Phys · endocrine
Calcium and Bone Disorders
Also known as hypercalcaemia · primary hyperparathyroidism · secondary hyperparathyroidism · tertiary hyperparathyroidism · hypercalcaemia of malignancy · PTHrP-mediated hypercalcaemia · humoral hypercalcaemia of malignancy · hypocalcaemia · hypoparathyroidism · post-surgical hypoparathyroidism · autoimmune hypoparathyroidism · pseudohypoparathyroidism · DiGeorge syndrome · 22q11.2 deletion syndrome · osteoporosis · DEXA scan · T-score · FRAX · bisphosphonate · alendronate · zoledronic acid · denosumab · teriparatide · raloxifene · drug holiday · osteomalacia · Looser zones · rickets · cinacalcet · calcitonin
Consultant-physician-depth guide to calcium homeostasis and bone disorders — hypercalcaemia (primary hyperparathyroidism, malignancy-associated, granulomatous, drug-induced), hypocalcaemia (post-surgical hypoparathyroidism, autoimmune, vitamin D deficiency, CKD, hypomagnesaemia), osteoporosis (DEXA, FRAX, bisphosphonates, denosumab, teriparatide, anabolic therapy, drug holidays), and osteomalacia (vitamin D deficiency, Looser zones) — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Calcium and Bone Disorders

The answer first
Calcium disorders are among the highest-yield topics in the physician exam because they are common, treatable, and test a candidate's ability to interpret an integrated hormone axis rather than a single number. The single most important initial step in any hypercalcaemic patient is to measure intact parathyroid hormone (PTH) simultaneously with the corrected calcium — this divides all hypercalcaemia into PTH-dependent (primary hyperparathyroidism) and PTH-independent (malignancy, granulomatous disease, vitamin D intoxication) causes. A high or inappropriately normal PTH in the face of hypercalcaemia is primary hyperparathyroidism until proven otherwise [1].
