Phys · endocrine
Thyroid Disorders
Also known as hyperthyroidism · thyrotoxicosis · Graves disease · toxic multinodular goitre · toxic adenoma · Plummer disease · subacute thyroiditis · de Quervain thyroiditis · postpartum thyroiditis · amiodarone-induced thyrotoxicosis · hypothyroidism · Hashimoto thyroiditis · myxoedema · myxoedema coma · thyroid storm · thyroid nodule · papillary thyroid carcinoma · follicular thyroid carcinoma · medullary thyroid carcinoma · anaplastic thyroid carcinoma · levothyroxine · carbimazole · propylthiouracil · radioiodine
Consultant-physician-depth guide to thyroid disorders — hyperthyroidism (Graves disease, toxic multinodular goitre, toxic adenoma, thyroiditis, amiodarone), thyroid storm, hypothyroidism (Hashimoto thyroiditis, post-treatment, iodine, drugs), myxoedema coma, thyroid nodules (Bethesda classification) and thyroid cancer (papillary, follicular, medullary, anaplastic) — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Thyroid Disorders
The answer first
Thyroid disorders are common, easily tested, and almost always treatable — but the physician exam rewards the candidate who distinguishes the cause of an abnormal thyroid function test rather than treating the number alone. The single most important initial question in any thyrotoxic patient is: is this true hormone overproduction (high radioactive iodine uptake, needs a thionamide, radioiodine or surgery) or a destructive thyroiditis releasing stored hormone (low uptake, self-limiting, never gets antithyroid drugs)? Confusing the two is the classic DWE trap. [1]
The framework is the hypothalamic–pituitary–thyroid axis. TSH is the most sensitive single test because of the log-linear negative-feedback relationship between TSH and free T4 — a small change in free T4 produces a large reciprocal change in TSH. A normal TSH excludes significant thyroid dysfunction in an ambulant outpatient. A suppressed TSH with a raised free T4 (and free T3) is overt thyrotoxicosis; a suppressed TSH with normal free T4 is subclinical hyperthyroidism (or early thyrotoxicosis) and needs repeat testing. A raised TSH with a low free T4 is overt primary hypothyroidism; a raised TSH with a normal free T4 is subclinical hypothyroidism. [1]
The three definitive treatments for Graves hyperthyroidism — antithyroid drugs, radioactive iodine, and surgery — are roughly equivalent in long-term outcome, and the choice is genuinely shared with the patient based on goitre size, eye disease, pregnancy intent, comorbidity and preference. Hypothyroidism, by contrast, is simple: levothyroxine monotherapy, weight-based dosed, titrated to a normalised TSH — with myxoedema coma the one emergency that demands intravenous levothyroxine and hydrocortisone. [1]
Thyroid physiology — why the axis drives interpretation
The thyroid synthesises T4 (thyroxine) and T3 (triiodothyronine) by iodinating tyrosine residues on thyroglobulin. T4 is the predominant secretory product (~80 micrograms/day) but is largely a prohormone; about 80% of circulating T3 is generated by peripheral 5'-deiodination of T4 in the liver, kidney, and target tissues. T3 is roughly four times more potent than T4 at the nuclear receptor. This peripheral conversion matters clinically — it explains why severe non-thyroidal illness shifts T4 to T3 conversion downwards (the "low T3 syndrome"), why amiodarone inhibits conversion (and is a useful second-line drug in thyroid storm, though propylthiouracil does this directly), and why levothyroxine alone replaces thyroid hormone in most patients without needing liothyronine (T3). [1]
TSH, secreted by thyrotrophs in the anterior pituitary, is itself regulated by TRH from the hypothalamus. The feedback loop is exquisitely sensitive. The log-linear relationship means TSH changes exponentially for an arithmetic change in free T4 — which is why TSH is the screening test of choice and why a TSH of 0.1 and 0.01 represent very different degrees of thyrotoxicosis. [1]
DWE high-yield: In an unwell inpatient, thyroid function tests can be misleading — the non-thyroidal illness syndrome (euthyroid sick syndrome) gives low T3, then low T4, and an inappropriately normal or low TSH. Do not diagnose new thyroid disease on a single set of inpatient TFTs. Recheck when the patient is well. [1]
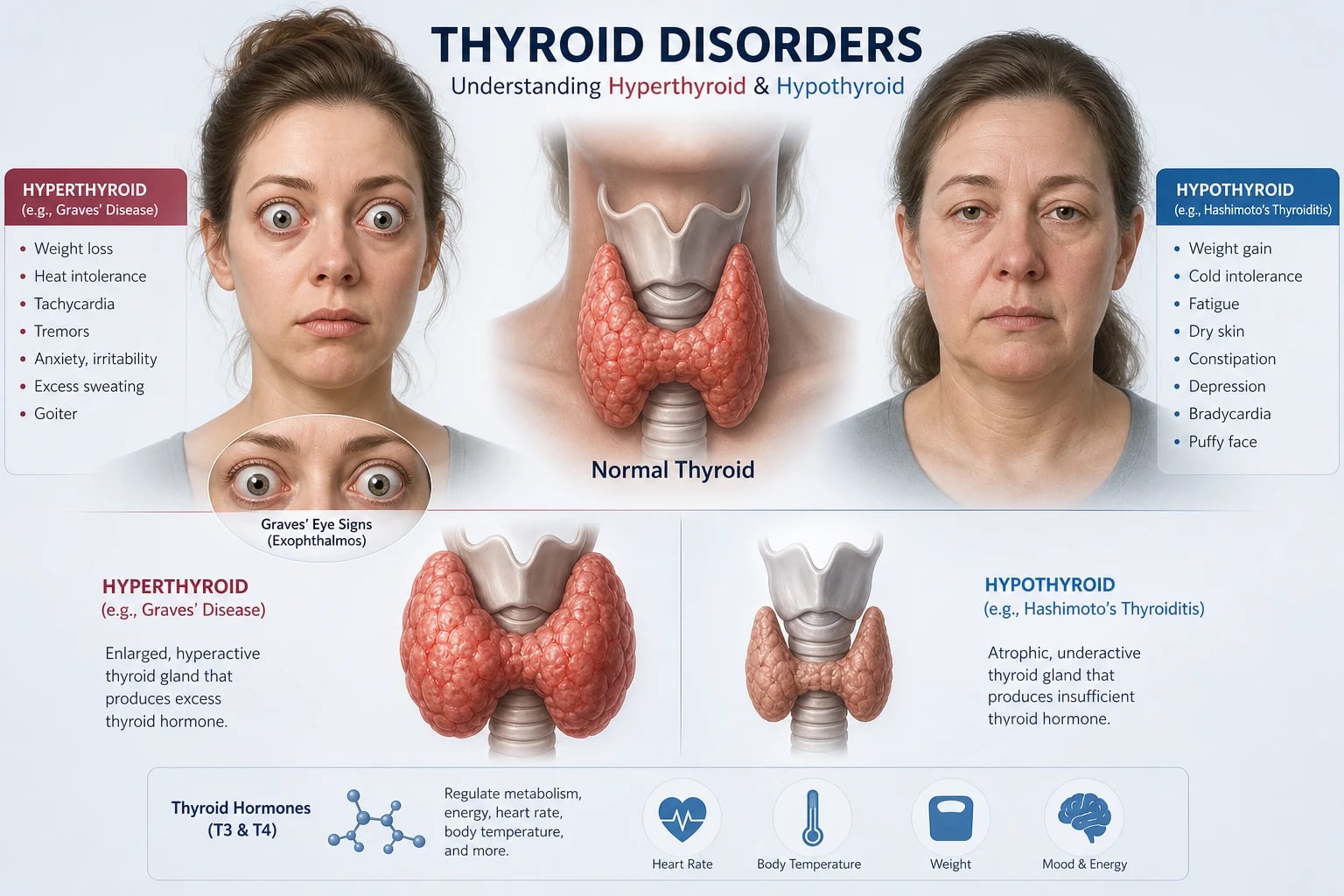
Hyperthyroidism and thyrotoxicosis
The terms overlap but are not identical. Thyrotoxicosis is the clinical state of excess thyroid hormone from any cause. Hyperthyroidism is thyrotoxicosis specifically caused by de novo hormone synthesis by the gland (Graves disease, toxic multinodular goitre, toxic adenoma, TSH-secreting adenoma, hCG-mediated, iodine-induced). Destructive release of preformed hormone — the thyroiditides — causes thyrotoxicosis but is not hyperthyroidism. The distinction is operationalised by the 24-hour radioactive iodine uptake (RAIU) scan: high uptake = true hyperthyroidism; low uptake = destructive or exogenous. [1]
