Phys · endocrine
Diabetes Mellitus
Also known as type 1 diabetes · type 2 diabetes · T1DM · T2DM · diabetes mellitus · insulin-dependent diabetes · non-insulin-dependent diabetes · LADA · MODY · latent autoimmune diabetes in adults · maturity-onset diabetes of the young · gestational diabetes · diabetic nephropathy · diabetic retinopathy · diabetic neuropathy · diabetic foot
Consultant-physician-depth guide to diabetes mellitus — pathophysiology, classification, diagnosis, glycaemic target individualisation, the modern pharmacological hierarchy for type 2, insulin therapy, microvascular and macrovascular complications, diabetic foot, glycaemic emergencies, diabetes in pregnancy, and diabetes technology — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Diabetes Mellitus
The answer first
Diabetes mellitus is a group of metabolic disorders defined by chronic hyperglycaemia resulting from defects in insulin secretion, insulin action, or both. The core classification is binary in practice but plural in reality: type 1 (absolute insulin deficiency from autoimmune beta-cell destruction) and type 2 (insulin resistance with progressive beta-cell failure) — together more than 95% of all cases. The remainder are specific monogenic (MODY), pancreatic (type 3c), drug-induced, and gestational forms that the physician must not miss because they change treatment. [1]
The diagnostic threshold is one of the most testable facts in physician exams: HbA1c of 48 mmol/mol (6.5%) or above on two occasions, or a fasting glucose of 7.0 mmol/L or above, or a 2-hour OGTT glucose of 11.1 mmol/L or above. In a symptomatic patient, a single random glucose of 11.1 mmol/L or above is diagnostic. [1]
The management logic for type 2 diabetes has been rewritten by the cardiovascular and renal outcome trials. The modern hierarchy is: lifestyle plus metformin, then add an SGLT2 inhibitor or GLP-1 receptor agonist chosen for the patient's cardiorenal profile — before escalating through insulin or sulphonylureas. Glucose-lowering is no longer the sole goal. In a patient with established atherosclerotic disease, heart failure, or chronic kidney disease, the organ-protective agent is the second-line drug regardless of HbA1c. [1]
Classification and the non-type-1/non-type-2 diagnoses
The single most dangerous classification error is mislabelling type 1 as type 2 in a thin adult with progressive insulin failure. These patients are sent home on escalating doses of oral agents and re-present in DKA. The four non-obvious subtypes to know cold: [1]
Latent autoimmune diabetes in adults (LADA) accounts for up to 10% of adult-onset diabetes. The clinical signature is: age over 30, autoimmune positivity (anti-GAD65 is the first test; anti-IA2 and zinc transporter-8 antibodies extend the panel), absence of the metabolic syndrome phenotype, and progressive insulin requirement within 6 years. LADA is type 1 diabetes presenting slowly. The practical rule: check a GAD65 antibody in any adult who is not stereotypically type 2 (lean, rapid glycaemic failure on oral agents, personal or family history of autoimmune disease). [1]
Maturity-onset diabetes of the young (MODY) is a monogenic autosomal dominant disorder — a family history across at least two generations with onset before 25 years and sustained endogenous insulin (no insulin requirement, C-peptide preserved). The most common form, HNF1A-MODY (MODY 3), is exquisitely sulphonylurea-sensitive — small doses of gliclazide are first-line and patients may be over-treated with insulin in error. HNF4A-MODY (MODY 1) is similar. GCK-MODY (MODY 2) is benign fasting hyperglycaemia (5.5 to 8.5 mmol/L from birth) that does not require treatment outside pregnancy and is often mislabelled as gestational diabetes. Genetic testing confirms the diagnosis and frequently changes management. [1]
Type 3c diabetes (pancreatogenic) follows pancreatic destruction — chronic pancreatitis, pancreatic ductal adenocarcinoma, cystic fibrosis, haemochromatosis, or pancreatectomy. The hallmarks are pancreatic exocrine insufficiency, low C-peptide, and a tendency to severe brittle hypoglycaemia because both glucagon and insulin secretion are lost. These patients often need pancreatic enzyme replacement and have an unpredictable response to exogenous insulin. [1]
| Feature | Type 1 | Type 2 | LADA | MODY | Type 3c |
|---|---|---|---|---|---|
| Onset age | Any, peak pubertal | Usually adult | Over 30 | Under 25 | Any |
| Body habitus | Often lean | Often obese | Variable | Variable | Variable |
| Antibodies | Positive (anti-GAD, IA2, ZnT8) | Negative | Anti-GAD positive | Negative | Negative |
| C-peptide | Low/absent | Normal or high initially | Falls over years | Preserved | Low |
| Insulin need | Immediate | Late course | Within months to years | Usually not (except MODY 1/3 may use SU) | Variable |
