Phys · cardiovascular
ECG Interpretation — Physician Level
Also known as electrocardiogram interpretation · 12-lead ECG · ECG reading · rhythm strip interpretation · electrocardiography
Consultant-physician-depth guide to systematic 12-lead ECG interpretation: rate, rhythm, axis, intervals, chamber enlargement, conduction disease, ischaemia/infarction patterns, electrolyte and drug effects, arrhythmias, and inherited channelopathies — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
ECG Interpretation — Physician Level
The answer first
Every 12-lead ECG is read in the same fixed sequence: Rate → Rhythm → Axis → Intervals → Chambers (P, QRS, ST-T) → Conduction → Ischaemia → Rhythm summary. A physician who abandons the sequence to chase the obvious pattern will miss the second abnormality that changes management. State the rate, the rhythm, the axis, and the intervals aloud — in that order — before you describe ST changes. This habit is what examiners listen for in a viva, and it is what catches the overlapping pathologies (the patient with AF who also has LBBB, old anterior Q waves, and LVH voltage). [1]
The two questions that drive every ECG in acute medicine are: Is there an occlusion that needs immediate reperfusion? and Is there a rhythm or conduction problem that needs pacing or electricity? If neither, slow down and interpret systematically. [1]
DCE trap: Examiners reward a candidate who names the rhythm and axis in one breath before the headline pattern. They fail a candidate who says "this is anterior STEMI" but cannot state whether the rhythm is sinus, the axis is normal, or the QRS is wide. [1]
Systematic approach — the five steps
Step 1 — Rate
Measure the rate from a lead II rhythm strip at the bottom of the tracing. [1]
| Method | How | When |
|---|---|---|
| 300 / large squares | Count large squares between R waves; divide into 300 | Regular rhythms |
| 1500 / small squares | Count small squares; divide into 1500 | Precise rate in regular rhythms |
| Count R waves × 6 | R waves in a 10-second (50 mm/s) strip × 6 | Any rhythm, especially irregular |
| 30 large squares × 10 | R waves in 30 large squares × 10 | Irregular rhythms, equivalent |
- Normal: 60–100 /min. Bradycardia < 60. Tachycardia > 100.
- In AF (irregular), never use the 300 method — count QRS complexes over the full 10-second strip and multiply by 6. State that the rate is an average because the rhythm is irregular.
- Atrial and ventricular rates may differ (e.g., complete heart block — atrial rate faster than ventricular). State both if they dissociate. [1]
Step 2 — Rhythm
Ask four questions on the lead II rhythm strip: [1]
- Is every P wave followed by a QRS, and every QRS preceded by a P? (AV conduction)
- Are the P waves upright in II and inverted in aVR? (sinus origin — "P-axis normal")
- Is the PR interval constant? (yes = sinus; variable = wandering pacemaker, AV block, junctional)
- Is the R–R regular? (regular vs irregularly-irregular vs regularly-irregular) [1]
- Irregularly irregular with no discrete P waves → atrial fibrillation.
- Sawtooth flutter waves at ~300/min with 2:1 conduction → atrial flutter at 150/min. A regular narrow-complex tachycardia at exactly 150/min is atrial flutter until proven otherwise.
- Regular narrow-complex tachycardia — the differential is sinus tachycardia, atrial flutter (2:1), SVT (AVNRT/AVRT), or focal atrial tachycardia. [1]
DWE high-yield: "A regular narrow-complex tachycardia at 150 bpm" — the single best answer is atrial flutter with 2:1 block, not SVT. Vagal manoeuvres or adenosine unmask the flutter waves. [1]
Step 3 — Axis
The mean frontal plane QRS axis is the sum of all depolarisation vectors. Normal is −30° to +90°. [1]
Quadrant method (leads I and aVF): [1]
| Lead I | Lead aVF | Axis |
|---|---|---|
| Positive | Positive | Normal |
| Positive | Negative | Left axis (confirm > −30°) |
| Negative | Positive | Right axis |
| Negative | Negative | Northwest (extreme right) |
Isoelectric-lead method (most accurate): the mean axis is perpendicular to the lead with the most equiphasic (biphasic) QRS, pointing toward the lead with the most positive deflection. [1]
| Axis | Definition | Common causes |
|---|---|---|
| Left axis deviation (LAD) | More negative than −30° | LAFB, LVH, inferior MI, left anterior pathway WPW, paced rhythm, chronic lung disease |
| Right axis deviation (RAD) | More positive than +90° | RVH, RVP, lateral MI, PE (acute), dextrocardia, sodium channel blocker toxicity, normal in children/tall thin adults |
The single best discriminator: If the axis is leftward and there are no pathologic Q waves or LVH to explain it, the diagnosis is left anterior fascicular block (LAFB) — QRS < 120 ms, LAD more negative than −45°, qR in I and aVL, rS in II/III/aVF. [1]
Step 4 — Intervals
| Interval | Normal | What it measures | Prolonged |
|---|---|---|---|
| PR | 120–200 ms | AV nodal conduction | First-degree AV block; hyperkalaemia; AV-nodal drugs |
| QRS | < 120 ms (≤ 110 normal) | Ventricular depolarisation | BBB, VT, hyperkalaemia, pre-excitation, pacing |
| QT (corrected, QTc) | < 440 ms (M), < 460 ms (F) | Total ventricular repolarisation | Long QT (congenital/drug/electrolyte) |
QTc correction (Bazett): QTc = QT / √(RR in seconds). Bazett over-corrects at high heart rates, so Fridericia (QT / ∛RR) is preferred at HR > 90. State the formula you use. [1]
- Long QT (QTc > 500 ms is high risk): congenital (LQT1–3), drugs (macrolides, fluoroquinolones, antipsychotics, methadone, antiarrhythmics), electrolytes (low K/Mg/Ca), hypothyroidism, hypothermia, ischaemia.
