Phys · dermatological
Cutaneous Manifestations of Systemic Disease
Also known as cutaneous manifestations of systemic disease · skin signs of internal disease · paraneoplastic dermatology · dermatomyositis · acanthosis nigricans · necrolytic migratory erythema · glucagonoma syndrome · calciphylaxis · calcific uremic arteriolopathy · dermatitis herpetiformis · sign of Leser-Trelat · Trousseau syndrome · migratory thrombophlebitis · Sweet syndrome · acute febrile neutrophilic dermatosis · pyoderma gangrenosum · erythema nodosum · erythema chronicum migrans · nephrogenic systemic fibrosis · pretibial myxoedema
Consultant-physician-depth guide to the skin as a window to systemic disease — a system-by-system framework covering endocrine (acanthosis nigricans, necrolytic migratory erythema of glucagonoma, pretibial myxoedema, diabetic dermopathy), rheumatological (malar rash of SLE, Gottron papules and heliotrope rash of dermatomyositis, sclerodactyly, palpable purpura of vasculitis, erythema nodosum, pyoderma gangrenosum), gastrointestinal (dermatitis herpetiformis and coeliac disease, pyostomatitis vegetans), renal (calciphylaxis, nephrogenic systemic fibrosis), hepatic (spider naevi, palmar erythema), haematological (Sweet syndrome and AML, leukaemia cutis), paraneoplastic (dermatomyositis, malignant acanthosis nigricans, sign of Leser-Trelat, Trousseau syndrome), infectious (erythema chronicum migrans, secondary syphilis) and nutritional (scurvy, pellagra, acrodermatitis enteropathica) clues. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Cutaneous Manifestations of Systemic Disease

The answer first
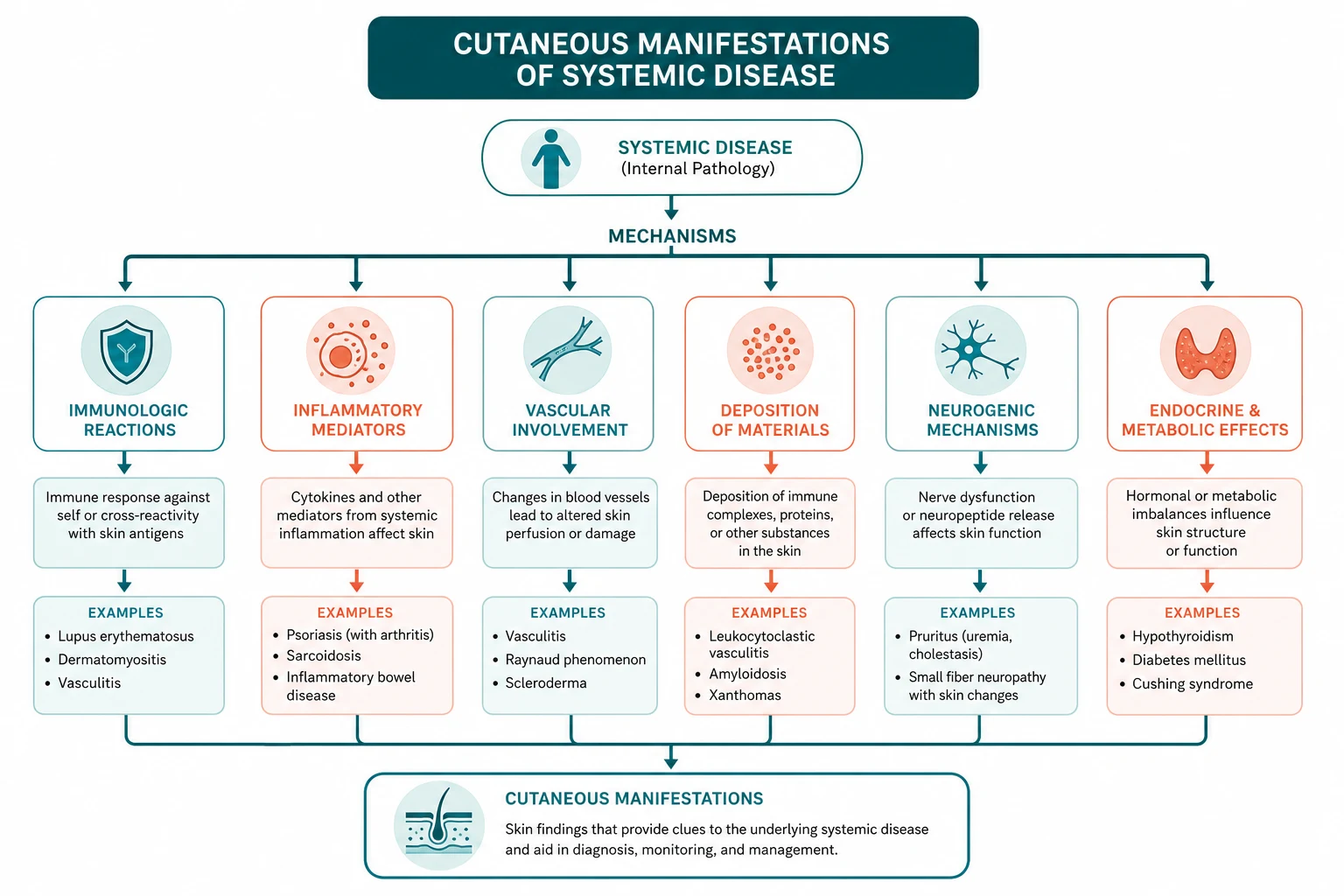
The skin is a window to internal disease. A single recognised lesion can collapse a differential list from dozens of conditions to one — Gottron papules to dermatomyositis, grouped vesicles on the elbows to coeliac disease, an expanding annular lesion after a tick bite to Lyme disease, painful purpuric plaques in a dialysis patient to calciphylaxis. The discipline of cutaneous manifestations of systemic disease is built on this principle: pattern recognition first, then targeted confirmation. [1]
Three ideas frame everything on this page: [1]
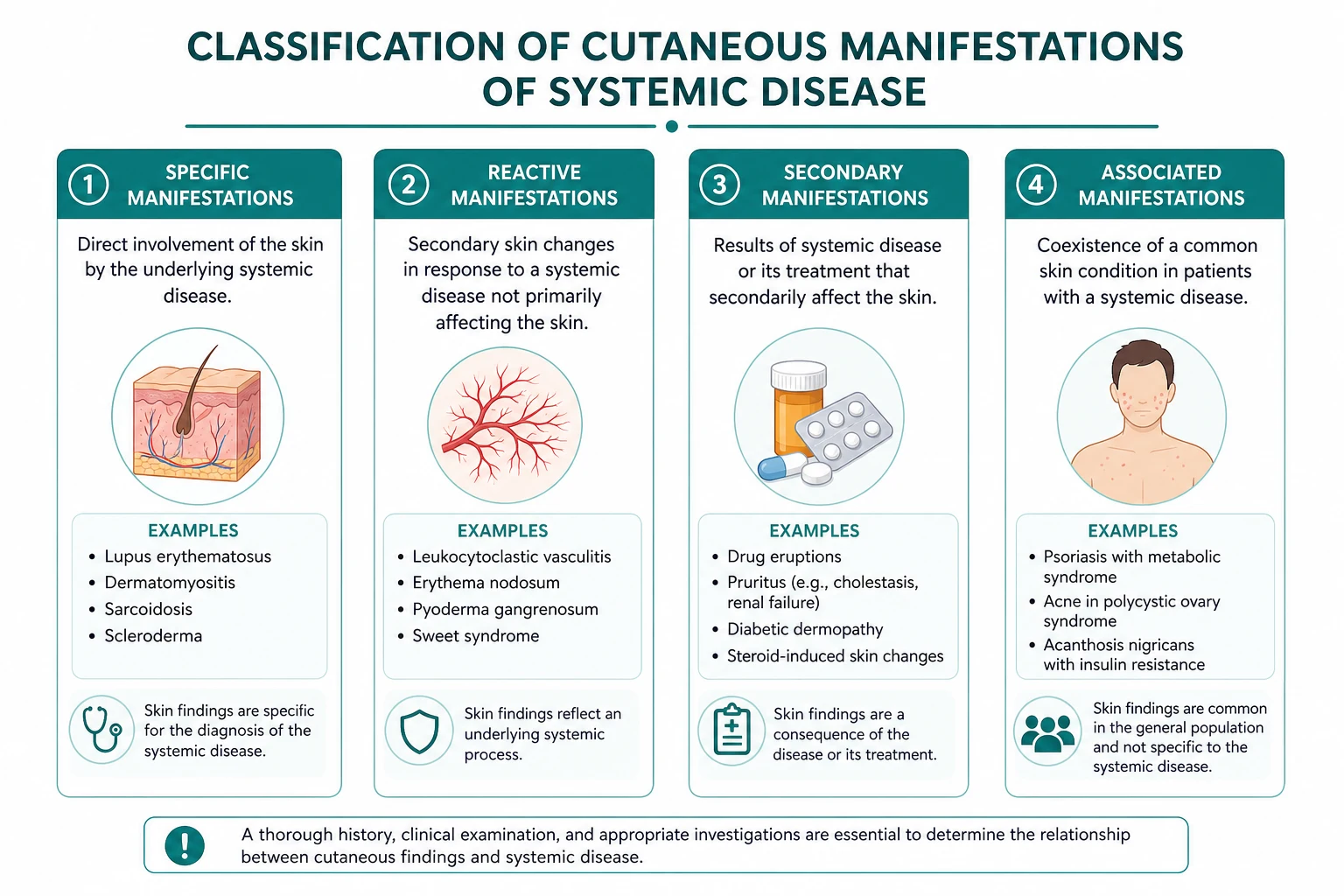
-
Recognise the specific lesion, then ask what system it signals. Acanthosis nigricans signals insulin resistance or a GI malignancy; necrolytic migratory erythema signals glucagonoma; palpable purpura signals small-vessel vasculitis; erythema nodosum signals sarcoidosis, IBD, streptococcal infection or a drug reaction; calciphylaxis signals advanced CKD with disordered calcium-phosphate metabolism. Each lesion carries a short, high-yield list of systemic associations — learn the list and you have the answer. [1]
-
A paraneoplastic skin sign often precedes the diagnosis of the underlying cancer. Adult-onset dermatomyositis, malignant acanthosis nigricans with tripe palms, the sign of Leser-Trelat, Trousseau migratory thrombophlebitis, necrolytic migratory erythema and Sweet syndrome can all be the first manifestation of an otherwise occult malignancy. Recognising the cutaneous marker is the event that triggers the cancer diagnosis — this is the highest-stakes application of dermatology in physician medicine [8] [13].
-
Some skin signs are medical emergencies. Calciphylaxis in a dialysis patient carries a one-year mortality above 50 per cent [4]. A new dermatomyositis in an adult mandates an immediate structured malignancy search. Suspected glucagonoma syndrome demands prompt measurement of glucagon and pancreatic imaging. Do not file these under "dermatology referral in outpatients" — they are urgent physician problems.
DWE high-yield: The paraneoplastic dermatology cluster — dermatomyositis (ovarian, lung, gastric), malignant acanthosis nigricans and tripe palms (gastric), sign of Leser-Trelat (GI adenocarcinoma), Trousseau migratory thrombophlebitis (pancreatic), necrolytic migratory erythema (glucagonoma), Sweet syndrome (acute myeloid leukaemia and myelodysplasia) — is the single most tested family of cutaneous-internal disease associations. [1]