Causes — the discriminating framework
| Cause | Mechanism | RAIU | Antibodies | Goitre |
|---|---|---|---|---|
| Graves disease | TSH receptor-stimulating antibody | Diffusely increased | TSH receptor antibody positive | Diffuse, smooth, bruit |
| Toxic multinodular goitre | Autonomous nodules | Patchy increased | Negative | Multinodular |
| Toxic adenoma (Plummer) | Single autonomous nodule | Single hot focus | Negative | Single palpable nodule |
| Subacute (de Quervain) thyroiditis | Viral granulomatous destruction | Low/suppressed | Negative initially | Tender, firm |
| Silent (painless) thyroiditis | Autoimmune destruction | Low | Anti-TPO often positive | Mild, non-tender |
| Postpartum thyroiditis | Autoimmune destruction postpartum | Low | Anti-TPO positive | Mild, non-tender |
| Amiodarone type 1 | Iodine-induced synthesis (Jod-Basedow) | Normal or increased | Negative | Nodular |
| Amiodarone type 2 | Destructive folliculitis | Low/suppressed | Negative | Normal |
| TSH-secreting pituitary adenoma | Inappropriate TSH drive | Increased | Negative | Diffuse |
| Exogenous (factitious) thyroid hormone | Excess levothyroxine or T3 | Low/suppressed | Negative | Atrophic / absent |
| Struma ovarii | Ectopic thyroid tissue in ovarian teratoma | Low at neck | Negative | Normal neck gland |
Graves disease is the commonest cause of hyperthyroidism in young adults (peak 20 to 40 years, female-to-male ratio 5 to 10:1) [1]. It is an autoimmune disorder driven by a TSH receptor stimulating antibody (TRAb) that mimics TSH at the receptor, causing diffuse follicular hyperplasia, increased synthesis and release of T4 and T3, and the characteristic smooth, diffuse goitre with an audible bruit from hypervascularity. The same autoimmune process, in genetically susceptible individuals (HLA-DR3, HLA-B8, CTLA-4), causes Graves orbitopathy in about 30 to 50% and, less commonly, pretibial myxoedema (dermopathy) and thyroid acropachy. TRAb is the diagnostic cornerstone — a positive TRAb in a thyrotoxic patient is Graves disease, no further imaging required [1].
Toxic multinodular goitre (TMNG) is the commonest cause in older adults living in iodine-deficient regions. Multiple autonomous nodules gradually evolve over years; the patient presents with subclinical or overt thyrotoxicosis, often triggered by an iodine load (contrast, amiodarone, iodine supplements). The goitre is large, multinodular, often retrosternal. TRAb is negative and the uptake scan shows patchy uptake with suppression of the intervening parenchyma. Apathetic hyperthyroidism — weight loss, atrial fibrillation, heart failure without adrenergic features — is classical in this population. [1]
Toxic adenoma (Plummer disease) is a single hyperfunctioning nodule that suppresses TSH and the surrounding gland. The patient is typically older than the Graves patient, has a single palpable nodule, and the uptake scan shows a single hot focus with suppression of the rest of the gland. Treatment is radioiodine (which selectively ablates the nodule) or surgery. [1]
Subacute (de Quervain) thyroiditis is a granulomatous thyroiditis following a viral upper respiratory tract infection (coxsackie, echovirus, mumps, influenza, SARS-CoV-2), associated with HLA-B35 [5]. The classic triphasic pattern: an initial thyrotoxic phase (1 to 3 months, neck pain radiating to the jaw, raised ESR and CRP, low RAIU), a hypothyroid phase (2 to 6 months), and recovery to euthyroidism in over 90%. About 15% develop permanent hypothyroidism [5]. Treatment is NSAIDs for mild pain and oral prednisolone 40mg daily tapered over 2 to 6 weeks for severe pain. Beta-blockade controls symptoms in the thyrotoxic phase. Antithyroid drugs do not work and must not be given.
Postpartum thyroiditis occurs in 5 to 10% of women within the first postpartum year, strongly associated with anti-TPO positivity. The same triphasic pattern; transient but 20 to 40% develop permanent hypothyroidism within 5 to 10 years. [1]
Amiodarone-induced thyrotoxicosis (AIT) is a high-yield topic because amiodarone is both iodine-rich (each 200mg tablet contains 75mg of iodine) and a direct follicular toxin, and because the underlying cardiac disease constrains management [6]. Type 1 is iodine-induced synthesis in an abnormal gland (nodular goitre or latent Graves) — treated with thionamides, often combined with potassium perchlorate; colour-flow Doppler shows increased vascularity. Type 2 is a destructive folliculitis in a normal gland — treated with oral glucocorticoids (prednisolone 40 to 60mg daily tapered over months); Doppler shows absent vascularity. Mixed forms are common; when the type is unclear, combined thionamide plus glucocorticoid is reasonable. The decision to continue or stop amiodarone is individualised — withdrawal is often impractical for life-threatening arrhythmias, and the drug's long tissue half-life means stopping has limited short-term effect [6].
