Phys · cardiovascular
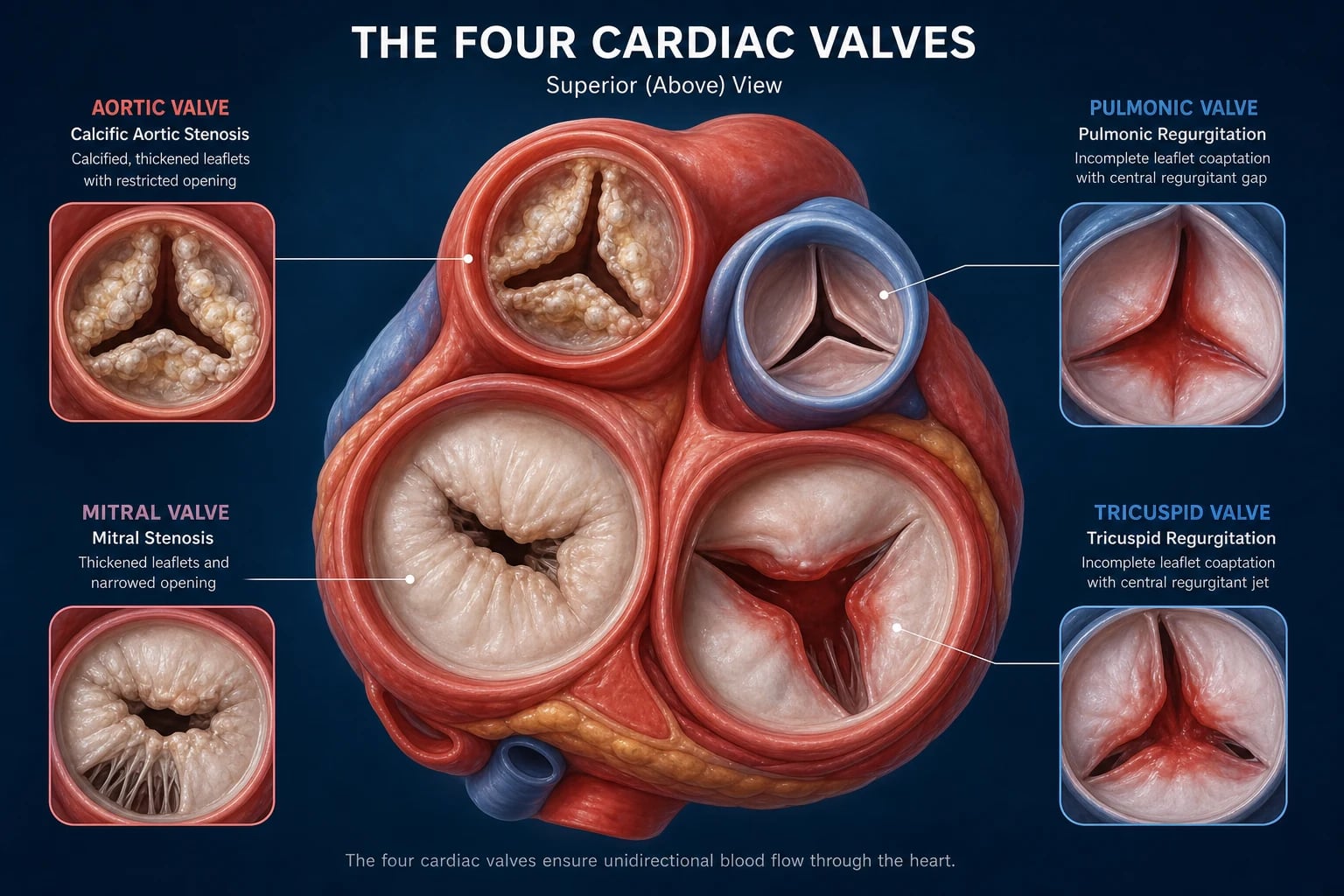
Valvular Heart Disease
Also known as valvular heart disease · aortic stenosis · aortic regurgitation · mitral stenosis · mitral regurgitation · tricuspid regurgitation · prosthetic valve · mechanical valve · bioprosthetic valve · TAVI · TAVR · MitraClip · TEER · balloon mitral valvotomy
Consultant-physician-depth guide to the four cardiac valves — aortic stenosis, aortic regurgitation, mitral stenosis, mitral regurgitation, tricuspid regurgitation, and prosthetic valves — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Valvular Heart Disease
The answer first
Valvular heart disease is driven by one of two questions: is there enough haemodynamic burden to warrant intervention, and if so, repair or replace, surgical or transcatheter? The two pivotal principles that govern everything below: [1]
- For stenotic left-sided valves, symptoms are the trigger. Once a patient with severe aortic stenosis or severe mitral stenosis develops symptoms, the risk of sudden death climbs steeply and intervention is indicated. Waiting is harmful.
- For regurgitant lesions, intervene before irreversible ventricular damage. Surgery in chronic aortic and mitral regurgitation is timed on symptoms and on echocardiographic thresholds of ventricular size and function — the goal is to operate before the ventricle has decompensated, because operating on a depressed ejection fraction carries much higher operative mortality and worse long-term outcome. [1]
The modern framework is the ACC/AHA stage classification — A (at risk), B (progressive), C (asymptomatic severe), D (symptomatic severe) — applied to every valve. It tells you the patient's position on the surveillance-to-intervention timeline at a glance. [1]
DWE high-yield: If you remember one sentence for valvular disease, remember this — the symptomatic patient with severe stenosis needs valve intervention, not medical therapy. No drug slows the progression of calcific aortic stenosis. [1]
Murmur framework
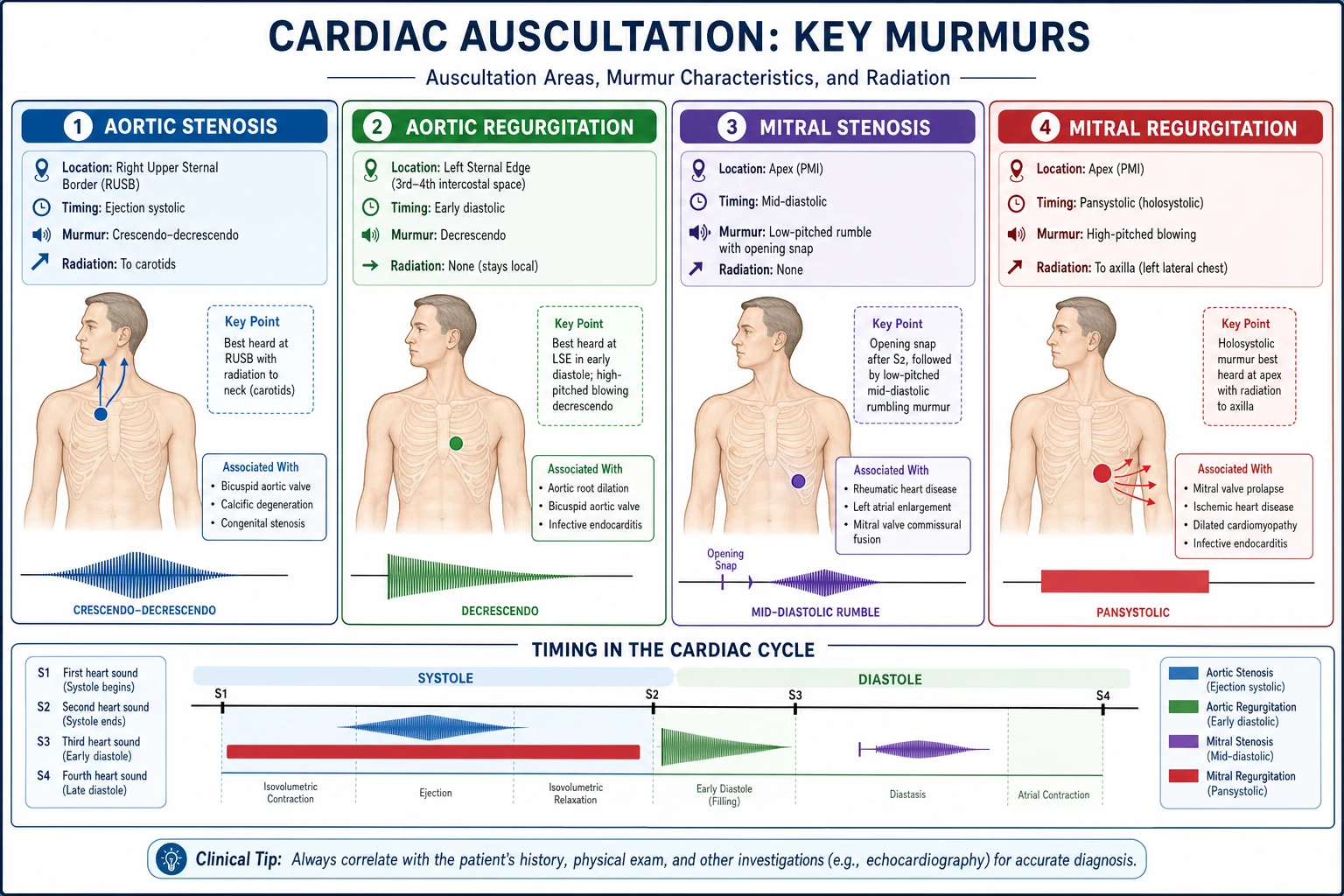
Classify every murmur by timing first, then site, then character. This is the single most reliable bedside discriminator and a PACES examiner expects it. [1]
| Timing | Murmur | Site | Radiation | Character | Modifiers |
|---|---|---|---|---|---|
| Ejection systolic | Aortic stenosis | Upper right sternal edge | To carotids | Crescendo–decrescendo | Slower-rising pulse; soft S2 |
| Pansystolic | Mitral regurgitation | Apex | To axilla | Blowing | Louder on expiration; soft S1 |
| Pansystolic | Tricuspid regurgitation | Lower left sternal edge | To right sternal edge / liver | Blowing | Louder on inspiration (Carvallo); prominent V wave |
| Pansystolic | VSD | Lower left sternal edge | None (localised) | Harsh | Thrill common |
| Early diastolic | Aortic regurgitation | Left sternal edge (3rd ICS) | None | High-pitched, decrescendo | Heard in left lateral position, breath held in expiration; wide pulse pressure |
| Mid-diastolic | Mitral stenosis | Apex | None (localised) | Low-pitched rumble; opening snap | Loud S1; bell of stethoscope, left lateral position |
DCE short-case trap: Examiners distinguish candidates by whether they use the dynamic manoeuvres. MR and VSD get louder on handgrip (afterload up) and softer on standing/amyl nitrate (preload/afterload down). The AS murmur does the opposite — softer with handgrip, louder on squatting-to-standing is less reliable; louder with passive leg raise (preload up). MVP is the classic that moves: click-murmur earlier and longer on standing. [1]