A diagnostic framework: pattern first, system second
Approach every unexplained skin lesion with a structured morphology-to-system framework. Describe the lesion (macule, papule, plaque, nodule, vesicle, bulla, purpura, ulcer, atrophy), note its site and distribution, then map it to the shortlist of systemic causes. [1]

The high-yield associations every physician must know
| Skin sign | Key systemic associations | First action |
|---|---|---|
| Acanthosis nigricans | Insulin resistance, obesity; if rapid onset or with tripe palms, gastric adenocarcinoma | HbA1c; if new and rapid, gastroduodenoscopy |
| Necrolytic migratory erythema | Glucagonoma (diabetes, weight loss, DVT) | Serum glucagon, pancreatic CT or octreotide scintigraphy |
| Pretibial myxoedema | Graves disease (dermopathy) | Thyroid function, TSH receptor antibody |
| Malar rash (spares nasolabial folds) | Systemic lupus erythematosus | ANA, anti-dsDNA, anti-Smith, complement |
| Discoid rash (scarring) | Chronic cutaneous lupus; systemic lupus in a minority | Skin biopsy with immunofluorescence (lupus band) |
| Gottron papules, heliotrope rash | Dermatomyositis — adult-onset carries malignancy risk | CK, myositis antibody panel, malignancy search |
| Sclerodactyly, nailfold capillary changes | Systemic sclerosis | ANA, anti-centromere or anti-Scl-70, pulmonary and renal screening |
| Palpable purpura | Small-vessel leucocytoclastic vasculitis | Cryoglobulins, ANCA, hepatitis B and C, complements, drug and infection screen |
| Erythema nodosum | Sarcoidosis (Lofgren syndrome), IBD, streptococcal, drugs, OCP, pregnancy | Chest X-ray, ASO titre, stool studies, biopsy |
| Pyoderma gangrenosum | IBD, arthritis, haematological malignancy | Exclude infection and vasculitis; do NOT debride |
| Dermatitis herpetiformis | Coeliac disease | Anti-tissue transglutaminase IgA, total IgA, duodenal biopsy |
| Calciphylaxis | Advanced CKD or dialysis, warfarin, obesity | Calcium, phosphate, parathyroid hormone, skin biopsy, sodium thiosulfate |
| Spider naevi, palmar erythema | Chronic liver disease (oestrogen excess); pregnancy | Liver function, synthetic function, hepatitis and iron studies |
| Petechiae, purpura | Thrombocytopenia, platelet dysfunction, coagulation disorder | Full blood count, film, coagulation, drug history |
| Sweet syndrome | Acute myeloid leukaemia, myelodysplasia, IBD, drugs, infection | Full blood count and film, marrow if cytopenias |
| Erythema chronicum migrans | Lyme disease (Borrelia burgdorferi) | Clinical diagnosis in endemic area; serology confirmation |
| Secondary syphilis rash on palms and soles | Treponema pallidum infection | Syphilis serology (treponemal and non-treponemal) |
Examiner logic: For every skin sign, the question "what is the single most likely underlying systemic disease?" is the DWE discriminator. The answer rests on a small set of high-yield, frequently tested associations — learn them as a table and you answer most MCQ stems. [1]
Endocrine cutaneous clues
Acanthosis nigricans — insulin resistance or malignancy
Acanthosis nigricans is a velvety, hyperpigmented thickening of the skin in flexural sites — the axillae, the back of the neck, the groin, the umbilicus and the knuckles. The benign form is common, driven by hyperinsulinaemia in obesity and type 2 diabetes mellitus; it is the cutaneous marker of insulin resistance and predicts progression to diabetes. [1]
The pathophysiology explains the clinical pattern. Excess insulin binds to insulin-like growth factor 1 (IGF-1) receptors on keratinocytes and dermal fibroblasts, driving epidermal proliferation. The same pathway is hijacked in the malignant variant, where tumour-derived growth factors — most notably transforming growth factor-alpha (TGF-alpha) — drive the proliferation independent of insulin [3].