DWE trap: "A 68-year-old man on amiodarone for ventricular tachycardia presents with new atrial fibrillation and weight loss, TSH suppressed, free T4 elevated. The colour-flow Doppler shows normal vascularity and the gland is non-tender." The discriminator is the Doppler — increased vascularity suggests type 1 (treat with thionamide), absent vascularity suggests type 2 (treat with glucocorticoid). In mixed or indeterminate cases, combine both. Continuing or stopping amiodarone is a cardiology-shared decision, not a reflex. [1]
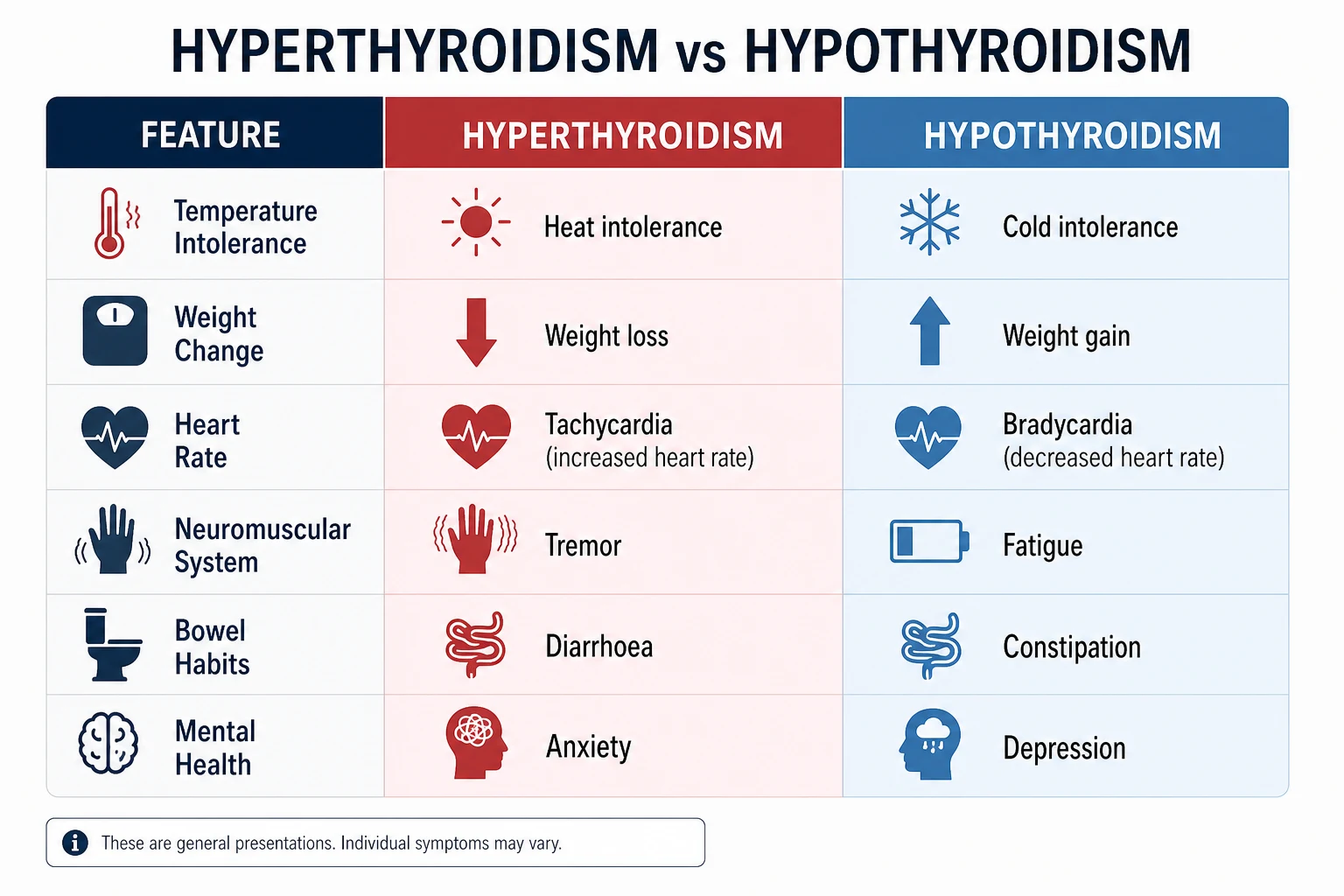
Clinical features of thyrotoxicosis
The clinical syndrome reflects a hypermetabolic state with adrenergic overdrive: [1]
| System | Hyperthyroid features |
|---|---|
| Constitutional | Heat intolerance, weight loss with increased appetite, fatigue, proximal myopathy |
| Cardiovascular | Palpitations, sinus tachycardia, atrial fibrillation (10 to 20%, higher in older adults), wide pulse pressure, high-output cardiac failure |
| Neuromuscular | Fine tremor, hyperreflexia, proximal muscle wasting, periodic paralysis (Asian men, low potassium), chorea |
| Gastrointestinal | Hyperdefaecation, steatorrhoea |
| Reproductive | Oligomenorrhoea, infertility, gynaecomastia, reduced libido |
| Dermatological | Warm moist palms, onycholysis (Plummer nails), palmar erythema, alopecia, pretibial myxoedema (Graves) |
| Psychiatric | Anxiety, irritability, insomnia, on occasion psychosis |
Graves orbitopathy is pathognomonic of Graves disease and is a long-case favourite. The autoimmune infiltration of orbital fat and extraocular muscles by TSH receptor antibody cross-reacting T cells produces: lid retraction and lid lag (sympathetic overdrive and Müller muscle overactivity); proptosis / exophthalmos (measured by Hertel exophthalmometry); extraocular muscle involvement (inferior and medial rectus most often — diplopia, ophthalmoplegia); soft tissue inflammation (chemosis, conjunctival injection, lid oedema); and the emergency — optic nerve compression (visual loss, colour desaturation, relative afferent pupillary defect). Smoking is the strongest modifiable risk factor and worsens treatment response. Severity is graded (NOSPECS) and activity by the clinical activity score (CAS) [4].
DCE short-case: When examining the thyroid patient, present systematically from the end of the bed: "On inspection there is bilateral proptosis with lid retraction and lid lag, a diffuse goitre visible in the neck, and a fine tremor of the outstretched hands. The pulse is irregularly irregular at 110. Eye signs indicate Graves disease." Then complete: visual acuity, colour vision (Ishihara), eye movements, exophthalmometry, fundoscopy for disc swelling. [1]
Investigations
The investigative strategy is staged and cause-directed: [1]
- TSH (suppressed), then free T4 and free T3 (raised). The T3-to-T4 ratio helps — Graves and toxic multinodular goitre raise both; some adenomas and early Graves are T3-toxicotic (free T3 high, free T4 normal) and easily missed if only T4 is measured.
- TSH receptor antibody (TRAb) — the modern first-line cause-discriminating test. A positive TRAb in a thyrotoxic patient confirms Graves and obviates the uptake scan [1]. Reserve the scan for TRAb-negative or equivocal cases.
- 24-hour radioactive iodine uptake (RAIU) scan — when the cause is unclear. High diffuse uptake (Graves), patchy uptake (TMNG), single hot focus (toxic adenoma), low or suppressed uptake (thyroiditis, exogenous, iodine load). Contraindicated in pregnancy and breastfeeding, and unreliable within 6 to 8 weeks of iodinated contrast.
- Thyroid ultrasound — goitre characterisation, nodule risk-stratification, colour-flow Doppler for amiodarone type discrimination.
- Anti-TPO — supportive in Hashimoto (hypothyroid) and postpartum/silent thyroiditis; not diagnostic alone.
- ESR and CRP — markedly raised in subacute thyroiditis; helps discriminate from Graves.
- ECG — atrial fibrillation in 10 to 20%, especially older patients.
- Other — consider calcitonin if a nodule raises medullary carcinoma suspicion (family history, MEN2); consider pituitary MRI and alpha-subunit if a TSH-secreting adenoma is suspected (inappropriately normal or raised TSH with raised free T4).
Management of hyperthyroidism
The 2016 ATA/AETA guidelines frame three definitive options — antithyroid drugs, radioactive iodine (I-131), and surgery — as roughly equivalent, with the choice driven by goitre size, eye disease, pregnancy intent, comorbidity and patient preference [1].
Antithyroid drugs (thionamides)
Carbimazole (methimazole in the US) is first-line outside pregnancy. It inhibits thyroperoxidase, blocking iodination of tyrosine. It is preferred over propylthiouracil (PTU) because it is once daily, more potent, and far less hepatotoxic (PTU carries a black-box warning for fulminant hepatic necrosis). The starting dose is 10 to 40mg daily depending on severity. Two regimens: [1]
- Titration regimen — start carbimazole 20 to 40mg daily, titrate down as the patient becomes euthyroid, then a low maintenance dose (5 to 10mg daily) for 12 to 18 months. Remission rate 40 to 50%; relapse rate 50 to 60% on stopping.
- Block-replace regimen — high-dose carbimazole (40 to 60mg daily, fully blocking synthesis) plus levothyroxine 100 micrograms daily to prevent hypothyroidism. Comparable remission rates; preferred where frequent monitoring is impractical, and where levothyroxine adds stability [1].
