Phys · endocrine
Diabetic Ketoacidosis and Hyperosmolar Hyperglycaemic State
Also known as DKA · diabetic ketoacidosis · hyperosmolar hyperglycaemic state · HHS · hyperosmolar hyperglycemic state · HONK · hyperosmolar non-ketotic coma · hyperglycaemic emergency · ketoacidosis · euglycaemic DKA · euglycemic diabetic ketoacidosis · fixed-rate intravenous insulin infusion · FRIII · beta-hydroxybutyrate · Kussmaul breathing · ketogenesis
Consultant-physician-depth guide to the two hyperglycaemic emergencies — diagnostic criteria for DKA (ketonaemia above 3 mmol/L or ketonuria 3+, glucose above 11, pH below 7.3, bicarbonate below 15) and HHS (glucose above 33, osmolality above 320, no significant ketosis, pH above 7.3), pathophysiology of insulin deficiency and ketogenesis, precipitant recognition, and the full JBDS management protocol (fluid resuscitation, fixed-rate insulin infusion 0.1 units/kg/hour, potassium replacement, dextrose switch, resolution criteria) and HHS-specific differences. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Diabetic Ketoacidosis and Hyperosmolar Hyperglycaemic State
The answer first
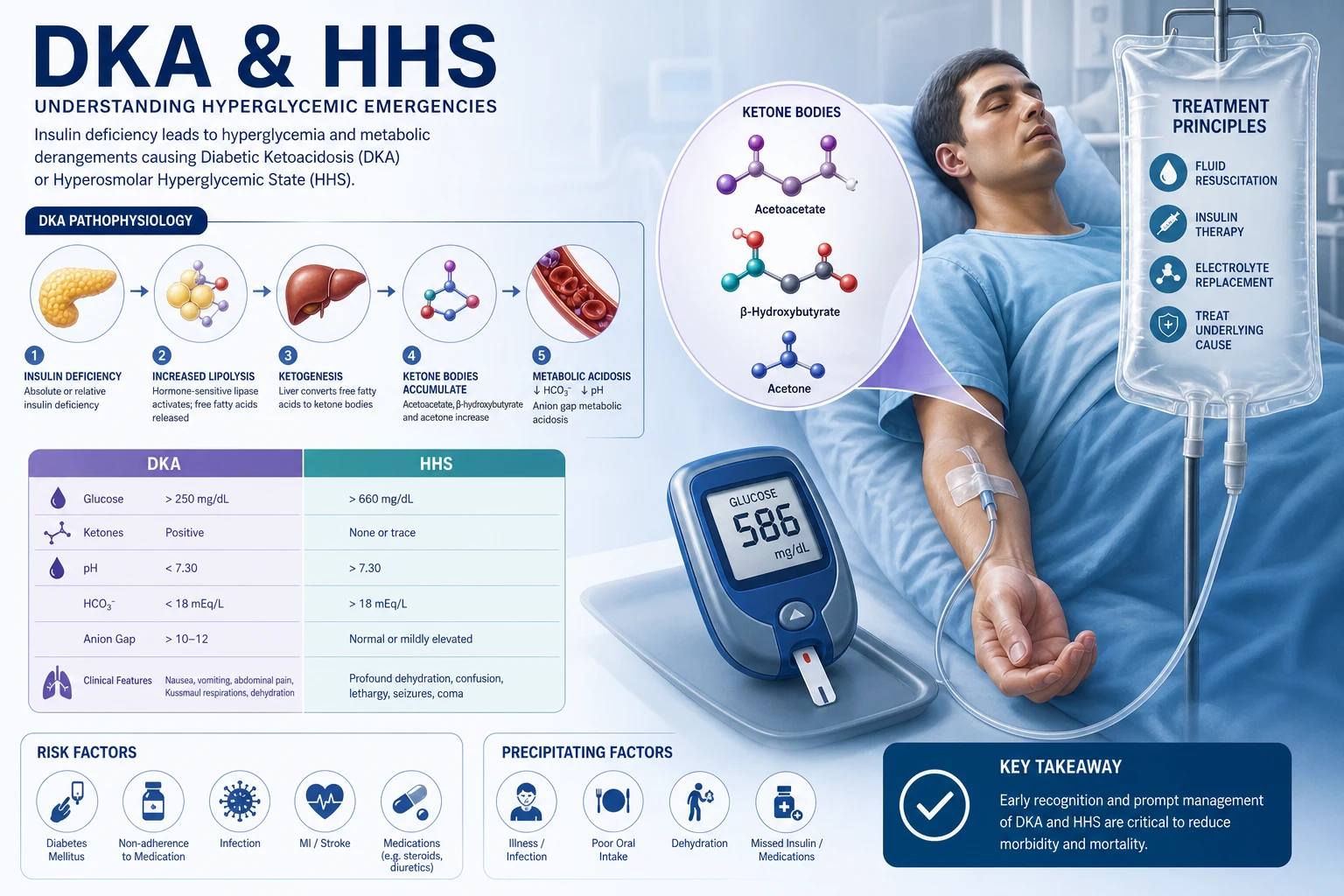
Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycaemic state (HHS) are the two hyperglycaemic emergencies. They are emergencies because they kill, and because a reproducible protocol saves lives. The registrar who can name the diagnostic criteria, start the correct fluid and insulin, and anticipate the complications (cerebral oedema, hypokalaemia, hypoglycaemia) will manage these patients well; the one who treats DKA as a glucose problem will harm the patient. [1]
The mandate is simple: [1]
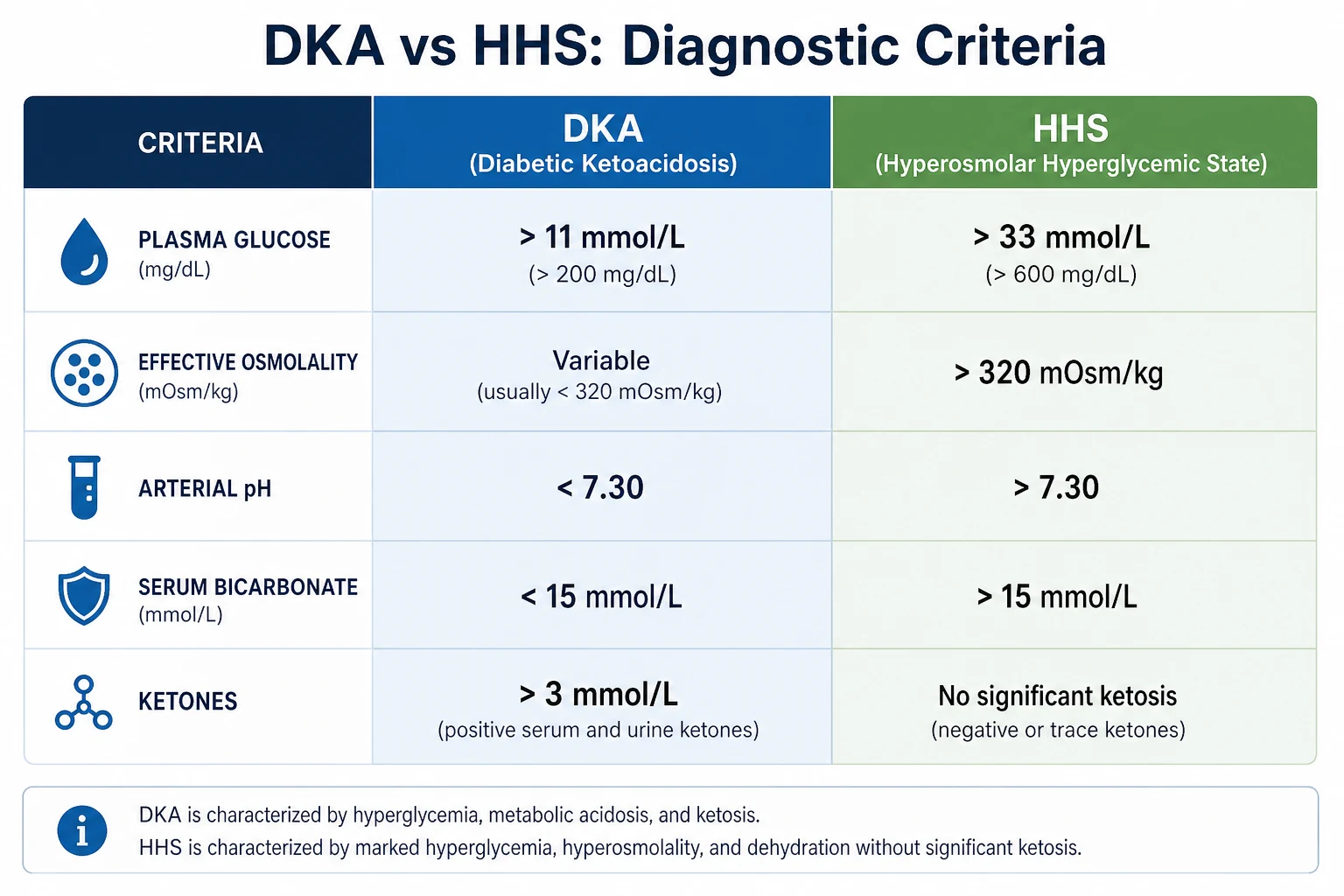
- Diagnose — DKA (ketones above 3, glucose above 11, pH below 7.3, bicarbonate below 15) or HHS (glucose above 33, osmolality above 320, minimal ketosis, pH above 7.3). The distinction changes the protocol.
- Resuscitate with fluid first — 0.9% saline 1 litre in the first hour. Fluid lowers glucose more than insulin does in the first hour, by restoring perfusion and switching off the osmotic diuresis.
- Start fixed-rate insulin — 0.1 units/kg/hour to suppress ketogenesis, not to chase glucose. The target is a falling ketone level and a rising bicarbonate. [1]4. Replace potassium before it falls — if the level is below 5.5 mmol/L, add potassium; the target is 4-5.5.