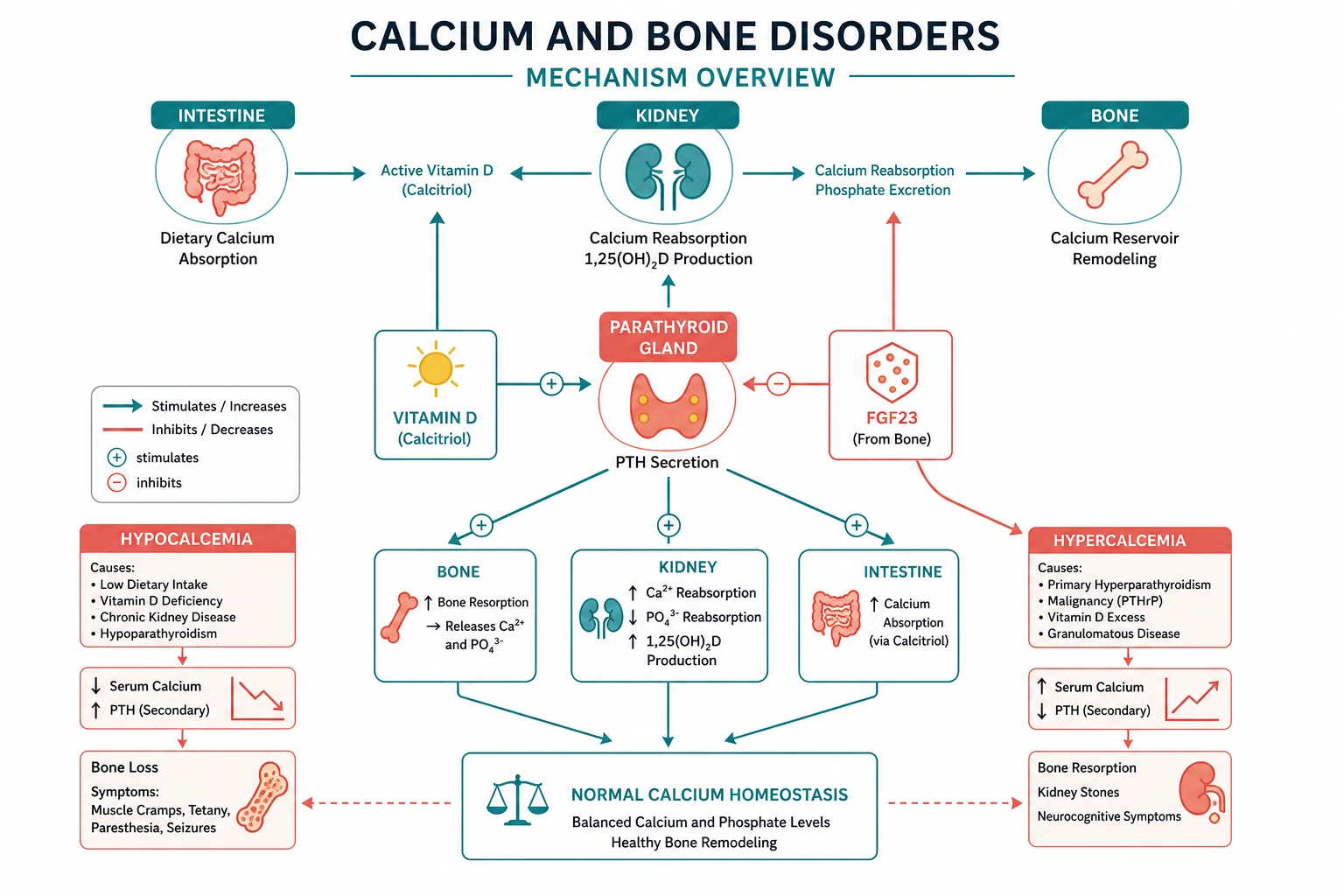
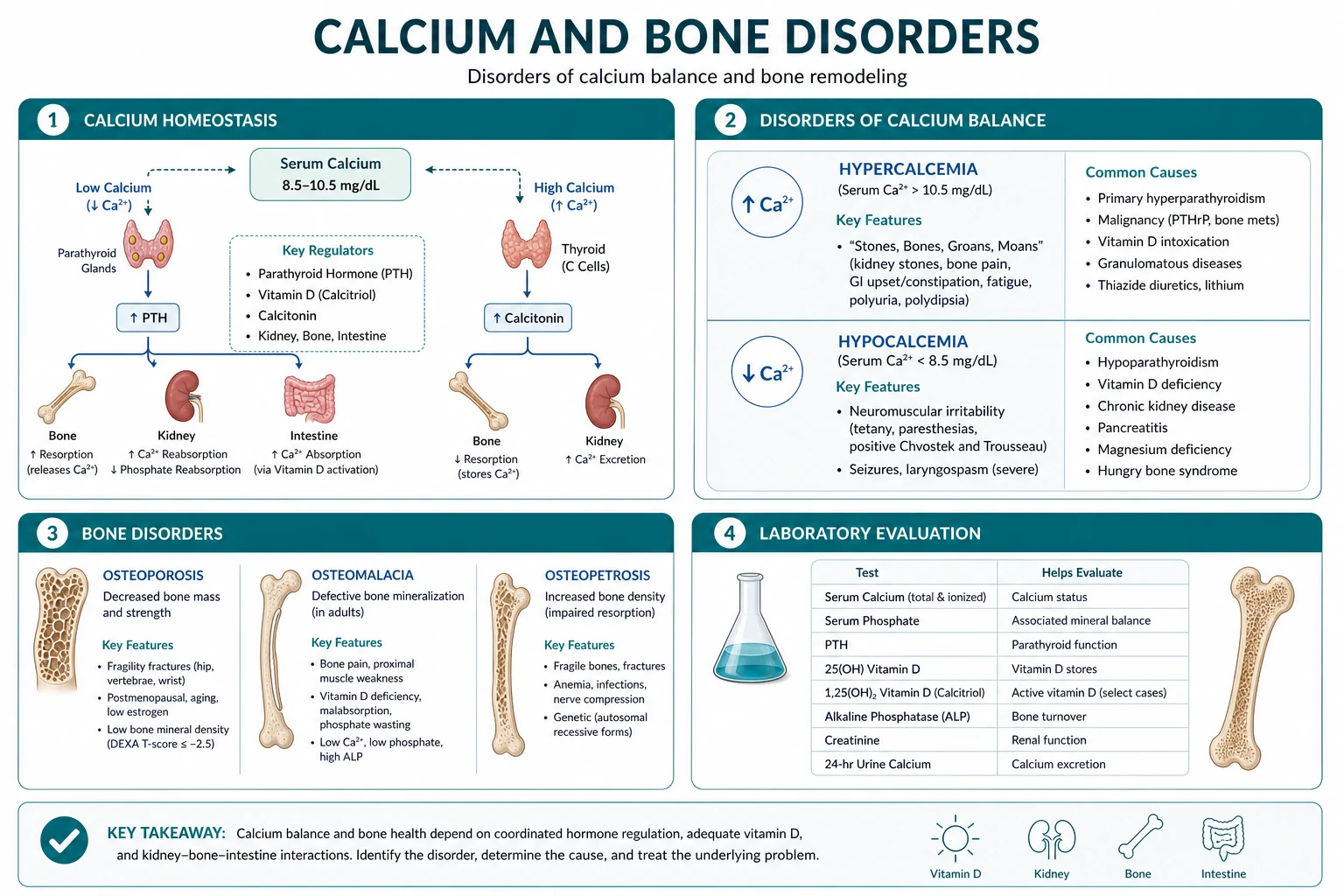
The framework is the calcium-PTH-vitamin D axis. PTH and 1,25-dihydroxyvitamin D are the two master regulators; calcitonin is a minor player in adults. PTH raises serum calcium by mobilising bone, increasing renal calcium reabsorption, and stimulating renal 1-alpha-hydroxylase to convert 25-hydroxyvitamin D to its active form. The active vitamin D then increases intestinal calcium absorption. This loop is exquisitely sensitive — a small change in serum calcium is detected by the calcium-sensing receptor on parathyroid chief cells, which adjusts PTH secretion within seconds. [1]
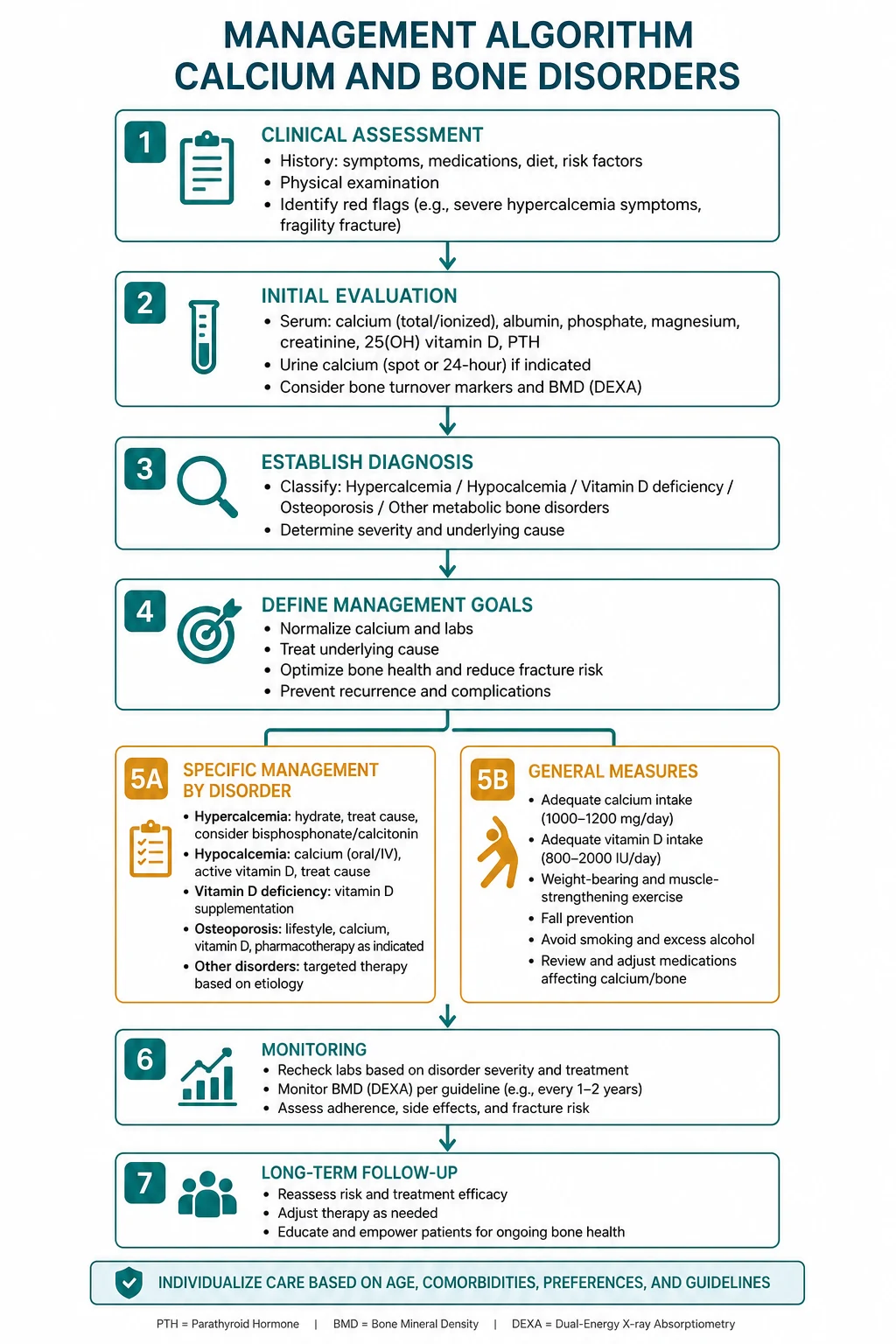
The management logic follows directly from the mechanism. Severe symptomatic hypercalcaemia demands volume expansion with IV normal saline first, then an antiresorptive agent (IV zoledronic acid or subcutaneous denosumab), with calcitonin for rapid bridge effect and dialysis as a last resort in renal failure. Primary hyperparathyroidism in a surgical candidate is cured by parathyroidectomy. Hypocalcaemia is treated with oral calcium and active vitamin D (calcitriol) for chronic forms, and IV calcium gluconate for symptomatic or severe acute presentations. Osteoporosis is defined by DEXA T-score below -2.5 and treated with an antiresorptive first-line, reserving anabolic therapy (teriparatide) for very high-risk patients [6].