Propylthiouracil (PTU) has the same thyroperoxidase action but additionally inhibits peripheral T4-to-T3 conversion at higher doses — useful in thyroid storm. PTU is first-line in the first trimester of pregnancy (carbimazole is teratogenic — aplasia cutis, choanal atresia, tracheo-oesophageal fistula, omphalocele) and in thyroid storm. Switch back to carbimazole from 16 weeks to limit PTU hepatotoxicity. Dose 100 to 600mg daily in divided doses. [1]
Adverse effects of thionamides:
- Agranulocytosis — occurs in 0.2 to 0.5%, typically within the first three months. The cardinal warning: every patient must be told to stop the drug and present urgently with fever, sore throat or mouth ulceration for a full blood count. If neutrophils are below 0.5, stop the drug, give broad-spectrum antibiotics, and switch to a different definitive therapy (the other thionamide is not safe — cross-reactivity). Routine FBC monitoring is not recommended (too low a yield), but a baseline FBC is sensible.
- Hepatotoxicity — carbimazole causes cholestatic dysfunction; PTU causes acute hepatocellular necrosis (rarely fulminant, needing transplant). Check LFTs at baseline and on clinical concern.
- Skin rash and urticaria — common, usually mild, often settles with antihistamine; severe rash warrants switching thionamide.
- ANCA-positive vasculitis — rare, more with PTU. [1]
Radioactive iodine (I-131)
Radioiodine ablation is definitive, outpatient, and effective — the goal is hypothyroidism (the patient is then committed to lifelong levothyroxine, which is straightforward). The 2016 guidelines position radioiodine as a first-line option for Graves disease, TMNG and toxic adenoma [1]. Contraindications: pregnancy (absolute), breastfeeding, inability to comply with isolation precautions, and active moderate-severe Graves orbitopathy (radioiodine can worsen eye disease — give prophylactic prednisolone if radioiodine is unavoidable). Counsel patients on radiation hygiene for 1 to 2 weeks (limit close contact with children and pregnant women, separate bathrooms, contraception). Antithyroid drugs must be stopped 3 to 7 days before treatment (carbimazole 5 to 7 days, PTU 4 to 6 days — PTU has a longer radioprotective effect) and can resume after 3 to 7 days if needed. Onset of effect over 6 to 18 weeks; about half of patients need a second dose.
Surgery (thyroidectomy)
Surgery is preferred when: a large compressive goitre (stridor, dysphagia), a suspicious or confirmed malignant nodule, pregnancy with poorly controlled disease or antithyroid drug allergy, coexisting hyperparathyroidism, or patient choice. Total or near-total thyroidectomy is now standard for Graves; subtotal thyroidectomy is an older technique. Render the patient euthyroid before surgery — carbimazole to euthyroid, then Lugol's iodine 5 to 7 drops three times daily for 10 days pre-operatively to reduce gland vascularity, plus beta-blockade. Complications: recurrent laryngeal nerve injury (hoarseness — assess vocal cords pre- and post-op), hypoparathyroidism (hypocalcaemia — check calcium post-op and discharge with calcium and calcitriol if needed), haematoma (airway emergency), and permanent hypothyroidism (expected after total thyroidectomy — lifelong levothyroxine). [1]
DCE trap: When asked "what is the best definitive treatment for this patient?" the answer is rarely single — the examiner wants to see you weigh the options by the patient's context. A young woman planning pregnancy and with mild eye disease — antithyroid drugs first, aiming for remission. An older man with a large compressive goitre and atrial fibrillation — surgery or radioiodine. A pregnant woman in the second trimester uncontrolled on PTU — surgery in the second trimester. State the reasoning, then the choice. [1]
Thyroid storm — the endocrine emergency
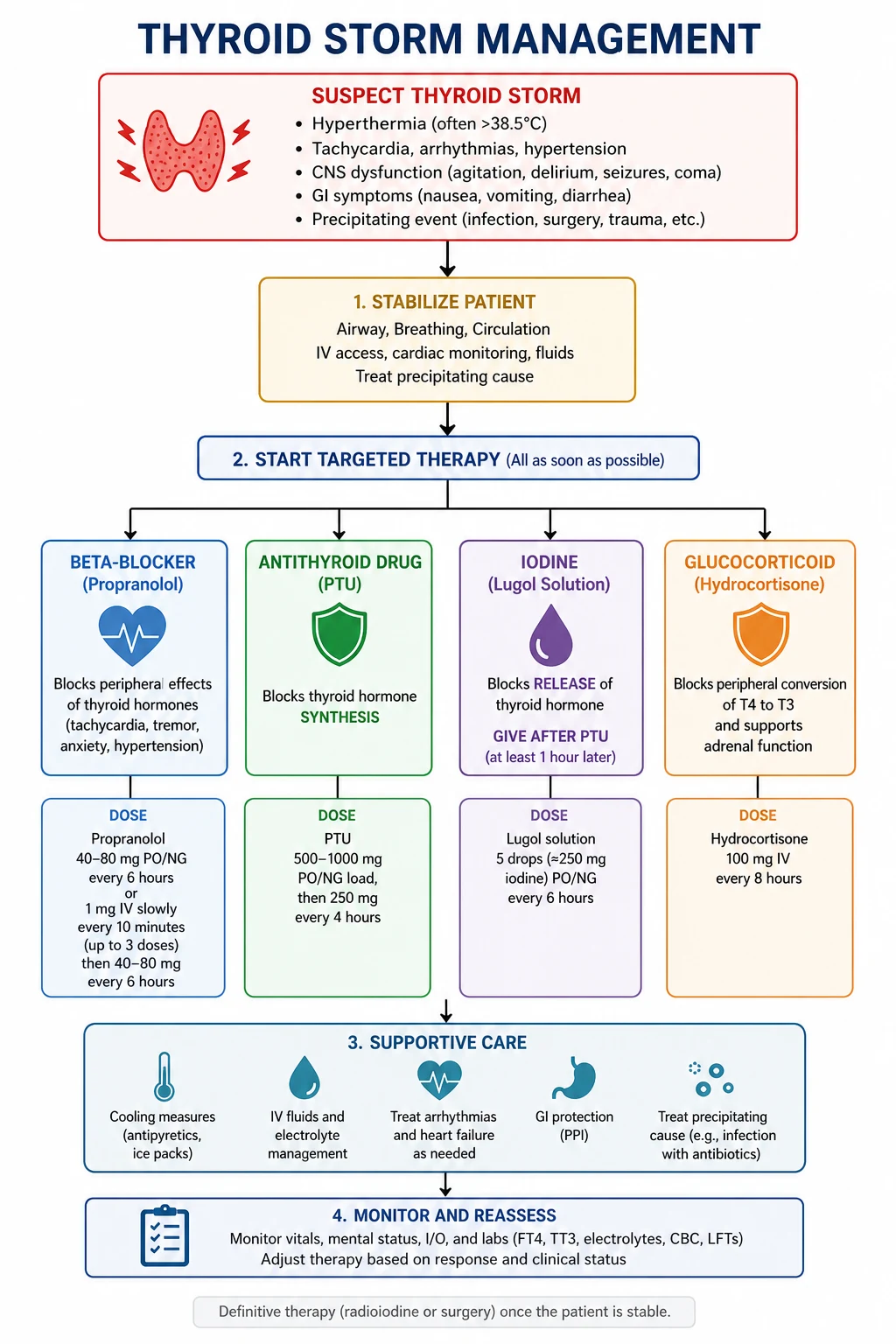
Thyroid storm is the life-threatening decompensation of severe thyrotoxicosis, carrying 10 to 30% mortality. The clinical diagnosis uses the Burch-Wartofsky point score (thermoregulatory dysfunction, central nervous system effects, gastrointestinal-hepatic dysfunction, cardiovascular dysfunction, precipitant history). A score above 45 is highly suggestive. [1]
Precipitants — almost always identifiable: infection (pneumonia, urosepsis), surgery (especially thyroidectomy on an unprepared gland), radioactive iodine treatment, iodine load (contrast, amiodarone), trauma, DKA, stroke, parturition, withdrawal of or non-adherence with antithyroid drugs. [1]
Clinical features — hyperpyrexia (often above 40 degrees Celsius, distinguishes from uncomplicated thyrotoxicosis), severe tachycardia or tachyarrhythmia (atrial fibrillation, ventricular arrhythmia), high-output cardiac failure, agitation, delirium, seizures, coma, vomiting, diarrhoea, jaundice. [1]
Emergency management — simultaneous, multi-modal, in ICU: [1]
- Supportive care — ABC, IV fluids, cooling (paracetamol, cooling blankets; avoid salicylates which displace T4 from thyroid-binding globulin and worsen thyrotoxicosis), oxygen, treat the precipitant.