- Switch to dextrose when glucose falls below 14 — keep the insulin running to clear ketones.
- Resolve and transition — ketones below 0.6, pH above 7.3, bicarbonate above 18; then overlap to subcutaneous insulin. [1]
The single most important principle for the exam: insulin in DKA exists to suppress ketogenesis, not to normalise glucose. The candidate who titrates insulin to glucose will stop the infusion too early, leave ketones circulating, and re-present in 12 hours [4].
Diagnostic criteria
DKA — the triad of ketosis, acidosis and hyperglycaemia
The diagnostic criteria for DKA in adults, drawn from the JBDS and ADA consensus, are [1][4]:
| Criterion | Threshold |
|---|---|
| Blood glucose | above 11 mmol/L or known diabetic |
| pH (venous) | below 7.3 |
| Bicarbonate | below 15 mmol/L |
| Anion gap | elevated (above 16) |
The anion gap confirms that the acidosis is a high-anion-gap metabolic acidosis — the ketones (acetoacetate and beta-hydroxybutyrate) are the unmeasured anions. Calculate it on every patient: anion gap = sodium minus chloride minus bicarbonate. [1]
Viva answer: "DKA is a triad of ketosis, metabolic acidosis, and hyperglycaemia. The diagnostic thresholds are a glucose above 11 in a known or suspected diabetic, a beta-hydroxybutyrate above 3, a venous pH below 7.3, and a bicarbonate below 15. I calculate the anion gap to confirm it is a high-anion-gap metabolic acidosis." [1]
Severity of DKA
The JBDS grades severity by the venous pH and bicarbonate, because these correlate with outcome [4]:
| Severity | pH | Bicarbonate |
|---|---|---|
| Mild | 7.25-7.30 | 15-18 |
| Moderate | 7.00-7.24 | 10-15 |
| Severe | below 7.00 | below 10 |
Severe DKA (pH below 7.0) warrants ICU admission, because these patients are at greatest risk of cardiovascular collapse and cerebral oedema. [1]
Euglycaemic DKA — the trap
Euglycaemic DKA is DKA with a glucose below 11 mmol/L. It is the single most easily missed form because the registrar who checks only glucose will be reassured by a near-normal reading. The classic setting is the patient on an SGLT2 inhibitor (empagliflozin, dapagliflozin) who presents with mild abdominal pain, a glucose of 9, and an incidental high-anion-gap acidosis [3].
