Phys · cardiovascular
Infective Endocarditis
Also known as IE · bacterial endocarditis · subacute bacterial endocarditis · SBE · acute bacterial endocarditis · native valve endocarditis · prosthetic valve endocarditis · right-sided endocarditis · culture-negative endocarditis
Consultant-physician-depth guide to infective endocarditis — pathogenesis, Modified Duke criteria, microbiology, antibiotic therapy (native vs prosthetic valve), surgical indications, prophylaxis, and complications — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Infective Endocarditis
Opening statement
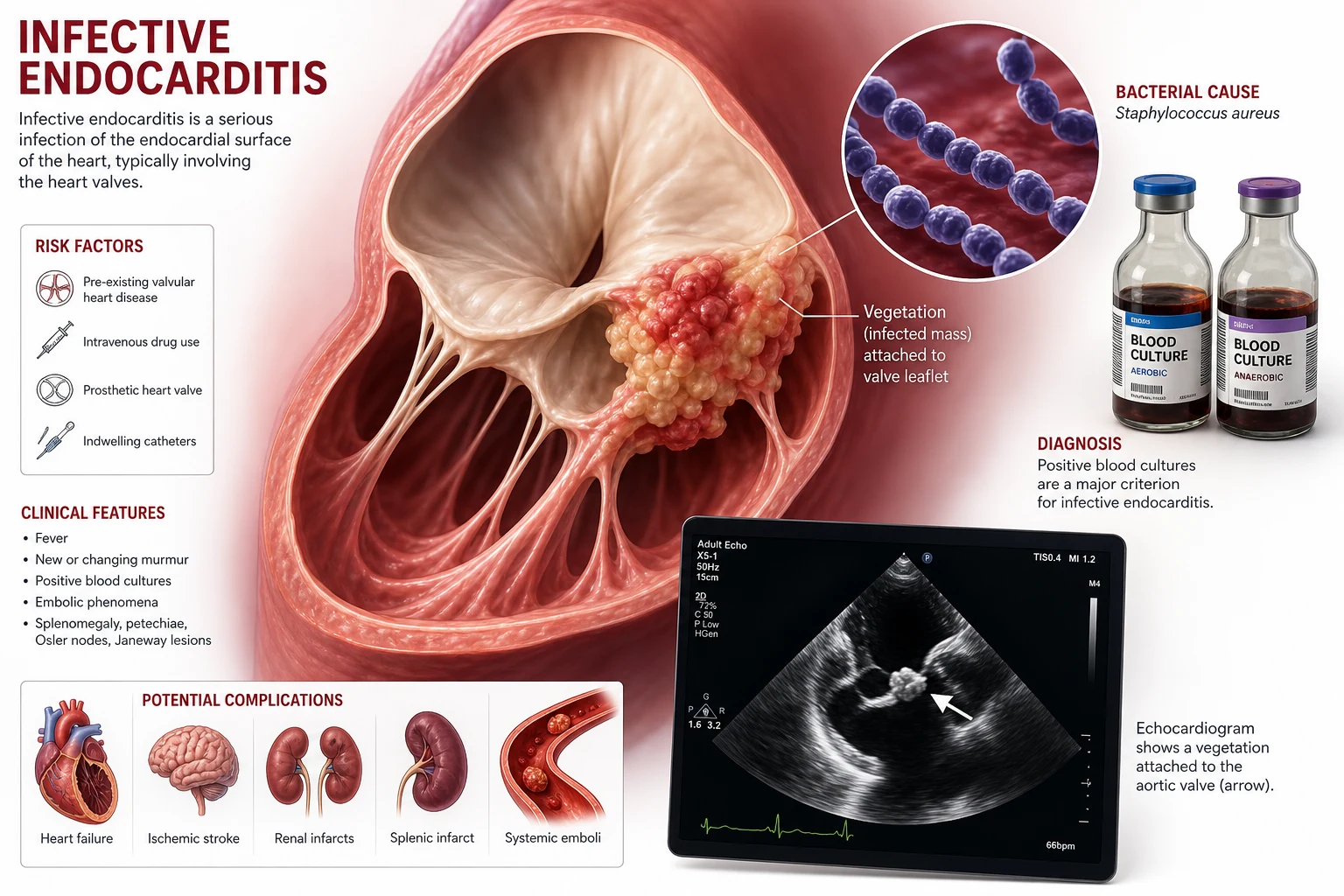
Infective endocarditis (IE) is microbial infection of the endocardial surface of the heart — most commonly a heart valve, but also septal defects, mural endocardium, or prosthetic material. It is a condition where every decision is time-critical: missing it kills the valve and the patient; over-diagnosing it commits the patient to four to six weeks of intravenous antibiotics and a lifetime of prosthetic valve surveillance. The registrar's job at 3 a.m. is not to make the diagnosis alone — it is to draw cultures, image the valve, start the right empiric regimen, and call the Endocarditis Team early. [1]
Three examiner facts anchor every IE question. First, the Modified Duke criteria are a diagnostic framework, not a checklist to be applied blindly — a single positive blood culture for Staphylococcus aureus is itself a major criterion. Second, heart failure is the single strongest indication for surgery, more than any microbiological or embolic consideration. Third, antibiotic prophylaxis is now restricted to a narrow high-risk group undergoing dental procedures — most patients previously given prophylaxis no longer need it. [1]
Pathophysiology — why this disease exists and why it matters clinically
The four-step pathogenesis
IE develops through a predictable sequence. Understanding it tells you who is at risk and why certain organisms dominate. [1]
Step 1 — Endothelial damage with non-bacterial thrombotic vegetation (NBTV). Normal cardiac endothelium is resistant to bacterial colonisation. Damage — from turbulent high-velocity jets (regurgitant valve, VSD, patent ductus), prosthetic material, or indwelling catheters — exposes subendothelial collagen and tissue factor. Platelets and fibrin deposit, forming a sterile vegetation. This NBTV is the foothold. Conditions producing low-flow or low-pressure areas (large atrial septal defect, chronic atrial fibrillation with smooth endothelium) rarely cause IE — turbulence is the key. [1]
Step 2 — Transient bacteraemia. Bacteria enter the bloodstream from mucosal surfaces, skin, or infected hardware. The everyday events — toothbrushing, chewing, dental scaling, IV cannulation, catheter manipulation — produce low-grade bacteraemia far more often than the dramatic events (dental extraction, surgery) we have historically blamed. This is why prophylaxis targeting only invasive procedures has limited population impact. [1]
Step 3 — Microbial adherence and multiplication. Organisms that cause IE possess specific virulence factors enabling them to adhere to the NBTV. Viridans streptococci produce dextran (a polysaccharide) that binds to fibrin-platelet clots — which is why oral streptococci dominate after dental procedures. Staphylococcus aureus expresses microbial surface components recognising adhesive matrix molecules (MSCRAMMs) — fibronectin-binding proteins A and B, clumping factors A and B — that mediate direct endothelial and vegetation adherence even without pre-existing NBTV. This explains why S. aureus can seed a previously normal valve and why its IE is more acute and destructive. [1]
Step 4 — Vegetation growth and dissemination. Once established, bacteria multiply within the avascular vegetation, protected from phagocytes and (partly) from antibiotics. Fragments of the friable vegetation embolise systemically (left-sided — brain, spleen, kidney, limb; right-sided — pulmonary). Sustained bacteraemia drives immune-complex formation (glomerulonephritis, Osler nodes, Roth spots) and chronic inflammation. [1]
Why this matters clinically
The pathogenesis tells you four things you will use at the bedside. Turbulence determines risk — so look for the regurgitant valve, the prosthetic material, the residual VSD. Adherence explains the organism — oral source gives viridans strep, healthcare exposure gives S. aureus, genitourinary manipulation gives enterococci. Avascularity of the vegetation explains why high-dose, bactericidal, prolonged therapy is required — the antibiotic must penetrate the clot. And immune-complex disease explains the peripheral stigmata — they are not embolic, they are immunological. [1]