- Short QT (QTc < 340 ms): hypercalcaemia, digoxin, short QT syndrome. [1]
Step 5 — Chambers, conduction, and morphology
Now read the morphology: P-wave shape (atrial enlargement), QRS voltage and configuration (ventricular hypertrophy, blocks), and the ST segment / T wave (ischaemia, electrolytes, drugs). [1]
Chamber enlargement
P wave — atrial enlargement
| Pattern | ECG finding | Cause |
|---|---|---|
| Left atrial enlargement (P mitrale) | P notched/bifid in II, duration > 120 ms; negative P-terminal force in V1 > 1 mm² (one small box in duration × amplitude) | Mitral stenosis, MR, HCM, long-standing HTN, HFrEF |
| Right atrial enlargement (P pulmonale) | Tall peaked P > 2.5 mm in II/III/aVF | Cor pulmonale, PE, COPD, PS, tricuspid atresia |
DCE trap: P pulmonale is common in COPD and PE — examiners pair it with RAD and a prominent S wave (S1Q3T3). Do not call it "ischaemic" just because the P waves look tall. [1]
LVH criteria
Voltage criteria are sensitive but not specific; combine with strain pattern for higher specificity. [1]
| Criterion | Threshold |
|---|---|
| Sokolow-Lyon | SV1 + RV5 (or RV6) ≥ 35 mm |
| Cornell voltage | R aVL + SV3 > 28 mm (M) or > 20 mm (F) |
| Romhilt-Estes (score ≥ 5 = definite) | Voltage + strain + LA enlargement + axis + delay |
- Strain pattern = asymmetric ST depression with T inversion in lateral leads (I, aVL, V5–V6). Its presence raises specificity for true LVH.
- Isolated voltage in a young, thin or athletic patient is not LVH — call it "voltage criteria only, no strain."
- ECG detects only ~50% of echocardiographic LVH, but with high specificity (low false positives). [1]
RVH
Less common and harder. Suggestive: RAD, tall R in V1 (R:S > 1), deep S in V5/V6, RV strain (T inversion V1–V3), and often an RBBB-type pattern. Causes: cor pulmonale, congenital heart disease, severe mitral stenosis. [1]
Conduction disease
AV block
| Type | ECG | Significance |
|---|---|---|
| First-degree | PR > 200 ms, all conducted | Usually benign; monitor; avoid if pacemaker needed for other reasons |
| Second-degree Mobitz I (Wenckebach) | Progressive PR lengthening until a dropped beat; conducted PR longest before the drop, shortest after | Usually AV-nodal, benign; monitor; rarely needs pacing |
| Second-degree Mobitz II | Constant PR, sudden non-conducted P; QRS often wide | Infra-nodal (His-Purkinje); high risk of complete block; permanent pacing indicated |
| 2:1 AV block | Every other P conducted | Indeterminate — examine PR and QRS; high-grade if symptomatic |
| Third-degree (complete) | P and QRS independent; atrial faster than ventricular | Needs permanent pacing if not reversible (or temporary if inferior MI, drugs, hyperkalaemia) |
Decision rule: Mobitz II and complete heart block are infranodal and demand pacing. Mobitz I is usually nodal and benign unless symptomatic or with anterior MI. In a right-sided (inferior) MI, complete heart block is often at the AV node and may resolve; in an anterior MI, complete heart block reflects septal infarction and carries a poor prognosis. [1]
Bundle branch block
- RBBB: QRS ≥ 120 ms, rsR′ ("M-shaped") in V1, deep wide S in I/V5/V6. Common, often benign (rate-related or structural). Does not obscure ischaemia interpretation the way LBBB does.