| Family history | Autoimmune clustering | T2DM, metabolic syndrome | Autoimmune | Autosomal dominant, 2+ generations | Pancreatic disease |
DWE trap: "A 32-year-old lean woman, BMI 22, presents with new diabetes, HbA1c 75 mmol/mol, no weight loss. Her father has hypothyroidism. What is the next investigation?" The answer is anti-GAD65 antibody — to diagnose LADA. Do not default to oral hypoglycaemics in a non-stereotypical type 2 patient. [1]
Pathophysiology — why the mechanism drives management
Type 1 diabetes is a T-cell-mediated autoimmune destruction of pancreatic beta cells. Autoantibodies (GAD65, IA-2, insulin autoantibody, ZnT8) are markers, not the effector mechanism. The autoimmune attack proceeds silently for months to years; by the time of symptomatic hyperglycaemia, approximately 80 to 90% of beta-cell mass is gone. The clinical consequence is absolute insulin deficiency — insulin replacement is non-negotiable from diagnosis. Without exogenous insulin, the patient develops ketoacidosis within days to weeks. The DCCT established that intensive insulin therapy (basal-bolus or pump) reduces microvascular complications by 35 to 76% in type 1 diabetes, at the cost of a threefold increase in severe hypoglycaemia. [1]
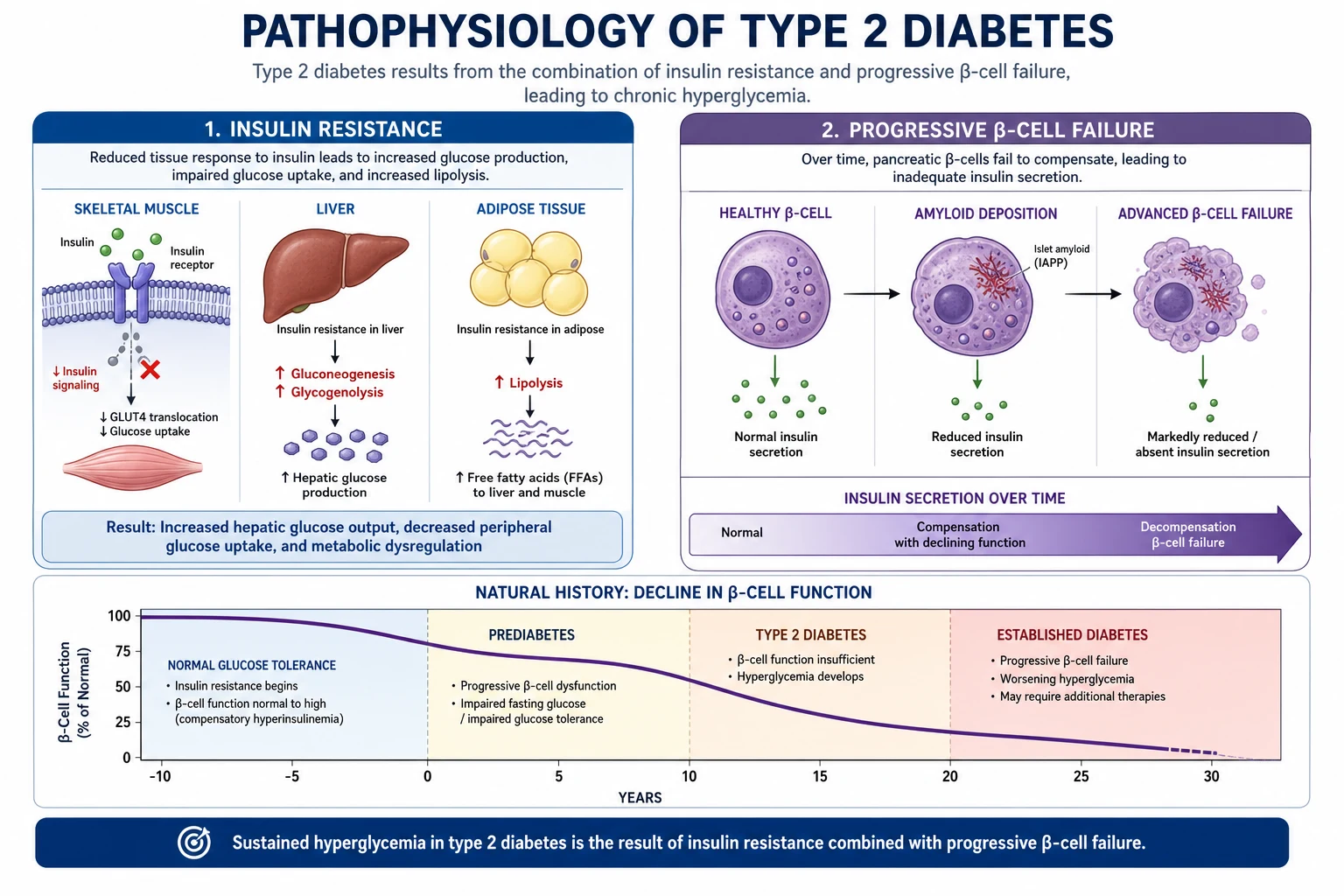
Type 2 diabetes is a dual defect: insulin resistance (impaired insulin-mediated glucose uptake in muscle and adipose, and impaired suppression of hepatic gluconeogenesis) combined with progressive beta-cell failure. Insulin resistance begins years before diagnosis and is driven by visceral adiposity, inactivity, genetics, and lipotoxicity. The beta cell initially compensates with hyperinsulinaemia, maintaining euglycaemia; over time, beta-cell function declines by approximately 4 to 6% per year, and fasting and postprandial glucose rise. The progressive beta-cell failure is the reason type 2 diabetes is a progressive disease requiring stepwise escalation — and the reason most patients eventually need insulin. [1]
The UKPDS established that in type 2 diabetes, intensive glycaemic control (median HbA1c 53 mmol/mol vs 63 mmol/mol) reduces microvascular complications by 25%, with a non-significant trend toward reduced myocardial infarction. The post-trial follow-up (UKPDS 80) revealed the legacy effect (metabolic memory): despite convergence of HbA1c after the trial ended, the intensive group showed persistent reductions in microvascular disease, myocardial infarction (15%), and all-cause mortality (13%) at 10 years. This is why early intensive control matters — a window of opportunity exists early in the disease. [1]
The ACCORD trial provided the counterpoint: in older patients with long-standing type 2 diabetes and established cardiovascular disease, intensive glycaemic targeting (HbA1c below 42 mmol/mol) increased mortality by 22%. The synthesis is: aggressive in newly diagnosed younger patients; cautious in older patients with comorbidity and established disease. Glycaemic targets must be individualised. [1]
Diagnosis
The diagnosis is laboratory-based, not capillary. Three equivalent diagnostic criteria — any one suffices in an asymptomatic patient if confirmed on a separate day: [1]
| Test | Threshold | Notes |
|---|---|---|
| HbA1c | 48 mmol/mol (6.5%) or above | Reflects mean glycaemia over 8 to 12 weeks. Falsely low in haemolysis, recent transfusion, pregnancy, uraemia. Confirm with a second sample. |
| Oral glucose tolerance test (2-hour) | 11.1 mmol/L or above | Use when HbA1c is discordant with glucose, or in haemoglobinopathy. |
| Random plasma glucose | 11.1 mmol/L or above | Diagnostic only in a symptomatic patient (polyuria, polydipsia, weight loss). |
Prediabetes — impaired fasting glucose (6.1 to 6.9 mmol/L) or impaired glucose tolerance (OGTT 7.8 to 11.0 mmol/L) or HbA1c 39 to 46 mmol/mol — identifies patients at high risk. Lifestyle intervention reduces progression to diabetes by approximately 58% (DPP), more than metformin (31%). [1]
DCE insight: Do not diagnose diabetes from a single point-of-care capillary glucose. Always send a laboratory HbA1c and fasting glucose. In the acutely unwell or steroid-treated patient, HbA1c may be misleading — use paired glucose values and re-test when stable. [1]
Glycaemic targets — individualise, do not standardise
The general HbA1c target for most adults is 53 mmol/mol (7.0%) or below. This is not universal. The target is a clinical decision weighing three factors: age and life expectancy, comorbidity burden, and hypoglycaemia risk. [1]
| Patient profile | Target HbA1c | Rationale |
|---|---|---|
| Young, newly diagnosed, no comorbidity | 48 to 53 mmol/mol (6.5 to 7.0%) | Microvascular prevention; legacy effect |
| Older with comorbidity, limited life expectancy | 58 to 64 mmol/mol (7.5 to 8.0%) | Avoid hypoglycaemia; ACCORD harm signal |
| Frail elderly, end-stage disease, frequent hypoglycaemia | 64 mmol/mol (8.0%) or below | Quality of life; avoid harm |
