Phys · cardiovascular
Hypertension
Also known as high blood pressure · raised blood pressure · systemic hypertension · essential hypertension · primary hypertension · secondary hypertension · resistant hypertension · hypertensive emergency · accelerated hypertension · malignant hypertension · isolated systolic hypertension
Consultant-physician-depth guide to hypertension — definition and classification across ANZ/UK/US guidelines, pathophysiology, secondary causes workup, target organ damage, lifestyle and pharmacological management, resistant hypertension, and hypertensive emergencies. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Hypertension
Key decision at the bedside
Hypertension is the single most important modifiable risk factor for cardiovascular disease and the leading attributable cause of death worldwide. The registrar's job at every encounter is threefold: confirm the BP is genuinely elevated (not white-coat), assess for target organ damage, and decide on a target and a plan the patient will actually follow. Do not reflexively start tablets on one raised reading. [1]
Definition and classification
The threshold depends on the guideline — know the difference
There are two diagnostic frameworks in worldwide use. Both are defensible; the trap is conflating them. [1]
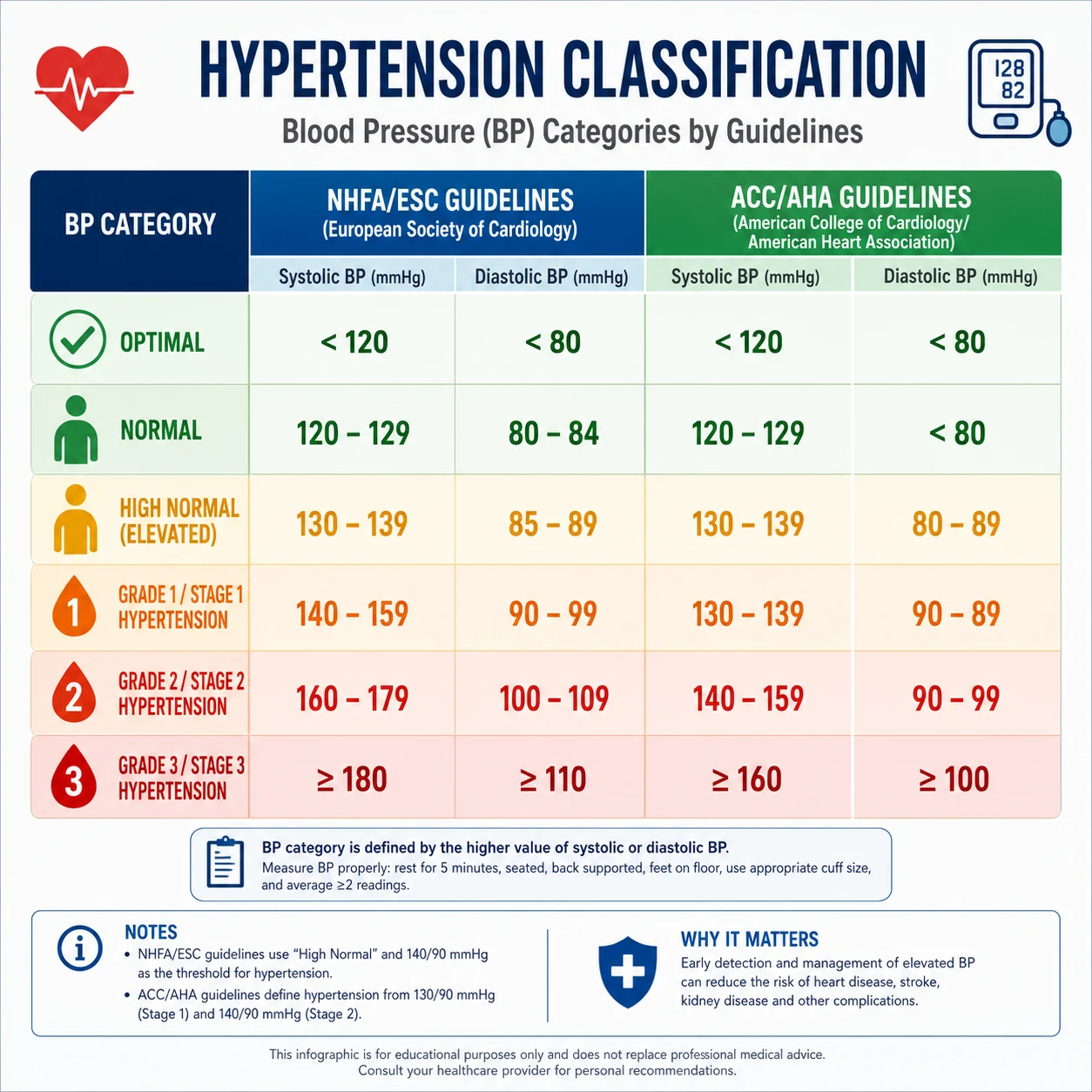
ESC/ESH 2023 and National Heart Foundation of Australia (NHFA) — the ANZ/UK standard: [1]
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Optimal | under 120 | under 80 |
| Normal | 120–129 | 80–84 |
| High normal | 130–139 | 85–89 |
| Hypertension | 140 or above | 90 or above |
| Grade 1 | 140–159 | 90–99 |
| Grade 2 | 160–179 | 100–109 |
| Grade 3 | 180 or above | 110 or above |
| Isolated systolic | 140 or above | under 90 |
2017 ACC/AHA — the US standard: [1]
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Normal | under 120 | under 80 |
| Elevated | 120–129 | under 80 |
| Stage 1 | 130–139 | 80–89 |
| Stage 2 | 140 or above | 90 or above |
The ACC/AHA 'Stage 1' (130–139/80–89) maps to ESC/ESH 'high normal'. In ANZ and UK practice, 140/90 mmHg remains the treatment threshold. The ACC/AHA framework labels far more people as hypertensive, and treatment decisions in the 130–139 band are driven by cardiovascular risk rather than the number alone. Quote the guideline you are using in the exam — never mix the two. [1]
Confirm before you diagnose
A single elevated clinic reading is not a diagnosis. Confirm with ambulatory blood pressure monitoring (ABPM) or home BP monitoring (HBPM) over several days. ABPM is the gold standard because it removes white-coat effect, captures nocturnal BP (a powerful prognostic marker), and correlates better with target organ damage than clinic readings. [1]
Equivalent thresholds across measurement methods (ESC/ESH 2023): [1]
| Method | Systolic | Diastolic |
|---|---|---|
| Office/clinic | 140 | 90 |
| ABPM (24-hour mean) | 130 | 80 |
| ABPM (daytime mean) | 135 | 85 |
| ABPM (nighttime mean) | 120 | 70 |
| Home BP (mean) | 135 | 85 |
Masked hypertension — normal clinic but raised out-of-office — carries the same risk as sustained hypertension. Suspect it in patients with stress, obstructive sleep apnoea, or a normal clinic reading but target organ damage out of proportion to the measured BP. [1]