Modified Duke criteria — the diagnostic framework
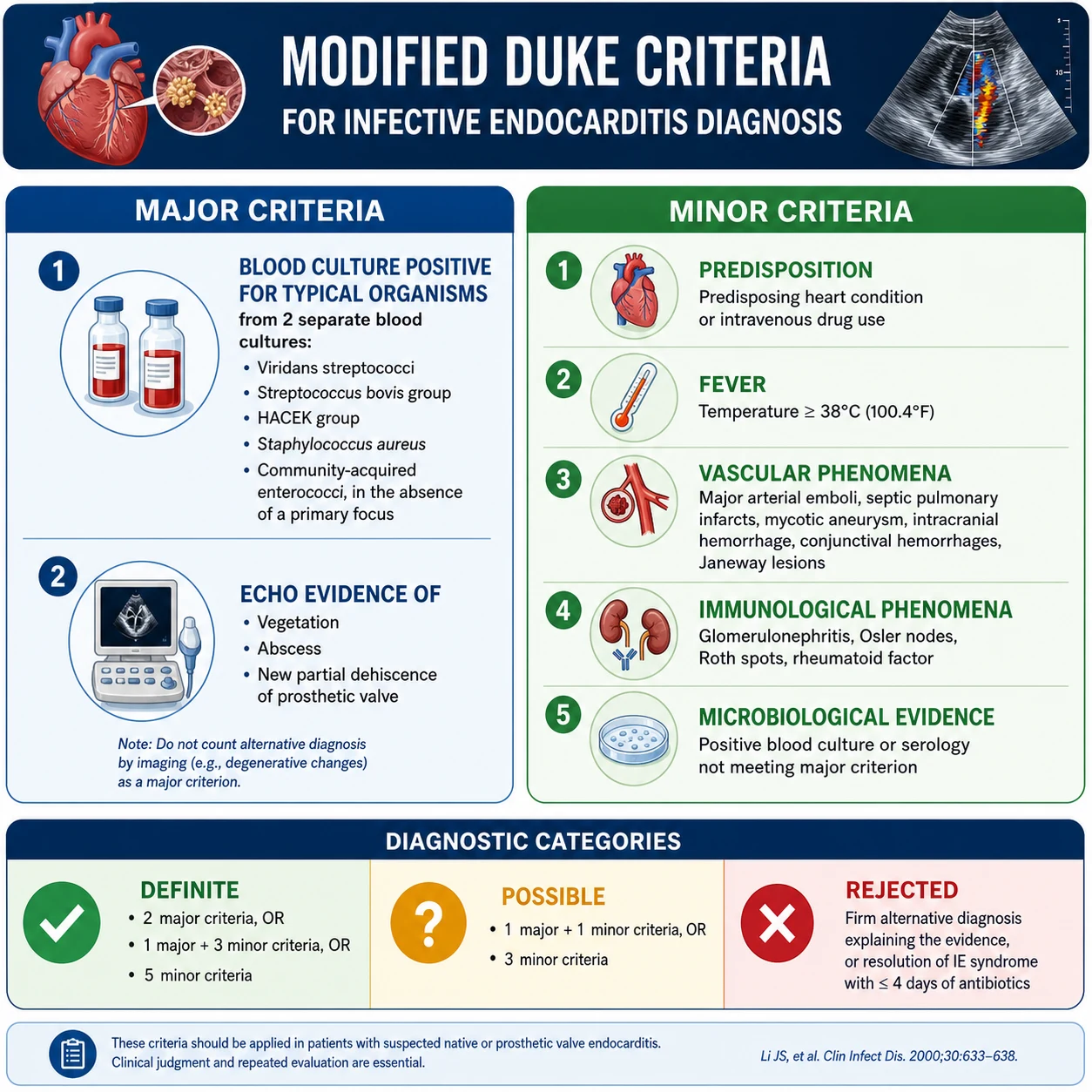
The Modified Duke criteria (Li et al, 2000) are the standard diagnostic framework. They are a probabilistic tool, not absolute — a patient may meet "possible" criteria and still need empiric therapy, or meet "definite" criteria and have an alternative diagnosis. The criteria are applied at presentation and serially as results return. [1]
Major criteria
Major criterion 1 — Positive blood cultures for typical organisms, from two separate sites:
- Viridans streptococci, Streptococcus gallolyticus (formerly S. bovis), HACEK group, or S. aureus
- OR community-acquired enterococci (in the absence of a primary focus) [1]
Major criterion 1b — Persistently positive blood cultures:
- At least two positive cultures drawn more than 12 hours apart, OR
- Three of three, or a majority of four or more separate cultures, with the first and last drawn at least one hour apart [1]
Major criterion 1c — Single positive culture for Coxiella burnetii OR anti-phase I IgG titre greater than 1:800. Coxiella (Q fever) is the classic culture-negative organism — it requires serology, not culture. [1]
Major criterion 2 — Evidence of endocardial involvement:
- Echocardiogram positive for IE: oscillating intracardiac mass on valve or supporting structures; OR abscess; OR new partial dehiscence of prosthetic valve
- OR new valvular regurgitation (an increase or change in a pre-existing murmur is not sufficient — it must be new regurgitation) [1]
Minor criteria
- Predisposition — predisposing heart condition (prosthetic valve, previous IE, congenital or acquired valve disease, hypertrophic cardiomyopathy) OR intravenous drug use
- Fever — temperature greater than 38°C
- Vascular phenomena — arterial embolus, septic pulmonary infarcts, mycotic aneurysm, intracranial haemorrhage, conjunctival haemorrhages, Janeway lesions
- Immunological phenomena — glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor
- Microbiological evidence — positive blood culture not meeting a major criterion, OR serological evidence of active infection with an organism consistent with IE [1]
Classification
- Definite IE — 2 major, OR 1 major + 3 minor, OR 5 minor
- Possible IE — 1 major + 1 minor, OR 3 minor
- Rejected — firm alternative diagnosis, OR resolution with less than 4 days of antibiotics, OR no pathologic evidence at surgery or autopsy, OR does not meet "possible" criteria [1]
The high-yield traps in the Duke criteria
Three traps repeat in exams. First, a single positive blood culture for S. aureus — regardless of whether a primary focus is identified, and regardless of nosocomial or community acquisition — is a major criterion, not a minor one. This was a key 2000 modification. Second, the old minor criterion "echocardiogram consistent with IE but not meeting major criterion" was eliminated — echo findings are now either major or absent. Third, Coxiella serology is a major criterion — a patient with Q fever serology and a murmur is one step from definite IE. [1]
Microbiology — know the organism, know the source
The organism predicts the source, the source guides the empiric regimen, and both inform surgical risk. The ICE-PCS cohort (Fowler et al, 2005) established S. aureus (31%) as the most common cause of IE globally, followed by viridans streptococci and enterococci. [1]
Native valve endocarditis
| Organism | Approximate frequency | Source / context | Key features |
|---|---|---|---|
| Staphylococcus aureus | 30-35% | Healthcare-associated, IVDU, skin | Acute presentation, destructive, metastatic infection |
| Viridans streptococci | 20-25% | Oropharyngeal, dental | Subacute, penicillin-sensitive, good prognosis |
| Streptococcus gallolyticus | 10% | Gastrointestinal — associated with colonic polyps and malignancy | Investigate the colon in every case |
| Enterococci (E. faecalis, E. faecium) | 10% | Genitourinary, biliary, elderly men | Often penicillin-resistant; combination therapy |
| Coagulase-negative staphylococci | 5% | Native valve — less common; prosthetic valve — common | Usually S. epidermidis |
| HACEK group | 2% (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella) | Oropharyngeal | Fastidious, slow-growing, large vegetations |
| Fungi (Candida, Aspergillus) | Less than 2% | Immunocompromised, IVDU, prolonged lines | Large friable vegetations, embolic, surgical mandatory |
| Polymicrobial | 5% | IVDU | Suggests right-sided source |
Culture-negative endocarditis
