Phys · cardiovascular
Heart Failure
Also known as cardiac failure · congestive cardiac failure · CCF · congestive heart failure · chronic heart failure · acute heart failure · HFrEF · HFpEF · systolic heart failure · diastolic heart failure
Consultant-physician-depth guide to heart failure diagnosis, classification, investigation, and the four pillars of guideline-directed medical therapy (GDMT) for HFrEF — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Heart Failure
The answer first
Heart failure is a clinical syndrome of breathlessness, fatigue, and fluid retention caused by a structural or functional cardiac abnormality that results in elevated intracardiac pressures or inadequate cardiac output at rest or with stress. The universal definition requires symptoms/signs of HF plus either an LVEF ≤40% (HFrEF), LVEF 41–49% (HFmrEF), or LVEF ≥50% with objective evidence of elevated filling pressures (HFpEF). [1]
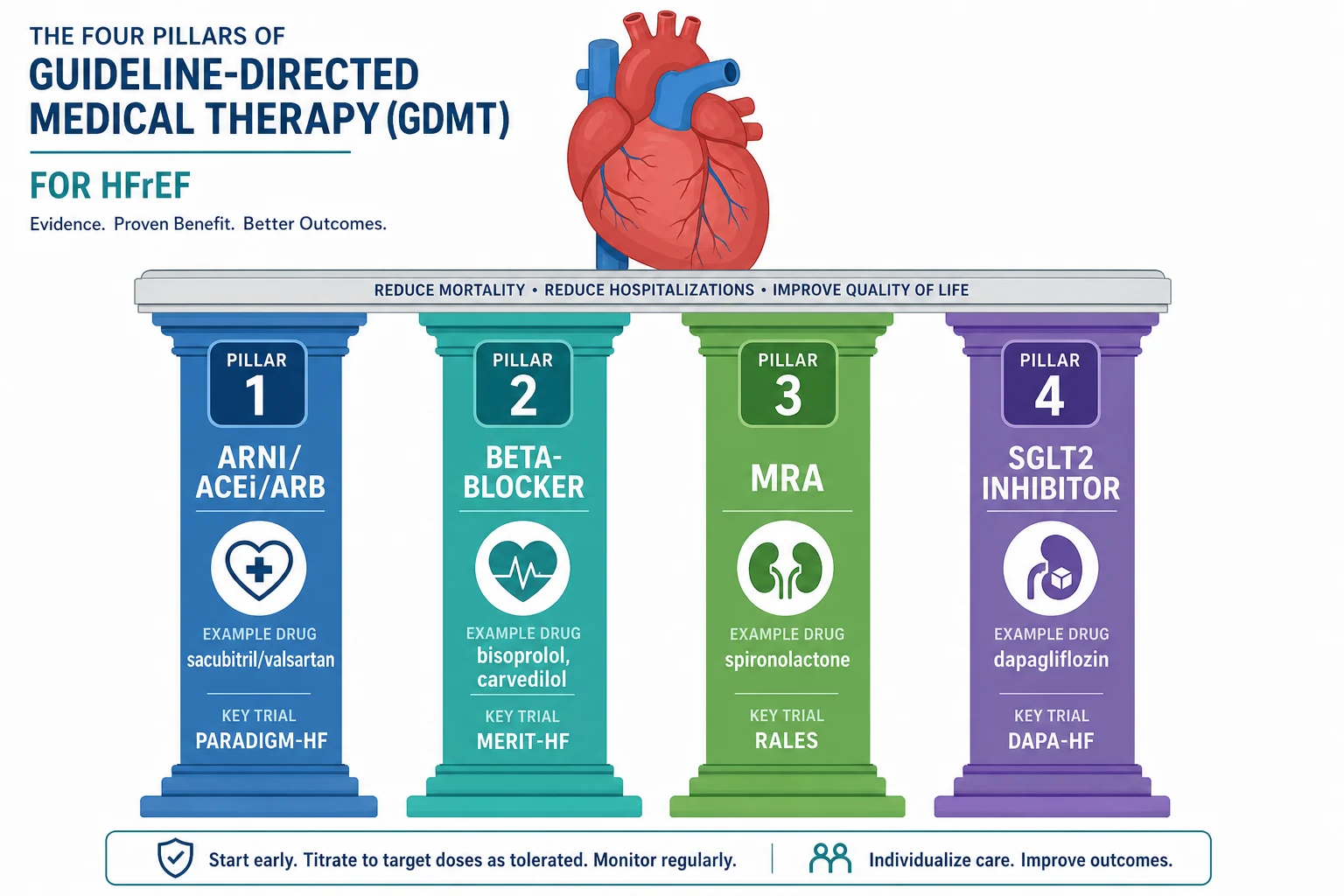
For HFrEF — the most evidence-rich phenotype — the management mandate is clear: every patient should be on all four pillars of guideline-directed medical therapy (GDMT) unless contraindicated: [1]
- ARNI (or ACE inhibitor / ARB if ARNI not tolerated)
- Beta-blocker (evidence-based: bisoprolol, carvedilol, metoprolol succinate, nebivolol)
- MRA (spironolactone or eplerenone)
- SGLT2 inhibitor (dapagliflozin or empagliflozin) [1]
Each class independently reduces mortality and hospitalisation. The modern approach is simultaneous initiation of all four at low dose, followed by rapid uptitration — not sequential addition. [1]
Classification
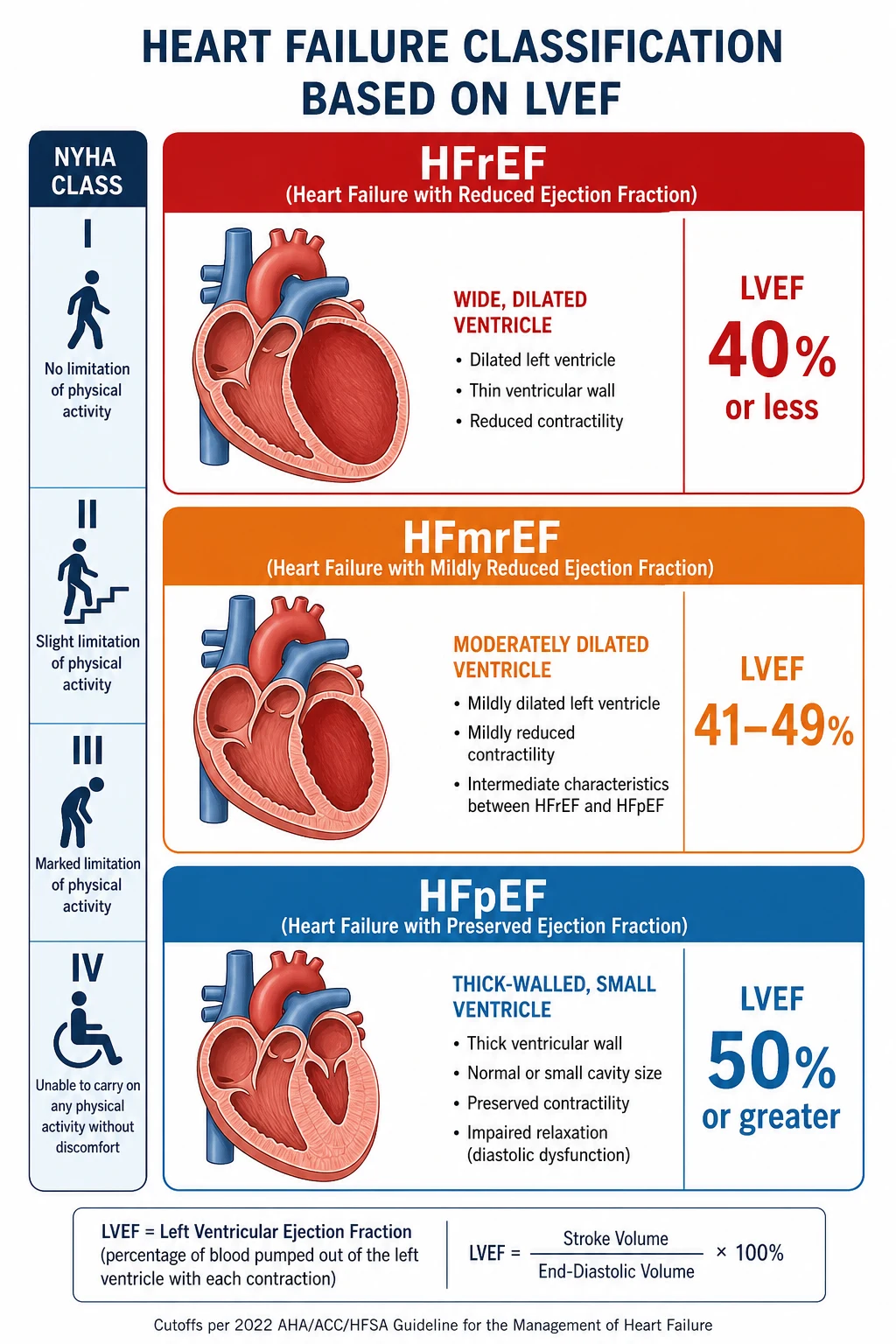
Heart failure is classified by left ventricular ejection fraction (LVEF) into three phenotypes with distinct management pathways: [1]
| Phenotype | LVEF | Key feature | GDMT evidence |
|---|---|---|---|
| HFrEF (reduced) | ≤40% | Dilated LV, impaired contractility | Strong for all four pillars |