Aortic stenosis
Definition and why it matters
Aortic stenosis (AS) is obstruction to left ventricular outflow. In adults the three causes are calcific disease of a trileaflet valve (most common in the developed world, an active inflammatory/osteogenic process, not passive wear), bicuspid aortic valve (congenital, presents 1–2 decades earlier, ~1–2% of the population), and rheumatic (rare in isolation, usually with mitral involvement). The genetic insight worth knowing: NOTCH1 mutations cause both bicuspid aortic valve and accelerated calcification by de-repressing the Runx2 osteogenic pathway [10].
AS matters because of its natural history: a long latent phase with a gradually narrowing valve, then a steep mortality cliff once symptoms appear. [1]
Severity grading (echo — memorise the thresholds)
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Peak jet velocity | 2.6–2.9 m/s | 3.0–3.9 m/s | ≥4.0 m/s |
| Mean gradient | — | — | ≥40 mmHg |
| Aortic valve area (AVA) | >1.5 cm² | 1.0–1.5 cm² | ≤1.0 cm² (≤0.6 cm² index) |
| Dimensionless index | — | — | ≤0.25 |
DWE trap — low-flow low-gradient AS. When a patient has reduced LVEF and the AVA looks small but the gradient is low, the severity may be true severe (afterload mismatch) or pseudo-severe (primary LV dysfunction with a valve that opens poorly because flow is low). A dobutamine stress echo resolves it: contractile reserve (≥20% stroke volume rise) with gradient rising to severe confirms true severe AS. No reserve predicts poor surgical outcome. There is also paradoxical low-flow low-gradient AS — preserved EF but low stroke volume from small hypertrophied ventricles (often elderly women) — which carries a poor prognosis and often warrants intervention. [1]
Clinical presentation
The classic symptom triad defines the natural-history inflection point:
- Angina (demand ischaemia from LV hypertrophy; 50% 5-year mortality without surgery)
- Syncope (typically exertional, from fixed cardiac output + vasodepressor reflex; 50% 3-year mortality)
- Heart failure (diastolic then systolic; 50% 2-year mortality) [1]
Examination: slow-rising, low-volume pulse (pulsus parvus et tardus); narrow pulse pressure; sustained, non-displaced apex (concentric LVH, not dilatation); ejection systolic murmur at the upper right sternal edge radiating to the carotids; soft or absent A2 (paradoxical splitting if severe); ejection click (only in bicuspid, not calcific). The murmur gets later-peaking (closer to S2) as severity increases — a high-yield bedside sign. [1]
When to intervene
Intervention (AVR) is indicated for:
- Symptomatic severe AS (Stage D) — any of angina, syncope or exertional dyspnoea. This is a class I indication and carries a clear survival benefit. Do not delay for medical optimisation.
- Asymptomatic severe AS (Stage C) with LVEF <60% (the only objective asymptomatic trigger).
- Asymptomatic very severe AS (peak velocity ≥5 m/s or mean gradient ≥60 mmHg) — low surgical risk and very low operative mortality. The RECOVERY trial showed that early AVR in very severe asymptomatic AS reduced the composite of operative mortality or cardiovascular death at long-term follow-up [9].
- Severe AS when other cardiac surgery is planned (CABG, mitral surgery).
- Consider (class IIa) asymptomatic severe AS with an abnormal exercise test, or rapid progression (>0.3 m/s/year).