Culture-negative IE accounts for 5-10% of cases. The differential has two limbs: organisms that require special media or serology (the "true" culture-negatives), and antibiotic-pretreated cultures (the most common cause). Always ask about recent antibiotics first. [1]
The culture-negative organisms to know by name: [1]
| Organism | Why it is culture-negative | How to diagnose |
|---|---|---|
| Coxiella burnetii (Q fever) | Obligate intracellular | Serology — anti-phase I IgG greater than 1:800 is a Duke major criterion |
| Bartonella spp. (B. henselae, B. quintana) | Fastidious, slow | Serology, PCR of valve tissue |
| Brucella | Fastidious, slow, needs enriched media | Serology, blood cultures held 21 days |
| Legionella | Needs buffered charcoal yeast extract | Serology, urinary antigen, PCR |
| Tropheryma whipplei | Very fastidious | PCR of valve tissue, PAS-positive macrophages |
| Mycoplasma / Ureaplasma | Cell-wall deficient | Serology, PCR |
| Fungi (Candida, Aspergillus) | May grow slowly or not at all | Blood cultures often negative; serology, valve histopathology |
The clinical clue to Coxiella endocarditis (the highest-yield culture-negative organism for exams): a patient with a prosthetic valve, culture-negative bloods, and exposure to farm animals, unpasteurised milk, or parturient cats. The clue to Bartonella: homelessness, body louse infestation, alcohol use disorder, or HIV. The clue to S. gallolyticus: investigate the colon — there is a 25-60% association with colorectal neoplasia. [1]
Prosthetic valve endocarditis
Prosthetic valve endocarditis (PVE) is classified by timing since surgery: early (less than 1 year) and late (greater than 1 year). Early PVE is dominated by coagulase-negative staphylococci (from perioperative contamination) and S. aureus. Late PVE mirrors native valve microbiology, with oral streptococci and enterococci prominent. PVE carries higher mortality and higher rates of paravalvular abscess, dehiscence, and conduction block — the bar for surgery is lower. [1]
Clinical features — what to look for and what it means
IE presents across a spectrum from acute fulminant (days) to subacute indolent (weeks to months). The classic triad of fever, murmur, and embolic or immune phenomena is the teaching anchor, but atypical presentations are common — especially in the elderly, the immunosuppressed, and PVE. [1]
Cardinal clinical features
Fever is present in 90% but may be absent in the elderly, immunosuppressed, or those already on antibiotics. A new murmur or a change in an existing murmur is present in 80-85% of left-sided IE; right-sided IE (tricuspid, often in IVDU) may have no audible murmur because the gradient across the tricuspid valve is low. [1]
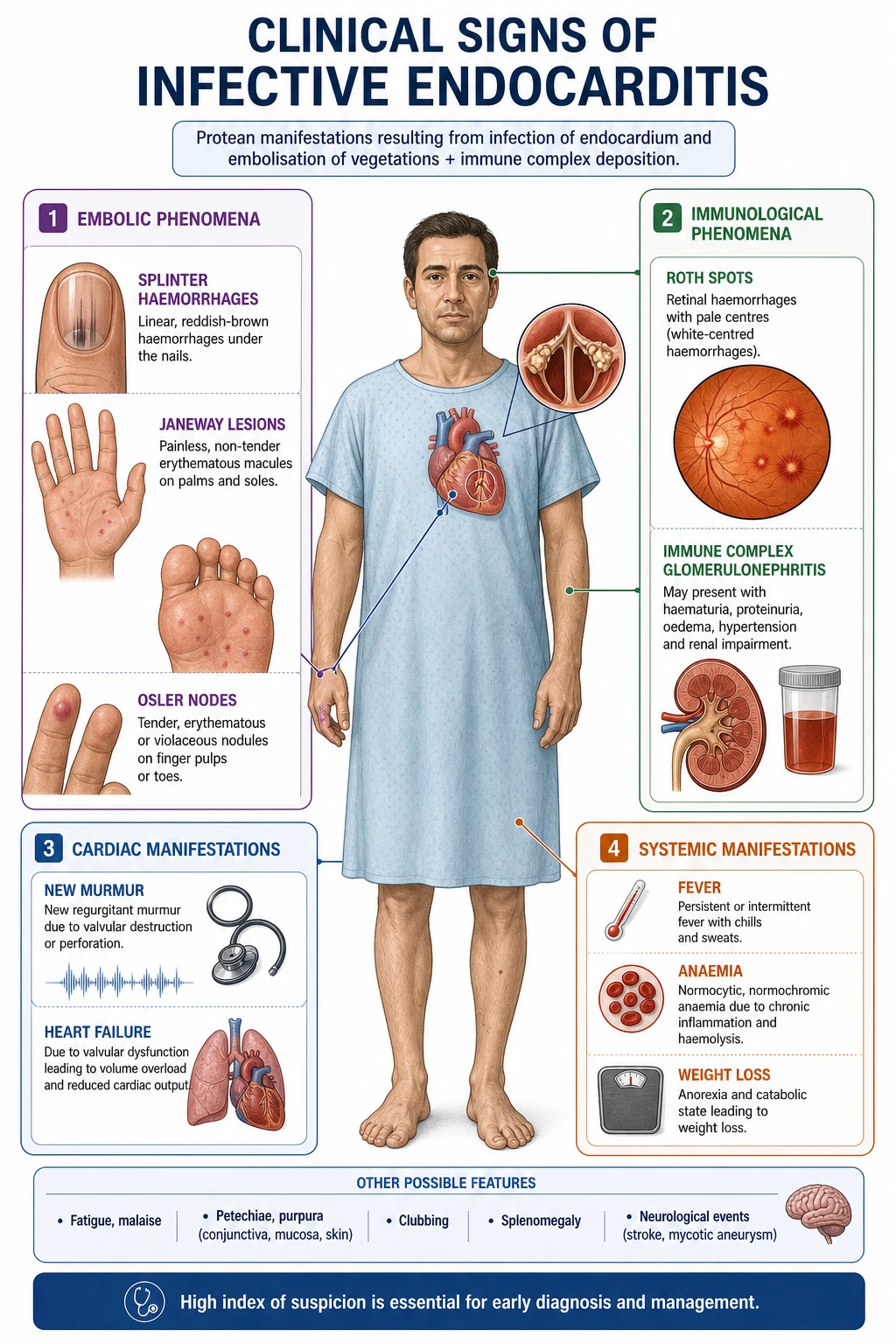
Embolic phenomena occur in 20-50% and may be the presenting event. The classic sites are cerebral (stroke), splenic (left upper quadrant pain), renal (flank pain, haematuria), mesenteric (abdominal pain), and peripheral limb (cold, painful pulseless limb). Septic pulmonary emboli (pleuritic chest pain, cavitated lung infiltrates) indicate right-sided IE. Retinal artery embolus (Roth spots are not embolic — see below) is rare but specific. Embolic risk is highest before antibiotics are started and falls rapidly within the first week of appropriate therapy — which is why early antibiotics matter. [1]
Immune phenomena reflect sustained immune-complex formation. Osler nodes are tender, pea-sized nodules on the finger or toe pads — they are painful, immunological, and resolve with treatment. Roth spots are retinal haemorrhages with a pale centre — immunological vasculitis, not emboli. Glomerulonephritis presents with haematuria, proteinuria, and rising creatinine — immune-complex mediated, often with low complement. Rheumatoid factor becomes positive in chronic IE — its presence is a minor Duke criterion. [1]
Vascular / septic embolic phenomena are distinct from immune phenomena and must not be confused. Janeway lesions are painless macular haemorrhages on the palms or soles — they are septic microemboli. Conjunctival petechiae, splinter haemorrhages (linear subungual, distal third of nail — though these are also common in healthy people and trauma), and major arterial embolus are all septic embolic. [1]
The Osler vs Janeway distinction — the single most-tested clinical sign
This is a guaranteed DCE short-case discriminator. Osler nodes are painful; Janeway lesions are painless. Osler nodes are immunological (immune complexes); Janeway lesions are septic emboli. Both are on the hands and feet. If the examiner asks "is this painful?" and the answer is yes, call it Osler; if no, call it Janeway. Roth spots are immunological (retina), not embolic. Splinter haemorrhages are embolic (nail bed). Mixing these up fails the station. [1]