- Beta-blockade — propranolol 60 to 80mg orally every 4 hours, or 1 to 2mg IV slowly every 15 minutes (or esmolol infusion if asthmatic or in heart failure — short half-life, titratable). Propranolol at higher doses also inhibits T4-to-T3 conversion. Use with care in heart failure — a fast rate may be the only thing maintaining cardiac output; consider esmolol in ICU with monitoring.
- Thionamide — propylthiouracil 500 to 1000mg loading, then 250mg every 4 hours (preferred over carbimazole because PTU also blocks peripheral T4-to-T3 conversion). Give orally or via NGT. PTU needs to be given before iodine.
- Iodine (Lugol's) — one hour after PTU — to invoke the Wolff-Chaikoff effect (iodine suppresses hormone release) and block new synthesis. Lugol's iodine 8 to 10 drops every 6 to 8 hours, or saturated solution of potassium iodide (SSKI) 5 drops every 6 hours. The sequencing is essential: iodine given first would fuel new hormone synthesis (Jod-Basedow effect) [1].
- Glucocorticoid — hydrocortisone 100mg IV every 8 hours. Treats any coexisting adrenal insufficiency (the hypermetabolic state increases cortisol clearance), and inhibits T4-to-T3 conversion and reduces TSH release.
- Treat the precipitant — antibiotics for infection, glucose and fluid for DKA, anticoagulation for atrial fibrillation.
- Definitive treatment once stable — typically radioiodine after recovery, or surgery after careful preparation.
DWE high-yield: The order matters. Beta-blocker first (symptom and conversion control), then PTU (block synthesis and conversion), then iodine at least one hour after the PTU (block release), then hydrocortisone. Treat the precipitant throughout. Lithium or cholestyramine can be added in refractory cases. [1]
Hypothyroidism
Hypothyroidism is common — prevalence about 5% overt and a further 5% subclinical, female predominance, rising with age. Hashimoto thyroiditis is the commonest cause in iodine-sufficient regions (Australia, NZ, UK, US), followed by post-treatment hypothyroidism (radioiodine, surgery), iodine deficiency (the commonest cause globally), and drugs (amiodarone, lithium, interferon, tyrosine kinase inhibitors such as sunitinib). [1]
Causes
| Cause | Mechanism |
|---|---|
| Hashimoto thyroiditis | Autoimmune lymphocytic infiltration with anti-TPO and anti-Tg; progressive follicular destruction |
| Post-radioiodine or post-surgical | Loss of functioning tissue |
| Iodine deficiency | Substrate deficiency (commonest globally) |
| Iodine excess | Wolff-Chaikoff effect (paradoxical) |
| Drugs — amiodarone, lithium, interferon, sunitinib, amiodarone | Multiple mechanisms |
| Central (secondary) hypothyroidism | Pituitary or hypothalamic disease — low TSH with low free T4 |
| Congenital | Dyshormonogenesis, thyroid agenesis |
Hashimoto thyroiditis is the prototype autoimmune thyroid disease. Antithyroid peroxidase (anti-TPO) and antithyroglobulin (anti-Tg) antibodies are the serological markers; anti-TPO is the more sensitive and is present in over 90% of patients [9]. The histology shows lymphocytic infiltration with Hürthle cell metaplasia and atrophy. The disease is far more common in women, peaks at 30 to 50 years, clusters with other autoimmune diseases (type 1 diabetes, coeliac disease, vitiligo, pernicious anaemia, Addison disease, premature ovarian failure). The clinical course is progressive — many patients present with subclinical disease (raised TSH, normal free T4) and progress to overt hypothyroidism over years; the presence of anti-TPO and a TSH above 10 mIU/L predicts progression. Hashimoto can rarely present with a transient hashitoxicosis phase — destructive release of stored hormone producing transient thyrotoxicosis, distinguished from Graves by a low RAIU and negative TRAb [9].
Clinical features of hypothyroidism
The syndrome reflects a general slowing of metabolism: [1]
| System | Hypothyroid features |
|---|---|
| Constitutional | Cold intolerance, weight gain (modest), fatigue, lethargy |
| Cardiovascular | Bradycardia, diastolic hypertension, pericardial effusion (rare tamponade), dyslipidaemia, accelerated atherosclerosis |
| Neuromuscular | Delayed relaxation of deep tendon reflexes, proximal myopathy, carpal tunnel syndrome, sensorineural deafness, ataxia |
| Gastrointestinal | Constipation, ileus, ascites (rare) |
| Reproductive | Menorrhagia, infertility, galactorrhoea (TRH stimulates prolactin), reduced fertility |
| Dermatological | Cool, dry, pale skin; periorbital puffiness; myxoedema (GAG deposition in dermis); brittle hair; slow-growing nails |
| Psychiatric | Depression, cognitive slowing; rarely myxoedema madness |
| Haematological | Macrocytic anaemia (often coexisting pernicious anaemia), normocytic anaemia of chronic disease |
Investigations
- TSH raised, free T4 low — overt primary hypothyroidism.
- TSH raised (usually above 10 mIU/L), free T4 normal — subclinical or early overt.
- Anti-TPO — confirms autoimmune aetiology and predicts progression.
- Other supportive — raised CK, raised LDL and total cholesterol, hyponatraemia (mild), macrocytosis (check B12 and folate), raised prolactin.
- Central hypothyroidism — low free T4 with inappropriately low or normal TSH; check pituitary axis and request MRI pituitary. [1]
Management — levothyroxine
Levothyroxine (T4) monotherapy remains the standard of care [2]. The starting dose is weight-based:
| Patient | Starting dose |
|---|---|
| Young, healthy, overt disease | 1.6 micrograms/kg/day (full replacement) |
| Older or with cardiac disease | Start 25 to 50 micrograms daily, titrate every 4 to 6 weeks |
| Subclinical hypothyroidism | 25 to 50 micrograms daily if TSH above 10, or symptomatic with antibodies |
| Pregnancy | Increase existing dose by 25 to 30% at confirmation of pregnancy |
Take on an empty stomach, at least 30 minutes before breakfast (absorption is reduced by food, calcium, iron, proton pump inhibitors, coffee, soy). Recheck TSH at 6 weeks (TSH half-life is 7 days — free T4 normalises first, TSH trails). The target TSH is within the reference range (typically 0.4 to 4.0 mIU/L); some aim for the lower half in younger patients. Once stable, check TSH annually. [1]
Combination T4/T3 therapy — the ATA guidelines conclude there is insufficient consistent evidence to recommend liothyronine (T3) combination therapy over levothyroxine alone [2]. A minority of patients remain symptomatic despite a normal TSH; a careful trial of combination therapy is a reasonable shared decision in a fully informed patient, but it is not standard of care.
