Phys · cardiovascular
Pericardial Disease
Also known as acute pericarditis · viral pericarditis · pericardial effusion · cardiac tamponade · constrictive pericarditis · recurrent pericarditis · Dressler syndrome · post-pericardiotomy syndrome
Consultant-physician-depth guide to the pericardial syndromes — acute pericarditis, pericardial effusion and cardiac tamponade, constrictive pericarditis, and recurrent pericarditis — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Pericardial Disease

The answer first
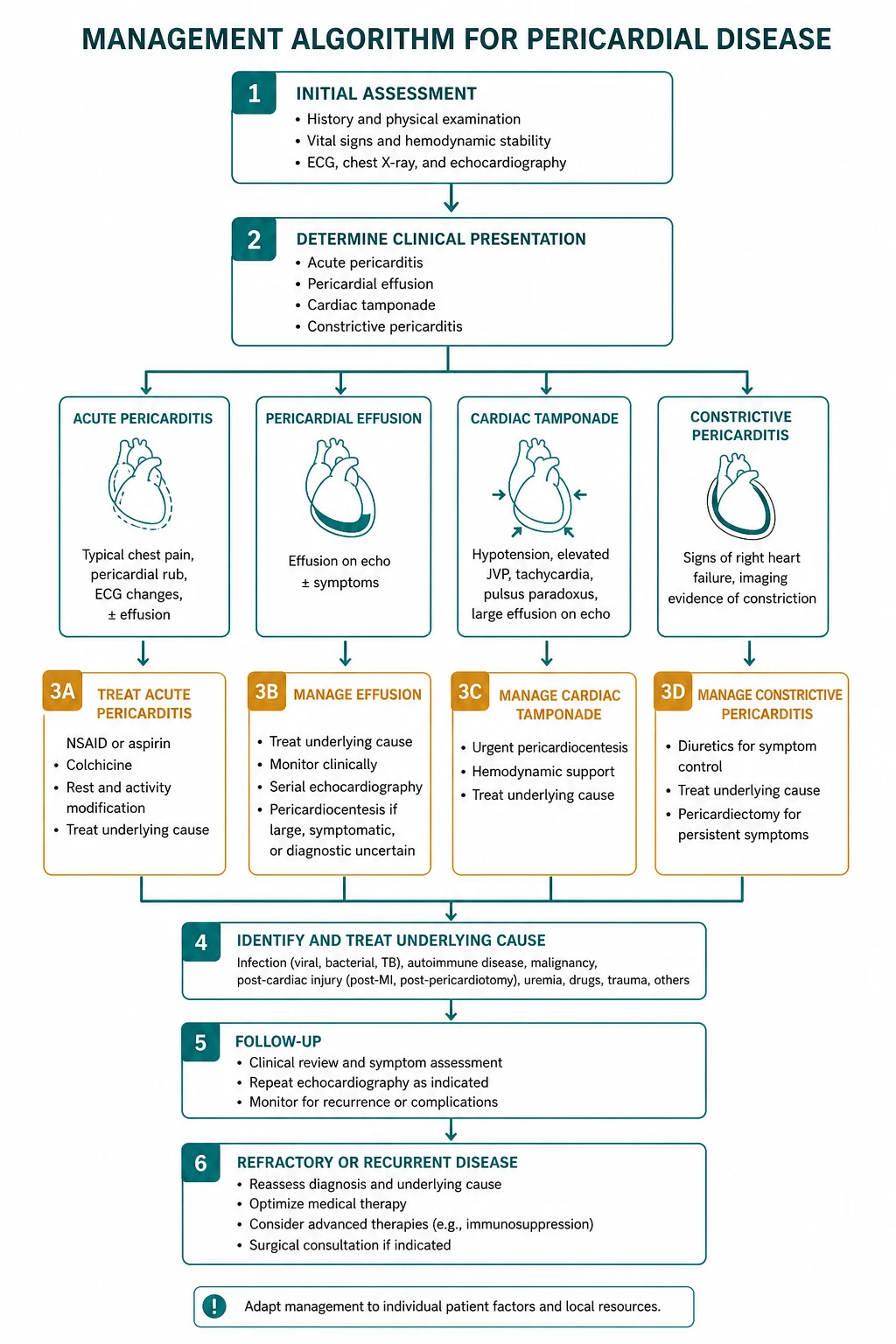
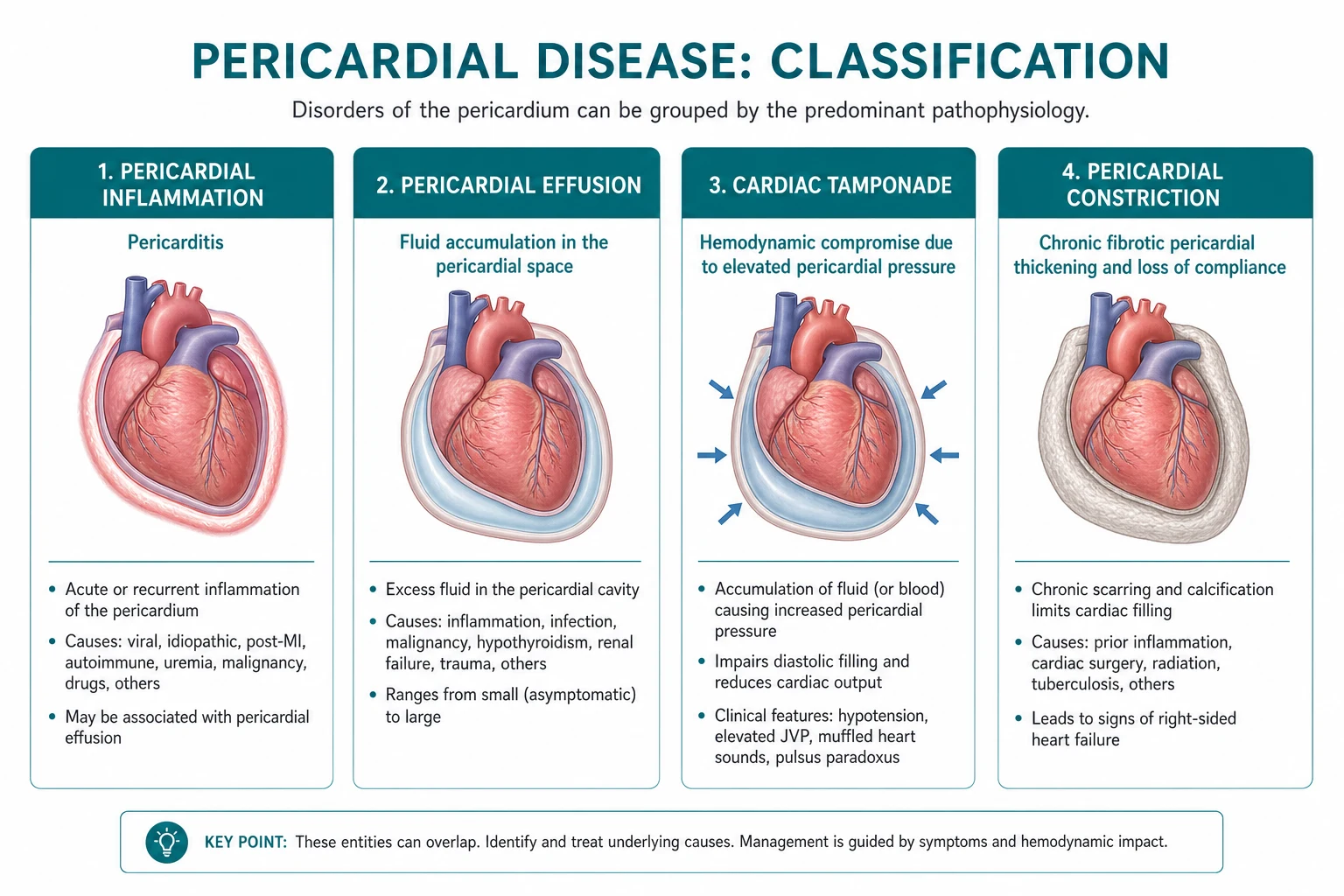
Pericardial disease is a family of syndromes that share the pericardium as their target organ but behave very differently. The four syndromes you must hold in mind are acute pericarditis, pericardial effusion with or without cardiac tamponade, constrictive pericarditis, and recurrent pericarditis. Each has a distinctive clinical fingerprint and a different urgency. [1]
The three management decisions that examiners test again and again: [1]
- Acute viral pericarditis is treated with NSAIDs plus colchicine — not steroids. Steroids increase recurrence risk and are reserved for NSAID failure, autoimmune disease, or uraemic pericarditis.
- Cardiac tamponade is a clinical diagnosis confirmed by echo, and the treatment is emergency pericardiocentesis — not fluid, not pressors, not waiting for the next set of bloods.
- Constrictive pericarditis presents as right heart failure with a raised JVP showing prominent X and Y descents and a pericardial knock, and the definitive treatment is pericardiectomy — but first you must distinguish it from restrictive cardiomyopathy. [1]
DWE high-yield: If a stem describes a young adult with sharp pleuritic chest pain that improves on sitting forward, plus diffuse ST elevation and PR depression on ECG, the answer is acute pericarditis — treat with ibuprofen or aspirin plus colchicine. Steroids are a distractor. [1]
Acute pericarditis
Clinical presentation
The classic triad is chest pain, a pericardial rub, and characteristic ECG changes — but you rarely need all three to make the diagnosis. [1]
Chest pain is the hallmark. It is sharp, pleuritic, and positional:
- Worse on deep inspiration and coughing — because the inflamed pericardium rubs against the parietal pleura and chest wall.
- Worse on lying flat — because the heart sits against the posterior pericardium, maximising contact with the inflamed surface.
- Better on sitting up and leaning forward — because gravity lifts the heart away from the posterior pericardium. This is the single most discriminating bedside feature. [1]
Pain may radiate to the trapezius ridge (left shoulder) because the pericardium shares C3–C5 innervation with the phrenic nerve. This trapezius radiation is underrecognised but highly suggestive of pericardial rather than ischaemic pain. [1]
Pericardial friction rub — a high-pitched, scratching, leathery sound best heard at the left sternal border with the patient sitting forward and holding breath in expiration. It classically has three components (atrial systole, ventricular systole, rapid ventricular filling) but is often biphasic or monophasic. It is transient and positional — its absence does not exclude pericarditis, and its presence is virtually pathognomonic. [1]
Low-grade fever, myalgia, and a recent viral prodrome support a viral aetiology. Dyspnoea is usually mild and splinting from pleuritic pain rather than haemodynamic compromise — significant dyspnoea suggests a large effusion or tamponade and mandates urgent echo. [1]
DCE short-case tip: When asked to examine a patient with suspected pericarditis, listen for the rub with the patient sitting forward in full expiration. State aloud: "I am listening for a pericardial friction rub at the lower left sternal edge." Examiners reward this because it shows you know where and how the rub is best heard. [1]
Diagnostic criteria
Diagnosis is clinical and requires at least two of the following four (ESC 2015, JACC 2020): [1]
| Criterion | Detail |
|---|---|
| Characteristic chest pain | Sharp, pleuritic, positional — worse lying flat, better sitting forward |
| Pericardial friction rub | Auscultatory; best at lower left sternal border, sitting forward |
| Characteristic ECG changes | New widespread ST elevation and/or PR depression |
| New or worsening pericardial effusion | On echocardiography |
Supporting evidence: elevated CRP and/or ESR, elevated troponin (indicating myopericarditis — common and does not imply ischaemia), and evidence of pericardial inflammation on cardiac MRI (late gadolinium enhancement of the pericardium). [1]
ECG features

The ECG is the single most tested investigation in DWE stems on pericarditis. Four stages evolve over days to weeks: [1]