| Pregnancy (pre-existing diabetes) | 42 mmol/mol (6.0%) or below | Congenital malformation and macrosomia prevention |
The ACCORD trial is the evidence for caution: in patients with established cardiovascular disease and a mean diabetes duration of 10 years, targeting HbA1c below 42 mmol/mol increased mortality by 22% and was stopped early. The mechanisms include severe hypoglycaemia, polypharmacy, and possibly the harm of rapid glycaemic correction. The lesson: the older, sicker patient is harmed by aggressive glycaemic control — focus on blood pressure, lipids, smoking cessation, and organ-protective agents instead. [1]
Management hierarchy for type 2 diabetes
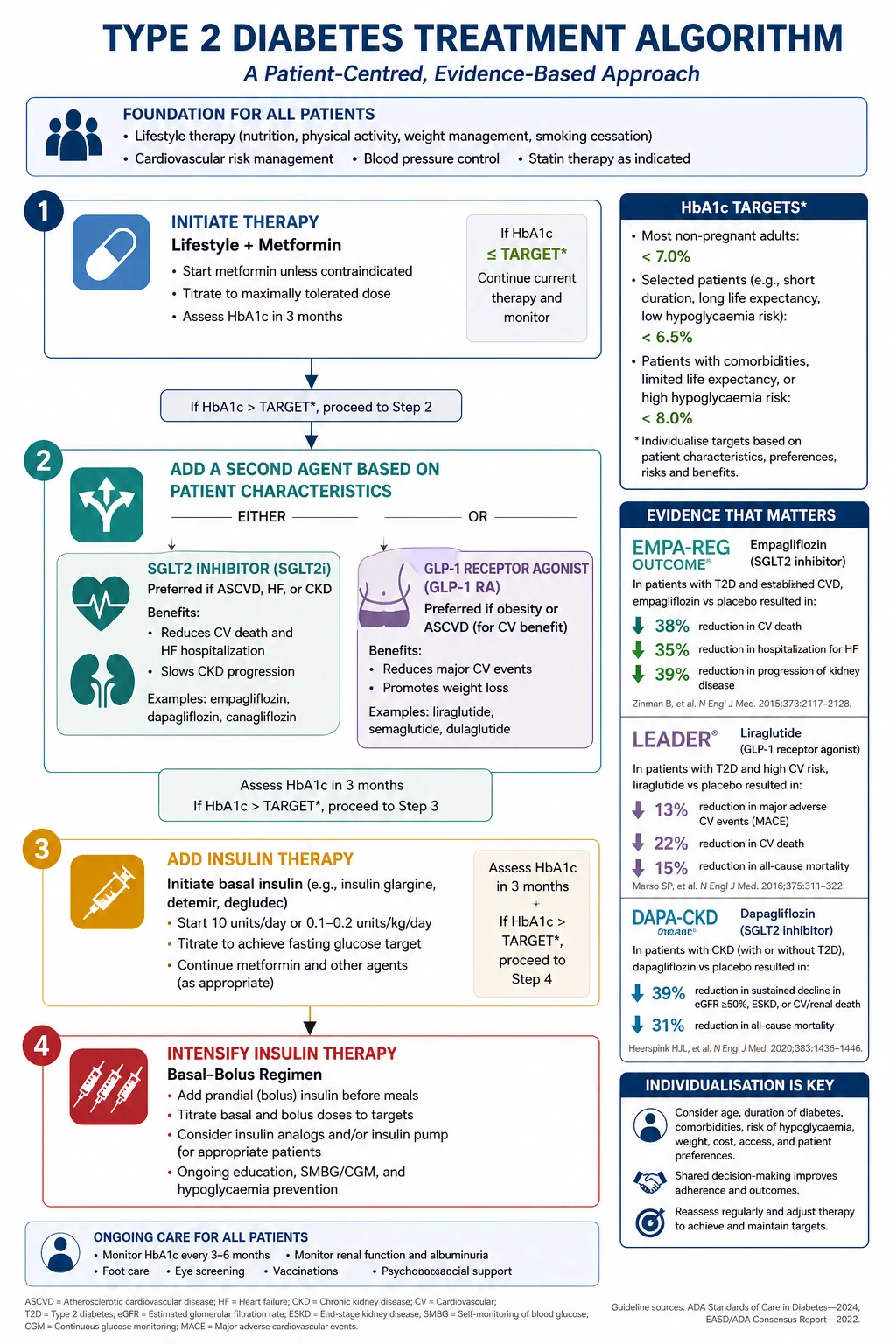
The modern algorithm is built on a single principle: treat the patient's cardiorenal risk, not just the HbA1c. The glucose number matters, but in a patient with atherosclerotic cardiovascular disease, heart failure, or chronic kidney disease, the drug choice is dictated by the organ it protects. [1]
Step 1 — Lifestyle and education. Medical nutrition therapy (Mediterranean or low-carbohydrate pattern, 5 to 7% weight loss), 150 minutes per week of moderate exercise, smoking cessation, and structured diabetes education. These alone reduce HbA1c by 1 to 2%. [1]
Step 2 — First-line pharmacotherapy: metformin. Metformin (start 500mg once daily, titrate to 1000mg twice daily with meals) reduces hepatic gluconeogenesis, is weight-neutral or weight-losing, has a low hypoglycaemia risk, and is inexpensive. The UKPDS established its cardiovascular and mortality benefit in overweight patients with newly diagnosed type 2 diabetes. It is contraindicated in severe renal impairment (eGFR below 30), and the dose is halved at eGFR 30 to 45. The feared complication is lactic acidosis — rare (approximately 3 per 100,000 patient-years) but occurs in acidaemic, hypoxic, or severely renally impaired patients. Withhold metformin perioperatively and during acute illness with haemodynamic instability. Long-term use causes vitamin B12 deficiency — check levels in patients on metformin for over 4 years with neuropathy or macrocytosis. [1]
Step 3 — Second-line: organ-protective agents, chosen by comorbidity. This is the paradigm shift. For most patients needing a second agent, the choice is between an SGLT2 inhibitor and a GLP-1 receptor agonist, selected by the patient's cardiorenal profile: [1]
| Patient profile | Preferred second agent | Evidence anchor |
|---|---|---|
| Established atherosclerotic cardiovascular disease | GLP-1 RA (liraglutide, semaglutide, dulaglutide) or SGLT2i (empagliflozin, canagliflozin) | LEADER, SUSTAIN-6, EMPA-REG OUTCOME |
| Heart failure (HFrEF or HFpEF) | SGLT2i (dapagliflozin, empagliflozin) | DAPA-HF, EMPEROR-Reduced |
| Chronic kidney disease | SGLT2i (dapagliflozin) | DAPA-CKD |
| Neither ASCVD, HF, nor CKD — focus on glycaemic and weight targets | GLP-1 RA or SGLT2i if weight loss desired; consider DPP-4 inhibitor, pioglitazone, or SU if cost-driven | SURPASS-2 (tirzepatide) |
SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin, ertugliflozin) reduce proximal tubular glucose reabsorption, causing glycosuria. The EMPA-REG OUTCOME trial showed empagliflozin reduced cardiovascular death by 38% and all-cause mortality by 32% in patients with type 2 diabetes and established cardiovascular disease — a result that reshaped the field. The DAPA-CKD trial extended this: dapagliflozin reduced the composite of worsening kidney function, end-stage kidney disease, or renal/cardiovascular death by 39%, in patients with and without diabetes. SGLT2 inhibitors are now a class recommended for heart failure and CKD regardless of diabetes status. Adverse effects: genital mycotic infection, volume depletion (reduce diuretics when starting), an uncommon risk of euglycaemic diabetic ketoacidosis (present with ketones, not high glucose — risk in perioperative fasting, insulin reduction, intercurrent illness), and a small amputation signal with canagliflozin (CANVAS) not seen with other agents. [1]
GLP-1 receptor agonists (liraglutide, semaglutide, dulaglutide, tirzepatide) mimic incretin, stimulating glucose-dependent insulin secretion, suppressing glucagon, slowing gastric emptying, and reducing appetite. The LEADER trial (liraglutide) reduced the composite of cardiovascular death, nonfatal MI, or nonfatal stroke by 13% and cardiovascular death by 22%. SUSTAIN-6 (semaglutide) showed a 26% MACE reduction, driven by nonfatal stroke. SURPASS-2 (tirzepatide, a dual GIP/GLP-1 agonist) showed superior HbA1c and weight reduction versus semaglutide — the most efficacious glycaemic and weight agent available. These agents are first choice for the obese patient with type 2 diabetes. Adverse effects: nausea and vomiting (titrate slowly), pancreatitis (uncommon, stop if suspected), and the SUSTAIN-6 retinopathy signal — more retinopathy complications with semaglutide, likely from rapid glycaemic improvement in patients with pre-existing proliferative disease (screen and treat retinopathy before aggressive escalation). [1]