- LBBB: QRS ≥ 120 ms, broad notched R in V5/V6/I/aVL, deep S (QS) in V1, no Q waves in lateral leads. LBBB itself produces secondary repolarisation changes — ST depression and T inversion discordant to the QRS — so ischaemia cannot be read normally. [1]
Fascicular block
| Block | Axis | QRS | Notes |
|---|---|---|---|
| LAFB | LAD more negative than −45° | < 120 ms, qR in I/aVL, rS in II/III/aVF | The commonest cause of unexplained LAD |
| LPFB | RAD +90° to +120° | < 120 ms, rS in I/aVL, qR in II/III/aVF | Rare; exclude RVH and lateral MI first |
Bifascicular and trifascicular block
- Bifascicular block = RBBB + LAFB (or RBBB + LPFB).
- Trifascicular block is loosely used for bifascicular block + first-degree AV block (all three fascicles affected: right + left anterior + left posterior with nodal delay). The risk of progression to complete heart block is real; permanent pacing is indicated if the patient is symptomatic (syncope) or progresses [6].
DWE high-yield: A patient with bifascicular block and syncope — the best next step is permanent pacemaker, not a Holter. The syncope is presumed to reflect transient complete heart block. [1]
Ischaemia and infarction
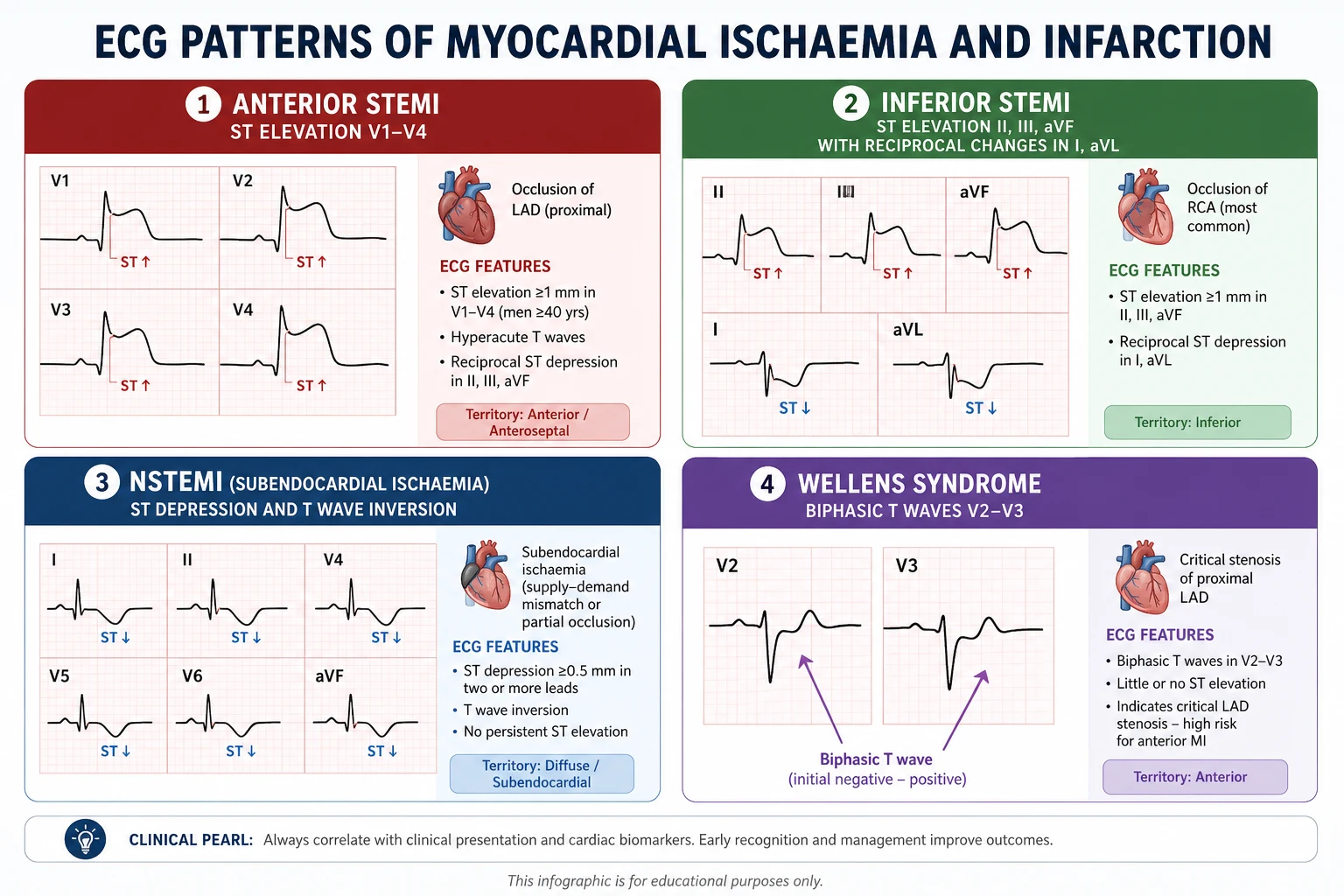
STEMI localisation
ST elevation must be ≥ 1 mm in limb leads or ≥ 2 mm in V2–V3 (men) / ≥ 1.5 mm (women), in two contiguous leads [7].