Other examination findings
Splenomegaly is present in 15-50% of subacute IE — it suggests chronicity. Clubbing appears late (after 6-8 weeks) and also suggests chronicity. New conduction block (PR prolongation, bundle branch block, complete heart block) on ECG suggests aortic root abscess — a surgical emergency. Pulsatile liver and elevated JVP indicate tricuspid involvement or right heart failure. Heart failure signs (basal crackles, elevated JVP, third heart sound) are ominous — heart failure is the strongest indication for surgery. [1]
Investigations — the diagnostic pathway
Blood cultures — the single most important investigation
Blood cultures are the highest-yield and most time-sensitive investigation. Draw three sets from three separate venepuncture sites, spaced at least 30 minutes apart, before starting antibiotics. Do not wait for a fever spike — bacteraemia in IE is continuous, not intermittent. Each set is one aerobic and one anaerobic bottle. Use antiseptic technique meticulously — a contaminated culture is a diagnostic disaster in suspected IE. If the patient has received antibiotics, use resin-containing bottles (which adsorb antibiotics) and hold cultures longer. [1]
If you suspect the patient has IE and they are haemodynamically stable, take cultures over 2-3 hours before starting empiric antibiotics. If they are septic or unstable, draw cultures and start antibiotics immediately — the empiric regimen will cover the likely organisms and you can narrow later. [1]
Echocardiography — TTE first, TOE in most
Transthoracic echo (TTE) is first-line. It detects vegetations greater than 2-3 mm, assesses valve function, and identifies haemodynamic consequences (regurgitation, ventricular function, pulmonary pressure). Its sensitivity for vegetations is 40-60% in native valve IE and lower in PVE. [1]
Transoesophageal echo (TOE) has sensitivity greater than 90% for native valve vegetations and 90-100% for PVE, abscess, and perforation. TOE is indicated in essentially every patient with suspected or definite IE, because it detects complications (abscess, perforation, dehiscence) that change management. The only exceptions are unequivocally uncomplicated native valve IE with a high-quality TTE that answers every clinical question. [1]
Specific indications for TOE:
- Prosthetic valve
- Suspected abscess or paravalvular complication (new conduction block, persistent fever on appropriate antibiotics)
- Negative or inconclusive TTE
- S. aureus bacteraemia with a prosthetic valve or intracardiac device
- Persistent bacteraemia despite appropriate antibiotics
- Embolic event with suspected IE [1]
Repeat echo if there is clinical deterioration, new murmur, new conduction block, or persistent fever. [1]
Other investigations
ECG — look for PR prolongation or new heart block, which indicates aortic root abscess. Chest X-ray — septic pulmonary emboli (cavitated nodules) suggest right-sided IE. Urinalysis — haematuria and proteinuria suggest glomerulonephritis. Bloods — FBE (anaemia of chronic disease, leucocytosis), ESR and CRP (elevated but non-specific), U&E (AKI from antibiotics, GN, or contrast), LFTs (may be normal). Immunology — rheumatoid factor (positive in chronic IE). Serology — send if cultures negative after 5-7 days: Coxiella, Bartonella, Brucella, Legionella, HIV. [1]
18F-FDG PET/CT — the 2023 ESC guideline elevated PET/CT to a major criterion when abnormal uptake around a prosthetic valve is detected more than 3 months after implantation. It is also useful for detecting metastatic infection (splenic, vertebral) and embolic events. PET/CT is not useful within 3 months of surgery (postoperative inflammation) or for native valves. [1]
Cardiac CT — complementary to TOE for detecting paravalvular complications, abscess, pseudoaneurysm, and for surgical planning. Coronary angiography — performed before elective valve surgery to identify concomitant coronary disease; omitted in emergency surgery or if the risk of contrast load is prohibitive. 18F-FDG PET/CT or WBC SPECT/CT for prosthetic material. [1]
Antibiotic therapy — the structured approach
Antibiotic therapy is organism-directed whenever possible, empiric when the organism is unknown, and always prolonged (2-6 weeks intravenous). The cardinal rules: bactericidal agents, high dose, intravenous, prolonged duration, and monitored for nephrotoxicity (especially with aminoglycosides). Below is the framework an ANZ registrar will use, anchored to Therapeutic Guidelines (Australia) and the 2023 ESC guideline. [1]
Empiric therapy (before organism identified)