DWE trap: The asymptomatic AS question is an exam favourite. The key is to actively look for symptoms with a symptom-limited exercise test (if the patient can exercise and has no symptoms). A positive test (symptoms, fall in blood pressure, or >2 mm ST depression) reclassifies them as symptomatic — operate. A negative test supports continued surveillance. [1]
SAVR vs TAVI/TAVR
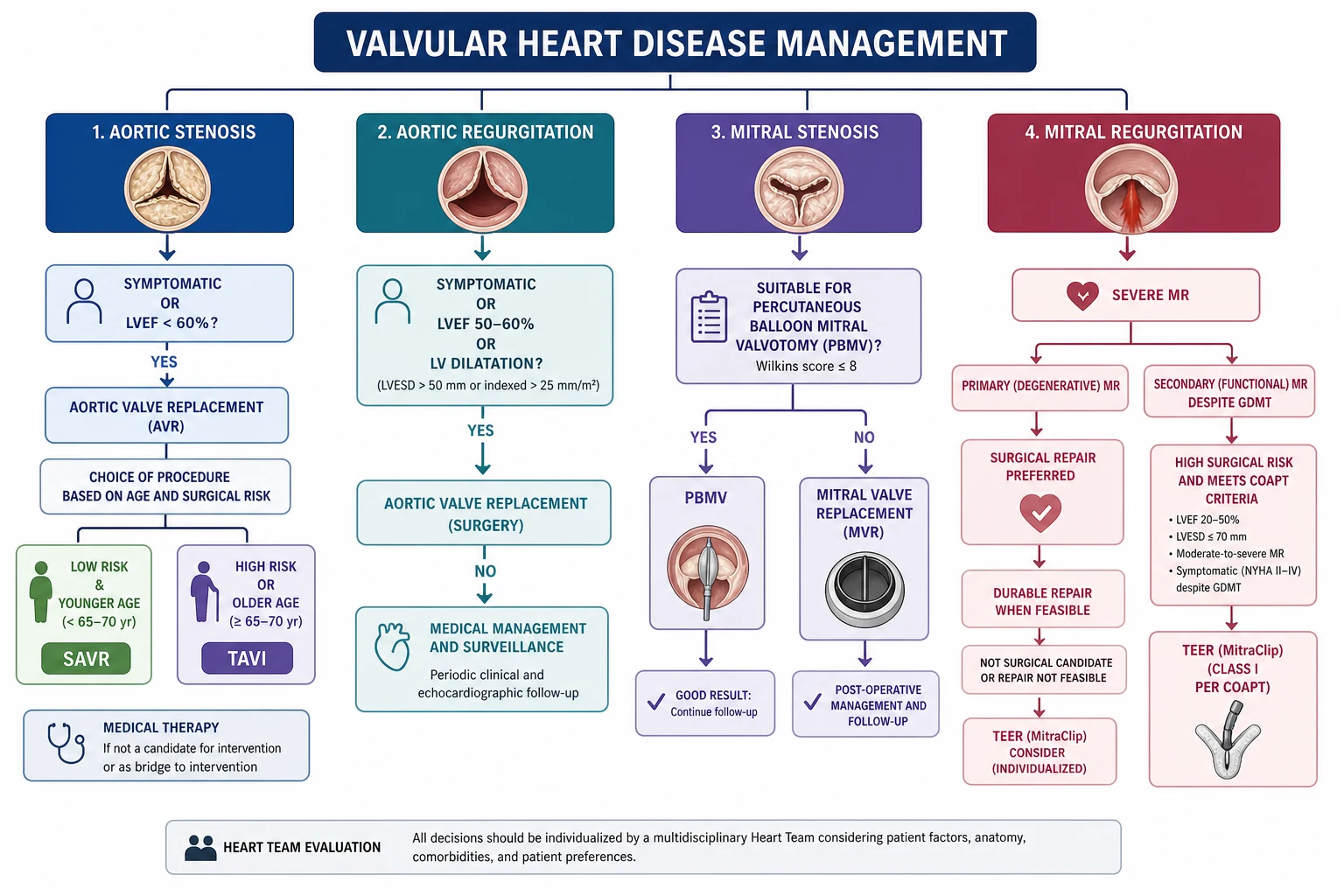
The decision integrates surgical risk (STS/EuroSCORE, and crucially the "heart team" clinical judgement including frailty, porcelain aorta, chest irradiation, hostile chest), age/life expectancy, and anatomical suitability (annulus size, vascular access, valve calcification). [1]
| Factor | Favours TAVI | Favours SAVR |
|---|---|---|
| Surgical risk | High / prohibitive | Low |
| Age | >75–80 years | <65–70 years |
| Access / anatomy | Suitable femoral access | Complex coronary needing CABG; bicuspid; unfavourable annulus |
| Life expectancy | <10–15 years | >20 years (durability of TAVI unknown at very long follow-up) |
| Comorbidity | Severe COPD, frailty, liver disease | — |
Evidence chain: PARTNER (Cohort B) established that TAVI is superior to medical therapy in patients who cannot undergo surgery [1]. PARTNER 3 showed TAVI with a balloon-expandable valve was non-inferior (and at 1 year superior) to SAVR in low-risk patients at 1 year [2], with 5-year data showing comparable outcomes and valve durability. The CoreValve US High Risk trial showed the self-expanding prosthesis was superior to SAVR in high-risk patients [3]. Current practice: SAVR is preferred in younger low-risk patients (longer durability track record, ability to address concurrent pathology, smaller risk of permanent pacemaker), TAVI in older/higher-risk patients, with the "middle group" (65–80, intermediate risk) discussed by the heart team.
Does medical therapy slow AS? No.
Three landmark trials answered this definitively and negatively: SEAS (simvastatin/ezetimibe) [7] and ASTRONOMER (rosuvastatin) [8] both failed to slow haemodynamic progression of mild-to-moderate AS. Statins are used only when indicated for concomitant coronary disease or hyperlipidaemia — never to delay the valve. There is no licensed disease-modifying therapy for calcific AS.
DWE trap on SEAS: SEAS reported a transient cancer signal that subsequent pooled analyses attributed to chance. Know the trial as the lipid-lowering negative study, and do not reproduce the cancer concern as if it were a confirmed harm. [1]
Bicuspid aortic valve (BAV)
BAV affects ~1–2% of the population (most common congenital cardiac anomaly) and is associated with early-onset AS/AR, aortopathy (ascending aortic aneurysm from intrinsic wall abnormality, not just haemodynamic), and coarctation of the aorta. Surveillance includes the aorta — repair when diameter ≥5.5 cm (≥5.0 cm with risk factors: family history, rapid growth >5 mm/year, planned AVR, uncontrolled hypertension). First-degree relatives of a BAV patient warrant screening echocardiography. [1]
Aortic regurgitation
Mechanism and causes
Aortic regurgitation (AR) results from disease of the valve leaflets (rheumatic, bicuspid, infective endocarditis, connective tissue disease, degenerative) or the aortic root/annulus (hypertension-related dilatation, aortic aneurysm/dissection, Marfan, syphilis, ankylosing spondylitis, giant cell arteritis). The leaflet-vs-root distinction matters because root disease may need aortic repair even with a normal-looking valve. [1]
Chronic vs acute — a critical split
- Chronic AR is well tolerated for decades. Volume overload leads to eccentric LV hypertrophy and dilatation; the ventricle becomes large and compliant. The body compensates with tachycardia (shorter diastole = less regurgitation) and peripheral vasodilatation.
