimised [1]3. Stage 3 CKD (eGFR 42) — affects anticoagulant and antiplatelet choice
- Ongoing tobacco dependence
- Likely multivessel disease — will require heart team discussion re: CABG vs PCI
- Polypharmacy and medication reconciliation" [1]
Integrated management plan
- Acute: Aspirin 300 mg + ticagrelor 180 mg loading; anticoagulation with UFH; high-intensity statin (atorvastatin 80 mg); arrange coronary angiography within 24 hours (high-risk NSTE-ACS per GRACE). Glycaemic control — insulin infusion if needed. [1]2. Revascularisation: At angiography, assess SYNTAX score. If multivessel disease (especially as a diabetic), involve the heart team for CABG vs PCI. If single-vessel culprit, PCI with DES.
- Secondary prevention: Lifelong aspirin + ticagrelor for 12 months; high-intensity statin to LDL <1.4; ACE inhibitor; beta-blocker; SGLT2 inhibitor for diabetes and likely HFrEF. Smoking cessation programme.
- Comorbidity: Optimise diabetes (consider GLP-1 RA), monitor renal function with ACEi and contrast, refer to cardiac rehabilitation. [1]
DCE examiner probing questions you must anticipate:
- "Why ticagrelor over clopidogrel?" → PLATO showed ticagrelor reduced CV death/MI/stroke by 16% vs clopidogrel without an increase in major bleeding, including a mortality benefit. The exception is patients needing fibrinolysis, in whom ticagrelor is contraindicated.
- "What is his bleeding risk?" → Calculate with the CRUSADE or ACUITY score; balance against ischaemic risk (GRACE).
- "He needs CABG — when do you stop his antiplatelets?" → Aspirin continued; ticagrelor 24 h, clopidogrel 5 days, prasugrel 7 days pre-operatively. [1]
DCE short-case approach: cardiovascular examination post-MI
Instruction: "Examine this patient's cardiovascular system. You have 7 minutes." [1]
Systematic routine
- End of bed: Scars (sternotomy — CABG; left chest wall — LIMA harvest; radial artery harvest scar; catheter access sites). Pacemaker/ICD box in prepectoral region.
- Hands: Splinter haemorrhages, peripheral cyanosis, tendon xanthomata (hyperlipidaemia), xanthelasma. Pulse: rate, rhythm (AF), character (slow-rising = AS, bisferiens = AR).
- Face: Xanthelasma, corneal arcus, high arched palate (Marfan — dissection risk).
- Neck: JVP (elevated in RV failure), carotid pulse (character, bruits).
- Precordium: Apex beat (displaced = LV dilatation; hyperdynamic = volume load), parasternal heave (RV pressure overload), thrills.
- Auscultation: S1, S2 (loud/soft/split), S3 (LV failure), S4 (non-compliant LV), murmurs (MR post-MI, AS, AR), pericardial rub.
- Lungs: Bilateral basal crackles (pulmonary oedema), pleural effusions.
- Abdomen: Hepatomegaly, ascites, pulsatile liver (TR), abdominal aortic aneurysm.
- Legs: Peripheral oedema, peripheral pulses, diabetic foot changes, arterial ulcers. [1]
Presentation template
"I examined Mr Davies's cardiovascular system. He has a midline sternotomy scar consistent with prior coronary artery bypass surgery, and a left radial artery harvest scar. He is comfortable at rest. The pulse is regular at 72/min, normal volume and character. Blood pressure is 130/80. There are no stigmata of infective endocarditis. The JVP is not elevated. The apex beat is in the 5th intercostal space, mid-clavicular line, and is normal in character. Heart sounds are normal with no added sounds. There are no murmurs. The chest is clear and there is no peripheral oedema. [1]
These findings are consistent with a patient post-CABG with no clinical evidence of current cardiac decompensation. I would like to review his ECG, echocardiogram, and current medications." [1]
Key DWE MCQ patterns
- Best initial antiplatelet in ACS going to PCI: Ticagrelor 180 mg (PLATO) — unless contraindicated or fibrinolysis planned. [1]2. STEMI with primary PCI within 120 min vs fibrinolysis: Primary PCI preferred if achievable within 120 min; otherwise fibrinolytics within 30 min ("door-to-needle").
- Troponin rise in sepsis without chest pain: Not a type 1 MI — classify as type 2 MI; treat the underlying cause.
- ST depression V1–V3 with tall R waves: Posterior STEMI — confirm with V7–V9; treat as STEMI (reperfusion indicated).
- Diabetic with three-vessel disease, high SYNTAX score: CABG preferred (FREEDOM, SYNTAX long-term).
- New loud pansystolic murmur at LSE day 3 post-MI: Post-MI VSD — echocardiogram, urgent surgical repair.
- Stable angina despite two anti-anginals: Refer for coronary angiography (refractory symptoms).
- LDL 1.8 mmol/L post-ACS on atorvastatin 80 mg: Add ezetimibe (and consider PCSK9 inhibitor) — target <1.4 mmol/L. [1]
References
[1] SYNTAX — CABG vs PCI in three-vessel/left main disease (CABG superior for high-complexity lesions; SYNTAX score guides strategy). [2] COURAGE — PCI + OMT vs OMT alone in stable CAD (no difference in death/MI; PCI improves symptoms). [3] CURE — Clopidogrel added to aspirin in NSTE-ACS (20% RRR in CV death/MI/stroke; foundation of DAPT). [4] PLATO — Ticagrelor vs clopidogrel in ACS (16% RRR primary endpoint; preferred P2Y12 inhibitor). [5] FOURIER — Evolocumab (PCSK9i) on top of statin in established CVD (15% RRR major CV events; LDL lowering beyond statin). [6] TRITON-TIMI 38 — Prasugrel vs clopidogrel in ACS with PCI (superior efficacy but more bleeding; contraindicated in prior stroke/TIA). [7] IMPROVE-IT — Ezetimibe added to simvastatin post-ACS (incremental LDL lowering reduces CV events; supports "lower is better"). [8] ATLAS ACS 2–TIMI 51 — Low-dose rivaroxaban + aspirin post-ACS (dual pathway inhibition reduces ischaemic events; more bleeding).
ESC ACS Guidelines (2023); ACC/AHA/SCAI Chronic Coronary Disease Guideline (2023); National Heart Foundation of Australia / CSANZ ACS Guidelines. [1]
References
- [1]Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease N Engl J Med, 2009.PMID 19228612
- [2]Boden WE, O'Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease N Engl J Med, 2007.PMID 17387127
- [3]Yusuf S, Zhao F, Mehta SR, et al. (CURE Investigators) Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation N Engl J Med, 2001.PMID 11519503
- [4]Wallentin L, Becker RC, Budaj A, et al. (PLATO Investigators) Ticagrelor versus clopidogrel in patients with acute coronary syndromes N Engl J Med, 2009.PMID 19717846
- [5]Sabatine MS, Giugliano RP, Keech AC, et al. (FOURIER Investigators) Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease N Engl J Med, 2017.PMID 28304224
- [6]Wiviott SD, Braunwald E, McCabe CH, et al. (TRITON-TIMI 38) Prasugrel versus clopidogrel in patients with acute coronary syndromes N Engl J Med, 2007.PMID 17982182
- [7]Cannon CP, Blazing MA, Giugliano RP, et al. (IMPROVE-IT) Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes N Engl J Med, 2015.PMID 26039521
- [8]Mega JL, Braunwald E, Wiviott SD, et al. (ATLAS ACS 2–TIMI 51) Rivaroxaban in patients with a recent acute coronary syndrome N Engl J Med, 2012.PMID 22077192