| Scenario | Regimen (ANZ primary) | Rationale |
|---|---|---|
| Native valve, community-acquired, stable | Ceftriaxone 2 g IV OD (covers streptococci, enterococci, HACEK, community S. aureus) | Broad Gram-positive cover; once-daily for OPAT |
| Suspected MRSA or severe beta-lactam allergy | Vancomycin 25-30 mg/kg IV loading then 15-20 mg/kg BD-TDS (target trough 15-20) PLUS Gentamicin | Vancomycin for MRSA; consider daptomycin if vancomycin MIC elevated |
| Prosthetic valve (early, less than 1 year) | Vancomycin PLUS Gentamicin PLUS Ciprofloxacin (or Rifampicin if staphylococcal confirmed) | Cover coagulase-negative staphylococci, MRSA, Gram-negatives |
| Prosthetic valve (late, greater than 1 year) | Vancomycin PLUS Gentamicin (then narrow to culture-directed) | Similar to early PVE empirically; late PVE microbiology mirrors native valve |
In ANZ, the Heart Foundation and Therapeutic Guidelines recommend ceftriaxone as the empiric backbone for community-acquired native valve IE because of its spectrum and convenience. In the UK and much of Europe, the regimen often adds amoxicillin for enterococcal and HACEK cover. [1]
Culture-directed therapy
Viridans streptococci, penicillin-susceptible (MIC less than or equal to 0.12 mg/L):
- Ceftriaxone 2 g IV OD OR Penicillin G 12-18 million units/day IV (in 4-6 divided doses)
- Duration: 4 weeks (standard) OR 2 weeks if uncomplicated native valve IE with ceftriaxone plus low-dose gentamicin for the first 2 weeks (the 2-week regimen is for the carefully selected, haemodynamically stable patient with a susceptible organism and no embolic, cardiac, or extracardiac complications) [1]
Viridans streptococci, relatively resistant (MIC 0.25-0.5 mg/L):
- Penicillin G or ceftriaxone for 4 weeks PLUS gentamicin for the first 2 weeks [1]
Staphylococcus aureus, methicillin-sensitive (native valve):
- Flucloxacillin (or nafcillin) 12 g/day IV in 4-6 divided doses for 4-6 weeks
- Gentamicin for the first 3-5 days is optional and provides no mortality benefit — many units omit it due to nephrotoxicity, especially with concomitant AKI
- For penicillin allergy (non-anaphylactic): cefazolin. For anaphylactic allergy: vancomycin [1]
Staphylococcus aureus, methicillin-resistant (MRSA):
- Vancomycin 25-30 mg/kg loading, then 15-20 mg/kg BD-TDS, targeting trough 15-20 mg/L, for 6 weeks
- Consider daptomycin 8-10 mg/kg/day if vancomycin MIC greater than 1.5 or failure [1]
Staphylococcal prosthetic valve endocarditis:
- Flucloxacillin (or vancomycin for MRSA) PLUS rifampicin 300-600 mg/day PLUS gentamicin for the first 2 weeks, total duration at least 6 weeks
- Rifampicin is added for prosthetic material because it sterilises the biofilm — but only once bacteraemia has cleared (usually after 3-5 days), to avoid rapid emergence of resistance [1]
Enterococci (ampicillin-susceptible):
- Ampicillin 12 g/day IV PLUS gentamicin (or ampicillin PLUS ceftriaxone, the alternative non-nephrotoxic regimen) for 4-6 weeks
- Ampicillin PLUS ceftriaxone is preferred in older patients and those with CKD to avoid gentamicin nephrotoxicity [1]
HACEK organisms:
- Ceftriaxone 2 g IV OD for 4 weeks (3 weeks for PVE) [1]
Fungal IE (Candida):
- Liposomal amphotericin B PLUS flucytosine, with early surgical intervention and long-term (often lifelong) fluconazole suppression [1]
Aminoglycoside monitoring
If gentamicin is used, monitor trough levels (less than 1 mg/L for once-daily dosing), renal function, and audiometry at baseline and weekly. Avoid gentamicin in the elderly, those with CKD, and when vancomycin is also being given (synergistic nephrotoxicity). In ANZ practice, gentamicin use has declined substantially because of nephrotoxicity and the availability of equally effective alternatives (ceftriaxone, ampicillin-ceftriaxone for enterococci). [1]
Outpatient parenteral antibiotic therapy (OPAT)
Once the patient is afebrile for several days, cultures negative, clinically improving, and surgical issues excluded, OPAT is appropriate for the remainder of therapy. Ceftriaxone 2 g OD is ideal for OPAT because of once-daily dosing. The 2023 ESC guideline formalised OPAT as a safe option in stable, uncomplicated IE, with weekly clinical and laboratory review. [1]
Surgical indications — when the operating room is the treatment
Approximately 50% of patients with left-sided IE undergo surgery during the index admission. The decision is made by the Endocarditis Team — cardiologist, infectious diseases physician, cardiac surgeon, microbiologist — and is governed by three principle indications: heart failure, uncontrolled infection, and embolic risk prevention. [1]
The three surgical principles