Calcium homeostasis — the axis that drives interpretation

Serum calcium exists in three fractions: ionised (approximately 50%, the physiologically active form), albumin-bound (approximately 40%), and complexed to anions (approximately 10%). Because the albumin-bound fraction is the largest, total calcium must be corrected for albumin: add 0.02 mmol/L for every 1 g/L the albumin is below 40 g/L (or subtract if above). In critical illness, acid-base status shifts the ionised fraction — acidosis decreases albumin binding and raises ionised calcium; alkalosis does the reverse. When in doubt, measure a direct ionised calcium. [1]
PTH — the minute-to-minute regulator
Parathyroid hormone is an 84-amino-acid peptide secreted by the four (usually) parathyroid chief cells. Its secretion is governed by the calcium-sensing receptor (CaSR) on the cell surface — a G-protein-coupled receptor that detects extracellular calcium and suppresses PTH release when calcium is high. Calcimimetics (cinacalcet) exploit this receptor. PTH acts through three organs: [1]
- Bone — stimulates osteoclast-mediated bone resorption (via osteoblast RANKL signalling) within minutes to hours, releasing calcium and phosphate.
- Kidney — increases distal tubular calcium reabsorption (the major site of fine-tuning), decreases proximal phosphate reabsorption (phosphaturia), and stimulates 1-alpha-hydroxylase in the proximal tubule to convert 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D.
- Gut — indirectly increases calcium absorption via the 1,25-dihydroxyvitamin D generated by the kidney. [1]
The net effect of PTH is to raise serum calcium and lower serum phosphate. This is the key biochemical pattern — in primary hyperparathyroidism you see high calcium, low or low-normal phosphate, and high or inappropriately normal PTH. [1]
Vitamin D — the day-to-day regulator
Vitamin D3 (cholecalciferol) is synthesised in the skin from 7-dehydrocholesterol under UV-B radiation, or ingested from diet (fatty fish, fortified foods) or supplements. It undergoends hepatic 25-hydroxylation (the storage form, measured as 25-hydroxyvitamin D or calcifediol) and then renal 1-alpha-hydroxylation to the active hormone, 1,25-dihydroxyvitamin D (calcitriol). The 1-alpha-hydroxylase enzyme is stimulated by PTH and hypophosphataemia, and inhibited by FGF23. Calcitriol binds the vitamin D receptor (VDR) in intestinal enterocytes to upregulate calcium-binding proteins (calbindins), increasing calcium and phosphate absorption. [1]
DWE high-yield: The test to order for vitamin D status is 25-hydroxyvitamin D (calcifediol) — it reflects body stores and has a half-life of 2 to 3 weeks. Do NOT order 1,25-dihydroxyvitamin D (calcitriol) as a screening test for deficiency — it has a short half-life, is maintained at normal or even high levels by secondary hyperparathyroidism until very late in CKD, and gives misleading results. Deficiency is defined as 25-hydroxyvitamin D below 50 nmol/L [7].
Calcitonin — the minor brake
Calcitonin is a 32-amino-acid peptide secreted by thyroid parafollicular C cells in response to hypercalcaemia. It inhibits osteoclast activity and lowers serum calcium modestly. It is therapeutically useful as a rapid-acting antiresorptive agent in acute severe hypercalcaemia (onset within hours, but tachyphylaxis after 48 hours) and in Paget disease. Medullary thyroid carcinoma secretes large amounts — calcitonin is the tumour marker. [1]
Hypercalcaemia
The discriminating framework — PTH first
The first step in evaluating any hypercalcaemic patient is to confirm the calcium is genuinely elevated (corrected for albumin or measure ionised), exclude obvious causes (thiazides, calcium supplements, immobilisation), and then measure intact PTH. This single test splits the differential: [1]
| PTH | Interpretation | Common causes |
|---|---|---|
| High or inappropriately normal | PTH-dependent (calcium is being actively conserved) | Primary or tertiary hyperparathyroidism, familial hypocalciuric hypercalcaemia (FHH) |
| Suppressed (below 2.0 pmol/L) | PTH-independent (the body is trying to excrete calcium but the influx overwhelms renal capacity) | Malignancy, granulomatous disease, vitamin D intoxication, thyrotoxicosis, immobilisation, milk-alkali syndrome |
DWE trap: A PTH in the upper half of the reference range in the presence of hypercalcaemia is not normal — it is inappropriately normal. The normal parathyroid gland would suppress PTH to near-zero in the face of hypercalcaemia. This pattern is primary hyperparathyroidism. [1]
Primary hyperparathyroidism
Primary hyperparathyroidism (PHPT) is the commonest cause of hypercalcaemia in the outpatient setting, affecting approximately 1 to 3% of adults, with a female-to-male ratio of 3 to 1 and a peak incidence in the sixth decade. The ** Fifth International Workshop (2022)** provides the current framework [1].
Pathology: A single parathyroid adenoma accounts for approximately 80% of cases. Four-gland hyperplasia accounts for 15 to 20%, and parathyroid carcinoma for less than 1%. Multiple adenomas can occur. The adenoma autonomously secretes PTH independent of the calcium-sensing receptor feedback, causing the classic biochemical triad: hypercalcaemia, hypophosphataemia (or low-normal), and elevated or inappropriately normal PTH. [1]
MEN syndromes: PHPT is a component of MEN1 (menin gene, chromosome 11; parathyroid hyperplasia, pancreatic neuroendocrine tumours, pituitary adenomas) where it is typically the first manifestation and the most penetrant feature. It also occurs in MEN2A (RET proto-oncogene; medullary thyroid carcinoma, phaeochromocytoma, parathyroid hyperplasia) though less commonly. Any patient with PHPT and a family history of endocrine tumours, or recurrent or multi-gland disease, warrants genetic screening for MEN1 or RET. [1]
Clinical presentation — the classical and the modern phenotype: [1]
The classical phenotype — stones, bones, abdominal groans, and psychic moans — is now rare in countries with routine biochemical screening: [1]
- Stones — nephrolithiasis or nephrocalcinosis in approximately 15 to 20% of untreated patients.
- Bones — osteitis fibrosa cystica (brown tumours), subperiosteal bone resorption (especially radial aspect of middle phalanges, distal clavicles, skull salt-and-pepper appearance). Now rare; the modern bone phenotype is preferential cortical bone loss at the distal third radius on DEXA.
- Abdominal groans — constipation, peptic ulcer disease, pancreatitis.
- Psychic moans — fatigue, depression, anxiety, cognitive impairment, and in severe hypercalcaemia, confusion and coma. [1]
The modern phenotype is asymptomatic or mildly symptomatic hypercalcaemia discovered on routine biochemistry. Patients may report non-specific fatigue, polyuria, polydipsia, bone pain, or mood disturbance. The 2022 Fifth Workshop emphasises that many patients labelled asymptomatic have subtle features (neurocognitive, cardiovascular) that improve after surgery, but the evidence for routine neuropsychiatric benefit is inconsistent [1].
Investigations:
- Corrected calcium elevated (typically 2.6 to 3.0 mmol/L; above 3.5 is severe hypercalcaemia). [1]- Intact PTH elevated or inappropriately normal — the diagnostic cornerstone.
- Phosphate low or low-normal (PTH is phosphaturic).