DWE trap: "An 80-year-old woman is started on full-dose levothyroxine 100 micrograms daily for overt hypothyroidism. Three days later she is admitted with new angina and atrial fibrillation." The error is starting full replacement in an older patient or one with cardiac disease. Always start low (25 to 50 micrograms) and titrate slowly — levothyroxine increases myocardial oxygen demand and can precipitate angina, infarction or arrhythmia in susceptible patients. [1]
Myxoedema coma
Myxoedema coma is the rare, life-threatening decompensation of severe, prolonged hypothyroidism — mortality 20 to 60% without prompt treatment. The classic patient is an older woman with undiagnosed or undertreated hypothyroidism who decompensates after a precipitant: infection (pneumonia, urosepsis), cold exposure, sedatives, opioids, anaesthesia, gastrointestinal bleed, stroke, myocardial infarction, or withdrawal of levothyroxine. [1]
Clinical features — the triad: hypothermia (often below 35 degrees, may be profound), altered mental state (lethargy progressing to stupor and coma, sometimes seizures), and hypoventilation (hypercapnic respiratory failure — a key cause of death). Look for the stigmata of severe hypothyroidism: bradycardia, hyponatraemia (dilutional from inappropriate ADH), hypoglycaemia, ileus, pericardial or pleural effusions, myxoedematous facies. [1]
Management — simultaneous, multi-modal, in ICU: [1]
- Supportive care — ABC, mechanical ventilation for hypoventilation (often needed), slow passive rewarming (rapid external warming causes vasodilation and cardiovascular collapse — use blankets, treat the thyroid failure and the temperature will correct), IV fluids (cautiously — hyponatraemia from ADH excess; may need hypertonic saline if severe), correct hypoglycaemia.
- Thyroid hormone replacement — IV levothyroxine. The loading dose is 200 to 500 micrograms IV, then 50 to 100 micrograms IV daily until oral absorption is reliable. Some add IV liothyronine (T3) 10 micrograms every 8 hours in severe cases — T3 is the active hormone at the receptor, and peripheral conversion is impaired in myxoedema. The theoretical risk of T3 is cardiac ischaemia from rapid metabolic support; weigh this against the severity of coma. [1]3. Hydrocortisone 100mg IV every 8 hours — coexisting autoimmune adrenal insufficiency is common in autoimmune thyroid disease, and the hypermetabolic state increases cortisol demand. Check a random cortisol and ACTH beforehand, but do not wait for the result — give empirically and taper as the patient recovers.
- Treat the precipitant — antibiotics, withdraw offending drugs, treat cardiac ischaemia.
- Avoid sedatives, opioids, and cold-exposure throughout. [1]
DWE high-yield: The diagnostic principle — myxoedema coma is a clinical diagnosis made at the bedside, not waited for on biochemistry. A hypothermic, hyponatraemic, hypoventilating obtunded older patient with stigmata of hypothyroidism is in myxoedema coma. Treat empirically with IV levothyroxine, hydrocortisone, and supportive care while the laboratory confirms. Mortality is high and rises with delay. [1]
Thyroid nodules
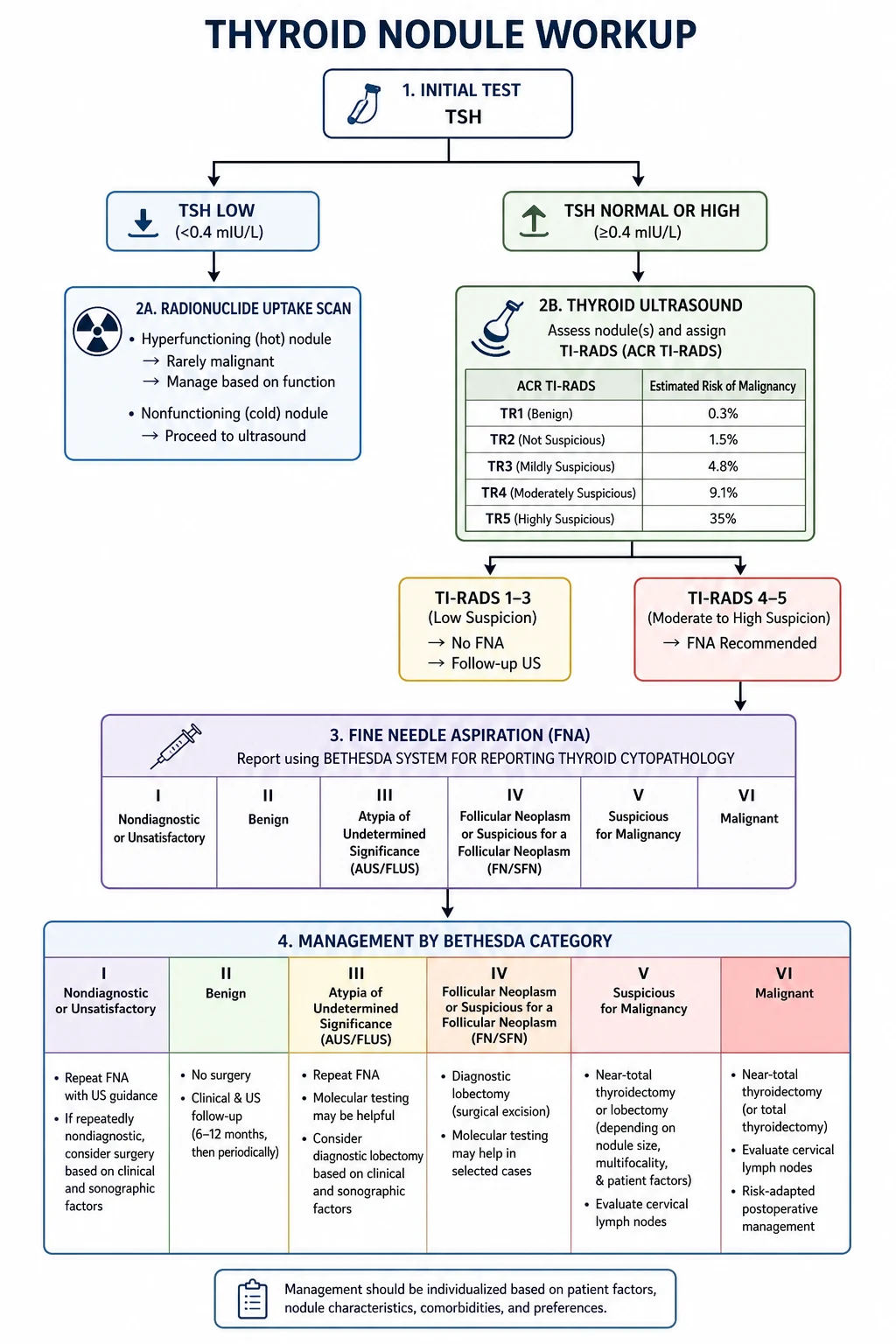
Thyroid nodules are found in 5 to 10% of adults on palpation and 19 to 67% on high-resolution ultrasound. The vast majority are benign. The aim of the workup is to identify the 5 to 15% that are malignant without over-investigating the rest. The 2015 ATA guidelines give a risk-stratified algorithm [3].
Workup
- TSH first. A suppressed TSH suggests autonomy (toxic adenoma, TMNG) — these nodules are usually benign and an uptake scan (rather than FNA) is the next test. A normal or raised TSH does not exclude autonomy and the nodule proceeds to ultrasound.
- Thyroid ultrasound with TI-RADS (Thyroid Imaging Reporting and Data System). High-risk features: hypoechogenicity, microcalcifications, irregular margins, taller-than-wide shape, extrathyroidal extension, abnormal lymph nodes. TI-RADS scores these features and assigns a category that directs whether to FNA.
- Fine-needle aspiration (FNA) — for nodules meeting size and TI-RADS criteria. Ultrasound-guided FNA is the standard.