1. Heart failure — the strongest indication. Heart failure due to valvular dysfunction (new severe regurgitation, obstruction, fistula, prosthetic dehiscence) is the single strongest indication for surgery and the most common reason for early mortality in IE. If heart failure is due to a surgically correctable lesion, operate — urgently or emergently. The degree of heart failure drives the timing: refractory pulmonary oedema or cardiogenic shock is an emergency; stable but symptomatic heart failure is urgent (within days). [1]
2. Uncontrolled infection. Surgery is indicated for:
- Persistent fever and positive blood cultures beyond 5-7 days of appropriate antibiotics (suggests abscess, infected prosthetic material, or metastatic focus)
- Perivalvular extension — abscess, fistula, heart block (PR prolongation or new bundle branch block on ECG)
- Fungal or highly resistant organisms that cannot be eradicated medically
- S. aureus PVE — early surgery is often considered because of high medical-therapy failure rates [1]
3. Prevention of embolism. Embolic risk is highest before antibiotics and falls rapidly after the first week. Surgery for embolic prevention is considered when:
- Vegetation greater than 10 mm AND a prior embolic event
- Vegetation greater than 15 mm regardless of embolic events (some guidelines use greater than 10 mm with other risk factors)
- Vegetation greater than 10 mm with severe valve dysfunction or other surgical indication [1]
The Kang et al (2012) RCT randomised 76 patients with left-sided IE, severe valve disease, and vegetations 10 mm or greater to early surgery (within 48 hours) versus conventional treatment. Early surgery reduced the composite of in-hospital death and embolic events (3% vs 23%, HR 0.10). This trial underpins early surgery for large mobile vegetations — though it excluded patients with embolic stroke and required severe valve disease, so it does not apply to all IE. [1]
Surgical timing — emergency, urgent, elective
| Timing | Indication | Window |
|---|---|---|
| Emergency | Refractory heart failure, cardiogenic shock, uncontrolled sepsis with surgically correctable lesion | Within 24 hours |
| Urgent | Mobile vegetation greater than 10 mm with embolus, abscess with conduction block, prosthetic dehiscence | Within days |
| Elective | Healed IE with residual severe valve dysfunction, fungal IE after stabilisation | Weeks |
The neurological complication — when surgery is deferred
Embolic stroke complicates up to 35% of IE. After an ischaemic stroke, surgery is deferred by at least 2-4 weeks (or 4 weeks after haemorrhagic stroke) because of the risk of haemorrhagic transformation under cardiopulmonary bypass anticoagulation. The exception is refractory heart failure, where the mortality of deferring surgery exceeds the neurological risk — in which case early surgery may proceed after neurosurgical consultation. This is an Endocarditis Team decision, not a registrar's. [1]
Prophylaxis — who, which procedures, which antibiotic
IE prophylaxis is one of the most over-applied and under-understood areas of medicine. The 2007 AHA guideline (Wilson et al) and subsequent ESC and NICE guidance restricted prophylaxis to a narrow high-risk group — a dramatic narrowing from previous practice. The rationale: bacteraemia from everyday activities (toothbrushing, chewing) is far more frequent than from procedures, and the evidence that prophylaxis prevents IE at the population level is weak. [1]
Who is at high risk (warranting prophylaxis)?
The 2007 AHA and 2023 ESC guidelines identify a narrow high-risk group: [1]
- Prosthetic cardiac valve or prosthetic material used for valve repair (including transcatheter-implanted prostheses and homografts)
- Previous IE
- Congenital heart disease:
- Unrepaired cyanotic CHD, including palliative shunts and conduits
- Completely repaired congenital heart defect with prosthetic material or device, during the first 6 months after the procedure (after which endothelialisation reduces risk)
- Repaired CHD with residual defects adjacent to the site of a prosthetic patch or device
- Cardiac transplant recipients who develop cardiac valvulopathy (AHA only — ESC does not include this) [1]
Patients with all other valve disease (bicuspid aortic valve, mitral valve prolapse with regurgitation, rheumatic or calcific valve disease, acquired valve disease, hypertrophic cardiomyopathy) and all other congenital heart disease do NOT receive routine prophylaxis. This is a frequent exam trap — the scenario of "mitral valve prolapse, dental work, which antibiotic?" has the answer "none." [1]
Which procedures warrant prophylaxis?