The clue that distinguishes malignant acanthosis nigricans is its abrupt onset, rapid progression, severity and extension to atypical sites (palms, mucosae). When acanthosis nigricans appears with tripe palms (thickened, velvety, rugose palmar skin) and the sign of Leser-Trelat, gastric adenocarcinoma is the diagnosis until proven otherwise, and urgent gastroduodenoscopy is mandatory [3]. The skin lesions often improve or resolve after resection of the tumour, confirming the paraneoplastic relationship.
DWE trap: Not all acanthosis nigricans is malignant. The benign form is common in obesity and diabetes and needs only lifestyle and metabolic management. The malignant variant is suggested by rapid onset, severity, mucosal involvement and the coexistence of tripe palms and the sign of Leser-Trelat. [1]
Necrolytic migratory erythema — glucagonoma
Necrolytic migratory erythema is the pathognomonic cutaneous marker of glucagonoma syndrome, caused by an alpha-cell pancreatic neuroendocrine tumour secreting glucagon. The classic triad is a migrating rash, new-onset diabetes and weight loss [1].
The rash is a painful, migratory, annular erythema with superficial epidermal necrosis and central crusting, appearing in periorificial and intertriginous sites — the groin, perineum, buttocks, perioral skin and distal extremities. It waxes and wanes, mimicking eczema, candidiasis or pemphigus, and is often misdiagnosed for months. The pathophysiology relates to hyperglucagonaemia with consequent amino acid and zinc depletion, which starves the epidermis; this explains why supplementation with amino acids or zinc, and suppression of glucagon with a somatostatin analogue (octreotide), can improve the rash [2].
The diagnosis is confirmed by a markedly elevated serum glucagon (often above 1000 ng per litre, normal less than 150), localisation of the pancreatic tumour with contrast CT or octreotide scintigraphy (or Gallium-68 DOTATATE PET), and assessment for hepatic metastases, as glucagonomas are frequently metastatic at presentation. Definitive treatment is surgical resection; octreotide provides symptom control and biochemical suppression when surgery is not curative. [1]
Exam trap: Necrolytic migratory erythema is one of the most frequently missed cutaneous-internal disease diagnoses because it mimics common dermatitides. A new, migrating rash with new diabetes and weight loss is glucagonoma until excluded — check glucagon and image the pancreas. [1]
Pretibial myxoedema and diabetic dermopathy
Pretibial myxoedema (thyroid dermopathy) is the localised deposition of glycosaminoglycans in the dermis of the shins, producing bilateral, asymmetric, non-pitting, waxy plaques or nodules. It is a manifestation of Graves disease and almost always coexists with Graves ophthalmopathy and a high thyroid-stimulating immunoglobulin level. Topical or intralesional corticosteroids under occlusion are the usual first-line treatment. [1]
Diabetic dermopathy (shin spots) is the most common cutaneous marker of diabetes mellitus — atrophic, hyperpigmented, asymptomatic macules on the shins, thought to reflect microvascular disease and minor trauma. It does not require treatment but signals microvascular complication risk and prompts a review of glycaemic control and end-organ surveillance. [1]
Rheumatological cutaneous clues
The malar rash and discoid lupus
The malar (butterfly) rash of systemic lupus erythematosus is a fixed, erythematous, photosensitive rash over the cheeks and bridge of the nose that spares the nasolabial folds. The fold-sparing distinguishes it from rosacea and seborrhoeic dermatitis, both of which involve the folds. The malar rash does not scar — this distinguishes it from discoid lupus, which produces scarring plaques with follicular plugging and a carpet-tack sign, and which may occur in isolation (chronic cutaneous lupus) or as part of systemic lupus. [1]
Dermatomyositis — Gottron papules and heliotrope rash
Dermatomyositis is the single most important paraneoplastic skin disease in physician medicine. The pathognomonic lesions are: [1]
- Gottron papules — violaceous (heliotrope-coloured) papules and plaques over the metacarpophalangeal, proximal and distal interphalangeal joints of the hands.
- Gottron sign — the same violaceous erythema over the elbows, knees and medial malleoli.
- Heliotrope rash — a symmetric violaceous erythema with oedema of the upper eyelids, often the first and most specific cutaneous clue.
- Nailfold changes — periungual erythema, ragged cuticles (Samitz sign) and dilated capillary loops.
- Shawl and V signs — photosensitive erythema over the posterior neck and shoulders (shawl) and the anterior chest (V), reflecting photodistribution. [1]
Adult-onset dermatomyositis carries a malignancy risk of roughly 15 to 25 per cent, with the risk clustering in the first three years around the diagnosis [8]. The myositis-specific antibodies refine the risk: anti-TIF1-gamma and anti-NXP-2 carry the strongest malignancy associations, while anti-Mi-2 carries a lower risk and anti-Jo-1 marks the antisynthetase syndrome with interstitial lung disease. The commonest malignancies are ovarian, lung, gastric, colorectal, pancreatic and breast. A structured malignancy search — CT chest abdomen pelvis, pelvic ultrasound in women, mammography, and upper and lower gastrointestinal endoscopy — is mandatory at diagnosis and for the subsequent three years [8].
DWE high-yield: Adult-onset dermatomyositis mandates a malignancy search. Anti-TIF1-gamma and anti-NXP-2 mark the highest malignancy risk. Most cancers are found in the first three years around the diagnosis. Ovarian cancer is the classic association in women. [1]
Systemic sclerosis — sclerodactyly and nailfold changes
Systemic sclerosis produces hard, thickened, bound-down skin (scleroderma) beginning distally in the fingers (sclerodactyly) and progressing proximally. The nailfold capillaries show dilated loops, dropout and microhaemorrhages on capillaroscopy, a pattern shared with dermatomyositis (the "scleroderma-dermatomyositis overlap" pattern on capillaroscopy). Raynaud phenomenon is nearly universal and usually precedes the skin disease by years. Anti-centromere antibody marks limited cutaneous disease (CREST: calcinosis, Raynaud, oesophageal dysmotility, sclerodactyly, telangiectasia); anti-Scl-70 (anti-topoisomerase I) marks diffuse cutaneous disease with a higher risk of interstitial lung disease and scleroderma renal crisis. [1]
Palpable purpura — small-vessel vasculitis
Palpable purpura — non-blanching, slightly raised, purplish lesions usually on the lower legs — is the hallmark of small-vessel leucocytoclastic vasculitis. The lesion is palpable because of the inflammatory infiltrate around the leaking vessel, and it does not blanch because red cells have extravasated. Causes include: [1]
- Drugs — beta-lactams, sulfonamides, non-steroidal anti-inflammatories, thiazides.