The mechanism: SGLT2 inhibitors cause glucosuria, which lowers plasma glucose. The low glucose suppresses endogenous insulin secretion and raises glucagon, and the high glucagon-to-insulin ratio drives ketogenesis in the liver. The glucose never rises much because the drug keeps excreting it — but the ketones accumulate. This is also seen in pregnancy (accelerated starvation), starvation, and alcohol misuse. [1]
DWE exam trap: Any unwell diabetic patient with an unexplained high-anion-gap acidosis needs a beta-hydroxybutyrate — even if the glucose is normal. A glucose of 9 does not exclude DKA on an SGLT2 inhibitor. [1]
HHS — profound hyperglycaemia and dehydration without significant ketosis
The diagnostic criteria for HHS are [1]:
| Criterion | Threshold |
|---|---|
| Blood glucose | above 33 mmol/L |
| Ketones | below 3 mmol/L (no significant ketosis) |
| pH (venous) | above 7.3 |
| Bicarbonate | above 15 mmol/L |
Calculate the effective (calculated) osmolality: 2 x sodium + glucose + urea. The measured osmolality is less useful because it includes ethanol and other osmoles that do not contribute to the tonicity-driven water shift. A urea above 7 mmol/L is itself an independent marker of severity and mortality in HHS. [1]
HHS is primarily a disorder of type 2 diabetes in older people. The residual insulin secretion is enough to suppress lipolysis and ketogenesis (which is why ketones are low and the pH is preserved), but not enough to prevent marked hyperglycaemia. The glucose rises insidiously over days to weeks, driving an osmotic diuresis that causes enormous water and electrolyte loss — patients are typically 6-9 litres behind. [1]
DKA versus HHS — the discriminator
| Feature | DKA | HHS |
|---|---|---|
| Patient | any age, often type 1 | older, type 2 |
| Tempo | hours | days to weeks |
| Glucose | above 11 | above 33 |
| Ketones | above 3 | below 3 |
| pH | below 7.3 | above 7.3 |
| Bicarbonate | below 15 | above 15 |
| Osmolality | variable | above 320 |
| Sensorium | variable, often alert | depressed, often stupor or coma |
| Breathing | Kussmaul (deep, sighing) | normal |
| Breath | ketotic (fruity) | normal |
| Mortality | 1-5% | 10-20% |
The two conditions overlap: some patients have a mixed DKA-HHS picture (severe hyperglycaemia with significant ketosis and acidosis). The protocol is to treat the dominant component first — fluid and insulin for both, with the ketone target driving duration. [1]
Pathophysiology
Insulin deficiency and counter-regulatory hormones
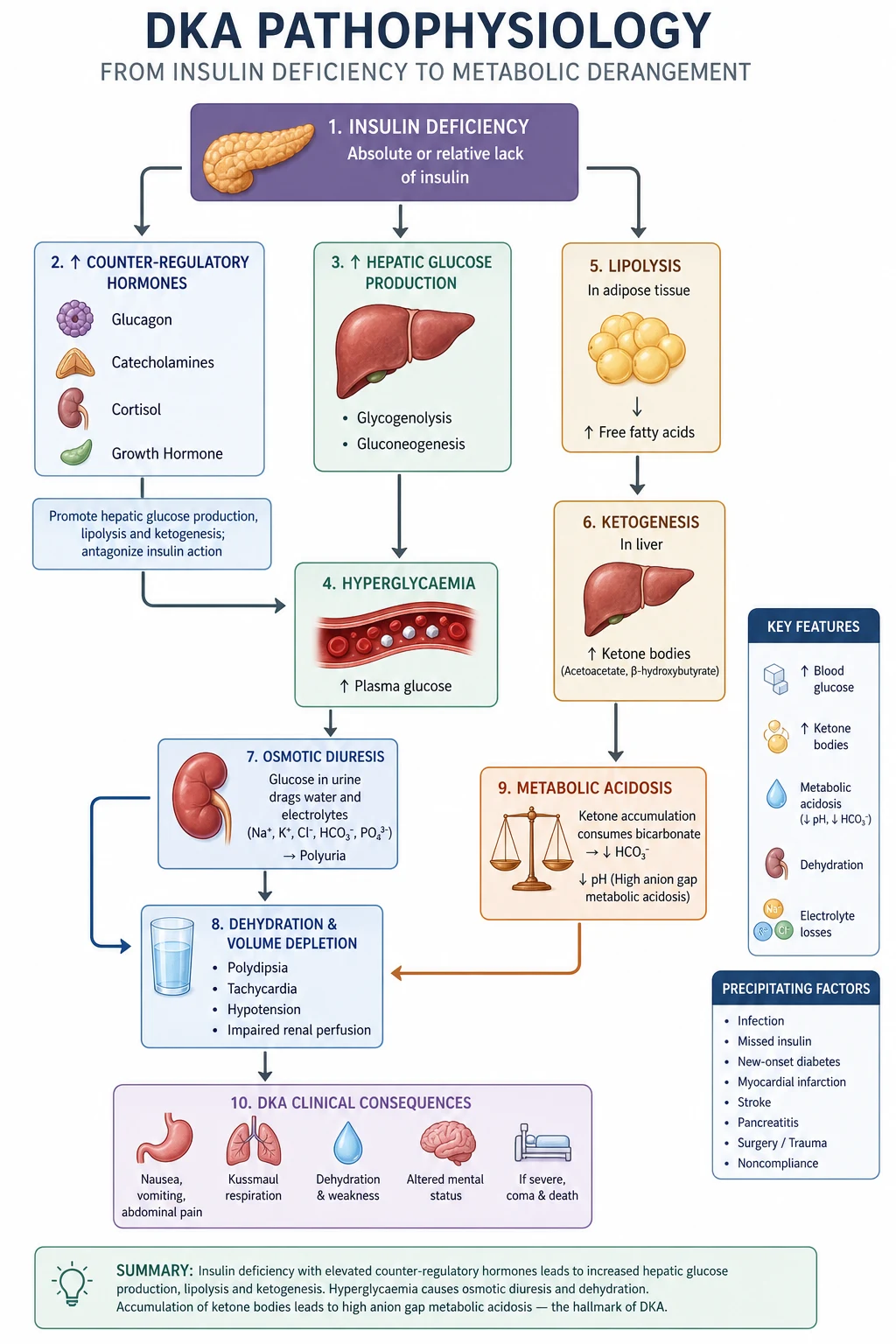
DKA begins with insulin deficiency — absolute in type 1 diabetes (no insulin), relative in type 2 (insulin resistance plus a precipitant that increases demand). The deficiency is amplified by a surge of counter-regulatory hormones (glucagon, catecholamines, cortisol, growth hormone), released in response to the precipitant (infection, infarction, omission). [1]
The consequences unfold in parallel: [1]
- Hyperglycaemia — insulin normally suppresses hepatic gluconeogenesis and glycogenolysis and promotes peripheral glucose uptake. Without it, the liver pours out glucose and the muscles cannot take it up. Counter-regulatory hormones accelerate gluconeogenesis (glucagon, cortisol) and glycogenolysis (catecholamines). Glucose rises.