| HFmrEF (mildly reduced) | 41–49% | Intermediate phenotype | SGLT2i recommended; other agents reasonable |
| HFpEF (preserved) | ≥50% | Thick-walled LV, impaired relaxation + elevated filling pressures | SGLT2i recommended; diuretics for congestion; treat comorbidities |
NYHA functional classification (symptom severity, used for all phenotypes): [1]
| Class | Description |
|---|---|
| I | No limitation; ordinary activity causes no symptoms |
| II | Slight limitation; comfortable at rest; ordinary activity causes symptoms |
| III | Marked limitation; less-than-ordinary activity causes symptoms |
| IV | Symptoms at rest; unable to carry out any physical activity without discomfort |
DCE trap: Examiners will ask you to state the patient's NYHA class and why it matters — it guides therapy decisions and prognosis. A patient who is breathless walking around the house is NYHA III, not II. [1]
Pathophysiology
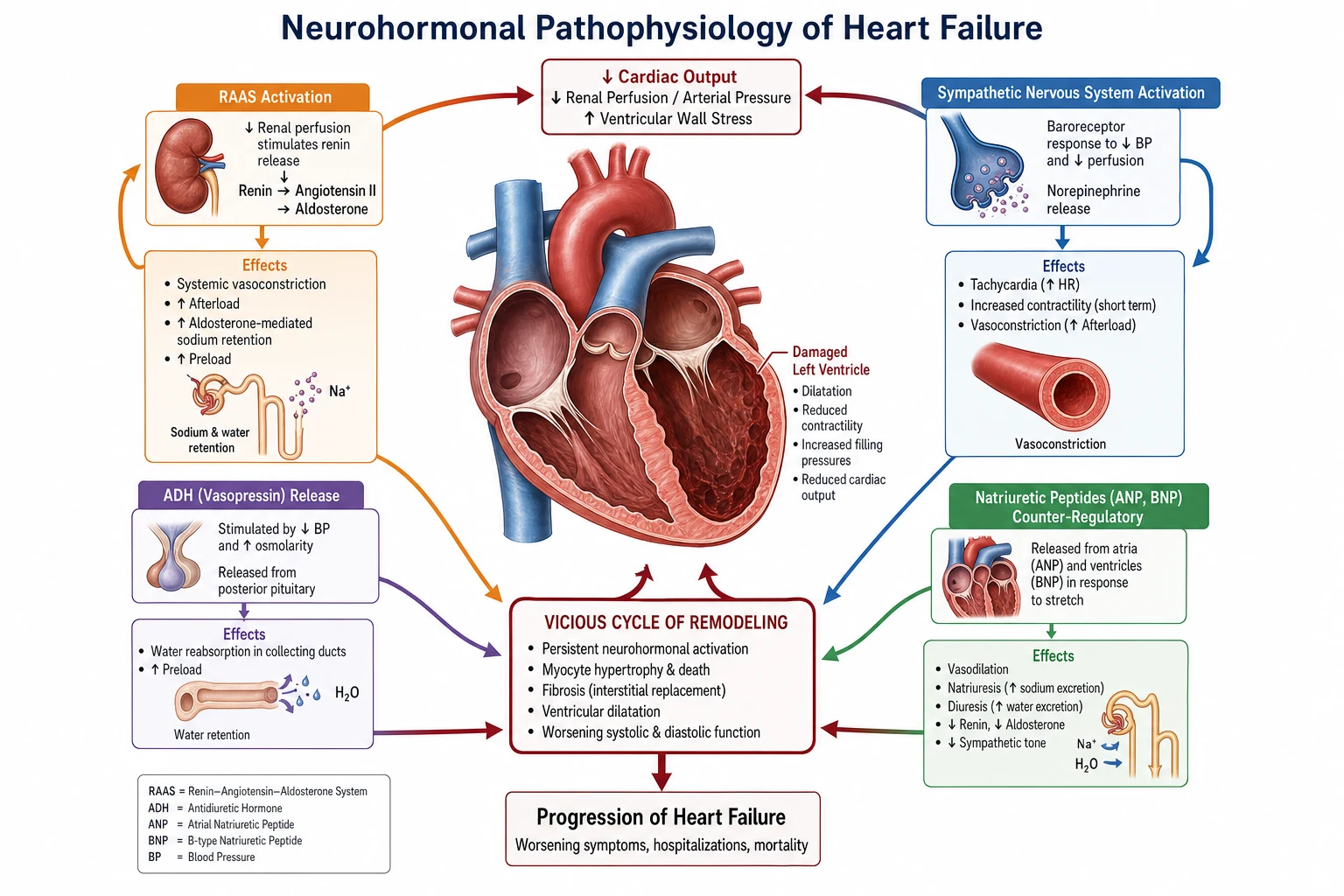
Heart failure is not simply a pump problem. It is a neurohormonal syndrome. When cardiac output falls, the body activates compensatory systems that are initially helpful but become maladaptive over time, driving progressive remodelling and worsening: [1]
| System | What it does | Why it harms long-term |
|---|---|---|
| RAAS (renin → angiotensin II → aldosterone) | Vasoconstriction, sodium/water retention | Increases afterload and preload; aldosterone drives fibrosis and remodelling |
| Sympathetic nervous system (norepinephrine) | Tachycardia, increased contractility, vasoconstriction | Increases myocardial oxygen demand; ischaemia; myocyte apoptosis; arrhythmias |
| ADH / vasopressin | Water retention (V2 receptors), vasoconstriction (V1) | Dilutional hyponatraemia; volume overload |
| Natriuretic peptides (ANP, BNP) | Vasodilation, natriuresis, RAAS antagonism (counter-regulatory) | Overwhelmed by maladaptive systems; BNP is a diagnostic biomarker |