- Acute AR (endocarditis, aortic dissection, trauma) is a catastrophe. The non-compliant, non-dilated LV cannot accommodate the regurgitant volume; LVEDP rises abruptly; forward output falls. The murmur is short or absent and the pulse pressure may be normal — do not be reassured by a "soft" auscultation. Acute severe AR is a surgical emergency and a relative contraindication to intra-aortic balloon pump (it worsens regurgitation). [1]
Clinical signs of chronic AR
- Pulse: large-volume "water-hammer" (collapsing); wide pulse pressure (high systolic, low diastolic). Signs of severity — Corrigan's (visible carotid pulsation), de Musset's (head bobbing), Quincke's (nailbed pulsation), Duroziez's (femoral systolic/diastolic murmur with compression), Traube's (pistol-shot over femorals), Müller's (uvular pulsation).
- Murmur: early diastolic, high-pitched, decrescendo, heard best at the left sternal edge, 3rd intercostal space (Erb's point), with the patient sitting forward, breath held in expiration. A concurrent flow ejection systolic murmur (increased total stroke volume) is common and can mislead toward AS — the wide pulse pressure and diastolic component distinguish AR. An Austin Flint murmur — a low-pitched mid-diastolic rumble at the apex — results from the regurgitant jet impinging on the anterior mitral leaflet; it mimics MS but there is no opening snap and no loud S1. [1]
Echo severity (key thresholds)
Severe AR: jet width/LVOT width ≥65% (or vena contracta ≥0.6 cm), pressure half-time <200 ms, regurgitant volume ≥60 mL/beat, regurgitant fraction ≥50%, and LV dilatation (LV end-diastolic diameter >6.5 cm). [1]
When to intervene (surgery, not TAVI, for native AR)
Surgical AVR (often with root repair) is indicated for:
- Symptomatic severe chronic AR — operate.
- Asymptomatic severe AR with LVEF 50–60% (incipient dysfunction) — class I.
- Asymptomatic severe AR with severe LV dilatation (indexed LVESD ≥25 mm/m² or LVEDD ≥65 mm) — class IIa; the trend matters, serial growth triggers referral.
- Severe AR when other cardiac surgery is planned.
- Moderate AR when other cardiac surgery is planned (concomitant AVR, class IIa). [1]
DWE trap — the LVEF 50–60% asymptomatic patient. This is the most tested asymptomatic indication. Below 50% LVEF the operative risk rises and long-term survival falls, so 50–60% is the sweet spot where early surgery prevents irreversible cardiomyopathy. Do not "watch and wait" once EF is dipping. [1]
There is no disease-modifying drug for chronic AR. Vasodilators (nifedipine, historically) were used to delay surgery in inoperable patients but are not a substitute for appropriately timed surgery; the evidence (nifedipine trials from the 1990s) is now considered superseded by earlier surgical referral. [1]
Mitral stenosis
Mechanism and epidemiology
Mitral stenosis (MS) is almost always rheumatic. Rheumatic carditis follows group A streptococcal pharyngitis; the resulting autoimmune response causes commissural fusion, leaflet thickening and chordal shortening over years. ANZ and UK examiners expect you to recognise MS especially in migrant populations (South Asian, Pacific Islander, African, Middle Eastern), where it remains common. Less common causes: severe mitral annular calcification (elderly, CKD), radiation, congenital, LA myxoma (mimic), and prosthetic valve thrombosis. [1]
The rheumatic mitral valve has a characteristic echo appearance: "hockey-stick" deformity of the anterior leaflet (diastolic doming), commissural fusion, and a fish-mouth orifice. [1]
Severity (memorise)
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Valve area | >1.5 cm² | 1.0–1.5 cm² | ≤1.0 cm² |
| Mean gradient | — | — | ≥10 mmHg (if in sinus rhythm) |
| Pressure half-time | — | — | ≥220 ms |
| Pulmonary artery systolic pressure | — | — | >50 mmHg |
Clinical presentation
MS causes a pressure-overload picture: raised LA pressure → pulmonary venous hypertension → exertional dyspnoea, orthopnoea, haemoptysis, and (if advanced) pulmonary hypertension and right heart failure. Two high-yield complications dominate the exam:
- Atrial fibrillation — very common in MS (the dilated, stressed left atrium is arrhythmogenic). New-onset AF with rapid ventricular response can precipitate acute pulmonary oedema by shortening diastole (MS is a diastolic disease — less filling time means higher LA pressure). Rate control is urgent.
- Thromboembolism — MS carries one of the highest embolic risks even in sinus rhythm; the stroke risk per year in rheumatic MS with AF exceeds that of non-valvular AF. [1]
Examination: malar flush; loud S1 (tense leaflets snapping shut); opening snap (the stenotic leaflets snap open in early diastole — the shorter the A2–OS interval, the more severe the MS, because LA pressure is higher); mid-diastolic rumble at the apex, heard with the bell, patient in the left lateral position, during expiration, especially after a brief exercise (e.g., sit-ups) to raise the heart rate and gradient. With pulmonary hypertension, a parasternal heave, loud P2 and a TR murmur appear. [1]
When to intervene
Intervention is indicated for symptomatic severe MS, or asymptomatic severe MS with pulmonary hypertension (PASP >50 mmHg), or new-onset AF. The intervention choice hinges on the Wilkins score — an echo score (1–4 each for leaflet mobility, thickening, calcification, and subvalvular involvement; total 0–16) that quantifies how favourable the valve is for percutaneous balloon mitral valvotomy (BMV/PMBV). [1]
- Wilkins score ≤8, no LA thrombus, no more than mild MR → balloon mitral valvotomy (BMV), the percutaneous procedure of choice. Excellent results, low complication rate, avoids surgery.
- Unfavourable valve (heavy calcification, Wilkins >8, subvalvular disease, LA thrombus, or significant MR) → surgical mitral valve replacement (or, rarely, open commissurotomy by an experienced surgeon). [1]
Anticoagulation: every MS patient with AF needs warfarin (DOACs have limited evidence in moderate–severe rheumatic MS and most guidelines still prefer warfarin). Even in sinus rhythm, anticoagulation is considered when there is LA thrombus or a prior embolic event. [1]
DWE trap: BMV is for the favourable rheumatic valve. The examiner will give you a heavily calcified, immobile valve (high Wilkins) and ask the best intervention — the answer is surgery (MVR), not BMV, because balloon dilation of a calcified valve produces severe MR. [1]
Mitral regurgitation
Degenerative vs functional — the pivotal distinction
Mitral regurgitation (MR) is divided by mechanism:
- Primary (degenerative) MR — disease of the leaflets themselves: Barlow's disease (bileaflet prolapse, myxomatous, excess tissue), fibroelastic deficiency (thin, prolapsing segment), or rheumatic (post-inflammatory restriction). Repair rate is high in expert hands. The leaflets are structurally abnormal; surgery is the definitive therapy.