Only dental procedures involving manipulation of gingival tissue, the periapical region of teeth, or perforation of the oral mucosa. This includes dental extraction, scaling, and periodontal procedures. [1]
Procedures that do NOT require prophylaxis (the traps):
- Routine dental cleaning, fillings, local anaesthetic injection
- Upper and lower GI endoscopy (gastroscopy, colonoscopy with or without biopsy, ERCP)
- Cystoscopy, urethral catheterisation, transoesophageal echo
- Vaginal delivery, caesarean section
- Percutaneous cardiac procedures (PCI, ablation)
- Body piercing or tattooing (not recommended for high-risk patients, but prophylaxis not formally advised) [1]
The Thornhill et al (2011) BMJ study showed that after NICE recommended complete cessation of prophylaxis in the UK in 2008, prescribing fell by about 80% with no immediate surge in IE — but subsequent longer-term analyses suggested a slow rise in IE incidence that remains debated. This controversy is examiner material: know that NICE (2008, updated) recommended NO routine prophylaxis, while AHA and ESC recommend prophylaxis for the high-risk group undergoing dental procedures. ANZ and most of the world follow AHA/ESC. [1]
Which antibiotic?
The standard regimen for dental prophylaxis, given 30-60 minutes before the procedure: [1]
| Scenario | Regimen |
|---|---|
| Standard (able to take oral) | Amoxicillin 2 g PO, 30-60 min before |
| Penicillin allergy (non-anaphylactic) | Cephalexin 2 g PO, OR Clindamycin 600 mg PO |
| Penicillin anaphylaxis / urticaria | Clindamycin 600 mg PO, OR Azithromycin/Clarithromycin 500 mg PO |
| Unable to take oral + penicillin allergy | Clindamycin 600 mg IV, OR Cefazolin/Ceftriaxone 1 g IV (if non-anaphylactic only) |
If the dose is forgotten before the procedure, give it as soon as possible (up to 2 hours after). [1]
Complications — the things that kill and disable
Cardiac complications
Heart failure is the leading cause of death in IE — from acute severe regurgitation (aortic or mitral), obstruction (large vegetation), fistula (aortic-to-right ventricle or atrium), or prosthetic dehiscence. It is the strongest indication for surgery. [1]
Perivalvular extension — abscess, pseudoaneurysm, fistula — occurs in 10-40% of native valve IE (higher in aortic and PVE). It manifests as persistent fever and bacteraemia on therapy, new conduction block (PR prolongation, bundle branch block, complete heart block — because the aortic root abscess erodes into the conducting system), and pericarditis (sometimes purulent). Diagnose with TOE and cardiac CT. Surgery is required. [1]
Prosthetic valve dehiscence — a paravalvular leak, often with new regurgitant murmur and haemolysis. Surgical. [1]
Neurological complications
Neurological complications occur in 20-40% of IE and are the second leading cause of death. Embolic ischaemic stroke is most common — typically a bland infarct in the territory of the middle cerebral artery, often with haemorrhagic transformation. Mycotic aneurysm (infected arterial wall aneurysm, typically distal middle cerebral artery) may rupture with catastrophic intracranial haemorrhage — suspect in any IE patient with sudden severe headache, and image with CT angiography. Brain abscess is less common. Encephalopathy may result from multiple microemboli or septicaemia. [1]
The management tension: anticoagulation is held during acute IE stroke (especially with haemorrhagic transformation), and surgery is deferred by at least 2 weeks after ischaemic stroke (4 weeks after haemorrhagic) — unless heart failure dictates otherwise. For patients on warfarin for a mechanical valve who develop IE, switch to unfractionated heparin (short half-life, reversible) — but this is a specialist decision. [1]
Systemic embolic complications
Splenic infarction or abscess (left upper quadrant pain, referred to left shoulder, peritonism) — image with CT; splenectomy may be required for abscess. Renal infarction (flank pain, haematuria) — supportive. Mesenteric embolus (acute abdomen, often missed pre-operatively). Limb embolus (cold, painful, pulseless limb — embolectomy required). Retinal artery embolus (visual loss). [1]
Renal complications
Acute kidney injury in IE has several overlapping causes: immune-complex glomerulonephritis (haematuria, proteinuria, low complement), antibiotic nephrotoxicity (aminoglycosides, vancomycin), contrast nephropathy (from CT coronary angiography), sepsis-related ATN, and embolic renal infarction. Distinguishing them requires urinalysis (dysmorphic red cells and red cell casts suggest GN), urinary electrolytes, and sometimes renal biopsy in refractory cases. Management is supportive plus addressing the cause — the GN usually resolves with IE treatment. [1]
Prognosis and follow-up
In-hospital mortality of IE is 15-20%, rising to 25-40% in PVE and S. aureus IE. Five-year mortality approaches 40%, driven by comorbidity, recurrent IE, and heart failure. Adverse prognostic factors: heart failure, S. aureus, prosthetic valve, age, diabetes, renal failure, large vegetation, embolic events, perivalvular abscess, and delay in surgery when indicated. [1]
After completion of therapy, patients need echocardiographic follow-up (baseline TTE at end of therapy, then periodic), dental review (every 6 months), education on prophylaxis and on symptoms of recurrence, and surveillance for metastatic infection. Recurrent IE occurs in 5-10% — distinguish relapse (same organism, within 6 months, often from inadequately treated source) from reinfection (different organism or after 6 months). [1]
The Endocarditis Team and heart valve centre
The 2023 ESC guideline reinforced the Endocarditis Team as the standard of care — a multidisciplinary group (cardiology, infectious diseases, cardiac surgery, microbiology, imaging, anaesthetics, pharmacy, specialist nursing) that meets regularly to make collective decisions. Patients managed within this structure have lower mortality. Complex IE (PVE, cardiac device infection, complicated IE, IE in pregnancy, IE in IVDU) should be referred to a Heart Valve Centre with on-site cardiac surgery, structured imaging, and an Endocarditis Team. [1]
Long-case integration — the IE patient with multiple problems
In a DCE long case, IE rarely presents in isolation. The archetypes are: prosthetic valve IE with AKI and neurological event; native valve IE in IVDU with hepatitis C and right-sided IE; S. gallolyticus IE with occult colorectal cancer; culture-negative IE in an elderly farmer with prosthetic valve (think Coxiella); IE in pregnancy. [1]
The long-case structure for IE is: recognise the syndrome (fever, murmur, Duke criteria), identify the organism and source, stratify the surgical indication (heart failure, uncontrolled infection, embolic risk), manage the complications (neurological, renal, embolic), address the comorbidity (IVDU, malignancy, pregnancy), and plan the long term (prophylaxis, surveillance, recurrence). Each of these is a problem on the list — see the case and viva artifacts for worked examples. [1]
Short-case integration — the cardiovascular examination in suspected IE
The DCE short case on IE examines three things: the valve lesion (usually a new or changing regurgitant murmur, often with a prosthetic click), the peripheral stigmata (Osler nodes, Janeway lesions, Roth spots, splinter haemorrhages, splenomegaly, clubbing), and the discussion (Duke criteria, organism, management). See the case artifact for the examination routine and presentation template. [1]
High-yield exam traps and discriminators
- Staph aureus bacteraemia is a Duke MAJOR criterion — even a single culture, even nosocomial. Do not classify it as minor.