| Stage | ECG finding |
|---|---|
| I (acute) | Diffuse concave (saddle-shaped) ST elevation in most leads; PR depression (especially in II, III, aVF, V4–V6); PR elevation in aVR |
| II | ST normalisation; T-wave flattening begins |
| III | Diffuse T-wave inversion (after ST segments have returned to baseline) |
| IV | Normalisation; T waves return to baseline or remain inverted |
Discriminating pericarditis from STEMI on ECG — the classic DWE discriminator table: [1]
| Feature | Pericarditis | STEMI |
|---|---|---|
| ST elevation distribution | Diffuse (multiple vascular territories) | Localised (one vascular territory — e.g. inferior, anterior) |
| ST morphology | Concave (saddle-shaped) | Convex (dome-shaped) |
| PR segment | Depression (in leads with ST elevation); elevation in aVR | Usually unaffected (except subtle PR changes in atrial infarction) |
| Reciprocal ST depression | Absent (except aVR) | Present in opposite leads |
| T-wave inversion timing | Occurs only after ST has normalised | Occurs while ST is still elevated |
| Q waves | Absent | May develop (pathological Q) |
DWE trap: Early repolarisation can mimic pericarditis. The discriminating feature is the PR segment: in pericarditis, PR depression is prominent; in early repolarisation, the PR segment is isoelectric or there is a notched J point. The ratio of ST elevation to T-wave amplitude in V6 (over 0.25 favours pericarditis) is a useful adjunct. [1]
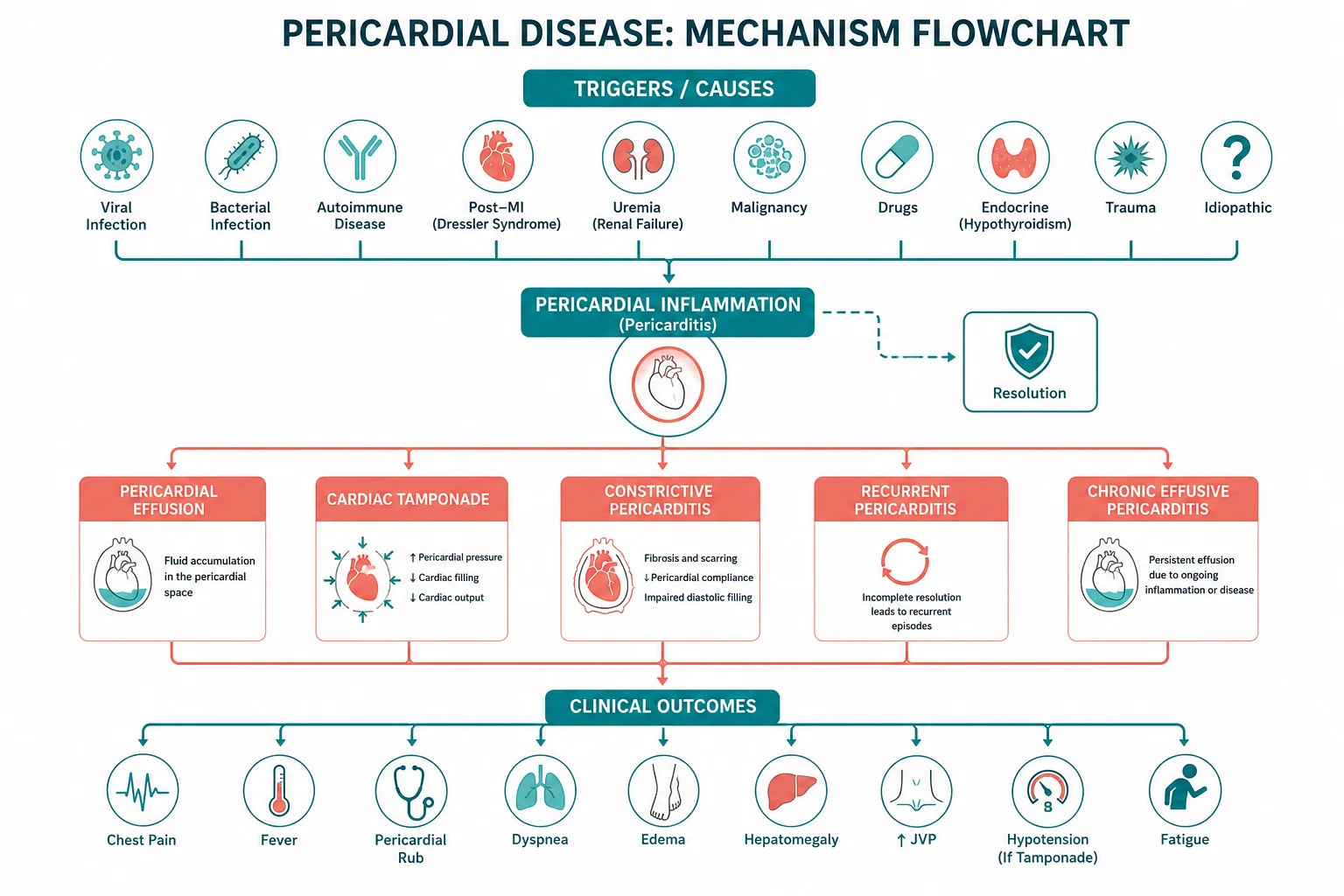
Aetiology
Most acute pericarditis in the community is idiopathic or viral (enteroviruses, echovirus, coxsackie B, adenovirus, parvovirus B19). The full differential to work through when the presentation is atypical or recurrent: [1]
| Category | Causes |
|---|---|
| Infectious | Viral (commonest); bacterial (pneumococcus, staph, strep); tuberculosis (endemic regions — ANZ in migrants from high-prevalence countries); fungal, HIV-related |
| Autoimmune / systemic | Systemic lupus erythematosus, rheumatoid arthritis, Sjogren, systemic sclerosis, vasculitis, inflammatory bowel disease |
| Post-cardiac injury | Post-MI (acute, days 1–3), Dressler syndrome (weeks to months post-MI, immune-mediated), post-cardiac surgery (post-pericardiotomy syndrome), post-ablation, chest trauma |
| Metabolic | Uraemia (common in dialysis patients), hypothyroidism |
| Malignancy | Lung, breast, lymphoma, melanoma — typically effusive rather than purely inflammatory |
| Drugs | Procainamide, hydralazine, isoniazid, penicillin (drug-induced lupus with serositis) |
| Radiation | Mediastinal radiotherapy (late, often constrictive) |
Examiner insight: In the ANZ context, always consider tuberculous pericarditis in a patient born in a TB-endemic country presenting with insidious fever, night sweats, and a large effusion. Send adenosine deaminase (ADA) on pericardial fluid if drained. [1]
Investigations
Essential for every patient: [1]
| Investigation | Why |
|---|---|
| 12-lead ECG | The pivotal test — diffuse ST elevation, PR depression (Stage I) |
| Echocardiogram (TTE) | Quantify any effusion, look for chamber collapse (tamponade physiology), assess LV and RV function, detect myopericarditis (regional wall motion abnormalities) |
| Bloods: FBE, CRP, ESR | CRP guides treatment response and disease activity; leucocytosis and neutrophilia support bacterial or severe inflammation |
| Troponin | Elevated in up to one-third (myopericarditis) — does not imply ACS; correlates with extent of myocardial involvement |
| U&E, creatinine | Exclude uraemic pericarditis (a reversible cause) |
| TFTs | Exclude hypothyroidism |
| ANA, RF, anti-dsDNA | Screen for autoimmune disease if recurrent, atypical, or accompanied by other features |
| Chest X-ray | May show enlarged cardiac silhouette with large effusion (over 200 mL); look for pneumonia, TB, malignancy |
| Blood cultures, viral serology, HIV test | If fever, immunosuppression, or specific suspicion |
Cardiac MRI (CMR) — reserved for atypical, recurrent, or complicated cases. It detects pericardial oedema and late gadolinium enhancement (LGE) of the pericardium, confirms active inflammation, assesses for concomitant myocarditis (subepicardial or mid-wall LGE), and can reveal early constriction. [1]
DCE long-case trap: Do not send an exhaustive autoimmune and infection panel on every first episode of viral pericarditis. The ESC and JACC reviews recommend a targeted workup — ANA, TFTs, U&E, HIV — with extended testing reserved for recurrent, atypical, or high-risk presentations. [1]
Management

First-line treatment for acute pericarditis is NSAIDs plus colchicine. The combination targets both the acute inflammation (NSAID) and the risk of recurrence (colchicine). [1]
Step 1 — NSAID (choose one): [1]
| Drug | Dose | Duration |
|---|---|---|