- Infections — hepatitis B and C, endocarditis, meningococcaemia, gonococcaemia.
- Cryoglobulinaemia — particularly type II mixed cryoglobulinaemia from chronic hepatitis C, often with arthralgia and neuropathy.
- ANCA-associated vasculitis — granulomatosis with polyangiitis, microscopic polyangiitis, eosinophilic granulomatosis with polyangiitis.
- Henoch-Schonlein purpura (IgA vasculitis) — palpable purpura, abdominal pain, arthritis and renal involvement, classically in children.
- Connective tissue disease — lupus, rheumatoid arthritis, Sjogren syndrome. [1]
Workup includes full blood count, film, ESR and CRP, cryoglobulins (with proper pre-warming of the collection), ANCA, complements (C3 and C4 fall together in cryoglobulinaemia and lupus, normal in ANCA vasculitis), hepatitis B and C serology, HIV, urinalysis for renal involvement, and a skin biopsy with histology (leucocytoclastic vasculitis) ± direct immunofluorescence (IgA deposition in Henoch-Schonlein). [1]
Erythema nodosum — the septal panniculitis
Erythema nodosum is the most common panniculitis — tender, erythematous, subcutaneous nodules symmetrically on the anterior shins that do not ulcerate and resolve with bruising. Histologically it is a septal panniculitis without vasculitis. The causes divide into: [1]
- Idiopathic — 30 to 55 per cent in most series.
- Infections — streptococcal pharyngitis (the most common identifiable infectious cause), tuberculosis, Yersinia, salmonella, fungal (histoplasmosis, coccidioidomycosis), viral.
- Sarcoidosis — particularly as part of Lofgren syndrome (erythema nodosum, bilateral hilar lymphadenopathy, polyarthritis, fever), which is a benign, self-limited form of acute sarcoid with a good prognosis.
- Inflammatory bowel disease — both Crohn disease and ulcerative colitis, often in parallel with bowel activity.
- Drugs — oral contraceptive pill, sulfonamides, penicillins, bromides.
- Pregnancy and Behcet disease. [1]
The workup of a first episode of erythema nodosum includes a chest X-ray (looking for hilar lymphadenopathy or tuberculosis), throat swab and ASO titre (streptococcal), stool studies if gastrointestinal symptoms, a tuberculin skin test or interferon-gamma release assay, a careful drug history, and a review for bowel symptoms and pregnancy [14].
DWE discriminator: Erythema nodosum in an acute sarcoid patient with bilateral hilar lymphadenopathy and arthritis is Lofgren syndrome — a clinical diagnosis with a good prognosis that does NOT require biopsy confirmation. [1]
Pyoderma gangrenosum — painful ulcers with pathergy
Pyoderma gangrenosum is a neutrophilic dermatosis characterised by painful ulcers with undermined, violaceous, boggy borders and pathergy (worsening with minor trauma). Lesions often begin as pustules or papules at sites of minor injury, rapidly enlarging into deep ulcers. Systemic associations include inflammatory bowel disease (ulcerative colitis more than Crohn disease), arthritis (seropositive and seronegative), and haematological malignancy (acute myeloid leukaemia, myelodysplasia, monoclonal gammopathies). [1]
The diagnosis is clinical, after exclusion of infection, vasculitis and other causes of leg ulceration; there is no pathognomonic histology. The cardinal management rule is never surgically debride, because pathergy worsens the ulcer. Treatment is systemic corticosteroids (prednisone 0.5 to 1 mg per kg per day) or ciclosporin for aggressive disease, with biologic therapy (infliximab, ustekinumab, JAK inhibitors) for refractory cases, alongside gentle local wound care. [1]
DCE high-stakes trap: Pyoderma gangrenosum and calciphylaxis both produce painful lower-leg ulcers, but their management is opposite. Calciphylaxis requires surgical debridement of necrotic tissue; pyoderma gangrenosum is worsened by surgical debridement. Confusing the two is a high-stakes clinical and exam error. [1]
Gastrointestinal cutaneous clues
Dermatitis herpetiformis — coeliac disease in the skin
Dermatitis herpetiformis is the specific cutaneous manifestation of coeliac disease — an intensely pruritic, vesiculobullous eruption of grouped (herpetiform) vesicles on the extensor surfaces (elbows, knees, buttocks, scalp). Almost all patients have some degree of gluten-sensitive enteropathy on duodenal biopsy, even without gastrointestinal symptoms [10].
The pathophysiology is precise. Gluten ingestion drives the formation of IgA antibodies to epidermal transglutaminase (TG3), which deposit as granular IgA in the dermal papillae, recruiting neutrophils and producing the subepidermal blister. The diagnostic gold standard is direct immunofluorescence of perilesional normal-appearing skin, showing granular IgA deposition in the dermal papillae. Biopsying the lesion itself is unhelpful, as the inflammation is non-specific — this is the most common biopsy error in dermatitis herpetiformis. [1]
Management combines two strands: [1]
- A strict lifelong gluten-free diet — definitive therapy for both the skin and the bowel. It takes months to control the rash but treats the underlying enteropathy and reduces the long-term risk of enteropathy-associated T-cell lymphoma and osteoporosis.
- Dapsone (50 to 200 mg orally daily) — a sulfone anti-inflammatory that inhibits neutrophil myeloperoxidase and chemoattraction, providing rapid symptomatic relief (within days) while the diet takes effect. Glucose-6-phosphate dehydrogenase deficiency must be excluded before starting (haemolysis risk), and full blood count and methaemoglobin monitoring are mandatory. [1]
DWE trap: The biopsy in suspected dermatitis herpetiformis must be of perilesional normal skin, not the lesion — granular IgA in dermal papillae is the diagnostic finding. Serology (anti-tissue transglutaminase IgA, anti-endomysial IgA, with total IgA to exclude IgA deficiency) supports the diagnosis. [1]
Pyostomatitis vegetans and oral clues
Pyostomatitis vegetans produces snail-track ulcers and vegetative pustules on the oral mucosa, and is a highly specific marker of inflammatory bowel disease, more often ulcerative colitis than Crohn disease. The skin counterpart is pyodermatitis vegetans. Recognition should prompt gastrointestinal evaluation. [1]
Erythema nodosum (covered above) is the other common cutaneous marker of IBD; it tends to mirror bowel activity and often resolves as the colitis is treated. [1]
Acrodermatitis enteropathica — zinc deficiency
Acrodermatitis enteropathica is a periorificial and acral dermatitis (around the mouth, anus, and on the hands and feet) with diarrhoea and alopecia, caused by zinc deficiency. It may be inherited (autosomal recessive defect in intestinal zinc absorption) or acquired (malnutrition, alcohol use disorder, inflammatory bowel disease, prolonged parenteral nutrition without zinc supplementation, after bariatric surgery). Diagnosis rests on a low serum zinc and clinical response to zinc supplementation (1 to 2 mg per kg per day of elemental zinc). Response is rapid and dramatic — a useful diagnostic confirmation. [1]
Renal and hepatic cutaneous clues
Calciphylaxis — the cutaneous emergency of CKD
Calciphylaxis (calcific uremic arteriolopathy) is the most feared cutaneous complication of advanced chronic kidney disease or dialysis. The pathophysiology is a vascular calcification syndrome: in the uraemic, hyperphosphataemic, inflamed milieu, vascular smooth muscle cells transform into osteoblast-like cells, depositing calcium in subcutaneous arterioles. This causes intimal proliferation, thrombosis and ischaemic infarction of the overlying skin and adipose tissue [4].