| Territory | Leads with ST elevation | Culprit artery |
|---|---|---|
| Anterior (septal) | V1–V4 | LAD / septal perforator |
| Anterior (apical) | V3–V4 | Distal LAD |
| Lateral | I, aVL, V5–V6 | Circumflex or diagonal |
| Inferior | II, III, aVF | RCA (90%) or circumflex |
| Right ventricular | V4R (ST elevation), consider V3R–V6R | Proximal RCA |
| Posterior | V7–V9 elevation; mirror in V1–V2 (tall R, ST depression, upright T) | RCA or circumflex |
The localisation rule: Inferior STEMI — look at III vs II. ST elevation in lead III > lead II points to RCA; equal elevation or more in II points to circumflex. Always record a right-sided ECG (V4R) in inferior STEMI to detect RV involvement — RV infarcts need preload and do not tolerate nitrates. [1]
Reciprocal changes
ST depression in leads opposite the infarct territory (e.g., ST depression in I/aVL in inferior STEMI, or in II/III/aVF in anterior STEMI) markedly raises the specificity of a true occlusion. Their presence supports a diagnosis of STEMI when the elevation is borderline. [1]
Posterior MI
Isolated posterior MI is easily missed because it produces ST depression and a tall R in V1–V2 — the mirror image of anterior STEMI. Confirm with posterior leads V7–V9 (ST elevation ≥ 0.5 mm). The tall R in V1 is also seen in RBBB, RVH, WPW, and Duchenne dystrophy — posterior MI is the diagnosis when there is inferior ischaemia or a clinical ACS story. [1]
STEMI equivalents — patterns you must not miss
These carry the same urgency as STEMI and require immediate reperfusion (primary PCI or thrombolysis). [1]
| Pattern | ECG features | Culprit | Management |
|---|---|---|---|
| Wellens syndrome [2] | Deep symmetrical T-wave inversion or biphasic T in V2–V3, during pain-free periods; preserved R waves; minimal/no troponin rise | Critical proximal LAD | Urgent angiography — do not stress test; avoid PCI delay |
| de Winter T waves [3] | Upsloping ST depression in V1–V6 with tall symmetrical positive T waves; often aVR ST elevation | Acute proximal LAD occlusion | Treat as STEMI — immediate reperfusion |
| Hyperacute T waves | Broad-based, tall, asymmetrical T waves, often with shortened QT, early in occlusion (before ST elevation develops) | Acute LAD occlusion (early) | Serial ECGs; treat as occlusion MI |
DCE trap: Wellens appears when the pain has settled — the ECG is most abnormal when the patient feels best. The examiner's trick is to present a pain-free patient with deep anterior T inversion and a near-normal troponin. The answer is urgent coronary angiography, not outpatient stress testing. [1]
STEMI in LBBB / paced rhythm — Sgarbossa criteria
LBBB distorts repolarisation, so you cannot read ischaemia the usual way. Use the Sgarbossa criteria [4] to diagnose occlusion MI:
| Criterion | Points |
|---|---|
| Concordant ST elevation ≥ 1 mm (in a lead with a positive QRS) | 5 |
| Concordant ST depression ≥ 1 mm in V1–V3 | 3 |
| Excessively discordant ST elevation (≥ 5 mm in a lead with negative QRS) | 2 |
A score of ≥ 3 is specific for occlusion MI (high specificity, low sensitivity). The modified Sgarbossa (Smith) criterion replaces the third rule with a proportional ratio — ST/S ratio ≥ 25% — improving sensitivity while keeping specificity. In a paced rhythm, the same criteria apply. [1]
ST depression and T-wave inversion — non-occlusion ischaemia
| Pattern | ECG | Significance |
|---|---|---|
| Subendocardial ischaemia | Horizontal/down-sloping ST depression, often in V4–V6 | Demand ischaemia, NSTEMI, severe 3-vessel disease |
| Reciprocal only | ST depression in leads opposite an unseen elevation | Look for hidden posterior or high-lateral STEMI |
| Post-ischaic T inversion | Deep symmetrical T inversion V1–V4 | Wellens, evolving STEMI, apical HCM, pulmonary embolism, stress cardiomyopathy |
| Cerebral T waves | Giant wide T inversion, QT prolongation | Raised intracranial pressure (SAH, ICH) |