Step 4 — Third-line and beyond. If HbA1c remains above target on dual therapy, add a third agent guided by the same principles, or progress to insulin. DPP-4 inhibitors (sitagliptin, linagliptin) are weight-neutral, modestly effective, and safe but have no cardiovascular benefit and are less potent than GLP-1 RAs. Pioglitazone reduces insulin resistance and has a secondary stroke prevention signal (IRIS) but causes fluid retention (avoid in heart failure), weight gain, and an increased fracture risk in women. Sulphonylureas (gliclazide, glipizide) stimulate insulin secretion, are cheap and effective, but cause weight gain and hypoglycaemia and have a weaker cardiovascular safety profile — now third- or fourth-line. Avoid glyburide (glibenclamide) in older patients and renal impairment — long-acting, high hypoglycaemia risk. [1]
Step 5 — Insulin. When beta-cell failure is advanced (catabolic features, marked hyperglycaemia, HbA1c above 75 mmol/mol on oral agents), start insulin. Do not delay insulin in the catabolic or insulin-deficient patient — the failure to start insulin in a patient who needs it is a major management error. [1]
DCE trap: When asked "what is the best second-line agent for this patient?" — answer by the comorbidity, not by the glucose. "This patient has heart failure, so dapagliflozin; this patient had an MI, so liraglutide; this patient has CKD, so dapagliflozin." Examiners are testing whether you know the organ-protection paradigm. [1]
Insulin therapy
Insulin is required from diagnosis in type 1 diabetes and in advanced type 2 diabetes. The principles are the same: mimic physiological insulin secretion with a basal component (suppresses hepatic gluconeogenesis between meals and overnight) and a prandial component (covers meal-related glucose excursions). [1]
Basal-bolus regimen (multiple daily injections, MDI) is the gold standard for type 1 and insulin-requiring type 2. A long-acting basal analogue (glargine U100, detemir, degludec) is given once daily (detemir may need twice daily), plus a rapid-acting analogue (lispro, aspart, glulisine) before each meal. Starting total daily dose (TDD): 0.5 units/kg/day in type 1 (with half as basal, half split between three meals); 0.2 to 0.3 units/kg/day in insulin-naive type 2. Titrate basal by fasting glucose (increase 2 units every 3 days until fasting glucose is 4 to 7 mmol/L). Prandial insulin is adjusted to carbohydrate intake and pre-meal glucose — carbohydrate counting is a core skill for type 1 patients. [1]
Premixed insulins (biphasic, 30/70) combine a fixed ratio of short- and long-acting insulin in one injection. They suit patients with type 2 diabetes on a regular meal pattern who cannot manage MDI, at the cost of inflexibility (meals must match the insulin peak) and higher hypoglycaemia risk. Less preferred in modern practice. [1]
Sliding scale insulin (correctional insulin only) — giving rapid-acting insulin reactively based on a capillary glucose reading, without a basal or scheduled component — is poor practice and should not be used as a sole regimen. It chases hyperglycaemia rather than preventing it and is associated with poor glycaemic control and prolonged hospital stay. The correct inpatient approach is a scheduled regimen (basal-bolus or basal plus correction) with a correctional scale layered on top for unexpected hyperglycaemia. [1]
Insulin pump therapy (continuous subcutaneous insulin infusion, CSII) delivers a programmable continuous basal infusion of rapid-acting insulin with patient-activated boluses for meals. In type 1 diabetes, pump therapy reduces HbA1c by approximately 0.3 to 0.6% versus MDI, reduces severe hypoglycaemia, and is the platform for hybrid closed-loop systems (see Technology below). Indications: type 1 patients with persistently elevated HbA1c on MDI, recurrent severe hypoglycaemia, dawn phenomenon, pregnancy planning, or patient preference. [1]
DWE high-yield: The most common error in starting insulin is under-dosing the basal component and over-relying on sliding-scale prandial correction. The correct framework is: basal to control fasting glucose, prandial to control postprandial excursions, correctional for unexpected readings. [1]
Microvascular complications
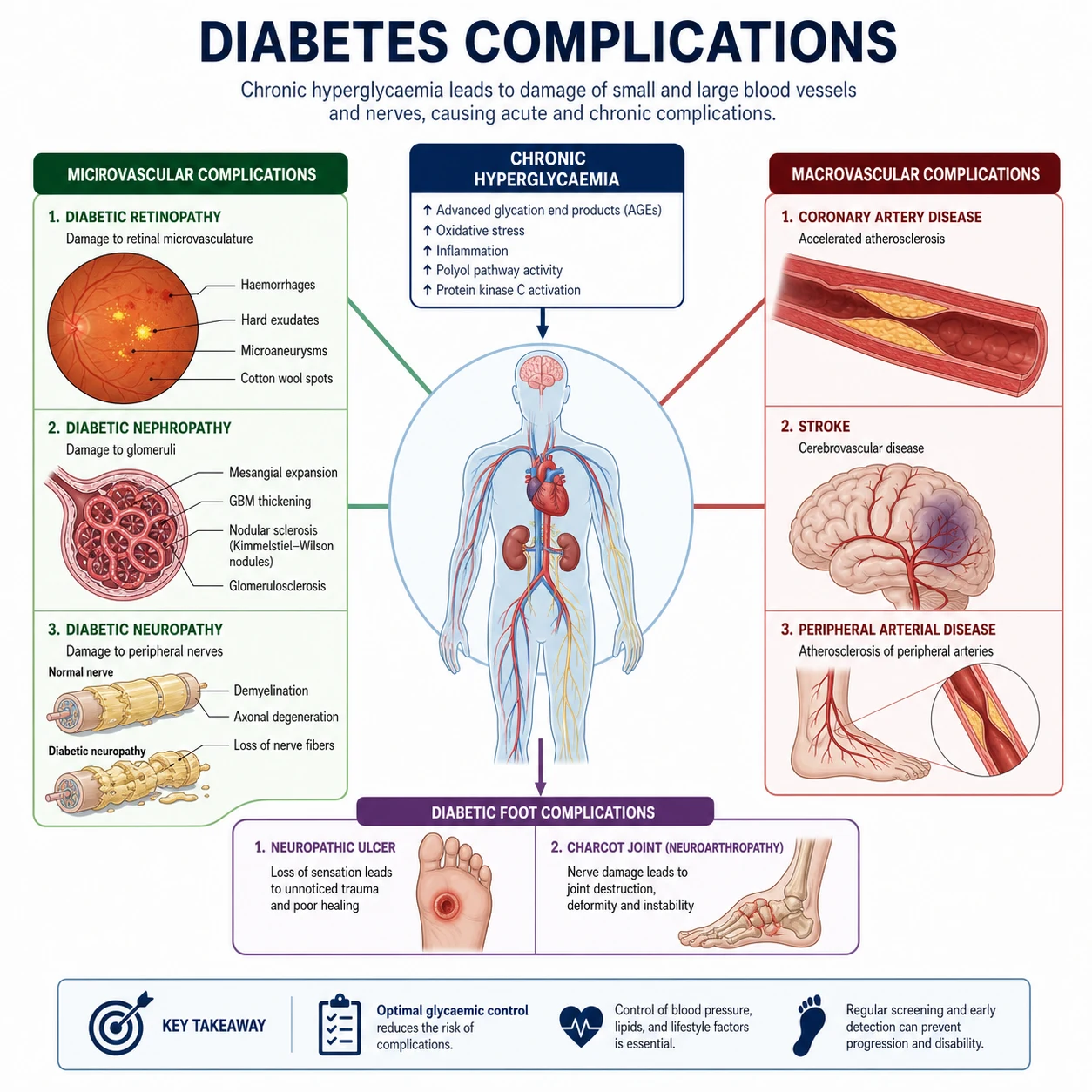
Microvascular complications — retinopathy, nephropathy, neuropathy — are the specific consequences of chronic hyperglycaemia. Their incidence is directly related to glycaemic control and diabetes duration. The DCCT (type 1) and UKPDS (type 2) both demonstrated that intensive glycaemic control reduces microvascular complications by 25 to 76%. [1]