- Secondary (functional) MR — structurally normal leaflets that fail to coapt because of LV remodelling: ischaemic (post-MI papillary muscle displacement or LV dilatation) or non-ischaemic (DCM). The MR is a consequence of the cardiomyopathy, so the first treatment is GDMT, CRT and revascularisation, not surgery. [1]
This distinction drives every management decision and is a near-constant exam theme. [1]
Clinical presentation
Chronic MR is volume-overload, well tolerated for years: fatigue, exertional dyspnoea, then overt heart failure. Acute MR (papillary muscle rupture post-MI, chordal rupture, endocarditis) causes sudden pulmonary oedema — the small non-compliant LA cannot accommodate the regurgitant volume, and the murmur may be surprisingly soft or early systolic (rapid equalisation of LA and LV pressure "cuts off" the murmur). [1]
Examination: displaced, hyperdynamic apex (volume overload); soft S1 (incomplete leaflet coaptation); pansystolic murmur at the apex radiating to the axilla, louder on expiration; S3 (not necessarily failure — it reflects the rapid early filling of the volume-loaded ventricle). In MVP, the murmur is preceded by a non-ejection click and is mid-to-late systolic. [1]
Echo quantification (key thresholds)
Severe MR: ERO ≥0.40 cm² (primary) or ≥0.20 cm² (functional, where lower thresholds apply because the regurgitant fraction is haemodynamically significant at smaller orifices), regurgitant volume ≥60 mL, regurgitant fraction ≥50%, large PISA radius, and systolic flow reversal in the pulmonary veins. Always assess mechanism (prolapse vs restriction vs flail) and the potential for repair with TOE. [1]
When to intervene
Primary (degenerative) MR — mitral valve repair is strongly preferred over replacement (preserves subvalvular apparatus, lower mortality, no anticoagulation). Indications:
- Symptomatic severe primary MR with preserved LV function (LVEF >30%) — surgery (repair), class I.
- Asymptomatic severe primary MR with LVEF 30–60% or LVESD ≥40 mm — surgery, class I. (These are the decompensation thresholds.)
- Asymptomatic severe primary MR with preserved LV but high likelihood of durable repair at a primary (high-volume) valve centre, and either new AF or pulmonary hypertension (PASP >50 mmHg) — class IIa. Increasingly, early repair in asymptomatic patients at expert centres is offered (the "watchful waiting" threshold has shifted toward earlier intervention because repair outcomes are now excellent). [1]
Functional MR — first optimise GDMT, CRT and revascularisation. Surgery (restrictive annuloplasty) or transcatheter edge-to-edge repair (TEER) is reserved for persistent severe functional MR despite optimal therapy. [1]
MitraClip / TEER — COAPT vs MITRA-FR
The transcatheter edge-to-edge repair (TEER, "MitraClip") clips the leaflets to reduce MR, modelled on the surgical Alfieri stitch. Two landmark RCTs gave discordant results and the exam expects you to reconcile them: [1]
- EVEREST II compared TEER with surgery in (mostly primary) MR — TEER was safer but less effective at eliminating MR; a reasonable option for high-risk surgical patients with degenerative MR [4].
- MITRA-FR (functional MR) was negative — adding TEER to optimal medical therapy did not reduce death or HF hospitalisation [6].
- COAPT (functional MR) was strongly positive — in carefully selected patients (severe MR, on maximally tolerated GDMT, with proportionate MR — the MR "disproportionate" to a only-moderately-dilated LV), TEER reduced HF hospitalisation and all-cause mortality at 24 months (29.1% vs 46.1% mortality) [5].
The reconciliation: COAPT enrolled patients with proportionate MR (severe MR relative to a less-dilated LV — the valve is the dominant problem), used strict adherence to GDMT, and enrolled more MR severity. MITRA-FR enrolled more disproportionate-to-LV-size patients (the cardiomyopathy dominates) and was neutral. The practical rule: TEER for functional MR helps patients in whom the MR is disproportionate to the LV size and GDMT is truly optimised. It is not a substitute for GDMT. [1]
DWE high-yield contrast: COAPT positive, MITRA-FR negative — same device, opposite result. The discriminator is proportionate vs disproportionate MR (MR severity relative to LV end-diastolic volume). "Proportionate MR" (MR severity matched to LV dilatation — the myopathy dominates) → MITRA-FR-like patient → TEER less likely to help. "Disproportionate MR" (severe MR in a smaller LV — the valve dominates) → COAPT-like patient → TEER helps. [1]
Tricuspid regurgitation
The functional era
Tricuspid regurgitation (TR) is now overwhelmingly functional — annular dilatation and right ventricular remodelling from left-sided heart disease (any cause of pulmonary hypertension: mitral disease, LV failure, pulmonary hypertension), rather than primary leaflet pathology (Ebstein's, carcinoid, rheumatic, endocarditis, pacemaker/ICD lead-induced). Treat the cause and you often improve the TR. [1]
Clinical signs
- Pansystolic murmur at the lower left sternal edge, louder on inspiration (Carvallo's sign — increased venous return to the right heart).
- Prominent V wave in the JVP (the regurgitant systolic wave).
- Pulsatile liver and peripheral oedema (right heart failure).
- Severe TR can produce a right-sided S3 and even a short early diastolic murmur from functional pulmonary regurgitation. [1]
When to intervene