Why it matters clinically
Blood pressure is a continuous risk variable — risk doubles for every 20/10 mmHg rise from 115/75. There is no sharp biological threshold; the cut-offs exist to trigger action. The reason hypertension is dangerous is sustained pressure driving target organ damage: left ventricular hypertrophy, heart failure, ischaemic heart disease, stroke, chronic kidney disease, hypertensive retinopathy, and aortic dissection. [1]
Pathophysiology
The simple model that explains management
Blood pressure equals cardiac output × systemic vascular resistance (SVR). In young hypertension, the problem is often increased cardiac output (sympathetic overactivity, high renin). In older patients with isolated systolic hypertension, the dominant problem is increased SVR from stiff, inelastic large arteries — each systole generates a higher pressure wave because the aorta cannot expand to absorb it. [1]
This model explains why certain drugs suit certain patients:
- ACE inhibitors and ARBs block the renin–angiotensin–aldosterone system (RAAS), lowering SVR and reducing sodium retention.
- Calcium channel blockers vasodilate arterioles, directly lowering SVR.
- Thiazides reduce plasma volume and have a mild vasodilatory effect.
- Beta-blockers reduce cardiac output and renin release — but their central effect on SVR is weaker, which is why they are no longer first-line for uncomplicated hypertension. [1]
The mechanisms in established hypertension
Three interacting systems drive sustained BP elevation: [1]
-
RAAS overactivity. Renin from the juxtaglomerular cells converts angiotensinogen to angiotensin I, then angiotensin-converting enzyme (ACE) produces angiotensin II — a potent vasoconstrictor that also stimulates aldosterone. Aldosterone causes sodium and water retention and potassium excretion. This is the rationale for ACE inhibitors, ARBs, and mineralocorticoid receptor antagonists. [1]
-
Sympathetic nervous system overactivity. Increased sympathetic tone raises heart rate, cardiac output, and vascular tone, and stimulates renin release. This is particularly important in early hypertension, obesity, and obstructive sleep apnoea. [1]
-
Sodium retention and endothelial dysfunction. Defective renal sodium excretion expands plasma volume. Damaged endothelium produces less nitric oxide (vasodilator) and more endothelin (vasoconstrictor), fixing SVR at a higher set point. [1]
Target organ damage — the reason we treat
Hypertension damages organs through mechanical stress and vascular injury: [1]
- Heart. Pressure overload causes concentric left ventricular hypertrophy (LVH). LVH is a predictor of heart failure, atrial fibrillation, and sudden death. Hypertension accelerates coronary atherosclerosis.
- Brain. Both ischaemic and haemorrhagic stroke. Small vessel disease causes lacunar infarcts, white matter changes, and vascular cognitive impairment. Hypertensive encephalopathy occurs when BP exceeds the autoregulatory ceiling of cerebral vessels.
- Kidney. Hyaline arteriolosclerosis causes nephrosclerosis — progressive proteinuria and GFR decline. Malignant hypertension causes fibrinoid necrosis and an acute nephritic picture.
- Eye. Hypertensive retinopathy ranges from arteriolar narrowing to flame haemorrhages, cotton-wool spots, papilloedema (grades III–IV), and visual loss.