| Ibuprofen | 600 mg orally every 8 hours (1800 mg/day) | 1–2 weeks at full dose, then taper over 2–4 weeks |
| Aspirin | 750–1000 mg every 8 hours (high dose) | 1–2 weeks at full dose, then taper |
| Indomethacin | 25–50 mg every 8 hours (avoid in elderly — CNS effects) | As above |
Taper after symptoms resolve and CRP normalises. Continue gastroprotection with a PPI. Adjust dose for renal impairment. [1]
Step 2 — Colchicine (weight-adjusted): [1]
| Weight | Dose | Duration |
|---|---|---|
| Over 70 kg | 0.5 mg twice daily | 3 months |
| 70 kg or under | 0.5 mg once daily (or 0.6 mg — regional brand) | 3 months |
Colchicine halves the recurrence rate at 18 months (ICAP trial, PMID 23992557 — recurrence 16.7% with colchicine vs 37.5% placebo). Do not load colchicine (the older high-dose loading regimen was abandoned due to gastrointestinal toxicity). Main side effect: diarrhoea — reduce dose if it occurs. [1]
Step 3 — Activity restriction: [1]
Restrict strenuous physical activity and competitive sport until symptom-free and CRP normal. For competitive athletes, the ESC recommends restriction until symptoms resolve and inflammatory markers normalise — typically 3 months. [1]
Step 4 — Treat the underlying cause: [1]
- Uraemic pericarditis — intensify dialysis (this is one of the few causes where steroids are NOT needed; haemodialysis resolves it).
- Autoimmune pericarditis — treat the underlying disease; steroids are appropriate here.
- Bacterial — targeted antibiotics plus drainage of any purulent effusion.
- Tuberculous — standard anti-TB therapy (6 months); adjunctive steroids reduce progression to constriction in TB pericarditis. [1]
When to use corticosteroids (and when NOT to)
Corticosteroids are the most overused and most harmful first-line agent in pericarditis. They are an independent risk factor for recurrence — increasing the recurrence rate up to four-fold in observational data. The ESC guidelines and JACC review restrict steroid use to specific indications. [1]
Indications for low-dose corticosteroids: [1]
| Indication | Rationale |
|---|---|
| NSAID failure or contraindication | Genuine intolerance, renal failure precluding NSAIDs, active peptic ulcer |
| Autoimmune pericarditis | SLE, rheumatoid, vasculitis — steroids treat the underlying disease |
| Uraemic pericarditis unresponsive to dialysis | If dialysis alone fails |
| Pregnancy (if NSAIDs contraindicated) | Colchicine and NSAIDs are relatively contraindicated in pregnancy |
When prescribed (if unavoidable): prednisone 0.2–0.5 mg/kg/day (low dose — the ESC moved away from the old high-dose 1 mg/kg regimens precisely because of recurrence risk). Maintain for 2–4 weeks then taper slowly over several weeks. Always combine with colchicine to mitigate recurrence. [1]
DWE high-yield: A stem that offers steroids as the first-line option for a first episode of viral pericarditis is a trap. The correct answer is an NSAID plus colchicine. Steroids are correct only when the stem specifies NSAID failure, autoimmune disease, or uraemia. [1]
Risk stratification — who to admit
Most patients with a first episode of uncomplicated viral pericarditis can be managed as an outpatient. The ESC and JACC reviews define high-risk features mandating hospital admission: [1]
| High-risk feature | Why it matters |
|---|---|
| Fever over 38 degrees | Suggests bacterial or systemic cause; recurrence risk |
| Subacute onset (over days, not hours) | Atypical for viral; suggests TB, malignancy |
| Large pericardial effusion (over 2 cm diastolic) | Tamponade risk |
| Cardiac tamponade | Emergency |
| Immunosuppression (HIV, chemotherapy, transplant) | Opportunistic infection risk |
| Oral anticoagulation | Risk of haemopericardium |
| Myopericarditis (elevated troponin with wall motion changes) | Risk of LV dysfunction, arrhythmia |
| Failure of initial outpatient NSAID therapy at one week | Reclassify as complex |
| Trauma | Risk of structural injury, haemopericardium |
Pericardial effusion and cardiac tamponade
Pericardial effusion
A pericardial effusion is an abnormal accumulation of fluid in the pericardial space (normally 15–50 mL). The haemodynamic significance depends on the rate of accumulation, not the volume — 200 mL accumulating rapidly can cause tamponade, while 2 litres accumulating over weeks may not. [1]
Causes of a large effusion (the DWE differential):
- Transudate — heart failure, cirrhosis, nephrotic syndrome, hypothyroidism (myxoedema)
- Exudate — malignancy (lung, breast, lymphoma, mesothelioma), infection (viral, bacterial, TB), autoimmune (SLE, rheumatoid), uraemia, post-cardiac injury (Dressler, post-surgery)
- Haemopericardium — trauma, aortic dissection, anticoagulation, post-procedure (catheter, pacemaker), cardiac rupture post-MI [1]