- ALP may be mildly elevated (reflecting high bone turnover).
- 25-hydroxyvitamin D — measure in all PHPT patients; deficiency is common and worsens the disease. Replete if below 50 nmol/L (cautiously, as it can raise calcium further).
- 24-hour urinary calcium — elevated in PHPT (above 250 mg in women, above 300 mg in men per the 2022 Workshop); low (below 100 mg) suggests FHH. [1]- Renal function and eGFR.
- DEXA — assess bone density (hip, lumbar spine, and distal third radius — the radius is the cortical site most affected by PHPT).
- Renal imaging (ultrasound or CT) to detect nephrocalcinosis or stones. [1]
Familial hypocalciuric hypercalcaemia (FHH) — the must-not-miss mimic: FHH is an autosomal dominant loss-of-function mutation of the calcium-sensing receptor. The parathyroid glands and renal tubules both perceive calcium as lower than it is, so PTH remains mildly elevated and the kidney avidly reabsorbs calcium. The result is lifelong mild hypercalcaemia with low urinary calcium excretion (fractional excretion of calcium below 0.01, or 24-hour urinary calcium below 100 mg) and a PTH that is in the normal or mildly elevated range. It is benign — patients do not develop complications and do not benefit from parathyroidectomy. Distinguishing FHH from mild PHPT is the classic exam discriminator — the calcium-to-creatinine clearance ratio (below 0.01 in FHH, above 0.02 in PHPT) is the key test [1].
When to offer parathyroidectomy — the Fifth Workshop criteria
Parathyroidectomy is the only definitive cure for PHPT and is recommended for all symptomatic patients (nephrolithiasis, fractures, severe hypercalcaemia) and for asymptomatic patients meeting the 2022 criteria [1]:
| Criterion | Threshold for surgery |
|---|---|
| Serum calcium | More than 0.25 mmol/L above the upper limit of normal |
| Renal | eGFR below 60, 24-hour urinary calcium above 250 mg (women) or 300 mg (men), nephrocalcinosis or nephrolithiasis on imaging, or history of kidney stones |
| Age | Below 50 years |
Patients not meeting surgical criteria (or declining surgery) are monitored with annual biochemistry and DEXA every 1 to 3 years. Cinacalcet (a calcimimetic that sensitises the calcium-sensing receptor, 30 to 60 mg orally twice daily) normalises calcium but not bone density — it is used for patients who are not surgical candidates or who have persistent post-surgical disease. [1]
Hypercalcaemia of malignancy
Hypercalcaemia of malignancy is the commonest cause of hypercalcaemia in hospitalised patients. It carries a poor prognosis (median survival 30 to 60 days without effective anticancer therapy) and is seen with two principal mechanisms [3][8]:
1. Humoral hypercalcaemia of malignancy (HHM) — PTHrP-mediated: The tumour secretes parathyroid hormone-related protein (PTHrP), which binds the PTH receptor and mimics its effects — bone resorption, renal calcium reabsorption, and increased 1-alpha-hydroxylase activity. The biochemistry resembles PHPT (hypercalcaemia, hypophosphataemia, elevated or high-normal calcitriol) but PTH is suppressed and PTHrP is elevated. Typical tumours: squamous cell carcinoma of the lung, renal cell carcinoma, bladder carcinoma, breast carcinoma, and ovarian carcinoma. HHM accounts for approximately 80% of hypercalcaemia of malignancy [8].
2. Local osteolytic hypercalcaemia: Direct tumour infiltration of bone by osteoclast-activating cytokines (RANKL, IL-6, MIP-1 alpha) causes massive local bone destruction, releasing calcium. Typical in multiple myeloma, breast carcinoma with extensive bone metastases, and lymphoma. The biochemistry shows hypercalcaemia with a normal or elevated phosphate (tumour lysis of bone releases both), and a suppressed PTH. [1]
The exam discriminator: PTH is suppressed in both forms of hypercalcaemia of malignancy. If PTHrP is available, it is elevated in HHM and normal in local osteolytic disease. Calcitriol may be elevated in HHM (PTHrP stimulates 1-alpha-hydroxylase) and in all lymphoma subtypes (lymphoma cells express 1-alpha-hydroxylase autonomously). [1]
Other causes of hypercalcaemia
| Cause | Mechanism | Key clue |
|---|---|---|
| Thiazide diuretics | Increased distal tubular calcium reabsorption | Medication history; mild hypercalcaemia, resolves on cessation |
| Vitamin D intoxication | Excess 1,25-dihydroxyvitamin D from supplements | Elevated 25-hydroxyvitamin D (above 150 nmol/L), hyperphosphataemia, suppressed PTH |
| Granulomatous disease (sarcoidosis, TB, fungal) | Macrophage 1-alpha-hydroxylase in granulomas converts 25-OH-D to active form autonomously | Elevated 1,25-dihydroxyvitamin D, responds to glucocorticoids |
| Milk-alkali syndrome | Excess calcium and absorbable alkali intake (calcium carbonate antacids) | History of high calcium intake, metabolic alkalosis, AKI, suppressed PTH |
| Immobilisation | Uncoupled bone resorption without mechanical loading | Young patients in rapid growth (adolescents) or high bone turnover (Paget disease); high bone markers |
| Thyrotoxicosis | Increased bone turnover | Thyroid function tests; resolves with treatment |
| Adrenal insufficiency (Addisonian crisis) | Increased bone resorption and hemoconcentration | Hyponatraemia, hyperkalaemia, hypotension |
| Vitamin A intoxication | Retinoid-stimulated bone resorption | History of supplement use |
DWE trap: A hospitalised patient with sarcoidosis and hypercalcaemia — the mechanism is autonomous macrophage 1-alpha-hydroxylase in the granulomas converting 25-OH-D to 1,25-dihydroxyvitamin D. Glucocorticoids are the treatment because they suppress the macrophage enzyme. Bisphosphonates work but are second-line. Do NOT give vitamin D supplements. [1]
Emergency management of severe hypercalcaemia

Severe hypercalcaemia (corrected calcium above 3.5 mmol/L) with symptoms (altered mental state, dehydration, AKI, cardiac arrhythmia) is a medical emergency. The 2023 Endocrine Society guideline and the 2016 Society for Endocrinology guidance provide the framework [3][4]:
Step 1 — Aggressive volume expansion: The immediate problem is that hypercalcaemia causes nephrogenic diabetes insipidus, volume depletion, and a further rise in calcium from reduced renal excretion. IV normal saline 3 to 6 L over the first 24 hours (200 to 300 mL/h initially, titrated to euvolaemia and urine output) is the single most important first step. It dilutes the calcium, restores glomerular filtration, and promotes calciuresis. [1]
Step 2 — Loop diuretic (controversial): Furosemide (10 to 20 mg IV) was traditionally added once the patient was volume-replete, to block the sodium-calcium co-transporter in the thick ascending limb and promote calciuresis. Its use is now controversial — modern guidelines do not recommend routine use because adequate saline alone achieves calciuresis, and furosemide risks volume depletion and electrolyte disturbance (hypokalaemia, hypomagnesaemia). Reserve it for patients with fluid overload (heart failure) where saline is constrained. Never give furosemide before volume repletion — it worsens hypercalcaemia by contracting the intravascular volume. [1]
Step 3 — Antiresorptive therapy: IV zoledronic acid 4 mg infused over 15 minutes is the first-line antiresorptive agent [3]. It inhibits osteoclast-mediated bone resorption and lowers calcium over 2 to 4 days, with a nadir at 4 to 7 days and a duration of effect of 1 to 4 weeks. Dose-reduce in renal impairment (creatinine clearance 35 to 60: reduce to 3.5 mg; below 35: use with caution or consider denosumab). Denosumab (subcutaneous 120 mg on days 1, 8, 15, and 29, then monthly) is an alternative when bisphosphonates are contraindicated (severe renal impairment) — it is not renally excreted and is effective [3].