DWE high-yield: Diffuse, widespread ST depression with ST elevation in aVR — the diagnosis is left main or severe 3-vessel disease (aVR sign), a high-risk ACS that needs urgent invasive management. Do not be reassured by "no ST elevation in the standard leads." [1]
Electrolytes
| Electrolyte | ECG change | Severity ladder |
|---|---|---|
| Hyperkalaemia | Peaked (tented) T → PR prolongation, P flattening → QRS widening → sine wave → asystole/VF | Sine wave = severe — give calcium gluconate immediately |
| Hypokalaemia | Flat/inverted T, ST depression, prominent U wave, QU prolongation, torsades risk | U wave taller than T = significant |
| Hypercalcaemia | Short QT (short ST segment), normal T | — |
| Hypocalcaemia | Long QT (prolonged ST segment), normal T | — |
The hyperkalaemia ladder is examined every year. The sequence is: tall peaked T waves → flattening/loss of P waves → widening of the QRS → "sine wave" merging of QRS and T → cardiac arrest. Calcium gluconate (10 mL of 10% IV) stabilises the myocardium within minutes; it does not lower potassium — follow with insulin–dextrose and a potassium binder/renin to shift and remove. [1]
Drug effects on the ECG
| Drug | ECG effect | Pitfall |
|---|---|---|
| Digoxin (therapeutic) | "Reverse-tick" ST depression (down-sloping, scooped), T flattening/inversion, short QT, increased PR | A benign effect, not toxicity — seen in lateral leads |
| Digoxin toxicity | Almost any arrhythmia — atrial tachycardia with block, bradycardia, AV block, bidirectional VT; "regularised" AF | Stop digoxin; check level; give Digibind (fragment) if severe |
| Amiodarone | QT prolongation, bradycardia, rarely T inversion | Monitor QT; stop if QTc > 500 ms |
| Class Ia (quinidine, procainamide) | QT prolongation, broadened QRS, torsades risk ("quinidine syncope") | Stop if QRS widens > 50% |
| Sotalol | Beta-blockade (bradycardia) + QT prolongation | Renal dosing; torsades risk |
| CCB / beta-blocker | Bradycardia, AV block (nodal) | — |
| Tricyclic antidepressants | Sinus tachycardia, QRS widening, QT prolongation, terminal R wave in aVR | Sodium bicarbonate for cardiotoxicity |
DWE high-yield discriminator: "Reverse-tick ST depression with a normal troponin and an controlled ventricular rate" = digoxin effect, not ischaemia. The clue is the patient is on digoxin and the changes are stable across serial ECGs. [1]
Arrhythmias
Narrow-complex tachycardia (QRS < 120 ms)
| Rhythm | ECG | First manoeuvre |
|---|---|---|
| Sinus tachycardia | Rate 100–150, normal P axis | Treat the cause |
| Atrial fibrillation | Irregularly irregular, no P waves | Rate control; consider anticoagulation (CHA₂DS₂-VASc) |
| Atrial flutter | Sawtooth waves, regular, often 150/min (2:1) | Vagal / adenosine to unmask waves; rate/rhythm control |
| AVNRT | Regular, ~180/min, P buried in QRS / pseudo-R′ in V1 | Vagal manoeuvres → adenosine |
| AVRT (WPW orthodromic) | Regular, narrow, short RP | Adenosine; avoid if AF + accessory pathway |
Wide-complex tachycardia (QRS ≥ 120 ms)
Default to ventricular tachycardia unless proven otherwise. The vast majority of regular wide-complex tachycardia in adults with structural heart disease is VT. [1]
Features favouring VT:
- AV dissociation (independent P waves, capture/fusion beats) — pathognomonic
- Concordance of QRS across the precordium (all positive or all negative)
- Extreme axis deviation, QRS > 160 ms
- History of ischaemic heart disease or cardiomyopathy [1]
Brugada algorithm (stepwise): absent AV dissociation? QRS > 100 ms in any precordial lead? Capture beats? Morphology criteria? — at each "yes," stop and call VT. [1]
DCE rule of safety: A regular broad-complex tachycardia in a patient with a cardiac history is VT until proven otherwise. Giving verapamil (an AV-nodal blocker) to VT can cause cardiovascular collapse. If unstable — synchronised cardiovert. If stable — amiodarone or procainamide. [1]
Polymorphic VT, torsades, and VF
- Polymorphic VT (PMVT): QRS morphology twists around a baseline.