This is why every GDMT agent works by blocking a maladaptive pathway: ACEi/ARNI block RAAS; beta-blockers block SNS; MRAs block aldosterone; SGLT2i reduce preload and have pleiotropic effects on cardiac metabolism and fibrosis. [1]
DWE high-yield: "Why do beta-blockers — negative inotropes — improve survival in heart failure?" Answer: by blocking chronic SNS activation that drives remodelling, arrhythmias, and myocyte death. The paradox is that drugs that acutely worsen contractility chronically save lives. [1]
Clinical presentation
Chronic heart failure
Symptoms (in order of frequency):
- Exertional dyspnoea (sensitive; progresses over time)
- Orthopnoea (suggests elevated left-sided filling pressures)
- Paroxysmal nocturnal dyspnoea (PND)
- Fatigue and exercise intolerance (low cardiac output)
- Ankle swelling (right-sided congestion)
- Less common: nocturnal cough, abdominal bloating, cachexia, confusion (elderly) [1]
Signs (elicit these systematically in the short case):
- Elevated JVP — the single most specific bedside sign of decompensated HF
- Basal inspiratory crackles — bilateral, don't clear with coughing
- Peripheral oedema — ankle/sacral; pitting; may be absent in chronic HF even with volume overload
- S3 gallop — specific but low-sensitivity; indicates elevated LVEDP
- Displaced apex beat — laterally displaced in HFrEF (dilated LV)
- Hepatomegaly and ascites — right-sided congestion
- Functional murmurs — mitral regurgitation (annular dilatation) or tricuspid regurgitation (RV dilatation) [1]
Acute decompensated heart failure
Acute onset or worsening of symptoms, often requiring emergency presentation:
- Acute pulmonary oedema: pink frothy sputum, respiratory distress, widespread crackles, hypoxia
- Cardiogenic shock: hypotension (SBP <90), cold peripheries, oliguria, altered mental state
- Precipitants: ACS, AF/atrial flutter, infection, non-adherence, anaemia, thyroid dysfunction, renal failure, NSAIDs [1]