- Osmotic diuresis — once glucose exceeds the renal threshold (around 10 mmol/L), it spills into the urine, dragging water and electrolytes with it. The patient loses water, sodium, potassium, magnesium and phosphate. This is why the total-body water deficit in DKA is 3-6 litres and in HHS is 6-9 litres.
- Lipolysis and ketogenesis — insulin normally suppresses hormone-sensitive lipase in adipose tissue. Without insulin, lipase runs unchecked, breaking down triglycerides into free fatty acids. These flood the liver, where the high glucagon-to-insulin ratio activates carnitine palmitoyltransferase-1, shuttling fatty acids into the mitochondria for beta-oxidation. The liver converts the resulting acetyl-CoA into ketone bodies. [1]
Ketogenesis — acetoacetate and beta-hydroxybutyrate
The two principal ketone bodies are acetoacetate and beta-hydroxybutyrate. A third, acetone, is a volatile breakdown product of acetoacetate, excreted via the lungs — it gives the breath its characteristic fruity or nail-polish-remover smell. [1]
The liver produces acetoacetate first. The redox state of the mitochondrion then determines the equilibrium between acetoacetate and beta-hydroxybutyrate [1]:
- In DKA, the high NADH-to-NAD+ ratio (from accelerated fatty acid oxidation) drives the equilibrium towards beta-hydroxybutyrate, which is the dominant ketone in untreated DKA (about 75-80% of total ketones).
- As insulin therapy restores normal metabolism and the NADH/NAD+ ratio falls, beta-hydroxybutyrate is converted back to acetoacetate. [1]
The ketone flip (exam trap): During recovery from DKA, the nitroprusside urine ketone test (which detects acetoacetate, not beta-hydroxybutyrate) can paradoxically rise as beta-hydroxybutyrate is converted to acetoacetate. A registrar who monitors urine ketones may think the DKA is worsening when it is actually resolving. Always monitor with beta-hydroxybutyrate, not urine ketones, during treatment. [1]
Why HHS differs from DKA
In HHS, the residual insulin secretion (typical of type 2 diabetes) is enough to suppress hormone-sensitive lipase — so free fatty acid delivery to the liver is low, and ketogenesis is minimal. The pH stays near normal. But the insulin is not enough to control the hyperglycaemia, which rises over days, driving a relentless osmotic diuresis. The patient presents profoundly dehydrated and hyperosmolar, with neurological depression proportional to the osmolality. [1]
Precipitants
The precipitant is the single most important determinant of survival in HHS, and the most common reason for recurrent DKA. Always ask: what tipped this patient over? [1]
The six precipitants to name
- Infection — the most common precipitant of both DKA and HHS. Search for it: pneumonia, urinary tract infection, cellulitis, sepsis. Send blood and urine cultures, a chest X-ray, and inflammatory markers on every patient.
- Infarction — myocardial infarction, stroke, mesenteric ischaemia. A silent myocardial infarction is a classic precipitant of HHS in an elderly diabetic. Do an ECG and troponin on every patient.
- Insulin omission or non-adherence — the most common precipitant of DKA in known type 1 diabetes. Ask specifically about missed doses, pump failure (in insulin pump users, DKA can develop within hours of catheter disconnection), and injection site problems.
- Initiation (new-onset type 1 diabetes) — up to 25% of new type 1 diabetes presents as DKA. This is the classic presentation in a child or young adult with weight loss, polyuria, and vomiting.
- Drugs — corticosteroids (gluconeogenesis, insulin resistance), atypical antipsychotics (olanzapine, clozapine), thiazides, sympathomimetics, and — crucially — SGLT2 inhibitors (euglycaemic DKA) [3].
- Pregnancy — a state of insulin resistance and accelerated starvation; DKA can occur at lower glucose levels and is a medical emergency for both mother and fetus.
Examiner question: "What is the most common precipitant of DKA in a known type 1 diabetic?" Answer: insulin omission, whether deliberate, accidental, or from pump failure. "And the most common precipitant of HHS?" Answer: infection, usually a urinary or respiratory tract infection in an elderly type 2 diabetic. [1]
Clinical features
DKA — the ketotic, acidotic picture
The patient with DKA is usually alert or only mildly confused (unlike HHS). The classic features are: [1]
- Polyuria and polydipsia — from the osmotic diuresis.
- Kussmaul respiration — deep, sighing, rapid breathing, a compensatory response to the metabolic acidosis. The body blows off CO2 to raise the pH.
- Ketotic breath — a fruity, sweet, or nail-polish-remover smell from exhaled acetone.
- Nausea and vomiting — from gastric stasis and the metabolic acidosis. Vomiting accelerates dehydration.
- Abdominal pain — common, especially in children. It is usually from gastric dilatation, hepatic capsule stretch, or ileus. But if the pain does not settle as the DKA resolves, reconsider a surgical abdomen (appendicitis, pancreatitis, mesenteric ischaemia) as the precipitant.
- Dehydration — dry mucous membranes, reduced skin turgor, tachycardia, hypotension, oliguria. [1]
HHS — the dehydrated, comatose picture
The patient with HHS is typically elderly, profoundly dehydrated, and neurologically depressed: [1]
- Altered mental status — ranging from drowsiness to coma, proportional to the osmolality. A patient with an osmolality above 350 is usually comatose.
- Focal neurological signs — seizures, hemiparesis, aphasia, which can mimic a stroke. These resolve as the osmolality falls.