- Vessels. Aortic dissection, abdominal aortic aneurysm, and peripheral arterial disease. [1]
Primary versus secondary hypertension
Primary (essential) hypertension accounts for approximately 90–95% of cases. It is a polygenic, multifactorial disorder driven by age, genetics, obesity, high salt intake, alcohol, physical inactivity, and stress. There is no single identifiable cause. [1]
Secondary hypertension accounts for 5–10%, but this proportion rises sharply in selected populations — resistant hypertension (up to 20%), hypertension under 40, and hypertension with suggestive features. Detecting a secondary cause can be curative or dramatically improve control. The key decision is when to look. [1]
When to screen for secondary hypertension
Screen when any of the following are present: [1]
- Onset under age 40 (especially without family history or obesity)
- Resistant hypertension (uncontrolled on three agents including a diuretic)
- Sudden onset or rapid acceleration, or a previously well-controlled patient whose BP is suddenly uncontrolled
- Hypertension with spontaneous or diuretic-induced hypokalaemia (primary aldosteronism)
- Episodic hypertension with headache, sweating, palpitations (phaochromocytoma)
- Abdominal or flank bruit, or unexplained CKD with hypertension (renal artery stenosis)
- Upper limb hypertension with radio-femoral delay or BP differential (coarctation)
- Snoring, obesity, daytime somnolence (obstructive sleep apnoea)
- Cushingoid features (Cushing syndrome) [1]
Secondary causes — a workup for each
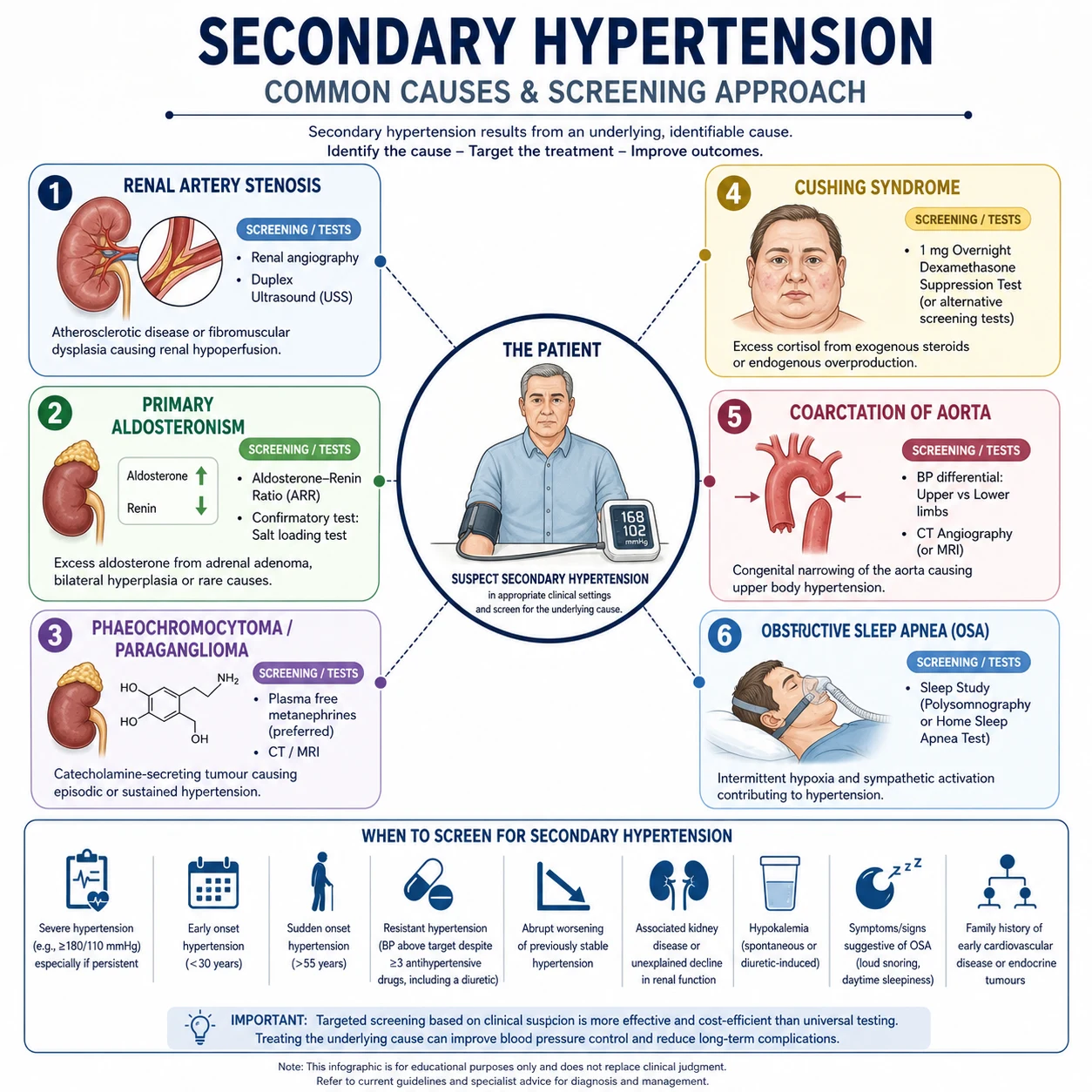
Primary aldosteronism
Primary aldosteronism (Conn syndrome) is the most common surgically curable cause of hypertension, found in 5–10% of all hypertensives and up to 20% of those with resistant hypertension. It is underdiagnosed. [1]
Mechanism. Autonomous aldosterone production (unilateral adrenal adenoma or bilateral adrenal hyperplasia) causes sodium retention, hypertension, and potassium loss. [1]
Clinical clue. Hypertension with hypokalaemia — but note that most patients with primary aldosteronism are normokalaemic, so do not wait for hypokalaemia to screen. [1]
Screening test — the aldosterone-to-renin ratio (ARR). A raised ARR (high aldosterone, suppressed renin) suggests autonomous aldosterone production. Ideally measure in the morning, seated, correcting hypokalaemia first. Withdraw spironolactone and eplerenone for at least 4 weeks (they raise renin and falsely lower the ratio). ACE inhibitors, ARBs, and diuretics can affect the ratio — interpret results in context. A screening ARR above the laboratory cut-off (commonly aldosterone/renin ratio with aldosterone elevated) requires confirmatory suppression testing (oral sodium loading, saline infusion, fludrocortisone suppression, or captopril challenge) per the Endocrine Society guideline (PMID 26934393) before proceeding. [1]
Subtype differentiation. Adrenal CT first, then adrenal venous sampling (AVS) to confirm lateralisation before adrenalectomy. Unilateral disease is treated with laparoscopic adrenalectomy; bilateral disease with mineralocorticoid receptor antagonist (spironolactone or eplerenone). [1]
Renal artery stenosis
Two mechanisms: atherosclerotic (90%, older patients with vascular disease) and fibromuscular dysplasia (10%, younger women). [1]
Clinical clues. New-onset hypertension over age 55 or under 30; abdominal or flank bruit; abrupt rise in creatinine after starting an ACE inhibitor; refractory hypertension; flash pulmonary oedema in the setting of bilateral disease. [1]