DCE short-case trap: Do not miss the functional TR murmur. In a dilated right ventricle, tricuspid annular dilatation produces a pansystolic murmur at the lower left sternal edge, louder on inspiration (Carvallo's sign). Examiners will ask you to explain why it varies with respiration. [1]
Differential diagnosis
The key DWE/DCE question: what else causes dyspnoea and fluid overload? [1]
| Condition | Discriminating features |
|---|---|
| COPD | Smoking history, wheeze, prolonged expirium, PFT obstruction; can coexist |
| Pulmonary embolism | Pleuritic pain, DVT risk factors, sudden onset, hypocapnia on ABG |
| Anaemia | Pallor, fatigue, normal JVP/crackles; check Hb |
| Cirrhosis with ascites | Stigmata of chronic liver disease; low albumin; coagulopathy |
| CKD | Elevated creatinine, proteinuria; bilateral leg oedema without pulmonary congestion |
| Hypoalbuminaemia | Low serum albumin from any cause; no JVP elevation |
| Venous insufficiency | Chronic leg changes (haemosiderin, lipodermatosclerosis); normal JVP |
| Pulmonary hypertension | Loud P2, RV heave, elevated JVP with prominent v-waves (TR) |
Key tool: BNP / NT-proBNP. Natriuretic peptides are the most powerful single blood test to rule in or out heart failure:
- NT-proBNP <300 pg/mL (BNP <100) → HF unlikely (high negative predictive value)
- NT-proBNP >450 pg/mL (age <50), >900 (age 50–75), >1800 (age >75) → HF likely
- Intermediate range → echocardiogram required [1]
Limitations: BNP is falsely low in obesity and can be falsely elevated by AF, renal failure, PE, sepsis, and age. It is a rule-out test first. [1]
Investigations
Essential for every patient
| Investigation | Why |
|---|---|
| Transthoracic echocardiogram (TTE) | The pivotal investigation: LVEF, LV size/wall thickness, valve function, RV function, pericardial effusion, estimated pulmonary artery pressure |
| ECG (12-lead) | Look for: AF/flutter, Q waves (prior MI), LVH, LBBB, low voltage (pericardial effusion/amyloid), QT interval |