- Torsades de pointes = PMVT in the setting of long QT — "twisting around the axis." Stop the offending drug, give IV magnesium (2 g), correct K⁺ (to > 4.5) and Mg, and overdrive pace if recurrent.
- PMVT with normal QT → ischaemia, Brugada, CPVT, catecholaminergic.
- Ventricular fibrillation → immediate defibrillation. [1]
Paced rhythms
A pacing spike precedes each captured beat. Assess: (1) Is there a spike? (2) Does the spike capture (a QRS follows)? (3) Is there appropriate sensing (no spikes into intrinsic QRS)?
- Failure to capture = spike with no QRS — lead displacement, battery depletion, threshold rise.
- Failure to pace = expected spike missing — oversensing, battery failure.
- Failure to sense = spikes falling on or near intrinsic T waves — undersensing, risk of R-on-T VF. [1]
Mimics and differentials
Pericarditis vs early repolarisation vs acute MI
| Feature | Pericarditis | Early repolarisation | Acute MI |
|---|---|---|---|
| ST shape | Concave (up-sloping) elevation | Concave elevation, J-point notch | Convex (domed) elevation |
| Leads | Diffuse (I, II, III, aVF, aVL, V2–V6) | Lateral/inferior, V4 especially | Territory-limited |
| Reciprocal changes | None (diffuse only) | None | Present (high specificity) |
| PR segment | Depressed (especially II, aVF; elevated aVR) | Normal | Variable |
| T waves | Initially upright; later invert | Upright tall T | Hyperacute then invert |
| Evolution | Days to weeks | Stable (compare old ECG) | Dynamic, hours |
Key discriminator: Diffuse concave ST elevation with PR depression and no reciprocal change is pericarditis. Territory-limited convex ST elevation with reciprocal change is STEMI. The single most specific feature distinguishing true STEMI from a mimic is the reciprocal change. [1]
Brugada pattern
Three repolarisation patterns in right precordial leads (V1–V2, sometimes V3), placed in the 2nd/3rd intercostal space: [1]
| Type | ST shape | coved/saddleback | Diagnostic? |
|---|---|---|---|
| Type 1 | Coved ST elevation ≥ 2 mm → negative T | Coved | Diagnostic (with clinical features) |
| Type 2 | ST elevation ≥ 2 mm, saddleback, positive T | Saddleback | Suggestive only |
| Type 3 | ST elevation < 2 mm | Either | Non-diagnostic |
Brugada syndrome requires a type 1 pattern (spontaneous or induced by sodium-channel blocker, e.g., ajmaline/flecainide) plus clinical features (syncope, aborted SCD, family history, nocturnal agonal respiration) [6]. An ICD is indicated for high-risk patients.
DWE trap: "Brugada pattern" (ECG only) is not "Brugada syndrome" (ECG + clinical). A fever can unmask a type 1 pattern. Sodium-channel blockers (flecainide, propafenone) and many drugs can worsen it — check the published drug lists. [1]
Long QT and torsades
- QTc > 470 ms (M) / > 480 ms (F) is prolonged; > 500 ms is high risk for torsades.
- Use the Schwartz score [5] for congenital LQTS: combines QTc (3/2/1 points for ≥480/460–479/450–459 ms), torsades (2), T-wave alternans (1), notched T in 3 leads (1), syncope with/without stress (2/1), congenital deafness (0.5), family history (1) and sudden death < 30 (0.5). ≥ 3.5 is high probability.
- Always exclude acquired causes first: drugs (macrolides, fluoroquinolones, antipsychotics, methadone, antiarrhythmics), hypokalaemia, hypomagnesaemia, hypocalcaemia, hypothyroidism, hypothermia, ischaemia.
- Management: stop culprit drug, correct electrolytes (K⁺ > 4.5, Mg²⁺ > 2.0), IV magnesium for torsades, overdrive pacing if recurrent. Congenital LQTS → beta-blocker ± ICD/LCSD.
WPW pre-excitation
- Short PR (< 120 ms), delta wave (slurred upstroke), widened QRS — the accessory pathway pre-excites the ventricle.
- Risk: AF conducting rapidly down the pathway → VF. In AF + WPW, the ECG shows irregular broad-complex tachycardia with varying QRS width — never give AV-nodal blockers (adenosine, verapamil, diltiazem, digoxin, beta-blockers); they allow the pathway to conduct faster. Cardiovert if unstable; otherwise procainamide or amiodarone.
- Definitive: catheter ablation of the accessory pathway. [1]
Hypertrophic cardiomyopathy
- High voltage (LVH criteria), deep T inversion V2–V6 (especially apical variant), abnormal Q waves (septal — deep narrow Q in lateral leads), left axis deviation, AF.