Step 4 — Calcitonin for rapid bridge: Calcitonin (4 to 8 IU/kg subcutaneously or intramuscularly every 12 hours) lowers calcium within hours by inhibiting osteoclasts and increasing renal calcium excretion. It is useful as a bridge while waiting for zoledronic acid to take effect (the first 48 hours). However, tachyphylaxis develops after approximately 48 hours — calcitonin alone is not adequate for sustained control. [1]
Step 5 — Glucocorticoids for specific causes: Prednisolone 20 to 40 mg daily (or hydrocortisone 200 mg IV daily) is indicated when the hypercalcaemia is granulomatous (sarcoidosis, TB) or vitamin D mediated — it suppresses the macrophage 1-alpha-hydroxylase and reduces intestinal calcium absorption. It is ineffective for PHPT and most malignancy-associated hypercalcaemia (except lymphoma, which often responds). [1]
Step 6 — Dialysis: Haemodialysis is reserved for severe hypercalcaemia refractory to the above, or when bisphosphonates are contraindicated and renal failure prevents saline-induced calciuresis. It is the fastest way to lower calcium (within hours) but is a temporary measure. [1]
DWE high-yield: The order and rationale — saline first (always, immediately), then a bisphosphonate (zoledronic acid 4 mg IV over 15 minutes) for the sustained calcium-lowering effect, calcitonin as a bridge for the first 48 hours while the bisphosphonate works, and glucocorticoids only if the cause is granulomatous or vitamin D mediated. Furosemide is not routine. Dialysis is the rescue therapy. [1]
Hypocalcaemia
Causes — the discriminating framework
Hypocalcaemia is defined as corrected calcium below 2.1 mmol/L (or ionised below 1.1 mmol/L). As with hypercalcaemia, the first step is to measure PTH — this divides the causes: [1]
| PTH | Category | Common causes |
|---|---|---|
| Low (inappropriately low for the hypocalcaemia) | Hypoparathyroidism | Post-surgical (commonest), autoimmune (APS1), congenital (DiGeorge 22q11.2), infiltrative (haemochromatosis), radiation |
| High (appropriate compensatory response) | PTH-resistant or vitamin D deficient | CKD, vitamin D deficiency, malabsorption, pseudohypoparathyroidism, hypomagnesaemia, pancreatitis, Fanconi syndrome, severe liver disease |
Post-thyroidectomy or post-parathyroidectomy hypocalcaemia is the commonest acute cause of hypocalcaemia in hospital. The mechanism is direct damage to, devascularisation of, or removal of the parathyroid glands. Check calcium within 6 to 12 hours post-operatively and monitor daily. Transient hypoparathyroidism (lasting days to weeks) is common; permanent hypoparathyroidism (persisting beyond 6 months) occurs in 1 to 5% of total thyroidectomies [5].
Autoimmune hypoparathyroidism is a component of autoimmune polyglandular syndrome type 1 (APS1) — an autosomal recessive AIRE gene mutation causing mucocutaneous candidiasis, hypoparathyroidism, and Addison disease. Hypoparathyroidism is usually the first endocrine manifestation (presents in childhood). [1]
DiGeorge syndrome (22q11.2 deletion) causes congenital thymic and parathyroid aplasia presenting with neonatal hypocalcaemia, cardiac defects (conotruncal), and characteristic facies. [1]
Vitamin D deficiency is extremely common, particularly in dark-skinned individuals, the housebound elderly, and those with malabsorption (coeliac disease, inflammatory bowel disease, post-bariatric surgery). Severe deficiency (25-hydroxyvitamin D below 25 nmol/L) causes secondary hyperparathyroidism and, if prolonged, osteomalacia. The PTH is elevated (appropriate), and ALP is high (reflecting high bone turnover) [7].
CKD causes hypocalcaemia through phosphate retention (which complexes with calcium), reduced 1-alpha-hydroxylase activity (reduced calcitriol synthesis), and skeletal resistance to PTH. The PTH is elevated (secondary hyperparathyroidism). In advanced CKD (stage 5D), tertiary hyperparathyroidism can develop — the parathyroid glands become autonomous and hypercalcaemia supervenes. [1]
Hypomagnesaemia is the often-missed cause of refractory hypocalcaemia. Magnesium is required for PTH secretion and for adenylate cyclase signalling at the PTH receptor target organs. Severe hypomagnesaemia (below 0.4 mmol/L) causes functional hypoparathyroidism — PTH secretion is impaired and target-organ responsiveness is blunted. The PTH is low or inappropriately normal. The calcium will not correct until the magnesium is repleted — this is a classic exam point [5].
Acute pancreatitis causes hypocalcaemia by saponification of calcium with free fatty acids released by pancreatic lipase in the retroperitoneum. It is a marker of severity. [1]
Fanconi syndrome (generalised proximal tubular dysfunction) causes hypocalcaemia through renal phosphate wasting, hypokalaemia, and acidosis; it may be inherited (cystinosis) or acquired (tenofovir, ifosfamide, multiple myeloma). [1]
Clinical features
The clinical features of hypocalcaemia reflect neuromuscular irritability and CNS dysfunction: [1]
- Neuromuscular: Perioral and digital paraesthesia, muscle cramps, carpopedal spasm, laryngospasm, bronchospasm, tetany.
- CNS: Irritability, anxiety, seizures (generalised or focal), confusion, and in chronic cases, extrapyramidal movement disorders from basal ganglia calcification.
- Cardiovascular: Prolonged QT interval on ECG (risk of torsades de pointes), decreased contractility, hypotension. [1]
Bedside signs:
- Chvostek sign — tapping the facial nerve (at the parotid, anterior to the ear) causes ipsilateral twitching of the facial muscles (upper lip). Present in approximately 10 to 25% of normocalcaemic individuals, so not highly specific.
- Trousseau sign — inflation of a blood pressure cuff above systolic for 3 minutes causes carpal spasm (main d'accoucheur — obstetrician's hand). More specific than Chvostek. [1]
Chronic hypocalcaemia (as in longstanding hypoparathyroidism) causes basal ganglia calcification (visible on CT), subcapsular cataracts, and dry, coarse skin with brittle nails. These are long-term complications of untreated disease [5].
Management
Acute symptomatic hypocalcaemia (tetany, seizures, prolonged QT, stridor):
- IV calcium gluconate 10% — 10 to 20 mL (1 to 2 g) over 10 minutes, diluted in 50 to 100 mL of 5% dextrose or normal saline, with cardiac monitoring. This is followed by a continuous infusion (calcium gluconate 100 mL of 10% in 1 L normal saline at 50 mL/h, titrated to corrected calcium) until symptoms resolve and oral therapy is established.