Clinically the lesion is unmistakable: exquisitely tender, purpuric, indurated plaques on the lower abdomen, thighs, or buttocks (proximal type) or the distal legs (distal type), which progress to hard, black, necrotic eschars with surrounding livedo. The proximal type carries the worse prognosis. Mortality at one year exceeds 50 per cent, with sepsis from infected necrotic tissue the leading cause of death [4].
Risk factors include dialysis, hyperphosphataemia, hypercalcaemia, high calcium phosphate product, warfarin (a significant, modifiable risk factor — stop it and transition to alternative anticoagulation), obesity, female sex, diabetes, hypoalbuminaemia, and high-dose calcium-based phosphate binders or vitamin D analogues. [1]
Management is multidisciplinary and intensive: [1]
- Wound care with surgical debridement of clearly necrotic tissue (in sharp contrast to pyoderma gangrenosum).
- Intravenous sodium thiosulfate — 25 grams over one hour during the last hour of each haemodialysis session, three times weekly. It chelates calcium, acts as an antioxidant and vasodilator, and has observational evidence of improved pain and wound healing [5].
- Correction of calcium and phosphate — non-calcium-based phosphate binders (sevelamer, lanthanum), dialysate calcium adjustment, cinacalcet for hyperparathyroidism.
- Stop warfarin — transition to low molecular weight heparin or a direct oral anticoagulant where indicated.
- Aggressive pain control and early treatment of infection — sepsis is the leading cause of death.
- Multidisciplinary input — nephrology, dermatology, surgery, infectious diseases, pain and palliative care, with honest prognostic discussion given the high mortality.
DWE high-yield: Calciphylaxis = painful purpuric plaques that necrose, in a dialysis patient, with calcification of cutaneous arterioles on biopsy, one-year mortality above 50 per cent, treated with sodium thiosulfate and surgical debridement. Stop warfarin. [1]
Nephrogenic systemic fibrosis — gadolinium in CKD
Nephrogenic systemic fibrosis is a fibrosing disorder of the skin and systemic organs that develops in patients with severe renal impairment (eGFR below 30 mL per minute per 1.73 metres squared) exposed to gadolinium-based contrast agents, particularly the older, less-stable linear (group I) agents such as gadodiamide [9].
Clinically it begins weeks to months after gadolinium exposure, with bilateral, symmetric, indurated, woody, brawny plaques, typically on the lower legs and progressing proximally, with peau d orange change, joint contractures, restricted mobility and pain. The fibrosis can extend systemically to involve the heart, lungs, liver and skeletal muscle, producing restrictive respiratory failure and death. There is no proven treatment; the focus is avoidance of gadolinium in advanced CKD, and restoration of renal function (for example by renal transplantation) where possible. [1]
The incidence of nephrogenic systemic fibrosis has collapsed since the restriction of group I linear gadolinium agents in severe CKD, the preferential use of more stable macrocyclic agents, and the policy of screening renal function before contrast-enhanced magnetic resonance imaging [9]. The lesson — a careful history of contrast exposure, an eGFR check, and the use of macrocyclic or group II agents at the lowest possible dose — is now standard radiological practice.
Uraemic frost, spider naevi and palmar erythema
Uraemic frost is the rare deposition of urea crystals on the skin in severe uraemia, producing a white, frosted appearance on the face, neck and chest. It reflects very advanced renal failure and is now uncommon with dialysis. [1]
Spider naevi (spider telangiectasias) and palmar erythema are the classic cutaneous markers of chronic liver disease, reflecting oestrogen excess from impaired hepatic metabolism. Spider naevi have a central arteriole with radiating legs that blanch with pressure and refill from the centre; they occur in the distribution of the superior vena cava (above the nipple line). A few spider naevi can be physiological in women and in pregnancy; the significance rises with number, distribution and the company they keep (palmar erythema, jaundice, scratch marks from pruritus, caput medusae, gynaecomastia, parotid enlargement, asterixis in encephalopathy). [1]
Pruritus with scratch marks (excoriations) in a patient with jaundice signals cholestatic pruritus, which can be severe and distressing. Management addresses the underlying cause, with cholestyramine, rifampicin, naloxone antagonists (naltrexone) and sertraline as second-line agents. [1]
Haematological and paraneoplastic cutaneous clues

Petechiae and purpura — thrombocytopenia and coagulation
Petechiae (pinpoint, non-blanching, macular lesions) signal thrombocytopenia or platelet dysfunction; causes include immune thrombocytopenic purpura, leukaemia, aplastic anaemia, drug-induced marrow suppression, disseminated intravascular coagulation, thrombotic thrombocytopenic purpura, and uraemia. Purpura (larger, non-blanching patches) signals vascular leak (vasculitis, amyloidosis, scurvy), coagulation factor deficiency (haemophilia, anticoagulation, liver disease, disseminated intravascular coagulation), or overwhelming infection (meningococcaemia). [1]
The first test is a full blood count with film and a coagulation screen; the film may reveal blasts (leukaemia), schistocytes (microangiopathy), Howell-Jolly bodies (splenic hypofunction), or features of megaloblastic anaemia. [1]
Sweet syndrome — acute febrile neutrophilic dermatosis
Sweet syndrome (acute febrile neutrophilic dermatosis) presents with fever, neutrophilia, and tender erythematous plaques or papules (often pseudovesicular, mimicking cellulitis) on the face, neck, upper trunk and arms. Histology shows a dense neutrophilic infiltrate in the upper dermis without vasculitis. The lesions show pathergy and respond dramatically to systemic corticosteroids. [1]
Sweet syndrome has three major settings [6] [7]:
- Classical or idiopathic — following upper respiratory infection (especially streptococcal), inflammatory bowel disease, or pregnancy.
- Malignancy-associated — most often haematological malignancy; acute myeloid leukaemia is the classic association, with myelodysplastic syndrome, lymphoma and chronic myeloid leukaemia also implicated. Solid tumours are less common. Any cytopenias, peripheral blood blasts, or atypical morphology in Sweet syndrome mandates a marrow examination.