Investigation. Renal artery Doppler ultrasound (non-invasive, measures peak systolic velocity), CT angiography, or MR angiography. Digital subtraction angiography is the gold standard but invasive. [1]
Management. Medical therapy with a RAAS blocker (ACE inhibitor or ARB) is first-line — these patients actually benefit most from RAAS blockade of the ischaemic renin–angiotensin axis, but creatinine must be monitored closely (an early rise up to 30% is acceptable). Routine renal artery stenting does not improve outcomes over medical therapy alone — the CORAL trial (PMID 24245566) showed no benefit of stenting over medical therapy for atherosclerotic renal artery stenosis. Reserve stenting for resistant hypertension, refractory flash pulmonary oedema, or rapidly declining renal function. [1]
Phaeochromocytoma
Clinical clue. The classic triad is episodic headache, sweating, and palpitations — often with marked BP lability. However, many patients have sustained hypertension. There may be orthostatic hypotension, weight loss, anxiety, or paroxysmal crises precipitated by anaesthesia, certain drugs, or abdominal palpation. [1]
Investigation. Plasma free metanephrines (or 24-hour urine fractionated metanephrines) are the most sensitive screening tests — metanephrines are the stable, continuous metabolites of catecholamines, produced constitutively within the tumour rather than only during paroxysms. A clearly negative result excludes phaeochromocytoma. Localise with CT or MRI, then functional imaging (MIBG or DOTATATE PET) to confirm and detect metastases. [1]
Management. Surgical resection after alpha-blockade first (phenoxybenzamine, then add a beta-blocker — never beta-blockade first, as unopposed alpha stimulation precipitates hypertensive crisis). The rule: alpha before beta. [1]
Cushing syndrome
Clinical clues. Cushingoid habitus (central obesity, moon face, buffalo hump), proximal myopathy, easy bruising, purple striae, glucose intolerance, osteoporosis. [1]
Investigation. Late-night salivary cortisol, 24-hour urine free cortisol, or 1 mg overnight dexamethasone suppression test. If confirmed, localise with pituitary MRI (Cushing disease) or adrenal CT. [1]
Coarctation of the aorta
Clinical clue. Upper body hypertension with radio-femoral delay, weak or delayed femoral pulses, BP differential between arms and legs, interscapular bruit. May present in adults with refractory hypertension or as an incidental finding. [1]
Investigation. Echocardiography, CT or MR angiography of the aorta. Refer for cardiology — surgical or endovascular repair. [1]
Obstructive sleep apnoea (OSA)
OSA is the commonest secondary cause in resistant hypertension — present in up to 70% of resistant hypertensives. Mechanism: intermittent hypoxia drives sympathetic surges and RAAS activation. [1]
Clinical clue. Obesity, loud snoring, witnessed apnoeas, daytime somnolence, large neck circumference. Many patients have resistant hypertension and a non-dipping nocturnal BP pattern on ABPM. [1]
Investigation. Polysomnography or home sleep study. Treatment with CPAP lowers BP modestly (3–5 mmHg) but improves symptoms and may reduce cardiovascular events. [1]
Assessment of target organ damage
Every new hypertensive patient requires a target organ damage (TOD) assessment. The presence and extent of TOD changes both the risk calculation and the urgency of treatment. [1]