Tricuspid valve annuloplasty (repair) at the time of left-sided surgery (e.g., mitral surgery) is indicated for severe TR or moderate TR with annular dilatation (≥40 mm or ≥21 mm/m²). Isolated tricuspid surgery for severe symptomatic TR is increasingly offered, and transcatheter tricuspid edge-to-edge repair (e.g., TriClip) is an emerging option for high-risk surgical patients. Untreated severe TR carries a poor prognosis independent of pulmonary pressure. [1]
Prosthetic valves
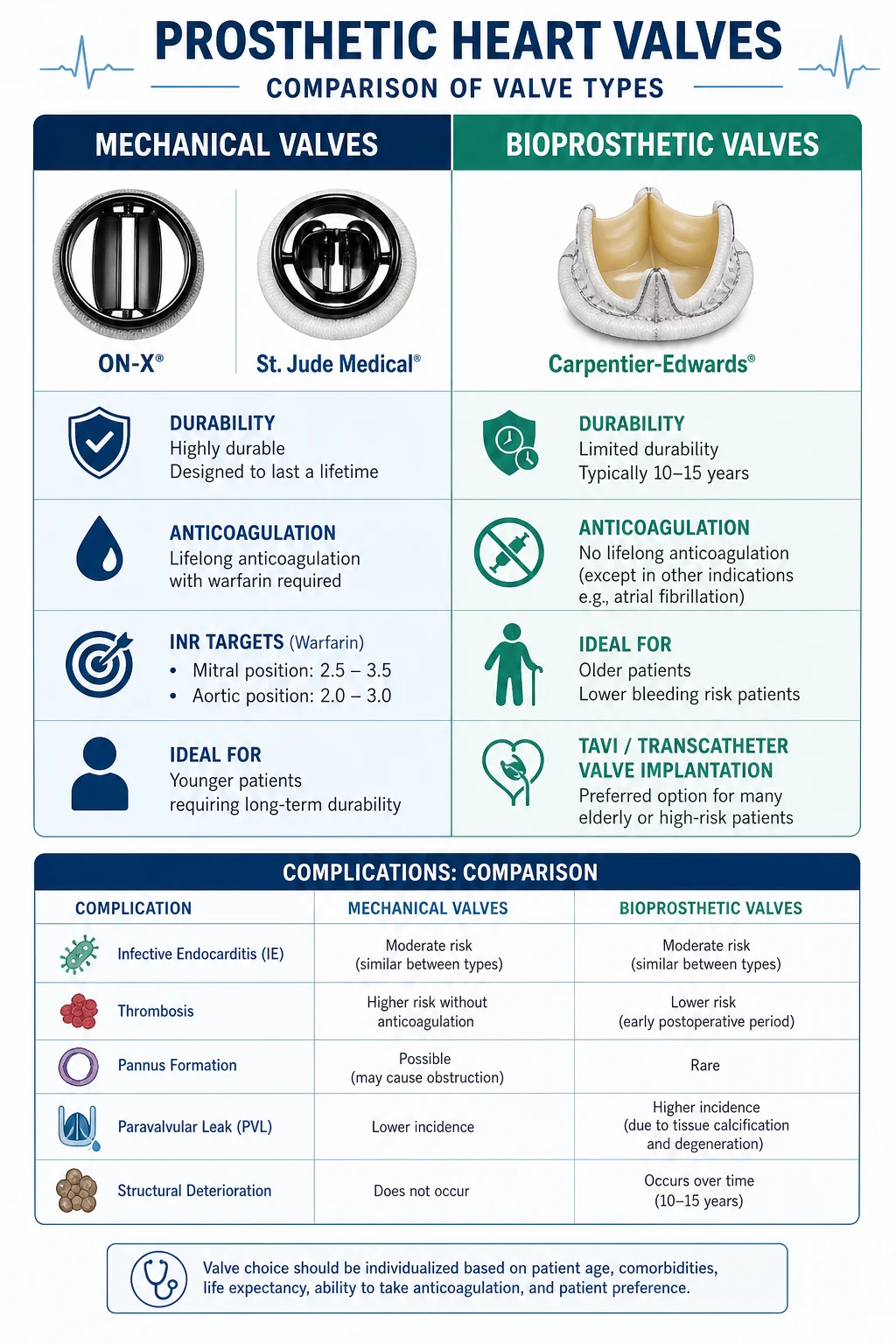
Mechanical vs bioprosthetic — the choice
| Feature | Mechanical (e.g., bileaflet, On-X) | Bioprosthetic (surgical or TAVI) |
|---|---|---|
| Durability | 20–30+ years (low structural failure) | 10–15 years surgical bioprosthesis; TAVI durability being established |
| Anticoagulation | Lifelong warfarin | Usually none after 3–6 months (unless other indication) |
| Reoperation risk | Very low | Higher (structural valve deterioration) |
| Preferred age | <50–65 years (you want durability) | >65–70 years (or any age if anticoagulation unsuitable) |
| Special cases | Women planning pregnancy — bioprosthesis often preferred to avoid warfarin teratogenicity (heparin in pregnancy is burdensome) | Patients with bleeding risk, falls, poor INR access, non-adherence |
The decision is shared, age- and life-expectancy-weighted. A 55-year-old who can safely take warfarin usually gets a mechanical valve (avoid reoperation at 70). An 80-year-old gets a bioprosthesis (limited life expectancy; no need for warfarin). The On-X mechanical aortic valve allows a lower INR target (1.5–2.0) at 3 months — the only mechanical valve with this evidence. [1]
Anticoagulation and INR targets (memorise — exam favourite)
| Valve position/type | INR target |
|---|---|
| Mechanical mitral | 2.5–3.5 (higher — mitral position is more thrombogenic) |
| Mechanical aortic (bileaflet, current generation) | 2.0–3.0 (or 2.5 target) |
| Mechanical aortic, older generation (caged-ball, tilting disc) | 2.5–3.5 |
| On-X mechanical aortic | 1.5–2.0 after 3 months |
| Bioprosthetic (surgical or TAVI) | Aspirin alone (75–100 mg); warfarin INR 2.5 for 3–6 months if risk factors, then aspirin |
| Mechanical + AF | Same as mechanical target (already anticoagulated) |
Add aspirin 75–100 mg to warfarin if there is concomitant atherosclerotic vascular disease or AF (at cost of slightly more bleeding). [1]
Critical DWE rule — DOACs and mechanical valves. DOACs are contraindicated in mechanical valves. The RE-ALIGN trial (dabigatran) showed more thromboembolism and bleeding with dabigatran than warfarin in mechanical valve patients. Never select a DOAC in a mechanical valve patient. Warfarin is the only option. [1]
Complications of prosthetic valves
| Complication | Presentation | Investigation | Management |
|---|---|---|---|
| Structural valve deterioration (SVD) | Late (10–15 yr bioprosthesis): new murmur, dyspnoea, haemolysis | TOE; rising gradients | Redo AVR/MVR (TAVI-in-TAVI/valve-in-valve if high risk) |
| Prosthetic valve thrombosis | Acute dyspnoea, stroke, embolism, muffled prosthetic sounds | TOE (mass on valve, reduced leaflet motion); fluoroscopy (immobile leaflet) — fluoroscopy uniquely shows leaflet motion in mechanical valves | Surgery if obstructive + high-risk; fibrinolysis if surgical risk prohibitive and right-sided or early post-op; UFH + warfarin if non-obstructive thrombus |
| Pannus (fibrous ingrowth) | Late, gradual obstruction; pannus is less thrombus-like on imaging | TOE/CT | Surgical revision |
| Infective endocarditis | Fever, new murmur, emboli, haemodynamic deterioration | TOE (more sensitive than TTE for prosthetic valves); modified Duke criteria | Prolonged IV antibiotics ± surgery (see infective-endocarditis topic) |
| Paravalvular leak | Haemolysis (anaemia, raised LDH), new murmur, heart failure if large | TOE; sometimes cardiac CT | Percutaneous closure device if symptomatic/haemolysis; surgery if large/dehiscent |
| Patient-prosthesis mismatch (PPM)** | High gradients despite a normally functioning valve (prosthesis too small for body size) | Calculate indexed effective orifice area | Prevent by sizing at implantation; medical management if present |
| Haemolysis | Anaemia, raised LDH/reticulocytes, low haptoglobin, dark urine | Bloods; TOE for paravalvular leak | Treat the leak (closure/reoperation) if structural; supportive if mild |
DCE long-case trap — the prosthetic valve patient with anaemia. Always think haemolysis from paravalvular leak or pannus. Send LDH, haptoglobin, reticulocytes and a film, and get a TOE. Do not simply label it iron deficiency without excluding a structural cause. [1]
Suspected prosthetic valve dysfunction — the workup
A prosthetic valve patient with new dyspnoea, stroke, fever or syncope needs: TTE (compare gradients to baseline — a rising gradient suggests obstruction or PPM), TOE (better visualisation of prosthetic regurgitation, vegetations, thrombus, pannus), fluoroscopy (assesses leaflet motion of mechanical valves — a leaflet that does not open fully is thrombosed or obstructed by pannus), and cardiac CT (valvular and aortic anatomy, paravalvular calcification). Baseline post-implant echo is essential so future changes are interpretable. [1]
Infective endocarditis prophylaxis
Who needs it (the narrowed indication)
Guidelines progressively narrowed prophylaxis. Current ACC/AHA and ESC practice restricts antibiotic prophylaxis before dental procedures to patients at highest risk of catastrophic outcome from endocarditis: [1]
- Prosthetic heart valves (mechanical, bioprosthetic, TAVI) or prosthetic material used for valve repair.