- Drug-induced — granulocyte colony-stimulating factor (the classic cause), sulfonamides, minocycline, all-trans retinoic acid. [1]
Systemic corticosteroids (prednisone 0.5 to 1 mg per kg per day for 2 to 4 weeks, tapering) are first-line; colchicine, dapsone and potassium iodide are alternatives. Malignancy-associated Sweet syndrome responds to corticosteroids but recurs if the underlying malignancy is not treated. [1]
DWE high-yield: Sweet syndrome with cytopenias or peripheral blasts is the cutaneous harbinger of acute myeloid leukaemia or myelodysplasia — a marrow examination is non-negotiable. [1]
Leukaemia cutis and other direct skin infiltrates
Leukaemia cutis is the direct infiltration of the skin by leukaemic cells, producing papules, plaques, nodules or ulcers that are often skin-coloured, violaceous, or haemorrhagic. It signals advanced or relapsed disease and often coexists with systemic involvement. Specific skin infiltrates also occur in lymphoma (T-cell leukaemia-lymphoma, cutaneous B-cell lymphoma) and in Langerhans cell histiocytosis. [1]
Sign of Leser-Trelat — sudden eruptive seborrhoeic keratoses
The sign of Leser-Trelat is the sudden eruption of numerous seborrhoeic keratoses, often with pruritus, in association with an underlying internal malignancy [11] [12]. The proposed mechanism is tumour-derived growth factors (particularly TGF-alpha and heparin-binding epidermal growth factor) driving epidermal proliferation. The classic association is adenocarcinoma of the gastrointestinal tract (gastric, colonic, pancreatic), with breast, lung and lymphoid malignancy also reported. The sign often coexists with malignant acanthosis nigricans and tripe palms.
The clinical and scientific debate around the sign of Leser-Trelat is honest and should be acknowledged: both seborrhoeic keratoses and internal malignancy are common in older people, so a causal association is statistically difficult to prove. Nonetheless, the consensus is that an abrupt change in number, distribution and symptom pattern of seborrhoeic keratoses, especially in a younger patient or with pruritus, justifies a thorough clinical evaluation including age-appropriate cancer screening, gastroscopy and colonoscopy [11].
Trousseau syndrome — migratory thrombophlebitis
Trousseau syndrome is migratory thrombophlebitis — superficial venous thrombosis appearing and resolving in different sites over time, often in unusual locations (the arms, the trunk), reflecting a paraneoplastic hypercoagulable state [13]. The classic underlying malignancy is pancreatic adenocarcinoma, but other mucin-producing tumours (gastric, lung, ovarian) are also implicated. The mechanism is tumour-derived tissue factor and mucin activating thrombosis; management is treatment of the underlying cancer and anticoagulation, with low molecular weight heparin generally preferred over warfarin for cancer-associated thrombosis (per contemporary guidelines).
The clinical lesson is direct: unexplained migratory or recurrent thrombophlebitis in an older patient mandates a search for occult malignancy, with pancreatic and other adenocarcinomas at the top of the differential. [1]
DWE discriminator cluster — paraneoplastic skin signs and their cancers:
Skin sign Classic malignancy Dermatomyositis (adult-onset) Ovarian, lung, gastric, colorectal, pancreatic Malignant acanthosis nigricans with tripe palms Gastric adenocarcinoma Sign of Leser-Trelat GI adenocarcinoma (gastric, colonic, pancreatic) Trousseau migratory thrombophlebitis Pancreatic adenocarcinoma Necrolytic migratory erythema Glucagonoma (pancreatic neuroendocrine) Sweet syndrome with cytopenias Acute myeloid leukaemia, myelodysplasia Erythema gyratum repens Lung and other solid tumours Acquired ichthyosis Lymphoma (Hodgkin and non-Hodgkin)
Infectious and nutritional cutaneous clues
Erythema chronicum migrans — Lyme disease
Erythema chronicum migrans (now usually called erythema migrans) is the pathognomonic cutaneous marker of early Lyme disease, appearing 7 to 14 days (range 3 to 33 days) after the bite of an infected Ixodes tick. It begins as an erythematous macule or papule at the bite site and expands over days to weeks into an annular lesion, classically with central clearing (the "bull's-eye" or target appearance) but more often a uniform erythematous patch. [1]
In an endemic area, erythema migrans is a clinical diagnosis — serology may be negative in the first weeks and is not required to start treatment. First-line therapy for early Lyme is doxycycline 100 mg orally twice daily for 14 to 21 days (or amoxicillin 500 mg three times daily or cefuroxime 500 mg twice daily in pregnancy or tetracycline allergy). Patients should be advised on tick avoidance and tick removal. [1]
Exam trap: The bull's-eye appearance is the classic but not the most common morphology — most erythema migrans lesions are uniform erythematous patches that expand. In endemic areas, treat clinically; do not wait for serology. [1]
Secondary syphilis — the rash on palms and soles
Secondary syphilis produces a diffuse, symmetric, maculopapular rash that classically involves the palms and soles — a distribution rare in other rashes and a high-yield exam discriminator. It may be accompanied by condylomata lata (moist wart-like lesions in the anogenital region), mucous patches, generalised lymphadenopathy, alopecia ("moth-eaten") and constitutional symptoms. Serology (treponemal — TPHA or treponemal enzyme immunoassay; and non-treponemal — rapid plasma reagin or venereal disease research laboratory) confirms the diagnosis. Treatment is a single dose of intramuscular benzathine penicillin G (1.8 g or 2.4 million units), with doxycycline or tetracycline in penicillin allergy. [1]
Scurvy, pellagra and acrodermatitis enteropathica — nutritional skin disease
Scurvy (vitamin C deficiency) produces perifollicular haemorrhage, corkscrew hairs, gingival bleeding, bruising, and poor wound healing — a result of defective collagen synthesis. Risk factors include dietary restriction, alcohol use disorder, isolated diets, and malabsorption. Treatment is ascorbic acid (1000 mg daily for a week, then maintenance). [1]