Symptoms — often asymptomatic until large; then dyspnoea (commonest), chest fullness, orthopnoea. Pleuritic pain may be absent if the pericardium is already stretched and non-inflamed. [1]
Examination — muffled heart sounds, Ewart sign (dullness and bronchial breathing below the left scapula from compression atelectasis), enlarged cardiac silhouette on CXR if over 200 mL. [1]
Echo classification by size (diastolic separation of pericardial layers):
- Small: under 1 cm
- Moderate: 1–2 cm
- Large: over 2 cm
- Very large: over 2.5 cm [1]
Cardiac tamponade
Cardiac tamponade is a clinical diagnosis — the emergency where accumulated pericardial fluid compresses the cardiac chambers, preventing diastolic filling, and causing obstructive shock. The diagnosis is made at the bedside, confirmed by echo, and treated by pericardiocentesis. [1]
Beck triad (the classic bedside triad, originally described in acute tamponade with rapid fluid accumulation):
- Hypotension — falling cardiac output from impaired filling
- Raised JVP — venous pressure rises because the right heart cannot accept venous return (the pericardial fluid prevents the right heart from expanding)
- Muffled heart sounds — fluid around the heart dampens transmission [1]
Pulsus paradoxus — the systolic blood pressure drops by more than 10 mmHg on normal inspiration. This is the most important additional sign. Mechanism: during inspiration, intrathoracic pressure falls, venous return to the right heart increases, the interventricular septum shifts leftward (because the pericardium cannot expand to accommodate the increased RV volume), and LV filling is impaired — dropping stroke volume and systolic BP. The exaggerated inspiratory fall is the bedside fingerprint of tamponade physiology. [1]
How to elicit pulsus paradoxus at the bedside (DCE short case): Inflate the cuff above systolic pressure. Deflate slowly. The first Korotkoff sound is heard only in expiration — note this pressure. Continue deflating until Korotkoff sounds are heard throughout the respiratory cycle. The difference between these two pressures is the paradox. Over 10 mmHg is abnormal; over 20 mmHg suggests significant tamponade. Demonstrate and explain aloud. [1]
Other clinical features: tachycardia, tachypnoea, narrow pulse pressure, distended neck veins with absent Y descent (because the right heart cannot relax to accept the rapid early-diastolic venous return). [1]
Echo findings in tamponade

Echocardiography is the confirmatory test. The key findings: [1]
| Echo finding | Significance |
|---|---|
| Pericardial effusion | Usually large and circumferential (but a localised clot post-surgery can also tamponade) |
| Right ventricular diastolic collapse | The most specific sign — the RV free wall buckles inward during early diastole because pericardial pressure exceeds RV diastolic pressure |
| Right atrial collapse | Sensitive but less specific; best when lasting over one-third of the cardiac cycle |
| IVC plethora | Dilated IVC with less than 50% collapse on sniff — reflects elevated right-sided pressures; sensitive but non-specific |
| Respiratory variation in mitral and tricuspid inflow | Over 25% variation in mitral E-wave velocity and over 40% in tricuspid E-wave on inspiration — direct evidence of ventricular interdependence |
ECG and CXR in tamponade
- ECG: low voltage (QRS under 5 mm in limb leads) from fluid short-circuiting the electrical signal; electrical alternans — beat-to-beat variation in QRS amplitude as the heart swings within the effusion. Electrical alternans with low voltage and a large effusion is highly suggestive of tamponade, though it is a late sign.
- CXR: enlarged globular cardiac silhouette (water-bottle heart) with clear lung fields. [1]
Management of tamponade
Cardiac tamponade is an emergency. The definitive treatment is emergency pericardiocentesis — drainage of the pericardial fluid. [1]
| Step | Action |
|---|---|
| 1. Recognise and call for help | Alert cardiology, echo, and the cardiac catheter lab or ICU |
| 2. Emergency pericardiocentesis | Echo-guided subxiphoid or apical approach; drain until haemodynamics improve; leave a drain in situ for 24–48 hours |
| 3. Fluid resuscitation (temporising) | Give 500 mL crystalloid boluses to maintain preload — but this is a bridge to drainage, not a treatment. Do not over-resuscitate |
| 5. Send fluid for analysis | Cell count, protein, LDH, glucose, Gram stain, culture, AFB and TB PCR, cytology, ADA |
| 6. Address the cause | Malignancy (systemic therapy), infection (antibiotics), anticoagulation reversal, aortic dissection (surgery) |
DCE trap: In a patient with tamponade who is shocked, the temptation is to give large volumes of fluid or start inotropes. Fluid is a temporising bridge only; the treatment is drainage. Inotropes do not help because the problem is not pump failure — it is obstructed filling. Pressors may worsen the already-elevated afterload on a heart that cannot fill. Drain the pericardium. [1]