- Profound dehydration — sunken eyes, dry tongue, reduced skin turgor, tachycardia, hypotension. The water deficit is 6-9 litres.
- No Kussmaul breathing, no ketotic breath — the preserved pH means no respiratory compensation is needed, and ketogenesis is minimal. [1]
Red flag: In HHS, the degree of neurological depression is proportional to the osmolality. If the osmolality is above 320 and the patient is fully alert, or if the osmolality is only mildly raised but the patient is deeply comatose, suspect an alternative or additional cause (stroke, sepsis, drug ingestion) and arrange a CT head. [1]
Investigations
The initial panel
Draw blood and send the following immediately: [1]
| Test | Why |
|---|---|
| Capillary glucose | the entry point — confirms hyperglycaemia |
| Venous blood gas (VBG) | pH, bicarbonate — confirms the acidosis; a VBG is adequate, no need for arterial |
| Beta-hydroxybutyrate | confirms and quantifies ketosis; the preferred ketone for monitoring |
| Electrolytes (Na, K, Cl, HCO3, urea, creatinine) | calculates the anion gap and osmolality; assesses potassium and renal function |
| Magnesium, phosphate | both fall during treatment; baseline for replacement decisions |
| Full blood count | leukocytosis is common (stress response) but does not confirm infection; a left shift does |
| ECG | silent myocardial infarction, and signs of hyper- or hypokalaemia |
| Blood cultures, urine culture, chest X-ray | the infection screen |
| Troponin | silent infarction, especially in HHS |
| Beta-hCG | in all women of childbearing age — pregnancy precipitates and is changed by DKA |
| Lipase | pancreatitis can precipitate or complicate |
Corrected sodium
In hyperglycaemia, the measured sodium is artefactually low because glucose draws water into the extracellular space, diluting the sodium. Correct it: [1]
Corrected sodium = measured sodium + 0.4 x (glucose minus 5.5) [1]
This matters because the corrected sodium changes the fluid choice. A patient with a measured sodium of 128 and a glucose of 40 has a corrected sodium of 128 + 0.4 x 34.5 = 128 + 13.8 = about 142 — normal. If the corrected sodium is low, use 0.9% saline; if it is high or normal, a balanced crystalloid (Plasma-Lyte or Hartmann's) is reasonable, especially to avoid the hyperchloraemic acidosis of large-volume saline. [1]
Why a venous gas is adequate
A venous blood gas gives a pH about 0.03 lower and a PaCO2 about 5-7 mmHg higher than arterial. For the diagnosis and monitoring of DKA, this is entirely adequate — the thresholds (pH below 7.3, bicarbonate below 15) are set for venous values. There is no need to subject an already-ill patient to an arterial puncture unless you need the oxygenation data. [1]
Management of DKA
The management of DKA follows the JBDS protocol, which has four simultaneous streams: fluid, insulin, potassium, and monitoring [4].
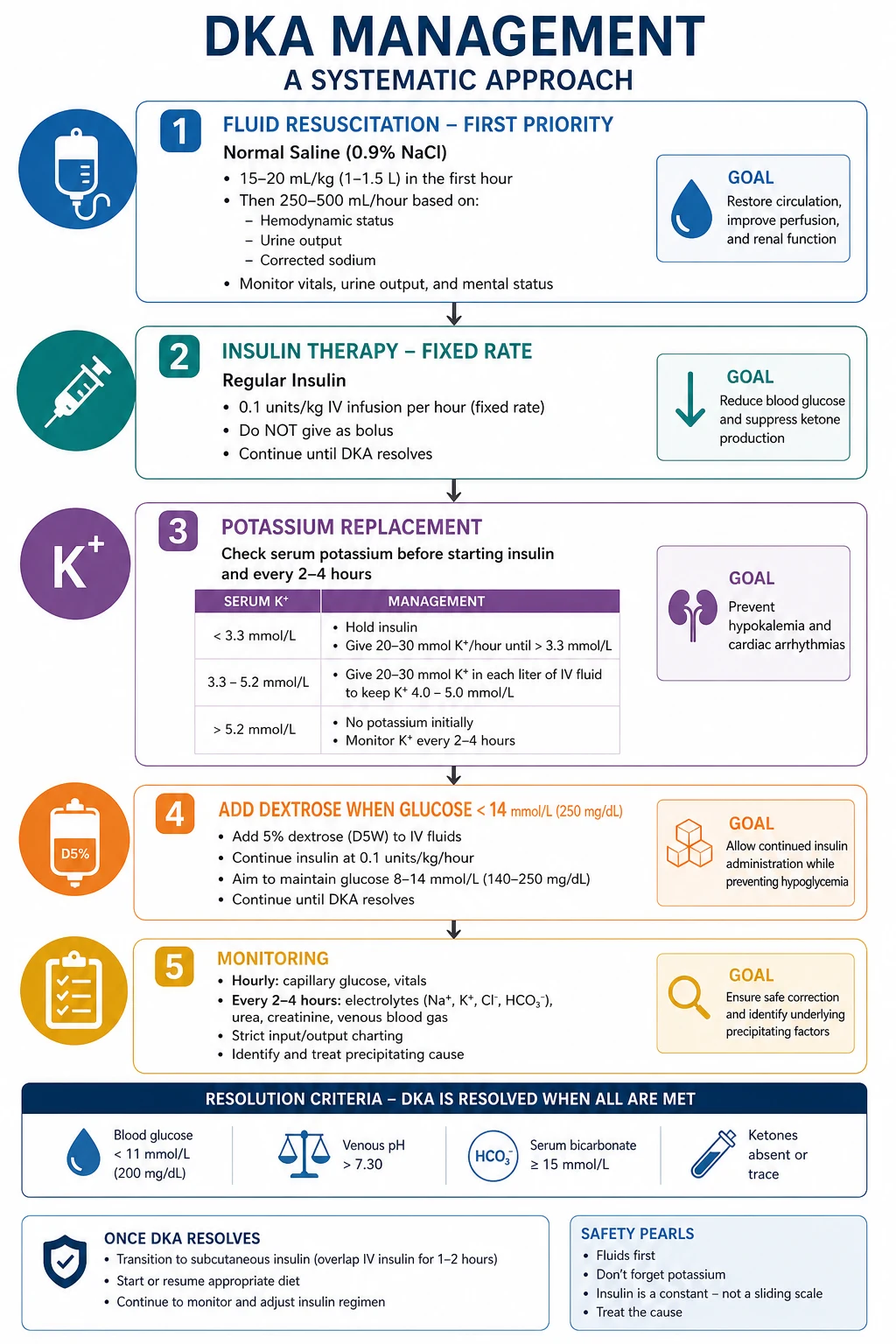
Step 1 — Fluid resuscitation (start immediately)
Fluid is the first intervention and the most important. It restores intravascular volume, improves tissue perfusion, and reduces the counter-regulatory hormone response. Fluid alone lowers glucose by 3-5 mmol/L in the first hour, before any insulin is given. [1]
The JBDS 0.9% saline protocol [4]:
| Time | Fluid |
|---|---|
| 0-1 hour | 0.9% saline 1 litre |
| 1-3 hours | 0.9% saline 1 litre over 2 hours |
| 3-5 hours | 0.9% saline 1 litre over 2 hours |
| 5-9 hours | 0.9% saline 1 litre over 4 hours |
| 9+ hours | 0.9% saline 1 litre every 6-8 hours |
Reassess the patient at every stage — fluid rate should be adjusted for cardiac and renal function. If the corrected sodium is high (above 155), 0.45% saline may be considered, but 0.9% is the default. If the sodium is normal or low, 0.9% is correct. [1]
Fluid choice — the evidence: The default is 0.9% saline, but it causes a hyperchloraemic acidosis that can make the bicarbonate appear not to recover even as the DKA resolves. The Van Zyl RCT compared 0.9% saline with Ringer's lactate and found no difference in time to pH normalisation, but a slower glucose fall with Ringer's lactate (the lactate is metabolised to glucose) [5]. Plasma-Lyte may avoid the hyperchloraemic acidosis and is increasingly used, but the evidence base is still evolving; 0.9% saline remains the JBDS default.