Pellagra (niacin or vitamin B3 deficiency) produces the classic triad of the three Ds — dermatitis, diarrhoea and dementia — and, untreated, death. The dermatitis is a photosensitive rash on exposed sites with Casal necklace (a rash encircling the neck in the distribution of a collar). Causes include dietary deficiency (maize-based diets), malabsorption, alcohol use disorder, carcinoid syndrome (tryptophan diverted to serotonin synthesis), and isoniazid therapy (which inhibits niacin synthesis from tryptophan). Treatment is nicotinamide. [1]
Acrodermatitis enteropathica (covered above) is the periorificial and acral dermatitis of zinc deficiency. [1]
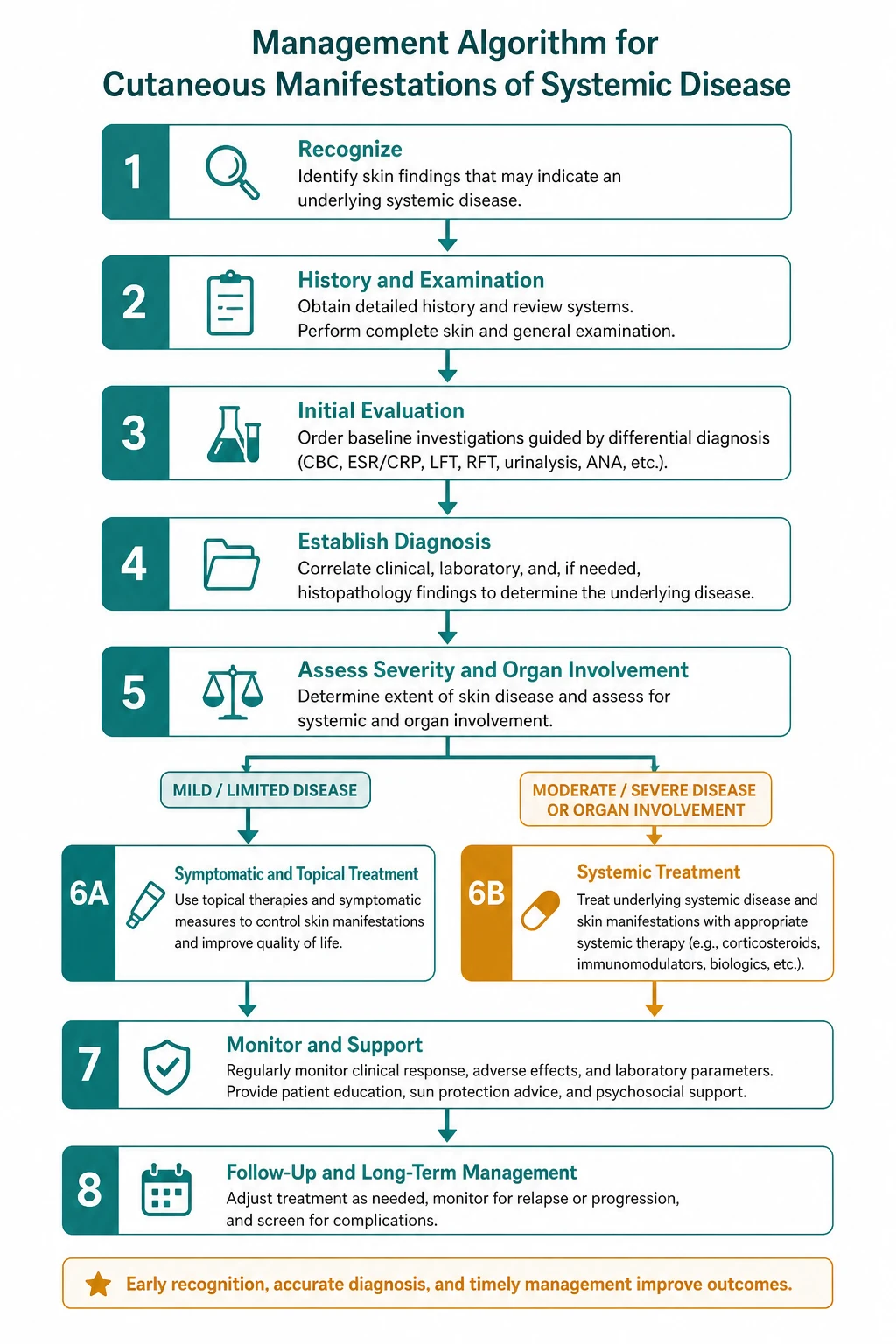
Approach to the diagnostic skin sign

When a cutaneous sign suggests systemic disease, work through a deliberate, structured approach: [1]
- Describe the lesion precisely — site, morphology (macule, papule, plaque, nodule, vesicle, bulla, purpura, ulcer, atrophy), colour, arrangement, distribution (localised, regional, photodistributed, acral, flexural, mucosal).
- Generate a differential from the morphology and distribution — a short list of high-yield systemic associations (use the table above as the starting point).
- Take a focused history — onset, progression, drugs, travel, tick exposure, sun exposure, bowel and systemic symptoms, weight loss, malignancy history, family history, occupation.
- Examine the patient fully — the lesion in context, the whole skin including scalp, nails, palms, soles, flexures and mucosae, and a systemic examination for lymphadenopathy, organomegaly, arthritis, and chest, cardiac and abdominal findings.
- Biopsy when indicated — punch or incisional biopsy including subcutaneous fat for panniculitis, and perilesional normal skin for direct immunofluorescence in suspected immunobullous disease (dermatitis herpetiformis, pemphigoid, pemphigus, lupus band test).
- Order targeted investigations — full blood count and film, ESR and CRP, glucose and HbA1c, renal and liver function, iron studies, then pattern-specific serology (anti-tissue transglutaminase and IgA for coeliac; ANA, extractable antibodies and complement for lupus; myositis antibody panel and CK for dermatomyositis; ANCA and cryoglobulins for vasculitis).
- Image when a mass or paraneoplastic sign is suspected — CT chest abdomen pelvis and pelvic ultrasound in suspected paraneoplastic dermatomyositis; pancreatic CT or octreotide scintigraphy in suspected glucagonoma; chest X-ray for sarcoid and tuberculosis in erythema nodosum; bone marrow in Sweet syndrome with cytopenias.
- Treat the underlying disease — the skin often tracks the systemic disease (the rash of necrolytic migratory erythema fades after glucagonoma resection; dermatomyositis improves with tumour removal; dermatitis herpetiformis clears with a gluten-free diet).
- Provide skin-directed therapy — dapsone for dermatitis herpetiformis, topical corticosteroids for cutaneous lupus and dermatomyositis, sodium thiosulfate and wound care for calciphylaxis, systemic corticosteroids or biologics for pyoderma gangrenosum and Sweet syndrome. [1]
Communication principle: A patient who learns that a rash on their elbows is actually coeliac disease, or that a velvety mark in the axilla is the first sign of stomach cancer, is often frightened and confused. Lead with the answer, explain the mechanism, set out the diagnostic and management plan, and engage the relevant specialty teams early. The dermatologist and the physician working together is the model for this field. [1]
DWE high-yield discriminators
- Adult-onset dermatomyositis is a paraneoplastic disease. Roughly 15 to 25 per cent of adults have an underlying malignancy, risk clustering in the first three years; anti-TIF1-gamma and anti-NXP-2 carry the highest risk. A structured malignancy search is mandatory [8].
- Malignant acanthosis nigricans with tripe palms points to gastric adenocarcinoma. Sudden, severe, mucosally involved acanthosis nigricans warrants urgent gastroduodenoscopy [3].
- Sign of Leser-Trelat points to GI adenocarcinoma. Sudden eruption of seborrhoeic keratoses, especially with pruritus, in an older patient warrants cancer screening [11].
- Trousseau migratory thrombophlebitis points to pancreatic cancer. Recurrent or migratory superficial thrombophlebitis in an older patient warrants a search for occult malignancy, pancreatic first [13].
- Necrolytic migratory erythema points to glucagonoma. The triad of migrating rash, new diabetes and weight loss — measure serum glucagon and image the pancreas [1].
- Sweet syndrome with cytopenias or blasts points to acute myeloid leukaemia or myelodysplasia. A marrow examination is non-negotiable [6] [7].
- Calciphylaxis in a dialysis patient has a mortality above 50 per cent. Sodium thiosulfate, surgical debridement, correction of calcium-phosphate, stop warfarin [4].
- Dermatitis herpetiformis is coeliac disease in the skin. Biopsy perilesional normal skin for granular IgA in dermal papillae; treat with a lifelong gluten-free diet plus dapsone bridge [10].
- Pyoderma gangrenosum is worsened by surgical debridement — the opposite of calciphylaxis. Never confuse the two.
- Nephrogenic systemic fibrosis follows gadolinium exposure in severe CKD — avoid group I linear agents; the incidence has collapsed with macrocyclic agents and renal screening [9].
DCE long-case integration
A typical long case in cutaneous manifestations of systemic disease might be a 58-year-old man with a three-month history of a violaceous facial rash, proximal muscle weakness, dysphagia and a new diagnosis of dermatomyositis with an anti-TIF1-gamma antibody and an ovarian mass on imaging; or a 64-year-old dialysis patient with rapidly progressive, exquisitely painful purpuric plaques on the thighs that are necrosing, found to have calciphylaxis. The structured approach: [1]
- Opening statement (SASPOP) — integrate the skin sign with the systemic context. Do not list the dermatology in isolation.