- Always check and correct magnesium — give IV magnesium sulfate 2 to 4 g if hypomagnesaemic.
- Calcium gluconate is preferred over calcium chloride for peripheral venous access (chloride is highly irritant and requires a central line). [1]
Chronic hypocalcaemia (hypoparathyroidism, CKD, post-surgical):
- Oral calcium — calcium carbonate 1 to 2 g (elemental) two to three times daily, or calcium citrate (preferred in patients on PPIs or with achlorhydria, as it does not require acid for absorption). [1]- Active vitamin D (calcitriol, 1,25-dihydroxyvitamin D) — 0.25 to 1.0 micrograms daily — is necessary for hypoparathyroidism and CKD because these patients cannot convert 25-OH-D to its active form. The dose is titrated to maintain calcium in the low-normal range (to avoid hypercalciuria and nephrolithiasis).
- Cholecalciferol (vitamin D3) loading — 50 000 IU weekly for 6 to 8 weeks, then 1000 to 2000 IU daily — for simple vitamin D deficiency (intact renal function and PTH axis).
- Recombinant human PTH (1-84) (natpara) — once-daily subcutaneous injection for refractory hypoparathyroidism, reduces calcium and calcitriol requirements. The 2016 guideline recommends it for patients uncontrolled on conventional therapy (symptomatic hypocalcaemia, hypercalciuria, hyperphosphataemia, or very high doses of calcium and calcitriol) [5].
DWE trap: A patient 2 days post-total thyroidectomy develops perioral tingling and carpopedal spasm. Corrected calcium is 1.6 mmol/L. The immediate management is IV calcium gluconate — this is an emergency. Do not wait for oral therapy to work. Check magnesium simultaneously. Once stabilised, transition to oral calcium and calcitriol, with a plan to reassess parathyroid recovery over weeks to months. [1]
Osteoporosis

Osteoporosis is a skeletal disorder characterised by compromised bone strength predisposing to an increased risk of fracture. Bone strength reflects the integration of bone density and bone quality. The clinical definition is operationalised by the DEXA T-score [6]:
| T-score | Category |
|---|---|
| Above -1.0 | Normal |
| -1.0 to -2.5 | Osteopenia (low bone mass) |
| Below -2.5 | Osteoporosis |
| Below -2.5 plus a fragility fracture | Severe (established) osteoporosis |
The T-score compares the patient's bone mineral density to that of a healthy young adult reference population (expressed in standard deviations). The Z-score (comparison to age- and sex-matched peers) is used for premenopausal women and men under 50 — a Z-score below -2.0 is defined as below the expected range for age. [1]
Risk factors and FRAX
The FRAX tool (Fracture Risk Assessment Tool, developed by the WHO Collaborating Centre at Sheffield) integrates clinical risk factors with or without femoral neck BMD to estimate the 10-year probability of major osteoporotic fracture (hip, clinical spine, proximal humerus, distal forearm) and hip fracture specifically. The clinical risk factors in FRAX are: [1]
- Age, sex, body mass index (below 20 or above the normal range matters)
- Previous fragility fracture (the strongest single risk factor)
- Parental history of hip fracture
- Current tobacco smoking
- Long-term oral glucocorticoid use (5 mg prednisolone or more daily for 3 months or longer) [1]- Rheumatoid arthritis
- Secondary osteoporosis (type 1 diabetes, untreated thyrotoxicosis, hypogonadism, chronic malabsorption, chronic liver disease, premature menopause below 45 years)
- Alcohol intake of 3 or more units per day [1]
Treatment thresholds (ANZ/NOGG/NICE aligned):
- T-score below -2.5 at any site — treat.
- Prior fragility fracture (hip or vertebral) — treat regardless of T-score.
- FRAX 10-year hip fracture probability at or above 3% or major osteoporotic fracture probability at or above 20% — treat (these are the AACE and Endocrine Society thresholds; NOGG uses age-specific thresholds).
- Patients on long-term glucocorticoids — treat at lower thresholds (the GC-adjusted FRAX is available). [1]
Treatment
First-line — bisphosphonates: Bisphosphonates are synthetic analogues of pyrophosphate that bind hydroxyapatite in bone and inhibit osteoclast-mediated resorption. They are the first-line treatment for osteoporosis [6]:
- Alendronate 70 mg orally once weekly — the most widely used and best-studied. Take fasting, with a full glass of water, and remain upright (sitting or standing) for at least 30 minutes before food or other medications. Oesophageal irritation, oesophagitis, and rarely oesophageal ulceration are the principal adverse effects — contraindicated in patients with Barrett oesophagus, strictures, achalasia, or inability to remain upright.
- Zoledronic acid 5 mg IV infusion over 15 minutes once yearly — for patients who cannot tolerate or adhere to oral therapy, or with malabsorption. The acute-phase reaction (fever, myalgia, arthralgia) occurs in approximately 10 to 30% after the first dose and is less common subsequently. Dental review before starting is advisable (risk of osteonecrosis of the jaw).
- Risedronate 35 mg orally once weekly or 150 mg once monthly — an alternative oral agent with a similar adverse-effect profile to alendronate. [1]
Drug holiday: After 3 to 5 years of oral bisphosphonate therapy (or 3 annual zoledronic acid infusions), reassess fracture risk. For patients at low-to-moderate risk (no prior fracture, moderate T-score), a drug holiday of 1 to 2 years is reasonable — the antiresorptive effect persists in bone for years after cessation due to the drug's skeletal retention. For patients at high risk (prior fracture, very low T-score below -2.5, or on glucocorticoids), continue therapy or switch agents [6].
DWE high-yield: The two rare but feared complications of long-term bisphosphonate therapy are atypical femoral fractures (prodromal thigh or groin pain, characteristic transverse or short-oblique fracture of the subtrochanteric or diaphyseal femur — investigate with a full-length femur X-ray or MRI if there is prodromal pain, and stop the bisphosphonate) and osteonecrosis of the jaw (exposed necrotic bone in the mandible or maxilla persisting for more than 8 weeks, particularly after dental extraction — refer to maxillofacial). Both are rare (approximately 1 per 10 000 to 1 per 100 000 patient-years) but the risk increases with duration of therapy. [1]
Denosumab: Denosumab is a monoclonal antibody that binds and neutralises RANKL, preventing osteoclast formation and activation. It is given as 60 mg subcutaneously every 6 months. It is an excellent alternative to bisphosphonates (not nephrotoxic, no gastrointestinal side effects, and at least as effective at reducing fractures). However, its effect is fully reversible on cessation — there is a rebound increase in bone resorption and a real risk of multiple vertebral fractures in the months after stopping. Denosumab should not be stopped without a plan to transition to an oral bisphosphonate to prevent this rebound [6].
Anabolic therapy — teriparatide: Teriparatide is recombinant human PTH (1-34), the first 34 amino acids of PTH. Given once-daily subcutaneously (20 micrograms), it has a paradoxical anabolic effect — intermittent low-dose PTH stimulates osteoblast activity and new bone formation (in contrast to continuous endogenous PTH, which is catabolic and causes bone resorption in primary hyperparathyroidism). Teriparatide is reserved for very high-risk patients — those with severe osteoporosis (T-score below -3.5), multiple fragility fractures, or fractures on bisphosphonate therapy. It is given for a maximum of 2 years (lifetime limit due to rat osteosarcoma data, though human risk appears negligible). After the course, transition to an antiresorptive to preserve the bone gained [6].