- Differentiate from athlete's heart: athlete's repolarisation (early repolarisation, tall T, isolated voltage) regresses with deconditioning; HCM T inversion is deep and persistent, and the wall thickness on echo is > 15 mm (or > 13 mm with family history). [1]
DCE long-case integration
In a long case, the ECG is one piece of a multi-system picture. Present it as part of the problem list, not in isolation. [1]
Template: "This 12-lead ECG shows atrial fibrillation with a controlled ventricular rate of 80, a normal axis, normal intervals, voltage criteria for left ventricular hypertrophy with lateral strain pattern, and old Q waves in the anterior leads consistent with her prior infarct." [1]
Then link each finding to a problem and an action:
- AF → anticoagulation decision (CHA₂DS₂-VASc), rate/rhythm control.
- LVH with strain → hypertensive heart disease; optimise BP; echo.
- Old anterior Q → ischaemic cardiomyopathy; check LVEF and GDMT. [1]
Use serial ECGs to track: evolving ischaemia (compare with old), response to therapy (rate control of AF), drug effect (digoxin over time), and electrolyte correction (potassium trends). [1]
DCE short-case approach — presenting an ECG
Instruction: "Interpret this ECG." [1]
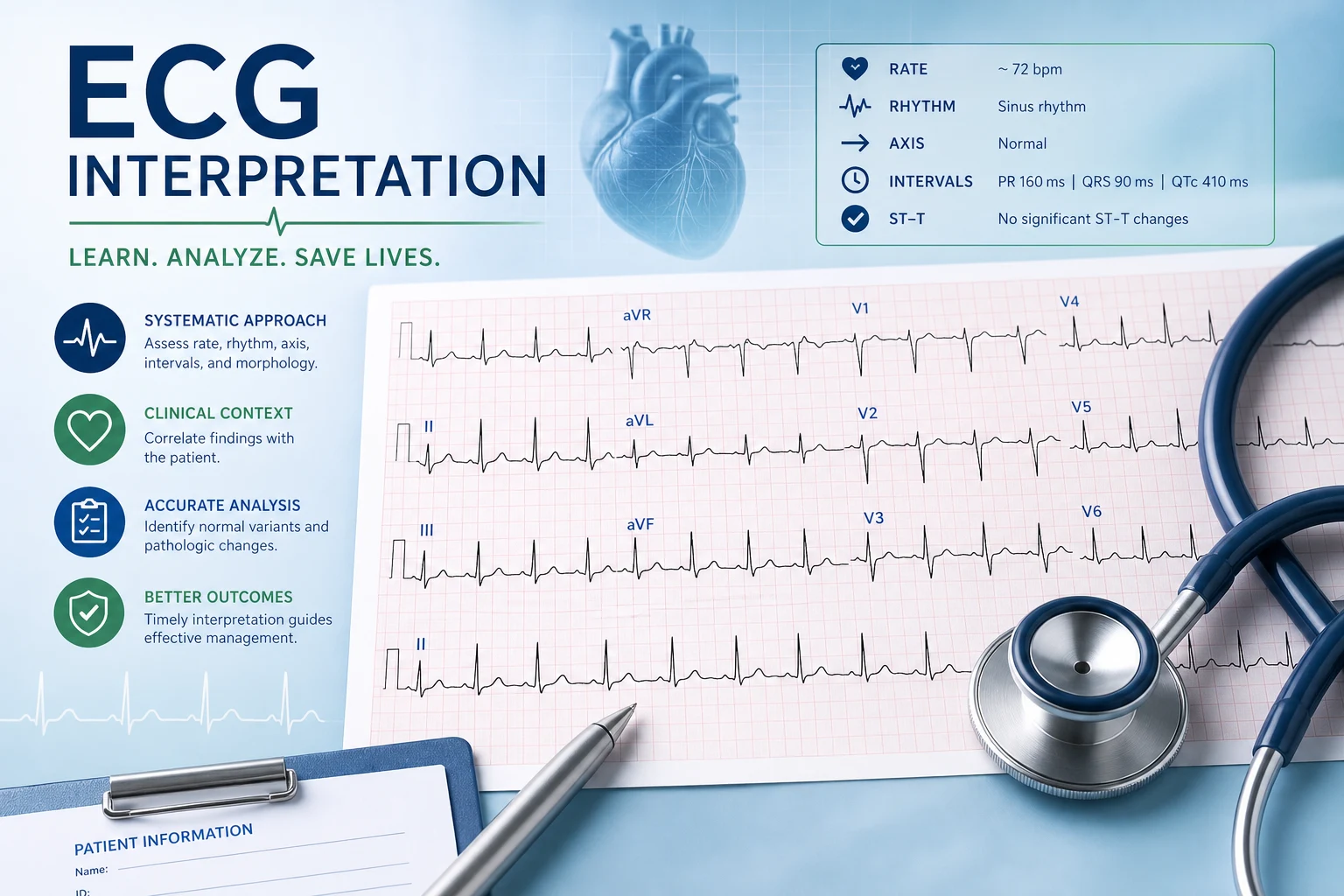
State in order, in one sentence each:
- Rate: "The rate is 75 per minute."