- Previous infective endocarditis.
- Certain congenital heart disease: unrepaired cyanotic CHD; completely repaired CHD with prosthetic material in the first 6 months; repaired CHD with residual defect adjacent to prosthetic material.
- Cardiac transplant recipients who develop cardiac valvulopathy (ACC/AHA). [1]
Rheumatic and most other native valve disease are no longer routine prophylaxis indications (the lifetime risk of antibiotic adverse effects and anaphylaxis is considered to outweigh the small absolute risk reduction). [1]
Which procedures (dental, mostly)
- Dental procedures involving manipulation of gingival tissue or the periapical region, or perforation of the oral mucosa — prophylaxis indicated in high-risk patients.
- Respiratory tract procedures — prophylaxis only if treating established infection (e.g., draining an abscess) in a high-risk patient, NOT for routine bronchoscopy or intubation.
- Skin/soft tissue, GI/GU tract — prophylaxis is not routinely recommended even in high-risk patients. Manage established infections with appropriate antibiotics; prophylaxis for procedures like colonoscopy, cystoscopy or TURP is not indicated solely to prevent endocarditis. [1]
Regional delta (high-yield): NICE (UK) historically took the most restrictive position — no antibiotic prophylaxis at all for any patient (2008 CG64), arguing the evidence for benefit was absent and the risks of antibiotics real. NICE has since softened (updated guidance) to allow a clinician-patient discussion about the (uncertain) benefits and risks, and to not routinely offer prophylaxis but to consider it in discussion with high-risk patients. ESC and ACC/AHA continue to recommend prophylaxis for the high-risk groups above. In an ANZ exam, default to the ACC/AHA/ESC position (prophylaxis for prosthetic valves, prior IE, specified CHD) and acknowledge the NICE position as a known regional variation. [1]
The prophylactic regimen (dental procedures)
| Setting | Agent & dose (single, 30–60 min before) |
|---|---|
| Standard (able to take PO) | Amoxicillin 2 g PO |
| Unable to take PO | Ampicillin 2 g IV/IM (or cefazolin/ceftriaxone 1g IV) |
| Penicillin allergy + unable to take PO | Clindamycin 600 mg IV (or vancomycin) |
Routine good oral hygiene and regular dental review are more important than one-off antibiotics for reducing the day-to-day bacteraemia that causes most endocarditis. [1]
Echo assessment of valve severity — summary
Echocardiography (TTE, with TOE when TTE is non-diagnostic or for prosthetic/intra-operative assessment) is the cornerstone. For each valve, integrate multiple parameters — never rely on one: [1]
| Valve | Key severity parameters |
|---|---|
| AS | Peak velocity, mean gradient, AVA, dimensionless index; dobutamine stress for low-flow low-gradient |
| AR | Jet width/LVOT, vena contracta, pressure half-time, regurgitant volume/fraction, LV size |
| MS | Valve area (planimetry, PHT, PISA), mean gradient, PASP; Wilkins score for BMV suitability |
| MR | ERO, regurgitant volume/fraction, PISA, pulmonary vein flow; mechanism (TOE); stress echo for equivocal severity |
| TR | Vena contracta, PISA, jet area/right atrium ratio; annular size; cause (left heart disease vs primary) |
A TOE is required when: TTE is technically difficult; suspected prosthetic dysfunction or endocarditis; assessment of mitral repairability; LA appendage thrombus before cardioversion; and intra-operatively. [1]
When to refer for surgery — the one-page rule
Refer to a heart team / valve clinic when any of these apply: [1]
- Symptoms attributable to severe valve disease (any valve).
- Severe AS with LVEF <60%, very severe AS, or abnormal exercise test (asymptomatic).
- Severe AR with LVEF ≤60% or severe LV dilatation (indexed LVESD ≥25 mm/m²).
- Severe primary MR with LVEF 30–60%, LVESD ≥40 mm, or new AF/pulmonary hypertension.
- Severe MS (valve area ≤1.0 cm²) with symptoms or PASP >50 mmHg or new AF.
- Severe TR that is symptomatic, or at the time of left-sided surgery.
- Any prosthetic valve with new dysfunction, fever suggestive of endocarditis, or haemolysis. [1]
The heart team (cardiology, cardiac surgery, imaging, anaesthesia) integrates surgical risk, anatomy, comorbidity and patient preference to recommend SAVR vs TAVI, repair vs replacement, and the timing of intervention. [1]
Comorbidity and pregnancy (high-yield)
- CKD / frailty / COPD shift the SAVR–TAVI balance toward TAVI and raise surgical risk scoring.
- Coronary disease is common alongside AS; concomitant CABG at SAVR is standard for significant coronary lesions. PCI can be staged around TAVI.
- Pregnancy in a mechanical-valve patient is high-risk and needs planned management: warfarin is teratogenic (weeks 6–12) but better at preventing valve thrombosis; heparin is safer for the fetus but less effective for the mother. Most protocols use dose-adjusted LMWH/UFH in the first trimester and around delivery, warfarin mid-pregnancy, with strict anti-Xa monitoring. A bioprosthesis is often preferred in women planning pregnancy to avoid this dilemma.
- AF complicating any valve disease needs anticoagulation per the valve type (warfarin for mechanical and severe rheumatic MS; DOAC acceptable for non-valvular/non-rheumatic contexts). [1]
DCE long-case approach
Opening statement (SASPOP)
"Mr Nguyen is a 78-year-old Vietnamese-born retired farmer presenting with three months of exertional chest tightness and two episodes of near-syncope on walking uphill, on a background of hypertension, type 2 diabetes, stage 3 CKD (eGFR 42) and permanent atrial fibrillation. [1]
His main problems are:
- Severe symptomatic aortic stenosis (mean gradient 52 mmHg, AVA 0.7 cm², LVEF 55%) — the primary problem requiring intervention
- Moderate functional MR and TR from LV/LA dilatation
- CKD stage 3a and diabetes — influence choice of contrast and periprocedural management
- Permanent AF — already anticoagulated
- Frailty and reduced functional capacity — influence SAVR vs TAVI decision
- Social: lives alone, limited family support, end-of-life values to clarify." [1]
Integrated management plan
Present in domains:
- Confirm severity and exclude mimics: TTE (already done); consider TOE if MR severity uncertain; CT aortogram and annulus sizing for TAVI planning; coronary angiography (or CT coronary if TAVI route chosen) to exclude concurrent CAD.
- Intervention decision: the heart team. STS-predicted mortality ~6%, frailty score elevated, hostile chest absent, femoral access adequate. Recommend TAVI (transfemoral, self-expanding or balloon-expandable) given age, frailty, CKD and comorbidity.
- Periprocedural: optimise diabetes and renal function; minimise contrast; continue anticoagulation planning (bridge per valve team); pre-procedure pacing assessment (TAVI conduction block risk).
- Comorbidity: GDMT for the functional MR/TR is largely addressed by treating the AS (afterload reduction). Continue antihypertensives and diabetes therapy.
- Follow-up and surveillance: post-TAVI echo baseline; lifelong surveillance for conduction disease (15–20% pacemaker risk), valve function and endocarditis prophylaxis education.