Step 2 — Fixed-rate intravenous insulin infusion (FRIII)
Start the FRIII after the first litre of fluid, once you have confirmed the potassium is above 3.3. [1]
FRIII = 0.1 units/kg/hour of soluble human insulin (Actrapid). [1]
- Weigh the patient (or estimate). Multiply weight in kg by 0.1 to get the hourly rate. An 80 kg patient gets 8 units/hour.
- Make up 50 units of Actrapid in 50 mL of 0.9% saline (1 unit/mL) and run at the calculated rate via an infusion pump.
- No loading bolus is recommended — the FRIII alone achieves a steady-state insulin level within 10-15 minutes. [1]
The goal of the FRIII is ketogenesis suppression, not glucose normalisation. The metabolic targets are [4]:
- Fall in ketones (beta-hydroxybutyrate) of at least 0.5 mmol/L/hour.
- Fall in glucose of about 3 mmol/L/hour.
- Rise in bicarbonate of about 3 mmol/L/hour. [1]
If these targets are not met, check: is the cannula working? Is the pump running? Is the insulin the right concentration? If all are correct and the ketones are not falling, increase the FRIII to 0.15 units/kg/hour (insulin resistance — common in type 2 with sepsis or obesity). [1]
Viva answer: "The fixed-rate intravenous insulin infusion is 0.1 units per kilogram per hour of soluble insulin. Its purpose is to suppress ketogenesis, not to lower glucose. I monitor the response with hourly ketones — I expect a fall of at least 0.5 mmol/L per hour. If the ketones are not falling, I check the line and the pump, and if those are correct I increase the rate to 0.15 units per kilogram per hour." [1]
Step 3 — Potassium replacement
The total-body potassium deficit in DKA is 3-5 mmol/kg, even though the initial serum potassium may be normal or high. This is because acidosis shifts potassium out of cells, and the lack of insulin prevents reuptake. When you give insulin, potassium moves back into cells and the serum level plummets. The most common cause of death during DKA treatment is hypokalaemia-induced arrhythmia. [1]
The replacement protocol [4]:
| Serum potassium (mmol/L) | Action |
|---|---|
| Above 5.5 | no potassium in the fluid; recheck within 2 hours |
| 3.5-5.5 | add 40 mmol/L potassium to the fluid |
| below 3.5 | senior review; give potassium at 40 mmol/L and delay insulin until above 3.5 (ideally above 3.3 minimum) |
The target range is 4-5.5 mmol/L. Check potassium hourly during the first few hours. Use pre-mixed bags of 0.9% saline with 40 mmol/L KCl where available. [1]
The potassium rule: If the potassium is below 3.3, do NOT start insulin yet. Give potassium first, with cardiac monitoring. Insulin in a hypokalaemic patient will precipitate a life-threatening arrhythmia. This is the single most dangerous avoidable error in DKA management. [1]
Step 4 — Switch to dextrose when glucose falls below 14
When the capillary glucose falls below 14 mmol/L, switch the fluid to a dextrose-containing solution (10% dextrose at 125 mL/hour, or 5% dextrose at a faster rate if 10% is unavailable) while continuing the FRIII unchanged. The rationale: the glucose is now low enough that continuing saline would risk hypoglycaemia, but the ketones are still present and the insulin must keep running to clear them. The dextrose provides a substrate so the insulin can continue to work safely. [1]
The 2023 JBDS update also recommends considering a reduction of the FRIII to 0.05 units/kg/hour at this point if the glucose is falling rapidly, to reduce the risk of hypoglycaemia [4].
Why this step matters: The most common management error is stopping the insulin when the glucose normalises. This leaves the ketones circulating, and the patient re-presents in DKA within hours. The insulin runs until the ketones are cleared, not until the glucose is normal. [1]
Step 5 — Resolution criteria
DKA is resolved when all three are met [4]:
- Ketones (beta-hydroxybutyrate) below 0.6 mmol/L
- Venous pH above 7.3
- Bicarbonate above 18 mmol/L [1]
Only when these are met do you transition to subcutaneous insulin. [1]
Step 6 — Transition to subcutaneous insulin
The transition must overlap the intravenous and subcutaneous insulin to avoid a gap in coverage: [1]
- Give the patient's usual subcutaneous insulin (or start a new basal-bolus regimen if this is new-onset diabetes: a total daily dose of 0.5-0.8 units/kg, split into a basal glargine/detemir half and a rapid-analogue prandial half).