- Osler nodes (painful, immunological) vs Janeway lesions (painless, septic embolic) — the most-tested physical sign.
- Heart failure is the strongest surgical indication — stronger than organism, vegetation size, or embolic history.
- Prophylaxis is restricted to prosthetic valve, prior IE, unrepaired/partially-repaired cyanotic CHD — mitral valve prolapse and bicuspid aortic valve do NOT get prophylaxis.
- Routine GI/GU procedures do not require prophylaxis — only dental procedures with gingival manipulation.
- Coxiella serology (anti-phase I IgG greater than 1:800) is a major criterion — the culture-negative organism most likely to be examined.
- PR prolongation on ECG means aortic root abscess until proven otherwise — TOE and urgent surgical referral.
- Prosthetic valve IE requires at least 6 weeks of therapy with rifampicin added for staphylococcal PVE (after bacteraemia clears).
- The 2-week regimen is only for uncomplicated viridans strep native valve IE with susceptible organism and no embolic, cardiac, or extracardiac complications — use ceftriaxone plus gentamicin.
- Streptococcus gallolyticus demands colonoscopy — 25-60% association with colorectal neoplasia. [1]
Regional guideline summary
| Body | Prophylaxis position | Key document |
|---|---|---|
| ESC (2023) | Prophylaxis for high-risk group (prosthetic valve, prior IE, specified CHD) undergoing dental procedures | Delgado et al, Eur Heart J 2023 (PMID 37622656) |
| AHA (2007, reaffirmed) | Prophylaxis for high-risk group undergoing dental procedures | Wilson et al, Circulation 2007 (PMID 17446442) |
| NICE (UK, CG64, updated 2016) | Prophylaxis NOT routinely recommended; not offered or given to at-risk patients undergoing dental or non-dental procedures | Thornhill et al BMJ 2011 (PMID 21540258) |
| NHFA / CSANZ (Australia) | Aligns with AHA — prophylaxis for high-risk group | Heart Foundation Australia |
| Therapeutic Guidelines (ANZ) | Empiric ceftriaxone backbone for community native valve IE; flucloxacillin for acute staphylococcal | eTG Antibiotic |
The ANZ registrar will follow AHA/ESC principles (high-risk group, dental procedures, amoxicillin), while being aware that NICE differs. This regional delta is examiner material for FRACP. [1]
References
- Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000;30(4):633-638. PMID: 10770721.
- Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications. Circulation. 2005;111(23):e394-e434. PMID: 15956145.
- Fowler VG Jr, Miro JM, Hoen B, et al. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA. 2005;293(24):3012-3021. PMID: 15972563.
- Moreillon P, Que YA. Infective endocarditis. Lancet. 2004;363(9403):139-149. PMID: 14726169.
- Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association. Circulation. 2007;116(15):1736-1754. PMID: 17446442.
- Kang DH, Kim YJ, Kim SH, et al. Early surgery versus conventional treatment for infective endocarditis. N Engl J Med. 2012;366(26):2466-2473. PMID: 22738096.
- Hubert S, Thuny F, Resseguier N, et al. Prediction of symptomatic embolism in infective endocarditis: construction and validation of a risk calculator. J Am Coll Cardiol. 2013;62(15):1384-1392. PMID: 23906859.
- Thornhill MH, Dayer MJ, Forde JM, et al. Impact of the NICE guideline recommending cessation of antibiotic prophylaxis for prevention of infective endocarditis. BMJ. 2011;342:d2392. PMID: 21540258.
- Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis. Eur Heart J. 2015;36(44):3075-3128. PMID: 26320109.
- Delgado V, Bjursten MF, Baddour LM, et al. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J. 2023;44(39):3948-4042. PMID: 37622656. [1]
References
- [1]Li JS, Sexton DJ, Mick N, Nettles R, Fowler VG Jr, Ryan T, Bashore T, Corey GR Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis Clin Infect Dis, 2000.PMID 10770721
- [2]Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America Circulation, 2005.PMID 15956145
- [3]Fowler VG Jr, Miro JM, Hoen B, et al. Staphylococcus aureus endocarditis: a consequence of medical progress JAMA, 2005.PMID 15972563
- [4]Moreillon P, Que YA Infective endocarditis Lancet, 2004.PMID 14726169
- [5]Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group Circulation, 2007.PMID 17446442
- [6]Kang DH, Kim YJ, Kim SH, et al. Early surgery versus conventional treatment for infective endocarditis N Engl J Med, 2012.PMID 22738096
- [7]Hubert S, Thuny F, Resseguier N, et al. Prediction of symptomatic embolism in infective endocarditis: construction and validation of a risk calculator in a multicenter cohort J Am Coll Cardiol, 2013.PMID 23906859
- [8]Thornhill MH, Dayer MJ, Forde JM, et al. Impact of the NICE guideline recommending cessation of antibiotic prophylaxis for prevention of infective endocarditis: before and after study BMJ, 2011.PMID 21540258
- [9]Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM) Eur Heart J, 2015.PMID 26320109
- [10]Delgado V, Bjursten MF, Baddour LM, et al. 2023 ESC Guidelines for the management of endocarditis Eur Heart J, 2023.PMID 37622656