| Organ | Investigation | What you are looking for |
|---|---|---|
| Heart | ECG | LVH (Sokolow-Lyon or Cornell voltage criteria), strain pattern, arrhythmia |
| Heart | Echocardiogram (if LVH suspected or in high risk) | Left ventricular hypertrophy, diastolic dysfunction, LV mass |
| Kidney | U&E, eGFR | CKD, baseline renal function before RAAS blockade |
| Kidney | Urine albumin-to-creatinine ratio | Microalbuminuria — an early marker of vascular damage |
| Eye | Fundoscopy | Hypertensive retinopathy (narrowing, AV nipping, haemorrhages, cotton-wool spots, papilloedema) |
| Vessels | Pulse examination, ABI if symptomatic | Peripheral arterial disease, radio-femoral delay |
| Metabolic | Fasting lipid, glucose/HbA1c | Concomitant risk factors |
| Other | FBE, TSH, LFTs | Baseline and screen for secondary causes |
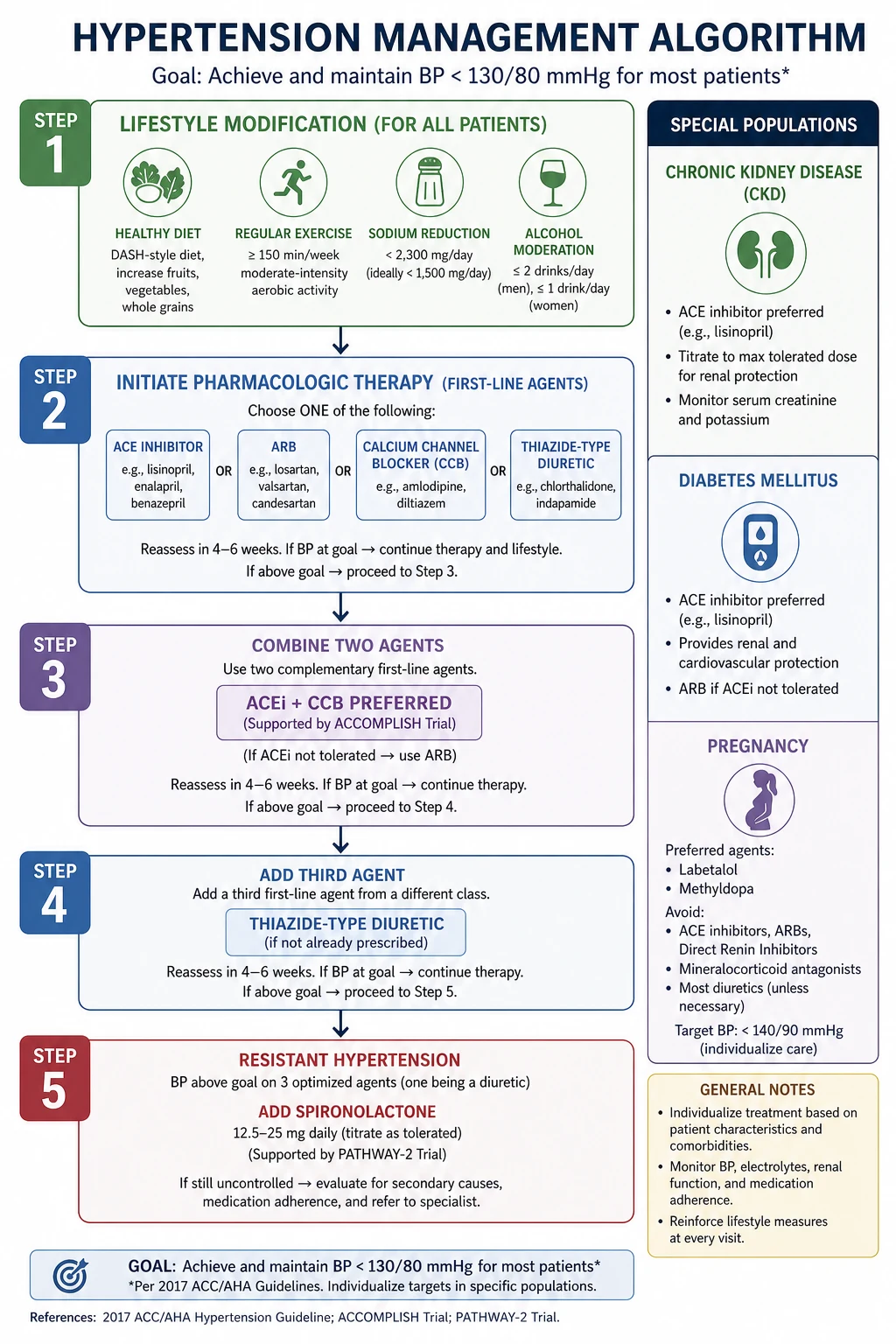
Lifestyle modification
Always offer lifestyle modification — it is the foundation, and for some motivated patients with grade 1 hypertension and low cardiovascular risk, it may suffice. It also enhances the effect of drug therapy. Quantify the expected benefit so you and the patient have realistic expectations. [1]
| Modification | Recommendation | Approximate systolic BP reduction |
|---|---|---|
| Weight reduction | Aim for BMI under 25; each 1 kg lost lowers BP | ~1 mmHg per kg |
| DASH diet | Fruit, vegetables, low-fat dairy, reduced saturated fat | 8–14 mmHg |
| Sodium restriction | under 5 g sodium/day (under 2 g) | 4–5 mmHg |
| Alcohol moderation | under 2 standard drinks/day (men), under 1 (women) | 2–4 mmHg |
| Smoking cessation | No direct BP effect, but reduces total CV risk | — |
These effects are additive. A patient who loses weight, restricts salt, and exercises can achieve reductions equivalent to a single antihypertensive agent. Set expectations honestly: lifestyle alone rarely controls grade 2–3 hypertension, but it should accompany every drug regimen. [1]
Pharmacological management
The four first-line classes
For uncomplicated hypertension, four drug classes are first-line: ACE inhibitor, ARB, calcium channel blocker, and thiazide/thiazide-like diuretic. All are broadly equivalent for initial BP lowering; the choice is driven by comorbidity, age, ethnicity, and side-effect profile. [1]
ACE inhibitors (e.g. perindopril, ramipril, enalapril). Block conversion of angiotensin I to angiotensin II, lowering SVR and aldosterone. First-line in diabetes with albuminuria, CKD, heart failure, and post-myocardial infarction. Side effects: dry cough (bradykinin accumulation, 10–20%), hyperkalaemia, acute kidney injury, angioedema (higher in Black and Asian populations). Contraindicated in pregnancy and bilateral renal artery stenosis. Never combine an ACE inhibitor with an ARB. [1]
Angiotensin receptor blockers (e.g. valsartan, telmisartan, candesartan). Block the angiotensin II type 1 receptor directly. Used when an ACE inhibitor is not tolerated (especially cough). Same renoprotective role in diabetes and CKD. Side effects: hyperkalaemia and AKI, but no cough and lower angioedema risk. Contraindicated in pregnancy. [1]
Calcium channel blockers. Two subtypes with distinct use:
- Dihydropyridines (amlodipine, nifedipine, felodipine) act on arterioles, causing vasodilation. Effective, especially in older patients and isolated systolic hypertension, and in Black patients. Side effects: ankle oedema (capillary leak, dose-dependent and not responsive to diuretics), flushing, headache, reflex tachycardia.