Hormone replacement therapy and SERMs: Oestrogen replacement (combined oestrogen-progestogen in women with a uterus, or oestrogen alone after hysterectomy) prevents bone loss and reduces fractures, but the risks (breast cancer, venous thromboembolism, stroke, coronary events — from the Women's Health Initiative) limit its use to women under 60 within 10 years of menopause for vasomotor symptoms, with bone protection as a secondary benefit. It is not first-line for osteoporosis alone. [1]
Raloxifene, a selective oestrogen receptor modulator (SERM), has oestrogen-agonist effects on bone (reduces vertebral fractures) and oestrogen-antagonist effects on breast (reduces oestrogen-receptor-positive breast cancer) and uterus. It increases the risk of venous thromboembolism (similar to oestrogen) and can cause hot flushes. It is an alternative for postmenopausal women with a lower fracture risk, particularly those with breast cancer risk [6].
Calcium and vitamin D supplementation: All patients with osteoporosis should receive adequate calcium (1000 to 1200 mg elemental per day, ideally from diet) and vitamin D (800 to 1000 IU daily, or enough to maintain 25-hydroxyvitamin D above 50 nmol/L). Supplements alone do not reduce fracture risk in community-dwelling adults without deficiency, but they are essential adjuncts to pharmacotherapy. [1]
DCE long-case integration: When presenting a patient with osteoporosis in the long case, state the T-score, the FRAX 10-year probability, the prior fractures, the secondary causes you have excluded (hyperthyroidism, hyperparathyroidism, hypogonadism, malabsorption, myeloma, glucocorticoids), and your treatment choice with its rationale, monitoring plan (repeat DEXA at 2 years, bone turnover markers if desired), and the drug-holiday decision point. [1]
Osteomalacia
Osteomalacia (literally soft bone) is the defective mineralisation of osteoid in adults (rickets is the equivalent in children, before epiphyseal closure). The hallmark is unmineralised osteoid seams on bone histology. The commonest cause is vitamin D deficiency, but it also arises from phosphate wasting, chronic kidney disease, and inherited disorders of vitamin D metabolism [7].
Causes
| Category | Examples |
|---|---|
| Vitamin D deficiency | Inadequate sunlight, dietary deficiency, malabsorption (coeliac disease, IBD, post-bariatric), liver disease (impaired 25-hydroxylation), anticonvulsants (phenytoin, phenobarbitone — accelerate vitamin D catabolism) |
| Renal disease | CKD (reduced 1-alpha-hydroxylase), dialysis-related |
| Phosphate deficiency | Renal phosphate wasting (X-linked hypophosphataemic rickets/osteomalacia, Fanconi syndrome, tumour-induced osteomalacia — a phosphaturic mesenchymal tumour secreting FGF23), antacid abuse (phosphate binding) |
| Vitamin D-dependent rickets type 1 | 1-alpha-hydroxylase deficiency (autosomal recessive) |
| Vitamin D-dependent rickets type 2 | Vitamin D receptor mutation (hereditary resistance to vitamin D) |
| Hypophosphatasia | Mutated tissue-non-specific ALP gene |
Clinical features
The clinical features of osteomalacia are often subtle and overlooked:
- Diffuse bone pain (particularly axial skeleton — spine, pelvis, rib cage), worse on weight-bearing or palpation.
- Proximal muscle weakness (waddling gait, difficulty rising from a chair — due to the myopathy of vitamin D deficiency).
- Bone tenderness on palpation of the tibial shins, ribs, and pelvis.
- Fractures — particularly incomplete, stress, or subtrochanteric. [1]
Investigations
The classic biochemical pattern in vitamin D deficiency osteomalacia:
- 25-hydroxyvitamin D low (below 25 nmol/L for severe deficiency).
- ALP elevated — a key marker. The ALP is high because of increased osteoblast activity depositing unmineralised osteoid.
- Calcium low or low-normal; phosphate low or low-normal.
- PTH elevated (secondary hyperparathyroidism — appropriate compensatory response).
- 1,25-dihydroxyvitamin D may be normal or low (it is maintained by secondary hyperparathyroidism until very late). [1]
Pseudo-fractures (Looser zones) on X-ray are the radiological hallmark — symmetric, narrow (1 to 2 mm), radiolucent lines perpendicular to the cortex, typically in the medial femoral neck (the classic site), pubic rami, ribs, scapulae, and lateral border of the scapula. They are stress fractures through unmineralised osteoid and do not extend fully across the bone. [1]
DWE trap: A patient with bone pain, proximal myopathy, and an elevated ALP — think osteomalacia from vitamin D deficiency, not Paget disease (where the ALP is markedly elevated but the calcium and phosphate are normal, and the bone scan shows intensely hot lesions) or malignancy. The 25-hydroxyvitamin D will be low, and the PTH will be elevated (secondary hyperparathyroidism). [1]
Management
- Cholecalciferol (vitamin D3) loading — 50 000 IU weekly for 6 to 8 weeks, or 300 000 to 600 000 IU total, then maintenance 800 to 2000 IU daily [7].
- Calcium supplementation — 1000 to 1200 mg elemental daily.
- Correct the underlying cause — treat malabsorption (coeliac disease with gluten-free diet), stop offending drugs where possible, resect the phosphaturic tumour in tumour-induced osteomalacia.