Diabetic retinopathy
Diabetic retinopathy is the leading cause of blindness in working-age adults. Screening is mandatory from diagnosis in type 2 and from 5 years after diagnosis (or puberty) in type 1, then annually via retinal photography or slit-lamp examination by a trained observer. Classification: [1]
| Stage | Key findings | Management |
|---|---|---|
| Non-proliferative (mild) | Microaneurysms, dot-blot haemorrhages | Optimise glycaemic and blood pressure control |
| Non-proliferative (moderate to severe) | Hard exudates, cotton-wool spots, venous beading, IRMA | Close monitoring; consider early laser |
| Proliferative | Neovascularisation on disc (NVD) or elsewhere (NVE), vitreous haemorrhage, retinal detachment | Panretinal photocoagulation; intravitreal anti-VEGF; urgent ophthalmology referral |
| Diabetic macular oedema | Fluid at macula, reduced visual acuity | Intravitreal anti-VEGF (ranibizumab, aflibercept); focal laser |
Risk factors: duration, poor glycaemic control, hypertension, nephropathy (the retinopathy-nephropathy link is strong — the patient with nephropathy nearly always has retinopathy), pregnancy (may accelerate), and rapid glycaemic improvement (early worsening). [1]
DCE insight: Always look for retinopathy in the diabetic long case. A patient with proteinuric nephropathy and no retinopathy should prompt a search for an alternative cause of nephropathy — the retinopathy-nephropathy link is a clinical rule. [1]
Diabetic nephropathy
Diabetic nephropathy is the most common cause of end-stage kidney disease worldwide. The earliest sign is albuminuria — microalbuminuria (urine albumin-to-creatinine ratio, ACR, 2.5 to 25 mg/mmol in men, 3.5 to 25 in women), progressing to macroalbuminuria (ACR above 25 mg/mmol). Albuminuria is not just a marker — it is the key therapeutic target. The natural history (untreated) is progressive albuminuria, declining eGFR, and ultimately ESKD over 10 to 20 years. [1]
Management:
- RAAS blockade (ACE inhibitor or ARB) is the cornerstone — reduces intraglomerular pressure and albuminuria, independent of blood pressure. Mandatory in any diabetic patient with albuminuria and/or hypertension. The combination of ACEi plus ARB is not recommended (increased AKI, hyperkalaemia, no added renal benefit — ONTARGET).
- SGLT2 inhibitors — the DAPA-CKD trial showed dapagliflozin reduced the renal composite by 39% in CKD patients with and without diabetes. Now recommended in diabetic CKD with eGFR above 20.
- Blood pressure target — 130/80 mmHg or below in the albuminuric diabetic patient.
- Glycaemic control — HbA1c 53 mmol/mol or below in most; individualise. [1]
Monitor: U&E (potassium and creatinine) 1 to 2 weeks after starting or uptitrating RAAS blockade; acceptable creatinine rise is up to 30%. Urine ACR and eGFR at least annually. [1]
DWE trap: "A diabetic patient starts ramipril and creatinine rises by 20%. What do you do?" Answer: continue — a rise up to 30% is expected and acceptable from the haemodynamic effect on the efferent arteriole. A rise above 30% suggests volume depletion, renal artery stenosis, or intercurrent nephrotoxin — investigate. [1]
Diabetic neuropathy
Diabetic neuropathy is a heterogeneous group of disorders. The pattern to know: [1]
Distal symmetric polyneuropathy (DSPN) is the most common — a "glove-and-stocking" sensory loss beginning in the toes, ascending symmetrically. Patients describe numbness, tingling, burning, and allodynia. Loss of protective sensation (10g monofilament not felt) is the single best predictor of foot ulceration. Motor involvement (intrinsic muscle wasting) occurs late. Management: optimise glycaemic control (only proven disease-modifying therapy); for neuropathic pain, first-line is a tricyclic (amitriptyline 10 to 75mg nocte), SNRI (duloxetine 30 to 60mg daily), or pregabalin/gabapentin. Topical capsaicin and lidocaine patches are adjuncts. Avoid opioids for chronic neuropathic pain. [1]
Autonomic neuropathy affects multiple systems and is underdiagnosed:
- Cardiovascular — resting tachycardia, orthostatic hypotension (drop of 20 systolic or 10 diastolic on standing, without compensatory tachycardia), silent myocardial ischaemia, impaired exercise tolerance. Orthostatic hypotension is managed with compression stockings, fludrocortisone, midodrine, and withdrawal of offending antihypertensives.
- Gastrointestinal — gastroparesis (early satiety, nausea, erratic glucose, postprandial fullness; manage with small frequent meals, metoclopramide, domperidone; erythromycin; gastric electrical stimulation in refractory cases; favour rapid-acting insulin given post-meal), diabetic diarrhoea, and constipation.
- Genitourinary — erectile dysfunction (early and common; treat with PDE5 inhibitors — sildenafil — after excluding cardiac contraindications), neurogenic bladder.