| Bloods: FBE, U&E, creatinine, eGFR, LFTs, TFTs | Screen for anaemia, renal dysfunction, hepatic congestion, thyroid disease |
| Iron studies (ferritin + transferrin saturation) | Iron deficiency (ferritin <100 or TSAT <20%) is present in ~50% of HF patients and independently worsens outcomes |
| NT-proBNP | Confirms/refutes HF diagnosis; stratifies prognosis |
| Troponin | May be chronically low-grade elevated; acute rise suggests decompensation or type 2 MI |
| Urinalysis | Rule out proteinuria as a contributor to oedema |
| Chest X-ray | Cardiomegaly, pulmonary venous congestion, Kerley B lines, pleural effusions, pulmonary oedema |
| HbA1c, fasting lipids | Comorbidity screening (diabetes, dyslipidaemia) |
Selected investigations (based on clinical context)
| Investigation | When |
|---|---|
| Coronary angiography | If ischaemia suspected as the cause; angina, prior MI, high-risk features |
| Cardiac MRI | Infiltrative disease (amyloid, sarcoid), myocarditis, LV non-compaction; tissue characterisation |
| CPET (cardiopulmonary exercise testing) | When diagnosis unclear; objective assessment of functional capacity and ventilatory efficiency |
| Right heart catheterisation | Pulmonary hypertension workup; suspected cardiogenic shock; pre-transplant assessment |
| Endomyocardial biopsy | Rare; suspected myocarditis, infiltrative disease, transplant rejection |
DWE trap: A common MCQ presents a patient with dyspnoea, normal echocardiogram LVEF but elevated filling pressures on echo (E/e' ratio >14, dilated LA). The answer is HFpEF, not "no cardiac cause." HFpEF requires objective evidence of elevated filling pressures, not just preserved LVEF. [1]
Management of HFrEF — the four pillars
Pillar 1: ARNI (or ACE inhibitor / ARB)
ARNI (sacubitril/valsartan) is the preferred first-line RAAS blocker for HFrEF, based on PARADIGM-HF which showed a 20% reduction in the composite of cardiovascular death or HF hospitalisation versus enalapril [1].