- Wait 30-60 minutes for the subcutaneous insulin to be absorbed.
- Ensure the patient has eaten.
- Then stop the FRIII. [1]
If you stop the FRIII and then give subcutaneous insulin, there is a window of 30-60 minutes with no insulin on board, and the DKA will recur. [1]
Bicarbonate — when NOT to use it
Routine bicarbonate is not recommended in DKA. The Glaser study showed that bicarbonate administration was an independent risk factor for cerebral oedema in children with DKA [2]. It is reserved for the exceptional case of pH below 6.9 with haemodynamic instability that is not responding to standard therapy — and only then in consultation with ICU. The acidosis corrects with fluid and insulin as the ketones are metabolised to bicarbonate.
Management of HHS
HHS shares the principles of DKA management (fluid, insulin, potassium, monitoring) but with crucial differences that reflect the older patient, the profound dehydration, the residual insulin, and the higher mortality [1].
Differences from DKA
| Aspect | DKA | HHS |
|---|---|---|
| Fluid deficit | 3-6 litres | 6-9 litres |
| Insulin dose | FRIII 0.1 units/kg/hour from the start | lower — 0.05 units/kg/hour, or fluid alone initially |
| Glucose fall target | 3 mmol/L/hour | 3 mmol/L/hour |
| Anticoagulation | standard VTE risk assessment | prophylactic LMWH routinely (high thrombotic risk) |
| Mortality | 1-5% | 10-20% |
| Cerebral oedema risk | significant (young) | lower but present |
HHS fluid protocol
Fluid is even more critical in HHS, but must be given cautiously because these patients are elderly and often have cardiac or renal comorbidity: [1]
- 0.9% saline 1 litre in the first hour, then 1 litre every 2 hours, adjusted to the clinical response and cardiac/renal status.
- Aim for a glucose fall of about 3 mmol/L/hour and an osmolality fall of 3-8 mOsm/kg/hour. Too rapid a fall risks cerebral oedema.
- If the corrected sodium is high (above 155), 0.45% saline may be used after initial resuscitation.
- Monitor for fluid overload (creatinine trend, oxygen saturation, auscultation) — reduce the rate if signs of overload appear. [1]
HHS insulin
Insulin is needed in HHS but at lower doses than DKA, because these patients still have residual endogenous insulin. Options: [1]
- Fluid alone initially — in many patients, fluid resuscitation alone will bring the glucose down substantially by restoring perfusion and reducing the counter-regulatory drive.
- Low-dose FRIII (0.05 units/kg/hour) — if the glucose is not falling adequately with fluid alone (slower than 3 mmol/L/hour), add a low-dose FRIII.
- Do not start insulin before potassium is above 3.3 — same rule as DKA. [1]
Because there is no significant ketosis, there is no ketone target — resolution is when the glucose is controlled and the osmolality is near normal, and the patient is eating and drinking. [1]
Anticoagulation
Prophylactic low-molecular-weight heparin (enoxaparin 40 mg subcutaneously daily, adjusted for renal function) is recommended in HHS unless contraindicated, because the severe dehydration and hyperviscosity create a high risk of venous and arterial thrombosis. DVT, PE, myocardial infarction, and stroke are among the leading causes of death in HHS. [1]
Treat the precipitant
In HHS, the precipitant (usually infection or infarction) is the primary determinant of survival. Identify and treat it aggressively: broad-spectrum antibiotics for sepsis within one hour, cardiology input for myocardial infarction. No amount of fluid and insulin will save a patient whose septic source is untreated. [1]
Complications
Cerebral oedema
Cerebral oedema is the most feared complication of DKA, occurring in about 0.5-1% of children and young adults (rarely in adults over 20). It carries a mortality of 20-40%. The Glaser NEJM 2001 case-control study identified three risk factors [2]:
- Low initial PaCO2 (reflecting severe acidosis and deeper compensation).
- High initial urea (reflecting severe dehydration).
- Bicarbonate administration — an independent, modifiable risk factor. [1]
The clinical signs appear 4-12 hours into treatment: headache, vomiting, drowsiness, bradycardia, rising blood pressure, pupillary changes, seizures. The moment you suspect it: [1]
- Reduce the fluid rate.
- Give mannitol (0.5-1 g/kg intravenously) or hypertonic 3% saline (2-5 mL/kg).
- Move to ICU for intubation and neuroprotection if the GCS is falling.
- Arrange a CT head (after stabilisation) to confirm and exclude alternatives. [1]
DWE exam trap: Bicarbonate is an independent risk factor for cerebral oedema in DKA (Glaser 2001). Do not give it routinely. [1]
Hypoglycaemia
The most common metabolic complication of treatment. It occurs when the insulin runs without adequate dextrose, or when the FRIII is not reduced as the glucose falls. Prevent it by: [1]
- Switching to dextrose when glucose falls below 14.
- Checking glucose hourly.
- Reducing the FRIII to 0.05 units/kg/hour if glucose is falling faster than 3 mmol/L/hour. [1]
Hypokalaemia
The most dangerous metabolic complication. Potassium falls as insulin drives it into cells and as the acidosis corrects. Prevent it by: [1]
- Checking potassium hourly in the first few hours.
- Adding potassium to the fluid whenever the level is below 5.5.
- Never starting insulin if potassium is below 3.3. [1]
Hypophosphataemia and hypomagnesaemia
Phosphate and magnesium both fall during treatment. Routine phosphate replacement does not improve outcome, but replace if the level is critically low (below 0.3 mmol/L) or if there is respiratory or skeletal muscle weakness. Replace magnesium if low — hypomagnesaemia perpetuates hypokalaemia by making the renal potassium channels leaky. [1]
Acute respiratory distress syndrome (ARDS)
A rare but recognised complication, thought to result from rapid fluid shifts and capillary leak. It presents with hypoxia and bilateral infiltrates. Management is supportive (oxygen, lung-protective ventilation in ICU). [1]
Thromboembolism
In HHS, the severe dehydration and hyperviscosity create a high risk of venous and arterial thrombosis — DVT, PE, myocardial infarction, and stroke are leading causes of death. Prophylactic anticoagulation is routine. [1]
Communication, shared decision-making and follow-up
Explaining the emergency to the family
"Your relative has a condition called diabetic ketoacidosis (or hyperosmolar hyperglycaemic state). It is a medical emergency caused by a lack of insulin (and a trigger like an infection). We are giving intravenous fluids and insulin to correct it, and we are looking for and treating the cause. The treatment takes about 24 hours, and most people recover fully, but we will be watching closely for complications." [1]
Sick-day rules and prevention
The most important long-term intervention after a DKA is patient education — the patient who understands sick-day rules is far less likely to re-present: [1]
- Never stop your insulin when you are unwell — you often need more. Illness raises glucose.