- Sweating — gustatory sweating, anhidrosis of the feet (contributes to skin fissuring and foot ulcers). [1]
Mononeuropathies — cranial nerve palsies (third nerve palsy with pupillary sparing is classic — microvascular infarct of the vasa nervorum), and mononeuropathies of the peripheral nerves. Usually monophasic and recover over months. [1]
Diabetic amyotrophy (lumbosacral radiculoplexus neuropathy) — asymmetric painful proximal thigh weakness, weight loss, often in older men with type 2. Usually self-limiting over months; may respond to immunotherapy in refractory cases. [1]
Macrovascular complications
Cardiovascular disease is the leading cause of death in diabetes — approximately two-thirds of diabetic patients die of cardiovascular causes. Diabetes confers a two- to fourfold increased risk of myocardial infarction and stroke, equivalent to the risk of a non-diabetic patient with a prior MI (the "diabetes as a coronary risk equivalent" concept). [1]
Risk factor management is the priority — more than glycaemic control alone: [1]
| Risk factor | Target | Evidence |
|---|---|---|
| Blood pressure | Below 130/80 mmHg (with albuminuria); below 140/90 otherwise | UKPDS 38; ADVANCE; ACCORD-BP |
| Lipids | Statin for all diabetics aged 40 to 75, or with ASCVD or additional risk factors | CARDS; HPS |
| Antiplatelet | Aspirin for secondary prevention (established ASCVD); consider for primary prevention in high risk | ASCEND |
| Smoking | Cessation | |
| Glycaemic control | Individualised HbA1c | UKPDS; ACCORD |
The Steno-2 trial is the definitive evidence for multifactorial intervention: in patients with type 2 diabetes and microalbuminuria, a target-driven approach addressing glucose, blood pressure, lipids, and aspirin reduced all-cause mortality by 46% and cardiovascular events by 59% at 13 years — a far greater effect than any single intervention. The lesson: diabetes care is integrated cardiovascular risk reduction, not just glucose management. [1]
Peripheral arterial disease is more common, more distal, and more severe in diabetes (see Diabetic foot). Stroke risk is doubled; silent cerebral infarcts occur. [1]
Diabetic foot
The diabetic foot is the long-case and short-case favourite. It is the end-product of three pathological processes operating together: neuropathy (loss of protective sensation and autonomic failure causing dry, fissured skin), ischaemia (peripheral arterial disease, often distal and infrapoplacated), and infection (often polymicrobial, deep, and occult due to immunopathy and neuropathy). The combination of neuropathy and ischaemia with even minor trauma (a tight shoe, a unnoticed nail, a fissure) leads to ulceration. [1]
Classification — the IWGDF/ PEDIG system (SINBAD or University of Texas): [1]
| Parameter | Assessment |
|---|---|
| Site | Toe, forefoot, midfoot, hindfoot — plantar vs dorsal |
| Ischaemia | Palpable pulses, ankle-brachial index (note: ABI may be falsely elevated due to medial calcinosis), toe pressures, Doppler |
| Neuropathy | 10g monofilament, vibration (128Hz tuning fork), pinprick, proprioception |
| Area/depth | Cross-sectional area; University of Texas grade (0 = pre/post-ulcerative, I = superficial, II = to tendon/joint capsule, III = to bone/joint) |
| Deformity | Charcot foot, claw toes, prominent metatarsal heads |
Management — a multidisciplinary approach:
- Offloading — total contact cast for plantar neuropathic ulcers (gold standard; offloads by distributing pressure), removable cast walkers, felted foam.
- Revascularisation — if ischaemia contributes, angioplasty or surgical bypass (diabetic patients have distal disease — pedal bypass is often required). Do not delay revascularisation in a critically ischaemic foot.
- Debridement — sharp surgical debridement of necrotic tissue and callus; drainage of abscesses.
- Infection — deep wound swab or bone biopsy (not surface swab — colonisation is misleading); empiric antibiotics for mild infection (flucloxacillin or cephalexin); broad-spectrum IV antibiotics (piperacillin-tazobactam, vancomycin) for severe infection with sepsis. Probe-to-bone test — if a sterile probe touches bone, osteomyelitis is likely (sensitivity ~66%, specificity ~85%). Confirm with MRI.
- Wound care — dressings, negative pressure wound therapy for post-surgical wounds. [1]
DCE short-case: When examining the diabetic foot, present systematically: inspect (deformity, callus, ulcers, colour, shoes), palpate (pulses — femoral, popliteal, dorsalis pedis, posterior tibial; temperature), assess neuropathy (10g monofilament to 10 sites, 128Hz tuning fork at the hallux, pinprick, ankle reflexes), and examine the shoes. Report: "This patient has a neuropathic plantar ulcer under the first metatarsal head with loss of protective sensation, palpable pulses, and no sign of ischaemia — consistent with a neuropathic diabetic foot ulcer." [1]
Glycaemic emergencies
Diabetic ketoacidosis (DKA)
DKA is the hallmark of type 1 diabetes but also occurs in type 2 (ketosis-prone, or with severe stress). The triad: hyperglycaemia, ketonaemia, and metabolic acidosis. Diagnostic criteria: glucose above 11 mmol/L (or known diabetes), ketones (beta-hydroxybutyrate) above 3 mmol/L, venous pH below 7.3 or bicarbonate below 15 mmol/L. [1]
Management is protocolised (see cross-reference to the DKA topic):
- Fluid resuscitation — 0.9% sodium chloride 15 to 20 mL/kg in the first hour, then titrated; restores intravascular volume and improves tissue perfusion. [1]2. Insulin — fixed-rate intravenous insulin infusion (FRII) at 0.1 units/kg/hour; suppresses ketogenesis and corrects acidosis. Target: ketone fall of 0.5 mmol/L/hour, glucose fall of 3 mmol/L/hour, bicarbonate rise of 3 mmol/L/hour.
- Potassium — insulin drives potassium intracellularly. Start replacement when serum potassium is below 5.5 (add 40mmol to each litre of fluid; hold if above 5.5, monitor hourly). The diabetic patient in DKA is total-body potassium-depleted even with a normal serum level.