| Drug | Starting dose | Target dose | Notes |
|---|---|---|---|
| Sacubitril/valsartan (ARNI) | 49/51 mg BID (or 24/26 mg BID if low BP or CKD) | 97/103 mg BID | Washout 36h from ACEi (risk of angioedema) |
| Ramipril (ACEi) | 2.5 mg BD | 10 mg BD | If ARNI not available/tolerated |
| Valsartan (ARB) | 40 mg BD | 160 mg BD | If ACEi cough/angioedema |
Monitoring: Check U&E at 1–2 weeks after initiation and each dose uptitration. Expect a creatinine rise of up to 30% and potassium up to 5.5 mmol/L — this is acceptable and does not mandate stopping. If creatinine rises >30% or K+ >5.5, reduce dose and investigate. [1]
Pillar 2: Evidence-based beta-blocker
Only four beta-blockers have mortality evidence in HFrEF: bisoprolol, carvedilol, metoprolol succinate, and nebivolol (for patients ≥70 years). Other beta-blockers are not equivalent. [1]
| Drug | Starting dose | Target dose | Notes |
|---|---|---|---|
| Bisoprolol | 1.25 mg OD | 10 mg OD | Most cardioselective; simplest dosing |
| Metoprolol succinate | 12.5–25 mg OD | 200 mg OD | Must be succinate, not tartrate |
| Nebivolol | 1.25 mg OD | 10 mg OD | For age ≥70 (SENIORS trial); NO-mediated vasodilation |
Key principle: Start low, go slow — but don't stop. Double the dose every 2–4 weeks toward target. Temporary congestion may need diuretic adjustment. [1]
Pillar 3: MRA (mineralocorticoid receptor antagonist)
| Drug | Starting dose | Target dose | Notes |
|---|---|---|---|
| Spironolactone | 12.5–25 mg OD | 50 mg OD | RALES trial in NYHA III–IV [3]; gynaecomastia in ~10% |
| Eplerenone | 25 mg OD | 50 mg OD | EMPHASIS-HF in NYHA II; lower gynaecomastia risk; post-MI |
Monitoring: K+ at 1 week, 1 month, then 3-monthly. The combination of RAAS blockade + MRA makes hyperkalaemia the key safety concern. [1]
Pillar 4: SGLT2 inhibitor
Dapagliflozin (DAPA-HF) and empagliflozin (EMPEROR-Reduced) reduce HF hospitalisation and cardiovascular death in HFrEF regardless of diabetes status [2]. This is the only drug class with benefit across the entire EF spectrum (HFrEF, HFmrEF, and HFpEF — EMPEROR-Preserved and DELIVER trials).
| Drug | Dose | Notes |
|---|---|---|
| Dapagliflozin | 10 mg OD | No dose adjustment for HF alone; monitor volume status |
| Empagliflozin | 10 mg OD | Same evidence base; equivalent efficacy |
Safety: Genital mycotic infections, volume depletion (monitor if on diuretics), euglycaemic DKA (rare in non-diabetics). Not recommended if eGFR <20. [1]
Additional HFrEF therapies
| Therapy | Indication | Evidence |
|---|---|---|
| Ivabradine | HFrEF (LVEF ≤35%) in sinus rhythm with HR ≥70 bpm despite max-tolerated beta-blocker | SHIFT trial; reduces HF hospitalisation |
| Hydralazine + nitrate | Self-identified African ancestry with HFrEF on optimal GDMT; or RAAS intolerance | A-HeFT; adds to GDMT |
| Digoxin | Symptom control / rate control in AF; no mortality benefit | DIG trial |
| Vericiguat | Recent HF worsening/hospitalisation | VICTORIA trial; modest benefit in high-risk patients |
| Loop diuretic (frusemide) | Symptomatic congestion | Symptom relief only; no mortality evidence |
Device therapy
| Device | Indication |
|---|---|
| ICD (primary prevention) | HFrEF LVEF ≤35%, NYHA II–III, ≥3 months optimal GDMT, expectation of survival >1 year with good functional status |
| CRT (cardiac resynchronisation therapy) | HFrEF LVEF ≤35% + LBBB (QRS ≥150 ms preferred) |
| ICM (implantable cardiac monitor) | Recurrent unexplained syncope in HF; arrhythmia surveillance |
Management of HFpEF
HFpEF has no mortality-reducing pharmacotherapy except SGLT2 inhibitors (EMPEROR-Preserved, DELIVER). Management is: [1]
- SGLT2 inhibitor (dapagliflozin or empagliflozin) — reduces HF hospitalisation
- Diuretics for congestion symptom control
- Aggressively treat comorbidities — hypertension, AF, diabetes, obesity, sleep apnoea
- Treat iron deficiency with IV iron (ferric carboxymaltose)
- Avoid overly aggressive preload reduction (may cause hypotension in stiff ventricles) [1]
DWE high-yield contrast: ACE inhibitors, ARBs, and beta-blockers — despite being first-line in HFrEF — have not shown consistent mortality benefit in HFpEF. The PEP-CHF, I-PRESERVE, and CHARM-Preserved trials were neutral. [1]
Acute decompensated heart failure
Immediate management (ABCDE)
- Airway/Breathing: Sit upright, high-flow oxygen if hypoxic (target SpO₂ >90%). NIV (CPAP or BiPAP) if pulmonary oedema with respiratory distress — reduces work of breathing and afterload.
- Circulation: IV access. If hypertensive (SBP >110): IV glyceryl trinitrate infusion (start 10–20 mcg/min, titrate) to reduce preload/afterload. If hypotensive: vasopressors/inotropes. [1]3. Diurese: IV frusemide — initial dose 20–40 mg IV if naive, or 1–2× the usual oral dose if on chronic frusemide. Assess response at 30 min (urine output target: 100–150 mL/h in first 2 hours).