- Check glucose every 2-4 hours and ketones if glucose is above 14.
- If ketones are above 1.5 and rising, or you are vomiting and cannot keep fluids down, seek help immediately.
- Stop SGLT2 inhibitors during acute illness with vomiting, diarrhoea, or reduced intake (the sick-day rule).
- Keep drinking fluids — dehydration is the pathway to DKA. [1]
Recurrent DKA — a special problem
Recurrent DKA, usually from insulin omission, is a form of self-harm often linked to mental illness, substance use, eating disorders, or psychosocial chaos. It carries a high long-term mortality. Management requires a coordinated approach: diabetes team, mental health, social work, and a structured care plan that addresses the root cause, not just the metabolic correction. [1]
Exam traps and high-yield discriminators
- DKA is a ketone problem, not a glucose problem. The insulin runs until ketones are below 0.6, not until glucose is normal. The glucose is managed with dextrose.
- Check the potassium before insulin. If it is below 3.3, replace first.
- Euglycaemic DKA on an SGLT2 inhibitor. A normal glucose does not exclude DKA. Check ketones in any acidotic diabetic.
- HHS is not DKA. Fluid first, low-dose insulin, prophylactic anticoagulation, and treat the precipitant (usually infection). Mortality is 10-20%.
- Cerebral oedema in young patients. Headache, vomiting, drowsiness — give mannitol or hypertonic saline. Bicarbonate increases the risk.
- Correct the sodium. The corrected sodium changes the fluid choice.
- The ketone flip. Monitor with beta-hydroxybutyrate, not urine ketones. Urine ketones can rise during recovery.
- Overlap the transition. Give subcutaneous insulin 30-60 minutes before stopping the FRIII, or the DKA recurs.
- A surgical abdomen can precipitate DKA. Abdominal pain that does not settle is not always just the DKA.
- Pregnancy lowers the threshold for DKA. DKA can occur at a glucose of 10-11 in pregnancy; check ketones in any pregnant diabetic who is unwell. [1]
DCE long-case integration — the complex DKA patient
A long-case patient with DKA will have multi-morbidity: type 1 or type 2 diabetes, a precipitant (infection, infarction, omission), and often an SGLT2 inhibitor or CKD. The candidate's job is to integrate the acute protocol with the precipitant workup and the patient's chronic disease. [1]
Opening statement (SASPOP): "Mr Patel is a 52-year-old man with type 1 diabetes for 30 years, who presents with two days of fever, cough, and vomiting, and is found to be in severe DKA with a pH of 7.05, ketones of 6.2, and glucose of 28, precipitated by a lobar pneumonia. His main problems are the DKA, the pneumonia, an acute kidney injury, and a background of diabetic nephropathy and retinopathy." [1]
Problem list: [1]
- Severe DKA (pH 7.05) — fluid, FRIII, potassium.
- Lobar pneumonia — the precipitant; antibiotics within one hour.
- Acute kidney injury on CKD — nephrology input, adjust doses.
- Diabetic nephropathy and retinopathy — long-term complications; will need follow-up. [1]
Integrated plan: run the JBDS protocol; treat the pneumonia with appropriate antibiotics; monitor renal function; arrange diabetes team review for transition and education. The insight is that the DKA will not resolve if the pneumonia is untreated — the infection is the engine driving the counter-regulatory hormone surge. [1]
Key references and guideline anchoring
- JBDS (UK, primary adult protocol): Savage et al., Diabet Med 2011 (PMID 21255074), updated 2023 — the fluid ladder, FRIII at 0.1 units/kg/hour, potassium targets, dextrose at glucose below 14, resolution criteria [4].
- ADA (US): Kitabchi et al., Diabetes Care 2009 (PMID 19564476) — the consensus on hyperglycaemic crises, criteria, and management [1].
- Cerebral oedema: Glaser et al., NEJM 2001 (PMID 11172153) — the landmark case-control identifying bicarbonate as a modifiable risk factor [2].
- Euglycaemic DKA: Peters et al., Diabetes Care 2015 (PMID 26078479) — the SGLT2 inhibitor association [3].
- Fluid choice: Van Zyl et al., QJM 2012 (PMID 22109683) — the RCT comparing 0.9% saline with Ringer's lactate [5].
The ANZ (ADS/ADIPS) and US (ADA) approaches align with the JBDS on the core protocol — FRIII, fluid resuscitation, potassium first, dextrose switch, resolution by ketones. The fluid choice (0.9% saline vs balanced crystalloid) is the main area of active debate, with the RCT evidence still favouring saline as the default. [1]
References
- [1]Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN Hyperglycemic crises in adult patients with diabetes Diabetes Care, 2009.PMID 19564476
- [2]Glaser N, Barnett P, McCaslin I, et al. Risk factors for cerebral edema in children with diabetic ketoacidosis. The Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics N Engl J Med, 2001.PMID 11172153
- [3]Peters AL, Buschur EO, Buse JB, Cohan P, Diner JC, Hirsch IB Euglycemic Diabetic Ketoacidosis: A Potential Complication of Treatment With Sodium-Glucose Cotransporter 2 Inhibition Diabetes Care, 2015.PMID 26078479
- [4]Savage MW, Dhatariya KK, Kilvert A, et al. Joint British Diabetes Societies guideline for the management of diabetic ketoacidosis Diabet Med, 2011.PMID 21255074
- [5]Van Zyl DG, Rheeder P, Delport E Fluid management in diabetic-acidosis--Ringer's lactate versus normal saline: a randomized controlled trial QJM, 2012.PMID 22109683