- Identify the precipitant — infection (urine, chest, line), missed insulin, new-onset type 1, MI, stroke, pancreatitis, drugs (SGLT2i — euglycaemic DKA), pregnancy. [1]
The modern DKA protocol monitors ketones, not glucose, as the primary target. Once glucose falls below 14, add 10% glucose at 125 mL/hour alongside the saline to allow continued insulin infusion while preventing hypoglycaemia — the insulin must keep running to clear ketones. [1]
Hyperosmolar hyperglycaemic state (HHS)
HHS occurs in type 2 diabetes — profound hyperglycaemia (glucose often above 30 mmol/L), marked dehydration (osmotic diuresis over days to weeks), and altered consciousness (osmotic cerebral effects), without significant ketosis (residual insulin suppresses lipolysis). Serum osmolality is above 320 mOsm/kg. The mortality (5 to 20%) is higher than DKA. [1]
Management differs from DKA: fluids first, insulin slower. Resuscitate with 0.9% saline (often 3 to 6 litres over the first 12 to 24 hours), correct electrolytes, and add low-dose insulin (0.05 units/kg/hour) only if glucose fails to fall after adequate fluid. Rapid insulin in HHS causes osmotic shifts and worsens outcomes — the fluid alone will lower glucose significantly. Anticoagulate (high VTE risk). Identify and treat the precipitant. [1]
DWE trap: "A patient on an SGLT2 inhibitor for type 2 diabetes presents with nausea and abdominal pain, glucose 9, pH 7.2, ketones 4.5." This is euglycaemic DKA — a characteristic SGLT2i complication, precipitated by fasting, surgery, or insulin reduction. The glucose is not high, but the ketones and acidosis are. Stop the SGLT2i, treat with FRII and dextrose-containing fluids (because the glucose is normal — you need a substrate for the insulin to act on). [1]
Diabetes in pregnancy
Diabetes in pregnancy encompasses pre-existing diabetes (type 1 or type 2 complicating pregnancy) and gestational diabetes mellitus (GDM) — glucose intolerance first recognised in pregnancy. [1]
Pre-existing diabetes: The preconception period is critical. Tight glycaemic control before conception (HbA1c 42 mmol/mol or below) reduces congenital malformations (neural tube defects, cardiac, caudal regression — from first-trimester hyperglycaemia) and miscarriage. Folate supplementation 5mg daily. Statins and ACE inhibitors/ARBs must be stopped preconception. Retinopathy may accelerate in pregnancy — screen each trimester. Insulin requirements rise in the second and third trimester and fall immediately postpartum. [1]
Gestational diabetes: Diagnosed by a 75g OGTT at 24 to 28 weeks (universal or risk-stratified screening). Australian thresholds: fasting glucose 5.1 mmol/L or above, 1-hour 10.0 or above, or 2-hour 8.5 or above (IADPSG criteria). Management: lifestyle first (diet, exercise), then insulin if targets are not met (fasting glucose below 5.0, 1-hour postprandial below 7.4). Metformin is used in selected patients (not type 2 in pregnancy — preference is insulin). GDM predicts a 30 to 50% risk of type 2 diabetes within 5 to 10 years — lifestyle intervention and annual glucose testing postpartum are essential. [1]
DCE insight: Diabetes in pregnancy is a high-yield long-case topic. The examiner wants to see: preconception counselling, glycaemic targets, the rationale for insulin, fetal surveillance (anomalies, macrosomia, shoulder dystocia, neonatal hypoglycaemia), and postpartum follow-up of the mother. [1]
Diabetes technology
Continuous glucose monitoring (CGM) measures interstitial glucose every 1 to 5 minutes via a subcutaneous sensor, providing real-time glucose, trend arrows, and alarms for hypo- and hyperglycaemia. In type 1 diabetes, CGM reduces HbA1c, increases time-in-range (target 70 to 180 mg/dL, 3.9 to 10 mmol/L — aim above 70% of the day), and reduces hypoglycaemia. Flash glucose monitoring (Freestyle Libre) is a simpler, lower-cost variant without alarms. CGM is now standard of care for most type 1 patients and increasingly used in insulin-treated type 2. [1]
Insulin pumps (continuous subcutaneous insulin infusion, CSII) deliver programmable basal insulin with meal boluses. In type 1 diabetes, pump therapy reduces HbA1c and severe hypoglycaemia versus MDI. [1]
Hybrid closed-loop systems (artificial pancreas) combine a CGM and a pump with an algorithm that automatically adjusts basal insulin delivery based on real-time glucose. These systems (Medtronic 780G, Tandem Control-IQ, Omnipod 5) are the current state of the art for type 1 diabetes — they increase time-in-range to above 70% with reduced hypoglycaemia and user burden. Fully automated closed-loop (without meal announcement) is the next frontier. [1]
DWE high-yield: "Time-in-range" (the percentage of the day glucose is 3.9 to 10 mmol/L) is now an endorsed complementary glycaemic endpoint to HbA1c. A patient with HbA1c 53 mmol/mol but only 40% time-in-range (with frequent excursions and hypoglycaemia) has worse glycaemic quality than one with the same HbA1c and 75% time-in-range. [1]
Diabetes and heart failure — the SGLT2i dual benefit
The intersection of diabetes and heart failure is a high-yield area reshaped by the SGLT2 inhibitor trials. Diabetes and heart failure coexist in 20 to 40% of patients and each worsens the other. [1]
The SGLT2i class has transformed both fields:
- EMPA-REG OUTCOME (2015): empagliflozin reduced heart failure hospitalisation by 35% in diabetics with established cardiovascular disease — the first signal.
- DAPA-HF (2019): dapagliflozin reduced the composite of worsening heart failure or cardiovascular death by 26% in HFrEF patients regardless of diabetes status. Cross-reference to the heart failure topic.
- DAPA-CKD (2020): dapagliflozin reduced the renal composite by 39% in CKD patients with and without diabetes. [1]
The clinical rule: every patient with type 2 diabetes and heart failure (HFrEF or HFpEF) should be on an SGLT2 inhibitor, and every patient with type 2 diabetes and CKD (eGFR above 20) should be on dapagliflozin — regardless of HbA1c. The agent is chosen for organ protection, not glucose. [1]
GLP-1 receptor agonists are the second pillar in diabetic heart failure risk reduction — but in the patient with established HFrEF, SGLT2i is the priority (GLP-1 RAs have neutral HF outcomes in established HFrEF but reduce atherosclerotic events). In the obese diabetic patient with HFpEF, GLP-1 RAs (especially semaglutide and tirzepatide) are emerging for their weight loss benefit, which improves HFpEF symptoms. [1]
Perioperative diabetes management
The perioperative diabetic patient is a common ward and long-case topic. The principles: [1]
- Elective surgery: aim for glycaemic control before surgery (HbA1c below 69 mmol/mol / 8.5% is a reasonable threshold; above this, consider deferral in major surgery). Fast from midnight. Hold oral hypoglycaemics on the morning of surgery (metformin held if contrast planned; SGLT2i held for 3 days preop due to euglycaemic DKA risk).
- Patients on insulin: do not stop basal insulin. Reduce the basal dose by 20 to 30% on the morning of surgery. Start a variable-rate intravenous insulin infusion (VRIII, formerly sliding scale) if the patient is fasting for more than one missed meal, or for emergency or major surgery. VRIII combines insulin, glucose (10% dextrose), and potassium in a protocolised infusion.
- Intraoperative: monitor capillary glucose hourly; target 6 to 10 mmol/L.
- Postoperative: resume usual regimen when eating normally; watch for hypoglycaemia. [1]
Follow-up and surveillance
The annual diabetic review is a viva and long-case staple. Present it as a checklist: [1]
| Domain | Assessment |
|---|---|
| Glycaemic | HbA1c; CGM/time-in-range data if applicable; hypoglycaemia frequency |
| Blood pressure | Target below 130/80 (albuminuria) or below 140/90 |
| Lipids | Statin if age 40+ or ASCVD or additional risk factors |
| Renal | eGFR, urine ACR annually |
| Eyes | Retinal screening annually (or biennial if low risk and no retinopathy in some guidelines) |
| Feet | Annual comprehensive foot examination (inspection, pulses, monofilament, vibration) |
| Neuropathy | Symptoms (pain, numbness); erectile dysfunction; autonomic |
| Weight and lifestyle | BMI, waist circumference; diet, exercise, smoking, alcohol |
| Medication review | Polypharmacy; adherence; adverse effects; aspirin if ASCVD |
| Vaccinations | Annual influenza; pneumococcal; COVID-19; hepatitis B for CKD |
| Depression and wellbeing | Screen (PHQ-2 or similar); diabetes distress is common |
High-yield exam discriminators and pitfalls
- Do not default to type 2 in a thin adult. Check GAD65 antibody — LADA is common and misdiagnosed.