- In CKD or hypoparathyroidism, use calcitriol (0.25 to 1 microgram daily) rather than cholecalciferol, because the 1-alpha-hydroxylation step is impaired. [1]
High-yield exam discriminators and pitfalls
-
PTH is the first test in any hypercalcaemia. A high or inappropriately normal PTH = primary hyperparathyroidism. A suppressed PTH = malignancy, granulomatous, vitamin D, drugs, or endocrine causes. Never treat hypercalcaemia without measuring PTH first (unless it is an emergency, in which case treat first and measure PTH concurrently). [1]
-
FHH mimics mild PHPT and does not need surgery. The calcium-to-creatinine clearance ratio is below 0.01. If you parathyroidectomise an FHH patient, the hypercalcaemia persists. [1]
-
Hypomagnesaemia causes refractory hypocalcaemia. The PTH is low or inappropriately normal. Replete magnesium first, then the calcium and PTH will correct. Missing this is a classic exam error. [1]
-
The order of emergency hypercalcaemia management: saline first, then zoledronic acid, calcitonin as a bridge for 48 hours, glucocorticoids for granulomatous or vitamin D mediated, dialysis for refractory renal failure. Furosemide is not routine. [1]
-
Denosumab rebound. Stopping denosumab without a transition bisphosphonate causes rapid bone loss and multiple vertebral fractures within months. Always have an exit plan. [1]
-
Teriparatide is anabolic, not antiresorptive. It is reserved for very high-risk patients and is time-limited to 2 years. After it, switch to an antiresorptive. [1]
-
Osteomalacia has an elevated ALP. The combination of bone pain, proximal myopathy, high ALP, low 25-hydroxyvitamin D, and elevated PTH (secondary hyperparathyroidism) is the pattern. [1]
-
Corrected calcium formula: add 0.02 mmol/L for every 1 g/L albumin below 40. Always correct before interpreting. [1]
-
Sarcoid hypercalcaemia responds to glucocorticoids. Do not give vitamin D; do give prednisolone. [1]
-
Post-thyroidectomy hypocalcaemia is the commonest acute cause. Check calcium within 6 to 12 hours, monitor daily, and give IV calcium gluconate for symptoms. [1]
Exam board facts
RACP DWE: Calcium disorders are well represented — expect MCQs on the PTH-based differential of hypercalcaemia, primary hyperparathyroidism criteria and management, emergency hypercalcaemia treatment sequencing, hypomagnesaemia and refractory hypocalcaemia, post-thyroidectomy hypocalcaemia, osteoporosis treatment selection (bisphosphonate vs denosumab vs teriparatide), and drug holidays. [1]
RACP DCE long case: The classic calcium long case is a multi-morbidity patient — primary hyperparathyroidism with osteoporosis and CKD, or hypercalcaemia of malignancy in a patient with advanced cancer, or post-surgical hypoparathyroidism with persistent symptoms — testing integrated management, problem-list synthesis, and the surgical versus medical decision. [1]
RACP DCE short case: Osteoporosis and the DEXA interpretation discussion is a favourite. Be ready to present a T-score, apply FRAX, discuss secondary causes, and outline a treatment plan with monitoring and the drug-holiday decision. [1]
MRCP Part 1/2: Hypercalcaemia causes (PTH-dependent vs PTH-independent), emergency management sequencing, and osteoporosis pharmacology (bisphosphonate mechanisms, denosumab, teriparatide, SERMs) are frequent. Chvostek and Trousseau signs, hypomagnesaemia, and FHH are common discriminating questions. [1]
MRCP PACES: Station 5 — endocrinology cases (primary hyperparathyroidism, osteoporosis discussion, post-thyroidectomy hypoparathyroidism). [1]
ABIM: Endocrinology comprises approximately 9% of the exam. Calcium disorders are core — diagnosis and management of hypercalcaemia (hyperparathyroidism, malignancy), hypocalcaemia (hypoparathyroidism, vitamin D deficiency), osteoporosis (DEXA, treatment), and osteomalacia. [1]
Key trials and guidelines to know cold
| Source | Topic | Key point |
|---|---|---|
| Fifth International Workshop PHPT (2022) [1] | Primary hyperparathyroidism | Current parathyroidectomy criteria; 24h urinary calcium thresholds updated |
| Fourth International Workshop PHPT (2014) [2] | Primary hyperparathyroidism | Predecessor guidelines; widely tested historical criteria |
| Endocrine Society Hypercalcemia of Malignancy (2023) [3] | Malignancy hypercalcaemia | Zoledronic acid and denosumab first-line; calcitonin as bridge |
| Society for Endocrinology Acute Hypercalcaemia (2016) [4] | Emergency management | Saline first; bisphosphonate second; furosemide not routine |
| Brandi Hypoparathyroidism Guideline (2016) [5] | Hypoparathyroidism | Calcium and calcitriol first-line; recombinant PTH (1-84) for refractory |
| AACE/ACE Osteoporosis (2020) [6] | Osteoporosis | High vs very-high risk stratification; anabolic-first for very high risk |
| Holick Vitamin D Guideline (2011) [7] | Vitamin D deficiency | Deficiency below 50 nmol/L; loading and maintenance doses |
| Stewart Hypercalcemia of Malignancy NEJM (2005) [8] | PTHrP mechanism | Definitive review of humoral vs local osteolytic hypercalcaemia |
Communication and shared decision-making
The choice between surgery and monitoring in asymptomatic PHPT is genuinely shared with the patient. The consultation framework: [1]
- Elicit the patient's understanding and goals — symptom burden, kidney stone history, concerns about surgery, anxiety about a parathyroid tumour.
- Present the evidence honestly — surgery is the only cure; cinacalcet controls the calcium but not the bone density; monitoring is safe in most asymptomatic patients who meet the criteria, but some will progress.
- Discuss the surgical risk — cure rate 95% or higher in experienced hands for single adenoma; risks include recurrent laryngeal nerve injury, permanent hypoparathyroidism, and failed exploration.
- Document the decision and review annually with biochemistry and DEXA. [1]
For the osteoporosis patient, frame the condition as common, treatable, and manageable — the goal is fracture prevention. Discuss the bisphosphonate benefit-to-harm ratio honestly (the fracture risk reduction is real and substantial; the rare complications are just that — rare). Address the patient's fear of the rare side-effects (atypical fracture, osteonecrosis of the jaw) with the actual numbers, and involve the patient in the drug-holiday decision. [1]
References and further reading
Fifth International Workshop on Primary Hyperparathyroidism (2022) [1]. Fourth International Workshop on Primary Hyperparathyroidism (2014) [2]. Endocrine Society Clinical Practice Guideline — Treatment of Hypercalcemia of Malignancy in Adults (2023) [3]. Society for Endocrinology Endocrine Emergency Guidance — Emergency Management of Acute Hypercalcaemia in Adult Patients (2016) [4]. Management of Hypoparathyroidism — Summary Statement and Guidelines (2016) [5]. AACE/ACE Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis — 2020 Update [6]. Endocrine Society Clinical Practice Guideline — Evaluation, Treatment, and Prevention of Vitamin D Deficiency (2011) [7]. Stewart AF — Hypercalcemia Associated with Cancer, NEJM (2005) [8]. Endocrine Society of Australia position statements. Osteoporosis Australia / Healthy Bones Australia guidelines. NICE Technology Appraisal TA464 (bisphosphonates for treating osteoporosis). Royal Osteoporosis Society guidance.
References
- [1]Bilezikian JP, Khan AA, Silverberg SJ, et al. Evaluation and Management of Primary Hyperparathyroidism: Summary Statement and Guidelines from the Fifth International Workshop J Bone Miner Res, 2022.PMID 36245251
- [2]Bilezikian JP, Khan AA, Potts JT Jr, et al. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Fourth International Workshop J Clin Endocrinol Metab, 2014.PMID 25162665
- [3]El-Hajj Fuleihan G, Cloutier MD, Beltrand J, et al. Treatment of Hypercalcemia of Malignancy in Adults: An Endocrine Society Clinical Practice Guideline J Clin Endocrinol Metab, 2023.PMID 36545746
- [4]Baggott A, Cardozo L, Frost J, et al. SOCIETY FOR ENDOCRINOLOGY ENDOCRINE EMERGENCY GUIDANCE: Emergency management of acute hypercalcaemia in adult patients Endocr Connect, 2016.PMID 27935816
- [5]Brandi ML, Bilezikian JP, Shoback D, et al. Management of Hypoparathyroidism: Summary Statement and Guidelines J Clin Endocrinol Metab, 2016.PMID 26943719
- [6]Camacho PM, Petak SM, Binkley N, et al. AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS/AMERICAN COLLEGE OF ENDOCRINOLOGY CLINICAL PRACTICE GUIDELINES FOR THE DIAGNOSIS AND TREATMENT OF POSTMENOPAUSAL OSTEOPOROSIS-2020 UPDATE Endocr Pract, 2020.PMID 32427503
- [7]Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline J Clin Endocrinol Metab, 2011.PMID 21646368
- [8]Stewart AF Clinical practice. Hypercalcemia associated with cancer N Engl J Med, 2005.PMID 15673803