- Non-dihydropyridines (diltiazem, verapamil) reduce heart rate and contractility. Useful in angina or rate control. Side effects: bradycardia, constipation (verapamil). Do not combine with a beta-blocker (risk of severe bradycardia and heart block). [1]
Thiazide and thiazide-like diuretics (chlorthalidone, hydrochlorothiazide, indapamide). Reduce plasma volume initially, then SVR with chronic use. The ALLHAT trial (PMID 12479763) established the thiazide-type diuretic chlorthalidone as at least as effective as ACE inhibitors and CCBs for cardiovascular outcomes in high-risk patients. Particularly effective in older patients, Black patients, and those with heart failure. Side effects: hypokalaemia, hyponatraemia, hyperuricaemia (gout), hyperglycaemia, hypercalcaemia, erectile dysfunction. Indapamide has a weaker effect on potassium and glucose. [1]
Beta-blockers — not first-line for uncomplicated hypertension
Beta-blockers (e.g. metoprolol, bisoprolol, atenolol) are less effective than first-line agents at reducing stroke in uncomplicated hypertension, and they carry metabolic side effects (weight gain, insulin resistance). First-line indications are comorbid: heart failure with reduced ejection fraction, post-myocardial infarction, angina, atrial fibrillation rate control, and young patients with sympathetic overactivity or intolerance of other classes. They remain useful as add-on therapy. Do not stop beta-blockers abruptly in patients with ischaemic heart disease (rebound hypertension and ischaemia). [1]
Combinations — what to combine and what to avoid
Most patients need two or more agents. The evidence favours starting combination therapy early (or as initial therapy) in grade 2 or higher hypertension. [1]
Preferred dual combination — ACE inhibitor (or ARB) + CCB. The ACCOMPLISH trial (PMID 19052124) showed that benazepril plus amlodipine was superior to benazepril plus hydrochlorothiazide for cardiovascular events in high-risk hypertensives (hazard ratio 0.80), despite equivalent BP control. This is now the preferred initial combination. [1]
Alternative dual combination — ACE inhibitor/ARB + thiazide. Synergistic (the RAAS activation from diuresis is blocked by the ACE inhibitor). Good in older patients and those with volume overload. [1]
Combinations to avoid:
- ACE inhibitor + ARB — no added BP benefit, increased AKI and hyperkalaemia. Contraindicated.
- ACE inhibitor/ARB + potassium-sparing diuretic/MRA — acceptable in heart failure, but requires close potassium monitoring in general hypertension.
- Dihydropyridine + non-dihydropyridine CCB — excessive bradycardia and heart block.
- Beta-blocker + verapamil/diltiazem — severe bradycardia and heart block. [1]
ANZ dosing reference (adults, oral)
| Drug | Starting dose | Usual max | Note |
|---|---|---|---|
| Perindopril (arginine) | 5 mg OD | 10 mg OD | Renoprotective |
| Valsartan | 80 mg OD | 320 mg OD | ARB |
| Amlodipine | 5 mg OD | 10 mg OD | Oedema dose-dependent |
| Chlorthalidone | 12.5 mg OD | 25 mg OD | Thiazide-like, potent |
| Indapamide modified-release | 1.5 mg OD | 1.5 mg OD | Weak K+/glucose effect |
| Spironolactone | 25 mg OD | 50 mg OD | Resistant HTN; gynaecomastia |
| Bisoprolol | 5 mg OD | 10 mg OD | Beta-blocker |
Blood pressure targets
The SPRINT trial (PMID 26551272) randomised high-risk, non-diabetic patients to an intensive target (systolic under 120 mmHg) versus standard (under 140). The intensive arm showed a 25% relative reduction in the composite of MI, stroke, heart failure, and CV death, and a 27% reduction in all-cause mortality — at the cost of more hypotension, syncope, electrolyte disorders, and AKI. This single trial shifted guidelines globally. [1]
Practical targets (ANZ/ESC-leaning): [1]
| Population | Office systolic/diastolic target |
|---|---|
| General adult (under 65) | under 130/80 mmHg (ESH 2023) |
| Older (65–79) | under 140/80, then to 130 if tolerated |
| Frail elderly / very elderly (over 80) | under 150, then to 140 if tolerated |
| Diabetes | under 130/80 |
| CKD (with albuminuria) | under 130/80 |
| Post-stroke | under 130/80 |
| Pregnancy | under 140/90 |
The guiding principle: lower is better, provided it is tolerated. In the elderly and frail, the risk of orthostatic hypotension, falls, and AKI tempers the target — titrate gradually, check standing BP, and accept a less aggressive number if the patient cannot tolerate the lower target. [1]
Resistant hypertension
Definition
Resistant hypertension is BP that remains above target despite adherence to three antihypertensive drugs at maximal or best-tolerated doses, including a diuretic, or BP controlled only with four or more agents. The 'including a diuretic' clause is essential — without a diuretic, apparent resistance is often volume overload. [1]
Before you label it resistant, exclude the mimics
Over half of apparent resistant hypertension is pseudo-resistance:
- White-coat effect — confirm with ABPM or HBPM. This is the single most common cause.