- Rhythm: "The rhythm is sinus — there is a P wave before every QRS and the P axis is normal."
- Axis: "The axis is normal at +30°."
- Intervals: "PR 160 ms, QRS 90 ms, QTc 420 ms — all normal."
- Morphology: "There is 2 mm of ST elevation in leads II, III and aVF with reciprocal ST depression in I and aVL."
- Conclusion: "This is an acute inferior STEMI, likely RCA territory, and I would activate the catheter laboratory now and request a right-sided ECG to assess for RV involvement." [1]
DCE trap: Examiners will press: "How do you know it is acute and not old?" — Answer: ST elevation with hyperacute T waves and reciprocal change is acute; old infarcts show Q waves and T inversion without ST elevation. Then ask for prior ECGs and troponin trend to confirm. [1]
Key DWE MCQ patterns
- Regular narrow-complex tachycardia at 150 bpm → atrial flutter with 2:1 block (unmask with adenosine/vagal).
- Regular broad-complex tachycardia in a patient with prior MI → VT until proven otherwise.
- Deep symmetrical T inversion in V2–V3, pain-free, preserved R waves, troponin minimally raised → Wellens syndrome → urgent angiography.
- Diffuse concave ST elevation + PR depression + no reciprocal change → acute pericarditis.
- Sine-wave QRS → severe hyperkalaemia → calcium gluconate now.
- ST elevation in LBBB meeting Sgarbossa (concordant ≥ 1 mm, or concordant ST depression V1–V3) → occlusion MI → reperfusion.
- Irregular broad-complex tachycardia with varying QRS width → AF with WPW → cardiovert (never AV-nodal blockers).
- QTc > 500 ms on a macrolide → stop drug, correct K/Mg, give magnesium.
- Tall R in V1 with ST depression V1–V2 in inferior ischaemia → posterior MI → posterior leads V7–V9.
- Bifascicular block + syncope → permanent pacemaker. [1]
References
[1] Kligfield et al. — AHA/ACCF/HRS ECG standardisation, Part I (defines normal limits, axis, intervals, chamber criteria). [2] de Zwaan, Bär & Wellens (1982) — Wellens syndrome: deep/biphasic T inversion in V2–V3 in a pain-free patient signals critical proximal LAD stenosis. [3] de Winter et al. (2008) — de Winter T waves: upsloping ST depression with tall symmetrical T waves is a STEMI equivalent for proximal LAD occlusion. [4] Sgarbossa et al. (1996) — Sgarbossa criteria for occlusion MI in LBBB (concordant ST change is highly specific). [5] Schwartz et al. (1993) — diagnostic score for long QT syndrome (QTc, torsades, syncope, family history). [6] Priori et al. (2013) — HRS/EHRA/APHRS consensus on inherited arrhythmia syndromes (Brugada, long QT, WPW). [7] Thygesen et al. (2018) — Fourth Universal Definition of Myocardial Infarction (ST-elevation thresholds, MI types).
ESC STEMI Guidelines (2017); ESC Atrial Fibrillation Guidelines (2020); ACC/AHA/HRS Bradycardia Guideline (2018); AHA/ACCF/HRS ECG Standardisation (Parts I–VI, 2007–2009). [1]
References
- [1]Kligfield P, Gettes LS, Bailey JJ, et al. Recommendations for the standardization and interpretation of the electrocardiogram: part I: The electrocardiogram and its technology: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: endorsed by the International Society for Computerized Electrocardiology Circulation, 2007.PMID 17322457
- [2]de Zwaan C, Bär FW, Wellens HJJ Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction Am Heart J, 1982.PMID 6121481
- [3]de Winter RJ, Verouden NJW, Wellens HJJ, Wilde AAM A new ECG sign of proximal LAD occlusion N Engl J Med, 2008.PMID 18987380
- [4]Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators N Engl J Med, 1996.PMID 8559200
- [5]Schwartz PJ, Moss AJ, Vincent GM, Crampton RS Diagnostic criteria for the long QT syndrome. An update Circulation, 1993.PMID 8339437
- [6]Priori SG, Wilde AA, Horie M, et al. HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes: document endorsed by HRS, EHRA, and APHRS in May 2013 and by ACCF, AHA, PACES, and AEPC in June 2013 Heart Rhythm, 2013.PMID 24011539
- [7]Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction (2018) Circulation, 2018.PMID 30571511