- Identify and treat the precipitant: ACS? Arrhythmia? Sepsis? Non-adherence? Thyroid? Anaemia?
- Escalate: If shock or refractory hypoxaemia — ICU for inotropes (dobutamine, milrinone), mechanical circulatory support (IABP, Impella, VA-ECMO). [1]
Key principles
- Do not routinely give morphine — associated with worse outcomes in registries; reserve for severe distress.
- Do not routinely give oxygen to non-hypoxic patients — vasoconstriction may worsen outcomes.
- Monitor urine output hourly in the first 6 hours — suboptimal diuresis predicts poor outcome. [1]
Comorbidities and complications
| Comorbidity | Why it matters | Management |
|---|---|---|
| Iron deficiency | Present in ~50%; worsens symptoms independent of anaemia | IV ferric carboxymaltose (FAIR-HF, AFFIRM-AHF) improves symptoms and exercise capacity |
| AF | Present in 30–40%; worsens HF; increases stroke risk | Anticoagulate (CHA₂DS₂-VASc); rate or rhythm control |
| CKD | Cardiorenal syndrome — bidirectional harm | SGLT2i (renoprotective); monitor K+; may need dose adjustment |
| Diabetes | Increases HF risk; some agents worsen HF (TZDs) | SGLT2i preferred; avoid pioglitazone |
| Depression | Common; worsens outcomes; affects adherence | Screen and treat |
| Obesity | Inflammation; volume overload; sleep apnoea | Weight management; screen for OSA |
| Sleep-disordered breathing | 50–70% of HF patients | Sleep study; CPAP/ASV if indicated |
Cardiorenal syndrome
A common DCE long-case trap. Five types exist; the key clinical question is: is the creatinine rising because of HF or despite HF treatment? [1]
- Type 1 (acute cardiorenal): Acute HF causes AKI (low forward flow, venous congestion).
- Type 2 (chronic cardiorenal): Chronic HF causes progressive CKD.
- Management principle: Venous congestion (not just low output) drives renal dysfunction. Decongestion helps the kidneys, even if creatinine rises transiently. Do not stop diuretics for a modest creatinine rise if the patient is still overloaded. [1]
Prognosis
- HFrEF 1-year mortality: ~10–15% on modern GDMT (down from ~20–30% pre-GDMT era).
- HFpEF prognosis: similar to HFrEF when matched for symptoms.
- Key prognostic markers: LVEF, NYHA class, BNP/NT-proBNP, peak VO₂ on CPET, 6-minute walk distance, renal function, hyponatraemia, QRS duration, troponin.
- The Seattle Heart Failure Model integrates multiple variables to estimate 1-, 2-, and 3-year survival. [1]
DCE long-case approach
Opening statement (SASPOP)
"Mrs Smith is a 72-year-old woman who presents with progressive exertional dyspnoea, orthopnoea, and bilateral ankle swelling over three months. She has a background of ischaemic heart disease (NSTEMI 2019, DES to LAD), type 2 diabetes, hypertension, stage 3B CKD (eGFR 38), and paroxysmal atrial fibrillation. [1]
Her main problems are:
- Heart failure with reduced ejection fraction (LVEF 32%), NYHA class III
- Iron deficiency anaemia (ferritin 45, TSAT 15%)
- Paroxysmal atrial fibrillation on apixaban
- Stage 3B CKD — cardiorenal overlap
- Polypharmacy (12 regular medications)
- Social isolation — lives alone, at risk of non-adherence" [1]
Integrated management plan
Present the plan in four domains: [1]
- Pharmacological: Confirm all four GDMT pillars on board; check doses against target; identify gaps (e.g., not on SGLT2i — add dapagliflozin 10 mg OD). Address iron deficiency (IV ferric carboxymaltose). Optimise AF anticoagulation.
- Device: Is she eligible for ICD/CRT? Check LVEF ≤35%, NYHA II–III, >3 months on optimal GDMT, >1 year expected survival. Check QRS duration for CRT.
- Comorbidity: Optimise diabetes (SGLT2i dual benefit); monitor renal function; address sleep apnoea risk.
- Social/communication: Medication reconciliation; heart failure nurse; advance care planning; cardiac rehabilitation. [1]
DCE examiner probing questions you must anticipate:
- "Why is her creatinine rising?" → Decongestion is the priority; modest creatinine rise is expected and acceptable if still overloaded.