- FNA cytology reported by the Bethesda System — six categories that direct management [8]:
| Bethesda | Category | Risk of malignancy | Usual management |
|---|---|---|---|
| I | Non-diagnostic / unsatisfactory | 5 to 10% | Repeat FNA with ultrasound guidance |
| II | Benign | 0 to 3% | Clinical and ultrasound surveillance |
| III | Atypia of undetermined significance (AUS) / follicular lesion of undetermined significance (FLUS) | 10 to 30% | Repeat FNA, molecular testing, or diagnostic lobectomy |
| IV | Follicular neoplasm / suspicious for follicular neoplasm | 25 to 40% | Diagnostic lobectomy (or molecular testing) |
| V | Suspicious for malignancy | 50 to 75% | Near-total thyroidectomy or lobectomy |
| VI | Malignant | 97 to 100% | Near-total thyroidectomy (with appropriate staging) |
- Calcitonin — if medullary carcinoma is suspected (family history, MEN2, calcification pattern, or suspicious cytology). A basal calcitonin above 100 pg/mL is highly suggestive.
- Molecular testing (Afirma, Thyroseq) — increasingly used for Bethesda III and IV nodules to triage surgery versus surveillance.
- CT or MRI of neck and thorax — for retrosternal extension, airway compression, or invasive malignancy. [1]
DCE trap: "A 45-year-old woman has a 3cm solitary thyroid nodule, TSH normal, no cervical lymphadenopathy. Ultrasound shows a solid hypoechoic nodule with microcalcifications. What is the next step?" The answer is ultrasound-guided FNA — the suspicious ultrasound features mandate cytology, not surveillance or scan. The TSH is normal, so an uptake scan does not help. [1]
Thyroid cancer
Thyroid cancer represents about 1% of all malignancies and is the commonest endocrine malignancy. The four histological types have very different biology: [1]
| Type | Frequency | Prognosis | Key features |
|---|---|---|---|
| Papillary | 80 to 85% | Excellent (10-year survival over 95%) | Lymphatic spread, psammoma bodies, orphan Annie nuclei, RET/PTC and BRAF V600E mutations |
| Follicular | 10 to 15% | Good (10-year survival 85%) | Haematogenous spread (bone, lung), capsular and vascular invasion (needs histology not cytology to diagnose), RAS mutations |
| Medullary | 2 to 3% | Variable (10-year survival 75%) | Parafollicular C cells, calcitonin, RET proto-oncogene, MEN2 association |
| Anaplastic | 1 to 2% | Very poor (median survival 4 to 6 months) | Older patients, rapidly enlarging mass, undifferentiated |
Papillary thyroid carcinoma is the commonest and most indolent. It presents as a thyroid nodule or cervical lymphadenopathy (cystic lymph nodes are a clue). Histological variants: classical, follicular variant (now partly reclassified as NIFTP — non-invasive follicular thyroid neoplasm with papillary-like nuclear features, which is essentially benign), tall cell (more aggressive), hobnail. Management: total thyroidectomy (with central and lateral neck dissection if nodes involved), often followed by radioiodine ablation for intermediate and high-risk disease, then TSH suppression with levothyroxine. Staging uses the AJCC TNM (8th edition) — age 55 is the critical cut-off: under 55 without distant metastases is stage I; over 55 has more nuanced staging. The dynamic risk stratification (ATA low / intermediate / high) integrates stimulated thyroglobulin, imaging and response to therapy [3].
Follicular thyroid carcinoma is distinguished from a benign follicular adenoma only by capsular or vascular invasion on histology — FNA cannot make the diagnosis (Bethesda IV is "follicular neoplasm" — surgery needed). It spreads haematogenously to bone and lung. A Hürthle cell variant is more aggressive and less radioiodine-avid. [1]
Medullary thyroid carcinoma (MTC) arises from parafollicular C cells, secretes calcitonin (the tumour marker), and is hereditary in 25% via germline RET proto-oncogene mutations (MEN2A, MEN2B, familial MTC). Every patient with MTC must have germline RET testing — a positive result identifies kindreds at risk, and prophylactic thyroidectomy is recommended in RET-positive children (the age depends on the mutation — MEN2B as early as infancy). Calcitonin doubling time is the strongest prognostic marker. Treatment is total thyroidectomy with central node dissection; radioiodine is ineffective (C cells do not uptake iodine). Tyrosine kinase inhibitors (cabozantinib, vandetanib) are options in advanced disease [7].
Anaplastic thyroid carcinoma is one of the most aggressive human malignancies. The patient — typically older — presents with a rapidly enlarging, painful neck mass, dysphagia, stridor, and hoarseness from recurrent laryngeal nerve invasion. The disease is almost universally fatal within months. Treatment is multimodality palliative — surgery where resectable (rare), external beam radiotherapy, and chemotherapy (taxanes, platinums) — but the priority is symptom control, airway maintenance, and goals-of-care discussion [3].
DWE high-yield: When given a thyroid nodule case, the discriminator is the Bethesda category. Bethesda III and IV are the zones of greatest uncertainty — know the malignancy risks (10 to 30% and 25 to 40%) and the management (repeat FNA or molecular testing for III; diagnostic lobectomy for IV). Bethesda V and VI go to surgery. Bethesda II is benign and is surveilled. [1]
Thyroid disease in pregnancy
Thyroid disease in pregnancy is a viva and long-case staple because the physiology and the pharmacology interact. hCG shares its alpha subunit with TSH and is a weak TSH agonist — in the first trimester, high hCG can cause gestational transient thyrotoxicosis (transient, non-autoimmune, often with hyperemesis gravidarum). Total T4 and T3 rise in pregnancy (thyroid-binding globulin increases under oestrogen); the free T4 and TSH (trimester-specific reference ranges) are the tests to use. TRAb crosses the placenta and can cause fetal and neonatal hyperthyroidism — measure TRAb at 20 to 24 weeks in a woman with current or past Graves; if elevated, monitor the fetus for tachycardia, growth restriction, and goitre [1].
- Overt hypothyroidism in pregnancy — treat aggressively; target TSH below 2.5 mIU/L in the first trimester and below 3.0 thereafter. Increase levothyroxine by 25 to 30% at confirmation of pregnancy (absorption is unchanged but demand rises).
- Hyperthyroidism in pregnancy — propylthiouracil in the first trimester, switch to carbimazole from 16 weeks (minimise both drugs' teratogenicity and hepatotoxicity in their respective windows). Avoid radioiodine (contraindicated) and beta-blockade beyond a short course (propranolol is associated with fetal growth restriction). Surgery, if needed, is in the second trimester. [1]
Subclinical thyroid disease
Subclinical hyperthyroidism (suppressed TSH, normal free T4 and T3) is common in older adults, particularly from toxic nodular goitre and excessive levothyroxine replacement. It is associated with atrial fibrillation (risk triples when TSH is below 0.1) and osteoporosis. The ATA recommends treatment when TSH is persistently below 0.1, especially in postmenopausal women and those with cardiac disease; for TSH 0.1 to 0.4, treatment is individualised [1].
Subclinical hypothyroidism (raised TSH, normal free T4) — treat if TSH above 10 mIU/L, or if symptomatic, anti-TPO positive, pregnant or planning pregnancy. For TSH 4.5 to 10, repeat in 3 to 6 months and monitor; many cases regress. [1]
High-yield exam discriminators and pitfalls
- Distinguish true hyperthyroidism from thyroiditis. High RAIU = Graves/TMNG/adenoma (treat with thionamide, radioiodine or surgery). Low RAIU = thyroiditis (self-limiting; NSAIDs or steroids, never antithyroid drugs).
- TRAb is the modern first-line discriminator in thyrotoxicosis — positive confirms Graves without needing a scan.
- Agranulocytosis on carbimazole — warn every patient about fever and sore throat in the first three months; check FBC if symptomatic.
- PTU in the first trimester and in thyroid storm — switch to carbimazole from 16 weeks.