- Non-adherence — the leading true cause of apparent resistance. Use a non-judgemental approach; consider urine drug screening for antihypertensives where available.
- Suboptimal regimen — no diuretic, or diuretic too low-dose; inappropriate combinations.
- Lifestyle factors — high salt intake, excess alcohol, NSAIDs, sympathomimetics, herbal supplements (liquorice), recreational drugs.
- Undiagnosed secondary cause — especially OSA and primary aldosteronism. [1]
The evidence-based fourth agent
If resistance is confirmed (true resistant hypertension), add spironolactone 25–50 mg daily. The PATHWAY-2 trial (PMID 26414968) — a double-blind, placebo-controlled, crossover trial of 314 resistant hypertensives on three agents — showed spironolactone was the most effective fourth-line agent, superior to placebo, bisoprolol, and doxazosin. The mechanism reflects the underlying pathophysiology: resistant hypertension is frequently driven by aldosterone-mediated sodium retention. [1]
Monitor potassium and renal function at 1–2 weeks, then monthly. Watch for gynaecomastia (spironolactone — switch to eplerenone if symptomatic) and hyperkalaemia (worse with CKD). If spironolactone is not tolerated or contraindicated, a beta-blocker (bisoprolol) or alpha-blocker (doxazosin) are second-line fourth agents. Referral to a hypertension specialist for refractory cases or suspected secondary causes is appropriate. [1]
Hypertensive emergency versus urgency
This distinction governs everything: where the patient is managed, how fast the BP comes down, and which drugs are used. [1]
Hypertensive emergency
A hypertensive emergency is severe BP elevation (typically systolic over 180 or diastolic over 120) with acute or worsening target organ damage. This is a medical emergency requiring admission to a monitored bed (ICU/HDU) and intravenous therapy. [1]
Examples:
- Hypertensive encephalopathy (headache, confusion, visual disturbance, seizures, papilloedema)
- Acute stroke (ischaemic or haemorrhagic) — treat per stroke-specific protocols; do not lower BP precipitously in ischaemic stroke
- Acute coronary syndrome
- Acute pulmonary oedema
- Aortic dissection
- Acute kidney injury with malignant hypertension (fibrinoid necrosis, microangiopathic haemolysis)
- Eclampsia / severe pre-eclampsia [1]
Goal of therapy. Lower BP gradually — by no more than 25% in the first hour, then toward 160/100 over 2–6 hours, then gradually to target over 24–48 hours. Rapid reduction risks hypoperfusion of organs that have autoregulated to chronic hypertension (brain, heart, kidneys). The exceptions are aortic dissection (rapid reduction to systolic under 120 over 15–30 minutes after pain control) and acute pulmonary oedema (rapid preload and afterload reduction). [1]
Hypertensive urgency
A hypertensive urgency is severe BP elevation without acute target organ damage — the patient has a high number but is asymptomatic and has no evidence of acute end-organ injury. This does not require IV therapy or admission. Manage by adjusting or adding oral agents, with close outpatient follow-up within 24–72 hours. Avoid rapid oral loading (e.g. short-acting nifedipine), which causes precipitous, uncontrolled BP drops and ischaemic events. [1]
Intravenous agents for hypertensive emergency
| Agent | Onset | Indication | Cautions |
|---|---|---|---|
| Labetalol (alpha+beta blocker) | 5–10 min | Most emergencies; safe in pregnancy/pre-eclampsia | Bradycardia, heart block, HF |
| Nicardipine (DHP CCB infusion) | 5–15 min | Most emergencies; stroke, pre-eclampsia | Reflex tachycardia; costly |
| Sodium nitroprusside (arterial+venous vasodilator) | seconds | Hypertensive encephalopathy, dissection (with beta-blocker) | Cyanide toxicity with prolonged use; raise ICP |
| Esmolol (ultra-short beta-blocker) | seconds | Aortic dissection (with nitroprusside), perioperative | Bradycardia, HF, asthma |
| Glyceryl trinitrate (venous > arterial vasodilator) | 2–5 min | Acute coronary syndrome, pulmonary oedema | Headache, tachyphylaxis; weak antihypertensive |
First-line for most emergencies: labetalol or nicardipine infusion, titrated. Both are safe, titratable, and widely used in ANZ/UK practice. Sodium nitroprusside is potent but reserved for the most severe cases (dissection, fulminant encephalopathy) due to cyanide/thiocyanate toxicity with infusions beyond 24–48 hours. In aortic dissection, the principle is beta-blockade first to control heart rate and shear stress, then vasodilation — give labetalol or esmolol, then add nitroprusside if needed. [1]
Hypertension in pregnancy
Pregnancy hypertension has its own classification, physiology, and pharmacology — and ACE inhibitors and ARBs are absolutely contraindicated (fetopathy). [1]
Classification:
- Chronic hypertension — present before pregnancy or before 20 weeks gestation.