Constrictive pericarditis
Constrictive pericarditis is the chronic sequela in which a thickened, fibrotic, and often calcified pericardium prevents normal diastolic filling of the heart. It presents as right heart failure — and the diagnostic challenge is to distinguish it from restrictive cardiomyopathy, which produces a nearly identical haemodynamic picture but requires entirely different management. [1]
Aetiology
The causes have shifted over decades. In the pre-antibiotic era, tuberculosis dominated. Today in ANZ and most developed settings, the commonest causes are: [1]
| Cause | Note |
|---|---|
| Idiopathic / post-viral | Commonest in modern series; may follow recurrent pericarditis |
| Post-cardiac surgery | Especially after CABG, valve surgery; often presents months to years later |
| Post-radiation | Mediastinal radiotherapy for lymphoma or breast cancer; latency of years to decades; often mixed constriction and restrictive cardiomyopathy (radiation damages both pericardium and myocardium) |
| Tuberculosis | Still common in endemic regions and migrant populations |
| Autoimmune | SLE, rheumatoid, vasculitis |
| Uraemic / dialysis-related | Less common now with better dialysis |
| Malignancy | Direct pericardial invasion or constriction after effusive disease |
| Prior purulent pericarditis | Bacterial; scars the pericardium |
Clinical presentation
Constrictive pericarditis presents with chronic right heart failure in a patient with a normal or near-normal LV ejection fraction: [1]
Symptoms:
- Peripheral oedema, abdominal distension (ascites), fatigue, exertional dyspnoea
- Anorexia, weight loss from chronic congestion and cardiac cachexia
- Often misdiagnosed initially as cirrhosis ("cardiac cirrhosis") or nephrotic syndrome because of the ascites and oedema [1]
Signs (the DCE short-case cluster): [1]
| Sign | Mechanism |
|---|---|
| Raised JVP | The pericardium cannot expand; venous return meets a fixed pericardial volume, so venous pressure rises to force filling |
| Prominent X and Y descent on JVP waveform | The hallmark — the X descent is preserved because atrial relaxation is normal; the Y descent is deep and rapid because early diastolic filling is vigorous (the ventricle fills rapidly until it hits the rigid pericardium, then stops abruptly — the pericardial knock) |
| Kussmaul sign | JVP rises on inspiration (paradoxical) instead of falling — because the rigid pericardium cannot accommodate the increased venous return, so it backs up into the neck veins. Best seen with the patient breathing normally at 45 degrees |
| Pericardial knock | An early diastolic sound (60–120 ms after S2) — high-pitched, heard at the left sternal border; produced by the abrupt cessation of rapid ventricular filling when the expanding ventricle hits the rigid pericardium. It is the constrictive equivalent of the S3 |
| Hepatomegaly, ascites, peripheral oedema | Chronic right heart congestion |
| Pulsus paradoxus | May be present but is less pronounced than in tamponade |
DCE short-case strategy: When you see a raised JVP with right heart failure signs, describe the JVP morphology explicitly — "the JVP is elevated with a prominent Y descent" — and listen for the pericardial knock. These two observations shift the differential from heart failure to constriction. Then state: "I would request an echocardiogram to assess for pericardial thickening, diastolic bounce, and ventricular interdependence, and a CT or MRI to measure pericardial thickness." [1]
Investigations
Echocardiography (TTE) — the first-line imaging test. Key features: [1]
| Echo finding | Significance |
|---|---|
| Pericardial thickening | Often visible; may show increased echogenicity |
| Diastolic septal bounce | The interventricular septum shifts abruptly toward the LV in early diastole — the echo signature of ventricular interdependence |
| Restrictive mitral inflow pattern | Prominent E-wave with short deceleration time (rapid early filling, abrupt stop) |
| Respiratory variation in mitral and tricuspid inflow | Exaggerated — over 25% variation in mitral E-wave, over 40% in tricuspid (ventricular interdependence) |
| Tissue Doppler e-prime (e') | Preserved or increased medial e' (annulus paradoxus) — unlike restrictive cardiomyopathy, where e' is reduced. This is because the myocardium itself is normal in constriction; the restriction is in the pericardium |
| Hepatic vein flow reversal on expiration | Sensitive and specific — due to ventricular interdependence |
CT and MRI — essential to confirm pericardial thickening and to characterise the pericardium: [1]