- Communication and shared decision-making: explain SAVR vs TAVI trade-offs (recovery time, pacemaker risk, durability uncertainty); clarify goals of care given frailty; advance care planning. [1]
DCE examiner probing questions you must anticipate:
- "Why TAVI rather than surgery in this man?" → Age, frailty, CKD, comorbidity; SAVR durability advantage less relevant at 78 with limited life expectancy; TAVI non-inferiority/superiority in intermediate-to-high risk.
- "What is his risk of needing a pacemaker?" → ~15–20% with self-expanding valves, lower with balloon-expandable; pre-existing RBBB raises risk.
- "Does he need anticoagulation after TAVI?" → 3–6 months of anticoagulation/antiplatelet therapy per protocol (often aspirin + clopidogrel then aspirin alone; some centres use warfarin briefly); he is already on anticoagulation for AF. [1]
DCE short-case approach: cardiovascular examination (murmur)
Instruction: "Examine this patient's cardiovascular system." [1]
Systematic routine (the murmurs station)
- End of bed: breathless, malar flush (MS), cachexia, skeletal features (Marfan → AR).
- Hands: splinter haemorrhages/Osler nodes (IE), clubbing (cyanotic CHD, IE), janeway lesions. Pulse: rate/rhythm (AF in MS/MR), character — collapsing (AR), slow-rising (AS), alternans (severe LVF).
- Blood pressure: narrow pulse pressure (AS), wide pulse pressure (AR — the high-yield discriminator).
- Face: malar flush (MS), high-arched palate, lens dislocation (Marfan).
- Neck: JVP (V wave in TR; elevated in right heart failure), carotid pulse character (pulsus parvus et tardus in AS; bounding in AR; carotid shudder/thrill in severe AS).
- Præcordium: apex site and character — displaced and hyperdynamic (volume overload: AR, MR), sustained and non-displaced (pressure overload: AS), parasternal heave (RV pressure overload — MS with pulmonary hypertension, TR).
- Auscultation — the heart of the exam. Listen systematically at: apex, lower left sternal edge (TR, VSD, AR), upper left sternal edge (pulmonary area), upper right sternal edge (aortic area — AS), and the back with the patient sitting forward for AR (left sternal edge in expiration). Always use dynamic manoeuvres in a murmur: inspiration (TR louder), expiration/holding breath (AR louder), handgrip (MR, AR louder), Valsalva/standing (MVP click earlier; HOCM murmur louder — the HOCM discriminator).
- Back and abdomen: basal crackles, sacral oedema, pulsatile liver (TR). [1]
Presentation template (aortic stenosis)
"I examined Mrs Patel's cardiovascular system. She is comfortable at rest at 45 degrees. The pulse is regular at 76, small in volume and slow-rising. The blood pressure is 120/80, with a narrow pulse pressure. The carotid pulse is delayed and weak, with a palpable thrill. [1]
The apex beat is in the 5th intercostal space, mid-clavicular line, and is sustained in character. There is no parasternal heave. On auscultation the first heart sound is normal and the second heart sound is soft, with paradoxical splitting. There is an ejection systolic murmur at the upper right sternal edge radiating to the carotids, peaking late in systole, with a palpable thrill. There is no diastolic murmur. The lungs are clear and there is no peripheral oedema. [1]
These findings are consistent with severe aortic stenosis. I would confirm with echocardiography and assess for symptoms to determine the timing of intervention." [1]
Key DWE MCQ patterns
- Symptomatic severe AS → AVR (not a medical option). The correct answer is never "start a statin" or "optimise medical therapy."
- Asymptomatic severe AS with LVEF 55% → AVR (the LVEF <60% trigger).
- Mechanical valve + new AF → warfarin (not a DOAC). DOACs are contraindicated in mechanical valves.
- Rheumatic MS with LA thrombus or AF → warfarin (not DOAC).
- Favourable rheumatic MS (Wilkins ≤8) → balloon mitral valvotomy; heavily calcified (Wilkins >8) → MVR.
- Functional MR after optimised GDMT with proportionate MR → TEER may help (COAPT-like); disproportionate MR (myopathy-dominated, MITRA-FR-like) → continue GDMT.
- Prophylaxis before dental work in a prosthetic valve → amoxicillin 2 g PO; clindamycin if penicillin-allergic. [1]8. Acute severe AR in endocarditis → urgent surgery; the absence of a loud murmur does not exclude it.
- Low-flow low-gradient AS with reduced EF → dobutamine stress echo to differentiate true vs pseudo-severe.
- Prosthetic valve + haemolysis + anaemia → paravalvular leak; send LDH/haptoglobin and get TOE. [1]
References
[1] PARTNER (Leon 2010) — TAVI vs medical therapy in inoperable severe AS. [2] PARTNER 3 (Mack 2019) — balloon-expandable TAVI vs SAVR in low-risk AS. [3] CoreValve US High Risk (Adams 2014) — self-expanding TAVI superior to SAVR in high-risk AS. [4] EVEREST II (Feldman 2011) — MitraClip vs surgery in (mostly primary) MR. [5] COAPT (Stone 2018) — MitraClip positive in proportionate functional MR on optimal GDMT. [6] MITRA-FR (Obadia 2018) — MitraClip negative in disproportionate functional MR. [7] SEAS (Rossebø 2008) — ezetimibe/simvastatin does not slow AS progression. [8] ASTRONOMER (Chan 2010) — rosuvastatin does not slow AS progression. [9] RECOVERY (Køber 2020) — early AVR in very severe asymptomatic AS reduces cardiovascular events. [10] Garg et al. (Nature 2005) — NOTCH1 mutations cause bicuspid aortic valve and calcific valve disease.
ACC/AHA Guideline on the Management of Patients With Valvular Heart Disease (2020); ESC/EACTS VHD Guidelines (2021); NICE CG200 (update) on endocarditis prophylaxis; NHFA/CSANZ guidance. [1]
References
- [1]Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery N Engl J Med, 2010.PMID 20961243
- [2]Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients N Engl J Med, 2019.PMID 30883058
- [3]Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis N Engl J Med, 2014.PMID 24678937
- [4]Feldman T, Foster E, Glower DD, et al. Percutaneous repair or surgery for mitral regurgitation N Engl J Med, 2011.PMID 21463154
- [5]Stone GW, Lindenfeld J, Abraham WT, et al. Transcatheter Mitral-Valve Repair in Patients with Heart Failure N Engl J Med, 2018.PMID 30280640
- [6]Obadia JF, Messika-Zeitoun D, Leurent G, et al. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation N Engl J Med, 2018.PMID 30145927
- [7]Rossebø AB, Pedersen TR, Boman K, et al. Intensive lipid lowering with simvastatin and ezetimibe in aortic stenosis N Engl J Med, 2008.PMID 18765433
- [8]Chan KL, Teo K, Dumesnil JG, et al. Effect of Lipid lowering with rosuvastatin on progression of aortic stenosis: results of the aortic stenosis progression observation: measuring effects of rosuvastatin (ASTRONOMER) trial Circulation, 2010.PMID 20048204
- [9]Kang DH, Park SJ, Lee SA, et al. Early Surgery or Conservative Care for Asymptomatic Aortic Stenosis N Engl J Med, 2020.PMID 31733181
- [10]Garg V, Muth AN, Ransom JF, et al. Mutations in NOTCH1 cause aortic valve disease Nature, 2005.PMID 16025100