- "Would you anticoagulate her?" → Yes; CHA₂DS₂-VASc is likely high; HAS-BLED must be considered.
- "What dose adjustments are needed for her CKD?" → Check each drug's renal threshold; apixaban dose depends on age/weight/creatinine.
- "What is her prognosis?" → Use Seattle HF Model; discuss honestly with the patient. [1]
DCE short-case approach: cardiovascular examination
Instruction: "Examine this patient's cardiovascular system." [1]
Systematic routine
- Hands: Clubbing (infective endocarditis, cyanotic HD), splinter haemorrhages, peripheral cyanosis, pulse (rate, rhythm, character — check for bounding pulse of AR, slow-rising of AS, alternans in severe LVF).
- Face: Malar flush (mitral stenosis), dysmorphic features (Marfan, Down), pallor.
- Eyes: Conjunctival pallor, xanthelasma, arcus senilis, Horner's syndrome.
- Mouth: Central cyanosis, high arched palate, dentition (endocarditis risk).
- Neck: JVP — assess for elevated pressure, waveform (cannon A waves, prominent V waves of TR, loss of A waves in AF). Carotid pulse — character and volume.
- Praecordium: Inspect for scars (sternotomy, pacemaker), visible impulses. Palpate apex beat (position and character — displaced in HFrEF, heaving in pressure overload, tapping in mitral stenosis). Palpate for parasternal heave (RV pressure overload), thrills.
- Auscultation: Listen systematically — apex, lower left sternal edge, upper left sternal edge (pulmonary), upper right sternal edge (aortic). Identify S1, S2 (split?), added sounds (S3, S4, clicks), murmurs (timing, location, radiation, grade, pitch, relationship to respiration).
- Back: Basal crackles (pulmonary oedema), pleural effusion (stony dull).
- Abdomen: Hepatomegaly (congestion), ascites, pulsatile liver (TR), splenomegaly.
- Legs: Peripheral oedema, peripheral pulses (femoral, popliteal, posterior tibial, dorsalis pedis), signs of DVT. [1]
Presentation template
"I examined Mr Jones's cardiovascular system. He is comfortable at rest. The pulse is irregularly irregular at 82/min, consistent with atrial fibrillation. Blood pressure is 130/80. The JVP is elevated 4 cm above the sternal angle. The apex beat is displaced to the 6th intercostal space, anterior axillary line, and is diffuse in character, suggesting left ventricular dilatation. On auscultation, there is a third heart sound at the apex and a soft pansystolic murmur radiating to the axilla, consistent with functional mitral regurgitation. Basal inspiratory crackles are present bilaterally, and there is pitting oedema to the mid-shin bilaterally. [1]
These findings are consistent with decompensated heart failure with reduced ejection fraction, complicated by atrial fibrillation and functional mitral regurgitation." [1]
Key DWE MCQ patterns
- Best initial drug in a new HFrEF patient: Start low-dose beta-blocker + RAAS blocker simultaneously (not sequential). Add MRA and SGLT2i early.
- Creatinine rises 25% after starting ramipril: Continue — acceptable rise up to 30%.
- Which beta-blocker in HF? Bisoprolol, carvedilol, metoprolol succinate, or nebivolol — not atenolol or propranolol.
- HFpEF management: SGLT2i + diuretics for congestion + treat comorbidities. ACEi/ARB/beta-blocker do not have mortality evidence in HFpEF.
- When to add ivabradine: Sinus rhythm, LVEF ≤35%, HR ≥70 despite max-tolerated beta-blocker.
- Patient with HF and iron deficiency (ferritin <100): Give IV ferric carboxymaltose — improves symptoms regardless of Hb. [1]
References
[1] PARADIGM-HF — ARNI vs enalapril in HFrEF (20% RRR composite CV death/HF hospitalisation). [2] DAPA-HF — Dapagliflozin in HFrEF (26% RRR composite worsening HF/CV death), independent of diabetes. [3] RALES — Spironolactone in severe HF (30% mortality reduction). [4] MERIT-HF — Metoprolol succinate in chronic HF (34% mortality reduction).
ESC HF Guidelines (2021); ACC/AHA/HFSA HF Guideline (2022); National Heart Foundation of Australia / CSANZ HF Guidelines. [1]
References
- [1]McMurray JJV, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure N Engl J Med, 2014.PMID 25176015
- [2]McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction N Engl J Med, 2019.PMID 31535829
- [3]Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators N Engl J Med, 1999.PMID 10471456
- [4]MERIT-HF Study Group Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF) Lancet, 1999.PMID 10376614