| Modality | Finding |
|---|---|
| CT | Pericardial thickness over 2 mm (normal is 1–2 mm); pericardial calcification (best seen on non-contrast CT); may show tubular ventricles and dilated atria |
| MRI | Pericardial thickening; pericardial late gadolinium enhancement indicating active inflammation; diastolic septal bounce on cine imaging; tagged MRI showing adherence of pericardium to myocardium (lack of normal sliding) |
Critical caveat: Pericardial thickness on imaging does not correlate perfectly with constriction — constriction can occur with a normal-thickness pericardium (especially early, inflammatory constriction), and a thickened pericardium may be non-constrictive. The diagnosis rests on the haemodynamic picture (clinical plus echo plus catheterisation), with imaging as support. [1]
Cardiac catheterisation — the haemodynamic confirmation when non-invasive imaging is equivocal: [1]
| Finding | Constriction |
|---|---|
| Equalised diastolic pressures | LV and RV diastolic pressures equalise (within 5 mmHg) — the pericardium prevents differential filling |
| Dip-and-plateau (square-root sign) | Ventricular pressure trace shows a rapid early diastolic dip followed by a plateau (rapid filling then abrupt stop against the rigid pericardium) |
| PA systolic pressure | Usually under 55 mmHg (higher suggests restrictive cardiomyopathy or mixed disease) |
| RVEDP / RV systolic pressure ratio | Over one-third favours constriction |
Constriction vs restriction — the critical differentiation
This is the most tested pericardial topic in DCE and DWE. The two conditions produce nearly identical right-heart-failure presentations but require opposite management — pericardiectomy for constriction, medical therapy for restriction. [1]
| Feature | Constrictive pericarditis | Restrictive cardiomyopathy |
|---|---|---|
| Underlying problem | Pericardium (rigid, thickened) | Myocardium (stiff, infiltrated — amyloid, eosinophilic, sarcoid, storage disease) |
| JVP — Y descent | Deep and rapid (prominent) | Less prominent |
| Kussmaul sign | Present | May be present (less discriminating) |
| Pericardial knock | Present | Absent (S3 may be present instead) |
| Apex beat | Impalpable or faint | Palpable, may be displaced |
| Echo — medial e' (tissue Doppler) | Preserved or increased (annulus paradoxus) — myocardium is normal | Reduced — myocardium is stiff |
| Echo — septal bounce | Present | Absent |
| Echo — hepatic vein flow | Expiratory diastolic flow reversal | Inspiratory systolic blunting |
| Echo — LV cavity size / wall thickness | Normal LV size; normal or thin walls; tubular ventricles | Often thick walls (especially amyloid); may have LV hypertrophy; biatrial enlargement |
| CT / MRI pericardial thickness | Over 2 mm; may show calcification | Normal pericardial thickness |
| MRI — myocardial LGE | Pericardial LGE (pericardial inflammation); myocardium spared | Myocardial LGE — subendocardial circumferential (amyloid), patchy (sarcoid), or diffuse |
| BNP | Normal or mildly elevated (myocardium normal) | Markedly elevated (myocardium diseased) |
| Cardiac catheterisation | Equal diastolic pressures; dip-and-plateau; RVEDP/RVSP over one-third | LV diastolic pressure may exceed RV by over 5 mmHg; PA systolic over 55 mmHg; dip-and-plateau may also be present |
| Treatment | Pericardiectomy (curative if early) | Medical — treat underlying cause; diuretics; disease-specific (amyloid: tafamidis/daratumumab) |
DWE high-yield discriminator: The single best discriminator on echo is the medial e' on tissue Doppler. Preserved e' with a restrictive transmitral pattern points to constriction (the myocardium is normal; the problem is the pericardium). Reduced e' points to restriction (the myocardium itself is stiff). This is tested repeatedly because it is the most reliable non-invasive discriminator. [1]
Management of constrictive pericarditis
Definitive treatment is pericardiectomy — surgical removal of the pericardium. This is a major cardiac surgery with a perioperative mortality of 5–15%, higher in elderly, irradiated, or calcific cases. Outcomes are best when surgery is performed early — before irreversible myocardial atrophy and liver damage (cardiac cirrhosis) develop. [1]
Important nuance — transient (reversible) constriction: Up to 20% of constrictive presentations are transient — caused by active pericardial inflammation rather than fixed fibrosis. These patients may resolve with a trial of anti-inflammatory therapy (NSAIDs or colchicine, sometimes a short steroid taper) for 2–3 months before committing to surgery. MRI evidence of pericardial LGE (active inflammation) supports a trial of medical therapy first. [1]
Stepwise approach: [1]
- Confirm the diagnosis — clinical, echo, CT/MRI, and cardiac catheterisation if any doubt.