- Problem list — prioritise the urgent (malignancy search in dermatomyositis; sepsis prevention in calciphylaxis) over the chronic.
- Integrated management plan — dermatology, oncology, nephrology, surgery, nutrition and palliative care as required.
- Communication and shared decision-making — honest prognostic discussion, multidisciplinary coordination, attention to pain and quality of life. [1]
The demonstration of integrated medicine — recognising the skin sign as the entry point to a multisystem disease, then orchestrating the relevant specialty teams — is what distinguishes a strong long-case answer. [1]
DCE short-case skin examination
In a short case you may be asked to examine a patient with a skin rash or to perform a general skin examination. A systematic routine: [1]
- End of bed — observe the patient's general appearance, distribution of the rash, photodistribution, any scaling, ulceration, or asymmetry.
- Face — malar rash (spares nasolabial folds in SLE), heliotrope rash and periorbital oedema (dermatomyositis), discoid lesions (scarring), oral mucosa (aphthae, lichen planus, pyostomatitis vegetans, Candida, hairy leukoplakia).
- Hands and nails — Gottron papules (dermatomyositis), periungual erythema and ragged cuticles (Samitz sign), nailfold capillary dilatation (dermatomyositis, systemic sclerosis), clubbing, palmar erythema (chronic liver disease), Janeway lesions and Osler nodes (endocarditis).
- Trunk — spider naevi (SVC distribution, chronic liver disease), V and shawl signs (dermatomyositis), seborrhoeic keratoses (sign of Leser-Trelat if sudden eruption), morphea or plaques of scleroderma.
- Lower limbs — erythema nodosum (shins), pyoderma gangrenosum (ulcers), palpable purpura (vasculitis), livedo reticularis (APS, polyarteritis), calciphylaxis (purpuric necrotic plaques), pretibial myxoedema (Graves), diabetic dermopathy, acrodermatitis enteropathica.
- Synthesis — describe findings morphologically, then synthesise a diagnostic statement, offer a differential, and propose confirmatory tests. [1]
Presentation template: "I examined this patient's skin systematically. On the face there is a violaceous erythema with oedema of the upper eyelids — a heliotrope rash — and over the knuckles there are violaceous Gottron papules. There is periungual erythema with ragged cuticles and dilated nailfold capillaries. On the trunk there is a photosensitive V-sign rash. These findings are pathognomonic of dermatomyositis. Given that adult-onset dermatomyositis carries a significant paraneoplastic risk, I would measure CK and a myositis antibody panel including anti-TIF1-gamma, and undertake a structured malignancy search with CT chest abdomen pelvis, pelvic ultrasound, mammography and upper and lower gastrointestinal endoscopy." [1]
Key references and evidence summary
| Topic | PMID | Key finding |
|---|---|---|
| Necrolytic migratory erythema (glucagonoma) | 15538929 | Clinical review of the glucagonoma syndrome and its dermatosis [1] |
| Cutaneous glucagonoma syndrome | 29450880 | Modern review of necrolytic migratory erythema [2] |
| Malignant acanthosis nigricans and gastric cancer | 28317636 | Classic paraneoplastic association with gastric adenocarcinoma [3] |
| Calciphylaxis pathophysiology and management | 25249804 | Medial calcification of arterioles, thrombosis, one-year mortality above 50 per cent [4] |
| Calciphylaxis (StatPearls) | 30085562 | Sodium thiosulfate, wound care, stop warfarin [5] |
| Sweet syndrome comprehensive review | 17655751 | Clinical settings, malignancy association, corticosteroid response [6] |
| Malignancy-associated Sweet syndrome | 3058878 | AML is the most common associated malignancy [7] |
| Cancer-associated dermatomyositis | 42409300 | Anti-TIF1-gamma and anti-NXP-2 mark highest malignancy risk; risk clusters in the first three years [8] |
| Nephrogenic systemic fibrosis and gadolinium | 16885403 | Group I linear gadolinium agents drive NSF in severe CKD [9] |
| Dermatitis herpetiformis (current concepts) | 21571167 | Granular IgA in dermal papillae, gluten-free diet as definitive therapy [10] |
| Sign of Leser-Trelat | 8682971 | Sudden eruptive seborrhoeic keratoses with GI adenocarcinoma [11] |
| Sign of Leser-Trelat (StatPearls) | 29261959 | TGF-alpha-driven mechanism; the clinical controversy [12] |
| Trousseau syndrome | 17496204 | Migratory thrombophlebitis from tumour-derived tissue factor, classically pancreatic [13] |
| Erythema nodosum | 17375516 | Septal panniculitis, causes include strep, sarcoid, IBD, drugs [14] |
Australasian College of Dermatologists clinical guidelines; NICE Clinical Knowledge Summaries for coeliac disease; KDIGO chronic kidney disease mineral and bone disorder guideline (for the calciphylaxis context); dermatology and internal medicine reference texts for the broader pattern-recognition framework. [1]
References
- [1]Elder DE The glucagonoma syndrome and necrolytic migratory erythema: a clinical review Eur J Endocrinol, 2004.PMID 15538929
- [2]Tiengo C, Sforazzini G, Abatangelo G, et al. A review of cutaneous manifestations within glucagonoma syndrome: necrolytic migratory erythema Int J Dermatol, 2018.PMID 29450880
- [3]Lopez-Lopez D, Martinez-Perez L, Munoz-Moreno MF, et al. Gastric Cancer Associated With Malignant Acanthosis Nigricans Am J Med Sci, 2017.PMID 28317636
- [4]Nigwekar SU, Kroshinsky D, Thadhani RI Calcific uremic arteriolopathy in end stage renal disease: pathophysiology and management Ochsner J, 2014.PMID 25249804
- [5]Westphal SG, et al. Calciphylaxis 2026.PMID 30085562
- [6]Cohen PR Sweet's syndrome--a comprehensive review of an acute febrile neutrophilic dermatosis Orphanet J Rare Dis, 2007.PMID 17655751
- [7]Cohen PR, Talpaz M, Kurzrock R Malignancy-associated Sweet's syndrome: review of the world literature J Clin Oncol, 1988.PMID 3058878
- [8]Voulgaris A, Lazaridou A, Arvanitaki A, et al. Cancer-associated dermatomyositis: A scoping review of the literature Autoimmun Rev, 2026.PMID 42409300
- [9]Marckmann P, Skov L, Rossen K, et al. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging J Am Soc Nephrol, 2006.PMID 16885403
- [10]Bolotin D, Petronic-Rosic V Dermatitis herpetiformis. Part I. Epidemiology, pathogenesis, and clinical presentation J Am Acad Dermatol, 2011.PMID 21571167
- [11]Schwartz RA Sign of Leser-Trélat J Am Acad Dermatol, 1996.PMID 8682971
- [12]Bernett CN, Schmieder GJ. Leser-Trélat Sign 2026.PMID 29261959
- [13]Varki A Trousseau's syndrome: multiple definitions and multiple mechanisms Blood, 2007.PMID 17496204
- [14]Schwartz RA, Nervi SJ Erythema nodosum: a sign of systemic disease Am Fam Physician, 2007.PMID 17375516