- The management hierarchy for type 2 diabetes is now metformin then organ-protective agent, not metformin then sulphonylurea. SGLT2i for HF, CKD, ASCVD; GLP-1 RA for ASCVD and weight.
- Glycaemic targets are individualised, not standardised. ACCORD showed harm from aggressive targets in older patients with established disease.
- Multifactorial intervention (Steno-2) beats single-agent intensive glycaemic control for macrovascular outcomes. Diabetes care is cardiovascular risk reduction.
- Sliding-scale insulin as a sole regimen is poor practice. Use scheduled basal-bolus with correctional scale layered on top.
- Retinopathy and nephropathy travel together. A proteinuric diabetic patient with no retinopathy should prompt a search for an alternative renal diagnosis.
- SGLT2 inhibitors cause euglycaemic DKA — present with ketones, not high glucose. Suspect in the perioperative or fasting patient on an SGLT2i.
- The diabetic foot is neuropathy plus ischaemia plus infection. Examine all three. Offloading is as important as antibiotics for the plantar neuropathic ulcer.
- Time-in-range is now a complement to HbA1c. CGM metrics are examinable.
- Diabetes in pregnancy is preconception care. The preconception HbA1c and folate matter more than the first-trimester glucose. [1]
Exam board facts
RACP DWE: Diabetes is heavily represented — expect MCQs on classification (LADA, MODY), pharmacology (SGLT2i/GLP-1 RA choice, metformin in CKD), complications (albuminuria management, retinopathy staging), and glycaemic targets (ACCORD harm). The cardiovascular outcome trials (EMPA-REG, LEADER, DECLARE, DAPA-HF, DAPA-CKD) are high-yield. [1]
RACP DCE long case: The classic diabetic long case is a multi-morbidity patient — type 2 diabetes with nephropathy, retinopathy, neuropathy, ischaemic heart disease, and foot disease — testing integrated management, problem-list synthesis, and the modern pharmacological hierarchy. [1]
RACP DCE short case: The diabetic foot examination is a favourite short case. Present systematically: inspect, palpate pulses, test neuropathy (monofilament, tuning fork, pinprick, reflexes), examine shoes. [1]
MRCP Part 1/2: Diabetes pharmacology, MODY subtypes (HNF1A sulphonylurea sensitivity, GCK no treatment), and DKA/HHS management are frequent. [1]
MRCP PACES: Station 5 endocrinology and the diabetic foot. [1]
ABIM: Endocrinology, Diabetes & Metabolism comprises approximately 9% of the exam. Diabetes management, pharmacology, and complications are core. [1]
Key trials to know cold
| Trial | Population | Intervention | Key result |
|---|---|---|---|
| DCCT (1993) | Type 1 diabetes | Intensive vs conventional insulin | Microvascular complications reduced 35 to 76%; 3x hypoglycaemia |
| UKPDS 33 (1998) | Newly diagnosed T2DM | Intensive (SU/insulin) vs conventional | Microvascular reduction 25%; no MI signal |
| UKPDS 80 (2008) | T2DM, post-trial follow-up | — | Legacy effect: persistent MI and mortality benefit |
| ACCORD (2008) | T2DM, established CVD | Intensive (HbA1c below 42) vs standard | Mortality increased 22% — stopped early |
| Steno-2 (2008) | T2DM, microalbuminuria | Multifactorial intervention | All-cause mortality reduced 46%; CV events reduced 59% |
| EMPA-REG (2015) | T2DM, established CVD | Empagliflozin | CV death reduced 38%; all-cause mortality reduced 32% |
| LEADER (2016) | T2DM, high CV risk | Liraglutide | MACE reduced 13%; CV death reduced 22% |
| SUSTAIN-6 (2016) | T2DM, high CV risk | Semaglutide | MACE reduced 26% (stroke-driven); retinopathy signal |
| DECLARE (2019) | T2DM, high CV risk | Dapagliflozin | HF hospitalisation reduced; MACE neutral |
| DAPA-HF (2019) | HFrEF, with/without DM | Dapagliflozin | Worsening HF/CV death reduced 26% |
| DAPA-CKD (2020) | CKD, with/without DM | Dapagliflozin | Renal composite reduced 39% |
| SURPASS-2 (2021) | T2DM | Tirzepatide vs semaglutide | Superior HbA1c and weight reduction |
Communication and shared decision-making
Diabetes is a chronic condition requiring daily self-management — the patient is the primary decision-maker. The consultation framework: [1]
- Elicit the patient's understanding and goals — "What does diabetes mean to you? What are you most worried about?"
- Frame management around their priorities — if they fear injections, discuss GLP-1 RA (weekly) versus insulin; if weight is the priority, emphasise GLP-1 RA or tirzepatide.
- Discuss hypoglycaemia openly — it is the barrier to intensive therapy, especially in older patients. Driving and occupational implications.
- Shared decision on glycaemic target — "For you, given your heart disease, we will target a moderate HbA1c to avoid hypos. The most important thing is the medications that protect your heart and kidneys."
- Cultural and dietary competence — tailor dietary advice to cultural food patterns; involve diabetes educators and dietitians.
- Advance care planning in advanced disease — de-escalate therapy in the frail and end-of-life patient. [1]
References and further reading
American Diabetes Association — Standards of Care in Diabetes (2025). Australian Diabetes Society guidelines. NICE NG28 (type 2 diabetes). KDIGO 2022 (diabetes in CKD). RACGP type 2 diabetes management. The landmark trials cited above (DCCT, UKPDS, ACCORD, Steno-2, EMPA-REG, LEADER, SUSTAIN-6, DECLARE, DAPA-HF, DAPA-CKD, SURPASS-2) define the modern evidence base. [1]
References
- [1]DCCT Research Group The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus N Engl J Med, 1993.PMID 8366922
- [2]UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group Lancet, 1998.PMID 9742976
- [3]Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HAW 10-year follow-up of intensive glucose control in type 2 diabetes N Engl J Med, 2008.PMID 18784090
- [4]ACCORD Study Group Effects of intensive glucose lowering in type 2 diabetes N Engl J Med, 2008.PMID 18539917
- [5]Gaede P, Lund-Andersen H, Parving HH, Pedersen O Effect of a multifactorial intervention on mortality in type 2 diabetes N Engl J Med, 2008.PMID 18256393
- [6]Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes N Engl J Med, 2015.PMID 26378978
- [7]Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes N Engl J Med, 2016.PMID 27295427
- [8]Marso SP, Bain SC, Consoli A, et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes N Engl J Med, 2016.PMID 27633186
- [9]Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular mortality and disease outcomes in a population with type 2 diabetes similar to that of the DECLARE-TIMI 58 trial: A nationwide observational study Diabetes Obes Metab, 2019.PMID 30609272
- [10]Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in Patients with Chronic Kidney Disease N Engl J Med, 2020.PMID 32970396
- [11]Frias JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes N Engl J Med, 2021.PMID 34170647
- [12]McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction N Engl J Med, 2019.PMID 31535829