- Differentiate from restrictive cardiomyopathy — using the echo and MRI criteria above. If restriction, do not proceed to surgery.
- Assess for transient constriction — if MRI shows pericardial LGE and the presentation is recent (within 3–6 months), trial 2–3 months of anti-inflammatory therapy with serial clinical and echo reassessment.
- Refer for pericardiectomy if constriction is fixed, progressive, or fails a medical trial.
- Diurese cautiously for symptom control while awaiting surgery — but diuretics alone do not resolve constriction.
- Treat the underlying cause — anti-TB therapy if TB-related (with adjunctive steroids to reduce progression to constriction). [1]
DCE long-case insight: In a patient with prior mediastinal radiotherapy, constriction may coexist with restrictive cardiomyopathy (radiation damages both pericardium and myocardium) and with coronary and valvular disease. This is one of the hardest long cases you can face. Acknowledge the mixed physiology, prioritise the dominant problem, and involve a multidisciplinary cardiothoracic team. [1]
Recurrent pericarditis and the pericardial syndromes
Recurrent pericarditis is the commonest complication of acute pericarditis, occurring in 15–30% of patients after a first episode. It is defined as a recurrence of pericarditic symptoms and signs after a symptom-free interval of at least 4–6 weeks. [1]
Risk factors for recurrence
| Risk factor | Note |
|---|---|
| Corticosteroid use during the first episode | Independent risk factor — up to four-fold increased recurrence. This is the central reason steroids are avoided first-line |
| Inadequate or too-brief colchicine | Premature cessation increases recurrence |
| Female sex | Slightly higher risk |
| NSAID non-responsiveness | Suggests non-viral or autoinflammatory cause |
| Prior recurrence | Each recurrence increases the risk of the next (clustering) |
| Autoinflammatory / autoimmune background | Familial Mediterranean fever, TRAPS, SLE |
The autoinflammatory basis
Recurrent pericarditis is increasingly understood as an autoinflammatory disease driven by interleukin-1 (IL-1). This reframes the management paradigm: rather than escalating anti-inflammatories, the modern approach targets IL-1 directly with biologic agents for refractory cases. [1]
Stepwise management of recurrent pericarditis
| Step | Therapy | Evidence |
|---|---|---|
| 1. Optimise colchicine | Colchicine 0.5 mg BID (or 0.5 mg daily if under 70 kg) for 6 months minimum (longer for multiple recurrences). Ensure adherence — the commonest reason for "treatment failure" is non-adherence or premature cessation | CORP (first recurrence) and CORP-2 (multiple recurrences, PMID 24694983) both showed colchicine halves recurrence |
| 3. Low-dose corticosteroid (if colchicine + NSAID fail) | Prednisone 0.2–0.5 mg/kg/day — the lowest effective dose; taper very slowly over months; always combine with colchicine to mitigate recurrence | Avoid high-dose regimens (over 0.5 mg/kg) — they increase recurrence |
| 4. IL-1 blockade (if refractory, colchicine-resistant, or steroid-dependent) | Anakinra (recombinant IL-1 receptor antagonist) 100 mg subcutaneously daily — taper after several months of remission; or rilonacept (long-acting IL-1 trap) 160 mg SC loading then 80 mg weekly | AIRTRIP (PMID 27825009) — anakinra prevented recurrence in a randomised withdrawal trial; RHAPSODY (rilonacept) showed rapid response and reduced recurrence |
| 5. Other immunosuppression | Intravenous immunoglobulin (IVIG) — limited evidence; considered for autoimmune or refractory cases. Cyclosporin, azathioprine — rarely, for truly refractory disease | Case series only |
| 6. Pericardiectomy | Last resort for truly refractory, incessant cases unresponsive to all medical therapy; performed at specialist centres | Rare; reserved for failure of maximal medical therapy |
Modern paradigm: The goal in recurrent pericarditis is steroid-free remission. Each escalation should move toward IL-1 blockade rather than higher steroid doses. Anakinra and rilonacept have transformed the management of colchicine-resistant, steroid-dependent recurrent pericarditis — patients who previously cycled through years of steroids (with all the attendant toxicity) now achieve remission with targeted IL-1 blockade. [1]
Special situations
Post-MI pericarditis and Dressler syndrome
Two distinct entities follow myocardial infarction:
- Early pericarditis (days 1–3 post-MI) — direct transmural inflammation; clinically a transient rub; usually benign. Continue treating the MI. Do not give steroids or high-dose NSAIDs in the acute phase (they impair scar formation and increase rupture risk) — use aspirin at moderate dose if symptomatic.