- Iodine in thyroid storm must follow PTU by at least one hour — else it fuels new hormone synthesis.
- Myxoedema coma is a clinical diagnosis — hypothermia, hypoventilation, hyponatraemia, obtundation; treat empirically with IV levothyroxine and hydrocortisone.
- Graves orbitopathy — always ask about smoking. Smoking is the strongest modifiable risk factor; sight-threatening disease needs urgent combined care with ophthalmology.
- Bethesda III and IV are the zones of uncertainty — know the malignancy risks and the management.
- Medullary thyroid carcinoma — check RET and calcitonin. Familial MEN2 kindreds need prophylactic thyroidectomy.
- Anaplastic carcinoma in an older patient with a rapidly enlarging mass — goals of care discussion; the prognosis is very poor. [1]
Exam board facts
RACP DWE: Thyroid disorders are well represented — expect MCQs on thyrotoxicosis causes (Graves vs thyroiditis vs amiodarone), antithyroid drug pharmacology (carbimazole vs PTU, agranulocytosis, pregnancy), thyroid storm management (the sequencing of beta-blocker, PTU, iodine, hydrocortisone), myxoedema coma, and thyroid nodule Bethesda categorisation. [1]
RACP DCE long case: The classic thyroid long case is a multi-morbidity patient — Graves with atrial fibrillation and heart failure, or post-radioiodine hypothyroidism with dyslipidaemia and osteoporosis, or amiodarone-induced thyrotoxicosis in a cardiac patient — testing integrated management, problem-list synthesis, and shared decision-making on the definitive treatment. [1]
RACP DCE short case: The thyroid examination is a favourite. Present systematically: inspect from the front and side, ask the patient to swallow a sip of water (a goitre moves on swallowing), palpate from behind, percuss the sternum for retrosternal extension, auscultate for a bruit, then examine for the systemic features of thyroid disease (eye signs, hands, reflexes) [1].
MRCP Part 1/2: Thyroid pharmacology (carbimazole vs PTU, agranulocytosis, hepatotoxicity), thyroid storm management, and pregnancy-related thyroid disease are frequent. Bethesda categorisation and thyroid nodule management are common. [1]
MRCP PACES: Station 3 — thyroid examination and eye signs. Station 5 — endocrinology cases (Graves with orbitopathy, hypothyroidism with cardiac manifestations). [1]
ABIM: Endocrinology comprises approximately 9% of the exam. Thyroid disorders are core — diagnosis and management of thyrotoxicosis, hypothyroidism, thyroid storm, myxoedema coma, and thyroid nodules. [1]
Key trials and guidelines to know cold
| Source | Population | Key result |
|---|---|---|
| ATA/AETA 2016 [1] | Hyperthyroidism | Framework for cause discrimination (TRAb, uptake scan), three definitive treatments, radioactive iodine safety, pregnancy management |
| ATA 2014 [2] | Hypothyroidism | Levothyroxine monotherapy is standard; weight-based dosing; combination T4/T3 not recommended routinely |
| ATA 2015 [3] | Thyroid nodules and differentiated thyroid cancer | Ultrasound risk stratification, Bethesda categorisation, dynamic risk stratification for thyroid cancer |
| EUGOGO 2016 [4] | Graves orbitopathy | Smoking cessation, selenium for mild, IV methylprednisolone (cumulative 4.5g) for moderate-severe, urgent referral for sight-threatening |
| ETA 2018 [6] | Amiodarone-associated thyroid dysfunction | Type 1 (thionamide plus perchlorate) vs type 2 (glucocorticoid), mixed forms combined, individualised amiodarone decision |
| ATA 2015 (MTC) [7] | Medullary thyroid carcinoma | RET testing, prophylactic thyroidectomy in RET carriers, calcitonin doubling time as prognostic marker |
| Bethesda 2017 [8] | Thyroid FNA cytology | Six diagnostic categories with malignancy risks directing management |
| Caturegli 2014 [9] | Hashimoto thyroiditis | Clinical and diagnostic criteria; anti-TPO as serological marker |
| Fatourechi 2003 [5] | Subacute thyroiditis | Incidence cohort, 15% permanent hypothyroidism, steroid does not prevent recurrence |
Communication and shared decision-making
The choice between antithyroid drugs, radioiodine, and surgery in Graves disease is genuinely shared with the patient — there is no single right answer. The consultation framework: [1]
- Elicit the patient's understanding and goals — symptoms, side-effect concerns, fertility, eye disease, lifestyle.
- Present the three options honestly — antithyroid drugs (12 to 18 months, 40 to 50% remission, daily tablet, small risk of agranulocytosis); radioiodine (single outpatient treatment, definitive, high likelihood of permanent hypothyroidism and daily levothyroxine, worsens eye disease if active); surgery (definitive, hospital, small risk of nerve injury and hypoparathyroidism).
- Address specific concerns — radiation fear, the misconception that radioiodine causes cancer or infertility, the inconvenience of antithyroid monitoring, the scar of surgery.
- Document the shared decision and review the plan at intervals. [1]
For the hypothyroid patient with persistent symptoms despite a normal TSH, acknowledge the symptom burden honestly, screen for coexisting conditions (iron deficiency, vitamin D deficiency, depression, sleep apnoea, perimenopause), and discuss — without overpromising — the limited evidence for combination therapy. [1]
For the patient newly diagnosed with Graves orbitopathy, the message is direct: stop smoking is the single most impactful action; sight-threatening symptoms (visual blurring, double vision, eye pain, colour desaturation) warrant urgent referral. [1]
References and further reading
2016 ATA/AETA Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis [1]. 2014 ATA Guidelines for the Treatment of Hypothyroidism [2]. 2015 ATA Management Guidelines for Thyroid Nodules and Differentiated Thyroid Cancer [3]. 2016 EUGOGO Guidelines for Graves Orbitopathy [4]. Fatourechi et al on subacute thyroiditis [5]. 2018 ETA Guidelines for Amiodarone-Associated Thyroid Dysfunction [6]. 2015 ATA Revised Guidelines for Medullary Thyroid Carcinoma [7]. 2017 Bethesda System for Reporting Thyroid Cytopathology [8]. Caturegli et al on Hashimoto thyroiditis [9]. NICE NG145 (thyroid disease). Endocrine Society of Australia position statements.
References
- [1]Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis Thyroid, 2016.PMID 27521067
- [2]Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the treatment of hypothyroidism: prepared by the american thyroid association task force on thyroid hormone replacement Thyroid, 2014.PMID 25266247
- [3]Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer Thyroid, 2016.PMID 26462967
- [4]Bartalena L, Baldeschi L, Boboridis K, et al. The 2016 European Thyroid Association/European Group on Graves' Orbitopathy Guidelines for the Management of Graves' Orbitopathy Eur Thyroid J, 2016.PMID 27099835
- [5]Fatourechi V, Aniszewski JP, Fatourechi GZ, Atkinson EJ, Jacobsen SJ Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study J Clin Endocrinol Metab, 2003.PMID 12727961
- [6]Bartalena L, Bogazzi F, Chiovato L, Hubalewska-Dydejczyk A, Links TP, Vanderpump M 2018 European Thyroid Association (ETA) Guidelines for the Management of Amiodarone-Associated Thyroid Dysfunction Eur Thyroid J, 2018.PMID 29594056
- [7]Wells SA Jr, Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma Thyroid, 2015.PMID 25810047
- [8]Cibas ES, Ali SZ The 2017 Bethesda System for Reporting Thyroid Cytopathology Thyroid, 2017.PMID 29091573
- [9]Caturegli P, De Remigis A, Rose NR Hashimoto thyroiditis: clinical and diagnostic criteria Autoimmun Rev, 2014.PMID 24434360