- Gestational hypertension — new hypertension after 20 weeks without proteinuria or end-organ dysfunction.
- Pre-eclampsia — new hypertension after 20 weeks with proteinuria or end-organ dysfunction (renal, hepatic, neurological, haematological). A multisystem disorder of placental origin.
- Chronic hypertension with superimposed pre-eclampsia. [1]
Treatment targets. Treat chronic and gestational hypertension to a target of 135–150/85–100 (aiming under 140/90). In pre-eclampsia, the aim is under 160/110 to prevent stroke. [1]
Safe first-line agents in pregnancy:
- Labetalol — first-line (combined alpha/beta-blocker).
- Methyldopa — safe, long history, but sedating and not used postpartum.
- Nifedipine (modified-release) — second-line CCB. [1]
Contraindicated: ACE inhibitors, ARBs, direct renin inhibitors, and nitroprusside. Diuretics are used cautiously (pre-eclampsia is a low-volume state). [1]
For severe hypertension in pregnancy (BP at or above 160/110), give IV labetalol or hydralazine, and magnesium sulphate for seizure prophylaxis in pre-eclampsia/eclampsia. The definitive treatment of pre-eclampsia is delivery — timed by gestational age and maternal–fetal status. [1]
Hypertension in CKD and diabetes
These comorbidities change both the drug choice and the target. [1]
In CKD, an ACE inhibitor or ARB is first-line, especially with albuminuria — the intraglomerular pressure reduction is renoprotective. Monitor creatinine and potassium within 1–2 weeks of initiation or dose change. A creatinine rise up to 30% is acceptable; a larger rise prompts investigation (volume depletion, NSAID use, renal artery stenosis). The combination of ACE inhibitor/ARB with diuretic and NSAID ('triple whammy') causes a high rate of AKI — counsel patients accordingly. Target is under 130/80 with albuminuria; under 140/90 without albuminuria. [1]
In diabetes, an ACE inhibitor or ARB is preferred when there is albuminuria or CKD, for renal protection independent of the BP effect. Target is under 130/80. The SGLT2 inhibitor class provides additional BP lowering (3–5 mmHg) and renoprotection, and is now standard in diabetic kidney disease. Avoid beta-blockers masking hypoglycaemia symptoms, and thiazide-induced hyperglycaemia. [1]
Follow-up and surveillance
- Review within 4–6 weeks of starting or changing therapy — check BP, renal function, electrolytes, and side effects.
- Once at target, review every 6–12 months. Check annual renal function, electrolytes, lipids, glucose, and re-assess TOD (ECG; urine ACR if indicated).
- Re-measure home or ambulatory BP periodically to confirm control and detect masked hypertension.
- Reinforce adherence and lifestyle at every visit — the single biggest reason for 'failure' is non-adherence. [1]
Common exam traps
- Conflating ACC/AHA (130/80) with ESC/ESH/NHFA (140/90) thresholds. State which guideline you are quoting.
- Combining an ACE inhibitor with an ARB. Never — it increases AKI and hyperkalaemia with no BP benefit.
- Missing primary aldosteronism. It is the commonest curable secondary cause, and most patients are normokalaemic. Screen with ARR in resistant hypertension and hypokalaemia.
- Treating resistant hypertension with more agents before adding spironolactone. PATHWAY-2 showed spironolactone is the most effective fourth agent.
- Rapidly lowering BP in hypertensive emergency. Autoregulation is shifted right — aim for no more than 25% reduction in the first hour to avoid hypoperfusion (brain, heart, kidney).
- Forgetting to check a standing BP in older patients. Orthostatic hypotension is common and dangerous; titrate gradually.
- Stopping an ACE inhibitor/ARB for a modest creatinine rise. Up to 30% rise is acceptable and expected; stopping denies the patient renoprotection.
- Using ACE inhibitors or ARBs in pregnancy. Absolutely contraindicated — fetal renal malformation and death.
- Beta-blockade before alpha-blockade in phaeochromocytoma. Unopposed alpha stimulation precipitates hypertensive crisis. Always alpha before beta.
- Renal artery stenting for routine atherosclerotic stenosis. CORAL showed no benefit over medical therapy — reserve stenting for selected cases. [1]
References
- [1]Wright JT Jr, Williamson JD, Whelton PK, et al. (SPRINT Research Group) A Randomized Trial of Intensive versus Standard Blood-Pressure Control N Engl J Med, 2015.PMID 26551272
- [2]Jamerson K, Weber MA, Bakris GL, et al. (ACCOMPLISH Trial Investigators) Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients N Engl J Med, 2008.PMID 19052124
- [3]Williams B, MacDonald TM, Morant S, et al. (British Hypertension Society's PATHWAY Studies Group) Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial Lancet, 2015.PMID 26414968
- [4]Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines Hypertension, 2018.PMID 29133354
- [5]Mancia G, Kreutz R, Brunström M, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA) J Hypertens, 2023.PMID 37345492
- [6]Funder JW, Carey RM, Mantero F, et al. The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline J Clin Endocrinol Metab, 2016.PMID 26934393
- [7]ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) JAMA, 2002.PMID 12479763
- [8]Cooper CJ, Murphy TP, Cutlip DE, et al. (CORAL Investigators) Stenting and medical therapy for atherosclerotic renal-artery stenosis N Engl J Med, 2014.PMID 24245566