- Dressler syndrome (weeks to months post-MI) — immune-mediated pericarditis with fever, pleuritic chest pain, raised inflammatory markers, and often a pericardial (and pleural) effusion. Treat with aspirin (high dose) or NSAIDs plus colchicine; steroids only if NSAIDs fail or are contraindicated. The incidence has fallen dramatically since the era of reperfusion (PCI reduces infarct size and the antigenic stimulus). [1]
Post-cardiac surgery (post-pericardiotomy syndrome)
Develops in 15–30% of patients after cardiac surgery (CABG, valve surgery). Presents days to weeks postoperatively with fever, pleuritic chest pain, pericardial rub, and effusion. Treat with NSAIDs or aspirin plus colchicine. A large multi-centre trial (COPPS-2) showed that prophylactic colchicine started 48–72 hours post-surgery halves the incidence of post-pericardiotomy syndrome. [1]
Uraemic pericarditis
Occurs in 6–10% of patients with advanced kidney failure (urea over 15 mmol/L or eGFR under 10), typically before or early in dialysis. The treatment is intensification of dialysis — this resolves the pericarditis. A large effusion with tamponade requires pericardiocentesis or a surgical pericardial window. NSAIDs and colchicine have a limited role; steroids are reserved for dialysis-resistant cases. [1]
Tuberculous pericarditis
Common in TB-endemic regions and a real consideration in ANZ migrant populations. Presents with insidious fever, night sweats, weight loss, and a large effusion (often progressing to tamponade or constriction). Diagnosis rests on pericardial fluid analysis (ADA over 40 U/L is highly sensitive; AFB culture and TB PCR) and pericardial biopsy. Treatment is standard 6-month anti-TB therapy. Adjunctive corticosteroids (prednisone 60 mg/day tapering over 12 weeks) reduce the risk of progression to constriction and reduce mortality — this is one of the few situations where steroids are strongly evidence-based in pericardial disease. [1]
Exam synthesis — high-yield discriminators
| Question | Discriminator |
|---|---|
| Pericarditis or STEMI? | Diffuse concave ST elevation + PR depression = pericarditis; localised convex ST elevation + reciprocal changes = STEMI |
| Steroids first-line for viral pericarditis? | No — NSAID + colchicine. Steroids reserved for NSAID failure, autoimmune, uraemic |
| What is the emergency treatment of tamponade? | Emergency pericardiocentesis — not fluid, not pressors |
| Constriction or restriction on echo? | Preserved medial e' = constriction; reduced e' = restriction. Septal bounce and pericardial thickening support constriction |
| What is the JVP morphology of constriction? | Prominent X and Y descent; Kussmaul sign (rises on inspiration) |
| Treatment of refractory recurrent pericarditis? | Anakinra (IL-1 blockade) — not more steroids |
| Does TB pericarditis get steroids? | Yes — adjunctive steroids reduce constriction and mortality in confirmed TB pericarditis |
| What is the most common cause of large effusion in a cancer patient? | Malignant involvement (lung, breast, lymphoma) |
Long-term outcomes and follow-up
- Acute viral pericarditis — excellent prognosis; over 80% have no recurrence; full recovery expected. The 15–30% who recur need colchicine optimisation and evaluation for non-viral causes.
- Cardiac tamponade — prognosis depends on the underlying cause; malignant effusions carry a poor prognosis (median survival months); traumatic and iatrogenic tamponade do well if drained promptly.
- Constrictive pericarditis — without pericardiectomy, progressive heart failure and death. With early pericardiectomy, 5-year survival is 70–80%; late or calcific constriction, irradiated patients, and those with myocardial involvement do worse.
- Recurrent pericarditis — modern IL-1 blockade has transformed outcomes; most patients achieve steroid-free remission. Quality of life is often markedly impaired during active disease. [1]
Regional guideline anchoring
- ESC 2015 Guidelines for the diagnosis and management of pericardial diseases (Adler et al, PMID 26320112) — the primary international guideline, still widely cited. Note: the ESC released updated 2025 guidelines on myocarditis and pericarditis.
- JACC State-of-the-Art Review 2020 (Imazio et al, PMID 31918837) — modernises the ESC approach; emphasises the steroid-sparing, IL-1-blockade paradigm for recurrent disease.
- ACC Expert Consensus on Pericarditis (2025) — the most recent US consensus; reinforces colchicine as first-line adjunct and IL-1 blockade for refractory cases.
- ANZ practice — follows ESC and ACC recommendations; Heart Foundation of Australia defers to international guidelines. Colchicine 0.5 mg (ANZ) or 0.6 mg (US) depending on regional formulation; anakinra and rilonacept accessed via specialist cardiology with funding via Pharmaceutical Benefits Scheme (PBS) authority or compassionate access pathways. [1]
Summary of verified references
- Adler Y, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J 2015;36(29):2921-64. PMID 26320112.
- Imazio M, et al. A randomized trial of colchicine for acute pericarditis (ICAP). N Engl J Med 2013;369:1522-8. PMID 23992557.
- Brucato A, et al. Effect of anakinra on recurrent pericarditis (AIRTRIP). JAMA 2016;316(18):1906-12. PMID 27825009.
- Imazio M, et al. Colchicine for multiple recurrences of pericarditis (CORP-2). Lancet 2014;383(9936):2242-8. PMID 24694983.
- Imazio M, et al. Management of acute and recurrent pericarditis: JACC State-of-the-Art Review. J Am Coll Cardiol 2020;75(1):76-92. PMID 31918837.
- Imazio M, et al. Colchicine in addition to conventional therapy for acute pericarditis (COPE). Circulation 2005;112(13):2012-6. PMID 16186437. [1]
ESC 2015 Pericardial Guidelines; JACC State-of-the-Art Review 2020; ACC Expert Consensus on Pericarditis 2025. [1]
References
- [1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J, 2015.PMID 26320112
- [2]Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for acute pericarditis N Engl J Med, 2013.PMID 23992557
- [3]Brucato A, Imazio M, Pauletto R, et al. Effect of Anakinra on Recurrent Pericarditis Among Patients With Colchicine Resistance and Corticosteroid Dependence: The AIRTRIP Randomized Clinical Trial JAMA, 2016.PMID 27825009
- [4]Imazio M, Belli R, Brucato A, et al. Efficacy and safety of colchicine for treatment of multiple recurrences of pericarditis (CORP-2): a multicentre, double-blind, placebo-controlled, randomised trial Lancet, 2014.PMID 24694983
- [5]Imazio M, Brucato A, Spodick DH, Adler Y. Management of Acute and Recurrent Pericarditis: JACC State-of-the-Art Review J Am Coll Cardiol, 2020.PMID 31918837
- [6]Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial Circulation, 2005.PMID 16186437